
(PAARR) TRAUMA INFORMED CLASSROOM MANAGEMENT INFORMED CLASSROOM … · CLASSROOM MANAGEMENT . ......
27
(PAARR) TRAUMA INFORMED CLASSROOM MANAGEMENT
Transcript of (PAARR) TRAUMA INFORMED CLASSROOM MANAGEMENT INFORMED CLASSROOM … · CLASSROOM MANAGEMENT . ......

(PAARR)
TRAUMA INFORMED
CLASSROOM MANAGEMENT

The Adverse Childhood Experiences (ACE) Study
The largest study of its kind ever done to examine the health and social effects of adverse childhood experiences over the lifespan (18,000 participants)
The majority of participants were 50 or older (62%), were white (77%) and had attended college (72%)
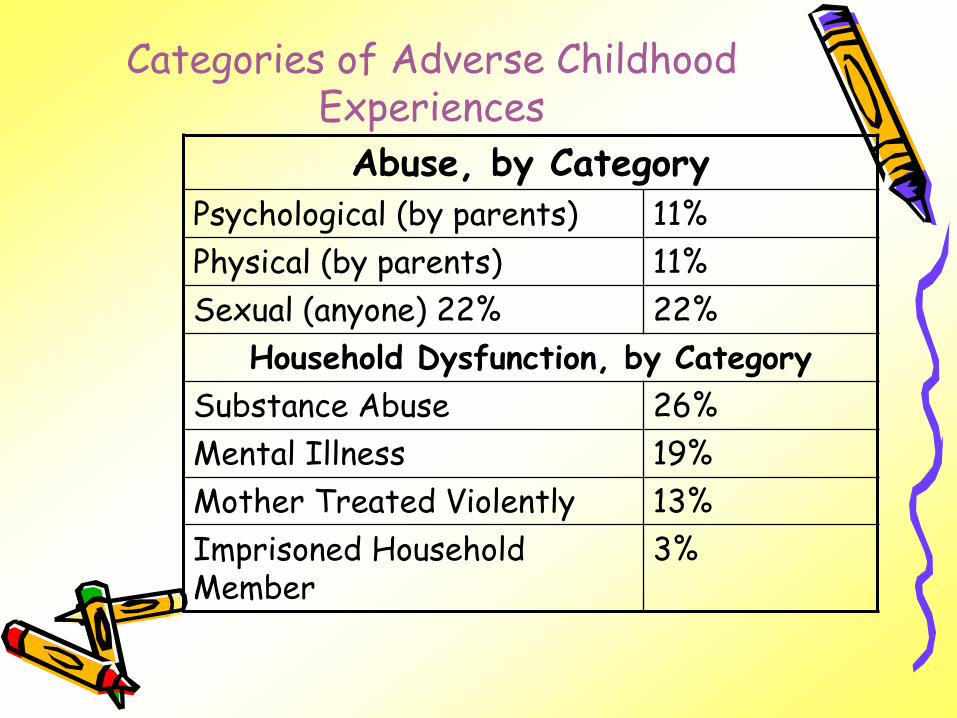
Categories of Adverse Childhood Experiences
Abuse, by Category Psychological (by parents) 11%
Physical (by parents) 11%
Sexual (anyone) 22% 22%
Household Dysfunction, by Category
Substance Abuse 26%
Mental Illness 19%
Mother Treated Violently 13%
Imprisoned Household Member
3%

Adverse Childhood Experiences Score
ACE Score Prevalence
0 48%
1 25%
2 13%
3 7%
4 or more 7%
•More than half have at least one ACE
•If one ACE is present, the ACE Score is likely to range from 2.4 to 4

ACE’s Study
• One in four was exposed to two categories of abusive experience,
• One in 16 to four categories
• Smoking • COPD • Hepatitis • Fractures • Diabetes • Obesity • Alcoholism • Other Substance Abuse • Depression and attempted suicide • Teen pregnancy – including paternity • Sexually transmitted diseases • Occupational health • Job performance

ACE’s Study
• Adverse Childhood Experiences determine the likelihood of the ten most common causes of death in the United States.
• With an ACE Score of 0, the majority of adults have few, if any, risk factors for these diseases.
• However, with an ACE Score of 4 or more, the majority of adults have multiple risk factors for these diseases or the diseases themselves.

Disrupted Neurodevelopment
Adverse Childhood Experiences
Early Death
Disease, Disability & Social
Problems
Adoption of Health Risk Behaviors
Death
Conception
Mechanism by Which Adverse Childhood Experiences influence Health & Wellbeing Throughout the
Lifespan

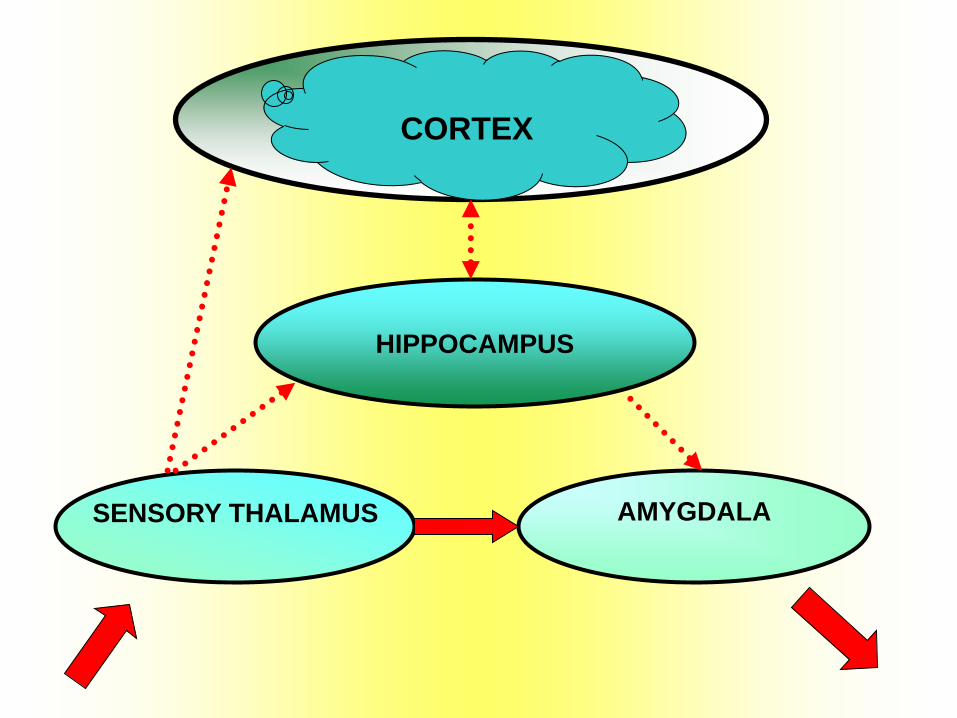
CORTEX
HIPPOCAMPUS
SENSORY
THALAMUS AMYGDALA

CORTEX
HIPPOCAMPUS
SENSORY THALAMUS
AMYGDALA

CORTEX
HIPPOCAMPUS
SENSORY THALAMUS
AMYGDALA

CORTEX
HIPPOCAMPUS
SENSORY THALAMUS
AMYGDALA
HIPPOCAMPUS
SENSORY THALAMUS
AMYGDALA
CORTEX

Exposure to Chronic Stress
Implications for Response
Recognition of fight-flight condition
Help to accurately assess degree of threat/danger
Reduce threat and increase safety
Minimize physiological hyperarousal
Reinforce Self-soothing techniques
Address continuing dissociation – grounding
Attend to physical illness
Tap cognitive skills
Understand addictive behaviors – substance and behavioral

CHILD TRAUMATIC STRESS AND
LEARNING IMPAIRMENTS
TYPE OF IMPAIRMENT MALTREATED CONTROL
Language/speech 12.6% 8.4%
Developmentally
Disabled 9.1% 1.3%
Hearing 9.0% 7.5%
Learning Disabled 7.4% 2.6%
ADD 3.9% .8%
Stages of Treatment
Stage One-Stabilization, Trust and Safety
Alliance building, safety affect regulation,
support, self care and stabilization issues
Stage Two-Trauma Work
Resolution and integration of trauma
Stage Three-Learning to Live in the Moment
Self and relational development and daily
life enhancement
Definition of a Physical Crisis:
A situation of confrontation between
client/client, client/staff, client/self, or
client/environment in which prior
interventions along the continuum may be
ineffective;
Or
Between a staff/client, where the client has
been “set up” or has not been allowed to
“save face”.

Avoidance Techniques
1. Defining the physical crisis
“Call a duck a duck….”
2. Assessing the potential for violence
• Trigger factors
• History
• Predictive factors
• Contraindications for physical restraint
3. A consistent philosophy of discipline
4. Crisis protocols
• Self awareness
• Intervention continuum
• Verbal intervention continuum
• Remediation

Avoidance Techniques (cont.)
5. Safe, therapeutic application of physical techniques
• Team approach
• Techniques
• De-escalation
• Physical and emotional safety
• Mediating considerations

Predictive Factors:
1. Severe emotional deprivation or overt rejection in early childhood.
2. Parental seduction.
3. Exposure to brutality and extreme violence.
4. Childhood fire setting.
5. Cruelty to other children and/or animals.
Menninger & Modlin, 1971
1. History of homicidal threats.
2. Lack of suicide attempts (among those who frequently threaten homicide).
3. Symbolic acts of murder.
4. Males.
5. Social class.
6. Depressed mood building
7. A penchant for weapons.
8. Dehumanizing view of mankind.
9. History of drug or alcohol abuse (presently under the influence).
10. A plan to injure or kill someone.
Walker, 1983

Discipline
A broad program designed to help the client learn new ways to handle his/her behavior and feelings.
PHASE 1 (Milieu)
STRUCTURE/ROUTINE
EXPECTATIONS
CHOICE
CONSEQUENCES (Positive and Negative)

DEPENDENCE INDEPENDENCE
P h y s i c a l V e r b a l N o n -V e r b a l
0 1 2 3 4 5 6 7 8 9 10 11
R S P R D T V D P S V R S T P P F E E C I C
E E H E I O E I R O E E U O H R A X Y O N O
S C Y S R U R R O L R M P U Y O C P E N T N
T L S T E C B E B V B I P C S X I R T E T
R U I R C H A C L I A N O H I I A E A R R
A S C A T I L T E N L D R I C M L S C N O
I I A I I N I M G E T N A I S T A L
N O L N V G O R I G L T I L
T N T E N V Y O
S E N
GENERAL FACTORS WHICH AFFECT FUNCTIONING IMMEDIATE FACTORS WHICH AFFECT FUNCTIONING
LEVEL ON THE CONTINUUM: LEVEL ON THE CONTINUUM:
I.Q. RELATIONSHIPS WITH STAFF
AGE RELATIONSHIPS WITH PEERS
LEARNING ABILITY MEDICATION
PSYCHO-SOCIAL HISTORY FAMILY DYNAMICS -- VISITS
EDUCATION LIFE PLAN -- STAFFING
EMOTIONAL STATE LEVEL OF SELF-ESTEEM
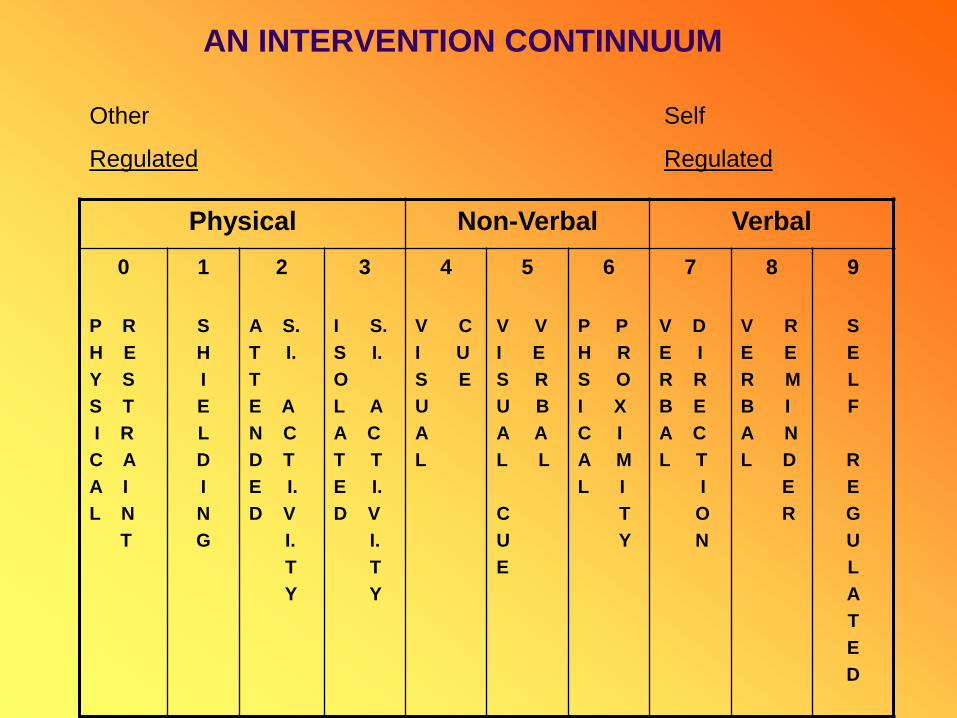
AN INTERVENTION CONTINNUUM
AN INTERVENTION CONTINNUUM
Other Self
Regulated Regulated
Physical Non-Verbal Verbal
0
P R
H E
Y S
S T
I R
C A
A I
L N
T
1
S
H
I
E
L
D
I
N
G
2
A S.
T I.
T
E A
N C
D T
E I.
D V
I.
T
Y
3
I S.
S I.
O
L A
A C
T T
E I.
D V
I.
T
Y
4
V C
I U
S E
U
A
L
5
V V
I E
S R
U B
A A
L L
C
U
E
6
P P
H R
S O
I X
C I
A M
L I
T
Y
7
V D
E I
R R
B E
A C
L T
I
O
N
8
V R
E E
R M
B I
A N
L D
E
R
9
S
E
L
F
R
E
G
U
L
A
T
E
D

A CONTINUUM OF VERBAL RESPONSE TECHNIQUES
RE-ESTABLISH
ESTABLISHING CONTACT
REDIRECTIVE
(PHYSICAL) ESCALATION
CONTACT PROBLEM-SOLVE
CLOSURE/ESCAPE
ENGAGEMENT
REFLECT I VE
SUPPORT I VE
PROTECT I VE
ESTABLISHING CONTACT
Engagement: Empathetic icebreakers used to create “helping” atmosphere.
Reflective Response: Active Listening):
Paraphrasing: Testing your understanding by repeating the statement in your own words.
Reflection of Feelings: Expressing an understanding of the feelings that you perceive behind the speaker’s verbal and no-verbal messages.
Perception Checking: Expressing your understanding of the person’s words and feelings and asking them to confirm it.
Illustrating: Asking for or giving examples of the issues being expressed or received.
Supportive Responses: Statements that express your willingness to work through the issue with the person and do your best to provide whatever
help and support that you’re able to provide.
Protective Responses: Statements that reassure the person that you (hopefully the “collective you”) will keep him/her safe and will not allow him/her
to hurt or be hurt. (Only say it if you can back it!)

PHASE II (Cognitive)
Remediation/Mutual Problem Solving
1. Intervention
2. Definition of Problem
3. Development of Alternative
4. Commitment to a Plan
5. Rehearsal
6. Reinforcement/Feedback
7. Reinvolve

TEAM LEADER RESPONSIBILITIES
ASSESS SITUATION
CALL FOR HELP (IF NEEDED)
STATE NEED (WHEN HELP ARRIVES)
BRIEFLY DESCRIBE SITUATION
CUE THE TEAM
DIRECT THE TEAM
DE-ESCALATE
REMEDIATE

FOR MORE INFORMATION
THE NATIONAL CHILD TRAUMATIC STRESS NETWORK www.NCTSN.org
ACE STUDY www.acestudy.org
SUBSTANCE ABUSE AND MENTAL HEALTH SERVICES ADMINISTRATION www.samhsa.gov
AMERICAN ACADEMY OF CHILD AND ADOLESCENT PSYCHIATRY www.aacap.org
THE SANCTUARY MODEL www.sanctuaryweb.com
TIM SCHAFFNER email; [email protected]

















