Palliative Care Self-Learning Packet - Community Care of North
19
Palliative Care Self Learning Packet Sherri Branski RN, MSN, AccessCare Jamie Philway MSW Community Care of Wake and Johnston Counties Joanne Koster MEd, MSW,LCSW, Community Care of Eastern Carolina
Transcript of Palliative Care Self-Learning Packet - Community Care of North

Palliative Care
Self Learning Packet
Sherri Branski RN, MSN, AccessCare Jamie Philway MSW Community Care of Wake and Johnston Counties Joanne Koster MEd, MSW,LCSW, Community Care of Eastern Carolina

2
Palliative Care Self-Learning Packet
Objectives:
1. Provide an introduction to palliative care. 2. Describe key aspects of effective communication with palliative care patients. 3. Review NC advance directives and MOST forms. 4. Provide resources and references on palliative care, hospice, and end of life.
Created by:
Sherri Branski RN, MSN, AccessCare Jamie Philyaw MSW, Community Care of Wake and Johnston Counties Joanne Koster MEd, MSW,LCSW, Community Care of Eastern Carolina

3
Our Changing World The life expectancy of the population of the United States has dramatically increased over the last 100 years. In 1900 the average person lived to be about 50 years old. By the year 2000 life expectancy rose to 76 years old. In the 1900s people generally died of an acute illness such as pneumonia, and often over a short period of time. Today, the leading causes of death are chronic diseases such as heart failure, emphysema, stroke, and cancer. People often live for years with disabling symptoms before dying. Care has shifted from the home to institutions such as hospitals or nursing homes. Seventy percent of American citizens die in an institution.
Table 1: Cause of Death, and Demographic/Social Trends
Early 1900s Current Medicine’s Focus Comfort Cure
Cause of Death Infectious Diseases/ Communicable Diseases Chronic Illnesses
Age Adjusted Death Rate 1720 per 100,000 (1900)
865 per 100, 000 (1997)
Average Life Expectancy 50 76 Number of Persons
> 65 years old 3.1 million ~ 35 million (estimate for 2000)
Site of Death Home Institutions
Caregiver Family Strangers/ Health Care Providers
Disease/Dying Trajectory Relatively Short Prolonged Sources: Field, M. J., & Cassel, C. K. (1997). Approaching Death: Improving Care at the End of Life (Report of the Institute of Medicine Task Force). Washington, D.C.: National Academy Press. Reprinted with permission.
Ventura, S. J., Anderson, R. N., Martin, J. A., & Smith, B. L. (1998). Births and deaths: Preliminary data for 1997. National Vital Statistics Reports, 47(4). Hyattsville, MD: National Center for Health Statistics.
Administration on Aging. (2000). Older Population by Age: 1900 to 2050. http://www.aoa.dhhs.gov./aoa/stats/AgePop2050Chart-numbers.html
The Challenge of Chronic Care Caring for patients with chronic illnesses has challenged our health care system. A landmark study, called the SUPPORT study (1995) studied information sharing for seriously ill patients and their physicians. The study was conducted in five teaching hospitals in the US. Key findings include:
• Only 47% of physicians knew when their patients preferred to avoid CPR • 46% of do-not-resuscitate (DNR) orders were written within 2 days of death • 38% of patients who died spent at least 10 days in an intensive care unit (ICU)
4
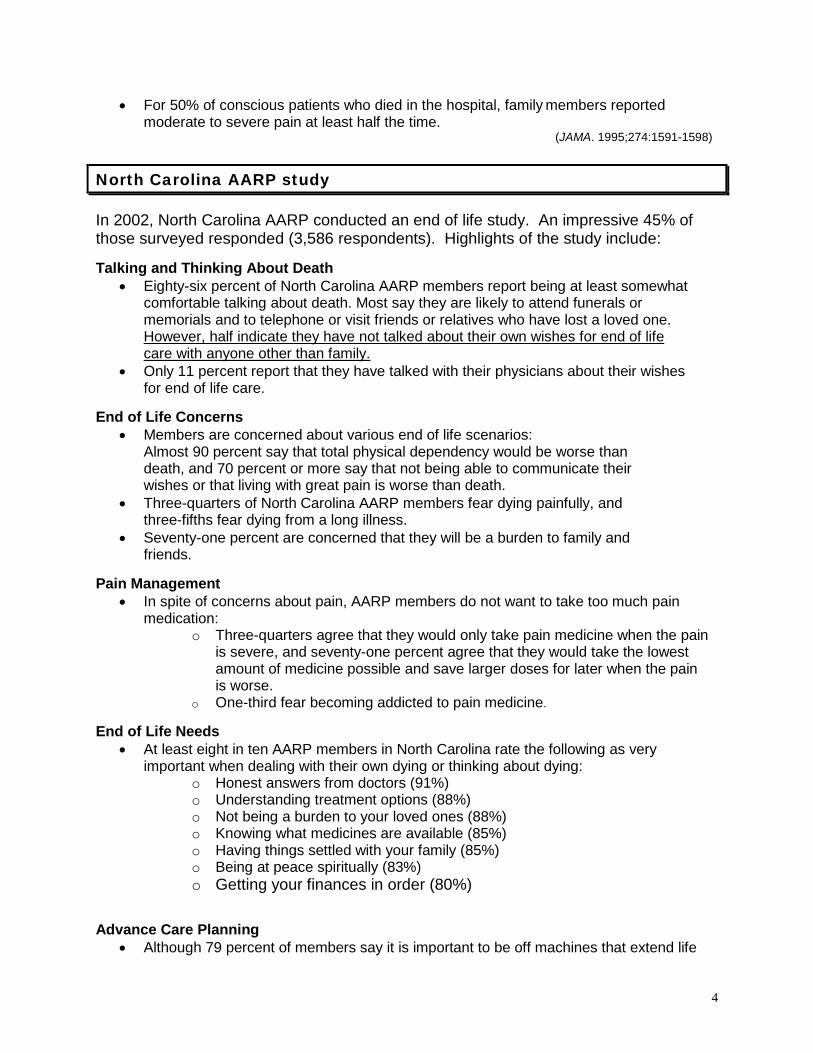
• For 50% of conscious patients who died in the hospital, family members reported moderate to severe pain at least half the time.
(JAMA. 1995;274:1591-1598)
North Carolina AARP study In 2002, North Carolina AARP conducted an end of life study. An impressive 45% of those surveyed responded (3,586 respondents). Highlights of the study include: Talking and Thinking About Death
• Eighty-six percent of North Carolina AARP members report being at least somewhat comfortable talking about death. Most say they are likely to attend funerals or memorials and to telephone or visit friends or relatives who have lost a loved one. However, half indicate they have not talked about their own wishes for end of life care with anyone other than family.
• Only 11 percent report that they have talked with their physicians about their wishes for end of life care.
End of Life Concerns
• Members are concerned about various end of life scenarios: Almost 90 percent say that total physical dependency would be worse than death, and 70 percent or more say that not being able to communicate their wishes or that living with great pain is worse than death.
• Three-quarters of North Carolina AARP members fear dying painfully, and three-fifths fear dying from a long illness.
• Seventy-one percent are concerned that they will be a burden to family and friends.
Pain Management
• In spite of concerns about pain, AARP members do not want to take too much pain medication:
o Three-quarters agree that they would only take pain medicine when the pain is severe, and seventy-one percent agree that they would take the lowest amount of medicine possible and save larger doses for later when the pain is worse.
o One-third fear becoming addicted to pain medicine. End of Life Needs
• At least eight in ten AARP members in North Carolina rate the following as very important when dealing with their own dying or thinking about dying:
o Honest answers from doctors (91%) o Understanding treatment options (88%) o Not being a burden to your loved ones (88%) o Knowing what medicines are available (85%) o Having things settled with your family (85%) o Being at peace spiritually (83%) o Getting your finances in order (80%)
Advance Care Planning
• Although 79 percent of members say it is important to be off machines that extend life
5
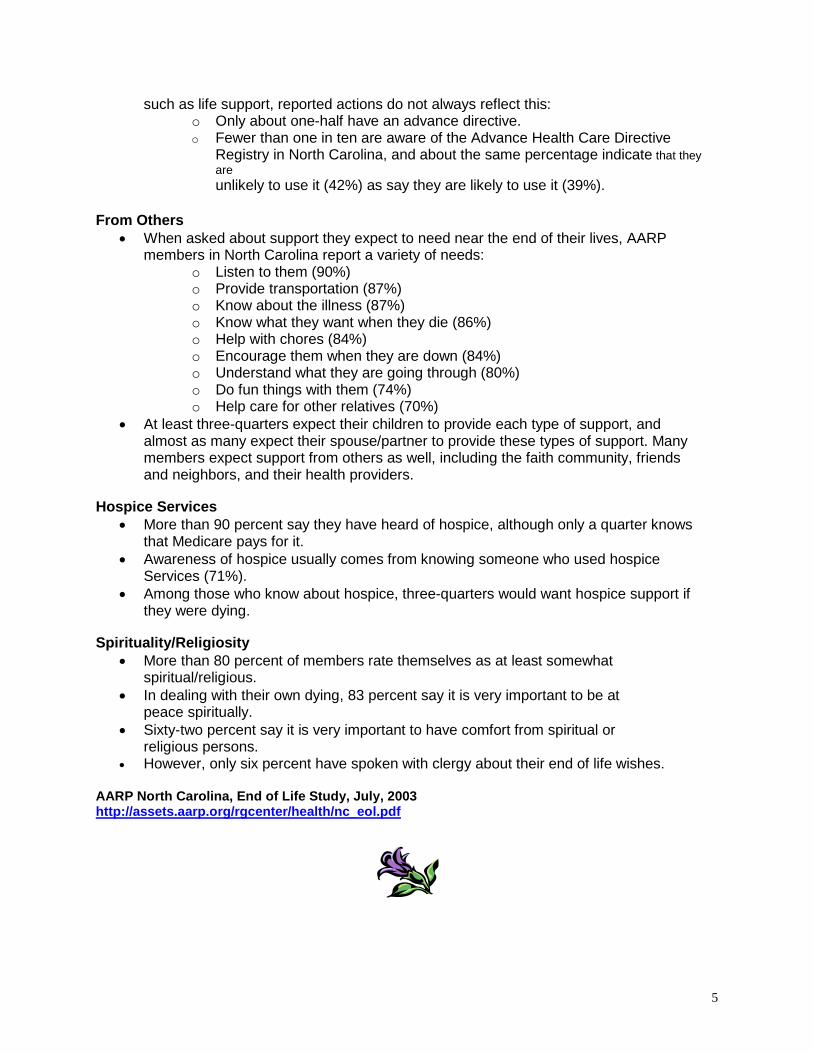
such as life support, reported actions do not always reflect this: o Only about one-half have an advance directive. o Fewer than one in ten are aware of the Advance Health Care Directive
Registry in North Carolina, and about the same percentage indicate that they are unlikely to use it (42%) as say they are likely to use it (39%).
From Others
• When asked about support they expect to need near the end of their lives, AARP members in North Carolina report a variety of needs:
o Listen to them (90%) o Provide transportation (87%) o Know about the illness (87%) o Know what they want when they die (86%) o Help with chores (84%) o Encourage them when they are down (84%) o Understand what they are going through (80%) o Do fun things with them (74%) o Help care for other relatives (70%)
• At least three-quarters expect their children to provide each type of support, and almost as many expect their spouse/partner to provide these types of support. Many members expect support from others as well, including the faith community, friends and neighbors, and their health providers.
Hospice Services
• More than 90 percent say they have heard of hospice, although only a quarter knows that Medicare pays for it.
• Awareness of hospice usually comes from knowing someone who used hospice Services (71%).
• Among those who know about hospice, three-quarters would want hospice support if they were dying.
Spirituality/Religiosity
• More than 80 percent of members rate themselves as at least somewhat spiritual/religious.
• In dealing with their own dying, 83 percent say it is very important to be at peace spiritually.
• Sixty-two percent say it is very important to have comfort from spiritual or religious persons.
• However, only six percent have spoken with clergy about their end of life wishes. AARP North Carolina, End of Life Study, July, 2003 http://assets.aarp.org/rgcenter/health/nc_eol.pdf

6
A Better Care System Seven Promises There are probably a number of ways to construct a vision of a better care system. One that has a special power is to think through the image of a single health care provider talking with a single sick and frightened patient and trying to imagine what that provider could promise -- in a care system that really worked the way it should. For patients with advanced stages of serious illnesses, it is just not possible to promise cure or restoration of health. What would matter to such a patient? Here are the seven promises that really seem to make a difference. In each case, there is a short name for the promise, its core statement, and a few examples of what it might mean to put practices in place to deliver on that promise. 1. GOOD MEDICAL TREATMENT: You will have the best of medical treatment, aiming to prevent
exacerbation, improve function and survival, and ensure comfort.
• Patients will be offered proven diagnosis and treatment strategies to prevent exacerbations and enhance quality of life, as well as to delay disease progression and death.
• Medical interventions will be in accord with best available standards of medical practice, and evidence-based when possible.
2. NEVER OVERWHELMED BY SYMPTOMS: You will never have to endure overwhelming pain,
shortness of breath, or other symptoms.
• Symptoms will be anticipated and prevented when possible, evaluated and addressed promptly, and controlled effectively.
• Severe symptoms—such as shortness of breath—will be treated as emergencies. • Sedation will be used when necessary to relieve intractable symptoms near the end of life.
3. CONTINUITY, COORDINATION, AND COMPREHENSIVENESS: Your care will be continuous,
comprehensive, and coordinated.
• Patients and families can count on having certain professionals to rely upon at all times. • Patients and families can count on an appropriate and timely response to their needs. • Transitions between services, settings, and personnel are minimized in number and made to
work smoothly. 4. WELL-PREPARED, NO SURPRISES: You and your family will be prepared for everything that is
likely to happen in the course of your illness.
• Patients and families come to know what to expect as the illness worsens, and what is expected of them.
• Patients and families receive supplies and training needed to handle predictable events. 5. CUSTOMIZED CARE, REFLECTING YOUR PREFERENCES: Your wishes will be sought and
respected, and followed whenever possible.
• Patients and families come to know the alternatives for services, and expect to make choices that matter.
• Patients never receive treatments they refuse. • Patients who want to live out the end of life at home, usually can.
6. USE OF PATIENT AND FAMILY RESOURCES (Financial, Emotional, and Practical): We will help
the patient and family to consider their personal and financial resources and we will respect their choices about the use of their resources.

7
• Patients and families will be aware of services available in their community and the costs of
those services. • Family caregivers’ concerns will be discussed and addressed. Respite, volunteer, and home
aide care will be part of the care plan when appropriate. 7. MAKE THE BEST OF EVERY DAY: We will do all we can to see that you and your family will have
the opportunity to make the best of every day.
• The patient is treated as a person, not a disease, and what is important to the patient is important to the care team.
• The care team responds to the physical, psychological, social, and spiritual needs of patient and family.
• Families are supported before, during, and after the patient’s death. Source: Seven Promises. Americans for Better Care of the Dying Reprinted with permission.
Palliative Care Palliative care has emerged in response to the needs of our chronically ill population (and to the delivery of those seven promises). Palliative care is defined by the World Health Association as:
An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Palliative care:
• provides relief from pain and other distressing symptoms; • affirms life and regards dying as a normal process; • intends neither to hasten or postpone death; • integrates the psychological and spiritual aspects of patient care; • offers a support system to help patients live as actively as possible until death; • offers a support system to help the family cope during the patients illness and in
their own bereavement; • uses a team approach to address the needs of patients and their families,
including bereavement counseling, if indicated; • will enhance quality of life, and may also positively influence the course of illness; • Is applicable early in the course of illness, in conjunction with other therapies that
are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical implications. http://www.who.int/cancer/palliative/definition/en/
8
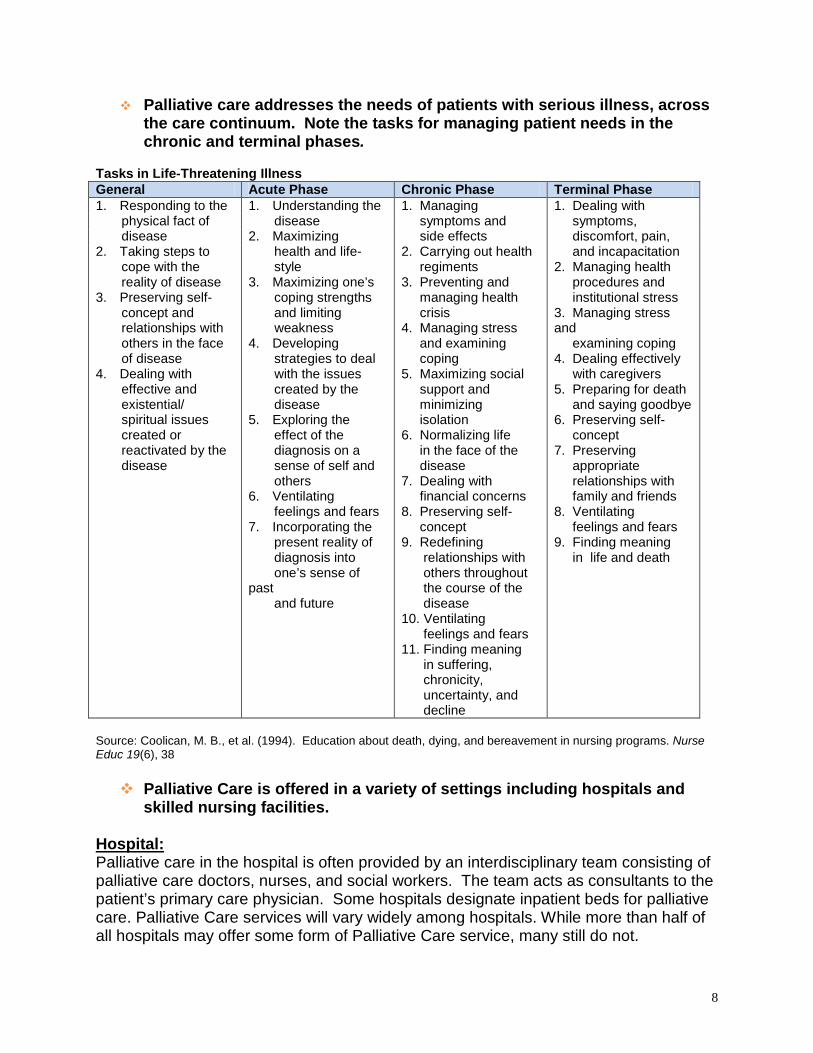
Palliative care addresses the needs of patients with serious illness, across the care continuum. Note the tasks for managing patient needs in the chronic and terminal phases.
Tasks in Life-Threatening Illness General Acute Phase Chronic Phase Terminal Phase 1. Responding to the physical fact of disease 2. Taking steps to cope with the reality of disease 3. Preserving self- concept and relationships with others in the face of disease 4. Dealing with effective and existential/ spiritual issues created or reactivated by the disease
1. Understanding the disease 2. Maximizing health and life- style 3. Maximizing one’s coping strengths and limiting weakness 4. Developing strategies to deal with the issues created by the disease 5. Exploring the effect of the diagnosis on a sense of self and others 6. Ventilating feelings and fears 7. Incorporating the present reality of diagnosis into one’s sense of past and future
1. Managing symptoms and side effects 2. Carrying out health regiments 3. Preventing and managing health crisis 4. Managing stress and examining coping 5. Maximizing social support and minimizing isolation 6. Normalizing life in the face of the disease 7. Dealing with financial concerns 8. Preserving self- concept 9. Redefining relationships with others throughout the course of the disease 10. Ventilating feelings and fears 11. Finding meaning in suffering, chronicity, uncertainty, and decline
1. Dealing with symptoms, discomfort, pain, and incapacitation 2. Managing health procedures and institutional stress 3. Managing stress and examining coping 4. Dealing effectively with caregivers 5. Preparing for death and saying goodbye 6. Preserving self- concept 7. Preserving appropriate relationships with family and friends 8. Ventilating feelings and fears 9. Finding meaning in life and death
Source: Coolican, M. B., et al. (1994). Education about death, dying, and bereavement in nursing programs. Nurse Educ 19(6), 38 Palliative Care is offered in a variety of settings including hospitals and
skilled nursing facilities. Hospital:
Palliative care in the hospital is often provided by an interdisciplinary team consisting of palliative care doctors, nurses, and social workers. The team acts as consultants to the patient’s primary care physician. Some hospitals designate inpatient beds for palliative care. Palliative Care services will vary widely among hospitals. While more than half of all hospitals may offer some form of Palliative Care service, many still do not.

9
Skilled Nursing Facilities: A recent report developed by the Center to Advance Palliative Care revealed four primary models utilized in progressive US skilled nursing homes. However most skilled nursing facilities still do not have formal palliative care services. 1. Palliative Care Consultation Service Palliative care providers who are not employed by the nursing home provide and bill for consultative services to residents as requested by the nursing home Medical Director, the patient’s attending physician or the nursing home Director of Nursing. 2. Hospice-based Palliative Care Consult Service Professional staff employed by a local hospice provides non-hospice palliative care Consultative services as requested by the nursing home Medical Director, the patient’s attending physician or the nursing home Director of Nursing. 3. Nursing Home Services Integrated Palliative Care Many nursing homes have embraced quality initiatives, such as pain and symptom management. 5.3 4. Hospice Care Hospice-eligible nursing home residents receive specialized end-of-life palliative care services from contracted hospice providers. Improving Palliative Care in Nursing Homes. June 2007. www.capc.org
Palliative care may be provided at any time during a person’s illness, even from the time of diagnosis. And, it may be given at the same time as curative treatment.
For additional references on palliative care go to: http://www.getpalliativecare.org/providers

10
What is hospice care and how does it differ from palliative care?
Hospice care is a form of palliative care that provides care to patients facing a life-limiting illness or injury.
Per the National Hospice and Palliative Care Organization (NHPCO) the focus of hospice relies on the belief that each of us has the right to die pain-free and with dignity, and that our loved ones will receive the necessary support to allow us to do so.
• Hospice focuses on caring, not curing and, in most cases; care is provided in the person’s home.
• Hospice care also is provided in freestanding hospice centers, hospitals, and nursing homes and other long-term care facilities.
• Hospice services are available to patients of any age, religion, race, or illness. • Hospice care is covered under Medicare, Medicaid, most private insurance
plans, HMOs, and other managed care organizations. http://www.caringinfo.org/LivingWithAnIllness/Hospice.htm
Medicare Hospice benefits require:
• Medicare Part A (Hospital Insurance) eligibility • Physician and the hospice medical director certify that patient is terminally ill and
has 6 months or less to live if the illness runs its normal course. • The patient signs a statement choosing hospice care instead of other Medicare-
covered benefits to treat the terminal illness.* • Patient receives care from a Medicare-approved hospice program.
* Medicare will still pay for covered benefits for any health problems that are not related to patient’s terminal illness. http://www.medicare.gov/publications/Pubs/pdf/02154.pdf
North Carolina Medicaid Hospice benefits:
• NC Medicaid benefits also require a physician and the hospice medical director certify that patient is terminally ill and has 6 months or less to live if the illness runs its normal course
• Hospice services are covered when provided in the following locations: a. The recipient’s private residence b. An adult care home under a written agreement with the hospice agency c. A hospice residential care facility or hospice inpatient unit d. A hospital, nursing facility, or ICF-MR under a written agreement with the
hospice agency • The patient must sign an election statement form which waives rights to certain
Medicaid services. See: http://www.ncdhhs.gov/dma/mp/3D.pdf

11
To find a hospice agency in North Carolina go to: http://carolinasendoflifecare.org/
“You matter because you are you, and you matter until the last moment of your life. We will do all we can, not only to help you die peacefully, but to live until you die.”
Dame Cicely Saunders, Founder of the Modern Hospice Movement
Communication
Effective communication with a patient/family unit is a crucial requirement to success in palliative care. A terminal illness is a family experience. In a recent study when nurses were asked what they wish they were taught in nursing school curriculum related to the terminally ill, the number one response was “how to talk to patients/families about dying.” (Coyne, 1999). The role of communication includes imparting necessary medical information so individuals may make informed decisions related to care. This may also help dispel preconceived notions/myths about illness or treatment. Communication also involves strong collaboration between members of the interdisciplinary team. Patient/Family Expectations Based on the expectations expressed by patients/families experiencing life-limiting diseases, it is important to communicate to patients and families that:
a. You will be honest and truthful. b. You will not abandon them. c. You will elicit and request their values and goals and will help as much
as is possible to achieve these. d. You will help them explore their realistic options. e. When assisting families to make decisions, you will consider the
overall situation (support systems, economics, technical aspects, locality and other issues).
f. You will respond to their questions within a reasonable time and encourage their questions as well.

12
g. You will ask—”What would you like me to do? What are your expectations? What do you need?”
h. You will work to insure that the entire health care team understands the care plan, communicates its goals to one another, and contributes to its development.
i. When you don’t know what to do, you will seek help. j. You will ask yourself, “What would I do if this was my family member?” k. You will take the time to listen.
Remember to be aware and sensitive to cultural differences, which may be related to:
a. sexual orientation b. religion c. age d. ethnicity e. gender f. past experiences g. social or economic status h. language
Listening
1. Sensitive listening is being present, not just physically, but mentally and emotionally as well.
2. Listening/presence occurs at five different levels, each requiring greater
energy and involvement. It’s like walking up steps...the higher you climb, the greater your energy and involvement (See Figure 1).
3. Being present and being silent are valuable communication skills. Figure 1: Listening Steps
Ener
gy &
Invo
lvem
ent
Helping Others/ Active Empathizing
Analyzing & Evaluating Information
Retaining Information
Understanding
Hearing
Adapted: Ray, M. C. (1992). I’m Here to Help (A Hospice Worker’s Guide to Communicating with Dying People and Their Loved Ones). New York, NY: Bantam Books. Reprinted with permission from Bantam Books, a division of Random House, Inc.

13
Guidelines for encouraging free conversation (Buckman, 1998)
1. Setting the right atmosphere a. Get comfortable and relay to the family member that you want to spend
some time with them (i.e. sitting down, leaning forward). b. Maintain undistracted eye contact. However, some cultures will avoid
direct eye contact. c. Interruptions are bound to happen. Focus back on the conversation as
quickly as possible. d. Learn and maintain a comfortable distance for you and the patient or
family member.
2. Does the patient or family member want to talk? a. They may be too tired. b. They may have had a conversation with someone else you are
unaware of that meets their needs. c. Ask if they feel like talking before attempting to engage them in a deep
conversation.
3. Attentive listening a. Don’t anticipate what may be said; listen. b. Don’t interrupt. Listen patiently until there is a break in the
conversation. c. Encourage the patient or family member to talk. This can be done by
using simple methods: 1) Nodding one’s head. 2) Comments like “I see,” or “Tell me more”. 3) Repeating 2-3 words from their last sentence, “...you were shocked
by the diagnosis”. 4) Reflection - “So you mean that...” or, “If I understand what you’re
saying, you’re feeling...” 5) Listening to patients and families is much like providing the
attention you would give a good friend who is sharing their concerns, their heart, and their joys.
6) Ask open-ended questions (e.g. “What does this mean to you?) d. Silence and nonverbal communication
1) Silence doesn’t always mean the person doesn’t want to talk. It may mean that they are in deep thought about something painful or sensitive. Give the person time without making them feel rushed.

14
2) Sometimes you may not know what to say. There are times when there isn’t anything to say. Saying nothing and remaining close can sometimes offer more comfort than words. Your presence and “being with” are vital forces.
3) Sometimes nonverbal communication techniques are used because the person doesn’t know how to express his/her needs. A patient who is frowning, fidgeting, and breathing deeply may be at a loss for words to express their anxiety.
e. Don’t be afraid to acknowledge your feelings 1) It’s okay to say things like “This is difficult for me to talk about” or “I
don’t know what to say.” The person feels relieved because they can sense when the nurse doesn’t feel comfortable. It also relieves pressure for the nurse in that he/she doesn’t have to have all of the answers.
2) Many patients/family members have asked variations of “Why is this happening?” It is okay to say “I don’t know. I wish I had an answer, but I don’t.” It is helpful to extend touch or hold their hand when discussing this so they can know that while we “don’t know,” we do really care, we can see their pain and it matters to us.
f. Avoid misunderstandings 1) If you are sure you understand what the person is saying,
acknowledge so. If you are unsure, ask him/her to clarify for you. 2) “Help me understand what you mean” is a gentle way to clarify.
g. Don’t change the subject; this is a natural response we often use to
avoid difficult conversations. h. Take your time in giving advice
1) Try not to give advice if at all possible unless asked for. 2) If you do give advice, do it unassumingly.
a) “Have you thought about...” b) “A friend of mine once tried...” c) “When I went through this with my friend, mother, etc. I found
this to be helpful...” i. Encourage Reminiscing
1) Giving patients and families an opportunity to reminisce and “tell their story” provides reassurance that their lives had meaning.
2) Reminiscing helps to ease the intensity of the present reality by incorporating memories and the reality of the relationship with that person.

15
Questions to Ask Patients & Families to Elicit End-of-life Goals
• What do you think is most important to your family?
• What are your needs at this time?
• What are your concerns at this time/and for the future?
• What do you want to accomplish or do?
• What do you wish you could still do?
• What are the things that bring you joy/comfort?
• What is important for you to maintain control over?
• What do you feel you have control over...disease/pain/decisions?
• What do you know about your illness/disease? Is there anything else you would like to know?
• How do you feel about your treatments (medications, radiation, chemo, DNR)?
• If you have pain, what would be an acceptable pain level for you on a 0-10 scale?
• What activities such as music, art, reading, massage, touch provide peace or comfort to you?
• What are the most important relationships in your life?
• Is there anyone you would like to see/talk to/visit with?
• What are you proud of? What are your greatest achievements?
• How and where do you want to live for the rest of your life?
• Where (environment) are you most comfortable?
• What are you hopeful about?
• What spiritual or religious practices bring you comfort?
• Is spiritual peace important to you? What would help you achieve spiritual peace?
Source: The Hospice of the Florida Suncoast, February 2001 printed with permission.
Communication Module, ELNEC The End-of-Life Nursing Education Consortium (ELNEC) is a national end-of-life care nursing education initiative administered by the American Association of Colleges of Nursing, Washington D.C., and City of Hope National Medical Center, Duarte, California. The project is funded by the Robert Wood Johnson Foundation. Materials are copyrighted by the American Association of Colleges of Nursing and City of Hope National Medical Center, and are used with permission. Further information about the ELNEC project can be found at www.aacn.nche.edu/elnec.

16
The CCNC Comprehensive Health Assessment offers the following questions for care managers to offer to patients as invitations to advanced care planning discussions:
a. If you became seriously ill, how sure are you that you would be treated according to your wishes and values? (Very sure, fairly sure, not sure)
b. Do you have someone who can make health care decisions for you if you were unable to speak for yourself? (HCPOA, natural surrogate, no, not sure)
c. Do you have opinions about how you would want to be treated if you had a serious or life threatening illness? (yes, no)
d. Are your opinions about how you would want to be treated understood by your regular doctor? (yes, no, not sure)
e. Have you put your opinions in writing? (living will, Five Wishes, DNR, MOST, no, not sure)
f. Is there a symptom(s) that most affects your quality of life or that keeps you from doing what you want to do daily? (Y/N) (examples: pain, shortness of breath, nausea, extreme tiredness, other)
g. How sure are you that you know how to get help if this symptom gets worse? (Very sure, fairly sure, not sure)
These questions can be further modified by care managers for discussions with pediatric patients and their families.
a. If your child has been diagnosed with a serious progressive condition, what will help you to feel confident in your child’s care?
b. Are your ideas about what you hope and want for your child’s treatment understood by your child’s regular doctor(s)?
c. Do you know all the doctors who are a part of your child’s care team?
d. Do you feel that you have a part in decision making/establishing goals for your child’s care?

17
e. What are your/your child’s needs at this time?
f. We want you and your child to be comfortable. What does that mean to you and your family?
g. Is there a symptom that affects your child’s ability to do what he/she wants or loves to do?
h. Do you know how to get help for your child’s care if you need it?
Determining Patient’s Preferences: Advance Care Planning
Advanced Care Planning is when a patient makes decisions about the kind of medical treatment that they would want at the end of life. Advanced Directives are legal documents in which a person gives written instructions about their wishes for health care if, in the future, they are unable to communicate their desires on their own behalf. Health Care Power of Attorney (HCPOA): A legal document authorizing a designated individual to make all necessary medical decisions on behalf of another person once a physician has determined the person to not be able to make these decisions for him/herself. Living Will: This advanced directive is a legal document expressing one’s preferences for the use of any treatment modalities in order to sustain life, when it has been medically determined that one is terminally ill or unable to benefit from further medical treatment. North Carolina MOST Form (Medical Orders for Scope of Treatment): A medical order set designed to help medical professionals know and honor the treatment wishes of their patients. The MOST form is intended to enhance the quality of a person’s care and to complement the advance care planning process. This form provides a summary of treatment preferences in a clear medical order. The MOST form is portable and may follow the patient from one setting to another. The MOST form is completed in concert with a Physician and is intended for those patients with advanced chronic illness.

18
See the DMA website for a patient education brochure on advance care planning (included in attachments).
http://www.ncdhhs.gov/dma/medicaid/AdvancedDirectCondensed.pdf
See attachments for copies of Advanced Directives forms and MOST form.
Attachments:
DMA brochure on advance directives
http://www.ncdhhs.gov/dma/medicaid/AdvancedDirectCondensed.pdf
NC Advance Directives form (Living Will) http://www.nclifelinks.org/
NC Advance Directives form (Health Care Power of Attorney) http://www.nclifelinks.org/
Five Wishes advanced care planning guide http://www.fivewishes.org/
NC Most Form http://www.ncdhhs.gov/dhsr/EMS/pdf/ncmostform.pdf
Frequently asked questions about the MOST form http://www.ncmedsoc.org/non_members/public_resources/eol/FinalMOSTFAQs1.pdf

19
Helpful Websites
Get Palliative Care: http://www.getpalliativecare.org/resources Center for the Advancement of Palliative Care: http://www.capc.org/ National Hospice and Palliative Care Organization: http://www.nhpco.org/templates/1/homepage.cfm Carolina Center for Hospice and End of Life Care: http://www.cchospice.org/ End of Life/Palliative Education Resource Center: http://www.eperc.mcw.edu/EPERC American Academy of Hospice and Palliative Medicine: http://www.aahpm.org/resources/ End of Life Nursing Education Consortium: http://www.aacn.nche.edu/ELNEC/index.htm Promoting Excellence in End of Life Care: http://www.promotingexcellence.org/ Education in Palliative and End of Life Care: http://www.epec.net/ Caring Connections: http://www.caringinfo.org/i4a/pages/index.cfm?pageid=1 NC Medical Society: http://www.ncmedsoc.org/pages/public_health_info/end_of_life.html