
Over a lifetime | 70 years of medical research
101
OVER A LIFETIME 70 years of medical research
-
Upload
qimr-berghofer-medical-research-institute -
Category
Documents
-
view
223 -
download
4
description
This is the story of how QIMR Berghofer became one of Australia's, and the world's, leading medical research institutes.
Transcript of Over a lifetime | 70 years of medical research

OVER A LIFETIME70 years of medical research

OVER A LIFETIME 70 YEARS OF MEDICAL RESEARCH
© 2015 QIMR Berghofer Medical Research Institute
Published by QIMR Berghofer Medical Research Institute
300 Herston Road Herston QLD 4006 Australia
Locked Bag 2000 RBH QLD 4029 Australia
T +61 7 3362 0222 E [email protected] W www.qimrberghofer.edu.au
QIMR Berghofer Medical Research Institute is a registered trademark.
All rights reserved. No part of this book may be reproduced by any mechanical, photographic, or electronic process, or in a form of a phonographic recording; nor may it be stored in a retrieval system, transmitted, or otherwise be copied for public or private use – other than for ‘fair use’ as brief quotations embodied in articles and reviews – without prior written permission of the author.
National Library of Australia Cataloguing-in-Publication
Author: QIMR Berghofer Medical Research Institute Title: Over a lifetime: 70 years of medical research
Edition: 1st ed. ISBN: 978-0-646-94387-9
Printed in Brisbane, Queensland, Australia.

CONTENTSForeword .................................................. 2
01 The beginning (1940s) ......................... 4
02 1950s ................................................ 16
03 1960s ................................................ 24
04 1970s ................................................ 34
05 1980s ................................................ 40
06 1990s ................................................ 50
07 Entering the 21st century ................... 62
08 Looking forward ................................ 82
Further reading ....................................... 94
‘You don’t dabble in science, you focus on an area and stick to it. People who make breakthroughs don’t do it overnight; they do it over a lifetime.’
Sir Gustav Nossal as recounted by Michael Good, QIMR Director (2000–2010)
1

FOREWORDIf you are driving north, out of the busy heart of Brisbane, through its commercial downtown, Fortitude Valley and Spring Hill, you will shortly crest the rise at the intersection of Bowen Bridge Road and Gregory Terrace. There you will see two edifices dedicated to science: on the right the handsome late-Victorian brick building, formerly home to the Queensland Museum, and in the middle of your field of vision the green-glass-fronted façade of QIMR Berghofer Medical Research Institute.
This modern building, built in three stages over the past thirty years, contains more than 50 laboratories, is the working space for more than 500 scientists, and is the centre for training more than 100 of the best and brightest PhD students in a wide range of medical research areas.
But it was not always so.
This is the story of how QIMR Berghofer became one of Australia’s, and the world’s, leading medical research institutes; from its genesis in the 1940s to the present day – 70 years packed with challenges and opportunities, inspirational leadership, and dedicated men and women, working to better the health and well-being of the people of this great state.
Professor Frank Gannon Director and CEO, QIMR Berghofer
2

This is the story of how QIMR Berghofer became one of Australia’s, and the world’s, leading medical research institutes.
3

THE BEGINNING (1940s)01It was not, perhaps, the type of headline Queensland Health Minister Arthur Jones had hoped for – but there it was, screaming out from the pages of Brisbane’s morning newspaper, The Courier-Mail.1
For 16 months, Queensland’s capital city had been in the grip of a gastroenteritis epidemic that had claimed the lives of at least 100 tiny tots, with penicillin proving useless and the newest drug of the day, streptomycin, having only modest success. Clearly this was not a run-of-the-mill tummy bug. The infection mostly affected children aged two or younger. It invaded the intestine, causing inflammation and internal bleeding; ‘an orange-coloured fluid of a rather offensive nature sometimes streaked with blood’ was reported.
‘The fact is, we are up against a special type of gastric trouble that has not been known here before,’ The Courier-Mail stated.
Salmonella bovismorbificans was believed to have snuck into Brisbane when a British bride ship made port in 1946, and Queensland’s finest scientific investigators had been tasked to identify how the bacteria had spread and what could be done to safeguard the toddlers affected.
‘The fact is, we are up against a special type of gastric trouble that has not been known here before.’
4

‘All resources of the Institute have been directed to solving the cause of gastro-enteritis,’ The Courier-Mail reported, referring to the infant Queensland Institute of Medical Research (QIMR).
An Act of Parliament established the Queensland Institute of Medical Research in 1945, the foundation staff being pathologist Dr Edward (Ted) Derrick, technician Veda Pask and cadet scientists Pauline Pope and Ian Cook 2, its doors opening in July 1946. Director Ian Mackerras commenced duties only weeks before The Courier-Mail’s alarming story. Mackerras, chosen from an international field of applicants to head this new research facility, was reportedly unimpressed. Was this what the government had intended of him? Was this what he expected?
Pauline Pope and Ian Cook were the first cadet scientists to join QIMR in July 1946.
5

Medical research in Queensland had been, until 1945, episodic. In 1876, Joseph Bancroft discovered Wuchereria bancrofti, a mosquito-borne parasitic roundworm responsible for lymphatic filariasis in humans: fever, chills, skin infections, painful lymph nodes, and ultimately thickening of the skin, earning the term ‘elephantiasis’. His son, Thomas Bancroft, linked mosquitoes to the transmission of dengue fever. In the early 1900s, Lockhart Gibson had determined that lead content in house paint was poisoning children. The state’s first medical research facility, the Australian Institute of Tropical Medicine, established in 1910 in Townsville, focused on tropical fevers, but it was short-lived, relocating to Sydney in 1930. There were three Commonwealth health laboratories established in northern Queensland – Townsville (1922), Rockhampton (1924) and Cairns (1928) – but their primary purposes were quarantine, and localised clinical and preventative medical services, not research. At that time, Queensland did not even have a medical school: the state’s doctors trained ‘down south’, in Victoria or New South Wales, or overseas.
Two ‘distractions’, as pathologist Derrick called them, were to both curb and inspire local research. In 1936, The University of Queensland began teaching medicine. Derrick was among those to provide teaching expertise. At the time, he headed the State Health Department’s Laboratory of Microbiology and Pathology. A medical graduate of The University of Melbourne, he had been a research scholar at the Walter and Eliza Hall Institute (WEHI), Australia’s first dedicated medical research facility; a pathology assistant at London Hospital; and had spent 10 years in country practice in North Queensland.
While honoured to give lectures in tropical, social and forensic medicine, researchers, like everyone else, had only so many hours in a day and Derrick, for one, was happiest when researching.3 Preparing and delivering lectures and dealing with administration back at the health department eroded the research time and Derrick was very much sought-after. He had conducted the first research on Q fever4, a debilitating condition sending abattoir workers and farmers to their beds. Derrick’s meticulous investigations determined Q fever was the result of bacteria which he named Rickettsia burnetti.5 He was also the first to isolate Leptospira pomona, affecting dairy cattle.
World War II was another distraction. Provisions were in short supply at the health department’s Laboratory of Microbiology and Pathology, and so were qualified staff: Derrick’s laboratory at its fullest capacity had only four staff members, none with tertiary qualifications.6 Yet the conflict in the Pacific arena highlighted the merit and need for medical research: the work of the Australian military’s Land Headquarters’ Medical Research Unit in North Queensland was giving Australian soldiers an edge in the battle against another enemy: debilitating fevers caused by malaria and scrub typhus.
Joseph Bancroft.
6

Dr Edward (Ted) Derrick was a visionary who pushed for medical research in Queensland.
In the 1944 departmental annual report, Derrick flagged the need for properly funded medical research. A Cabinet submission in November that year made an emphatic case. The departmental memo left no doubt: ‘…the large number of cases of scrub typhus and malaria in New Guinea exemplify the need; the dramatic results from the sulpha drugs and penicillin the value’. To retain the status quo was impossible, he argued: ‘A good deal of research work was done in the Laboratory of the Health Department in pre-war years and a little since the war began…because of the transfer of staff to the services and the overwhelming of the Director by routine duties’.7
Derrick reasoned that in selecting subjects for research, ‘priority should be given to those problems that occur particularly in Queensland’8; that while Australia had five medical research institutes — Walter and Eliza Hall Institute in Melbourne (1915); the Institute of Medical Research at Royal North Shore Hospital, Sydney (1920); Baker Institute at Melbourne’s Alfred Hospital (1927); Kanematsu Institute at Sydney Hospital (1937) and the Institute of Medical and Veterinary Science in Adelaide (1938) — localised research was ‘so limited in extent that it is in the immediate future unlikely to meet the needs of the Australian people’.9 Derrick left no doubt that Queensland had a responsibility — an obligation — to fulfil as a defender of public health: ‘If we do not investigate these, no other country can do it for us’.10
His plea hit a nerve. Health Minister Tom Foley established a medical research advisory committee, chaired by Derrick, to prepare proposals for the expansion of medical research in Queensland.
On 6 September 1945, a Bill was introduced into Queensland Parliament to establish ‘the Queensland Institute of Medical Research’. Its mission would be open-ended: it was to research ‘any branch or branches of medical science’ with particular interest directed towards Queensland fevers and tropical diseases, lead poisoning and viral illnesses affecting children, industrial diseases and the incidence of health issues ‘in relation to social and nutritional status’.11 While the move was widely welcomed, parliamentarians let their voices be heard to question impartiality and financial support being offered. ‘I picture the director…wrapped and swathed in red tape from the minute he is first chosen…his every action and every thought subjected to not only direction but multitudinous direction and supreme over every other form of direction — ministerial direction,’ put Member for Logan, Tom Hiley.12 ‘Medical research will continue for all time…If he is to grapple with the problems of the various diseases from which human beings suffer, he must be free from financial difficulty so that the salary given to the director should be more than enough to leave his mind free,’ said Member for Albert, Thomas Plunkett.13 The Queensland Institute of Medical Research Act 1945 was proclaimed in January 1946 and a management council appointed. As a branch of the state health department, its chair was to be the departmental director-general, then Sir Raphael Cilento. Other councillors represented the hospitals, British Medical Association Queensland branch14, and The University of Queensland. Derrick was appointed acting deputy director and given the job of making it happen, with the princely budget of £15 000 (less the £2000 earmarked as the director’s salary) for the first year.
On 6 September 1945, a Bill was introduced into Queensland Parliament to establish ‘the Queensland Institute of Medical Research’.
7

8

World War II had only just concluded. While rations remained for everyday items such as tea, sugar, butter, clothing and petrol, other goods proved surplus to requirements. Derrick, a teetotal Methodist who had once entertained the idea of being a missionary, scrimped and salvaged. Office furniture was acquired through Army disposals; laboratory equipment including microscopes, centrifuges, a mechanical shaker, hot air oven, vacuum pressure pump and analytical balance, purchased from the disbanded Land Headquarters Medical Research Unit in Cairns. Scientific journals, stacked on the floor in a spare room of the Health Department’s William Street building were rescued: Derrick later admonishing himself for not retrieving more before junior clerks threw them in the incinerator to make space.15
And what of a building? It was just as well Derrick had felt that ‘the most important requisite for research is not the building nor the equipment but the research worker’.16 Soon after American soldiers descended on Brisbane in late 1941, responding to the war in the West Pacific, part of the inner city public golf course of Victoria Park was commandeered as the United States Army Services of Supply Brisbane headquarters. About 100 pre-fabricated temporary buildings mushroomed across the rolling green expanse from Herston Road, across York’s Hollow to Gregory Terrace. While the Queensland Housing Commission used some of the vacated
buildings on the Gregory Terrace side post-war, Derrick saw potential in one hut close to The University of Queensland’s medical school on the Herston side of the golf course. It was well-lit, large and open — 1100 square metres; it could be partitioned to create laboratories, sterilising and media rooms, offices and workshops — and there was ample car parking. Two other aspects may have swayed Derrick’s choice. Hut 8, as it was called, behind the barbed wire fence just off Herston Road, sandwiched between two huts used by the university, was in easy walking distance of the Brisbane General Hospital.17 It was also a bargain, the Commonwealth willing to sell it for £1840. Strangely, at a time when unoccupied buildings were commonly ransacked, homeless people taking up temporary residence as squatters or pilfering supplies for sale on the black market18, Hut 8 and its neighbours were left untouched. Why? The rumour of cadavers used by anatomy students served as an other-worldly deterrent!
So what that it was makeshift, unlined and unfinished, thought Derrick? This accommodation was to be only temporary: even the Brisbane City Council agreed that the hut remain on its former golf green only until 1948. No one envisaged this would be the home of the state’s premier medical research body for nearly 30 years!
In the post-World War II sell-off of equipment and buildings, Hut 8 was purchased at a bargain price to house Queensland’s first medical research institute.
To leave no doubt as to ownership, deputy director Ted Derrick took to signwriting the Institute’s name in large letters with a grease pencil. Photo by John Tonge.
9

Dr Ian Mackerras, formerly principal research officer of the Division of Economic Entomology of Australia’s Council for Scientific and Industrial Research (CSIR), took up his position as director on 2 June 1947. He brought with him a distinguished record both of personal research and of directing research teams with broad interests in medical zoology, parasitology, entomology and malariology. In 10 years, his research team had produced nearly 100 scientific papers chiefly relating to veterinary entomology; he’d served in both world wars, and had enjoyed success in malaria control work. A chain-smoking extrovert and raconteur, Mackerras had married into the Bancroft family, Queensland’s medical research and natural science pioneers.
Mackerras wasted little time in letting his thoughts on research be known in a paper entitled ‘The ways and means of research’.19 The first purpose of a research institution, he wrote, was to acquire knowledge: ‘It is not so important that it should have any immediate value for example in the prevention or cure of disease; what does matter is that something new may be added to the sum of the world’s wisdom and understanding…the great majority of big discoveries and innumerable smaller ones which have benefitted mankind have come from pure research…research for its own sake fosters, as nothing else can, the urge always to explore, without which initiative is lost and no research institution can live.’
Chain-smoking extrovert Ian Mackerras argued that the Institute’s work should be ‘untrammelled’ — unimpeded by red tape or interference.
10

While the government directive to look into the gastro epidemic was thinly repudiated in Mackerras’s comments — research should be ‘untrammelled’, he said, adding that a research organisation could be ‘impeded’ in several ways including funding shortfalls, red tape or ‘outside direction or interference’20 — it did fit within his basic aims of addressing infectious diseases, understanding their transmission ‘with preventive rather than curative medicine as the ultimate goal’.21 He proposed a three-stage growth period with units working in parasitology, virology, bacteriology, biochemistry, pathology and animal ecology. This partly reflected his own research interests, experience and training: at the CSIR, Mackerras was known for his work on blowfly pest in sheep and buffalo fly and ephemeral fever in cattle which Mackerras believed might be similar to dengue in humans. But it also showed realism, working with the skills and resources available, and big dreams. In his mind, the only medical research organisation in Australia that the QIMR should compare itself to was the Walter and Eliza Hall Institute.22
DR IAN MURRAY MACKERRASFounding Director 1947–1961
Born 1898, New Zealand
Entomologist, parasitologist, zoologist
Married to Mabel Josephine Mackerras née Bancroft
Resigned to take up research fellowship in the Commonwealth Scientific and Industrial Research Organisation’s division of entomology, Canberra
Died 1980
DID YOU KNOWBrisbane was not fully sewered until the early 1970s.
In 1944, Australia was the first country to manufacture penicillin for the domestic market at the Commonwealth Serum Laboratories (CSL) in Melbourne.
In 1946, electron microscopes were developed in Britain with potential to magnify more than 50 000 times.
11

Much of the Institute’s early work leaned heavily towards zoonoses — infectious diseases of animals that can be spread to humans. Native animals were caught and studied for parasites, the parasites in turn examined under microscope to learn more about them. Biochemist JP Callaghan joined the Institute in 1948. Mackerras’s wife Josephine, a qualified medical practitioner and scientist in her own right, was appointed senior parasitologist. She was a Bancroft by birth, the nearest Queensland had to esteemed medical lineage. Grandfather Joseph Bancroft led the discovery of the parasitic worm which causes filariasis. Indeed Filaria bancrofti was named in his honour. And he was one of the first to suggest that mosquitoes transmitted disease — although just how was left to the next generation, son Thomas Bancroft, Josephine’s father.23 With a WEHI fellowship behind her, she’d met Mackerras while pursuing further study at The University of Sydney in 1924. She served in World War II
Dr Josephine Mackerras née Bancroft: her father and grandfather were medical research and natural science pioneers in Queensland.
as a medical doctor and malaria researcher. Her interest in parasites seemed insatiable as a personal research assistant Ruth Thomson (née Smith) recalls24: ‘My enduring memory is of all her roadkill. If there was a dead animal on the road, she had to pick it up, bring it to the laboratory and dissect it, looking for parasites. More often than not my first task for the day involved a newspaper-wrapped parcel left on the desk, a smelly mashed body that I’d need to pick over to collect parasites, embedding them in paraffin and preparing slides for Mrs Mack’s viewing and analysis.
‘And I recall coming across Mrs Mack in the insectary, one arm in a mosquito cage being savagely bitten as she calmly read a book. When I asked what she was doing, she simply said, ‘Just feeding the mosquitoes’. They need a feed of blood to breed and Mrs Mack maintained that her years growing up at Deception Bay had made her immune!
Ian Mackerras studying his collection. The Institute’s early work leaned heavily towards zoonoses, infectious diseases of animals spread to humans.
12

‘In the 1950s, a large number of displaced Europeans were arriving in Brisbane. They relished the freedom of bushwalking. Mrs Mack became very concerned that these new settlers had brought with them stowaways in the form of intestinal tapeworms and we had no idea whether our native animals would act as intermediary hosts to these parasites. We established the first breeding colony of bandicoots, discovering that gestation is 12.5 days precisely. Mrs Mack worked with native rats, frogs, bats, possums, marsupial mice and the usual laboratory animals too. Geese and a couple of pet cats earned their keep as blood givers and cages of cockroaches, mosquitoes and mantis as well as two huge carpet pythons completed our menagerie.
‘Working with Mrs Mack was never dull. You never knew what each day would bring or who — although I would have to remind her to take a break and eat some lunch, taken usually with her husband. When international or interstate dignitaries visited, drawn to the Institute to talk with this scientist whose work in parasitology was so highly regarded, she’d fob off the VIPs with a momentary glance up from the microscope and a beseeching ‘Do be a dear and show them around’ to her cadet.’
‘Working with Mrs Mack was never dull.’
13

AUTOCLAVES IN THE HUTThe first two autoclaves were gas-fired and lit
by a wax taper. They were upright, about 90
centimetres high and about 45 centimetres in
diameter. Water was put in the bottom with a
bucket. The lid was extremely heavy and a wire,
through a pulley on the roof, was counterpoised
with a lead weight equal to the weight of the lid.
That lid was sealed with about 10 thumb screws
which were tightened with a spanner. The
chamber was manually sealed and the air was
expelled by turning a valve. The pressure and
time were also manually controlled. When the
cycle was completed, it had to be cooled before
opening and emptying. One autoclave was used
for waste and dirty products while the other
was used for media and clean material being
sterilised for use.
— Ian Cook —
ReminiscenceAnd what of the gastro outbreak? Salmonella was found in soiled cloth nappies and scrubbing brushes used before laundering as well as in hospital ward sinks. Improved hygiene practices were recommended. Domestic cockroaches were found to be the main culprit spreading salmonella infection, particularly Salmonella bovismorbicans.
The Institute’s investigations brought to 20 the species of Salmonella known in Queensland.25 Further research by Ian Mackerras and Pauline Pope determined that cockroaches acquired infections readily, and that 15 per cent were ‘chronic carriers’, retaining an infection for more than a fortnight.26 Josephine Mackerras went on to study cockroaches as vectors for disease, intermittently over many decades. The gastro outbreak also provided an opportunity to develop bacteriological studies more rapidly than expected and made a real contribution to disease control.
14

ENDNOTES 1 The Courier-Mail, 4 November 1947, p2
2 A married couple, the Blanchards, rounded out the foundation staff, Jack serving as an attendant and security officer while his wife worked as cleaner.
3 AMA Queensland News Bulletin, obituary of Edward Derrick, 1976
4 The ‘Q’ stands for ‘query’ not ‘Queensland’ as the cause was not known and this discovery turned out to be of international importance.
5 Renamed Coxiella burnetti. Refer Mackerras IM Australian Academy of Science, Biographical memoirs of deceased fellows, Edward Holbrook Derrick 1898–1976
6 Cooke RA, ‘Q fever. Was Edward Derrick’s contribution undervalued’, Medical Journal of Australia 15 December 2008, vol 189, number 11/12 p660
7 Copy of departmental memo, from Derrick to D/Director General of Health and Medical Service, 17 November 1944
8 Derrick EH ‘The birth of the Queensland Institute of Medical Research’, Medical Journal of Australia 1972,2:952-59, p953
9 Ibid, p954
10 Ibid, p953
11 The Queensland Institute of Medical Research Act 1945
12 Hansard, Wednesday 3 October 1945, p583
13 Ibid, p594
14 The Australian Medical Association had yet to be established.
15 Derrick op.cit. p957
16 Cabinet submission memo, 17 November 1944
17 Now known as Royal Brisbane and Women’s Hospital.
18 The Courier-Mail, 17 August 1947
19 Published in the Institute’s second annual report, 1947
20 Ibid
21 Typescript, ’25 years of microbiology at QIMR’, Australian Society for Microbiology, 20 July 1972, author unknown
22 QIMR Annual Report, 1947, p11
23 For more information about the Bancrofts, read The Bancroft Tradition, see Further Reading.
24 Interview with author, 27 January 2015. Ruth Smith was Josephine Mackerras’s research assistant in the 1950s for nearly five years. She married at 21, in 1959, and as was the practice of the day, resigned. Years later, as Ruth Thomson, she re-established her science career in an animal laboratory at The University of Queensland.
25 Mackerras IM and Mackerras MJ, ‘Salmonella infections in Queensland’, Australian Journal of Experimental Biological Medicine, 27: 163-172
26 Mackerras IM and Pope P, ‘Experimental salmonella infections in Australian cockroaches’, Australian Journal of Experimental Biological Medicine 26, 1948
15

Whether the ‘Brisbane Line’ defence plan truly existed or has become a part of military mythology, the topic of populating northern Australia, or conceding to the tropic’s problematic climate, had been feverishly argued for decades prior to World War II. Indeed, the issue polarised delegates attending the 1920 Australasian Medical Congress held in Brisbane 10 years after the Australian Institute of Tropical Medicine’s short-lived establishment in Townsville. Some viewed the sparsely populated region as a natural protective factor, while others identified northern Australia’s development as an economic imperative and a matter of national security. Supporters of the latter, including Dr John Elkington, the first director of the Commonwealth Health Department’s Tropical Hygiene Division, warned that epidemic germs posed the real invasion threat, more dangerous than troops from Asian neighbours. ‘Disease is not to be explained or legislated away; it has no respect for geographical or statutory boundaries and it usually gives no warning of its onslaught. Its successful prevention and control is a highly technical process which carries responsibilities of life and death’, Elkington argued.1 He went on to stress the need for ‘the white race’ to colonise the Australian tropics ‘without loss of longevity, mentality, fertility, health and physique’.2
World War II undoubtedly heightened awareness of tropical ills. Soldiers suffered fevers and fungal and parasitic infections in the humid muddy conditions. By the end of September 1942, 1752 sick Australians had been evacuated from the Kokoda Track3, dysentery, malaria and scrub typhus proving as much an enemy as the Japanese. By June 1943, an estimated 25 000 Australians in Papua and New Guinea had contracted malaria.4 General Douglas MacArthur, the Allies’ Supreme Commander in the South West Pacific, reportedly said: ‘This will be a long war if for every Division I have facing the enemy; I must count on another Division in hospital with malaria, and a third Division convalescing from this debilitating disease’.5 That’s not to say the Japanese weren’t immune: just better prepared initially, succumbing in even greater numbers when supplies of quinine ran out.6
1950s02
General Douglas MacArthur saw malaria as a threat to success in the South West Pacific. Photo courtesy State Library of Queensland.
16

The Land Headquarters Malaria Research Unit’s assembly of medical researchers in Cairns made significant headway. Among its staff were Lieutenant Colonel Ian Mackerras and Major Josephine Mackerras.
Her work specifically — breeding and maintaining a stock of infected mosquitos for testing on volunteers, trialling synthetic anti-malarial drugs, is credited with reducing the incidence of infection in the armed forces. His work extended to identifying a mosquito Aedes polynesiensis as a carrier of dengue fever in the Pacific.
Against this background, the Mackerras alliance with Derrick, known and respected for his work on Q fever, made a tropical orientation obvious for the newly formed Queensland Institute of Medical Research.
’Fevers were cropping up, particularly in the cane cutters and the workers on the pineapple farms,’ recalls Ralph Doherty, who joined the Institute as a medical researcher after completing his medical studies and internship in the early 1950s.7 ‘It was an industrial problem and a medical problem because one chap may test positive and get workers’ compensation while another would test negative and yet have exactly the same disease, but miss out (on compensation). Both could be very sick, very unwell, for some time. This was a matter of great concern to the unions.’
Innisfail, Cassowary Coast’s main township, was known for its sugar industry, established in 1879 by Irishman Thomas Henry FitzGerald, who brought a workforce of predominantly Kanaka South Sea Islanders overseen by Irish labourers. Banana plantations also flourished. Both crops were labour-intensive back-breakers. Invariably the workers willing and able to withstand the humid tropics were new to Australia, seeking refuge from Italy, Greece and Malta following European turmoil.
Major Josephine Mackerras’ war-time malaria work was credited with reducing the incidence of infection in Australia’s armed forces.
The bacterial infection leptospirosis was also known as the ‘canecutters’ curse’ as it was often picked up while working in muddy fields, barefoot.
17

In July 1951, the Institute established a field station annexed to the local hospital in Innisfail, about 260 kilometres north of Townsville. The field station’s main role was to learn more about the fevers endemic in the area, and to look at ways of controlling, curing or preventing them. Particular attention was given to three ailments: leptospirosis (also called Weil’s disease), scrub typhus and dengue. Derrick wrote on the challenges of North Queensland’s fevers, not the least being its distinctive climatic zones: very wet coastal plains where sugar cane flourished, the cooler tablelands, and the hot dry plains, extending further west and up to the Gulf of Carpentaria.8 The cane cutters’ curse was leptospirosis, a bacterial infection most commonly picked up while walking barefoot through muddy cane fields. The bite from a mite Trombicula deliensis, found in densely vegetated areas, transmitted scrub typhus, while dengue fever was mosquito-borne, carried specifically by Aedes aegypti. In the 1950s, Derrick noted that ‘intelligently directed control measures can sweep the tide (of scrub typhus and dengue) back’.9
In their first 12 months at the field station, Dr Ces Sinnamon and research assistant Veda Pask travelled more than 32 000 kilometres from Ingham to Cooktown and inland to Herberton and Mareeba, investigating more than 300 patients.10
In March 1953, Ralph Doherty replaced Sinnamon in Innisfail. He was new to medical research, having spent a year in the small rural town of Alpha as a young doctor following graduation and internship, and he was eager to investigate.
In their first 12 months at the field station, Dr Ces Sinnamon and research assistant Veda Pask travelled more than 32 000 kilometres from Ingham to Cooktown and inland to Herberton and Mareeba, investigating more than 300 patients.
The Institute set up a field station at Innisfail in 1951, annexed to the local hospital.
18

‘The field station was a good training ground, requiring both clinician and scientific investigator in one. I’d see patients in hospital, get the blood samples, set up cultures, inoculate mice and record the details,’ he recalls.
While medical research had identified the causes of these fevers, there was still much to learn, notably incubation, diagnosis and treatments. ‘In North Queensland, the doctors in town were treating (leptospirosis) with pretty big doses of penicillin and getting good results despite European studies a few years earlier suggesting it (penicillin) didn’t work,’ recalls Doherty. ‘We confirmed that if you treat them early, people recovered from the Australian strains. Scrub typhus was being treated with another antibiotic of the day, chloramphenicol. We were fortunate that in the time I was in North Queensland, people recovered from scrub typhus without developing the complication of aplastic anaemia, a side-effect for which chloramphenicol developed a bad reputation.’
Science graduate Dorothy Elliott at work in the Innisfail field station laboratory, May 1955.
Patients weren’t always keen to come back for their check-ups so QIMR field researchers, like Ralph Doherty, tracked them down for the follow-up blood tests.
19

Between 1951 and 1955, 404 leptospirosis cases were closely examined. Incubation of the infection was eventually pinned down to 9.7 days.11 Lepto had been thought of as an occupational disease. It soon became apparent that it infected more people than cane cutters, with children, housewives, timber cutters and miners also affected. Josephine Mackerras’s 1956 investigations into unexplained fevers with headache and ‘burning eyes’ among patients at the Aboriginal mission community of Lockhart River turned out to be lepto too12, sourced back to water from a well.13
Within five years of the opening of the Innisfail field station, enough had been learnt and translated for improved diagnosis and treatment. The focus was to shift to preventive measures including better understanding animals’ roles as carriers of bacteria and viruses.
Dengue fever, bringing with it high temperatures, aching joints and muscles, extreme tiredness and a red spotty rash, had not been seen since the war. In 1953, 18 suspected cases were reported in Townsville. Blood samples were transported in dry ice to Brisbane for analysis and laboratory work-ups. By 1954, dengue fever had been reported as far north as Cairns, west to Biloela and south to Gladstone. Its re-emergence underscored the Institute’s need to maintain research into arboviral diseases.
This is a relatively simple sample of a mite by Dr Robert Domrow whose work at the Institute straddled three years until the 1970s with involvement continuing from his work at Queensland Museum.
Scientists captured what they saw through the microscope by drawing in fine detail.
DID YOU KNOWThe DNA molecule was found to exist in the form of a three-dimensional double helix in 1953. Molecular biology developed from this landmark discovery.
20
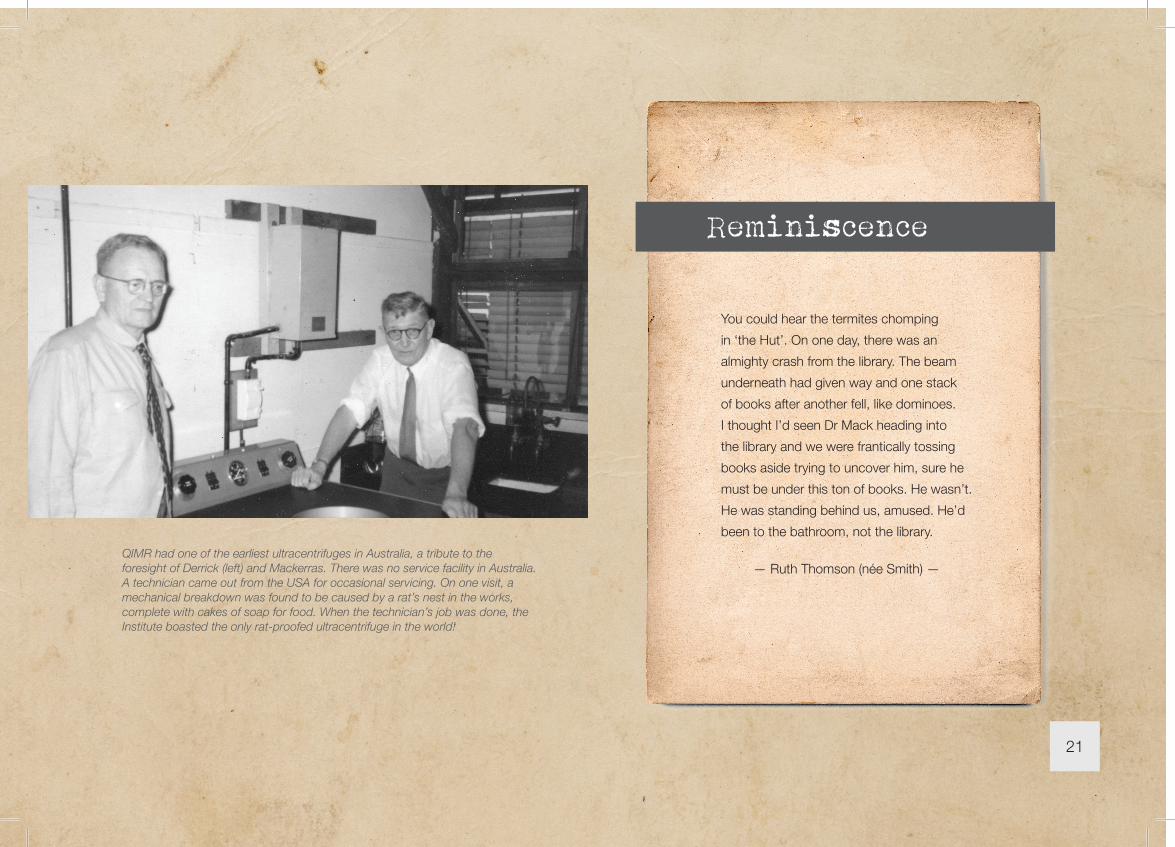
You could hear the termites chomping
in ‘the Hut’. On one day, there was an
almighty crash from the library. The beam
underneath had given way and one stack
of books after another fell, like dominoes.
I thought I’d seen Dr Mack heading into
the library and we were frantically tossing
books aside trying to uncover him, sure he
must be under this ton of books. He wasn’t.
He was standing behind us, amused. He’d
been to the bathroom, not the library.
— Ruth Thomson (née Smith) —
Reminiscence
QIMR had one of the earliest ultracentrifuges in Australia, a tribute to the foresight of Derrick (left) and Mackerras. There was no service facility in Australia. A technician came out from the USA for occasional servicing. On one visit, a mechanical breakdown was found to be caused by a rat’s nest in the works, complete with cakes of soap for food. When the technician’s job was done, the Institute boasted the only rat-proofed ultracentrifuge in the world!
21

To round out a decade of fevers, Derrick was called up in January 1958 to go west. He had traced Q fever back to infected cattle in 1934: now a shearing mob was dropping like flies at Tambo in central western Queensland. Could Q fever be the culprit? John Pope, who had commenced his science career in 1949 as a cadet at the Institute and was the younger brother of the Institute’s first female cadet Pauline, went with Derrick. He recalls with humour the approach to testing shearers for possible exposure to the bacteria: ‘We needed to get blood samples to check antibodies. Dr Derrick, who was a member of the Temperance League, reckoned the pub was the most likely place we’d find these fellas after work. And sure enough they were there: men with great muscly arms and veins like horses. Dr Derrick was doing the bleeding and he turned quietly to me and said ‘John, maybe you’d like to do the next chap’. And the bloke laughed and said ‘S’pose you’re going to tell me this is the first time you’ve ever done this?’ and I said ‘You don’t think we’d do that to you, do you?’ Truth is, it was my first venepuncture and fortunately successful: I’d only ever watched until then!’ Detailed analysis of animals followed before the Institute could report the source of the problem. Pope recalls: ‘The sheep had ticks engorged about the size of the first joint of your little finger, and when the sheep were shorn, the shearers cut the ticks off and they’d fall to the floor. It was summer, hot and dry, with all the dust and activity in the shearing shed, the organisms would go up in the air and be breathed in.’14
DID YOU KNOWIn the days before tissue culture, the latest technique used in animal virology was inoculation of small animals: rats, mice, ferrets and guinea pigs. The Institute would breed three or four hundred mouse litters a week. The mouse colony played a humble but vital role.
Investigators were to be further tested when asked to look at a family north of Brisbane, living on a pineapple farm. Mother, father and four grown-up sons had become ill over a nine-week period. They tested positive to Q fever but infection could not be traced to the usual sources, cattle or sheep. Enquiring minds searched for another route: milk was tested, and fertiliser from the meatworks. The unlikely carrier turned out to be bandicoots, nocturnal foragers, covered in infected ticks.15
22

ENDNOTES 1 Sir Raphael Cilento Medicine in Queensland; A Monograph, Council of the
Royal Historical Society of Queensland, 1963 p64
2 Ibid, p64
3 http://kokoda.commemoration.gov.au/jungle-warfare/malaria-and-dysentery.php accessed 26 April 2015
4 https://www.awm.gov.au/blog/2010/08/27/the-war-on-malaria/ accessed 26 April 2015
5 http://jmvh.org/article/army-malaria-institute-its-evolution-and-achievements-first-decade-1965-1975/ accessed 26 April 2015
6 Kokoda.commemoration.gov.au op cit
7 Interview with author, 9 February 2015
8 Derrick EH ‘The Challenge of North Queensland Fevers’, Australasian Annals of Medicine, vol. 6 no. 3, August 1957
9 Ibid, p175
10 QIMR Annual Report, 1952 p15
11 QIMR Annual Report, 1968
12 Lockhart River is almost 900 kilometres north of Innisfail on the Cape York Peninsula.
13 QIMR Annual Report, 1957
14 Interview with author, 3 March 2015
15 QIMR Annual Report, 1959
Photo courtesy State Library of Queensland.
23

Sometimes a gift can lead to a lifetime’s collecting. It may be battered, tattered, dog-eared … but there’s a fascination for it; an irresistible desire to acquire or learn more — and so it was at the Queensland Institute of Medical Research.
Shortly before leaving the Institute in 1961, Ian Mackerras learned of a collection of arthropods — midges, mites, ticks and other biting insects — held at the Sydney School of Public Health and Tropical Medicine. A team from that school and the Commonwealth Serum Laboratories (CSL) had caught the insects in the late 1950s around Townsville for research purposes. While the research team had since been dispersed, the collection remained, unprocessed, in a freezer. Mackerras, whose own intimate study of midges, mosquitoes and ticks had contributed to veterinary and human medicine, saw potential in this neglected, unwanted collection and sought it, still frozen, for QIMR purposes.
’It was an era of arbovirus stamp collecting,’ recalls Brian Kay, a cadet scientist in 1963. ‘The number of known viruses spread by mosquitoes increased from three or four to about 70 in Australia alone in just a few years.’1
1960s03
QIMR director Ralph Doherty chairs a World Health Organisation meeting on mosquito-borne viruses in the Philippines, 1969.
24

For years, the Institute had been part of a loose collaboration with the Walter and Eliza Hall Institute (WEHI) investigating the causes of epidemic polyarthritis, particularly Murray Valley encephalitis (MVE). QIMR’s contribution revealed that the MVE virus survived between epidemics in Australia’s north. Blood samples taken on Mornington Island in Queensland’s Gulf of Carpentaria, more than 2200 kilometres from the southern epidemic outbreaks, showed antibodies: evidence of previous MVE infection.
That led QIMR to further investigate the mosquito-borne virus situation in the north with another field station at Mitchell River Aboriginal Mission (now Kowanyama) for detailed, long-term study. ‘Our team isolated a number of arthropod-borne viruses, including MVE, as well as a range of others new to Australia and, in some cases, new to the world of science,’ recalls Ralph Doherty. Among them were Kunjin, a variant of the widespread West Nile virus, linked with both encephalitis and fever with a rash, and Sindbis virus, known then to be virulent in South and East Africa, Egypt, Israel, and the Philippines but not, until then, Australia, and the first isolation in Australia of bovine ephemeral viruses Akabane and Aino, both causing serious disease in cattle.
Field trips added enormously to the understanding of insects as vectors of infections. Intrepid researchers, often led by entomologist Harry Standfast, would take off for trappings, sometimes using baits, other times hoisting a windsock-sized net to trail above a Mini Moke. Over 12 months until June 1964, weekly trappings in Innisfail collected 37 423 mosquitoes representing 56 species. Back in Brisbane, the Institute’s insectary at Hut 8 bred insects for study. Standfast, Kay and others learned about environmental factors such as temperature, wind, the effects of moonlight, daylight and rain on mosquito activity, along with isolation of viruses.
On field expeditions to capture insects, devices ranged from small traps to windsock-sized nets rigged on top of vehicles.
25

And what of the CSL insects? They were, Doherty recalls, in quite a sad state on arrival. ‘There was evidence of previous thaw – freeze cycles. Hopes that any viruses would be detected were not great.’2 As it turned out, one suspension from a pool of 88 female saltmarsh mosquitos Aedes vigilax proved interesting: an inoculated mouse developed partial paralysis from an unknown virus, designated T48, affecting the brain. Experiments were repeated with a consistent result. The International Reference Centre at Yale Arbovirus Research Laboratory was sent freeze-dried samples of the micro-organisms. Its verdict? This was a distinct virus, deserving of its own name. Doherty, as the lead investigator, named it Ross River virus in honour of the site from which the mosquitoes were found.
John Harrison and Lee Emanuel at the Innisfail field station, 1960.
ROSS RIVER VIRUSFurther research confirmed Ross River virus was the main cause of epidemic polyarthritis — painfully swollen joints and muscles, extreme tiredness, fever and a raised red rash.
A blood test can now definitively diagnose Ross River fever from other look-alikes: however rest, gentle exercise and time remain the staple treatment.
Ross River fever cases hit a 20-year high in Queensland in 2015, with about 3500 cases confirmed in just the first three months.
26

A common house mouse, caught in Derrick’s pantry, was the unlikely source of another investigation that ultimately led to the Institute’s initial interest in cancer research. John Pope had begun his scientific career as a cadet at QIMR. For 14 years, he worked closely with Derrick and was accustomed to the animals brought in for investigations. In the house mouse, Pope isolated a virus. Over three years, Pope studied the virus in lab animals, observing that it had the ability to cause leukaemia. For this work, he was awarded a PhD — a first for the Institute — and a 12-month postdoctoral Rockefeller Foundation Fellowship, pursuing more work on virus-causing tumours in animals in the United States. ‘Virologists had established that a virus could cause leukaemia in animals. On that long boat trip back to Brisbane, I decided to pursue a suspicion that human leukaemia might also be of viral origin although there was no convincing evidence for this theory,’ Pope recalls.3
On the other side of the world, English medical researcher Anthony Epstein was also mulling over the possibility that viruses, known to cause illnesses like influenza or chickenpox, could also be responsible for some human cancers. Epstein, who had also trained at Rockefeller Institute, had been baffled as to where to start until he had heard a doctor from Uganda speak of a childhood cancer common throughout sub-Saharan Africa. Burkitt lymphoma, named after that doctor, Denis Burkitt, was unknown in the west. Epstein reportedly thought, ‘A cancer which is restricted by temperature and rainfall: that’s where to look for a cancer virus!’4 Epstein and colleagues managed to culture cells from biopsies of Burkitt lymphoma. When he looked at these cells using an electron microscope, Epstein saw a striking resemblance to the herpes virus. Intense investigation by several laboratories made it obvious that this virus was a new member of the herpes family. It became known as Epstein Barr virus (EBV), Barr being Epstein’s research assistant Yvonne Barr. The first human cancer virus had been found.John Pope — his work led to the
Institute’s move into cancer research.
A common house mouse was the unlikely source of another investigation that ultimately led to the Institute’s initial interest in cancer research.
27

Meanwhile in Brisbane, Pope also had succeeded in growing cell lines from Burkitt lymphoma biopsies, from two patients in Papua New Guinea. In 1965, QIMR did not have an electron microscope — so much more powerful than the conventional light microscope — and had to call on the Australian National University in Canberra to assist. Excitingly, EBV was confirmed in both. ‘In Australia in 1966, telex was the best communication and we heard that Tony (Epstein) was in New Guinea, flying south. Doherty, the Institute’s director, managed to contact Tony. We were able to go to the Brisbane airport, bring him back to my lab, show him the GOR culture and get him back to the airport in time.5 We were to enjoy a happy collaboration built on a lucky set of events,’ Pope recalls.
He also found EBV particles in cell lines grown from patients with leukaemia. Puzzlingly though, these cells were not of malignant origin. Pope went on to show that EBV was able to ‘immortalise’ one of the components of human white blood cells, known as B lymphocytes. This process became known as ‘transformation’ and has become critical in understanding the link between EBV and human disease.
Epstein Barr virus seen through a microscope: the virus causing glandular fever and some rare, and nasty, cancers.
28

In a further piece of truly intuitive investigation, Pope’s laboratory sought a link between EBV and infectious mononucleosis (IM), more commonly known as glandular fever, the ‘kissing disease’. Pope obtained blood samples from nurses at Royal Brisbane Hospital and looked for a rising immune response. There was none. He knew that infectious mononucleosis had a very long incubation period and that by the time people presented with symptoms, the immune response could have already spiked. His line of enquiry was to be proven correct, only Pope would not go down in history for the discovery: American virologist Werne Henle beat him to publication. EBV was to provide decades’ more investigation.
In 1961, Ian Mackerras resigned, taking up a research fellowship in the Commonwealth Scientific and Industrial Research Organisation’s division of entomology in Canberra. Within months, his wife had joined him. Derrick served as the Institute’s director until his retirement in 1966; to be replaced by Ralph Doherty, not quite 40 years old and none too fussed with newspaper reports drawing attention to his boyish, fresh face.
Fluorescence microscopy played a vital role in the early research into EBV.
The tea room had a caneite ceiling and
possums made happy homes in the space
above with a few entry holes in the ceiling.
It was often an amusement for visitors to
be able to pass biscuits to the possums
begging for food.
— John Pope —
Reminiscence
29

30

By the mid-1960s, Hut 8 was a source of derision. The Sunday Truth newspaper wrote of ‘scandalous conditions’ as world-class researchers worked in one of Brisbane’s greatest fire hazards.6
Publicly Derrick had maintained diplomacy, reportedly saying: ‘It’s a matter of balance. It will cost 600 000 pounds for a new Institute. Two schools can be built for that’.7 Privately he was taking no risks. ‘There was an explosives store adjacent in which the alcohol and inflammables were kept. The fire brigade told Dr Derrick that the building would take just 15 minutes to burn from end to end. That’s why he took all his papers home every night. He wasn’t going to risk losing his life’s work,’ Pope remembers.8
When Tony Epstein visited the Institute, he was surprised by the crude and dusty lab conditions. ‘Conducting tissue culture in the old hut was fraught with the hazard of contamination. Ill-fitting windows and gaps in the ceiling combined with the warm humid summers in Brisbane to regularly cause a wipe-out of our experiments by fungal contamination,’ Pope recalls.9
For some years, Derrick had lobbied at home and abroad for improved facilities, maintaining long-distance communication with the Wellcome Trust, a philanthropic offshoot of the multinational pharmaceutical company Wellcome, advocating for medical research. In June 1966, a three-paragraph letter from Wellcome Trust dashed his hopes: his application for funding support to build a new institute ‘did not obtain the requisite priority’.10
The brick building adjacent to Hut 8 stored explosives. Ted Derrick, for one, always took his paperwork home at night for fear of a fire.
Second director Ted Derrick snowed under by paperwork.
31
DR EDWARD (TED) HOLBROOK DERRICKDirector 1961–1966
Deputy director 1947–1961
Born 1898, Victoria
Medical practitioner, pathologist
Discovered the cause of Q fever
Died 1976
32

ENDNOTES 1 Interview with author, 10 February 2015
2 Interview with author, 9 February 2015. Read also ‘Epidemic Polyarthritis – the search for its cause’ by Ralph Doherty in Milestones of Australian Medicine, edited by John Pearn, Amphion Press, Brisbane, 1994
3 Interview with author, 10 March 2015
4 Cancer Virus, the story of Epstein Barr Virus, Dorothy H Crawford, A Rickinson and I Johannessen, Oxford University Press, 2014
5 GOR or Goratola was the name John Pope gave to the EBV-positive cell line as a code for the patient from which the sample had been grown.
6 Sunday Truth, 7 November 1965
7 Ibid
8 Interview with author, 10 March 2015
9 Interview with author, as above
10 Letter from PO Williams to EH Derrick, 13 June 1966
I spent that first day – and year – assigned
to the mouse house. I smelt like a walking
ammonia bomb on the homeward journey.
— Brian Kay —
Reminiscence
33

In 1973, Pat Killoran, the head of Queensland’s Department of Aboriginal and Island Affairs made a grave observation in his departmental annual report. Aboriginal people, he said, had had enough of being continually ‘researched, inquired into and investigated’. Their wish was to ‘be left alone…to settle to a pattern of conventional and normal living’.1
His comments were echoed in an opinion piece published in the Medical Journal of Australia the following year. A phony war was being waged, the column contested, full of bluster and rhetoric, a build-up of intelligence data evident with very little decisive action.2 Less curiosity and more outcomes were needed if Indigenous health issues were to be truly tackled.
Back at QIMR, those comments stung. Many researchers were well known for their field work at Aboriginal missions and remote communities. Hadn’t they spent 10 years at Mitchell River mission (now Kowanyama ) focusing on the incidence of airborne viruses, trying to unravel the lifecycle of the virus causing Murray Valley encephalitis?
1970s04 Many researchers were well known for their field work at Aboriginal missions and remote communities.
With so much work in the far north, a field station was established within the then-Mitchell River Aboriginal Mission, now known as Kowanyama.
34
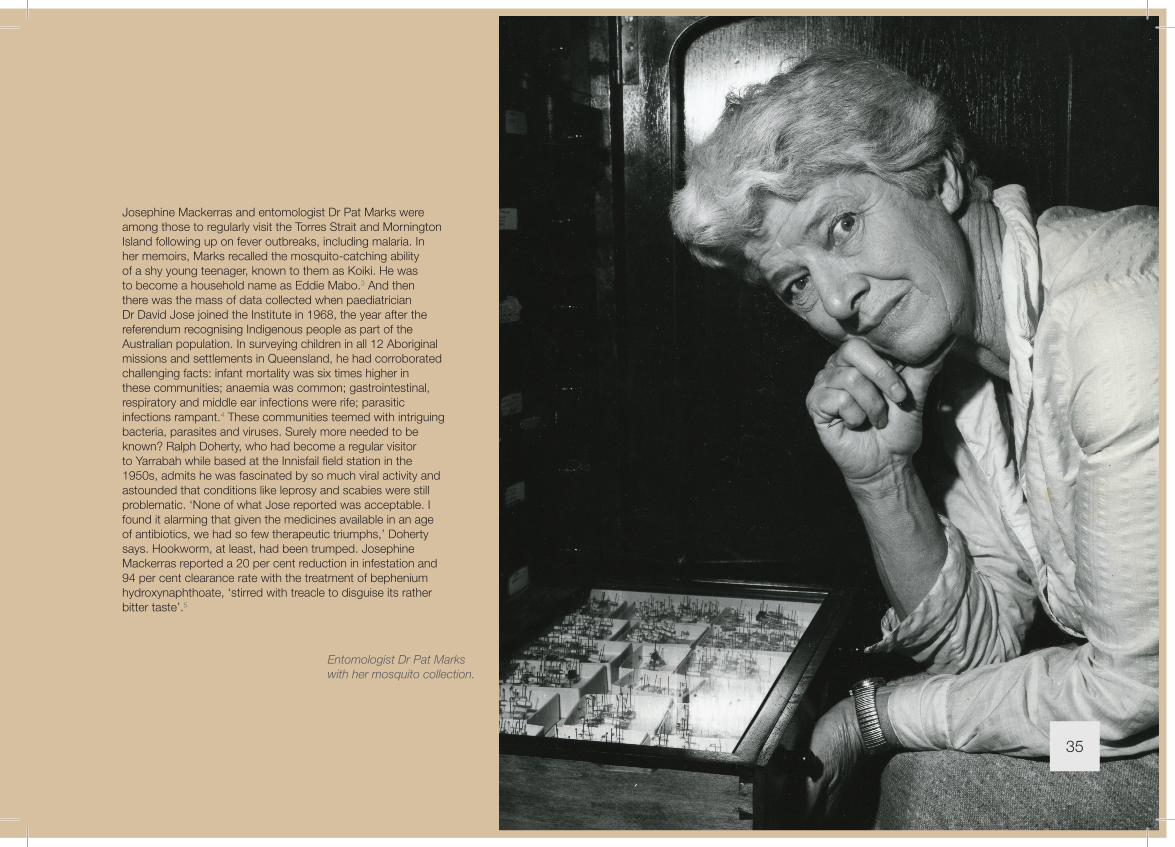
Josephine Mackerras and entomologist Dr Pat Marks were among those to regularly visit the Torres Strait and Mornington Island following up on fever outbreaks, including malaria. In her memoirs, Marks recalled the mosquito-catching ability of a shy young teenager, known to them as Koiki. He was to become a household name as Eddie Mabo.3 And then there was the mass of data collected when paediatrician Dr David Jose joined the Institute in 1968, the year after the referendum recognising Indigenous people as part of the Australian population. In surveying children in all 12 Aboriginal missions and settlements in Queensland, he had corroborated challenging facts: infant mortality was six times higher in these communities; anaemia was common; gastrointestinal, respiratory and middle ear infections were rife; parasitic infections rampant.4 These communities teemed with intriguing bacteria, parasites and viruses. Surely more needed to be known? Ralph Doherty, who had become a regular visitor to Yarrabah while based at the Innisfail field station in the 1950s, admits he was fascinated by so much viral activity and astounded that conditions like leprosy and scabies were still problematic. ‘None of what Jose reported was acceptable. I found it alarming that given the medicines available in an age of antibiotics, we had so few therapeutic triumphs,’ Doherty says. Hookworm, at least, had been trumped. Josephine Mackerras reported a 20 per cent reduction in infestation and 94 per cent clearance rate with the treatment of bephenium hydroxynaphthoate, ‘stirred with treacle to disguise its rather bitter taste’.5
Entomologist Dr Pat Marks with her mosquito collection.
35

Under Doherty’s directorship, the Institute formally established its first Aboriginal health research unit in 1971. An anthropologist joined the team of biomedical scientists; Doherty convinced that understanding culture was as important to success as biomedical investigations. Killoran’s comments signalled tentative steps towards self-determination. Suddenly, ethics were being drawn into question. Was it really okay to arrive in a community and expect children to line up for mouth swabs, faecal samples and body inspections without fully-informed parental approval? The intentions had been good and honourable but after Killoran’s statement, eagerness lost momentum and Indigenous health, as a research area waxed and waned, for at least 30 years.6
Virology was one area gaining momentum, spurred on by John Pope’s Epstein Barr virus work. A young scientist, Denis Moss, who had begun as a cadet in 1962, was working in Pope’s laboratory in 1974 when he made the seemingly trivial observation: some white blood cells, lymphocytes, exposed to EBV seemed to transform initially and then died within 10 to 14 days. ‘German virologist Harald zur Hausen was visiting the lab and I was scheduled to deliver a seminar.7 I clearly remember the moment during the presentation, when my eyes fixed on the figures displayed by the overhead projector and — talk about a light bulb moment! — I saw the solution to this problem of dying cultures and what it meant in terms of making an EBV vaccine,8’ remembers Moss wryly. Early experiments had used foetal-cord blood from women delivering babies at
Visits to Aboriginal communties were well-intended, the presence of illnesses so stunningly higher than in the wider Queensland population that researchers wanted to know why. By 1973, however, First Australians were saying ‘enough is enough’. They wanted more positive outcomes, and less curiosity. Some argue the same could be said of the Close the Gap campaign in 2007.
A seemingly trivial observation by young scientist Denis Moss in 1974 became a lifetime obsession with Epstein Barr virus.
The Institute formally established its first Aboriginal health research unit in 1971.
36

the Royal Women’s Hospital. All of these samples were non-immune. Then Moss had used blood from laboratory donors, some of whom were immune to EBV. ‘Only cultures from immune individuals died; cultures from non-immune individuals continued to grow. If we could unravel the mechanism involved in causing these cultures to die, we had a real chance of making an EBV vaccine!’ The cell death later became known as ‘regression’, the result of killer T cells in immune individuals. ‘If only we could make a vaccine that induced these killer T cells in non-immune people, we might be able to prevent EBV-associated diseases,’ Moss thought at the time. Moss retired in 2015, the vaccine eluding him although his findings remain at the core of progressive immunotherapy work, through his protégé Rajiv Khanna.
Victoria Park had only ever been intended as temporary premises. Yet it was well into the 1970s before an alternative was found. Derrick, Doherty and the QIMR Council had pressed the issue of inadequate accommodation for years: indeed a 1970 Cabinet-initiated committee on the future of the Institute had recommended rehousing as a priority. A site had been found, at the back of the children’s hospital within the Royal Brisbane campus, off Bramston Terrace. Money was the issue. The Queensland government would not commit to the expected £68 000 price tag. For almost a decade, Derrick had maintained long-distance correspondence with the Wellcome Foundation, the philanthropic arm of the pharmaceutical multinational, seeking its financial support. It wasn’t forthcoming. Health Minister Douglas Tooth offered Doherty a vacant office block in
37

the city.9 Doherty turned it down, saying the accommodation was too small. ‘I was perhaps too blunt. Tooth’s response for the next few years was notably cool,’ Doherty later admitted to Mackerras.10 Plans were scaled back and budgets pruned before final government approval was granted. Some cynics say the Institute may have remained at Victoria Park longer if not for another paper circulated around the Cabinet room at the same time: a traffic plan for Brisbane requiring part of the park for road works. The northern busway now skirts the golf course, its Herston bus stop standing in Hut 8’s place.
Institute staff were both excited and dubious about a new home after so long. And then Murphy’s Law struck — the first building contractor went bankrupt and more delays ensued. In October 1976, QIMR relocated to its new laboratories, officially opened by Governor Colin Hannah in February 1977.
Derrick did not live to see this. He died in July 1976, aware that an appropriate home was imminent.
Governor Colin Hannah signs the visitors’ book at the new Bramston Terrace headquarters of QIMR, February 1977.
38

ENDNOTES 1 Department of Aboriginal and Islander Affairs Annual Report, Queensland,
1973
2 Medical Journal of Australia, vol2 no 5 1974
3 Elizabeth Marks, Mosquitoes and Memories, Memoirs, accessed online at http://www.serf.qut.edu.au/downloads/collections/en_marks/mosquito_mem_pt2.pdf, 24 April 2015. Koiki was Eddie Mabo who rose to prominence as the successful principal plaintiff in the landmark High Court of Australia ruling on native land title.
4 QIMR Annual Report, 1973
5 QIMR Annual Report, 1960
6 Under Michael Good’s directorship, an Indigenous health unit was established headed by Koori woman Janelle Stirling that went beyond the research to include encouraging young Aboriginal and Torres Strait Islander students to explore medical science as a career option. In 2015, awareness is such that all research groups consider the relevance their work has on the health of Australia’s First People.
7 Zur Hausen researched on cancer of the cervix, discovering the role of papilloma viruses, for which he received the Nobel Prize in Physiology or Medicine 2008.
8 Interview with author, February 2015
9 The Courier-Mail, 9 January 1972
10 Personal letter, 29 August 1978 to IM Mackerras
The new QIMR in Bramston Terrace, Herston.
39

World Expo 88, the largest bicentennial celebration of European occupation of Australia, is widely credited with Brisbane’s coming of age. Rallied by the theme song Together we’ll show the world1, it was a six-month party attracting nearly 16 million visitors into a global village populated by 36 nations, all Australian states (even three American states showing off their individuality) and countless corporates and multi-lateral organisations. Brisbane shook off its oversized country town image and embraced alfresco living and multiculturalism.
The director of QIMR at the time, Chev Kidson, is also widely recognised as the catalyst that transformed a small well-respected medical research body working on mostly local health issues into an international player.
1980s05The director of QIMR at the time, Chev Kidson, is also widely recognised as the catalyst that transformed a small well-respected medical research body working on mostly local health issues into an international player.
Above: World Expo 88. Image courtesy Brisbane City Council.
Director Dr Chev Kidson could see the world shrinking and the importance of being part of a global village.
40

A molecular biologist and doctor of medicine, Kidson’s years in the United States as a researcher coloured his outlook.2 He saw beyond the borders of Queensland. He was, fans and detractors alike admit, a visionary. Kidson saw health and disease entwined with economic development, and tropical countries grappling with endemic infections and swirling epidemics. He felt a social responsibility to act to help near-neighbours, and he acknowledged self-interest too. The world was shrinking: with so much air travel, disease could spread…fast. It was in Queensland’s interests to work to contain, prevent or cure illnesses offshore that had potential to affect locals.
‘The health department did not want to believe dengue was back in Queensland.’
The re-emergence of dengue fever after nearly three decades was a case in point. The first cases were seen in March 1981 in Cairns and Townsville. An outbreak was recognised on Thursday Island from October. By May 1982, almost 40 per cent of the island’s population were infected. Isolated cases were being reported from other islands in the Torres Strait as well as other North Queensland towns.3 ‘The health department did not want to believe dengue was back in Queensland. “It’s a third world problem” we heard,’ recalls Brian Kay. ‘At the same time, Texas in the USA confirmed a recurrence. Clearly, either Texas or Queensland had joined the third world or dengue wasn’t so selective.’ A telegram from Thursday Island’s medical superintendent to the health department’s head office advising he was the latest victim of what he suspected to be dengue fever finally galvanised authorities. ‘Everyone was pretty horrified.’ Entomological surveys indicated the carrier, Aedes aegypti, was widely found throughout Queensland, as far south as Dirranbandi and west to Mornington Island. Once on Thursday Island, Kay quickly initiated successful local control measures. ‘Litter and rusty water tanks harboured the mosquitoes. We needed a clean-up campaign, as well as insecticide and fogging.’
Brian Kay is world-renowned for his mosquito control tactics, needed with the re-emergence of dengue fever in Queensland in 1981.
Aedes aegypti, a vicious daytime biter spreading dengue fever.
41

By the mid-1980s, QIMR was recognised as Australia’s centre for medical entomology, best able to mobilise expertise and effort to control mosquito-borne disease outbreaks. It was also a World Health Organisation reference centre for arboviruses. Yet for all the work carried out on Murray Valley encephalitis, Ross River fever and dengue in the past 30 years, malaria had been virtually ignored. Aside from occasional cases in the Torres Strait, it didn’t rate mentioning, not like the other tropical fevers QIMR had concentrated on. However, South East Asia was attracting more young Australian travellers whose parents and grandparents remembered the impact of malaria on soldiers in both World War II and the Vietnam War. Significant public funds were earmarked for a malaria vaccine. ‘Funding was available; there was a call for this. Work on MVE and Ross River fever, in Kidson’s mind, was too esoteric,’ recalls Brian Kay. Kidson recognised a need for a malaria vaccine for far more than Australian travellers. Malaria was the third most prevalent parasitic disease in the world with about 800 million cases a year. While eager to find a vaccine, Kidson was also realistic. ‘The advent of a useful vaccine could greatly assist but it would be foolish to imagine that vaccines alone can solve the malaria problems. Integrated control programs are needed too,’ Kidson maintained.4
Rusty water drums made perfect breeding grounds for virus-carrying mosquitos. So did piles of old car tyres. A big clean-up was needed.
42

Serendipity was to play a hand in guiding new research interests. Three major advances in scientific technology had come together in the late 1970s: the creation of monoclonal antibodies5; discovery of how to grow malaria parasites outside the body6; and the promise of cloning malaria genes arising from early stages of molecular biology. Development of a malaria vaccine using new monoclonal and molecular biology technologies presented an opportunity for Australia to take a leadership role in these emerging technologies. Such a move was strongly supported politically by the likes of federal science minister Barry Jones, and Kidson knew it: QIMR needed to capitalise on technological advances to make its name abroad. Allan Saul, recruited as a post-doctoral fellow, recalls how the Institute quickly exploited the first two developments: ‘Very soon after Trager and Jensen’s discovery, we had the first lines of Plasmodium falciparum7 growing in the lab. These came from patients infected with malaria in Papua New Guinea. We also became one of the first groups in Australia to make monoclonal antibodies, from mice vaccinated with cultured malaria’.8
Cancer geneticist Georgia Chenevix-Trench, another Kidson recruit, recalls the eagerness to try out and adapt emerging techniques. ‘When we (Chenevix-Trench and husband, geneticist Nick Martin) came to Brisbane, there was no email, no fax, and no other research going on elsewhere in Brisbane. QIMR was Queensland’s only institute of medical research. Molecular biology was just starting off here and I was seen as an overseas expert because that’s where I’d come from.
‘We felt we’d come to the end of the scientific world! But I remember Peter Upcroft (molecular biologist, also hired by Kidson) talking about the most exciting development in molecular biology at the time, polymerase chain reaction. It was such a simple, if somewhat mind-numbingly tedious, technique to adapt, using three water baths of different temperatures.’
New arrivals to the Institute like Saul, Martin, Upcroft and Chenevix-Trench brought cutting-edge skills and new thinking, supporting Kidson’s expansionist vision of QIMR as a research leader in the global village. They faced initial coolness and wariness from the Institute’s ‘old guard’. ‘The Institute was very small, had existed largely from funding from the state government and had a very public service mentality,’ recalls Saul. ‘There was quite a lot of tension among some of the staff who feared that all these new people Chev was bringing in would dilute the available funding and change the culture.’ Denis Moss, an Institute ‘lifer’, agrees: ‘Chev inevitably stood on toes. He encouraged many to leave voluntarily, others to leave kicking.’
PROFESSOR CHEV KIDSONDirector 1978–1990
Born 1932, Australia
Graduate, The University of Sydney Medical School
Doctor, molecular biologist
Foundation Professor of Medical Biochemistry at The University of Queensland
Became Professor in Tropical Medicine at Mahidol University, Bangkok, Thailand on leaving QIMR
Died 2014
43

While most recruits were relatively junior, trained in emerging scientific fields, some key senior appointments shaped the Institute’s future directions. Australian-born Kay Ellem had worked in the United States for the previous 20 years. He was internationally renowned for his work in cancer cell biology. Like Kidson, he was a University of Sydney medical school alumnus, graduating a few years ahead of the new Institute director. Boreham came from England to head the Institute’s parasitology unit. Experienced in parasitology, entomology and pharmacology, Boreham had worked in Gambia and Kenya under the auspices of the British Medical Research Council and the World Health Organisation. Bob MacLennan, a University of Queensland medical graduate, had the unusual distinction of having worked on all continents in the world. While at the International Agency for Research on Cancer, MacLennan had pressed for global cancer registration. He was brought in to establish the Institute’s first program of research in cancer epidemiology. ‘Bob MacLennan had the foresight to see that genetics played a big part in epidemiology,’ recalls Nick Martin, a behavioural geneticist whose interests in psychiatric illnesses were to be tempered by the Institute’s skin cancer research. ‘The biggest risk factor for most diseases is family history, which in most cases means genes.’
Kidson balanced young, eager ‘bright minds’ with internationally distinguished established players, including Kay Ellem, Bob MacLennan and Peter Boreham.
44

MacLennan’s own research interests had been directed at bowel cancer, leading the Institute to investigate the link between diet and cancer. Gynaecological cancers were also to become central to the Institute’s research efforts along with the viral-influenced cancers. ‘If you put “gene” and “cancer” in the same grant application, you were almost guaranteed to get funding as the link seemed so novel,’ remembers Chenevix-Trench, whose lab was part of a global collaboration that identified a gene fault heightening the risk of breast cancer; the same gene fault that led Hollywood star, Angelina Jolie, to undergo a preventive double mastectomy in 2013, followed by removal of her ovaries.
Cancer geneticist Georgia Chenevix-Trench.
45

But it was skin cancer that became synonymous with QIMR research.
The Sunshine State was dubiously known as the melanoma capital of the world. Folklore suggested why — a fair-skinned population oiling up to gain a tan — but scientific evidence was lacking. QIMR’s cancer research spanned from cell biology to human behaviour, environment and genetics.
The Sunshine State was dubiously known as the melanoma capital of the world.
Epidemiologist Adele Green.
The number of moles on a person’s skin is the strongest risk factor for melanoma; the greater the number of moles, the higher the risk. In epidemiological studies, QIMR nurses count the numbers of moles of different sizes on the skin of study participants to assess each person’s risk of melanoma.
46

In 1986, epidemiologist Adele Green sought the support of the community of Nambour, a sugar town on the Sunshine Coast north of Brisbane, to study locals’ chances of developing skin cancers. ‘Letters were sent, using the electoral roll, inviting participation and people were so excited,’ recalls team member Lea Jackman. ‘We turned up at the Chamber of Commerce where we were taking registrations, and doing skin cancer checks. It all took time – everything was paper-based, there was no computer then. Photos were taken of hands and faces and we’d take silicone imprints of the backs of the hands too. What a messy process that was! We had to slap a gooey substance onto the skin and peel it off to reveal the lines, rating them from one to six to indicate sun exposure and skin damage.’ That research led to the world’s most extensive population study of skin cancer spanning 20 years. It confirmed the effectiveness of regular sunscreen use in minimising the most common of skin cancers, squamous cell carcinoma, and paved the way for the Cancer Council’s popular ‘Slip, Slop, Slap!’ sun-safety campaign.
‘We may have started with a local view of disease but our view is very much global: what difference can we achieve in a given area of disease universally,’ Green stresses.
Epidemiologist Adele Green’s study of sun exposure and skin damage paved the way for the popular Slip, Slop, Slap! skin cancer message.
An early Slip, Slop, Slap! Campaign. Image courtesy Cancer Council QLD.
47

Kidson’s influx of recruits swelled staff from 60 to 150, creating a sardine tin-like environment, relegating some to conditions reminiscent of Hut 8. Geneticist Martin, recruited in 1986, worked in a demountable shed for the first months of his appointment. Green, who had joined in 1987, worked in the sick bay ‘because there was no office spare and I didn’t need a wet lab’.9 By the time Kidson departed, QIMR’s budget was about 10 times that of 1977–78 with a 60-fold escalation in competitive grant monies10: the QIMR Trust also had been founded to encourage bequests and community and private contributions (in 1980, the Queensland Government covered 70 per cent of the Institute’s budget).11 On 23 March 1988, Queensland Parliament passed amendments
Green ‘goop’ created a silicone imprint of the lines and ageing of the back of participants’ hands.
The survey techniques used were paper-based. Now most is online.
Nambour residents were very keen to participate in the skin cancer research.
to the Act under which the Institute was constituted. The Institute, until then loosely part of the Department of Health’s organisational structure, became a statutory body, with increased responsibilities transferring to the QIMR Council to administer the Institute directly, on behalf of the Minister for Health. Scientific staff no longer had public service tenure; they were instead judged on their scientific excellence. And their endeavours were extending well beyond Queensland borders, attracting visiting researchers and inviting collaborations abroad into Papua New Guinea, China, Thailand, Vietnam and the Solomons. As the Expo jingle went, QIMR was ‘showing the world what it could do’.
48

ENDNOTES 1 Listen to the lyrics at https://www.youtube.com/watch?v=zasJJIHswno
2 Chev Kidson was the foundation professor in Medical Biochemistry at the University of Queensland immediately before his appointment to the Institute.
3 ‘Dengue fever. Reappearance in northern Queensland after 26 years’, first published in Medical Journal of Australia 04/1984; 140(5):264-8, accessed from http://www.researchgate.net/publication/16496791_Dengue_fever._Reappearance_in_northern_Queensland_after_26_years, accessed Apr 16, 2015
4 QIMR Annual Report, 1985-86, p7
5 Read about Cesar Milstein’s contribution at http://www.whatisbiotechnology.org/exhibitions/milstein
6 Read about William Trager and JB Jensen’s contribution at http://www.sciencemag.org/content/193/4254/673.abstract
7 Plasmodium falciparum is the protozoan parasite that causes malaria.
8 That research, somewhat circuitously, also led to the development of better pre-natal testing of pregnancies at risk of haemolytic anaemia in newborns.
9 Interview with author, 2 February 2015
10 Ralph Doherty private papers
11 QIMR Annual Report, 1980
49

In taking his last sabbatical at QIMR in 1988, internationally recognised hepatologist and University of Queensland clinical researcher Lawrie Powell became well acquainted with the Institute’s staff and science. His appointment as fifth director in 1989 saw the arrival en bloc of his research team, co-chief investigators June Halliday and Graham Cooksley among them. They had worked together on iron metabolism and haemochromatosis (HC) and liver disease for years, funded by successive NHMRC program grants since 1982.
For Halliday, the move brought her career full circle.1 ‘I’d met Ian Mackerras on a science trip to Heron Island in the late 1940s. At the end of my second year of university, a friend and I had holiday jobs squeezing fruit on an assembly line at West End. We literally bumped into Dr Mackerras in the city after a fairly miserable first week of making juice and once he heard what we were doing, he immediately offered us vacation scholarships!’ she recalls.2 Halliday (formerly June von Alpen) received the first Mackerras scholarship to undertake an honours degree in biochemistry at the Institute in 1950 and 1951 and specialised in liver disease and iron research from 1969.
Prior to his arrival, Powell’s lab had developed a blood test to measure serum ferritin, the iron protein in the blood, and used it as a marker to assess hepatic iron concentration. At the Institute, Cooksley extended the research repertoire to include the immunology of liver disease and viral hepatitis. The team demonstrated that while the liver could withstand and recover from many insults, cirrhosis was a step too far, predisposing patients to liver cancer. But it was the team’s description of HC as a common familial iron-overload disorder which raised eyebrows, with many in medical circles accusing the group of over-diagnosis. A later epidemiological study confirmed one in 10 Australians of European descent had the iron-overload gene yet were asymptomatic.
1990s06
PROFESSOR LAWRIE POWELLDirector 1990–2000
Born 1934, New South Wales
Graduate, The University of Queensland Medical School, 1958
Clinical hepatologist and liver researcher
Order of Australia 1990
Now Director of Research at Royal Brisbane and Women’s Hospital (RBWH), Director of the Centre for the Advancement of Clinical Research at RBWH, Professor Emeritus at The University of Queensland
50

The team’s efforts identified the likely location of the gene responsible. ‘It took a huge effort to identify a microsatellite marker as either within or very close to the HC gene. We debated among ourselves whether to submit this for publication or withhold,’ recalls Powell. ‘I erred on the side of caution but was out-voted on the ‘publish or perish’ premise. The article was submitted and published in the American Journal of Human Genetics. We discovered later that a group in St Louis had raised $20 million from a venture capital company to employ 30 postdoctoral scientists to focus on finding the gene – and we were able to eventually confirm their findings over a weekend using our extensive database with demographic details and DNA samples.’3 Further research has confirmed the carrier frequency of the mutated gene is one in 10 in the general population or one in 200 affected. The race to clone the gene responsible for causing HC was on, and QIMR was one of six groups internationally trying to do it.4
‘Too much iron is not a good thing – nor too little. Too much ferritin stored in the liver damages it,’ explains Halliday. ‘We now know that haemochromatosis, once thought of as rare and only in men, is a quite common inherited disorder and that it can be readily controlled. Early diagnosis prevents complications and allows family members to be diagnosed and treated too.’
Liver researcher June Halliday made a surprise return to the Institute as part of Powell’s entourage. Her science career began at the Institute in the late 1940s, nurtured by Ian Mackerras. 51

HAEMOCHROMATOSIS
Nature Medicine declared
haemochromatosis the ‘genetic
disorder of the 21st century’.5
Tests are now widely used to
diagnose iron deficiency and
iron-overload.
QIMR Berghofer Medical
Research Institute continues to
lead liver disease research.
Nature Medicine has declared haemochromatosis, the focus of much of Lawrie Powell’s lifetime research, ‘the genetic disorder of the 21st century’.
52

As a medical practitioner and researcher, Powell was not unique. About five per cent of the Institute faculty were then medically trained. Within the next 10 years, the proportion of medical researchers who were both scientists and clinicians would rise to 15 per cent. ‘Medicine provides one with perhaps the most embracing background available to understand our biological world,’ his deputy director, cancer researcher Kay Ellem, once reflected.5 Just as Kidson had introduced global thinking, Powell firmly believed in research for the relevance of patients. ‘The importance of collaborative research between basic scientists and physician scientists was apparent. Medical research should be clinically relevant,’ Powell says. ‘Together we could address patient and disease oriented research.’6
‘Translational research’ as it was being called, was very much on the minds of government funding bodies too. It was one thing to reveal an unknown, but discovery alone did not add to the gross domestic product. Governments wanted returns on their investment: they wanted tangible products. In 1990, the Australian government established a program encouraging private–public collaboration, linking researchers with industry for a more focused view to commercialisation. Cooperative research centres, or CRCs, operated across manufacturing, information services, mining and infrastructure, agriculture, environmental services and medical sectors. QIMR became home to two CRCs: Vaccine Technology and Discovery of Genes for Common Human Diseases. QIMR became the first medical research institute outside Victoria to partner with the Australian Medical Research and Development Corporation (AMRAD), its charter to commercialise Australian medical discoveries.
Kay Ellem, Powell’s deputy and acting director for some time, had a knack for fighting through red tape as well as uncovering biological mysteries.
53

One of the CRC for Vaccine Development’s earliest announcements was a world-first human trial of a gene therapy approach to melanoma. The volunteer, recruited in November 1993, had advanced secondary cancers of the lung and brain. The trial involved genetically engineering a hormone extracted from the patient, a process carried out by US biotech Samatrix Therapy Corporation, and reinjecting it. Formal approval was also required of nine separate regulatory institutions in Australia and the USA, a task skilfully negotiated by Kay Ellem. ‘I’m not sure anyone would even contemplate this task today, let alone achieve success,’ ponders cancer immunotherapist Chris Schmitt, an Ellem protégé. The patient received three fortnightly injections beginning in January 1994. The trial had brought together cell biology, cancer and virology researchers across the Institute and they held their breath, as one, awaiting a response. Theirs was more than pure scientific curiosity. The volunteer was one of their own: Greg Johnson, the lead researcher in the Leukaemia Foundation of Queensland’s Daikyo Research Laboratory. This was a last ditch attempt to stem the cancer using a therapy he himself had helped pioneer. Johnson died within three months of the last injection but while he’d lost his own battle, he’d provided hope for future cancer sufferers: a clear immune response had been evidenced, and on post-mortem there was little sign of inflammatory cell infiltration in his cancers. The killer T cell had done its job: cancer immunotherapy really had potential.
AN ODD INHERITANCE
Since 1992, scientific animal technician Mary Duke has been on
nursery duty for aquatic snails smaller than a baby’s fingernail.
Oncomelania hupensis quadrasi might be teensy but they carry a
big problem: each one may have as many as 500 schistosomiasis
parasites, very common and creating a very big public health
problem in China, the Philippines, Africa and South America.
The Institute ‘inherited’ the prized parasite lifecycle when WEHI
immune-parasitologist Graham Mitchell retired.
Keeping that parasitic lifecycle alive is important so that all life
stages can be studied and vulnerability determined for more
effective infection control. And a secret to the snails’ successful
captivity? Canadian Maple leaves, raked, boxed and transported
from a Melbourne park to the Institute’s secure research facility,
and steeped for 12 months in water.
54

Technological advances continued to make the seemingly impossible possible. The Institute had been quick to use flow cytometry7, for example, the technology used to analyse physical and chemical characteristics of particles in a fluid as they pass through a beam of light. ‘Cell counting, cell sorting, protein engineering and detection of biomarkers: flow cytometry is a powerful technology for particles of interest such as cells, chromosomes or bacteria,’ says Grace Chojnowski, recruited from Peter MacCallum Cancer Institute in 1993. ‘It made searching for a needle in a haystack possible.’
Lasers made looking for a needle in a haystack possible.55

Computer technology brought an end to handwritten scientific notes transcribed by typists. ‘We had to learn to type!’ recalls Peter Parsons with a shudder. Self-described ‘resident nerd’ Allan Saul helped colleagues become acquainted with keyboards and a computer mouse by encouraging Pac-Man competitions. ‘Pac-Man was the standard with its graphics made up from dashes, squares and dots and the computer had a whopping capacity of five megabytes,’ Saul remembers. While the Institute’s first minicomputer was bought for computer-modelling of malaria and arbovirus disease transmission, the genetic epidemiology lab became the most ardent adopter of the technology. ‘When I arrived in 1992, Nick Martin’s group had just bought an IBM RS/6000 server. It was state-of-the-art and very expensive – about $20 000 which was real money, the equivalent to a year’s salary. It was good gear for the time, but my four-year-old iPhone is 50 times more powerful than that 1992 server,’ laughs John Pearson, who joined in 1992 to look after that lab’s software development and data analysis. The lab also launched the Institute’s first website, a novelty in 1994. ‘The internet was only a couple of years old and no one imagined there ever being more than a few thousand organisations in the world involved: it was very much a government and academia thing. Commercial enterprises weren’t even allowed!’
Epidemiologists like Bob MacLennan were early adopters of the computer age, recognising the power they could unleash.
IMAGINE...56

Queensland Premier Wayne Goss officially opened the Institute’s third home, the Bancroft Centre, an 11-storey facility in Herston Road, in October 1991. Goss was generous in noting bipartisan support for the Institute’s expansion: planning had begun years earlier during Joh Bjelke-Petersen’s premiership with Mike Ahern as health minister. ‘Herston was the favoured site for a number of reasons and Mike Ahern agreed with leasing land from the RBH campus for 99 years as we walked around the site,’ recalls QIMR Council member Bryan Campbell.8
‘Herston was favoured firstly because we believed medical research would benefit from proximity with the adult, children’s and women’s hospital as well as the medical school. This encouraged more cooperative relationships. Visibility was also important. The location of the land available gave it street frontage, high visibility from passing traffic. People would see the QIMR signage and recognise it, instead of it being kept a secret.’
Premier Wayne Goss engrossed in science.
Well out of politics by the time the Bancroft Centre opened, former Queensland Health Minister, Technology Minister and Premier Mike Ahern had set the wheels in motion for the Institute’s expansion, physically and technologically.
Up until the 1990s, Australian families relied on encyclopaedias for authoritative information. The 28 volumes of Encyclopaedia Britannica edition 15, first published in 1974, were the most globally available with more than 4000 contributing authors from 100 countries. One full set would take 250 megabytes of data.
A laboratory’s information storage by 2002 was considered substantial at 5 gigabytes, about the same as a DVD full-length movie today.
57

While Powell had been proud to preside over the Bancroft Centre opening in 1991, he was eyeing off options for further expansion by 1996. In particular, he believed a site directly across the road, owned by the Brisbane City Council, had potential. ‘Soorley was not of the same opinion,’9 recalls Powell, who met with the then-Lord Mayor numerous times to discuss reuse of the land.10 The apparent impasse was frustrating.
In March 1998, Soorley organised a private dinner in the President’s Room of the city’s Irish Club. Supping together were Powell, The University of Queensland Vice-Chancellor John Hay, former Australian tennis doubles champion Ken Fletcher and an Irish-American entrepreneur, and friend of Fletcher’s, named Charles (Chuck) Feeney. ‘He (Feeney) spent the dinner asking questions and I really couldn’t see where he was going with them at the time,’ recalls Powell. Feeney heard that medical research was thwarted in Australia by a lack of funds. He also learned that Australian businesses and wealthy alumni had yet to develop a tradition of philanthropic giving. As they rose from dinner, Powell invited the American to visit the following day for a walk around the facility – and sandwiches.
‘I had no idea I was inviting the person who would fulfil a once-in-a-lifetime dream,’ Powell says somewhat sheepishly.
The 11-storey Bancroft Centre was the Institute’s first ‘tower’.
58

Feeney was indeed a generous guy. A self-made billionaire, he was uncomfortable with the trappings mega-money bought. He once told New York Times reporter Judith Miller that while some people found money attractive ‘you can’t wear two pair of shoes at one time’.11 Feeney’s solution was to give his money away. Between 1982 and 1997, he disbursed $610 million in 1500 grants anonymously across America via his private foundation The Atlantic Philanthropies.12 A further $148 million had been given to overseas charities. And he planned to give away the remainder of his fortune, which after selling the global Duty Free Shopper chain he had established decades earlier, amounted to some $3.5 billion. ‘I simply decided I had enough money. It doesn’t drive my life,’ he told Miller.13
Feeney provided initial funding for the $60 million Cancer Research Centre at QIMR, the first cancer research facility of its kind in the southern hemisphere, comparable in size to the large cancer research institutes in North America and Europe, and Feeney’s first philanthropic investment in Australia. As he had done elsewhere, Feeney’s pledge had a couple of provisos: the state and federal governments needed to match his gift. ‘He promised $20 million conditional on us raising the rest within six months,’ Powell says — and he didn’t want public recognition.
59

‘Even Council didn’t know who this ‘white knight’ was at first,’ confirms Campbell. Feeney’s Atlantic Philanthropies was soon to fund the Translational Research Institute, a joint venture between The University of Queensland’s Diamantina Institute, Queensland University of Technology’s Institute of Health and Biomedical Innovation, Mater Medical Research Institute, and the Princess Alexandra Hospital’s Centre for Health Research. The playing field was changing. How would the state’s established — indeed, signature — medical research facility play it? Ellem, Powell’s deputy director, was to muse: ‘Sometimes unexpected gifts are bestowed upon us which make new directions possible.’
When a questionnaire was going out, we would gather around a big table that sat 30, and for a week we would physically fold printed questionnaires into envelopes, stick thousands of labels onto those envelopes, and then stick postage stamps on every single one because we knew people paid more attention to an envelope that carried a stamp rather than a franking mark, because it felt more personal. In due course, the papers could be returned. The compactus was crammed with millions of pieces of paper from thousands of questionnaires, which was an appropriate way to store the information at the time but did nothing for analysis. Students were hired to type the answers into databases that I’d create and scientists would analyse the data.
Nowadays the forms are filled in online and the answers immediately feed into a database for analysis.
— John Pearson —
REMINISCENCE
60

ENDNOTES 1 Halliday continued to work at QIMR as an NHMRC senior principal
research fellow until mandatory retirement in 1995.
2 Interview with author, 24 February 2015
3 As retold to author, first published ‘A Career Forged in Iron’, American Association for the Study of Liver Diseases, 2014
4 A St Louis research group successfully cloned the gene first. Refer Feder et al Nature Genetics, 1996
5 Kay Ellem’s reflection, 1947 Alumni Yearbook, Scots College, Sydney 1997
6 Interview with L Powell, 24 February 2015, supplemented by ‘Bridging the gap between science and clinical medicine: mentors and memories’, Medical Journal of Australia, 16 December 2012 p657
7 Queensland Cancer Fund provided a fluorescent activated cell sorter — an early form of flow cytometry — in 1980.
8 Interview with author, 27 February 2015
9 Jim Soorley was Lord Mayor of Brisbane from 1991–2003.
10 Interview with author, 24 February 2015
11 Conor O’Clery, The Billionaire who wasn’t: How Chuck Feeney secretly made and gave away a fortune, Public Affairs, New York, 2013, 236
12 Ibid, p235
13 Ibid, p235
61

The broad toothy smile spoke volumes as the sandy-haired man moved to unveil the commemorative wall plaque marking the official opening of QIMR’s Comprehensive Cancer Research Centre. August 2001 saw Queensland’s Premier Peter Beattie flushed with the success of another example of his government’s ‘Smart State’ strategy, a clever sloganeering exercise used to emphasise Queensland’s investment attributes beyond tourism, mining and agriculture. Here was the state’s signature research institute – no longer the only, but certainly the pre-eminent – with a staff of 440, a budget that had trebled in nine years, two independent scientific reviews lauding its work, poised to contribute substantially to the new biotechnology and knowledge-based research ‘Smart State’ fostered.
ENTERING THE 21ST CENTURY07
62

Powell retired in 2000, and in a move reminiscent of the past, a ‘bright young mind’ was promoted to the directorship. Michael Good joined the Institute in October 1988 as one of Kidson’s recruits. Kidson had supervised the medically trained Good’s Bachelor of Medical Science at The University of Queensland in 1975 — ‘I had been working as a registrar in a cancer ward with lots of adolescents and a lot of them dying, and it had quite an effect on me. It is a great privilege to be a doctor and save some lives, but if you can develop a cure, you can save millions,’ Good recalls of the moment his career changed course. Kidson had encouraged Good to go to Melbourne to undertake his PhD in immunology. At WEHI, Good was supervised by Sir Gustav Nossal1 who passed on sage advice still respected 40 years on: ‘He told me: “You don’t dabble in science, you focus on an area and stick to it. People who make breakthroughs don’t do it overnight; they do it over a lifetime”.’ When QIMR was appointed lead institute for the federal CRC on Vaccine Development, Good, who was working on malaria and rheumatic fever, became its director.
Powell had pushed for translational science, taking basic research findings on to clinical applications. He’d inspired Good who now, as the Institute director, was to take that philosophy further: ‘If your research reveals something that could be useful as a vaccine or a treatment, I believe it is your responsibility to develop it as a product; no-one else will have your passion’.
PROFESSOR MICHAEL GOODDirector 2000–2010
Born 1954, Queensland
Graduate, The University of Queensland Medical School, 1978
Joined Institute, 1988
Research interests: Immunity and immunopathogenesis to malaria and group A streptococcus/rheumatic fever, with particular relevance to the development of vaccines
Order of Australia for services to medical research, 2008
Eureka Prize for Leadership, 2009
Now Principal Research Leader and NHMRC Australia Fellow, Institute for Glycomics, Griffith University
63

The Institute had taken a few guarded steps towards commercialisation. In May 1997, then-CSIRO scientist Jim Alyward came to QIMR organic chemist Peter Parsons’ melanoma genomics laboratory with an anonymous test tube containing sap diluted in sterile water. For decades, Alyward’s family had sworn by the milky sap from Euphorbia peplus for treating sunspots. If Parsons’ team could confirm some molecular changes, Alyward could use his biochemistry expertise to isolate the active ingredients and develop a new topical treatment. Of course, plants and herbs have been used for thousands of years to cure or prevent disease: ginger, garlic, ginseng, aloe, foxglove, poppy and Echinacea to name a few. But with modern science’s development of powerful synthetic medicines, nature’s antidotes were eschewed — considered varyingly unsophisticated, unreliable, unworthy or uneconomic. Somewhat sceptical, Parsons coined the contents Alyward yielded MPA (Magic Potion Alyward) and gave Alyward a terse ‘don’t ring us, we’ll ring you’. And call back Parsons did on confirming a graduate student’s observations of profound change in appearance of melanoma cells, similar to that produced in the compounds his lab had already tested. ‘The difference was the potency and extent of cell reversion, almost back to the shape and appearance of a healthy melanocyte,’ Parsons recalls.
For months, Alyward carried out his investigations after hours, sometimes visiting QIMR at night to test his compound against melanoma cells left over from the day’s experiments in Parsons’ laboratory. When his company Peplin was formed, QIMR researchers became integral to his race to patent, providing substance from mouse experiments to clinical trials. Peplin listed on the Australian Stock Exchange in 2000 with more than 1600 shareholders willing to invest in the dream of a new non-surgical skin cancer treatment.2 The Institute held no pecuniary interest. In 2009, Leo Pharma Australia acquired Peplin Operations Pty Ltd. Picato® gel is sold as a topical treatment for sun spots, manufactured on the Gold Coast, with Australia’s Therapeutic Goods Administration (TGA) and the US Food and Drug Administration (FDA) approval.
Euphorbia peplus.
64

QIMR’s long-running Epstein-Barr virus (EBV) research offers another example of devoted belief, taking lab bench findings to the patient’s bedside. Rajiv Khanna, who started working with EBV in 1990 as Denis Moss’s first post–doctoral researcher, tells: ‘The Lancet published an article in 1998 from St Jude’s Hospital, reporting a breakthrough using our information. It showed the T cell was the perfect tool for use in transplant patients, particularly bone marrow recipients. Here in Brisbane, a doctor from the Prince Charles Hospital contacted us about a patient who had had a lung transplant and now presented with liver cancer. The patient was EBV positive. He had, at best, a couple of months to live. Could we devise an immunotherapy that attacked only the cancer and not the new lung? That was a very good question!’ Six weeks later, Moss and Khanna stood by the bedside and watched as cultivated T cells, known to be the Achilles heel of otherwise ‘immortal’ EBV cells, were slowly infused through the patient’s drip. ‘His immune system was poorly suppressed; he had fungal infection, swelling in his legs, as well as lymphoma of the liver.’ After two infusions, a CT scan showed the liver nodules were diminishing. After four infusions, the cancer had vanished and so had the fungal infection. Two years later, Khanna received a phone call: ‘Our man was back in hospital with another cancer, in the lung’. The team was able to develop a therapy using leftover cells from the earlier treatment, kept in liquid nitrogen. He received his treatment on a Friday and after observation went home. Another phone call the following Monday devastated Khanna. Their man had collapsed at home. He was dead. A post-mortem showed that his death was due to
65

internal bleeding. ‘It was not something we could have known or foreseen but what we were also surprised — excited — to learn was that the post-mortem also showed that the cancer had been annihilated in just 48 hours.’
The Cooperative Cancer Research Centre, opened in 2001, positioned the Institute perfectly to support further development of research, to move it closer to marketability. The QIMR Council was fully behind what were seen as essential advances to further strengthen the Institute as a world-leader in medical research. Further legislative amendments in 1997 had initiated a subtle changing in the Council’s membership structure. Instead of being loaded with hospital and health department representatives, Council members offered a wider mix of expertise from corporate governance and health ethics, to financial management, law, fundraising, science, and a specific representative from the National Health and Medical Research Council. The Chair, when Good became director, was Mount Isa Mines former chief executive, Sir Bruce Watson, an astute businessman and engineer.3
Q-Pharm Pty Ltd commenced trading as a private company on 1 July 2002. Established as a ‘spin-out’ enterprise from The University of Queensland, the company effectively was a joint venture of the University and the Institute, with the business founders Wayne Hooper and Ron Dickinson its other shareholders. Located within the world-class facilities of the Institute’s new cancer research centre, it conducted a busy program of contract clinical research for the global biotechnology and pharmaceutical industries. For the Institute, Q-Pharm offered opportunity, for the first time, to test its vaccine and drug research in-house. The first true FTIH (first-time-in humans) trial was in 2003.
The establishment of Q-Pharm in 2002 has provided the Institute with a unique point of difference, enabling human clinical trials in-house.
66

In September 2004, the Institute created Q-Gen Pty Ltd as a commercial arm for contract manufacture of therapeutics: gene therapies, dendritic cell therapies and immunotherapies. There was, however, one line of investigation Good would not countenance. Stem cell research worldwide was being trumpeted as the key to curing cancers, heart disease, Alzheimer’s, repairing damaged organs and spinal cord injuries. While adult stem cells had been used for decades, the move to use embryonic stem cells was divisive in the community – and within QIMR. The Institute’s governing Council felt it was a ‘natural fit’ given the genetic research work carried out over decades. Good put his foot down on ethical grounds: ‘Over my dead body,’ were his words. Some saw his stand as blinkered: embryonic stem cells were easier to grow in laboratories; they were ‘pluripotent’, that is, able to separate into all tissues of an organism yet incapable of developing alone. Others respected him for standing true to his values. ‘I was very upfront. I had a few run-ins over that and stood firm,’ says Good.
The Cooperative Cancer Research Centre had also gone over budget, exceeding the combined pledges of ‘white knight’ Chuck Feeney and the state and federal governments. Feeney suggested that Good try cultivating philanthropy among Australia’s richest. In 2002, former Toowoomba mayor, state parliamentarian and property developer Clive Berghofer became the nation’s most generous supporter of cancer research, committing $1 million a year for five years to QIMR. The cancer research building was renamed the Clive Berghofer Cancer Research Centre in his honour.
Research needs money — that’s a given. In the early days of the Institute, the state government provided full funding. As the Institute grew in reputation, bequests were received intermittently, along with occasional grants from outside sources such as the National Institutes of Health (US), Cancer Council, National Breast Cancer Foundation and Australian Research Council. The mainstay of grant funding was, and remains, the NHMRC, weighing up the highly competitive individual project applications against track record, publications, excellence and health priorities. In the 1990s, then-director Powell had rather excitedly accepted ‘NHMRC block funding’ for QIMR, a lump sum guarantee for five years. ‘It gave the Institute credibility,’ says Good, who inherited the arrangement. ‘Up until then, no research institute north of Sydney had received block funding. It meant we were up there with the best of researchers and that was priceless for our reputation.’ But while it allowed research institutes a known sum that they could distribute within their own projects as needed, funding did not increase with inflation and research costs were escalating. ‘If we’d remained in that arrangement we would have lost out,’ says Good who negotiated a withdrawal. He went on to negotiate on behalf of independent medical research institutes for separate funding to cover infrastructure overheads. Again he faced detractors, primarily university chiefs who felt their labs were being stripped. Good was unmoved: ‘We could turn on a light and know the electricity bill wasn’t going to inhibit our scientific discovery. Universities had enjoyed that luxury for years.’
As director, Good used every opportunity to improve funding, including speaking with then-Health Minister Tony Abbott.
67

Increasing focus on cancer breakthroughs did not detract from the Kidson-inspired pledge to defend public health issues offshore either. As lead agency for the Australian Centre for International and Tropical Health and Nutrition, established in 1995 to promote better public health education, training and research, QIMR had a hand in dealing with diverse problem areas: malaria and scabies, schistosomiasis and the mosquito-borne viral illnesses dengue and Ross River fever to name a few. Parasitologist Don McManus had joined the Institute in the late 1980s. By the early 2000s, he had strong working relationships in China and the Philippines, investigating schistosomiasis infection which, left untreated, can damage the liver, spleen, lungs and bladder. Water buffalo were found to help spread the parasite. That insight led to years working on a veterinary vaccine to impact the parasite or its eggs.
68

In more recent years, it has led to a novel public education program, successfully trialled in rural China, and expected to expand to the Philippines in late 2015. QIMR Berghofer researchers turned information about intestinal worm infections, a major issue in disadvantaged tropical and sub-tropical communities globally, affecting about two billion people, into a fun and educational children’s cartoon shown in schools. The 10-minute cartoon The Magic Glasses4 features a small child looking through ‘magic glasses’ to see worm eggs and larvae in bright colours. The animation explains the importance of hand washing, wearing shoes, covering food and using toilets to be healthy. ‘Sometime just a simple change in behaviour and attitudes makes a drastic difference in the spread of disease,’ says McManus, the team leader. ‘If we want to eliminate these parasitic illnesses, we need more than vaccines and drugs. We need public health education.’
69

The Magic Glasses’ impact in China was powerful. Children’s knowledge of infection was assessed before and after viewing the DVD and the cartoon’s effectiveness measured against traditional posters. Teachers, parents, health staff and officials were interviewed as part of the program development too. The children were also tested for parasitic worm infection and treated when needed. ‘Tailoring the message to the children made an enormous difference to disease rates, and reinfection among those who saw the cartoon four times during the school year was spectacularly halved.’
It was also through the Australian Centre for International and Tropical Health and Nutrition that QIMR mosquito control experts were deployed to South East Asia on public health missions. On one such mission, in the central Vietnam province of Khanh Hoa, the QIMR team found that 92 per cent of dengue fever mosquito production occurred in huge 2000-litre containers that international humanitarian fund UNICEF had provided to give locals safe drinking water. They also found that tiny creatures called Mesocyclops, endemic in Vietnam, had a taste for Aedes aegypti eggs. Community-based dengue control projects, collaborating with the Vietnam Ministry of Health and National Institute of Hygiene and Epidemiology, proved this novel biological approach was both effective and inexpensive: by 2005, Aedes aegypti mosquitoes had been eradicated from 40 communes in northern and central Vietnam, protecting some 380 000 people from dengue and dengue haemorrhagic fever.5 AUSAID committed to five years’ funding for further control programs in southern Vietnam. The Vietnamese government transferred responsibility for the southern Mesocyclops program to local residents and community collaborators in 2010.6
70

The Institute’s expertise in mosquito control has been widely sought after and shared in Asian countries, empowering communities in Vietnam and, pictured here, in Cambodia, to keep themselves safe.
71

When New Zealand authorities detected an illegal invader on the country’s North Island on Boxing Day 1998, the Institute’s mosquito control laboratory’s leader, Brian Kay, was called on to become part of a scientific strike force to halt the march of Aedes camptorhynchus, Australia’s Southern Saltmarsh mosquito. The vicious day-time biter, known colloquially as ‘Campto’, thrives in Australia’s cool coastal southern woodlands. New Zealand’s North Island presented an idyllic home-away-from-home. ‘There was very good reason to be concerned about this illegal immigrant’s arrival,’ Kay affirms. ‘It promised to introduce arboviruses to a population – human and native animals – without protective antibodies; symptoms may not be readily recognised or diagnosed, promoting further spread of infection. Campto was a biosecurity hazard that needed containment.’ Of particular concern was the introduction of Ross River fever.
Only one year earlier, New Zealand had sourced Kay’s expertise to review that country’s program for surveillance and action against mosquito populations posing public health threats. He was well-known for developing the Abate 50SG insecticide granule, the mainstay of Australian mosquito control for more than 25 years, and co-pioneering use and evaluation of environmentally-friendly control products: an Institute ‘lifer’, his entire scientific career was dedicated to arbovirus and mosquito research in Australia and South East Asia.
The war on Campto required perseverance. It took 12 years and NZ$70 million to eradicate. It required legislative changes, public education, continual field surveillance, relentless air and ground-based chemical attacks and genetic investigations to determine whether multiple infiltrations had been mounted. New Zealand declared victory on 1 July 2010.7
Mosquito control expert Brian Kay was New Zealand’s go-to guy when the neighbouring nation found it had been invaded by an illegal Australian immigrant, the vicious day-time biting mosquito Aedes camptorhynchus.
72

By then Good had moved on, establishing his malaria and rheumatic fever research laboratory at Griffith University, after 10 years as director, and almost his entire scientific life at Queensland’s signature research institute.
With Good’s departure in June 2010, cancer researcher Adele Green stepped up as acting director while the QIMR Council commenced an international search for the person to lead Queensland’s long-established medical research institute. They wanted someone with a stellar scientific background and equally strong organisational skills: a networker, a collaborator, a visionary. Frank Gannon, Director-General of the Science Foundation Ireland (SFI), was their man.
A graduate of the National University of Ireland, Galway and the University of Leicester, England, the molecular biologist is an internationalist. His career over more than 30 years had shuttled him between his homeland Ireland and the United States, France and Germany, pursuing his scientific passion: the regulation of gene expression by the oestrogen receptor, particularly relating to breast and ovarian cancers. In 1987, Gannon was appointed founding director of The National Diagnostics Centre at the University of Galway, established by the Irish government to accelerate the transfer of biotechnology to industry. When he left in 1994 to move to the European Molecular Biology Organisation (EMBO), the centre’s earnings had reached £1 million, growing at a rate of 25 per cent per annum. On returning to Ireland to become the SFI Director-General, Gannon headed the government-backed hub funding basic and applied research
PROFESSOR FRANK GANNONDirector and CEO 2011–present
Born 1947, Sligo, Ireland
Graduate, B.Sc. (Hons), University College, Galway, Ireland, 1970
PhD, University of Leicester, England, 1973
Molecular biologist
Research interests: the regulation of gene expression by the oestrogen receptor, important in breast and endometrial cancer, providing novel approaches to treatments for these and other cancers
Executive Director, European Molecular Biology Organisation (EMBO), 1994–2007
Director-General, Science Foundation Ireland, 2007–2010
73

in science, technology, engineering and mathematics (STEM), encouraging development and competitiveness of industry and enterprise, supporting study and career pathways and helping the community understand the value of STEM, particularly to the growth of Ireland’s economy. Gannon was singled out by Ireland’s Minister for Science, Technology and Innovation, Conor Lenihan, for the strength in collaborations that had seen Ireland become recognised as a leading research force in immunology and nanotechnology. ‘SFI is playing a key role in getting people thinking and working smarter, generating new ideas and getting more for less right across the economy,’ said Minister Lenihan.8 ‘The fact that there is now more engagement between SFI-funded researchers and the enterprise sector is a source of particular optimism for future commercial output.’
That was just what the QIMR Council wanted for the Institute’s future. ‘Professor Gannon was the ideal candidate for the role. He has significant experience in managing science, widespread ties with the international scientific community and a passion for scientific excellence,’ Council Chair, Professor John Hay AC, said at the time.9
The medical research institute where Gannon arrived in Brisbane in January 2011 was no longer the one and only. ‘Smart State’ policies had seen the Queensland Government invest about $1.05 billion in science infrastructure in the previous 10 years, leveraging a further $1.7 billion from the Commonwealth and industry partners, to build an
internationally significant scientific community of about 18 000 scientists clustered in southern Queensland. No-one could take away the Institute’s distinction of being the state’s original defender of public health, but how could it hold its standing in this competitive environment going forward? What could it do best?
‘Growth brings with it new opportunities but also the need to adhere to the qualities of research for which QIMR is renowned. The decision to leave Ireland was difficult, but the challenge of contributing to increasing the scientific reputation of Brisbane worldwide was something that I looked forward to eagerly,’ Gannon reflects. ‘I saw strength in our diversity,’ he says, as he recalls the first months acquainting himself intimately with the Institute’s programs and people. Perhaps also, he channelled the founding director Mackerras who, in 1947, wrote of a need to ‘guard against diffusing our energies too widely’.10
Known as a collaborator and networker, Gannon set about breaking down administrative barriers or ‘silos’, encouraging multidisciplinary sharing of thoughts and knowledge across projects in-house. He was also quick to start forging and strengthening relationships with universities and health services. ‘One does not work best on one’s own,’ Gannon says. Hence, the Australian Infectious Diseases Research Centre, a collaborative research initiative with The University of Queensland since 2012; the tripartite Queensland Mental Health Research Alliance; the cancer and infectious diseases-focused Queensland Emory Development (QED) Alliance with The University of Queensland and Emory University, USA; and the Queensland Head and Neck Cancer Centre.
QIMR Berghofer Director and CEO, Professor Frank Gannon, and QUT Vice-Chancellor, Professor Peter Coaldrake, sign an MOU at a ceremony at BIO Philadelphia with witnesses including Queensland Premier, The Hon Annastacia Palaszczuk.
74

Gannon’s arrival also coincided with further redevelopment of the Institute’s campus, a 15-storey third tower on the site of the former Queensland Radium Institute linking the Bancroft Centre and Clive Berghofer Cancer Research Centre. Chuck Feeney had again contributed, pledging $27.5 million towards the new facility, part of an astonishing $102 million gifting to Queensland medical research projects11, met by state and federal funding. And Clive Berghofer showed extraordinary local commitment again — $50 million. In 2013, the Institute changed its name, becoming the QIMR Berghofer Medical Research Institute.
75

Since arriving in Australia, Gannon has noticed unease within scientific ranks brought about by several federal reviews in health and medical research, questioning research’s role, value, funding and future. The McKeon Report, published in early 2013, advocated for greater collaboration and commercialisation as well as an acceleration of clinical trials. That report also recognised the need to attract, retain and build the knowledge industry. Tellingly, perhaps, it specifically identified a need to build health professionals’ research capacity and to drive research within the health system itself.12 Another review was commissioned in late 2014 to specifically consider the viability, contribution and accountability of the nation’s almost 70 independent medical research institutes – those not directly attached to universities or hospitals. QIMR Berghofer is among them. At the time of writing, no findings had been tabled. Yet Gannon says this vacuum of not knowing is unhelpful. With his past experience in the successes of the Science Foundation Ireland, he’s seen how people and scientific discoveries can mature when properly supported. ‘We’re full-time professional researchers and I’ve had to think through how to create an environment where people are not scared of the future.’ He sees a recently approved plan as a pre-emptive strike to ward off fears providing a level of financial surety. The Institute will underwrite team heads, group leaders and senior scientists’ salaries for up to five years if grant funding is not forthcoming. ‘It’s like a “get out of jail free” card,’ Gannon says wryly. ‘The scientific excellence must be evident, grant applications will still need to be submitted, but this serves as a buffer to let the scientific investigation continue. I
see it as future-proofing the Institute, a drawcard to retain and attract great minds. If we kowtow to the top-down approach of what science is relevant, I suggest in the Australian context, the cochlear implant would never have been developed. What a difference that has made to so many lives. That’s what we continue to strive for – making that difference.’
In 2014, QIMR Berghofer Medical Research Institute took full ownership of the clinical trial facility, Q-Pharm, a move reinforcing the Institute’s status nationally and internationally, as a leading translational facility. In its 13 years of trading, Q-Pharm conducted 350 early-phase clinical trials, supporting translational research arising from QIMR Berghofer. Co-located, Q-Pharm and Q-Gen provide the Institute with a unique ability in Australia to take medical research from discovery through manufacturing of specialist materials, and onto human testing, and all under one roof.
In June 2015, Q-Gen, having met industry Good Manufacturing Practice Standards, became the first Australian manufacturing facility to receive Therapeutic Goods Administration (TGA) approval to manufacture cellular therapies for human use, specifically clinical grade T cell therapies, opening the way for clinical trials of new cancer treatments. Queensland’s Premier, Annastacia Palaszczuk, summed it up like this: ‘This can have a ripple effect when it comes to attracting more scientists and more investment.’13
76

77

‘Most people think you only get your name in lights when you’ve passed on. I’m very glad to be here to see it,’ says Clive Berghofer, the nation’s most generous supporter of cancer research, after whom the Institute has been renamed.
GETTING BY WITH A BIT OF HELP FROM OUR FRIENDS
‘My health is more important than my wealth. Without it, I have nothing.’
That’s how Darling Downs property developer and medical research supporter Clive Berghofer sums up his reason for giving.
In 2002, Berghofer, one of Australia’s wealthiest individuals, became the nation’s most generous supporter of cancer research and he’s chuffed, even somewhat amused, by the reaction of people seeing his name on not one but two buildings in inner-city Herston. ‘Most think you only get your name in lights when you’ve passed on. I’ve had to assure people that I am Clive, I am really alive and I’m very glad to be here to see it!’
78

79

Berghofer’s generosity isn’t new. He reckons he gives, on average, $20 000 a week to charities, mostly community-based, supporting the city he helped shape, Toowoomba. And he’s been involved in leukaemia research fundraising since the 1980s, moved by the plight of a Toowoomba resident whose husband could not travel to Sydney for bone marrow transplant treatments.
‘I lead by example,’ says Berghofer. ‘If I’m going to ask someone to do something, I’ll do it first. Helping people gives me great pleasure. I’m regularly stopped by strangers and thanked for saving their life or a relative’s. I only wish other affluent business people would do the same and give generously. It’s time we started doing more to help each other.’
Of course, community support of medical research is not limited to the very wealthy or the corporate world. Ordinary Australians contribute significantly to QIMR Berghofer’s funding capacity. Take, for example, Sunny Drescher. Since her first cent auction and raffle in 2004, Drescher has handed over more than $121 600 to the QIMR Berghofer Medical Research Institute. She holds three Happy Face Cent Auctions a year at the Aspley Leagues Club in Brisbane, amassing at least 100 prizes every time, some bought by Drescher, many donated after some persuasive talking from the octogenarian.
In between events, her rumpus room resembles a gift emporium: toys, toiletries, manchester, glassware, sporting goods, jewellery and homewares piled neatly, some titivated with cellophane and ribbon, others awaiting wrapping. ‘I love helping other people and I hope some answers can be found, particularly for little ones who are sick,’ Drescher offers quite simply.
Sunny Drescher’s cent auctions have raised nearly $122 000.
80

ENDNOTES 1 Renowned research biologist and former director of the Walter and Eliza
Hall Institute in Melbourne.
2 Peplin was bought out by Danish pharmaceutical Leo Pharmacy in 2009 following successful phase III clinical trials.
3 QIMR Annual Report, 2001–2002, Also Ten Years of Q-Pharm Pty Ltd fact sheet
4 QIMR Berghofer was grateful for the funding support by UBS Optimus Foundation, Zurich, Switzerland and collaborations with scientists from The University of Queensland and Hunan Institute of Parasitic Diseases in China in developing The Magic Glasses program.
5 QIMR Annual Report, 2005
6 Read more at http://www.sciencedirect.com/science/article/pii/S0001706X14003180
7 Read more about this world-first eradication achievement. Mosquito eradication: The story of killing Camtpo, edited by BH Kay and RC Russell, CSRIO Publishing, Melbourne, 2013
8 http://www.sfi.ie/news-resources/press-releases/science-body-backs-600-research-industry-links-for-smart-jobs-minister-okeeffe.html 25 June 2015
9 http://www.qimrberghofer.edu.au/page/News__Events/Media_Centre/Media_Releases/Archive/2010/QIMR_appoints_new_Director_and_CEO/ 25 June 2015
10 QIMR Annual Report, 1947, in spelling out ‘the ways and means of research’, p11
11 Chuck Feeney’s The Atlantic Philanthropies also contributed $50 million towards the $354 million Translational Research Institute Queensland at the Princess Alexandra Hospital and $25 million towards QUT’s Hub for Sustainable and Secure Infrastructure. Media release, Queensland Government, 27 July 2009
12 Access the Strategic Review of Health and Medical Research summary report, February 2013, at http://www.mckeonreview.org.au/downloads/Strategic_Review_of_Health_and_Medical_Research_Feb_2013-Summary_Report.pdf
13 Media release http://www.qimrberghofer.edu.au/page/News__Events/Media_Centre/Media_Releases/QIMR_Berghofer_gains_licence_to_produce_cancer_therapies/ 25 June 2015
14 Interview with author, 8 May 2015. Read more about Clive Berghofer: Clive, as told to Don Talbot, Clive Berghofer Publishing, 2002
81

When QIMR Berghofer director Frank Gannon looks to the future, his views are coloured by remarkable medical discoveries in his own lifetime.
‘Consider that a few decades ago a person died from a heart attack. Now more often than not, they recover but live with a chronic illness that needs to be managed. That is how I see cancer. Numerically cancer still affects extremely high numbers of people. More people get cancer because people are living longer, and because diagnostic testing is better. Those that do develop cancer live longer generally too. The future is that people will live with cancer, rather than die from it.’1
LOOKING FORWARD08
82

Whereas cancer treatment has revolved around often extensive surgeries, high-energy radiation and a cocktail of drugs to destroy cancer cells, the future promises targeted, cellular immunotherapies. Gannon points to the outcomes of a world-first brain cancer trial the Institute conducted in early 2015. Research scientists led by Rajiv Khanna developed a technique to modify patients’ T cells in the laboratory, effectively training them to attack a virus known to be linked to the aggressive brain cancer, Glioblastoma Multiforme (GBM), a virus called cytomegalovirus. When the killer T cells destroyed the virus, they destroyed the cancer too. About 800 Australians are diagnosed with GBM annually. Fewer than 10 per cent survive beyond five years despite surgery, radiotherapy and chemotherapy. Most of QIMR Berghofer study participants lived much longer than their six-month prognosis. In some, the cancer stopped growing.
There’s an urgent need for new clinical treatments, says Gannon, and while this particular therapy requires more testing, it does highlight how immunotherapy — manipulating a person’s own immune system — offers a rich new frontier for cancer treatment.
83

The GBM treatment grew out of the Institute’s long-running investigations into viruses causing cancers, dating back to John Pope’s 1960s’ discovery of mouse leukaemia.
Just as many people carry Epstein Barr virus (EBV) — or ‘the kissing disease’ — half of all Australians have cytomegalovirus, yet show no symptoms.
In another link with EBV, QIMR Berghofer researchers collaborate with University of Hong Kong Li Ka Shing Faculty of Medicine to perfect an immunotherapy for nasopharyngeal carcinoma (NPC), an aggressive throat cancer, linked to EBV and commonly found in Asia.
84

85

In saying that the future for cancer treatment lies in targeted immunotherapies, ‘target’ becomes the key word. What is unusual about this cancer cell? Is it the DNA, a genetic flaw or vulnerability? Is there something different about the way cells grow? Is lifestyle a factor or environment? This is where QIMR Berghofer’s multidisciplinary approach comes to the fore, its epidemiology and population studies and geneticists helping to unlock the age-old question: ‘why?’ ‘It is important to play to our strengths: and our strength, at QIMR Berghofer, can be in our diversity with people from different disciplines looking at an issue in different ways,’ says Gannon.2
Personalised therapy extends also to mental health. Gannon describes it as ‘the next epidemic, a tsunami we can see coming from a distance’, applauding predecessor Michael Good for recognising the Institute’s responsibility to better understand mental health. During his final term as director, Good persuaded the Institute’s Council to invest in a new laboratory and woo psychiatrist and computational neuroscientist Michael Breakspear to Brisbane. Breakspear
is not a fan of psychiatry’s key diagnostic tool DSM-V3: it is too subjective, open to interpretation. He likes cold hard data. Breakspear’s laboratory is part of the international Human Connectome Project, creating an atlas of communication routes throughout the brain drawn from MRI scans of 1200 people, including 300 pairs of twins. ‘Rather than offering a blanket diagnosis for autism or schizophrenia or depression or dementia for example, a neurologist will one day be able to observe abnormal brain circuitry to see exactly what has gone wrong and propose a personalised regimen of therapy or medication,’ Breakspear explains. He maintains this could enhance appropriate early intervention. ‘Brain function problems sit on a continuum. We have suicide, the number one killer of young Australian men who don’t get to realise their life’s potential, which is a terrible loss to the nation, and we have an ageing population and a growing number of people developing dementia, another great loss that I don’t believe is just a part of growing older.’
86

Psychiatrist and computational neuroscientist Michael Breakspear leads QIMR Berghofer into a brave new world of mental health research, as part of an international effort creating an atlas of communication routes in the brain to better understand mental illness and brain functions.
87

Brothers Dylan and Lawson Reid plan their epic motorbike ride across all continents, raising funds for the Institute’s mental health research. Their adventure began in 2015.
WITH A BIT OF HELP FROM MORE FRIENDSBrisbane brothers Dylan and Lawson Reid admit to being adventurous by nature but their two-year epic journey across all continents riding motorbikes has a purpose bigger than thrill-seeking memories. They’re riding to raise awareness of mental health issues, and to raise money to enable QIMR Berghofer to develop an objective diagnostic tool for major depressive disorders.
Their sister, Heidi, an epidemiologist working on malaria, died in 2011, aged just 27. Diagnosed with major depressive disorder 10 years earlier, she had pursued life with zest, trying to shake off the overwhelmingly burdensome companion, depression.
‘We can’t help but wonder how things could have been different had she been diagnosed earlier,’ says eldest, Dylan, 33. ‘Our family has a history of depression and suicide, particularly down our Dad’s side. Mum and Dad did the best they could with the information available to manage Heidi’s depressive disorder and get her the best help possible. However, it doesn’t matter how much money you spend: if you don’t get the diagnosis right, you’re not going to get the treatment right.’
The Reid brothers have a $200 000 fundraising goal and a promise to come home in one piece.
88

89

90

New molecular techniques also give researchers hope of understanding more about mental illnesses including, for example, anorexia nervosa. One of four recognised eating disorders, anorexia nervosa is often mistakenly seen as an affliction of teenage girls in pursuit of the body beautiful. In reality, it affects more than 53 000 Australian men and women and has the highest mortality rate of any psychiatric illness: more than one in five people with anorexia nervosa, who died prematurely, committed suicide. QIMR Berghofer leads the Anorexia Nervosa Genetics Initiative, the world’s largest and most rigorous genetic investigation into the condition, involving more than 13 000 volunteers across Australia, Denmark, Sweden and the United States. Study leader, Nick Martin, says greater understanding of the genetic makeup will help develop more effective therapies and medications for this life-threatening, body-wasting condition.
Genetic investigation will play an increasing role in understanding cancers and common conditions like asthma, affecting about one in six children and one in nine adults in Australia. While common, it can also be very serious, accounting for about 36 000 hospital admissions and more than 400 deaths annually. The Institute’s interest in asthma research began in the 1950s, with Ted Derrick studying climate, pollens and dust.4 Other factors, like overwhelming emotion and stress, are now known to be triggers, but what of genetics? QIMR Berghofer leads Australian Asthma Genetics Consortium, working with researchers from The University of Melbourne, Monash University, The University of Western Australia, Woolcock Institute and the Melbourne Children’s Hospital to identify genes increasing individuals’ risk.
Gannon maintains an imperative to continue work on conditions that, while rare or unheard of in Australia, are common, debilitating, and life-shortening. It is the ‘noble’ thing to do for impoverished populations. Like Kidson before him, Gannon sees Queensland as part of a global village, actively encouraging partnerships abroad.
91
Back in the Institute’s formative days, there were those who questioned the wisdom of legislative wording allowing ‘research into any branch or branches of medical science’. QIMR foundation director Ian Mackerras responded in this way: ‘The great majority of big discoveries, and innumerable smaller ones which have benefitted mankind have come from pure research. Research for its own sake fosters, as nothing else can, the urge to always explore, without which initiative is lost and no research institute can live … We should be actuated in all that we do primarily by the spirit of inquiry and but secondarily, if at all, by thoughts of immediate application or the ephemeral credit that may be gained therefrom’.5 Researchers today are similarly questioned: Gannon understands that. His example of the cochlear ear implant developed by Graeme Clarke in Melbourne is a case in point. So too are the Institute’s own decades of work to fight malaria. There are treatments, yet no magic bullet — yet. UNICEF says one child dies every 30 seconds from malaria. More than 250 million people across the world are affected by this debilitating illness. QIMR Berghofer’s research over decades has been multi-pronged: understanding the patterns
of transmission, investigating the genetic make-up of the malaria parasite, studying the nature of immunity to malaria in animal models and human volunteers, investigating the effectiveness of malaria drugs in clinical trials and potential vaccines. Gannon’s response underscores what Mackerras maintained nearly 70 years ago. Research, by QIMR Berghofer and CSIRO, published in 2015, revealed that people infected with malaria have higher levels of a smelly sulphur-based chemical on their breath. This observation paves the way for an ingenious new diagnostic tool — faster, simpler and more accessible than blood tests — a breath test.
Scientific discovery can be, says Gannon, ‘like getting to the top of a hill, only to see there’s another climb’. It’s unrelenting, unforgiving — and utterly enthralling. And the QIMR Berghofer Medical Research Institute will be there; continuing the role it was trusted with in 1945 to be the Number 1 Public Health Defender.
Scientific discovery can be ‘like getting to the top of a hill, only to see there’s another climb’. It’s unrelenting, unforgiving – and utterly enthralling.
92

ENDNOTES 1 Interview with author, 6 March 2015
2 Interview with author, 4 June 2015
3 Diagnostic and Statistical Manual of Mental Disorders 5
4 Refer to such articles as EH Derrick, ‘Seasonal variation of asthma in Brisbane: its relation to temperature and humidity’ or ‘Annual variation of asthma in Brisbane: its relation to the weather’, published in International Journal of Biometeorology, in 1960s
5 IM Mackerras, ‘The ways and means of research’, QIMR Annual Report, 1947, p6
93

R Patrick, A History of Health and Medicine in Queensland 1824–1960, University of Queensland Press, Brisbane 1987
IM Mackerras, EN Marks, ‘Bancrofts: a century of scientific endeavour’, Proceedings of the Royal Society of Queensland, vol. 84 no.1, 1973
J Pearn, L Powell eds, The Bancroft Tradition, Amphion Press, Brisbane
RL Doherty ed, A Medical school for Queensland, Boolarong Publications, 1986
Typescript unpublished, Dr Mabel Josephine Mackerras, 1968 held in John Oxley Library collection, State Library of Queensland
EH Derrick Spirit of the researcher, Australasian Medical Publishing Company Limited, 1949
EH Derrick ‘Challenge of north Queensland fevers’, Australasian Annals of Medicine, vol. 6 no 3 August 1957
EH Derrick, ‘Seasonal variation of asthma in Brisbane: its relation to temperature and humidity’, International Journal of Biometeorology, vol.19, no.3, pp239–51, 1965
EH Derrick, ‘Annual variation of asthma in Brisbane: its relation to the weather’, International Journal of Biometeorology, vol.10 no 1, pp91–99, 1966
TJ Bancroft, D Mackerras, DR Hacker, Just as the twig is bent : a short biography of the life of Dr Mabel Josephine Mackerras B. Sc., M.B.M. Sc., D. Sc, self-published, 2003
Sir R Cilento, Medicine in Queensland: A monograph, Council of the Royal Historical Society of Queensland, 1963
Queensland Institute of Medical Research Act 1945
Review of the Queensland Institute of Medical Research Act 1945 discussion paper
C O’Clery, The Billionaire who wasn’t: How Chuck Feeney secretly made and gave away a fortune, Public Affairs, New York, 2013
KH Rieckmann, AW Sweeney, ‘Army Malaria Institute: its evolution and achievements 1965–1975’, Journal of Military and Veterans Health, vol. 20 no.1
LW Powell, ‘Bridging the gap between science and clinical medicine: mentors and memories’, Medical Journal of Australia vol. 177 21, 16 December 2012
LW Powell, ‘A career forged in iron’, American Association for the Study of Liver Disease, 2014
J Pearn ed., Some Milestones of Australian Medicine, Amphion Press, Brisbane, 1994
BH Kay and RC Russell eds.,Mosquito eradication: The story of killing Camtpo, CSRIO Publishing, Melbourne, 2013
D H Crawford, A Rickinson and I Johannessen, Cancer virus: The story of Epstein Barr Virus, Oxford University Press, Oxford, 2014
FURTHER READING
94

Bringing together this commemorative corporate history of the QIMR Berghofer Medical Research Institute was rather like piecing together a ‘wasgij’, those mind-bending jigsaws that do not display the picture on the cover and intentionally include a piece that does not belong. While oral histories lend themselves to differing personal perspectives, they add a richness and detail that are not captured in documents such as annual reports and yet say much of a time, a place and an organisation.
Alas, not every person, nor every aspect of research, could possibly have been included in this history. Nor indeed could everyone who contributed some memory be cited. Genuine thanks are extended to those who did give time and patience. Genuine thanks also is extended to all who have served, and continue to serve, the QIMR Berghofer Medical Research Institute in laboratories and administrative offices, for the difference you all make to Queensland, Australia, and to world health.
Photographs courtesy: Brisbane City Council, Cancer Council QLD, State Library of Queensland, The Courier-Mail, Tony Phillips Photography, Bancroft family collection, Dr E.H. Derrick, Professor Ralph Doherty, Madeleine Flynn, Heather Matthews, Jacki Phelps, Ruth Thomson, Dr John Tonge, past and present staff of the Institute.
Reasonable attempts have been made to identify and acknowledge the photographers of images contained in this publication. QIMR Berghofer Medical Research Institute welcomes contact from photographers so that archival records may be updated accordingly and due attribution can be made to respect the moral rights of the author.
ACKNOWLEDGMENTS
95




QIMR BERGHOFER | OVER A LIFETIM
E — 70 Y
EA
RS
OF M
ED
ICA
L RE
SE
AR
CH








![JIMI HENDRIX: LIFETIME (Pre 9/18/70) RECORD · PDF file11/27/17 JIMI HENDRIX: LIFETIME (Pre 9/18/70) RECORD COLLECTION [with DISCOGRAPHY] 45s & EP (139) pieces LPs (144) separate](https://static.fdocuments.net/doc/165x107/5a8edfac7f8b9a085a8d76cd/jimi-hendrix-lifetime-pre-91870-record-jimi-hendrix-lifetime-pre-91870.jpg)









