Original Article Imaging findings of bile duct hamartomas ... · Original Article Imaging findings...
9
Int J Clin Exp Med 2015;8(8):13145-13153 www.ijcem.com /ISSN:1940-5901/IJCEM0012001 Original Article Imaging findings of bile duct hamartomas: a case report and literature review Qiu-Sheng Shi 1* , Ling-Xi Xing 1* , Li-Fang Jin 1 , Han Wang 2 , Xiu-Hong Lv 3 , Lian-Fang Du 1 1 Department of Ultrasound, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China; 2 Department of Radiology, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China; 3 Department of Pathology, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China. * Co-first authors. Received June 27, 2015; Accepted August 11, 2015; Epub August 15, 2015; Published August 30, 2015 Abstract: Bile duct hamartomas (BHs), also called von Meyenburg complex (VMC), are benign biliary malformations that originate from disorganization of the small intrahepatic bile ducts. This disorganization is often associated with the abnormal involution of embryonic ductal end plates in the liver. This is clinically significant, as the development of BHs can cause diagnostic confusion with liver metastases and small hepatocellular carcinoma (SHCC). Currently, we report a specific case of BHs and review the literature to better define and diagnose BHs. In the following case, a 37 year-old male bearing a lesion in his liver is presented and undergoes both radiological and pathological diag- nosis. The lesion is preliminarily suspected to be a hepatic hemangioma by examination of conventional ultrasound (US), contrast enhanced ultrasound (CEUS), computerized tomographic scanning (CT) and magnetic resonance imaging (MRI). However, SHCC is suspected by follow-up analysis of US and CEUS, due to the patient’s background history of hepatitis B and growth of the lesion and a tumor-feeding vessel in BHs via CEUS. However, BHs are finally diagnosed by biopsy pathology under the guidance of ultrasound. Therefore, we believe pathology is imperative for correct diagnosis of BHs over other similar diseases when the imaging findings are atypical. Here we report the novel and unique detection of a tumor-feeding vessel, which mimicked SHCC strongly, during the course of CEUS. We also present a comprehensive review of the previous reported radiological examination related to BHs. Keywords: Bile duct hamartomas (BHs), pathology, ultrasound (US), contrast enhanced ultrasound (CEUS), com- puterized tomographic (CT), magnetic resonance imaging (MRI) Introduction Bile duct hamartomas (BHs), also known as von Meyenburg complex (VMC), were initially described by the Swiss pathologist Hanns von Meyenburg [1] in 1918. BHs have been previ- ously described as benign liver malformations resulting from maldevelopment of the ductal end plates, which remain in a persistent dou- ble-layered cylindrical structure similar to the fetal ductal plate [2, 3]. Therefore, pathologi- cally, BHs can be defined by examining dilated intrahepatic bile ductules and the surrounding fibrous stroma [4, 5]. BHs are typically detected during laparotomy or autopsy, and the prevalence of BH formation is age-dependent, varying from 1% in children to 5.6% in adults in a large series of autopsy sam- ples [4, 6, 7]. Macroscopically, BHs can be char- acterized by the visualization of many grayish- whitish or yellow small nodules scattered throughout the liver, either intraparenchymally or subcapsularly [6, 8-10]. BHs may be detect- ed as single or multiple hamartomas, with a diameter ranging from 1 to 15 mm [11]. During diagnosis, its characteristics can mimic that of liver metastases, especially when the patient has previously suffered a primary malignancy [9, 11]. Patients with BHs are usually symptomatic. Jaundice, epigastralgia, and fever can occur. Jaundice, a major symptom, is caused by obstruction of the biliary tract owing to the mucus secreted by biliary papillomas [4, 6, 12].
Transcript of Original Article Imaging findings of bile duct hamartomas ... · Original Article Imaging findings...

Int J Clin Exp Med 2015;8(8):13145-13153www.ijcem.com /ISSN:1940-5901/IJCEM0012001
Original Article Imaging findings of bile duct hamartomas: a case report and literature review
Qiu-Sheng Shi1*, Ling-Xi Xing1*, Li-Fang Jin1, Han Wang2, Xiu-Hong Lv3, Lian-Fang Du1
1Department of Ultrasound, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China; 2Department of Radiology, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China; 3Department of Pathology, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China. *Co-first authors.
Received June 27, 2015; Accepted August 11, 2015; Epub August 15, 2015; Published August 30, 2015
Abstract: Bile duct hamartomas (BHs), also called von Meyenburg complex (VMC), are benign biliary malformations that originate from disorganization of the small intrahepatic bile ducts. This disorganization is often associated with the abnormal involution of embryonic ductal end plates in the liver. This is clinically significant, as the development of BHs can cause diagnostic confusion with liver metastases and small hepatocellular carcinoma (SHCC). Currently, we report a specific case of BHs and review the literature to better define and diagnose BHs. In the following case, a 37 year-old male bearing a lesion in his liver is presented and undergoes both radiological and pathological diag-nosis. The lesion is preliminarily suspected to be a hepatic hemangioma by examination of conventional ultrasound (US), contrast enhanced ultrasound (CEUS), computerized tomographic scanning (CT) and magnetic resonance imaging (MRI). However, SHCC is suspected by follow-up analysis of US and CEUS, due to the patient’s background history of hepatitis B and growth of the lesion and a tumor-feeding vessel in BHs via CEUS. However, BHs are finally diagnosed by biopsy pathology under the guidance of ultrasound. Therefore, we believe pathology is imperative for correct diagnosis of BHs over other similar diseases when the imaging findings are atypical. Here we report the novel and unique detection of a tumor-feeding vessel, which mimicked SHCC strongly, during the course of CEUS. We also present a comprehensive review of the previous reported radiological examination related to BHs.
Keywords: Bile duct hamartomas (BHs), pathology, ultrasound (US), contrast enhanced ultrasound (CEUS), com-puterized tomographic (CT), magnetic resonance imaging (MRI)
Introduction
Bile duct hamartomas (BHs), also known as von Meyenburg complex (VMC), were initially described by the Swiss pathologist Hanns von Meyenburg [1] in 1918. BHs have been previ-ously described as benign liver malformations resulting from maldevelopment of the ductal end plates, which remain in a persistent dou-ble-layered cylindrical structure similar to the fetal ductal plate [2, 3]. Therefore, pathologi-cally, BHs can be defined by examining dilated intrahepatic bile ductules and the surrounding fibrous stroma [4, 5].
BHs are typically detected during laparotomy or autopsy, and the prevalence of BH formation is age-dependent, varying from 1% in children to
5.6% in adults in a large series of autopsy sam-ples [4, 6, 7]. Macroscopically, BHs can be char-acterized by the visualization of many grayish-whitish or yellow small nodules scattered throughout the liver, either intraparenchymally or subcapsularly [6, 8-10]. BHs may be detect-ed as single or multiple hamartomas, with a diameter ranging from 1 to 15 mm [11]. During diagnosis, its characteristics can mimic that of liver metastases, especially when the patient has previously suffered a primary malignancy [9, 11].
Patients with BHs are usually symptomatic. Jaundice, epigastralgia, and fever can occur. Jaundice, a major symptom, is caused by obstruction of the biliary tract owing to the mucus secreted by biliary papillomas [4, 6, 12].

Bile duct hamartomas
13146 Int J Clin Exp Med 2015;8(8):13145-13153
However, these symptoms are nonspecific. A close relationship has been reported to exist between BHs and the following congenital dis-orders: Caroli’s disease, polycystic liver dis-ease, congenital hepatic fibrosis, mesenchymal hamartomas, bile duct atresia and autosomal recessive polycystic kidney disease [5, 8, 13, 14]. While VMC is a benign condition, there is an ongoing debate as to whether BHs have the potential to induce malignant degeneration to cholangiocarcinoma and hepatocellular carci-noma [6, 8, 11, 13-15]. Here, we report a case of VMC diagnosed through several radiological examinations, including ultrasound (US), con-trast-enhance ultrasound (CEUS), computer-ized tomographic scanning (CT) and magnetic resonance imaging (MRI). We present novel results via CEUS that suggest the occurrence of a tumor-feeding vessel. The imaging is enhanced in the arterial phase without early
disappearance in the delay phase in CEUS. Additionally, we believe imaging strategies are not sufficient to achieve a most definitive diag-nosis of BHs in the absence of typical imaging findings.
Case report
Here, we report the occurrence of a hypoechon-ical solid nodule in the right liver lobe detected by B-mode ultrasonography in a 37 year-old male. Our study had been approved by the eth-ics committee of Shanghai First People’s Hospital and the informed consent had been waived. Considering that the patient had a his-tory of Hepatitis B, development of a malignant tumor could not be ruled out. At the initial screening, CT scanning missed the nodule because it was imaged in only one frame, which was reluctantly discovered in a later retrospec-
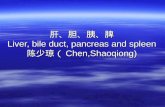
Figure 1. Imaging of patient findings via US and CEUS. (A) At initial examination, a heterogeneous hypoechoic nodule was located in the liver parenchyma via US (red arrow). (B) At initial examination, there was no blood flow in the inte-rior of the nodule (red arrow). (C) The result of a second examination shows a similar heterogeneous nodule located in the liver parenchyma (red arrow). (D) The results of a second examination show sporadic internal blood flow in the interior of the nodule (red arrow). (E-H) At first CEUS examination, enhancement of the hypervascular nodule is earlier than the surrounding liver parenchyma. The arrival time, peak time and regression time of Sonovue® are (E) 12 seconds, (F) 19 seconds and (G) 24 seconds, respectively (red arrows). (H) A tumor-feeding vessel connecting the branch of hepatic artery and the lesion (red arrow). (I-L) At second CEUS examination, enhancement of the hy-pervascular nodule is also earlier than the surrounding liver parenchyma. The arrival time, peak time and regression time of Sonovue® are (I) 10 seconds, (J) 17 seconds, and (K) 24 seconds, respectively. (L) The tumor-feeding vessel is again detected (red arrows).

Bile duct hamartomas
13147 Int J Clin Exp Med 2015;8(8):13145-13153
tive analysis of the CT imaging. Additionally, the patient refused to undergo a MRI examination. CEUS was further implemented, with the pri-mary consideration being liver benign lesion. Six months later, follow-up with US, CEUS and MRI showed that the lesion had slightly increased in size (on US and CEUS) and indi-cated the presence of a tumor-feeding vessel. The MRI findings suggested that the lesion was benign. Because SHCC could not be ruled out on US and CEUS, considering the patient’s his-tory of hepatitis B, a biopsy was indispensable in order to identify the final diagnosis. The patient had suffered right abdominal discom-fort, but did not present with other clinical symptoms such as fever, nausea or vomiting, cough and expectoration, gastrointestinal dys-function, jaundice, hematemesis or melena. Laboratory examination found no abnormal results, including α-FP and other tumor-related index. Next, we present the strategies used for diagnosis:
Conventional ultrasound (US)
The first ultrasound examination was conduct-ed at initial screening. A solid non-homoge-neous hypoechoic lesion was detected in the liver, measuring 8.9×13.6 mm (Figure 1A). This lesion was located in the upper segment of the right anterior hepatic lobe, and was considered a benign lesion due to its clear boundary, regu-lar shape and the missing internal blood flow
(Figure 1B). The ultrasound findings at the six-month follow-up were roughly consistent with that of the first time, with a slightly increased lesion size of 13.5×13.8 mm (Figure 1C). However, we additionally detected an internally sporadic blood flow (Figure 1D), which was initially suggestive of a malignant transforma- tion.
Contrast enhanced ultrasound (CEUS)
During the first examination, a 2.5 ml solution of the microbubble contrast agent Sonovue® was injected into the median cubital vein. Twelve seconds later, the dye began to delin-eate the lesion outline (Figure 1E), and reached peak contrast at 19 seconds (Figure 1F). The contrast lasted 24 seconds and then began to subside (Figure 1G). In the retrospective analy-sis six months later, a tumor-feeding vessel was observed during the contrast enhancement course, which was not detected at first exami-nation of the CEUS data (Figure 1H).
At the six-month follow-up, both the arrival and peak contrast times were two seconds earlier than that of the first examination, 10 seconds (Figure 1I) and 17 seconds (Figure 1J), respec-tively. Similar to the initial screening, imaging started to subside at 24 seconds (Figure 1K). Again, the tumor-feeding vessel was also detected (Figure 1L). By CEUS examination, the lesion demonstrated a slight increase in size,
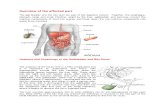
Figure 2. Imaging of patient findings via CT and MRI. (A, B) CECT examination displayed no enhancement in both of hepatic arterial phase and portal venous phase (red arrows). (C-E) Conventinal MRI examination. (C) T1WI, the lesion is hypointense (red arrow). (D) T2WI, the lesion is hyperintense (red arrow). (E) DWI, the lesion shows free diffusion (red arrow). (F-H) Gadolinium-enhanced T1WI. (F) The lesion displays rim enhancement in the hepatic arterial phase, and marginal tuberculiform enhancement in both (G) portal venous phase and (H) hepatic vein (red arrows).

Bile duct hamartomas
13148 Int J Clin Exp Med 2015;8(8):13145-13153
which was an 11×15 mm in measurement, as compared to the initial measurement of 8.9×13.6 mm. CEUS of the nodule displayed an enhancement in the arterial phase, similar to the majority of liver cancers. However, the malignant liver lesions on CEUS typically disap-pear earlier than the surrounding liver paren-chyma in the delay phase, but that trait did not emerge in our patient. Thus, valid conclusions could not be drawn to differentiate BHs and liver metastases via US and CEUS alone. Because of the changes in size and hemody-namics of lesion, a malignant lesion (SHCC or liver metastasis) was initially suspected.
Contrast enhanced computed tomographic (CECT)
To perform CECT, the arterial phase scanning and the porto-venous phase scanning were respectively started at 8 s and 35 s after a bolus of Ultravist 370 was injected. At the initial screening, CT imaging did not recognize the liver nodule as it was detected in only one cross-section. However, the nodule was detect-ed in the following retrospective study of CT imaging by improving the brightness and con-trast. Compared with the surrounding liver parenchyma, the density of the lesion was
slightly lower and non-homogeneous. There was no enhancement in either hepatic arterial phase or in portal venous phase of iohexol-enhanced imaging (Figure 2A, 2B).
Magnetic resonance imaging (MRI)
A MRI examination was performed at the six-month follow-up. A round lesion measuring 15 mm in diameter was found in the upper seg-ment of the right anterior hepatic lobe, with hypo-intense signals on T1-weighted images (T1WI) (Figure 2C), hyper-intense signals on T2-weighted images (T2WI) (Figure 2D), and high diffusion on diffusion-weighted imaging (DWI) (Figure 2E), respectively. After Magnevist was injected intravenously, the lesion was clearly imaged with rim enhancement in the hepatic arterial phase (Figure 2F) of enhanced T1WI, and marginally nodular enhancement was detected in portal venous phase (Figure 2G) and delayed phase (Figure 2H). Therefore, a liver hemangioma was suggested via the MRI results.
Biopsy under ultrasound guidance
Due to inconclusive diagnosis by the imaging studies, a biopsy was performed with a dispos-
Figure 3. Lesion biopsy under ultrasound guidance and pathological examination. (A) The lesion is clearly presented by two-dimensional sonogram. (B) The biopsy needle is inserted into the lesion through the liver parenchyma. (C-F) Pathological examination. (C, D) The lesion displays hyperplasia of the fibrocollagenous stroma and bile ducts ((H) and (E) staining, (C) ×100, (D) ×400). (E, F) The bile duct epithelia is positive for CK (Immunohistochemistry of CK, (E) ×100, (F) ×400).

Bile duct hamartomas
13149 Int J Clin Exp Med 2015;8(8):13145-13153
able core tissue biopsy needle, MN1820, Bard® Magnium®, USA, under the guidance of ultrasound instrument equipped with a punc-ture probe, Hitachi, Japan (Figure 3A, 3B). Three strips of tissue samples measuring 1 cm in diameter and 21 mm in length were obtained. The sample strips were placed on sterilized glass and turned over to prepare smear glass. Next, the strips were dipped in absolute alcohol to fix the specimens for pathological exami- nation.
The resulting pathological sections were reviewed by specialists in hepatobiliary pathol-ogy. It was determined that the morphology and structure of the hepatic cells had no obvious abnormalities. However, the small bile duct cells were in an irregular arrangement sur-rounded by plenty of fibrocollagenous stroma. In addition, the bile duct epithelia were signifi-cantly hyperplastic without cellular heteromor-phism (Figure 3C, 3D). The results of the immu-nohistochemistry demonstrated that cytoke- ratins (CK) CK8, CK18 and CK19 staining were all positive, while hepatocyte staining was neg-ative (Figure 3E, 3F). Due to this staining, the histological origin of the lesion was considered to be bile duct epithelium. Therefore, bile duct hamartoma was finally defined by pathology.
The patients were additionally followed-up both four months and nine months after the biopsy. At these times, the size of the lesion was 13.6×14.9 mm and 13.7×15.7 mm, respective-ly. The nodule increased one to two mm in nine months. Due to the benign results of biopsy before, BHs were considered the correct patho-logic results.
Discussion
As mentioned above, BHs are considered benign liver malformations resulting from derangement of brephic bile duct cells, which is proposed to be triggered by a disruptive or isch-emic factor during bile duct lamina remodeling [8, 13]. These nodules typically measure less than 1 cm on gross observation, strongly simu-lating liver metastases on macroscopical inspection and in imaging studies [9, 10]. Microscopically, BHs consist of a variable num-bers of dilated, tortuous or branching intrahe-atic bile ducts surrounded by monoptychial columnar or cubical bile duct epithelium. The background is composed of abundant fibrocol-
lagenous stroma with little vascular prolifera-tion. Furthermore, the dilated bile ducts may have some bile in their lumina [6, 10].
Two kinds of classification methods for BHs have been mentioned in the literature. Based on the degree of biliary tract dilatation within the lesions, BHs can be divided into three classes: (i) predominantly solid, (ii) predomi-nantly cystic and (iii) intermediate lesions [4, 8, 16, 17]. The connections between the abnor-mal dilated cysts and the draining bile ducts BHs are also divided in two types: (i) draining or (ii) non-draining [8, 18]. However, it is also strongly believed that there is no communica-tion either among the deformed bile ducts or between them and the normal biliary system [19].
Sonographic findings of BHs detect hypoecho-ic, hyperechoic, or mixed non-homogeneous echoic lesions [10, 11, 13, 20, 21]. A specific ultrasonic characteristic of BHs is the so-called “multiple comet-tail echoes” that have been inferred to be strong diagnostic evidence towards BHs [10, 11, 21]. However, this finding was not significant in our case study. Instead, CEUS was used to evaluate the microcircula-tion inside the lesion. Recently, Murphy-Lavallee et al. [11, 22] have suggested a unique phenomenon wherein all metastases display degrees of enhancement in the arterial phase on CEUS, no matter the appearances on con-trast enhanced CT and contrast enhanced MRI [11]. There has been no contrast enhancement reported in most cases of CEUS examination for BHs, but this finding is currently being dis-puted [10, 13]. For example, Berry et al. [11, 23] and Phillip et al. [11] reported cases of mul-tiple BHs that did not demonstrate any enhancement in all three phases of the pro-cess (arterial, portal venous, and delayed phase) via CEUS. On the other hand, Hohmann et al. [11, 24] highlighted the presence of con-trast enhancement on CEUS in a BH measuring 5 mm in size. Imaging of the lesion was syn-chronized and consistent with that of the nor-mal liver parenchyma in arterial phase and por-tal venous phase, and ‘washout’ in the delayed phase [11]. Our results of CEUS roughly agree with the findings of Hohmann et al. The imaging of the lesion displayed enhancement in arterial phase, similar to imaging in liver malignancies. These differences may vary based on lesion

Bile duct hamartomas
13150 Int J Clin Exp Med 2015;8(8):13145-13153
size. Typically, liver malignancies on CEUS show that the lesion disappears earlier than the sur-rounding liver parenchyma in the delay phase. In our case, they are synchronous in portal venous phase and delay phase. Innovatively, we have also found a tumor-feeding vessel dur-ing the course of CEUS, which has never been reported. Thus, valid conclusions cannot be drawn between imaging differences in BH and liver malignancies.
BH lesions are always low-density on CT scan-ning images. In the published literature, no enhancement of BHs has been captured in all phases of CECT after intravenous injection of iodine contrast medium [13], as in our case. However, exceptions exist in two cases [13, 25] in which the imaging of lesions was homoge-neously enhanced on post-contrast imaging of CECT.
The typical imaging features of BHs on MRI are hypo signal on T1WI and hyper signal on T2WI [11, 19]. However, controversy exists when con-sidering enhancement of gadolinium-enhanced T1WI [11]. Both enhancement [13, 18, 21, 26, 27] and non-enhancement [11, 13] have been reported. In our case, rim enhancement was detected in the hepatic arterial phase, and marginal tuberculiform enhancement was detected in both the portal venous phase and the delayed phase of enhanced T1WI. This was speculated to be resulting from the compressed liver parenchyma surrounding the lesion and inflammatory cell infiltration [21, 27]. As a promising part of MRI, diffusion-weighted imag-ing (DWI) has attracted a lot of attention in dif-ferentiating benign lesions from malignant lesions, due to diffusion rate. It is thought that benign lesions display free diffusion on DWI, while malignant lesions show restricted diffu-sion [11]. According to this theory, the lesion in our case could be inferred to be benign. Additionally, it has been suggested that the false negative rate of CT and MRI remains high for liver metastasis less than 1.5 cm in size, which may also explain the discrepancies in the T2W1 enhancement. This size coincides with the vast majority of BHs, so the differential diagnosis would be difficult and may vary with lesion size [28].
Magnetic resonance cholangiopancreatogra-phy (MRCP) imaging has the ability to identify the communication between BHs and the nor-
mal biliary system, also known as the ‘starry sky’ phenomenon. The dilated bile ducts of BHs are hyper intense isolated nodules scattered in both of the liver lobes, and may or may not com-municate with the draining bile ducts [6, 10, 13, 21, 27, 28]. MRCP can facilitatefacilitate the differential diagnosis of BHs and other bile duct anomalies such as Caroli disease by ana-lyzing the association with the draining bile ducts [13]. However, based on whether there are connections between the abnormal dilated cysts and the draining bile ducts, some believe that BHs can be divided in two types, existence or absence of the communication [8, 13].
The most important differential diagnosis of BHs would be to rule out liver metastases, which would interfere with different treatment strategies [29], especially when the patient has a history of malignancy [2, 28]. Other similar diseases include primary hepatocellular carci-noma, intrahepatic cholangiocarcinoma and circumscribed inhomogeneous fatty liver [2, 28], simple hepatic cyst, small liver abscess, and lymphoma. To our knowledge, CEUS of BHs has been reported in few papers, and the accu-racy of CEUS in the diagnosis of BHs has not been reported. CT helps slightly in differentiat-ing BHs from liver metastasis but has poor tis-sue contrast resolution [21]. Comparatively, if accompanied with typical imaging, MRI may be of the greatest value in the differential diagno-sis of BHs and liver metastasis, although it remains controversial, as described above. In addition, the dilated bile ducts of BHs can dis-play the characteristic “starry sky” appearance in some cases on MRCP [6, 10, 13, 21]. We believe that pathological examination is required in those lesions with atypical radiologi-cal performance, such as solitary lesions or enhanced post-gadolinium during MRI [21], as in our case.
BHs may also be confused with peribiliary gland hamartoma (PGH), also known as intrahepatic bile duct adenoma, originating from peribiliary glands. Microscopic examination of PGH reveals disordered peribiliary gland acini embedded in fibrotic tissue which causes chronic inflammation [8, 30]. Microscopical examination of BHs shows small irregular and dilated bile ducts embedded in fibrocollage-nous stroma without inflammation [8, 10, 31, 32]. Part of the dilated bile ducts turn into small

Bile duct hamartomas
13151 Int J Clin Exp Med 2015;8(8):13145-13153
cysts and maybe contain inspissated bile in them [8, 30, 33]. However, it is difficult to dis-tinguish BHs from PGH by macroscopical exam-ination or imaging methods. The only difference is that PGH has been considered to have delayed or prolonged enhancement on contrast enhanced CT and MRI [8]. The most precise identifying method to distinguish BH and PGH should be immunohistochemistry. The serous and mucous cells comprised in acini and tubules of PGH express D10 and 1F6, which are also secreted by the intrahepatic peribiliary glands [30, 34, 35]. Another related investiga-tion demonstrates that PGH can be marked specifically by five foregut antigens (D10, 1F6, MUC6, MUC5AC, and TFF2) as well as the exo-crinosity of acid mucin [35]. Therefore, imaging examination may help somewhat in indicating the most likely differential diagnosis of BHs and PGH, with the final diagnosis depending on pathology.
Conclusion
BHs are benign liver malformations, with an extremely low probability of malignant transfor-mation. Recently, they have attracted a lot of attention because they simulate the perfor-mance of liver metastasis on gross observation and imaging examination. As mentioned, it is difficult with imaging studies alone to differenti-ate BH from similar disease. However, when imaging, we believe MRI is most important for differential diagnosis. Pathological examina-tion is necessary when a history of primary malignancy exists or the patient has atypical appearance on radiological images. In addition, we present diagnosis of BHs from a small lesion in the liver of a young patient with hepatitis. We also present a novel association between BHs and tumor-feeding vessels that has never been reported, potentially creating a new link between benign lesions and tumor vasculature. Of course, we cannot rule out that our case may be an individual phenomenon.
Acknowledgements
This project was carried out with financial sup-port from the National Natural Science Foundation of China (Grant Nos. 30332369/H1205 and 81171352/H1805) and the Science and Technology Support Projects of the Science and Technology Commission of Shanghai (Grant No. 124119a5300).
Disclosure of conflict of interest
None.
Abbreviations
BHs, Bile duct hamartomas; VMC, Von Meyen- burg complex; US, Ultrasound; CEUS, Contrast enhanced ultrasound; CT, Computerized tomo-graphic scanning; MRI, Magnetic resonance imaging; T1WI, T1-weighted images; 2WI, T2-weighted images; DWI, Diffusion-weighted imaging; CK, Cytokeratin; MRCP, Magnetic res-onance cholangiopancreatography; PGH, Peribiliary gland hamartoma.
Address correspondence to: Dr. Lian-Fang Du, Department of Ultrasound, Shanghai First People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, 85 Wu Jin Road, Shanghai 200080, China. Tel: +86-13386259562; Fax: (0086) 021-37798276; E-mail: du_lianfang2013@ 163.com
References
[1] H vM. Über die Zyztenleber. Beitr Pathol Anatom 1918; 64: 47-532.
[2] Michalakis K, Coppack SW and Koak Y. Von Meyenburg complex in a bariatric patient. J Gastrointestin Liver Dis 2011; 20: 120.
[3] Terada T and Moriki T. Monolobar ductal plate malformation disease of the liver. Pathol Int 2010; 60: 407-412.
[4] Karahan OI, Kahriman G, Soyuer I and Ok E. Hepatic von Meyenburg complex simulating biliary cystadenocarcinoma. Clin Imaging 2007; 31: 50-53.
[5] Hettinger M, Klotz M, Bolay L and Weber P. [Multiple bile duct hamartomas of the liver--a rare differential diagnosis to liver metastasis]. Ultraschall Med 2005; 26: 150-153.
[6] van Vlerken LG, van Leeuwen MS, Schipper ME and van Erpecum KJ. The “Von Meyenburg complex”: an unusual cause of cholangitis? Clin Res Hepatol Gastroenterol 2011; 35: 762-764.
[7] Redston MS and Wanless IR. The hepatic von Meyenburg complex: prevalence and associa-tion with hepatic and renal cysts among 2843 autopsies [corrected]. Mod Pathol 1996; 9: 233-237.
[8] Ioannidis O, Iordanidis F, Paraskevas G, Ntoumpara M, Tsigkriki L, Chatzopoulos S, Ko-tronis A, Papadimitriou N, Konstantara A, Makrantonakis A, Sakkas A and Kakoutis E. Incidentally discovered white subcupsular liver nodules during laparoscopic surgery: biliary

Bile duct hamartomas
13152 Int J Clin Exp Med 2015;8(8):13145-13153
hamartoma and peribiliary gland hamartoma. Klin Onkol 2012; 25: 468-470.
[9] van Baardewijk LJ, Idenburg FJ, Clahsen PC and Mollers MJ. [Von Meyenburg complexes in the liver: not metastases]. Ned Tijdschr Ge-neeskd 2010; 154: A1674.
[10] Zheng RQ, Zhang B, Kudo M, Onda H and In-oue T. Imaging findings of biliary hamartomas. World J Gastroenterol 2005; 11: 6354-6359.
[11] Lung PF, Jaffer OS, Akbar N, Sidhu PS and Ryan SM. Appearances of von meyenburg complex on cross sectional imaging. J Clin Im-aging Sci 2013; 3: 22.
[12] Aoki S, Okayama Y, Kitajima Y, Hayashi K, Imai H, Okamoto T, Akita S, Gotoh K, Ohara H, No-mura T, Joh T, Yokoyama Y and Itoh M. Intrahe-patic biliary papilloma morphologically similar to biliary cystadenoma. J Gastroenterol Hepa-tol 2005; 20: 321-324.
[13] Mortele B, Mortele K, Seynaeve P, Vandevelde D, Kunnen M and Ros PR. Hepatic bile duct hamartomas (von Meyenburg Complexes): MR and MR cholangiography findings. J Comput Assist Tomogr 2002; 26: 438-443.
[14] Nasr D, Bidot ML, Roche M, Paveliu S, Morel P, Naouri A, Odet E, Esquis P, Pilleul F and Ber-nard P. [Von Meyenburg disease found during laparoscopic surgery: report of two cases]. Ann Chir 2006; 131: 468-470.
[15] Kanematsu M, Kondo H, Semelka RC, Matsuo M, Goshima S, Hoshi H, Moriyama N and Itai Y. Early-enhancing non-neoplastic lesions on gadolinium-enhanced MRI of the liver. Clin Ra-diol 2003; 58: 778-786.
[16] Alvarez Posadilla M, Linares Torres P, Jorquera Plaza F, Rueda Castanon R, Gonzalez de Fran-cisco T and Olcoz Goni JL. [Importance of mag-netic resonance imaging in the diagnosis of multiple small biliary hamartomas (von Meyen-burg complexes)]. Gastroenterol Hepatol 2006; 29: 378-379.
[17] Federle MP and VS A. Hepatobiliary and pan-creas. Abdomen. Diagnostic imaging. Edited by Federle MP. Amirsys Inc: 2004. pp. 1-114.
[18] Wohlgemuth WA, Bottger J and Bohndorf K. MRI, CT, US and ERCP in the evaluation of bile duct hamartomas (von Meyenburg complex): a case report. Eur Radiol 1998; 8: 1623-1626.
[19] Lin S, Weng Z, Xu J, Wang MF, Zhu YY and Jiang JJ. A study of multiple biliary hamartomas based on 1697 liver biopsies. Eur J Gastroen-terol Hepatol 2013; 25: 948-952.
[20] Xu AM, Xian ZH, Zhang SH and Chen XF. Intra-hepatic cholangiocarcinoma arising in multiple bile duct hamartomas: report of two cases and review of the literature. Eur J Gastroenterol Hepatol 2009; 21: 580-584.
[21] Shin YM. Biliary hamartoma presented as a single mass. Korean J Hepatol 2011; 17: 331-334.
[22] Murphy-Lavallee J, Jang HJ, Kim TK, Burns PN and Wilson SR. Are metastases really hypovas-cular in the arterial phase? The perspective based on contrast-enhanced ultrasonography. J Ultrasound Med 2007; 26: 1545-1556.
[23] Berry JD, Boxer ME, Rashid HI and PS S. Case report: Microbubble contrast-enhanced ultra-sound characteristics of multiple biliary ham-artomas (von Meyenberg complexes). Ultra-sound 2004; 12: 95-97.
[24] Hohmann J, Loddenkemper C and Albrecht T. Assessment of a biliary hamartoma with con-trast-enhanced sonography using two different contrast agents. Ultraschall Med 2009; 30: 185-188.
[25] An C, Park S and Choi YJ. Diffusion-weighted MRI in intrahepatic bile duct adenoma arising from the cirrhotic liver. Korean J Radiol 2013; 14: 769-775.
[26] Gong J, Kang W and Xu J. MR imaging and MR Cholangiopancreatography of multiple biliary hamartomas. Quant Imaging Med Surg 2012; 2: 133-134.
[27] Semelka RC, Hussain SM, Marcos HB and Woosley JT. Biliary hamartomas: solitary and multiple lesions shown on current MR tech-niques including gadolinium enhancement. J Magn Reson Imaging 1999; 10: 196-201.
[28] Nagano Y, Matsuo K, Gorai K, Sugimori K, Kunisaki C, Ike H, Tanaka K, Imada T and Shi-mada H. Bile duct hamartomas (von Mayen-burg complexes) mimicking liver metastases from bile duct cancer: MRC findings. World J Gastroenterol 2006; 12: 1321-1323.
[29] Mimatsu K, Oida T, Kawasaki A, Aramaki O, Ku-boi Y, Katsura Y and Amano S. Preoperatively undetected solitary bile duct hamartoma (von Meyenburg complex) associated with esopha-geal carcinoma. Int J Clin Oncol 2008; 13: 365-368.
[30] Kim YS, Rha SE, Oh SN, Jung SE, Shin YR, Choi BG, Byun JY, Jung ES and Kim DG. Imaging findings of intrahepatic bile duct adenoma (peribiliary gland hamartoma): a case report and literature review. Korean J Radiol 2010; 11: 560-565.
[31] Tohme-Noun C, Cazals D, Noun R, Menassa L, Valla D and Vilgrain V. Multiple biliary hamarto-mas: magnetic resonance features with histo-pathologic correlation. Eur Radiol 2008; 18: 493-499.
[32] Liu CH, Yen RF, Liu KL, Jeng YM, Pan MH and Yang PM. Biliary hamartomas with delayed 99mTc-diisopropyl iminodiacetic acid clear-ance. J Gastroenterol 2005; 40: 540-544.
[33] Christine AL and ME. Gastrointestinal and Liv-er Pathology. In: Christine AL, Elizabeth M, edi-tiors. Philadelphia: Churchill Livingstone; 2005. pp. 600-602.

Bile duct hamartomas
13153 Int J Clin Exp Med 2015;8(8):13145-13153
[34] Bhathal PS, Hughes NR and Goodman ZD. The so-called bile duct adenoma is a peribiliary gland hamartoma. Am J Surg Pathol 1996; 20: 858-864.
[35] Hughes NR, Goodman ZD and Bhathal PS. An immunohistochemical profile of the so-called bile duct adenoma: clues to pathogenesis. Am J Surg Pathol 2010; 34: 1312-1318.