Pain as an Embodied Emotion - University of Readingxy905589/Salomons_NoE_Final_APA.pdf · Pain as...
15
Pain as an Embodied Emotion Since William James first proposed somatic responses as the foundation of emotion in the 19 th century, there has been a vigorous debate about the role of the body in shaping emotional experience. James’ original view was that the mind perceives a physiological response and that the particular nature of this peripheral response determines the emotion.(James, 1884) Based on evidence that de-afferentation left emotional responses intact and that physiological responses are relatively slow and non-specific, the Canon-Bard theory proposed that brain and somatic responses to stimuli occur simultaneously and relatively independent of each other.(Cannon, 1927) Later cognitive theories suggested that it is the brain’s evaluation of somatic signals that determines the emotional experience.(Lazarus & Folkman,, 1984) Despite these challenges and alternative theories, James’ original theory remains influential, spawning new theories of how the peripheral responses contribute to emotional experience(Kreibig, 2010). These include Damassio’s Somatic Marker Hypothesis, which emphasizes the role of somatic signals in generating emotions, particularly within the context of decision making. The Somatic Marker Hypothesis outlines a more active role for the brain than James’ original theory, allowing that the brain encodes somatic states in a way that allows emotional states to occur independent of peripheral input.(Damasio, 1991) The nature of the interaction between brain and body that gives rise to specific emotions continues to be a subject of intense study. One approach to better understanding this interaction is to study one specific emotional experience to determine how each part of the body-brain axis contributes to what makes that emotion unique. In this respect, pain might be particularly instructive. The International Association for the Study of Pain has defined pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.(Merskey, Bogduk, & ., 1994) Within the context of this discussion, it is noteworthy that pain is viewed as both a sensory and emotional experience, but also that potential damage to the body is at the core of the experience. The fact that the emotional experience of pain is focused on events occurring in the body, and that it is encoded along with sensory information such as location and temporal characteristics suggests that information from the body might play a particularly strong role in shaping the emotional experience. As such, it might serve as a model for how the body can contribute to an emotion in a way consistent with James’ original vision. IS PAIN SPECIFIED IN THE BODY? Viewed within a Jamesian framework, we would expect the specific emotional experience of pain to correspond to a specific somatic representation. Such a representation might take the form of receptors that are largely specialized for processing nociceptive inputs. The existence of primary afferent nociceptive receptors has been central to a long standing historical debate regarding whether pain is the product of specific, labelled lines, or a pattern of distributed inputs. The specificity account is commonly associated with Rene Descartes, and was accompanied by Louis Lafarge’s famous diagram (see Figure 1 below) which conveyed Descartes’ hypothesis that that the pain system consists of a direct line from the skin to a pain centre in the brain.(Descartes, Clerselier, LaForge, & Schuyl, 1664) Activation of this line was viewed as necessary and sufficient for the experience of pain, with the implication that the pain experience corresponded to peripheral input in a 1:1 fashion. The brain is viewed largely as a relay centre for messages from the periphery, as evidenced by Descartes’ metaphor of the brain as a bell to be rung by tugging on a string in the periphery.
Transcript of Pain as an Embodied Emotion - University of Readingxy905589/Salomons_NoE_Final_APA.pdf · Pain as...

Pain as an Embodied Emotion
Since William James first proposed somatic responses as the foundation of emotion in the 19th century, there has been a vigorous debate about the role of the body in shaping emotional experience. James’ original view was that the mind perceives a physiological response and that the particular nature of this peripheral response determines the emotion.(James, 1884) Based on evidence that de-afferentation left emotional responses intact and that physiological responses are relatively slow and non-specific, the Canon-Bard theory proposed that brain and somatic responses to stimuli occur simultaneously and relatively independent of each other.(Cannon, 1927) Later cognitive theories suggested that it is the brain’s evaluation of somatic signals that determines the emotional experience.(Lazarus & Folkman,, 1984) Despite these challenges and alternative theories, James’ original theory remains influential, spawning new theories of how the peripheral responses contribute to emotional experience(Kreibig, 2010). These include Damassio’s Somatic Marker Hypothesis, which emphasizes the role of somatic signals in generating emotions, particularly within the context of decision making. The Somatic Marker Hypothesis outlines a more active role for the brain than James’ original theory, allowing that the brain encodes somatic states in a way that allows emotional states to occur independent of peripheral input.(Damasio, 1991)
The nature of the interaction between brain and body that gives rise to specific emotions continues to be a subject of intense study. One approach to better understanding this interaction is to study one specific emotional experience to determine how each part of the body-brain axis contributes to what makes that emotion unique. In this respect, pain might be particularly instructive. The International Association for the Study of Pain has defined pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.(Merskey, Bogduk, & ., 1994) Within the context of this discussion, it is noteworthy that pain is viewed as both a sensory and emotional experience, but also that potential damage to the body is at the core of the experience. The fact that the emotional experience of pain is focused on events occurring in the body, and that it is encoded along with sensory information such as location and temporal characteristics suggests that information from the body might play a particularly strong role in shaping the emotional experience. As such, it might serve as a model for how the body can contribute to an emotion in a way consistent with James’ original vision.
IS PAIN SPECIFIED IN THE BODY?
Viewed within a Jamesian framework, we would expect the specific emotional experience of pain to correspond to a specific somatic representation. Such a representation might take the form of receptors that are largely specialized for processing nociceptive inputs. The existence of primary afferent nociceptive receptors has been central to a long standing historical debate regarding whether pain is the product of specific, labelled lines, or a pattern of distributed inputs. The specificity account is commonly associated with Rene Descartes, and was accompanied by Louis Lafarge’s famous diagram (see Figure 1 below) which conveyed Descartes’ hypothesis that that the pain system consists of a direct line from the skin to a pain centre in the brain.(Descartes, Clerselier, LaForge, & Schuyl, 1664) Activation of this line was viewed as necessary and sufficient for the experience of pain, with the implication that the pain experience corresponded to peripheral input in a 1:1 fashion. The brain is viewed largely as a relay centre for messages from the periphery, as evidenced by Descartes’ metaphor of the brain as a bell to be rung by tugging on a string in the periphery.

FIGURE 1: Lafarge’s depiction of a direct line for pain
Muller’s doctrine of specific nerve energies(Muller, 1840) provided early theoretical support for the specificity view. Muller posited that perceptual experiences are the product of the pathways through which they are transmitted. The brain receives information about the external world from sensory nerves, with the quality of sensation determined by specific coding (which Mueller viewed as either a product of the specific energy of individual sensory nerves or the properties of the brain region on which they terminate). This theory was supported within the tactile domain by the discovery of receptors for specific tactile experiences (e.g. Meissner’s corpuscles responding to touch, Ruffini’s corpuscles responding to warmth and Krause end bulbs responding to cool). Maximillion von Frey hypothesized that in addition to these specific receptors for touch, warmth and cold, the sensation of pain was subserved by free nerve endings.(vonFrey, n.d.) Based on the work of Blix, Goldscheider and Donaldson, von Frey further suggested that there was anatomical specificity for these various tactile sensations, such that stimulation of different areas of skin would preferentially produce percepts corresponding to the type of receptors.(Norrsell, Finger, & Lajonchere, 1999) This “anatomical assumption” has not been supported by subsequent research but the “physiological assumption” of receptor specificity remained influential and critical to subsequent research on nociception-specific receptors.(Melzack & Wall, 2004)
An alternate, pattern-based theory was proposed by Nafe in1929.(Nafe, 1929) Nafe suggested that it was not the specificity of the receptor that determined the experience, but rather the spatial and temporal pattern of discharge, which changed according to the type of stimulation. This pattern of discharge could also be coded across a population of afferent fibres, explaining the variation in perceptual experience. While this theory was strongly challenged at the level of primary afferents (see below), it has remained highly influential, particularly at higher levels of the neuroaxis.

The specificity account of pain was reinvigorated by the discovery of peripheral nerve endings selectively responsive to stimuli in the noxious range. Sherrington’s prescient description of “nocicipient” cutaneous end-organs specific for noxious stimuli(Sherrington, 1903) followed on from von Frey’s theories and was later validated by the discovery of “nociceptors”: primary afferents responsive only to stimuli that could result in potential injury. Some of these were specific to mechanical stimulation(Burgess & Perl, 1967) while others were polymodal(Bessou & Perl, 1969).
As our understanding of nociceptors has grown, the variety and specificity of information sent to the spinal cord has become apparent, with the structure of the nociceptor supporting the perceptual, emotional and behavioural response to stimulation. For example, A-delta fibres are small (1-6μm), myelinated fibres that convey nociceptive information quickly (5-36 m/s), allowing them to contribute to “first pain”, while C-fibres are unmyelinated fibers whose slow (0.2-1.5 m/s) but sustained firing is responsible for a lasting “second pain”. These fibres are, in turn, commonly associated with different behavioural responses, with first pain eliciting immediate withdrawal responses and second pain associated with behaviours aimed at protecting the body and nurturing injury. Behavioural routines are further specified by nociceptors specifically responsive to different modalities of noxious stimulation (e.g., hot, cold, chemical etc.).(Basbaum, Bautista, Scherrer, & Julius, 2009; Cavanaugh et al., 2009; Julius & Basbaum, 2001) The heterogeneity and functional specificity of nociceptors has led many contemporary theorists to conclude that the specificity account of pain was largely correct, at least to the level of the spinal cord (cf. Editorial “Specificity versus patterning theory: continuing the debate” by Allan Basbaum and accompanying discussion by Woolf, Casey, Fields and Apkarian, Pain Research Forum, 2011: http://www.painresearchforum.org/forums/discussion/7347-specificity-versus-patterning-theory-continuing-debate).
This pre-spinal level of specificity suggests that the emotional experience of pain can be largely shaped by the peripheral input that is received. First, firing of nociceptors automatically signals the potential for injury, therefore conferring biological significance on the eliciting stimulus and priming threat routines. Furthermore, the ability of nociceptors to encode for the modality of input alongside sensory information such as location, and temporal and spatial patterning gives them a powerful influence over the emotional and behavioural response. A sudden, stabbing pain in the abdomen is a very different emotional experience than a slow throbbing pain in the toe, even in the absence of top-down information about what the pains might signify, and these varying emotional experiences are largely shaped by the different primary afferent information received. Even when previous knowledge and top-down cognitive and emotional responses modify pain, these top-down influences are largely limited by the information specified by peripheral input. An individual prone to heartburn might recognize a burning sensation in the chest as a signal to take antacid, but might become more alarmed about the possibility of a heart attack if they experience a more severe squeezing feeling around their heart that spreads to their arms and neck. As this example demonstrates, top-down processing associated with cognitive, emotional and behavioural responses is largely selected based on bottom-up signals encoding location, temporal patterning and intensity.
The importance of this nociceptive input in shaping the emotional response to injury (or potential injury) becomes readily apparent when that input is compromised or unavailable. Individuals with Nav1.7 sodium channel deletions (resulting in blocking of primary afferent

nociceptive input) are congenitally insensitive to pain.(Minett et al., 2012) A recent interview with one such patient (“AR”) demonstrated how different the response to potential injury is when it is generated in an entirely top-down manner. At one point during testing with noxious laser stimulation, AR calmly stated that “we should probably stop, my hand feels like when I used to burn it with a lighter”. Through previous experience (possibly demonstrating to peers his ability to stoically endure fire?), AR had learned what pattern of innocuous sensations were associated with injury. In another example, AR described “the last time I broke my ankle” (indicating how frequently such individuals sustain serious injuries because of lack of peripheral nociceptive responses) and how he had to rely on input from other sensory modalities (the sound of bone cracking, the sight of displaced bone, the feeling of blood flowing to the area) to become aware of the injury. These descriptions are illuminating in two respects: first because they demonstrate that in the absence of nociceptive input, defensive responses to potential injury are entirely reliant on learning (necessitating a history of injuries before learned responses can become effective). Secondly, both descriptions were noteworthy for their emotionally neutral tone. AR recalled the cracking and displacement of his ankle in an emotionally blunted manner more appropriate for reciting a bus schedule. Similarly, the potential for a burn to the hand elicited a verbal response that was devoid of any sense of threat or emotional urgency. It is clear that in the case of pain, having highly specific information available at the level of primary afferent is critical to pain’s role as an unlearned warning signal, alerting the organism to immediate somatic threat and facilitating appropriately urgent responses.
In considering specificity of primary afferent input from the periphery, however, Melzack and Wall(Melzack & Wall, 1965) make a critical distinction between physiological and psychological specialization. Physiological specialization is the assumption that receptors differ in the lowest threshold at which they can be triggered by a particular form of energy. Given the evidence cited above, physiological specialization is generally accepted. Psychological specialization is the further claim that each psychological experience of the body must have a specific receptor, which is both necessary and sufficient for that experience. In the case of pain, this latter assumption is contradicted by a variety of phenomena where pain does not correspond with the level of nociceptive input from the area where pain is experienced. These include referred pain (pain that is experienced in a site other than injury, as when arm or shoulder pain is experienced during a heart attack), episodic analgesia (where pain is not felt immediately after injury due to demands of the context of injury), phantom limb pain, and allodynia (pain elicited by a stimulus not intense enough to trigger nociceptors).
IS THERE SPECIFICITY AT THE LEVEL OF THE BRAIN?
Since the first neuroimaging studies of pain,(Davis, Wood, Crawley, & Mikulis, 1995; Jones, Brown, Friston, Qi, & Frackowiak, 1991; Talbot et al., 1991) hundreds of studies have used functional neuroimaging to examine the response to acute nociceptive stimuli. As identified by several meta-analyses,(Apkarian, Bushnell, Treede, & Zubieta, 2005; Duerden & Albanese, 2013; Farrell, Laird, & Egan, 2005) these studies identify a pattern of neural activation common across nearly every study. Areas responding to pain include anterior cingulate cortex, insula, thalamus, primary and secondary somatosensory cortices and motor and premotor regions. Due to the ubiquity of their activation in pain studies, these regions came to be known as the “pain matrix” and have been considered a potential biomarker for pain in medical and legal settings.(Reardon, 2015) The specificity of these regions has been called into question, largely in response to a line of research into “social pain”. Foundational studies(Eisenberger, Lieberman, & Williams, 2003; Kross, Berman,

Mischel, Smith, & Wager, 2011) in this area observed activation in “pain matrix” regions when individuals experienced a sense of social exclusion. These studies have played an important function in drawing attention to the potential overlap between neural systems responsive to nociception and to other emotionally evocative experiences and outlining potential evolutionary mechanisms responsible for this overlap.(Macdonald & Leary, 2005) A more controversial interpretation of this work, however, and one that has been particularly prevalent in accounts of this work in the popular press – is that this potential mechanistic overlap implies experiential overlap. In other words, that pain matrix activation suggests that social exclusion “hurts” (i.e. feels like the emotional response to tissue damage). Given that social stimuli are not associated with nociceptive input, such a claim would undermine the role of nociceptors in guiding the specific emotional experience of pain. Evaluating this claim requires asking whether activation of the “pain matrix” is sufficient evidence for the presence of pain. Downar and Davis and colleagues(J. Downar, Crawley, Mikulis, & Davis, 2000; Jonathan Downar, Mikulis, & Davis, 2003) first called the specificity of these responses into question in an early series of fMRI experiments, demonstrating that a network of regions largely overlapping the pain matrix were associated with the novelty and relevance of environmental stimuli rather than their painfulness. Following on from this work, Mouraux and colleagues(A. Mouraux & Iannetti, 2009; André Mouraux, Diukova, Lee, Wise, & Iannetti, 2011) demonstrated “pain matrix” activation in response to salient (but non painful) stimuli in other sensory modalities (visual, auditory, non-painful tactile). It has been argued that such studies do not necessarily demonstrate that “pain matrix” responses are non-specific, since pain is not explicitly measured and it can therefore not be ruled out that “a non-nociceptive pricking sensation or a very loud noise could be experienced as painful”.(Eisenberger, 2015)
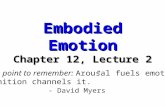
To test this possibility we have recently tested neural responses to noxious mechanical stimulation in two patients congenitally insensitive to pain due to a deletion in the NaV1.7 sodium channel. These individuals’ responses to tactile stimulation are fully intact and their ratings of sensation were comparable to those of healthy controls. Thus, the stimuli were fully matched for both physical and perceptual stimulus intensity and only differed in the presence of perceived pain. The congenitally insensitive patients had robust “pain matrix” activation, equivalent to that of healthy controls (see figure 2). These studies demonstrate that “pain matrix” activation is not sufficient evidence for the presence of pain.
Recent evidence further suggests that an intact “pain matrix” is not necessary for pain perception. We have demonstrated intact pain responses (using multiple dependent measures including pain ratings, psychophysiological responses, facial action coding and verbal reports) in an individual with extensive damage to the “pain matrix” (including near-complete ablation of the anterior cingulate and insular cortices) as well as key limbic structures like the amygdala.(Feinstein et al., 2010, 2015) These findings, together with previously mentioned studies demonstrating “pain matrix” activation in response to non-painful stimuli, seriously call into question whether the “pain matrix” is either necessary or sufficient for the experience of pain.

FIGURE 2 The “Pain Matrix” in Pain-Free Individuals: (A) shows the Neurosynth-based “pain matrix” (red) and the regions where all control subjects had significant activation in response to noxious stimulation (blue). (B) shows activation levels (z-scores) of single subjects within regions of the “pain matrix” (C) shows the Neurosynth-based “pain matrix” (red) and “pain matrix” regions where pain-free individuals had significant activation (yellow). (D) shows the conjunction (green) of pain-free and control activations within the Neurosynth-based “pain matrix” regions.

WHAT ROLE FOR THE BRAIN IN PAIN?
Does evidence for the non-specificity of the pain matrix suggest that the brain plays a limited role in the perceptual experience of pain? Perhaps there was some truth in Descartes’ original conceptualization of the brain as a bell to be rung by a string in the periphery? Perhaps there is no specific representation of pain in the brain and it merely reacts as it might to any salient, adaptively relevant stimulus?
Prior to evaluating this possibility, we must consider a more mundane explanation for the lack of specificity observed in neural responses detected in the neuroimaging literature, namely that technical limitations make fMRI poorly suited to detect pain-specific responses. The temporal resolution of fMRI (the most popular of these techniques) is on the order of seconds, far below the timescale of nociceptive input. Furthermore, fMRI relies on oxygenated blood flow as a proxy for neuronal activation, introducing temporal delays and further measurement imprecision. Finally, the spatial resolution (in cubic millimetres) is too coarse to differentiate between smaller populations of more specialized neurons. Spatial resolution might be a particular problem in understanding the role of ubiquitous “pain matrix” regions like insula and ACC whose integrative role means several types of neurons might exist in close proximity to each other. Indeed, noci-responsive neurons have been found in both regions using techniques with higher spatial resolution,(Frot, Faillenot, & Mauguière, 2014; Frot, Mauguière, Magnin, & Garcia-Larrea, 2008; Hutchison, Davis, Lozano, Tasker, & Dostrovsky, 1999) suggesting that the non-specificity of activations detected using fMRI (and other neuroimaging techniques with equal or worse spatial resolution) might simply reflect technical limitations that obscure differences between activation driven by nociceptive responses from those driven by other types of input.
It is also possible that the fMRI analyses being used are sub-optimal in terms of detecting differences. GLM based univariate analyses typically focus on single voxels, but employ spatial blurring to account for non-independence of adjacent voxels. A cluster-based thresholding technique is then commonly used to determine whether a sufficient number of adjoining voxels reach a threshold level of activation under a particular condition. Such an approach largely ignores and even obscures the spatial pattern that gives rise to overall activation within a particular cluster. Two activation maps might therefore identify a common cluster, but arising from different spatial patterns. Utilizing this spatial information is the basis for a newer machine-learning technique called multivoxel pattern analysis (MVPA), which seeks patterns of activation that distinguish between conditions. This technique has recently been used to demonstrate that sensory data in one modality elicit characteristic patterns of activation in regions of primary somatosensory cortex traditionally viewed as dedicated to other sensory modalities.(Liang, Mouraux, Hu, & Iannetti, 2013)
MVPA has been used by Wager and colleagues(Wager et al., 2013) to derive a “neurosignature” for pain. In a comprehensive set of experiments, Wager and colleagues first established a neurosignature that differentiated between four levels of perceived pain. They then demonstrated that this neurosignature could distinguish between painful and non-painful stimuli in an independent data set. In a third experiment they used the neurosignature to distinguish between social and physical pain. Finally, they demonstrated the sensitivity of this neurosignature to an analgesic agent (reminfentanil). In a follow up study, the same group used MVPA along with a separate modifiability criteria to demonstrate patterns of activation that exclusively distinguished pain and social exclusion, further challenging the neural overlap account of social and physical pain.(Woo et al., 2014)

The notion that emotional experiences that are perceptually distinct from each other will have distinct neural representations is intuitive; so it is tempting to conclude that these analytical advances have succeeded in locating pain-specific circuitry in the brain. It is important, however, to distinguish between empirical and mechanistic specificity. If I look out the window in the morning and can’t see whether rain is falling from the sky, I might use other data to determine whether it is raining. I observe dark clouds in the sky, people are wearing raincoats or walking with umbrellas, there are rain puddles on the ground and passing cars are using their windshield wipers. Intriguingly in this situation, the measures that provide the greatest discriminative power (e.g. windshield wipers) provide no information about how or why it started to rain. In fact, we would learn most about how the rain got there by examining the marker providing the least discriminative power (dark clouds, which can be observed in many different weather conditions). This analogy helps to illustrate the distinction between empirical and mechanistic specificity. Markers that are useful for discriminating one state from another may be merely epiphenomenal, providing no information about the conditions necessary for that state to exist. They provide empirical specificity, but the degree to which we can infer mechanistic specificity of any of the constituent regions remains an open question. In the case of the MVPA derived pain signature, the degree to which this distinction matters depends on what the signature is being used for. For experimental purposes requiring a quantitative measure of neural activity characterizing acute pain, empirical specificity is enough. If, however, we want to better understand how the brain gives rise to the specific experience of pain (or, more specifically, evaluate whether empirical specificity implies mechanistic specificity in the case of pain), these findings are only a start. Moving towards a better understanding will be aided by testing and corroborating models derived from human imaging results with methods that allow for stronger causal and directional inferences. These include studies in non-human species where cell populations and circuitry can be modified, and studies of individuals with relevant genetic mutations or lesions.
As outlined in the previous paragraph, the fact that dark clouds are causally linked to rain is not undermined by the fact that they are not sufficient evidence that it is raining. Similarly the fact that particular regions might be activated during mental states other than pain (i.e. are not sufficient evidence for the presence of pain) does not mean they aren’t involved in the generation of pain. In fact, in evaluating the degree of mechanistic specificity implied by empirically specific “neurosignatures”, Zaki and colleagues(Zaki, Wager, Singer, Keysers, & Gazzola, 2016) point out that these signatures may very well reflect patterns of neural activation in a set of regions which individually may not be specific to that state. This is clearly a pattern theory account. Within this context, it is worth noting that in seeking patterns of spatial activation specific to a state, MVPA and similar techniques implicitly assume a pattern account of neural representation.
Given the evidence reviewed above, and the variable link between nociception and pain, it seems doubtful that there is psychological specialization for pain at any level of the nervous system. In other words, there is no afferent neuron or brain region that is both necessary and sufficient for the psychological experience of pain. In terms of physiological specialization, however, extant evidence suggests a distinction between the periphery and the brain. There is strong evidence for primary afferents specialized to detect stimuli intense enough to cause injury. As we ascend the neuroaxis, however, physiologically specific transmission becomes less prominent, beginning at the dorsal horn of the spinal cord, the first relay between the periphery and brain. Some primary afferent nociceptors synapse on nociceptive specific

neurons (primarily in laminae I-II) but these are relatively rare. More common are deeper-lying wide dynamic range (WDR) neurons that receive afferent input from both A-delta and C fibers but also from larger A-beta fibres sensitive to non-nociceptive sensory input in various modalities.(D’Mello & Dickenson, 2008) In this sense, though primary afferent input is largely specific to sensory input able to cause injury (and pain), at the spinal cord and above, this information is increasingly integrated with non-nociceptive information. At the level of the brain, there is little current evidence for physiological specialization. Rather, neuroimaging provides stronger support for a pattern account, where pain is represented across a network of regions, none of which is specific to pain. Indeed, the two most ubiquitous “pain matrix” regions – anterior cingulate and insular cortices – have been implicated in a wide range of cognitive, affective and regulatory functions.(Menon & Uddin, 2010; Shackman et al., 2011) Within this context, it is noteworthy that the most prominent recent update to the specificity account – Craig’s mechanistic account of pain as a “homeostatic emotion” – places important limitations on the degree of specialization in the brain. Based on compelling anatomical evidence, Craig’s account posits lines that are largely labelled for nociceptive input not only at the primary afferent level, but from spinothalamic tract neurons originating from laminae I. It is noteworthy, however that the brain regions viewed as part of this mechanism (particularly at the cortical level) are not viewed as pain-specific but, rather, as subserving the regulation of a wider class of homeostatic functions (e.g. itch, hunger, thirst, changes in blood pressure).
This arrangement, whereby nociceptive input is increasingly integrated with other sensory, cognitive and affective information at ascending levels of the neuroaxis serves an important adaptive function. Information-rich input from the periphery allows for defensive responses which require little higher order processing. In fact, nociceptive flexion reflexes demonstrate that rudimentary defensive responses can occur without any involvement from the brain. An optimal defensive system, however, requires recognition that some nociceptive input presents little danger (for example, an experimental pain study in which the participant receives well-controlled nociceptive stimuli and is assured that they will not cause lasting damage) while some sub-nociceptive input might represent grave threat to the body (e.g. a dull abdominal sensation from a region where a malignant tumor has previously been removed). Emotional responses can be generated simply by nociceptive input but also by higher-order evaluations of the meaning of the input. Fields has referred to these as primary and secondary affect, respectively.(Fields, 1999) This combination of bottom-up and top-down influences, whereby sensory input is sufficient to trigger a “quick and dirty” emotional response that can be supplemented and adjusted on the basis of top-down contextual evaluations is similar to LeDoux’s account of adaptively critical emotions like fear.(LeDoux, 1996)
Conclusion:
It is impossible to discuss the role for the body in forming the emotional experience of pain, or to consider the implications of this discussion for other emotional experience without re-visiting the historical debate about specificity vs. pattern based representation of pain. The evidence reviewed here suggests that there is considerable physiological specificity at the level of primary afferent input, but that this input becomes increasingly integrated with other sensory and emotional information as it moves up the neuroaxis. This arrangement allows for more nuanced evaluation of threat but also introduces greater ambiguity, which may,

under some circumstances lead to maladaptive pain experiences that do not accurately reflect specific threat to the body. Some evidence supports the existence of nociresponsive neurons in the brain. Nevertheless, it must be concluded that despite recent analytical advances, neuroimaging has not provided strong evidence for specific, dedicated circuits subserving pain processing. Rather, pain representation in the brain appears to be an emergent property of activation across circuits subserving processes common to a broader class of adaptively salient stimuli.
In considering pain as a model for how an emotion might be the product of specific input from the body, a question is whether it serves as a model for all emotions or only for “homeostatic emotions” whose primary adaptive function is to motivate action on the basis of the state of the body. A primary role of pain is to motivate withdrawal or other protective behavioural responses. These are dependent on specific information about the somatic location, intensity and temporal characteristics of a potentially dangerous stimulus. Towards this end, it makes intuitive adaptive sense to have rich data from dedicated fibers in the body to facilitate “quick and dirty” responses (to use LeDoux’s terminology). At higher levels of processing, it is important to contextualize the information in light of other threats or safety signals. In this sense, shared processing with other classes of adaptively salient stimuli is not only efficient, but advantageous, as it allows for more holistic judgements about threat and appropriate response. Other emotions like sadness generally require less specific information about the state of the body, so the adaptive utility of highly specific somatic signatures is questionable. Though pain has a high level of somatic specificity, this specificity does not appear to be a necessary property of other emotions but, rather, a reflection of the adaptive motivational purpose that pain serves. Thus, instead of asking whether emotions are specified in the body, we should ask whether a particular emotion requires specific information from the body to serve its adaptive purpose.
Apkarian, A. V., Bushnell, M. C., Treede, R.-D., & Zubieta, J.-K. (2005). Human brain
mechanisms of pain perception and regulation in health and disease. European
Journal of Pain (London, England), 9(4), 463–484.
https://doi.org/10.1016/j.ejpain.2004.11.001
Basbaum, A. I., Bautista, D. M., Scherrer, G., & Julius, D. (2009). Cellular and molecular
mechanisms of pain. Cell, 139(2), 267–284. https://doi.org/10.1016/j.cell.2009.09.028
Bessou, P., & Perl, E. R. (1969). Response of cutaneous sensory units with unmyelinated
fibers to noxious stimuli. Journal of Neurophysiology, 32(6), 1025–1043.
Burgess, P. R., & Perl, E. R. (1967). Myelinated afferent fibres responding specifically to
noxious stimulation of the skin. The Journal of Physiology, 190(3), 541–562.
Cannon, W. B. (1927). The James-Lange theory of emotions: A critical examination and an
alternative theory. American Journal of Psychology, 44, 169–181.

Cavanaugh, D. J., Lee, H., Lo, L., Shields, S. D., Zylka, M. J., Basbaum, A. I., & Anderson,
D. J. (2009). Distinct subsets of unmyelinated primary sensory fibers mediate
behavioral responses to noxious thermal and mechanical stimuli. Proceedings of the
National Academy of Sciences of the United States of America, 106(22), 9075–9080.
https://doi.org/10.1073/pnas.0901507106
D’Mello, R., & Dickenson, A. H. (2008). Spinal cord mechanisms of pain. British Journal of
Anaesthesia, 101(1), 8–16. https://doi.org/10.1093/bja/aen088
Damasio, A. (1991). Somatic Markers and the Guidance of Behavior. New York: Oxford
University Press.
Davis, K. D., Wood, M. L., Crawley, A. P., & Mikulis, D. J. (1995). fMRI of human
somatosensory and cingulate cortex during painful electrical nerve stimulation.
Neuroreport, 7(1), 321–325.
Descartes, R., Clerselier, C., LaForge, L., & Schuyl, F. (1664). L’homme et un Traitte de la
ormation du Foetus du Mesme Autheur. Paris: Carles Angot.
Downar, J., Crawley, A. P., Mikulis, D. J., & Davis, K. D. (2000). A multimodal cortical
network for the detection of changes in the sensory environment. Nature
Neuroscience, 3(3), 277–283. https://doi.org/10.1038/72991
Downar, Jonathan, Mikulis, D. J., & Davis, K. D. (2003). Neural correlates of the prolonged
salience of painful stimulation. NeuroImage, 20(3), 1540–1551.
Duerden, E. G., & Albanese, M.-C. (2013). Localization of pain-related brain activation: a
meta-analysis of neuroimaging data. Human Brain Mapping, 34(1), 109–149.
https://doi.org/10.1002/hbm.21416
Eisenberger, N. I. (2015). Social pain and the brain: controversies, questions, and where to
go from here. Annual Review of Psychology, 66, 601–629.
https://doi.org/10.1146/annurev-psych-010213-115146
Eisenberger, N. I., Lieberman, M. D., & Williams, K. D. (2003). Does rejection hurt? An FMRI
study of social exclusion. Science (New York, N.Y.), 302(5643), 290–292.
https://doi.org/10.1126/science.1089134

Farrell, M. J., Laird, A. R., & Egan, G. F. (2005). Brain activity associated with painfully hot
stimuli applied to the upper limb: a meta-analysis. Human Brain Mapping, 25(1),
129–139.
Feinstein, J. S., Khalsa, S. S., Salomons, T. V., Prkachin, K. M., Frey-Law, L. A., Lee, J. E.,
… Rudrauf, D. (2015). Preserved emotional awareness of pain in a patient with
extensive bilateral damage to the insula, anterior cingulate, and amygdala. Brain
Structure & Function. https://doi.org/10.1007/s00429-014-0986-3
Feinstein, J. S., Rudrauf, D., Khalsa, S. S., Cassell, M. D., Bruss, J., Grabowski, T. J., &
Tranel, D. (2010). Bilateral limbic system destruction in man. Journal of Clinical and
Experimental Neuropsychology, 32(1), 88–106.
https://doi.org/10.1080/13803390903066873
Fields, H. L. (1999). Pain: an unpleasant topic. Pain, Suppl 6, S61–69.
Frot, M., Faillenot, I., & Mauguière, F. (2014). Processing of nociceptive input from posterior
to anterior insula in humans. Human Brain Mapping, 35(11), 5486–5499.
https://doi.org/10.1002/hbm.22565
Frot, M., Mauguière, F., Magnin, M., & Garcia-Larrea, L. (2008). Parallel processing of
nociceptive A-delta inputs in SII and midcingulate cortex in humans. The Journal of
Neuroscience: The Official Journal of the Society for Neuroscience, 28(4), 944–952.
https://doi.org/10.1523/JNEUROSCI.2934-07.2008
Hutchison, W. D., Davis, K. D., Lozano, A. M., Tasker, R. R., & Dostrovsky, J. O. (1999).
Pain-related neurons in the human cingulate cortex. Nature Neuroscience, 2(5), 403–
405. https://doi.org/10.1038/8065
James, W. (1884). What is an Emotion? Mind, 9, 188–205.
Jones, A. K., Brown, W. D., Friston, K. J., Qi, L. Y., & Frackowiak, R. S. (1991). Cortical and
subcortical localization of response to pain in man using positron emission
tomography. Proceedings. Biological Sciences / The Royal Society, 244(1309), 39–
44. https://doi.org/10.1098/rspb.1991.0048

Julius, D., & Basbaum, A. I. (2001). Molecular mechanisms of nociception. Nature,
413(6852), 203–210. https://doi.org/10.1038/35093019
Kreibig, S. D. (2010). Autonomic nervous system activity in emotion: a review. Biological
Psychology, 84(3), 394–421. https://doi.org/10.1016/j.biopsycho.2010.03.010
Kross, E., Berman, M. G., Mischel, W., Smith, E. E., & Wager, T. D. (2011). Social rejection
shares somatosensory representations with physical pain. Proceedings of the
National Academy of Sciences of the United States of America, 108(15), 6270–6275.
https://doi.org/10.1073/pnas.1102693108
Lazarus, R. S., & Folkman,, S. (1984). Stress, Appraisal and Coping. New York: Springer.
LeDoux, J. (1996). The emotional brain: The mysterious underpinnings of emotional life.
New York: Touchstone Press.
Liang, M., Mouraux, A., Hu, L., & Iannetti, G. D. (2013). Primary sensory cortices contain
distinguishable spatial patterns of activity for each sense. Nature Communications, 4,
1979. https://doi.org/10.1038/ncomms2979
Macdonald, G., & Leary, M. R. (2005). Why does social exclusion hurt? The relationship
between social and physical pain. Psychological Bulletin, 131(2), 202–223.
https://doi.org/10.1037/0033-2909.131.2.202
Melzack, R., & Wall, P. D. (1965). Pain mechanisms: a new theory. Science, 150(699), 971–
979.
Melzack, R., & Wall, P. D. (2004). The Challenge of Pain (Vol. 2nd). London: Penguin
Books.
Menon, V., & Uddin, L. Q. (2010). Saliency, switching, attention and control: a network
model of insula function. Brain Structure & Function, 214(5-6), 655–667.
https://doi.org/10.1007/s00429-010-0262-0
Merskey, H., Bogduk, N., & . (1994). Classification of chronic pain. In Descriptions of chronic
pain syndromes and definitions of pain terms. Elsevier, New York: International
Association for the Study of Pain.

Minett, M. S., Nassar, M. A., Clark, A. K., Passmore, G., Dickenson, A. H., Wang, F., …
Wood, J. N. (2012). Distinct Nav1.7-dependent pain sensations require different sets
of sensory and sympathetic neurons. Nature Communications, 3, 791.
https://doi.org/10.1038/ncomms1795
Mouraux, A., & Iannetti, G. D. (2009). Nociceptive laser-evoked brain potentials do not
reflect nociceptive-specific neural activity. Journal of Neurophysiology, 101(6), 3258–
3269. https://doi.org/10.1152/jn.91181.2008
Mouraux, André, Diukova, A., Lee, M. C., Wise, R. G., & Iannetti, G. D. (2011). A
multisensory investigation of the functional significance of the “pain matrix.”
NeuroImage, 54(3), 2237–2249. https://doi.org/10.1016/j.neuroimage.2010.09.084
Muller, J. (1840). Handbuch der Physiologie des Menschen. Koblenz, Germany: J. Holscher.
Nafe, J. P. (1929). A quantitative theory of feeling. The Journal of General Psychology, 2(2-
3), 199–211.
Norrsell, U., Finger, S., & Lajonchere, C. (1999). Cutaneous sensory spots and the “law of
specific nerve energies”: history and development of ideas. Brain Research Bulletin,
48(5), 457–465.
Reardon, S. (2015). Neuroscience in court: The painful truth. Nature, 518(7540), 474–476.
https://doi.org/10.1038/518474a
Shackman, A. J., Salomons, T. V., Slagter, H. A., Fox, A. S., Winter, J. J., & Davidson, R. J.
(2011). The integration of negative affect, pain and cognitive control in the cingulate
cortex. Nature Reviews. Neuroscience, 12(3), 154–167.
https://doi.org/10.1038/nrn2994
Sherrington, C. S. (1903). Qualitative difference of spinal reflex corresponding with
qualitative difference of cutaneous stimulus. The Journal of Physiology, 30(1), 39–46.
Talbot, J. D., Marrett, S., Evans, A. C., Meyer, E., Bushnell, M. C., & Duncan, G. H. (1991).
Multiple representations of pain in human cerebral cortex. Science (New York, N.Y.),
251(4999), 1355–1358.
vonFrey, M. (n.d.). Beiträge zur Sinnesphysiologie der Haut. Ber. Ges. Wiss., 47, 166.

Wager, T. D., Atlas, L. Y., Lindquist, M. A., Roy, M., Woo, C.-W., & Kross, E. (2013). An
fMRI-based neurologic signature of physical pain. The New England Journal of
Medicine, 368(15), 1388–1397. https://doi.org/10.1056/NEJMoa1204471
Woo, C.-W., Koban, L., Kross, E., Lindquist, M. A., Banich, M. T., Ruzic, L., … Wager, T. D.
(2014). Separate neural representations for physical pain and social rejection. Nature
Communications, 5, 5380. https://doi.org/10.1038/ncomms6380
Zaki, J., Wager, T. D., Singer, T., Keysers, C., & Gazzola, V. (2016). The Anatomy of
Suffering: Understanding the Relationship between Nociceptive and Empathic Pain.
Trends in Cognitive Sciences, 20(4), 249–259.
https://doi.org/10.1016/j.tics.2016.02.003