Original Article Prevalence of HCV and HBV infection in HIV-infected patients … · 2018. 8....
12
Int J Clin Exp Med 2016;9(6):10615-10626 www.ijcem.com /ISSN:1940-5901/IJCEM0023203 Original Article Prevalence of HCV and HBV infection in HIV-infected patients receiving combined antiretroviral therapy and the impact of co-infections on mortality: a retrospective cohort in Xinjiang, China Peierdun Mijiti 1 , Zhang Yuexin 2 , Maimaitili Wubuli 2 , Pan Kejun 2 , Halmurat Upur 3 1 Department of Epidemiology and Biostatistics, Xinjiang Medical University, Urumqi, China; 2 Department of Infec- tious Diseases, The First Affiliated Hospital, Xinjiang Medical University, Urumqi, China; 3 Xinjiang Medical Univer- sity, Urumqi, China Received January 4, 2016; Accepted April 1, 2016; Epub June 15, 2016; Published June 30, 2016 Abstract: Objectives: To evaluate the prevalence of HBV and/or HCV among HIV-infected patients in Xinjiang, China and to assess the impact of co-infections on all-cause mortality following the combined antiretroviral therapy (cART). Methods: Routinely collected clinical data from 3425 HIV-infected patients enrolled in the National Free Antiret- roviral Treatment Program in Xinjiang from 1 January 2005 to 31 December 2011 were retrospectively analyzed. Results: 2448 (70.9%) patients were tested for hepatitis B surface antigen (HBsAg) and HCV antibody (anti-HCV) before cART. Of them, 168 (6.8%) were positive for HBsAg, 919 (37.5%) were positive for anti-HCV, and 67 (2.7%) were positive for both markers. Patients were followed for a median of 1.7 years (interquartile ranges: 0.5-2.9) after initiation of cART. After adjustment on potential confounders, higher risks of mortality were associated with HIV/HBV dual co-infection (aHR=2.30, 95% CI: 1.11-4.78), HIV/HCV dual co-infection (aHR=1.93, 95% CI: 1.25-2.99), and HIV/HBV/HCV triple co-infection (aHR=5.48, 95% CI: 2.90-10.33) compared to HIV mono-infection. Only one fourth of patients with positive HBsAg received appropriate cART (TDF+3TC based regimen). Few (0.9%) patients with HCV infection received HCV treatment during the follow-up. Conclusions: Co-infections with HBV or HCV is frequent in HIV patients and increases the mortality risk in patients receiving cART. Strengthening the knowledge of health care providers on management and care of co-infected hepatitis and HIV patients is needed in China to reduce the mortality risk of co-infected patients. Keywords: Human immunodeficiency virus, hepatitis virus, co-infection, all-cause mortality, China Introduction The control and prevention of human immuno- deficiency virus (HIV) infection remains a public health priority in China. To December 2011, an estimated 780,000 individuals were living with HIV, and approximately 154,000 had acquired immune deficiency syndrome (AIDS) [1]. In the past decade, the Chinese government has ta- ken a comprehensive, evidence-based appro- ach in responding to HIV/AIDS [2]. Particularly as a result of the National Free Antiretroviral Treatment Program (NFATP), HIV-related mor- tality has been decreasing in China since 2003 [3, 4]. Combined antiretroviral therapy (cART) has significantly reduced AIDS-related mortali- ty and increased patient’s life expectancy. Su- bsequently, non-AIDS related disease, particu- larly liver disease caused by hepatitis B virus (HBV) and hepatitis C virus (HCV) infection is emerging in western countries as a major cause of mortality in HIV-infected patients [5]. HIV, HBV, and HCV share similar transmission routes with common coinfections [6]. Up to 25% of HIV-infected individuals in the United States have HCV infection [7]. HBV coinfects 6-14% of individuals infected with HIV in Western Europe and the United States [8]. Prevalence of HBV and HCV among HIV-infected individuals in resource-limited countries is various. A study in Nigeria reported 17.8% and 11.3% of HIV-
Transcript of Original Article Prevalence of HCV and HBV infection in HIV-infected patients … · 2018. 8....

Int J Clin Exp Med 2016;9(6):10615-10626www.ijcem.com /ISSN:1940-5901/IJCEM0023203
Original ArticlePrevalence of HCV and HBV infection in HIV-infected patients receiving combined antiretroviral therapy and the impact of co-infections on mortality: a retrospective cohort in Xinjiang, China
Peierdun Mijiti1, Zhang Yuexin2, Maimaitili Wubuli2, Pan Kejun2, Halmurat Upur3
1Department of Epidemiology and Biostatistics, Xinjiang Medical University, Urumqi, China; 2Department of Infec-tious Diseases, The First Affiliated Hospital, Xinjiang Medical University, Urumqi, China; 3Xinjiang Medical Univer-sity, Urumqi, China
Received January 4, 2016; Accepted April 1, 2016; Epub June 15, 2016; Published June 30, 2016
Abstract: Objectives: To evaluate the prevalence of HBV and/or HCV among HIV-infected patients in Xinjiang, China and to assess the impact of co-infections on all-cause mortality following the combined antiretroviral therapy (cART). Methods: Routinely collected clinical data from 3425 HIV-infected patients enrolled in the National Free Antiret-roviral Treatment Program in Xinjiang from 1 January 2005 to 31 December 2011 were retrospectively analyzed. Results: 2448 (70.9%) patients were tested for hepatitis B surface antigen (HBsAg) and HCV antibody (anti-HCV) before cART. Of them, 168 (6.8%) were positive for HBsAg, 919 (37.5%) were positive for anti-HCV, and 67 (2.7%) were positive for both markers. Patients were followed for a median of 1.7 years (interquartile ranges: 0.5-2.9) after initiation of cART. After adjustment on potential confounders, higher risks of mortality were associated with HIV/HBV dual co-infection (aHR=2.30, 95% CI: 1.11-4.78), HIV/HCV dual co-infection (aHR=1.93, 95% CI: 1.25-2.99), and HIV/HBV/HCV triple co-infection (aHR=5.48, 95% CI: 2.90-10.33) compared to HIV mono-infection. Only one fourth of patients with positive HBsAg received appropriate cART (TDF+3TC based regimen). Few (0.9%) patients with HCV infection received HCV treatment during the follow-up. Conclusions: Co-infections with HBV or HCV is frequent in HIV patients and increases the mortality risk in patients receiving cART. Strengthening the knowledge of health care providers on management and care of co-infected hepatitis and HIV patients is needed in China to reduce the mortality risk of co-infected patients.
Keywords: Human immunodeficiency virus, hepatitis virus, co-infection, all-cause mortality, China
Introduction
The control and prevention of human immuno-deficiency virus (HIV) infection remains a public health priority in China. To December 2011, an estimated 780,000 individuals were living with HIV, and approximately 154,000 had acquired immune deficiency syndrome (AIDS) [1]. In the past decade, the Chinese government has ta- ken a comprehensive, evidence-based appro- ach in responding to HIV/AIDS [2]. Particularly as a result of the National Free Antiretroviral Treatment Program (NFATP), HIV-related mor-tality has been decreasing in China since 2003 [3, 4]. Combined antiretroviral therapy (cART) has significantly reduced AIDS-related mortali-
ty and increased patient’s life expectancy. Su- bsequently, non-AIDS related disease, particu-larly liver disease caused by hepatitis B virus (HBV) and hepatitis C virus (HCV) infection is emerging in western countries as a major cause of mortality in HIV-infected patients [5].
HIV, HBV, and HCV share similar transmission routes with common coinfections [6]. Up to 25% of HIV-infected individuals in the United States have HCV infection [7]. HBV coinfects 6-14% of individuals infected with HIV in Western Europe and the United States [8]. Prevalence of HBV and HCV among HIV-infected individuals in resource-limited countries is various. A study in Nigeria reported 17.8% and 11.3% of HIV-

HBV/HCV co-infection with HIV in China
10616 Int J Clin Exp Med 2016;9(6):10615-10626
infected patients were coinfected with HBV and HCV [9], respectively, and a study from Thailand reported the prevalence of HBV infection was 11.3% and HCV infection was 3.9% in HIV-infected patients [10]. Reports from China showed HBV prevalence ranged from 6.3-19.4% and HCV prevalence ranged from 14.7-62.4% among HIV-infected individuals, depend-ing on the regions and the population studied [11-14].
HIV accelerates the progression to hepatic fibrosis induced by hepatitis viruses, frequently leading to cirrhosis and hepatocellular carcino-ma. Hepatitis viruses may influence HIV dis-ease progression and treatment outcomes [15]. Previous studies show that HCV coinfec-tion increases the risk of AIDS-related, liver-related, and all-cause mortalities among indi-viduals infected with HIV, despite the use of cART [16-18]. However, the impact of HIV/HBV coinfection on mortality in patients receiving cART is less clear. Some studies report that HIV/HBV coinfection increases the risk of liver-related and all-cause mortality [19-21], where-as other studies report no effect on mortality [22-24].
Although HBV and HCV infections are frequent in HIV-infected individuals in China, their impact on survival in patients receiving cART is little known. The predominant HBV genotype and transmission mode in China are very different from those in western countries, potentially causing different risks. HIV/HCV coinfected patients barely seek for HCV treatment in China, and the potent antiretroviral drug which is active against both HIV and HBV-tenofovir disoproxil fumarate (TDF) is not accessible to most of Chinese patients [25]. Therefore, it is necessary to investigate the impact of coinfec-tions on survival in patients receiving cART in China.
In this study, we evaluated the prevalence of HBV and HCV prior to cART among HIV-infected patients from 2005 to 2011 in Xinjiang (a prov-ince in northwestern China), and assessed the impact of HIV/HBV, HIV/HCV, and HIV/HBV/HCV coinfections on mortality following cART.
Methods
Study design
This study was a retrospective cohort study of 3425 patients infected with HIV enrolled in the
NFATP in Xinjiang, China from 1 January 2005 to 31 December 2011.
Data source
The NFTATP, initiated in 2002 and expanded in 2003, uses a county-level, community-care model to provide free cART, follow-up, monitor-ing, and care to rural and low-income urban patients infected with HIV. Currently, the NFATP includes more than 3000 ART sites (hospitals and clinics attached to local centers for dis-ease control and prevention) across China [26].
Briefly, all patients infected with HIV in China receive periodic medical evaluations following diagnosis. Patients meeting the national treat-ment guideline criteria (i.e., CD4 cell count <200 cells/μL, or World Health Organization [WHO] disease stage-III and stage-IV) are referred to a local ART site for treatment. In 2008, the national treatment guidelines were revised to also include patients with a CD4 cell count between 200-350 cells/μL. Prior to cART, a baseline evaluation of patients (clinical assessment and basic laboratory tests) was conducted by healthcare providers at the ART sites. Following cART, follow-up visits were scheduled at 2 weeks, 1 month, 2 months, 3 months, and every 3 months thereafter to mon-itor the safety, tolerability and adherence to antiretroviral drugs. At baseline and each fol-low-up visit, sociodemographic and clinical data were collected by the healthcare providers and transferred to the NFATP database using a standard case report form. In addition if there was a change in medication (excluding a dos-age change) or the treatment was discontinued or withheld for any reason during the follow-up, a treatment termination form or lost-form-fol-low-up form was completed and transferred to the NFATP database [27].
In this study, we captured the baseline and out-come data in the NFATP database for 3425 patients from 12 hospitals in 6 prefectures (four hospitals from Urumqi, three from Yili, one from Akesu, one from Hetian, two from Tulufan, and one from Hami) of Xinjiang province from 2005 to 2011. Baseline data used for analysis included: sociodemographic information, hei- ght, weight, WHO disease stage, CD4 cell count, test results for hepatitis C antibody (anti-HCV) and hepatitis B surface antigen (HBsAg), hema-tological test results (hemoglobin level, liver enzymes, and fasting blood glucose), and cART

HBV/HCV co-infection with HIV in China
10617 Int J Clin Exp Med 2016;9(6):10615-10626
regimens received by patients. Other serologi-cal markers for HBV and HCV such as HBV-DNA, HCV-RNA, genotypes were barely tested in HIV-infected patients in Xinjiang; therefore they were not routinely collected in NFATP database. Baseline data such as HIV viral load, renal func-tion, and other blood chemicals were not avail-able for many of the patients because they could hardly afford these tests; so they were not included in the analysis.
Patient selection
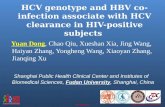
The inclusion criteria were: ≥18 years of age, no history of cART before enrollment in the NFATP, met the criteria in the national treatment guide-lines of China, and received cART before 31 December 2011. Patients who had no anti-HCV and HBsAg test results at baseline, lost to fol-low-up before receiving cART, or did notreceive cART before 31 December 2011 were excluded from the study (Figure 1).
Mortality reporting and observation period
Healthcare providers at the ART sites moni-tored mortality during the follow-up period. Survival time was calculated from the date of cART initiation until the date of mortality or cen-soring. The patients were censored on their date of withdrawal from the NFATP or on 31 December 2011, whichever occurred first. The
Statistical analysis
Continuous variables were summarized using medians and interquartile ranges (IQRs). Ca- tegorical variables were expressed as absolute frequencies and percentages. Sociodemogra- phic and hematological characteristics were compared using Kruskal-Wallis rank tests for continuous variables and Pearson’s chi-square tests for categorical variables. Pairwise com-parisons were made if overall test was signi- ficant.
Mortality rates were calculated as the number of deaths divided by person-years (PYs) of fol-low-up with 95% confidence interval (CI) [28].
Survival curves stratified by coinfection status were computed by the Kaplan-Meier (KM) method, and the log-rank test was used to com-pare KM curves.
We categorized the patients into four groups according to coinfection status: HIV monoinfec-tion, HIV/HBV coinfection [defined as HBsAg (+)/anti-HCV (-)], HIV/HCV coinfection [defined as HBsAg (-)/anti-HCV (+)], and HIV/HBV/HCV coinfection [defined as HBsAg (+)/anti-HCV (+)]. We used a Cox proportional hazard (PH) regres-sion analysis to evaluate the impact of coinfec-tion status on survival, adjusting for potential confounders. The PH assumption was tested
Figure 1. Selection of study patients in the National Free Antiretroviral Treat-ment Program in Xinjiang, China.
reasons for withdrawal in- cluded loss from follow-up (missing >3 follow-up vis-its), treatment termination, or transfer to another he- althcare facility. The with-drawal date was the last date the patient was seen in the clinic.
Ethics statement
The Ethics Committee of First Affiliated Hospital of Xinjiang Medical University reviewed and approved the analysis. All private inform- ation was kept confidential and used for population an- alysis only. Written inform- ed consent was obtained from all patients before en- rollment in the NFATP.

HBV/HCV co-infection with HIV in China
10618 Int J Clin Exp Med 2016;9(6):10615-10626
using both graphical (log-log plots) and Goodness-of-Fit approaches. Initially, we evalu-ated the risk of mortality stratified by coinfec-tion status using a univariate analysis. We then fitted three Cox PH models in our multivariate analysis. Model 1 was adjusted for baseline sociodemographics. Model 2 was adjusted for baseline sociodemographics, body mass index (BMI), anemia, fasting blood-glucose level, and
elevated aspartate aminotransferase (AST). Model 3 was adjusted for the same variables as Model 2 and cART regimens. To identify interaction effects, we added two-way multipli-cative interaction terms for the predictors in the models. No interaction effects were statisti-cally significant, and their inclusion did not change the significance of the main effects. Adjusted and unadjusted hazard ratios (HRs)
Table 1. Baseline characteristics of 2448 HIV-infected patients stratified by coinfection statusCharacteristics (n, %) Total (n, %) HIV only HIV/HBV HIV/HCV HIV/HBV/HCV χ2 PTotal 2448 1428 (58.3) 101 (4.1) 852 (34.8) 67 (2.8)Residency*,‡,※,† 87.76 P<0.001 Urumqi 360 (14.7) 179 (12.5) 28 (27.7) 146 (17.1) 7 (10.4) Akesu 461 (18.8) 321 (22.5) 15 (14.9) 111(13.0) 14 (20.9) Yi Li 1476 (60.3) 811 (56.8) 51 (50.5) 574 (67.4) 40 (59.7) Others 151 (6.2) 117 (8.2) 7 (6.9) 21 (2.5) 6 (9.0)Age at HIV diagnosis‡,※,†,§ 40.42 P<0.001 ≥45 years 220 (9.0) 165 (11.6) 15 (14.9) 37 (4.3) 3 (4.5) <45 years 2228 (91.0) 1263 (88.4) 86 (85.1) 815 (95.7) 64 (95.5)Gender*,‡,§,† 526.93 P<0.001 Male 1330 (54.3) 499 (34.9) 69 (68.3) 706 (82.9) 56 (83.6) Female 1118 (45.7) 929 (65.1) 32 (31.7) 146 (17.1) 11 (16.4)Ethnic group*,※,† 55.20 P<0.001 Uyghur 2112 (86.3) 1240 (86.9) 69 (68.3) 743 (87.2) 60 (89.5) Han 241 (9.8) 129 (9.0) 31 (30.7) 78 (9.2) 3 (4.5) Others 95 (3.9) 59 (4.1) 1 (1.0) 31 (3.6) 4 (6.0)Route of HIV infection*,‡,§,※,† 989.83 P<0.001 Intravenous drug use 900 (36.8) 174 (12.1) 31 (30.7) 647 (75.9) 48 (71.6) Unprotected sex 1189 (48.6) 991 (69.4) 52 (51.5) 137 (16.1) 9 (13.4) Blood transfusion 17 (0.6) 8 (0.6) 2 (2.0) 6 (0.7) 1 (1.6) Unknown 342 (14.0) 255 (17.9) 16 (15.8) 62 (7.3) 9 (13.4)WHO disease stage Stage I/II 1618 (66.1) 946 (66.2) 61 (60.4) 568 (66.7) 43 (64.2) 1.71 0.634 Stage III/IV 830 (33.9) 482 (33.8) 40 (39.6) 284 (33.3) 24 (35.8)BMI value 11.71 0.069 <18.5 kg/m2 191 (7.8) 101 (7.1) 6(5.9) 78 (9.2) 6 (9.0) 18.5-25 kg/m2 2097 (85.7) 1218 (85.3) 87 (86.2) 733 (86.0) 59 (88.0) ≥25 kg/m2 160 (6.5) 109 (7.6) 8 (7.9) 41 (4.8) 2 (3.0)cART regimens‡ 31.04 P<0.001 TDF+3TC based 612 (25.0) 308 (21.6) 22 (21.8) 260 (30.5) 22 (32.8) AZT+3TC based 1592 (65.0) 955 (66.9) 70 (69.3) 527 (61.9) 40 (59.7) D4T+3TC based 200 (8.2) 134 (9.4) 7 (6.9) 55 (6.5) 4 (6.0) Others 44 (1.8) 31 (2.2) 2 (2.0) 10 (1.1) 1 (1.5)Abbreviations: HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; BMI, body mass index; cART, combined antiretroviral therapy; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine; AZT, zidovudine; D4T, stavudine; WHO, world health organization. *HIV/HBV coinfection vs. HIV monoinfection, P<0.001; ‡HIV/HCV coinfection vs. HIV monoinfection, P<0.001; §HIV/HBV/HCV coinfection vs. HIV monoinfection, P<0.001; ※HIV/HBV coinfection vs. HIV/HBV/HCV coinfection, P<0.001; †HIV/HBV coinfection vs. HIV/HCV coinfection, P<0.001.

HBV/HCV co-infection with HIV in China
10619 Int J Clin Exp Med 2016;9(6):10615-10626
and 95% CIs were computed. We performed all analysis using SPSS version 17.0 and used two-sided hypothesis tests with an alpha of 0.05 to determine statistical significance.
We defined anemia as a hemoglobin level less than 13 g/dl for men and less than 12 g/dl for women. Fasting blood glucose was dichoto-mized into ≥6.1 mmol/L or <6.1 mmol/L to allow the combining of impaired fasting glucose and diabetes mellitus (DM) because of small number of DM patients. The cART regimens included zidovudine (AZT) or stavudine (D4T) + lamivudine (3TC) + efavirenz (EFV) or nevirap-ine (NVP), TDF+3TC+EFV or NVP, and other regi-mens (single or dual antiretroviral therapy excluding TDF). We categorized the cART regi-mens into “AZT+3TC based”, “D4T+3TC based”, “TDF+3TC based” and “others” to adjust for the effect of cART regimen on survival.
Results
We excluded 977 patients from the analysis for not meeting the inclusion criteria (Figure 1). Therefore, our analysis included a total of 2448 individuals, accounting for 29.1% of total patients enrolled in the NFATP during the study period in Xinjiang. Sociodemographic charac-teristics of the excluded patients were not sig-nificantly different from patients included in the analysis.
Baseline characteristics
Sociodemographic and hematological charac-teristics of the patients are shown in Tables 1 and 2. The mean age of the patients was 34.72±8.17 years. Majority of patients were ethnic Uyghur and Yili residents. The most fre-quent source of HIV infection was unprotected sex, followed by intravenous drug use (IDU), and blood transfusion. 65.0% of patients received AZT+3TC based cART regimens, fol-lowed by TDF+3TC based regimens (25.0%), and D4T+3TC based regimens (8.2%).
Baseline coinfection rates
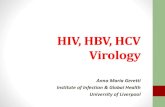
Overall, 168 patients (6.8%) tested positive for HBsAg, 919 patients (37.5%) tested positive for anti-HCV, and 67 patients (2.7%) tested posi-tive for both HBsAg and anti-HCV prior to receiv-ing cART. We stratified the prevalence of posi-tive tests for HBsAg and anti-HCV by routes of HIV infection. Among the patients who contract-ed HIV through IDU, the overall prevalence rates of positive HBsAg and anti-HCV tests were 8.8% and 77.2%, respectively; and annual prevalence rates of positive HBsAg and anti-HCV from 2005 to 2011 were not significantly different (P>0.05) (Figure 2). The overall preva-lence rates of positive tests for HBsAg and anti-HCV among patients who contracted HIV though unprotected sex were lower (5.1% and
Table 2. Hematological characteristics of 2448 patients infected with HIV stratified by coinfection status at baseline Characteristics (n, %) Total HIV only HIV/HBV HIV/HCV HIV/HBV/HCV χ2 PMedian CD4 count (cells/μl, IQRs) 228 (137, 309) 231 (140, 315) 219 (135, 309) 228 (135, 303) 191 (120, 305) 2.00 0.572
CD4 count category 3.88 0.274
<200 cells/μl 1002 (40.9) 581 (40.7) 46 (45.5) 341 (40.0) 34 (50.7)
≥200 cells/μl 1446 (59.1) 847 (59.3) 55 (54.5) 511 (60.0) 33 (49.3)
Anemia*,‡ 53.38 P<0.001
yes 998 (40.8) 666 (46.6) 32 (31.7) 271 (31.8) 29 (43.3)
No 1450 (59.2) 762 (53.4) 69 (68.3) 581 (68.2) 38 (56.7)
Fasting blood glucose§ 27.28 P<0.001
≥6.1 mmol/L 147 (6.0) 78 (5.5) 7 (6.9) 53 (6.2) 9 (13.4)
<6.1 mmol/L 2044 (83.5) 1226 (85.9) 74 (73.3) 691 (81.1) 53 (79.1)
Missing data 257 (10.5) 124 (8.7) 20 (19.8) 108 (12.7) 5 (7.5)
Elevated ALT*,‡,§ 131.90 P<0.001
≥2 ULN 231 (9.4) 53 (3.7) 16 (15.8) 151 (17.7) 11 (16.4)
<2 ULN 2217 (90.6) 1375 (96.3) 85 (84.2) 701 (82.3) 56 (83.6)
Elevated AST*,‡,§
≥2 ULN 201 (8.2) 44 (3.1) 15 (14.9) 130 (15.3) 12 (17.9) 120.28 P<0.00
<2 ULN 2247 (91.8) 1384 (96.9) 86 (85.1) 722 (84.7) 55 (82.1)Abbreviations: HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; IQRs, interquartile ranges; ALT, alanine aminotransferase; AST, aspar-tate aminotransferase; ULN, upper limit of normal (ULN for ALT and AST is 40 IU/l). *HIV/HBV coinfection vs. HIV monoinfection, P<0.001; ‡HIV/HCV coinfection vs. HIV monoinfection, P<0.001; §HIV/HBV/HCV coinfection vs. HIV monoinfection, P<0.001.

HBV/HCV co-infection with HIV in China
10620 Int J Clin Exp Med 2016;9(6):10615-10626
12.3%, respectively), and annual prevalence rates of positive HBsAg and anti-HCV from 2005 to 2011 were not significantly different (P>0.05) (Figure 3).
Baseline characteristics of patients with coin-fections are shown in Tables 1 and 2. All base-line and hematological characteristics were similar between the patients with HIV/HCV coinfection and those with HIV/HBV/HCV coin-fection (P>0.05 for each comparison). Compa- red to those with HIV monoinfection, patients with HIV/HBV coinfection were more likely to be male, ethnic Han, and more than 45 years old,
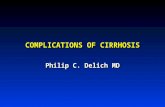
ence in survival between the patients with HIV/HBV coinfection and those with HIV/HCV coin-fection (log-rank test: P>0.05). Each of the other pairwise comparisons between the patient groups showed a significant difference in survival (log-rank test: P<0.001 for each pair-wise comparison) (Figure 4).
The univariate Cox PH regression analysis showed that, compared with the patients with HIV monoinfection, those with HIV/HBV/HCV coinfection had the highest risk of mortality (crude HR=9.01, 95% CI: 5.31-15.27), followed by those with HIV/HBV (crude HR=2.93, 95% CI:
Figure 2. Trends of HBsAg and anti-HCV prevalences among individuals who contracted HIV through IDU (n=900) in Xinjiang, China, 2005-2011.
Figure 3. Trends of HBsAg and anti-HCV prevalences among individuals who contracted HIV through unprotected sex (n=1189) in Xinjiang, China, 2005-2011.
and contract HIV through IDU (P<0.001 for each com-parison), but less likely to have anemia, and patients with HIV/HCV coinfection were more likely to be male, less than 45 years old, and contract HIV through IDU (P<0.001 for each compari-son). Patients with HIV/HBV coinfection were more like-ly to contract HIV through unprotected sex than those with HIV/HCV or HIV/HBV/HCV coinfection (P<0.001 for each comparison). The median CD4 counts were similar among the four groups (P>0.05). Elevated ALT and AST were more fre-quent within each group of patients with coinfections compared with the patients with HIV monoinfection (P<0.001 for each pairwise comparison).
Univariate and multivariate analyses of mortality risk stratified by coinfection status
Patients were followed for a median of 1.7 years (IQRs: 0.5-2.9), resulting in a total of 4712 person years (PYs) of follow-up. The overall mo- rtality rate was 3.14 deaths per 100 PYs (95% CI: 2.67-3.69) (Table 3). Kaplan-Me- ier analysis found no differ-

HBV/HCV co-infection with HIV in China
10621 Int J Clin Exp Med 2016;9(6):10615-10626
1.48-5.77) and HIV/HCV coinfections (crude HR=2.30, 95% CI: 1.60-3.30) (Table 3).
The results of the multivariate Cox PH regres-sion models are shown in Table 4. After adjust-ing for sociodemographics, comorbidities and cART regimens (Model 3), HIV/HBV (aHR=2.30, 95% CI: 1.11-4.78), HIV/HCV (aHR=1.93, 95% CI: 1.25-2.99), and HIV/HBV/HCV (aHR=5.48, 95% CI: 2.90-10.33) coinfections were still as- sociated with increased risk of mortality com-pared with HIV monoinfection. However, there were no significant differences in mortality risk between the patients with HIV/HCV and HIV/HBV coinfections (HIV/HBV vs. HIV/HCV, aHR =0.84; 95% CI: 0.41-1.73). Patients with HIV/
HCV and HBV treatment during the follow-up
Of 168 patients diagnosed with positive HBsAg, 44 (26.2%) received TDF+3TC based cART regi-mens, and 124 (73.8%) were given other cART regimens without TDF. During the follow-up, one death (2.3%) was observed among patients in the former group, whereas 29 (23.4%) deaths were observed among patients in the latter group, the difference was significant (P<0.01).
Among 919 patients with positive anti-HCV test, 8 patients (0.9%) received treatment with interferon and ribavirin. No death was observed among those with HCV treatment during the follow-up.
Table 3. Univariate analysis of mortality stratified by coinfection status
Co-infection status Number of deaths
Total PYs of Follow-up
Mortality rate (per 100 PYs, 95% CI) HR (95% CI) P
HIV/HBV coinfection 10 189 5.29 (2.85, 9.83) 2.93 (1.48, 5.77) 0.002HIV/HCV coinfection 68 1609 4.23 (3.34, 5.36) 2.30 (1.60, 3.30) <0.001HIV/HBV/HCV coinfection 19 119 15.97 (10.19, 25.04) 9.01 (5.31, 15.27) <0.001HIV monoinfection 51 2796 1.82 (1.38, 2.39) 1.00Overall 148 4712 3.14 (2.67, 3.69) - -Abbreviations: HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; HR, hazard ratio, CI, confi-dence interval, PYs, person years.
Figure 4. Kaplan-Meier survival estimates of all-cause mortality stratified by coinfection status. Log-rank tests: HIV/HBV coinfection vs. HIV/HCV coinfection, P>0.05; HIV/HBV coinfection vs. HIV/HBV/HCV coinfection, P<0.001; HIV/HCV coinfection vs. HIV/HBV/HCV coinfection, P<0.001; HIV monoinfection vs. HIV/HBV coinfection, P<0.001; HIV monoinfection vs.HIV/HCV confection, P<0.001.
HBV/HCV coinfection had greater risk of mortality co- mpared to patients with HIV/HCV coinfection (aHR= 2.84; 95% CI: 1.64-4.92) and HIV/HBV (aHR=2.38; 95% CI: 1.04-5.44) coinfe- ction.
Other covariates associat-ed with a significantly in- creased mortality risk in the multivariate regression model (model 3) included being Akesu residents, ma- le gender, age ≥45 years, CD4 count <200 cells/μl, anemia, lower BMI value, elevated AST, and D4T+3TC based cART (Table 4). Co- variates associated with a significantly decreased risk of mortality included WHO disease stage I/II and TDF+ 3TC based cART.

HBV/HCV co-infection with HIV in China
10622 Int J Clin Exp Med 2016;9(6):10615-10626
Discussions
Xinjiang province is an important consumption and transit area on the drug trafficking routes in China and has a high prevalence of HIV infec-
tion from IDU. The HIV prevalence in Xinjiang was three times higher than the national aver-age at the end of 2011.1 Because of the shared mode of transmission, persons with a high risk of HIV infection are more likely to have HBV and
Table 4. Multivariate Cox proportional hazard regression models for the risk of mortality stratified by coinfection status
VariablesModel 1 Model 2 Model 3
P aHR (95% CI) P Ahr (95% CI) P aHR (95% CI)Co-infection status HIV/HBV coinfection 0.008 2.60 (1.28, 5.27) 0.039 2.16 (1.04, 4.50) 0.025 2.30 (1.11, 4.78) HIV/HCV coinfection 0.004 1.94 (1.24, 3.04) 0.001 2.13 (1.39, 3.32) 0.003 1.93 (1.25, 2.99) HIV/HBV/HCV coinfection <0.001 5.23 (2.81, 9.72) <0.001 5.33 (2.83, 10.04) <0.001 5.48 (2.90, 10.33) HIV monoinfection Reference Reference ReferenceResidency Others <0.001 0.22 (0.10, 0.51) 0.008 0.31 (0.13, 0.74) 0.004 0.28 (0.11, 0.66) Yi Li <0.001 0.29 (0.20, 0.45) <0.001 0.30 (0.19, 0.48) <0.001 0.40 (0.25, 0.65) Urumqi <0.001 0.10 (0.05, 0.19) <0.001 0.07 (0.04, 0.14) <0.001 0.07 (0.03, 0.13) Akesu Reference Reference ReferenceAge at HIV diagnosis ≥45 years vs. <45 years 0.006 1.98 (1.21, 3.24) 0.001 2.37 (1.42, 3.94) 0.001 2.45 (1.47, 4.07)Gender Male vs. Female 0.002 2.31 (1.37, 3.87) 0.005 2.17 (1.28, 3.74) 0.003 2.25 (1.31, 3.87)Ethnic group Uighur Reference Reference Reference Han 0.308 0.59 (0.21, 1.63) 0.724 0.83 (0.30, 2.31) 0.627 0.78 (0.28, 2.16) Others 0.551 0.82 (0.44, 1.56) 1.04 (0.54, 1.99) 0.999 1.00 (0.53, 1.91)WHO disease stage Stage I/II vs. Stage III/IV - - <0.001 0.44 (0.30. 0.65) <0.001 0.50 (0.33, 0.73)BMI value <18.5 kg/m2 - - <0.001 2.33 (1.53, 3.56) <0.001 2.29 (1.50, 3.49) ≥25 kg/m2 - - 0.085 2.05 (0.91, 4.63) 0.123 1.91 (0.84, 4.34)
18.5-25 kg/m2 - - Reference Reference CD4 count category <200 cells/μl vs. ≥200 cells/μl - - <0.001 3.19 (2.09, 4.87) <0.001 3.25 (2.14, 4.94)Anemia Yes vs. No - - <0.001 1.91 (1.32, 2.76) 0.002 1.81 (1.25, 2.64)Elevated AST ≥2ULN vs. <2ULN - - 0.031 1.67 (1.05, 2.65) 0.004 1.99 (1.25, 3.17)
Fasting blood glucose - ≥6.1 mmol/L - - 0.112 0.55 (0.27, 1.15) 0.424 0.74 (0.36, 1.54) Missing data - - 0.881 1.04 (0.63, 1.73) 0.664 1.12 (0.67, 1.87) <6.1 mmol/L - - Reference Reference cART regimens‡
TDF+3TC based - - - - <0.001 0.07 (0.02, 0.29) D4T+3TC based - - - - 0.003 1.98 (1.27, 3.09) Others - - - - 0.212 1.80 (0.72, 4.53) AZT+3TC based - - - - Reference Abbreviations: HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; cART, combined antiretroviral therapy; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine; AZT, zidovudine; D4T, stavudine. AST, aspartate aminotransferase; BMI, body mass index; ULN, upper limit of normal (ULN for AST is 40 IU/l); 95% CI, 95% confidence interval; aHR, adjusted hazard ratio.

HBV/HCV co-infection with HIV in China
10623 Int J Clin Exp Med 2016;9(6):10615-10626
HCV infections [8]. We found that positive tests for HBsAg and anti-HCV were more common among patients with HIV infections (6.8% and 37.5%, respectively) than within the Xinjiang general population (4.6% and 3.1%, respective-ly) [29]. The prevalence of HCV and HBV coin-fection may vary, however, depending on the route of HIV acquisition [8]. In our study, 12.3% of patients who acquired HIV via unprotected sex tested positive for anti-HCV, which was greater than in previous studies in China (6.6%-8.3%) [11, 12]. We found that 77.2% of patients in our study who contracted HIV through IDU tested positive for anti-HCV, which was similar to the rate among such patients across 10 provinces of China (78.5%) [12] but lower than that in Guangxi province (95.1%) [30] and Yunnan province (99.1%) [31]. Chronic HBV infection is highly endemic in China and varies geographically [32]. Compared with other prov-inces, Xinjiang has lower HBV endemicity, which is reflected in the HBV endemicity among patients with HIV infections. Compared with other studies [11, 13], we found that a smaller proportion of patients with HIV infection tested positive for HBsAg (5.1% of those who acquired HIV via unprotected sex and 8.8% of those who acquired HIV via IDU).
Our results show that coinfection with HBV and HCV is frequent prior to cART initiation among patients infected with HIV in Xinjiang. Coin- fection with viral hepatitis complicates the delivery of cART by increasing the risk of drug-related hepatoxicity, increases liver-related mortality, and impacts on the selection of spe-cific agents (e.g., agents active against both HIV and HBV) [6]. All patients diagnosed with HIV in China should be routinely screened for HBV and HCV prior to cART so that they are properly managed.
Ours is the largest study to date evaluating the impact of HBV and HCV infections on mortality among patients infected with HIV and receiving cART in Western China. With adjustment for potential confounding effects, the mortality risk was greater among patients with HIV/HCV coinfection than among patients infected with HIV alone (aHR=1.93, P<0.05). This result is consistent with findings reported by Hernando V, et al. [17] and Hua L, et al. [18]. However, this finding should be interpreted with caution because active HCV infection is not identified in
this study. Interestingly, a recent study by Rockstroh JK, et al. reported that anti-HCV pos-itive patients with undetectable HCV-RNA (resolved infection) also had a 7-fold excess of liver-related deaths compared to anti-HCV neg-ative patients, although he explained this might be attributed to risk behaviors such as alcohol consumption and drug-using habits [33]. Further study is needed to clarify the impact of resolved HCV infection on mortality in Chinese patients receiving cART.
Studies of the impact of HIV/HBV coinfection on mortality risk among patients receiving cART in western countries have produced conflicting results. These controversial results might be partially attributable to small sample size, short follow-up period, failure to adjust for comorbidi-ties, and effects from the use of TDF-containing cART [34]. With adjustment for sociodemo-graphics, lower BMI, anemia, elevated AST, elevated fasting blood glucose, lower CD4 counts, cART regimens, etc. we found that Chinese patients with HIV/HBV coinfection still had twice the mortality risk (aHR=2.30, P<0.05) of patients with HIV monoinfection, similar to the results of a Taiwanese cohort study [35].
Among HIV-negative patients, HBV/HCV coin-fection seems to increase the severity of liver injury, the probability of liver cirrhosis, and the risk of developing hepatocellular carcinoma [36]. Similar results were also reported among patients infected with HIV. Bonacini M, et al. reported patients with HIV/HBV/HCV coinfec-tion had greater risk of liver-related mortality than those with HIV/HBV or HIV/HCV coinfec-tions [37]. Teira R, et al. reported HIV/HBV/HCV coinfected patients had higher risk of all-cause mortality compared to HIV/HCV coinfected patients (mortality rate ratio: 1.90, P<0.05) [38]. We also observed a higher risk of mortali-ty among patients with HIV/HBV/HCV coinfec-tion those with HIV/HBV or HIV/HCV coinfec-tions. However, the cause of mortality was not differentiated in the database we used, so we could not evaluate the impact of triple coinfec-tions on liver-related mortality, which should be assessed in further study.
We found that anemia, elevated AST, lower BMI value, male gender, older age at HIV diagnosis (45 years and older), and CD4 count <200 (cells/μl) at baseline were associated with increased risk of mortality, which was consis-

HBV/HCV co-infection with HIV in China
10624 Int J Clin Exp Med 2016;9(6):10615-10626
tent with other studies in China and abroad [3, 4, 39]. In addition, we found use of TDF+3TC based cART was associated with decreased risk of mortality and use of D4T+3TC based cART was associated with increased risk of mortality compared to use of AZT+3TC based cART. Particularly, a smaller death rate was observed in patients with HBV infection who received TDF+3TC based cART compared with those received other cART regimens. These results are consistent with other studies abroad China [40, 41]. Although TDF+3TC based cART are proved to be a potent therapy active against both HIV and HBV, we found only one fourth of patients who tested positive for HBsAg received it in northwestern China. TDF was in the sec-ond-line antiretroviral agents before 2012 in China and was not offered to majority of HIV patients for free. In the current revised version of China national antiretroviral treatment guide-lines (issued in 2012), TDF+3TC based cART regimens are among the first-line antiretroviral regimens and offered for free. Future studies should be conducted to evaluate the cost-effectiveness of Tenofovir as first-line antiretro-viral therapy in China.
Similarly, extremely low HCV treatment rate (0.8%) was found among HIV patients with posi-tive anti-HCV results. HCV infection is curable if properly treated with interferon and ribavirin [42]. However, a significant number of coinfect-ed patients are not treated with s standard drug therapy in China because it is beyond affordability of most coinfected patients. In addition, HCV testing and treatment are not available in rural healthcare settings in China [43]. Effort must be made, via multidisciplinary healthcare infrastructures, to increase the affordability and accessibility of HCV testing and treatment, especially in the more vulnera-ble groups (such as injection drug users, men who sex with men, people with excessive use of alcohol).
There are several limitations to our study that should be considered. First, results from this study may not be generalized to the entire pop-ulation in China, since most of patients in this study are ethnic minorities. Second, a complete set of serological markers for HBV and HCV, such as HBV-DNA, HCV-RNA, and genotypes, are unavailable in this study, which is our major limitation. Third, we lacked of information reg-
arding excessive alcohol consumption, which is associated with liver-related mortality [44]. In addition, death is not differentiated by specific cause in the database; therefore the impact of coinfections on liver-related mortality and oth- er cause-specific mortality is not evaluated. Moreover, data on CD4 cell counts and HIV viral load during follow-up are not accessible to us, therefore, we are not able to evaluate the impact of hepatitis virus infection on virological and immunological response to cART in Chinese patients, which should be investigated in future studies.
Our study suggests that HBV and HCV infec-tions are frequent among Chinese patients infected with HIV, and only a small number of coinfected patients receive HBV and HCV treat-ment, which negatively influences mortality risk after initiation of cART. Screening and surveil-lance of HBV and HCV should be enhanced prior to initiating cART. Efforts should be made to increase affordability and accessibility of HBV/HCV testing and treatment in HIV-infected patients.
Acknowledgements
This work was supported by the National Key Technology Research and Development Pro- gram (2014BAI10B00). We would like to thank Prof. Rune Andersson from institute of Biom- edicine, Sahlgrenska Academy at Gothenburg University, Sweden for reviewing our manu-script and giving important comments.
Disclosure of conflict of interest
None.
Address correspondence to: Hamulati Wufuer, Xin- jiang Medical University, No. 393, Xinyi Road, Urumqi 830011, China. Tel: +86 991 4366167; Fax: +86 991 4366014; E-mail: [email protected]
References
[1] Mijiti P, Yahepu D, Zhong X, Sun Y, Zhao T, Zhao Z, Abuduaili Z, Zhou H, Meng F, Dai J, Huang A. Awareness of and Willingness to Use Oral Pre-Exposure Prophylaxis for HIV Prevention among HIV-Serodiscordant Heterosexual Cou-ples: A Cross-Sectional Survey in Xinjiang, Chi-na. PLoS One 2013; 8: e67392.
[2] Wu Z, Sullivan SG, Wang Y, Rotheram-Borus MJ, Detels R. Evolution of China’s response to HIV/AIDS. Lancet 2007; 369: 679-690.

HBV/HCV co-infection with HIV in China
10625 Int J Clin Exp Med 2016;9(6):10615-10626
[3] Zhang F, Dou Z, Ma Y, Zhang Y, Zhao Y, Zhao D, Zhou S, Bulterys M, Zhu H, Chen RY. Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study. Lancet Infect Dis 2011; 11: 516-24.
[4] Zhang F, Dou Z, Ma Y, Zhao Y, Liu Z, Bulterys M, Chen RY. Five-year outcomes of the China Na-tional Free Antiretroviral Treatment Program. Ann Intern Med 2009; 151: 241-51.
[5] Joshi D, O’Grady J, Dieterich D, Gazzard B, Agarwal K. Increasing burden of liver disease in patients with HIV infection. Lancet 2011; 377: 1198-209.
[6] Koziel MJ, Peters MG. Viral hepatitis in HIV in-fection. N Engl J Med 2007; 356: 1445-54.
[7] Kim AY, Onofrey S, Church DR. An epidemio-logic update on hepatitis C infection in persons living with or at risk of HIV infection. J Infect Dis 2013; 207 Suppl 1: S1-6.
[8] Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006; 44 Suppl: S6-9.
[9] Ladep NG, Agaba PA, Agbaji O, Muazu A, Ugo-agwu P, Imade G, Cooke G, McCormack S, Tay-lor-Robinson SD, Idoko J, Kanki P. Rates and impact of hepatitis on human immunodeficien-cy virus infection in a large African cohort. World J Gastroenterol 2013; 19: 1602-10.
[10] Tsuchiya N, Pathipvanich P, Rojanawiwat A, Wichukchinda N, Koga I, Koga M, Auwanit W, Kilgore PE, Ariyoshi K, Sawanpanyalert P. Chronic hepatitis B and C co-infection in-creased all-cause mortality in HAART-naive HIV patients in Northern Thailand. Epidemiol Infect 2013; 141: 1840-8.
[11] Shen YZ, Wang ZY, Qi TK, Jiang XY, Song W, Tang Y, Wang JR, Liu L, Zhang RF, Zheng YF, Dai ZS, Lu HZ. Serological survey of viral hepatitis markers among newly diagnosed patients with HIV/AIDS in China. HIV Med 2013; 14: 167-75.
[12] Yan YX, Gao YQ, Sun X, Wang W, Huang XJ, Zhang T, Li M, Zang CP, Li ZC, Wu H. Prevalence of hepatitis C virus and hepatitis B virus infec-tions in HIV-positive Chinese patients. Epide-miol Infect 2011; 139: 354-60.
[13] He N, Chen L, Lin HJ, Zhang M, Wei J, Yang JH, Gabrio J, Rui BL, Zhang ZF, Fu ZH, Ding YY, Zhao GM, Jiang QW, Detels R. Multiple viral coinfections among HIV/AIDS patients in Chi-na. Biosci Trends 2011; 5: 1-9.
[14] Chen X, He JM, Ding LS, Zhang GQ, Zou XB, Zheng J. Prevalence of hepatitis B virus and hepatitis C virus in patients with human immu-nodeficiency virus infection in central China. Arch Virol 2013; 158: 1889-94.
[15] Lacombe K, Rockstroh J. HIV and viral hepati-tis coinfections: advances and challenges. Gut 2012; 61 Suppl 1: i47-58.
[16] Van der Helm J, Geskus R, Sabin C, Meyer L, Del Amo J, Chêne G, Dorrucci M, Muga R, Por-ter K, Prins M; CASCADE Collaboration in Euro-Coord. Effect of HCV infection on cause-specif-ic mortality after HIV seroconversion, before and after 1997. Gastroenterology 2013; 144: 751-760.
[17] Hernando V, Perez-Cachafeiro S, Lewden C, Gonzalez J, Segura F, Oteo JA, Rubio R, Dalmau D, Moreno S, Amo JD; CoRIS. All-cause and liv-er-related mortality in HIV positive subjects compared to the general population: differ-ences by HCV co-infection. J Hepatol 2012; 57: 743-751.
[18] Hua L, Andersen JW, Daar ES, Glesby MJ, Hol-labaugh K, Tierney C. Hepatitis C virus/HIV coinfection and responses to initial antiretrovi-ral treatment. AIDS 2013; 27: 2725-34.
[19] Hawkins C, Christian B, Ye J, Nagu T, Aris E, Chalamilla G, Spiegelman D, Mugusi F, Mehta S, Fawzi W. Prevalence of hepatitis B co-infec-tion and response to antiretroviral therapy among HIV-infected patients in Tanzania. AIDS 2013; 27: 919-927.
[20] Nikolopoulos GK, Paraskevis D, Hatzitheodor-ou E, Moschidis Z, Sypsa V, Zavitsanos X, Kala-pothaki V, Hatzakis A. Impact of hepatitis B vi-rus infection on the progression of AIDS and mortality in HIV-infected individuals: a cohort study and meta-analysis. Clin Infect Dis 2009; 48: 1763-71.
[21] Konopnicki D, Mocroft A, de Wit S, Antunes F, Ledergerber B, Katlama C, Zilmer K, Vella S, Kirk O, Lundgren JD; EuroSIDA Group. Hepati-tis B and HIV: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA co-hort. AIDS 2005; 19: 593-601.
[22] Otto-Knapp R, Cortes CP, Saavedra F, Wolff M, Weitzel T. Hepatitis B prevalence and influence on HIV treatment outcome and mortality in the Chilean AIDS Cohort. Int J Infect Dis 2013; 17: e919-924.
[23] Hoffmann CJ, Charalambous S, Martin DJ, Innes C, Churchyard GJ, Chaisson RE, Grant AD, Fielding KL, Thio CL. Hepatitis B virus in-fection and response to antiretroviral therapy (ART) in a South African ART program. Clin In-fect Dis 2008; 47: 1479-85.
[24] Law WP, Duncombe CJ, Mahanontharit A, Boyd MA, Ruxrungtham K, Lange JM, Phanuphak P, Cooper DA, Dore GJ. Impact of viral hepatitis co-infection on response to antiretroviral ther-apy and HIV disease progression in the HIV-NAT cohort. AIDS 2004; 18: 1169-77.

HBV/HCV co-infection with HIV in China
10626 Int J Clin Exp Med 2016;9(6):10615-10626
[25] Maimaiti R, Zhang Y, Pan K, Wubuli M, Anders-son R. Frequent coinfection with hepatitis among HIV-positive patients in Urumqi, China. J Int Assoc Provid AIDS Care 2013; 12: 58-61.
[26] Ma Y, Zhang F, Zhao Y, Zang C, Zhao D, Dou Z, Yu L, Fang H, Zhu TY, Chen RY. Cohort profile: the Chinese national free antiretroviral treat-ment cohort. Int J Epidemiol 2010; 39: 973-9.
[27] Dou Z, Chen RY, Xu J, Ma Y, Jiao JH, Durako S, Zhao Y, Zhao D, Fang H, Zhang F. Changing baseline characteristics among patients in the China National Free Antiretroviral Treatment Program, 2002-09. Int J Epidemiol 2010; 39 Suppl 2: ii56-64.
[28] Zhu H, Napravnik S, Eron JJ, Cole SR, Ma Y, Wohl DA, Dou Z, Zhang Y, Liu Z, Zhao D, Yu L, Liu X, Cohen MS, Zhang F. Decreasing Excess Mortality of HIV-Infected Patients Initiating An-tiretroviral Therapy: Comparison with Mortality in General Population in China, 2003-2009. J Acquir Immune Defic Syndr 2013; 63: e150-7.
[29] Jin XM, Dong HJ, Sun SY, Re XD, L XM, Gao Q, et al. Epidemiological investigation on serop-revalence of viral hepatitis in general popula-tion in Xinjiang. Shanghai J Preventive Med 1995; 7: 448-51.
[30] Garten RJ, Zhang J, Lai S, Liu W, Chen J, Yu XF. Coinfection with HIV and hepatitis C virus among injection drug users in southern China. Clin Infect Dis 2005; 41 Suppl 1: S18-24.
[31] Zhang C, Yang R, Xia X, Qin S, Dai J, Zhang Z, Peng Z, Wei T, Liu H, Pu D, Luo J, Takebe Y, Ben K. High prevalence of HIV-1 and hepatitis C vi-rus coinfection among injection drug users in the southeastern region of Yunnan, China. J Acquir Immune Defic Syndr 2002; 29: 191-6.
[32] Liang X, Bi S, Yang W, Wang L, Cui G, Cui F, Zhang Y, Liu J, Gong X, Chen Y, Wang F, Zheng H, Wang F, Guo J, Jia Z, Ma J, Wang H, Luo H, Li L, Jin S, Hadler SC5, Wang Y. Reprint of: Epidemiological serosurvey of Hepatitis B in China-Declining HBV prevalence due to Hepati-tis B vaccination. Vaccine 2013; 31 Suppl 9: J21-8.
[33] Rockstroh JK, Peters L, Grint D, Soriano V, Re-iss P, Monforte Ad, Beniowski M, Losso MH, Kirk O, Kupfer B, Mocroft A; EuroSIDA in EuroCoord. Does hepatitis C viremia or geno- type predict the risk of mortality in individuals co-infected with HIV? J Hepatol 2013; 59: 213-20.
[34] Jain MK. Mortality in patients coinfected with hepatitis B virus and HIV: could antiretroviral therapy make a difference? Clin Infect Dis 2009; 48: 1772-1774.
[35] Sheng WH, Chen MY, Hsieh SM, Hsiao CF, Wang JT, Hung CC, Chang SC. Impact of chron-ic hepatitis B virus (HBV) infection on out-comes of patients infected with HIV in an area where HBV infection is hyperendemic. Clin In-fect Dis 2004; 38: 1471-7.
[36] Hamzaoui L, El Bouchtili S, Siai K, Mahmoudi M, Azzouz MM. Hepatitis B virus and hepatitis C virus co-infection: a therapeutic challenge. Clin Res Hepatol Gastroenterol 2013; 37: e16-20.
[37] Bonacini M, Louie S, Bzowej N, Wohl AR. Sur-vival in patients with HIV infection and viral hepatitis B or C: a cohort study. AIDS 2004; 18: 2039-45.
[38] Teira R. Hepatitis-B virus infection predicts mortality of HIV and hepatitis C virus coinfect-ed patients. AIDS 2013; 27: 845-8.
[39] Jarrett OD, Wanke CA, Ruthazer R, Bica I, Isaac R, Knox TA. Metabolic syndrome predicts all-cause mortality in persons with human immu-nodeficiency virus. AIDS Patient Care STDS 2013; 27: 266-71.
[40] Velen K, Lewis JJ, Charalambous S, Grant AD, Churchyard GJ, Hoffmann CJ. Comparison of tenofovir, zidovudine, or stavudine as part of first-line antiretroviral therapy in a resource-limited-setting: a cohort study. PLoS One 2013; 8: e64459.
[41] Price H, Dunn D, Pillay D, Bani-Sadr F, de Vries-Sluijs T, Jain MK, Kuzushita N, Mauss S, Núñez M, Nüesch R, Peters M, Reiberger T, Stephan C, Tan L,Gilson R. Suppression of HBV by tenofovir in HBV/HIV coinfected patients: a systematic review and meta-analysis. PLoS One 2013; 8: e68152.
[42] Rockstroh JR, Bhagani S. Managing HIV/hepa-titis C co-infection in the era of direct acting antivirals. BMC Med 2013; 11: 234.
[43] Qian HZ, Vermund SH, Kaslow RA, Coffey CS, Chamot E, Yang Z, Qiao X, Zhang Y, Shi X, Jiang Y, Shao Y, Wang N. Co-infection with HIV and hepatitis C virus in former plasma/blood do-nors: challenge for patient care in rural China. AIDS 2006; 20: 1429-35.
[44] Bonacini M. Alcohol use among patients with HIV infection. Ann Hepatol 2011; 10: 502-7.