Oncology Registrars’ Forum - Royal College of … · Royal College of Radiologists & the Oncology...
32
1 Oncology Registrars’ Forum Trainee Survey 2011 Comprehensive Report October 2011 Report prepared by: Dr Nick MacLeod, ORF Chair & Representative for the West of Scotland Dr Esme Hill, ORF Vice-Chair & Representative for Oxford Dr Ruth Davis, ORF Representative for Wessex Dr Susan Masson, ORF Representative for Severn Dr Alison Tree, ORF Representative for the Less than Full-Time Trainees Anna Campbell, ORF Secretariat, Royal College of Radiologists Royal College of Radiologists 38 Portland Place London W1B 1JQ Tel: 020 7299 1134 Fax: 020 7631 4257 Email: [email protected] Web: www.rcr.ac.uk
-
Upload
nguyenkhanh -
Category
Documents
-
view
234 -
download
0
Transcript of Oncology Registrars’ Forum - Royal College of … · Royal College of Radiologists & the Oncology...

1
Oncology Registrars’ Forum Trainee Survey 2011
Comprehensive Report October 2011
Report prepared by: Dr Nick MacLeod, ORF Chair & Representative for the West of Scotland Dr Esme Hill, ORF Vice-Chair & Representative for Oxford Dr Ruth Davis, ORF Representative for Wessex Dr Susan Masson, ORF Representative for Severn Dr Alison Tree, ORF Representative for the Less than Full-Time Trainees Anna Campbell, ORF Secretariat, Royal College of Radiologists Royal College of Radiologists 38 Portland Place London W1B 1JQ Tel: 020 7299 1134 Fax: 020 7631 4257 Email: [email protected] Web: www.rcr.ac.uk

2
Contents Page Number
Introduction 3 Development of the survey 3 Participants 3 Procedure 3 Response rates 3
Results
1. Education 4-10 1.1 Structured teaching 4 1.2 Practical education 7 1.3 Access to learning resources 10
2. Examinations 11-12 2.1 First FRCR Examination 11 2.2 Final FRCR Examination 11
3. Training Programmes & Assessment Practices 13-16 3.1 Training programmes and educational support 13 3.2 Assessment and appraisal 13 3.3 Audit 15 3.4 Study leave 15 3.5 Additional qualifications 16
4. Regional Clinical Oncology Service Commitments 17-23 4.1 Management of oncology in-patients 18 4.2 Acute Oncology 19 4.3 On-call commitments 20 4.4 Hospital at Night 20 4.5 Service vs. training 22
5. Research, Out of Programme Activities 24-27 5.1 Who is out of programme and what they are doing 24 5.2 When is OOPE being undertaken 24 5.3 Funding and financial considerations 25 5.4 Academic career intentions 25 5.5 Benefits of time spent out of programme in research 25 5.6 Respondents not currently out of programme 26 5.7 General points regarding research and out of programme activities 26 5.8 Response to open questions 26
6. Royal College of Radiologists & the Oncology Registrars’ Forum 28 7. Career, Work/Life Balance & Less than Full-Time Training 29-30 7.1 The future 29 7.2 Recruitment 29 7.3 Less than full-time training 29 7.4 Leaving oncology 30 7.5 Work/life balance and morale 30
8. Demographics 31
9. Conclusion 31
Appendix List of Tables and Charts 32
3
Introduction This report summarises the results of an on-line survey carried out by the Oncology Registrars‟ Forum (ORF) in April and May 2011. As with the similar survey carried out in 2009, it aimed to assess trainees‟ views on every aspect of their training, including educational experience, service provision versus training, out of programme activities, the FRCR Examinations and work/life balance. Development of survey The survey questions were designed by a small team of ORF members, based significantly on questions used in the 2009 survey. The survey comprised eight sections covering educational experience, examinations, training programmes and assessment, regional service commitments, research and out of programme activities, the College and ORF, and career and work/life balance. In addition, demographic information was collected, allowing data to be analysed by region, year of training, age and gender. There was a selection of free text (open) questions in every section, allowing respondents to comment on every aspect of their training. Participants Invitations to participate in the survey were emailed to all clinical oncology trainees who are current members of the Royal College of Radiologists. Respondents were split along gender lines 58% to 42% female to male which reflects the overall gender split of current trainees. 82% of respondents were between 30 and 40 years old. 32% of respondents identified themselves as post-FRCR, 38% were between First and Final FRCR and the remaining 30% were pre-FRCR. Procedure Surveys were completed between 1 April 2011 and 10 May 2011, with trainees being sent a link to the survey in an email. The survey software allocated each trainee‟s email address a unique identifier allowing the software to send out reminders to those who had not responded. Using this process meant that the trainees participated on a confidential, anonymised basis. Response rates The survey was sent to 375 trainees. 268 were returned, giving an overall response rate of 71.5%, a significant increase on the 2009 Survey (52%). Response rates by deanery were also calculated and are as summarised below.
Deanery Response rate %
Deanery Response rate %
East of England 73.3 North of Scotland 100.0
East Midlands 90.5 East of Scotland 50.0
London & KSS 55.4 South East Scotland 88.9
Mersey 75.0 West of Scotland 86.7
North Western 72.7
Northern 81.8 Northern Ireland 61.5
Oxford 62.5
South West Peninsula 75.0 Wales 83.3
Severn 66.7
Wessex 100.0
West Midlands 91.3
Yorks & Humber 83.9
4
1. Education
1.1 Structured Teaching Trainees were asked a variety of questions related to the formal teaching that they receive in their
departments. Views were sought as to the general standard of teaching from different staff groups, who was responsible for the organisation of teaching and whether such teaching was „bleep free‟. The survey ascertained how many hours of teaching trainees are receiving each week. In addition, information was specifically sought about radiology teaching, as a good understanding of cross sectional imaging is essential for the modern, practising clinical oncologist.
Structured teaching within departments usually consists of didactic teaching, case-based discussions
and journal club. Time allocated for teaching ranges from an entire morning or afternoon per week for structured teaching in some departments, in addition to supporting attendance at an all day Year 1 or Year 2 FRCR course, whilst some slot in teaching sessions as breakfast meetings prior to the normal working day.
Quality and Organisation 45% of respondents rated the standard of consultant-led teaching in their departments as good or
excellent, with another 35.7% rating this as satisfactory which is an improvement on the 2009 figures. However, as in 2009, 7% of respondents stated that consultant led teaching was sought but rarely provided, and 11.5% stated that it was unsatisfactory. Similar figures were stated for registrar-led teaching and teaching by other professions, e.g. physicists.
The organisation of teaching is the responsibility of consultants in 20% of departments, whereas in
34% this is the responsibility of one or more registrars. In the remaining 45% the organisation of teaching is a joint responsibility between registrars and consultants.
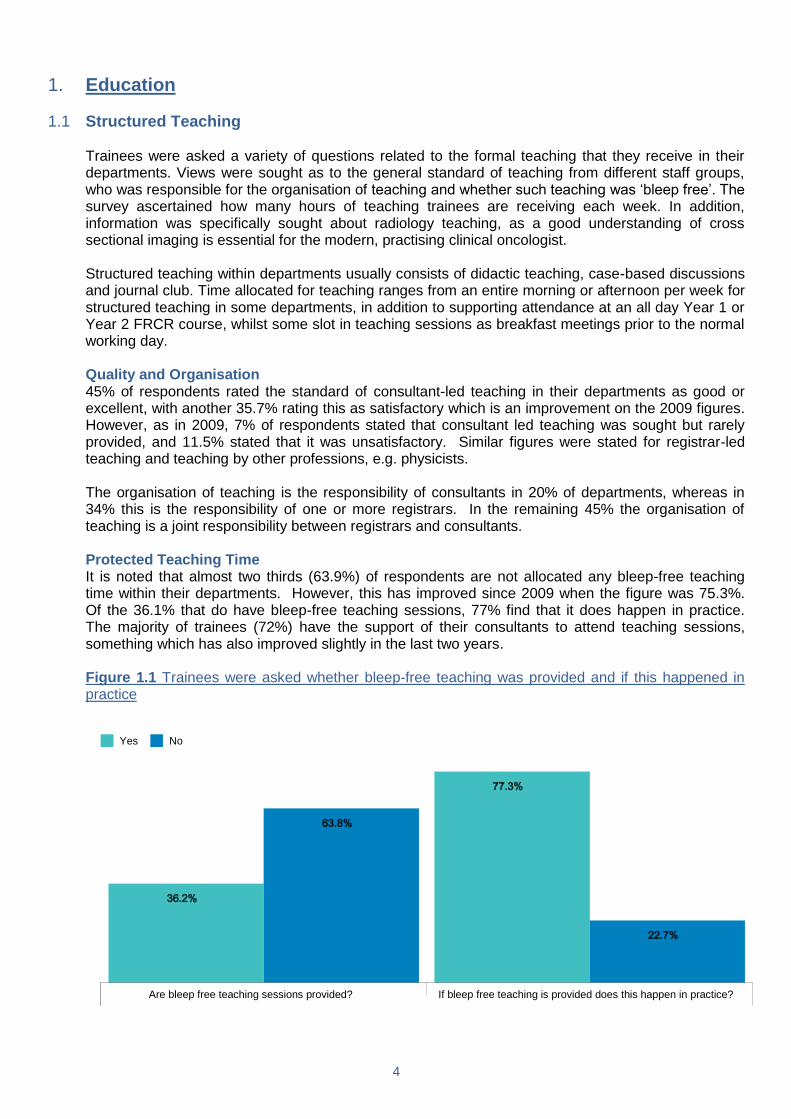
Protected Teaching Time It is noted that almost two thirds (63.9%) of respondents are not allocated any bleep-free teaching
time within their departments. However, this has improved since 2009 when the figure was 75.3%. Of the 36.1% that do have bleep-free teaching sessions, 77% find that it does happen in practice. The majority of trainees (72%) have the support of their consultants to attend teaching sessions, something which has also improved slightly in the last two years.
Figure 1.1 Trainees were asked whether bleep-free teaching was provided and if this happened in
practice
Are bleep free teaching sessions provided? If bleep free teaching is provided does this happen in practice?
63.8%
22.7%
36.2%
77.3%
Yes No
5
Figure 1.2 Trainees were asked whether their supervisors ensured that they could attend teaching sessions
27.6%
72.4%
Yes
No
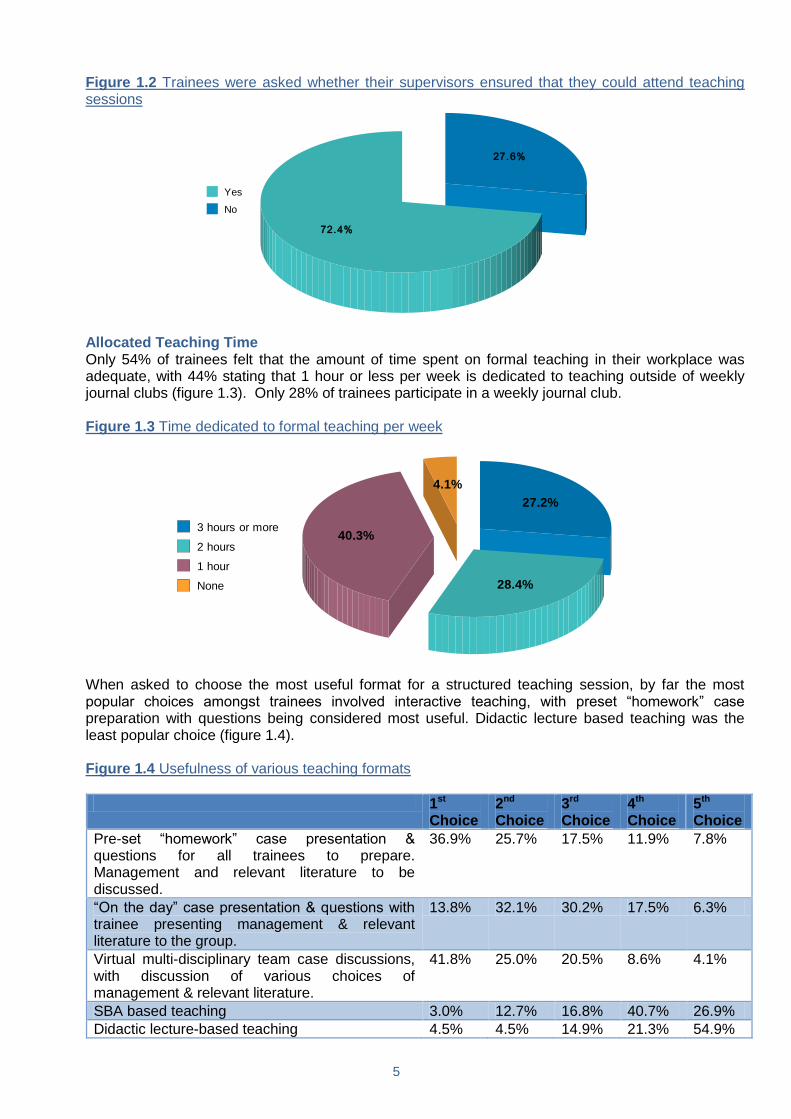
Allocated Teaching Time Only 54% of trainees felt that the amount of time spent on formal teaching in their workplace was
adequate, with 44% stating that 1 hour or less per week is dedicated to teaching outside of weekly journal clubs (figure 1.3). Only 28% of trainees participate in a weekly journal club.
Figure 1.3 Time dedicated to formal teaching per week
27.2%
28.4%
40.3%
4.1%
3 hours or more
2 hours
1 hour
None
When asked to choose the most useful format for a structured teaching session, by far the most
popular choices amongst trainees involved interactive teaching, with preset “homework” case preparation with questions being considered most useful. Didactic lecture based teaching was the least popular choice (figure 1.4).
Figure 1.4 Usefulness of various teaching formats
1st Choice
2nd Choice
3rd Choice
4th Choice
5th Choice
Pre-set “homework” case presentation & questions for all trainees to prepare. Management and relevant literature to be discussed.
36.9% 25.7% 17.5% 11.9% 7.8%
“On the day” case presentation & questions with trainee presenting management & relevant literature to the group.
13.8% 32.1% 30.2% 17.5% 6.3%
Virtual multi-disciplinary team case discussions, with discussion of various choices of management & relevant literature.
41.8% 25.0% 20.5% 8.6% 4.1%
SBA based teaching 3.0% 12.7% 16.8% 40.7% 26.9%
Didactic lecture-based teaching 4.5% 4.5% 14.9% 21.3% 54.9%
6
Aside from time specifically set aside for teaching, just over two thirds of trainees felt that they spent enough time discussing educational cases with their supervising consultants. Although 34% did not, it is hoped however that with the rotational nature of training posts this percentage does not continuously represent the same group of trainees.
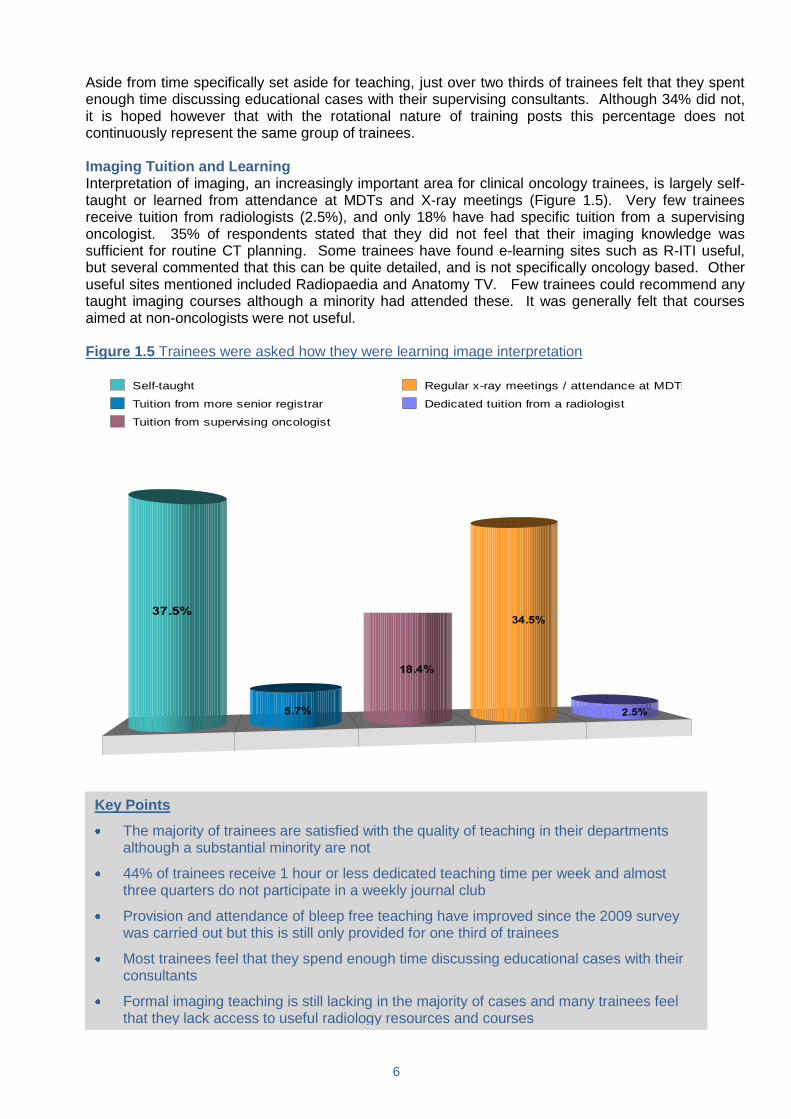
Imaging Tuition and Learning Interpretation of imaging, an increasingly important area for clinical oncology trainees, is largely self-
taught or learned from attendance at MDTs and X-ray meetings (Figure 1.5). Very few trainees receive tuition from radiologists (2.5%), and only 18% have had specific tuition from a supervising oncologist. 35% of respondents stated that they did not feel that their imaging knowledge was sufficient for routine CT planning. Some trainees have found e-learning sites such as R-ITI useful, but several commented that this can be quite detailed, and is not specifically oncology based. Other useful sites mentioned included Radiopaedia and Anatomy TV. Few trainees could recommend any taught imaging courses although a minority had attended these. It was generally felt that courses aimed at non-oncologists were not useful.
Figure 1.5 Trainees were asked how they were learning image interpretation
Self-taught
Tuition from more senior registrar
Tuition from supervising oncologist
Regular x-ray meetings / attendance at MDTs
Dedicated tuition from a radiologist
Key Points
The majority of trainees are satisfied with the quality of teaching in their departments although a substantial minority are not
44% of trainees receive 1 hour or less dedicated teaching time per week and almost three quarters do not participate in a weekly journal club
Provision and attendance of bleep free teaching have improved since the 2009 survey was carried out but this is still only provided for one third of trainees
Most trainees feel that they spend enough time discussing educational cases with their consultants
Formal imaging teaching is still lacking in the majority of cases and many trainees feel that they lack access to useful radiology resources and courses
7
1.2 Practical Education
In this section, trainees were asked a number of questions about the quality of the practical education
that they received. More in depth questions were posed on training in systemic therapy and, in particular, radiotherapy training.
Quality of Educational Experience Not surprisingly, trainees have a wide range of perceptions about the quality of training available in
their workplace (Figure 1.6). Most trainees consider that training received in the outpatient and inpatient settings and in multidisciplinary meetings is at least satisfactory, although only a small minority consider this practical training to be excellent. The small number of trainees whose experiences in this area were rated as „poor‟ or „very poor‟ gave reasons for this, including time pressures, emphasis on service provision and lack of consultant supervision. A number of trainees stated that they are not encouraged to participate in MDTs which are often dominated by a small number of consultants and are very time pressured, leaving little time for educational discussion.
Figure 1.6 Trainees were asked to rate the quality of their practical experience
Very Poor Poor Average Good Excellent
Outpatient clinics 0.7% 5.6% 31.0% 50.7% 11.9%
Inpatient management 1.1% 8.6% 45.9% 38.8% 5.6%
Active participation in multidisciplinary meetings
1.9% 9.7% 44.0% 39.6% 4.9%
Active participation in radiotherapy planning meetings
8.2% 13.8% 38.1% 34.3% 5.6%
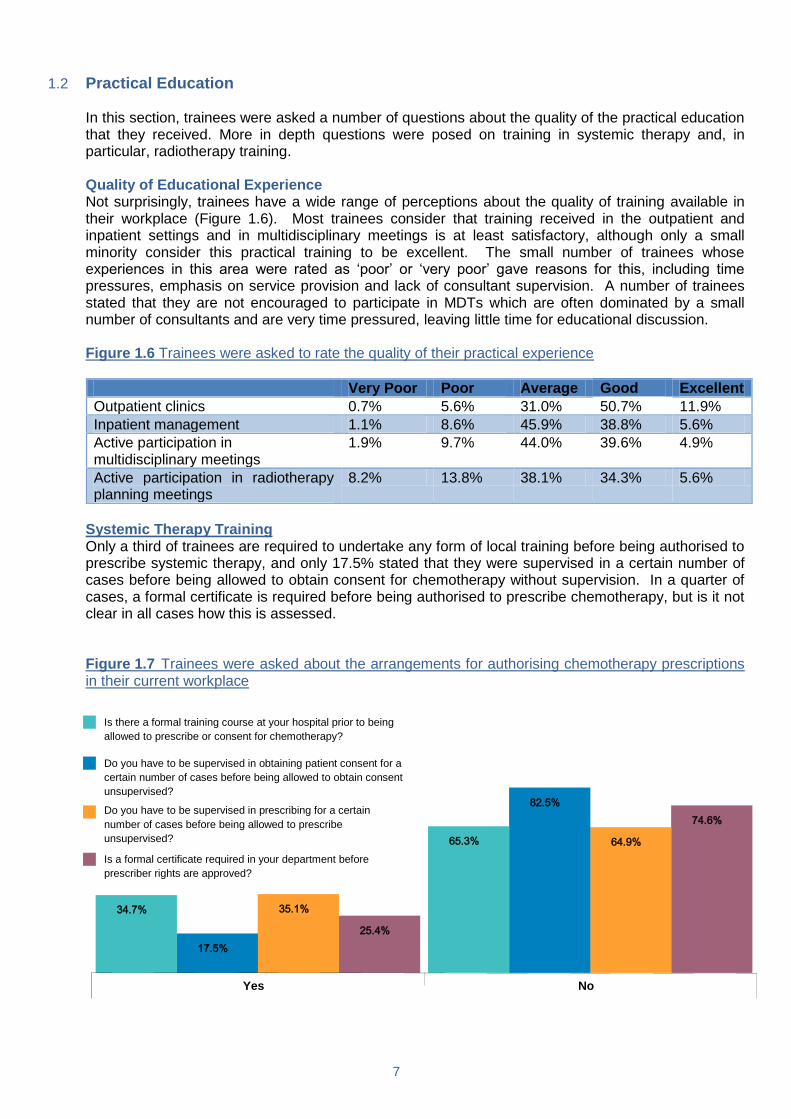
Systemic Therapy Training Only a third of trainees are required to undertake any form of local training before being authorised to
prescribe systemic therapy, and only 17.5% stated that they were supervised in a certain number of cases before being allowed to obtain consent for chemotherapy without supervision. In a quarter of cases, a formal certificate is required before being authorised to prescribe chemotherapy, but is it not clear in all cases how this is assessed.
Figure 1.7 Trainees were asked about the arrangements for authorising chemotherapy prescriptions
in their current workplace
Yes No
74.6%
25.4%
64.9%
35.1%
17.5%
82.5%
34.7%
65.3%
Is there a formal training course at your hospital prior to being
allowed to prescribe or consent for chemotherapy?
Do you have to be supervised in obtaining patient consent for a
certain number of cases before being allowed to obtain consent
unsupervised?
Do you have to be supervised in prescribing for a certain
number of cases before being allowed to prescribe
unsupervised?
Is a formal certificate required in your department before
prescriber rights are approved?
8
However, the vast majority of respondents (96%) considered that they were provided with an appropriate level of supervision in deciding whether patients were fit to receive chemotherapy, and a similar proportion felt that their current posts provided sufficient experience in systemic therapy practice. Similarly, 95% felt that they were appropriately supervised in initiation of new systemic therapy prescriptions. 80% of trainees had access to clear guidelines on selection of chemotherapy by tumour site and 72.5% were aware of departmental guidelines for the management of treatment related toxicities.
These results are very similar to those reported by the 2009 ORF survey, reflecting little change in
practice over time. Radiotherapy Training Overall, a substantial proportion of trainees felt that outpatient work (43%), inpatient work (42%) or
administrative work (42%) interrupt radiotherapy planning time on a weekly basis. Only 20% considered their radiotherapy planning sessions to be protected time (only interrupted in cases of emergencies that require immediate attention). 21% of trainees carried out the majority of their radiotherapy planning outside the hours of 9am-5pm.
Free text comments from trainees suggest that radiotherapy planning time is very often the first area
to suffer when the burden of service commitment increases. In some cases trainees indicated that they had no dedicated radiotherapy planning time at all in their weekly timetable, even when trainees currently in medical oncology rotational posts were excluded. In contrast however, some comments from trainees reflected very positive experiences, referring to excellent training, supervision and feedback from consultants and protected sessions for planning.
Radiotherapy Planning Meetings 63.2% of trainees believed that radiotherapy planning meetings would be a useful exercise; 72% of
trainees agreed that such meetings have educational value, and two thirds stated that these meetings help preparation for the Final FRCR Examination. However, only half of trainees had ever participated in radiotherapy planning meetings. Most frequently, where these occur, they are attended by medical staff, and less frequently by other staff such as planning/treatment radiographers or physicists. Comments from trainees suggested that the most useful formats involve senior clinicians and/or the physicists and radiographers reviewing trainees‟ plans and discussion of how each case is planned, with reasons.
65% of respondents were authorised to prescribe palliative radiotherapy and 29% to prescribe radical
radiotherapy. Levels of supervision were considered to be good; over 98% of trainees considered that they are adequately supervised in radiotherapy prescribing for their level of training. A few trainees (less than 20%) are required to obtain a local certificate to prescribe radiotherapy; generally the attainment of the First and Final FRCR Examinations permit independent prescriptions of palliative and radical radiotherapy, respectively. Most trainees felt that their consultants provided constructive feedback on their radiotherapy plans, but in 25% of cases trainees‟ were not present when the supervising consultant reviewed their plans.
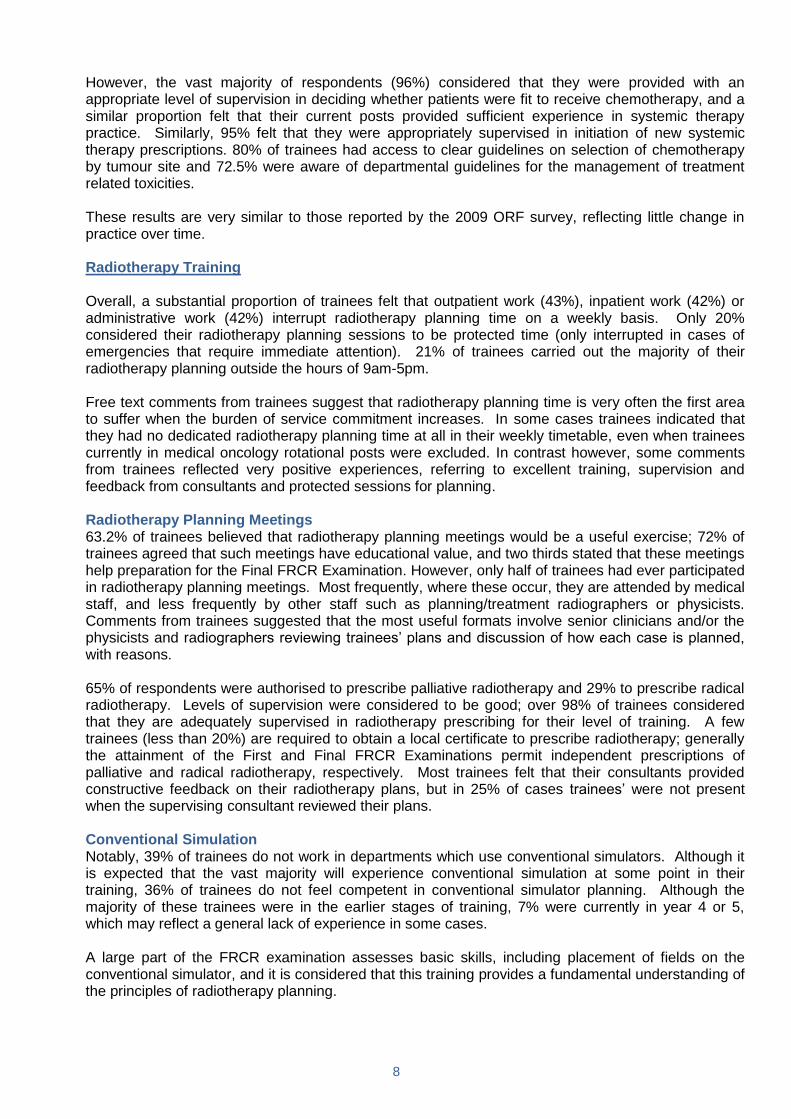
Conventional Simulation Notably, 39% of trainees do not work in departments which use conventional simulators. Although it
is expected that the vast majority will experience conventional simulation at some point in their training, 36% of trainees do not feel competent in conventional simulator planning. Although the majority of these trainees were in the earlier stages of training, 7% were currently in year 4 or 5, which may reflect a general lack of experience in some cases.
A large part of the FRCR examination assesses basic skills, including placement of fields on the
conventional simulator, and it is considered that this training provides a fundamental understanding of the principles of radiotherapy planning.
9
Figure 1.8 Trainees were asked whether they felt competent in conventional simulator planning
7.4%
57.1%
30.1%
5.5%
Strongly agree
Agree
Disagree
Strongly disagree
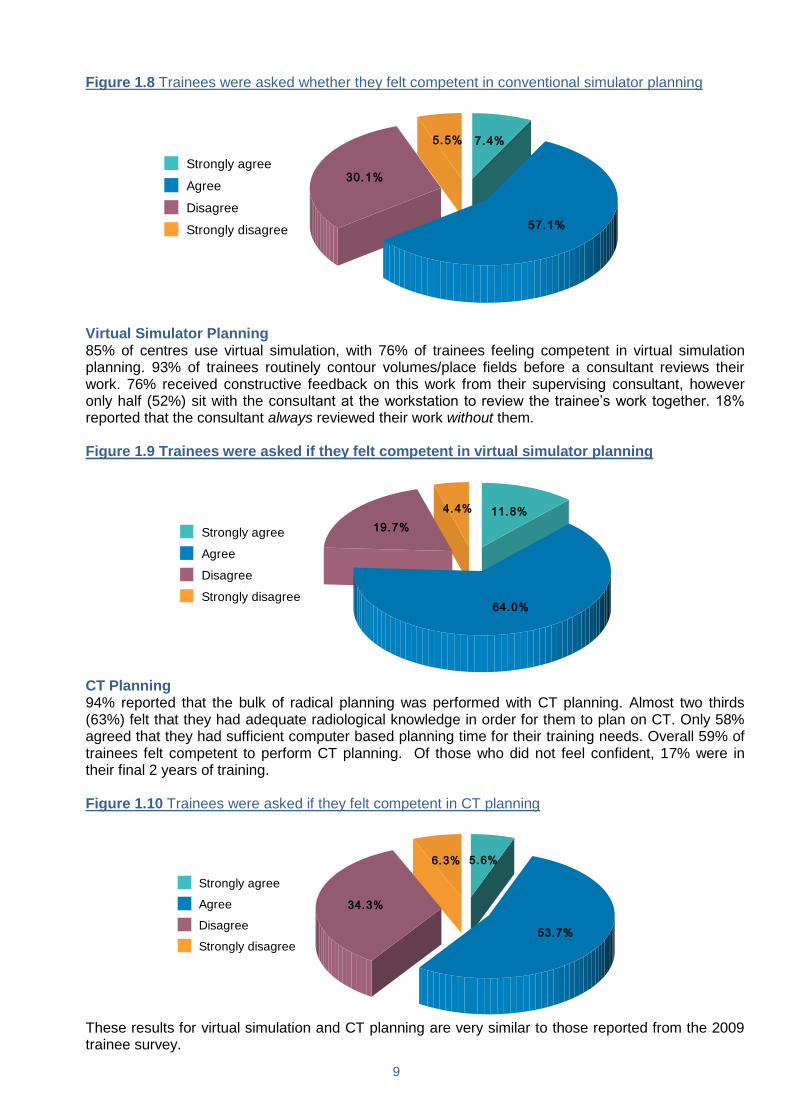
Virtual Simulator Planning 85% of centres use virtual simulation, with 76% of trainees feeling competent in virtual simulation
planning. 93% of trainees routinely contour volumes/place fields before a consultant reviews their work. 76% received constructive feedback on this work from their supervising consultant, however only half (52%) sit with the consultant at the workstation to review the trainee‟s work together. 18% reported that the consultant always reviewed their work without them.
Figure 1.9 Trainees were asked if they felt competent in virtual simulator planning
11.8%
64.0%
19.7%
4.4%
Strongly agree
Agree
Disagree
Strongly disagree
CT Planning 94% reported that the bulk of radical planning was performed with CT planning. Almost two thirds
(63%) felt that they had adequate radiological knowledge in order for them to plan on CT. Only 58% agreed that they had sufficient computer based planning time for their training needs. Overall 59% of trainees felt competent to perform CT planning. Of those who did not feel confident, 17% were in their final 2 years of training.
Figure 1.10 Trainees were asked if they felt competent in CT planning
5.6%
53.7%
34.3%
6.3%
Strongly agree
Agree
Disagree
Strongly disagree
These results for virtual simulation and CT planning are very similar to those reported from the 2009
trainee survey.
10
Formal Radiotherapy training Only 20% of trainees had attended any formal training courses in radiotherapy planning at the time of
the survey, but 34.9% intended to do so in the future. Comments on radiotherapy training in general As discussed above, experiences with radiotherapy training vary widely between institutions.
Trainees with positive experiences tended to be those who had time dedicated to planning and who were encouraged or required to volume or plan patients‟ radiotherapy prior to it being reviewed by planning staff or consultants. Where planning meetings exist these are felt to be a valuable experience, particularly where trainees were required to perform some preparation in advance.
1.3 Access to learning resources Trainees have variable access to good quality journals and textbooks through their institutions. 38%
of trainees stated that they do not regularly read oncology journals. Trainees in the early stages of training have commented that they feel they require a large amount of time to learn the basics of the speciality but they do not have a large amount of time available for wider reading. Several trainees feel that access to major oncology journals should be available for all trainees. It is recognised however that providing this access would be a large financial burden for institutions.
Key Points
The majority of trainees feel that their experience with systemic therapy is sufficient
Only a minority of trainees have access to radiotherapy planning meetings, these vary in nature but are on the whole felt to be a positive educational experience
Only 60% of trainees use conventional simulation in their current workplace
63% of trainees felt competent in conventional simulation, 76% in virtual simulation and 59% in CT planning
A small minority have attended formal radiotherapy training courses
25% of trainees‟ plans are reviewed by the supervising oncologist in the absence of the trainee

11
2. Examinations 2.1 First FRCR Examination Those who had taken the First FRCR Examination within the last 12 months (26.4% of respondents)
were asked a series of questions on this theme. 60.6% had passed the exam, and for 72.1% this was not their first attempt. Trainees were asked how many times they had attempted the exam, and there was a spread of answers with 62.7% having tried twice. 32.1% had received feedback on their exam performance and 66.7% of these found the feedback helpful.
Regarding the recent changes to the format of the exam, 74.6% felt they had been given enough
information. When asked about whether there was sufficient time to answer each question, almost 78% of trainees felt there was enough time to answer at least 80% of the answers.
Figure 2.1 Trainees were asked what percentage of Single Best Answers (SBA) they had time
to consider fully
48.6%
28.6%
14.3%
8.6%
100%
80% - 99%
60% - 79%
Less than 60%
First FRCR courses 90.1% had attended a formal lecture course in preparation for the First FRCR Examination. A minority
were unable to attend a course or found it difficult to do so, due to geographical distance or lack of study leave budget.
For 64.1% the course formed part of an MSc and 61% of these have opted into the MSc. Regarding
conflict between studying for the MSc and studying for the FRCR, 48% felt there was significant conflict, but the remainder felt there was either no conflict or only a slight conflict.
60.6% had attended a pre-exam revision course and a good spread of national courses was
mentioned. Most people felt that studying for the First FRCR had not adversely affected their clinical experience, although some commented in the free text that a proportion of the questions were not relevant to clinical practice, and many asked for more practice questions to be made available.
2.2 Final FRCR Examination There was a change in exam format between the Autumn 2010 sitting and the Spring 2011 sitting
(http://www.rcr.ac.uk/docs/oncology/pdf/CO2%20split%20announcement%20July%202010.pdf). As of spring 2011, candidates were required to pass the SBA written exam (Part A) before being permitted to sit the clinical and oral exams (Part B). This complicated the analysis of the Final FRCR questions for this survey and for this reason, we have only analysed the answers of those who sat the exam in Spring 2011.
At the Spring 2011 sitting 74.1% had passed Part A and 70% of those had gone on to pass Part B.
All candidates were sent a bar chart diagram comparing each entrant‟s performance against their peers in Part A. 92.6% felt the diagram was easy to understand and 81.5% had found it useful. 98% of all candidates felt they had been well informed regarding the recent changes to the exam format.
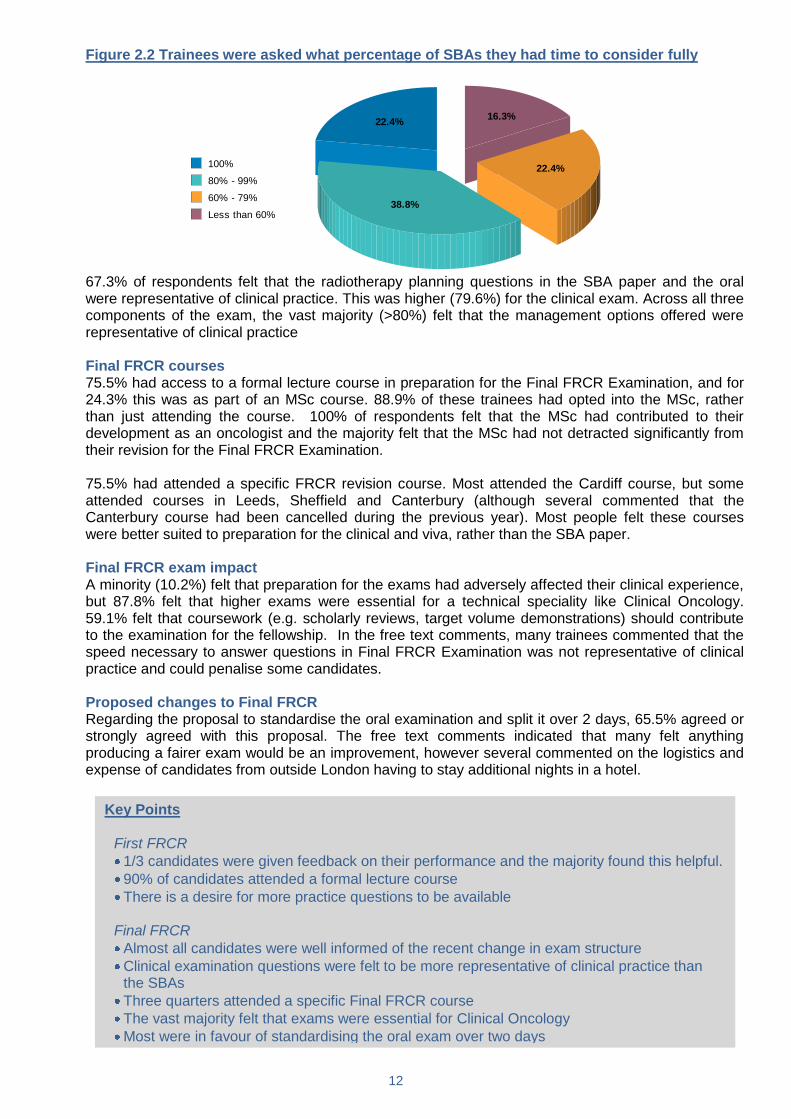
61.2% felt they had sufficient time to answer more than 80% of the SBA questions. 16.3 % only had
time to answer less than 60% of the SBA questions.
12
Figure 2.2 Trainees were asked what percentage of SBAs they had time to consider fully
22.4%
38.8%
22.4%
16.3%
100%
80% - 99%
60% - 79%
Less than 60%
67.3% of respondents felt that the radiotherapy planning questions in the SBA paper and the oral
were representative of clinical practice. This was higher (79.6%) for the clinical exam. Across all three components of the exam, the vast majority (>80%) felt that the management options offered were representative of clinical practice
Final FRCR courses 75.5% had access to a formal lecture course in preparation for the Final FRCR Examination, and for
24.3% this was as part of an MSc course. 88.9% of these trainees had opted into the MSc, rather than just attending the course. 100% of respondents felt that the MSc had contributed to their development as an oncologist and the majority felt that the MSc had not detracted significantly from their revision for the Final FRCR Examination.
75.5% had attended a specific FRCR revision course. Most attended the Cardiff course, but some
attended courses in Leeds, Sheffield and Canterbury (although several commented that the Canterbury course had been cancelled during the previous year). Most people felt these courses were better suited to preparation for the clinical and viva, rather than the SBA paper.
Final FRCR exam impact A minority (10.2%) felt that preparation for the exams had adversely affected their clinical experience,
but 87.8% felt that higher exams were essential for a technical speciality like Clinical Oncology. 59.1% felt that coursework (e.g. scholarly reviews, target volume demonstrations) should contribute to the examination for the fellowship. In the free text comments, many trainees commented that the speed necessary to answer questions in Final FRCR Examination was not representative of clinical practice and could penalise some candidates.
Proposed changes to Final FRCR Regarding the proposal to standardise the oral examination and split it over 2 days, 65.5% agreed or
strongly agreed with this proposal. The free text comments indicated that many felt anything producing a fairer exam would be an improvement, however several commented on the logistics and expense of candidates from outside London having to stay additional nights in a hotel.
Key Points
First FRCR
1/3 candidates were given feedback on their performance and the majority found this helpful.
90% of candidates attended a formal lecture course
There is a desire for more practice questions to be available Final FRCR
Almost all candidates were well informed of the recent change in exam structure
Clinical examination questions were felt to be more representative of clinical practice than the SBAs
Three quarters attended a specific Final FRCR course
The vast majority felt that exams were essential for Clinical Oncology
Most were in favour of standardising the oral exam over two days

13
3. Training Programmes and Assessment Practices There are 18 deaneries supporting approximately 375 clinical oncology trainees across the UK.
Approximately one third of all UK trainees are a part of the London Specialty School of Clinical Oncology. A regional breakdown of results is not presented in this report to preserve anonymity of respondents but the data has been reviewed at this level. A larger or smaller size of training programme does not necessarily infer superior training.
3.1 Training Programmes and Educational Support Overall 51.3% of trainees rated their training programme as excellent or above average, a slight
improvement from 2009. Figure 3.1 Trainees were asked to rate their training programme
Excellent
Above average
Average
Below average
Poor
The majority of trainees reported that they felt well supported by their College Tutor (over 80%) and
Training Programme Director (over 90%). Figure 3.2 Trainees were asked to identify how well supported they felt
Strongly Disagree
Disagree Agree Strongly Agree
I feel well supported by my College Tutor 1.1% 13.4% 66.9% 18.6%
I feel well supported by my Educational Supervisor 1.1% 6.7% 62.8% 29.4%
I feel well supported by my training Programme Director
1.1% 7.8% 64.7% 26.4%
Within reasonable limits, I am able to configure my rotation to suit my needs
4.1% 19.3% 66.2% 10.4%
3.2 Assessment and Appraisal In terms of formal assessment, Workplace Based Assessments (WpBA) were rolled out nationally
from September 2010 for all trainees on the new 2010 curriculum and those on the 2007 Curriculum. The ePortfolio was also implemented in September 2010. Therefore this is the first ORF Trainee Survey to provide feedback on trainee opinion on these schemes.
14
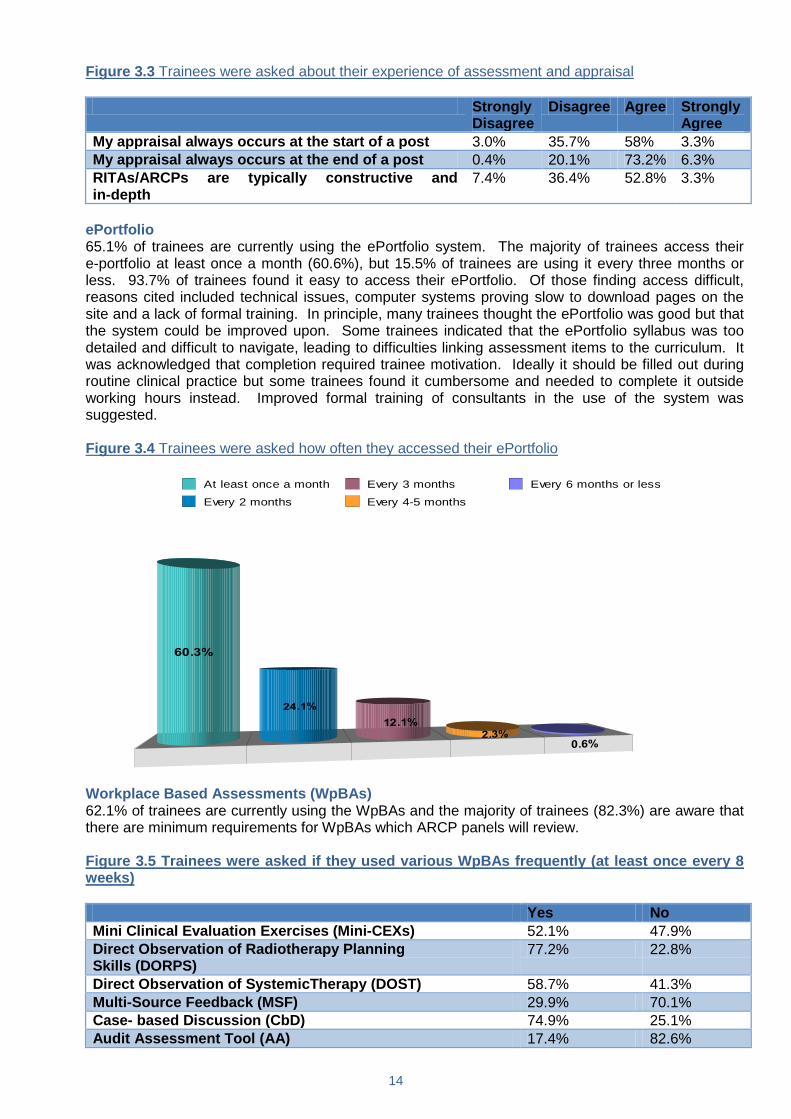
Figure 3.3 Trainees were asked about their experience of assessment and appraisal
Strongly Disagree
Disagree Agree Strongly Agree
My appraisal always occurs at the start of a post 3.0% 35.7% 58% 3.3%
My appraisal always occurs at the end of a post 0.4% 20.1% 73.2% 6.3%
RITAs/ARCPs are typically constructive and in-depth
7.4% 36.4% 52.8% 3.3%
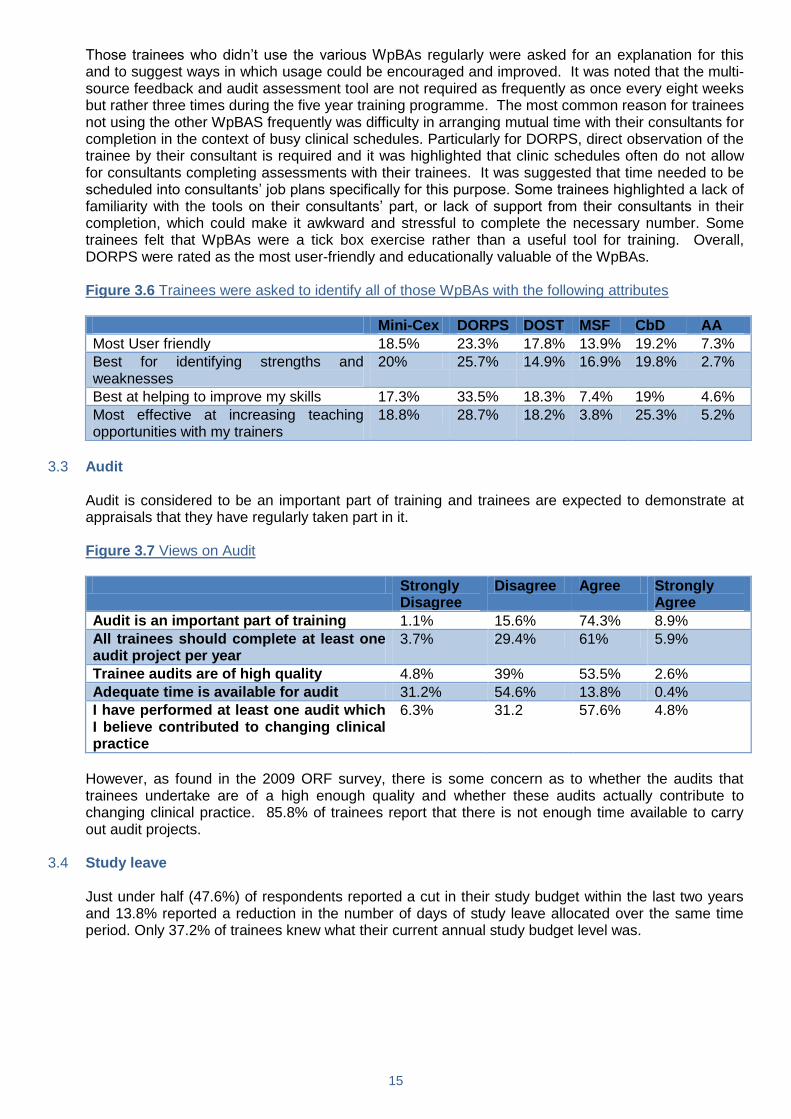
ePortfolio 65.1% of trainees are currently using the ePortfolio system. The majority of trainees access their
e-portfolio at least once a month (60.6%), but 15.5% of trainees are using it every three months or less. 93.7% of trainees found it easy to access their ePortfolio. Of those finding access difficult, reasons cited included technical issues, computer systems proving slow to download pages on the site and a lack of formal training. In principle, many trainees thought the ePortfolio was good but that the system could be improved upon. Some trainees indicated that the ePortfolio syllabus was too detailed and difficult to navigate, leading to difficulties linking assessment items to the curriculum. It was acknowledged that completion required trainee motivation. Ideally it should be filled out during routine clinical practice but some trainees found it cumbersome and needed to complete it outside working hours instead. Improved formal training of consultants in the use of the system was suggested.
Figure 3.4 Trainees were asked how often they accessed their ePortfolio
At least once a month
Every 2 months
Every 3 months
Every 4-5 months
Every 6 months or less
Workplace Based Assessments (WpBAs) 62.1% of trainees are currently using the WpBAs and the majority of trainees (82.3%) are aware that
there are minimum requirements for WpBAs which ARCP panels will review. Figure 3.5 Trainees were asked if they used various WpBAs frequently (at least once every 8
weeks)
Yes No
Mini Clinical Evaluation Exercises (Mini-CEXs) 52.1% 47.9%
Direct Observation of Radiotherapy Planning Skills (DORPS)
77.2% 22.8%
Direct Observation of SystemicTherapy (DOST) 58.7% 41.3%
Multi-Source Feedback (MSF) 29.9% 70.1%
Case- based Discussion (CbD) 74.9% 25.1%
Audit Assessment Tool (AA) 17.4% 82.6%
15
Those trainees who didn‟t use the various WpBAs regularly were asked for an explanation for this and to suggest ways in which usage could be encouraged and improved. It was noted that the multi-source feedback and audit assessment tool are not required as frequently as once every eight weeks but rather three times during the five year training programme. The most common reason for trainees not using the other WpBAS frequently was difficulty in arranging mutual time with their consultants for completion in the context of busy clinical schedules. Particularly for DORPS, direct observation of the trainee by their consultant is required and it was highlighted that clinic schedules often do not allow for consultants completing assessments with their trainees. It was suggested that time needed to be scheduled into consultants‟ job plans specifically for this purpose. Some trainees highlighted a lack of familiarity with the tools on their consultants‟ part, or lack of support from their consultants in their completion, which could make it awkward and stressful to complete the necessary number. Some trainees felt that WpBAs were a tick box exercise rather than a useful tool for training. Overall, DORPS were rated as the most user-friendly and educationally valuable of the WpBAs.
Figure 3.6 Trainees were asked to identify all of those WpBAs with the following attributes
Mini-Cex DORPS DOST MSF CbD AA
Most User friendly 18.5% 23.3% 17.8% 13.9% 19.2% 7.3%
Best for identifying strengths and weaknesses
20% 25.7% 14.9% 16.9% 19.8% 2.7%
Best at helping to improve my skills 17.3% 33.5% 18.3% 7.4% 19% 4.6%
Most effective at increasing teaching opportunities with my trainers
18.8% 28.7% 18.2% 3.8% 25.3% 5.2%
3.3 Audit Audit is considered to be an important part of training and trainees are expected to demonstrate at
appraisals that they have regularly taken part in it. Figure 3.7 Views on Audit
Strongly Disagree
Disagree Agree Strongly Agree
Audit is an important part of training 1.1% 15.6% 74.3% 8.9%
All trainees should complete at least one audit project per year
3.7% 29.4% 61% 5.9%
Trainee audits are of high quality 4.8% 39% 53.5% 2.6%
Adequate time is available for audit 31.2% 54.6% 13.8% 0.4%
I have performed at least one audit which I believe contributed to changing clinical practice
6.3% 31.2 57.6% 4.8%
However, as found in the 2009 ORF survey, there is some concern as to whether the audits that
trainees undertake are of a high enough quality and whether these audits actually contribute to changing clinical practice. 85.8% of trainees report that there is not enough time available to carry out audit projects.
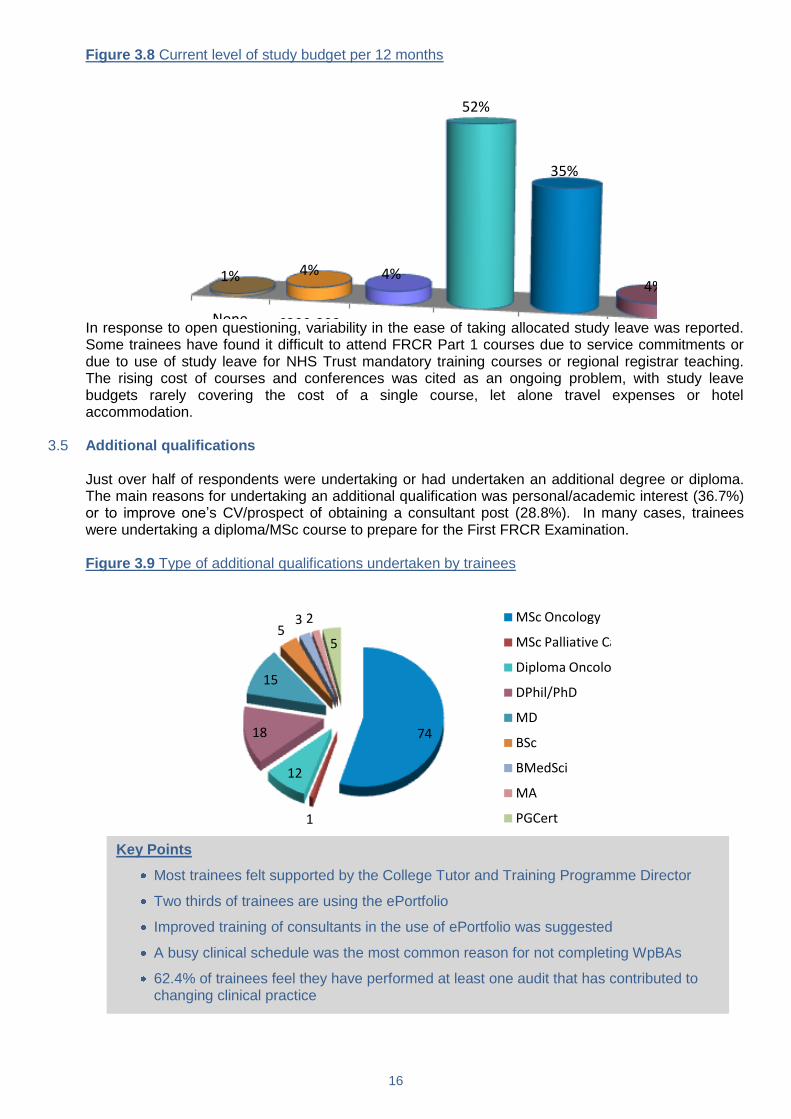
3.4 Study leave Just under half (47.6%) of respondents reported a cut in their study budget within the last two years
and 13.8% reported a reduction in the number of days of study leave allocated over the same time period. Only 37.2% of trainees knew what their current annual study budget level was.
16
Figure 3.8 Current level of study budget per 12 months
None £200-399 £400-599 £600-799 £800-999 £1000+
1% 4% 4%
52%
35%
4%
In response to open questioning, variability in the ease of taking allocated study leave was reported.
Some trainees have found it difficult to attend FRCR Part 1 courses due to service commitments or due to use of study leave for NHS Trust mandatory training courses or regional registrar teaching. The rising cost of courses and conferences was cited as an ongoing problem, with study leave budgets rarely covering the cost of a single course, let alone travel expenses or hotel accommodation.
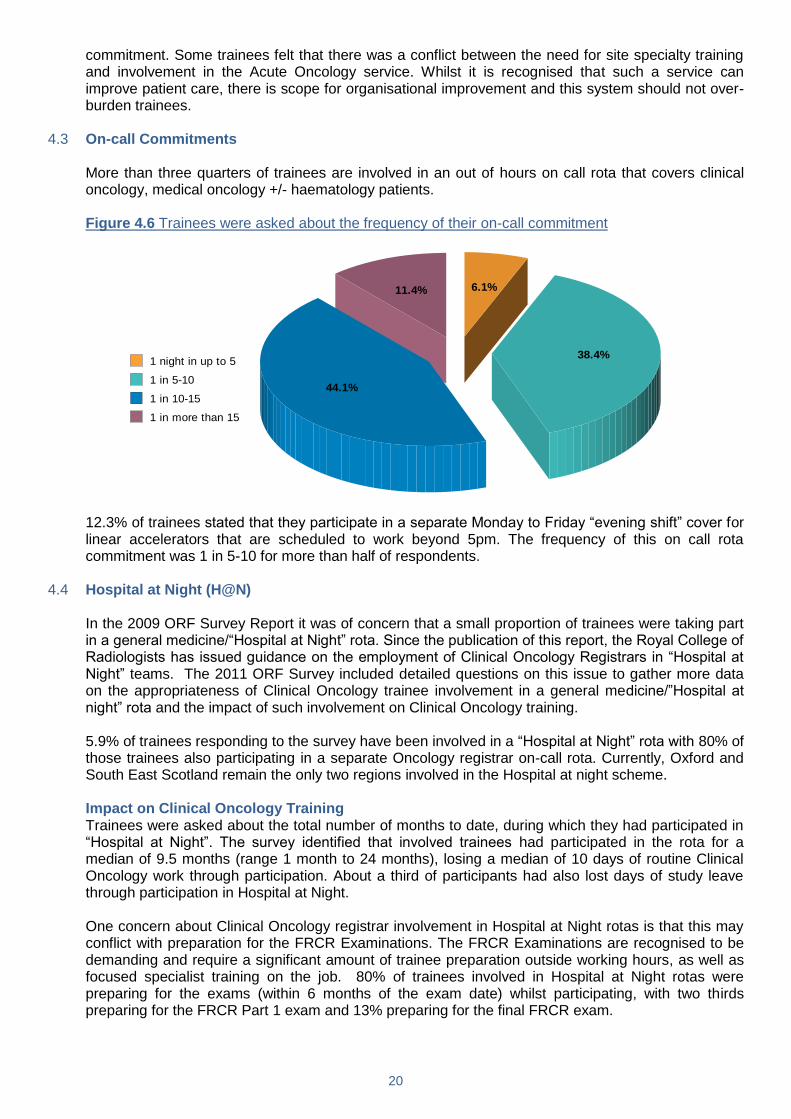
3.5 Additional qualifications Just over half of respondents were undertaking or had undertaken an additional degree or diploma.
The main reasons for undertaking an additional qualification was personal/academic interest (36.7%) or to improve one‟s CV/prospect of obtaining a consultant post (28.8%). In many cases, trainees were undertaking a diploma/MSc course to prepare for the First FRCR Examination.
Figure 3.9 Type of additional qualifications undertaken by trainees
74
1
12
18
15
53 2
5
MSc Oncology
MSc Palliative Care
Diploma Oncology
DPhil/PhD
MD
BSc
BMedSci
MA
PGCert
Key Points
Most trainees felt supported by the College Tutor and Training Programme Director
Two thirds of trainees are using the ePortfolio
Improved training of consultants in the use of ePortfolio was suggested
A busy clinical schedule was the most common reason for not completing WpBAs
62.4% of trainees feel they have performed at least one audit that has contributed to changing clinical practice

17
4 Regional Clinical Oncology Service Commitments The structure and delivery of service has changed considerably in recent years with the reforms of
specialty training for newly qualified doctors. These changes, as well as the implementation of the European Working Time Directive (EWTD) in August 2009, are thought to have affected the workload of trainees indirectly, by affecting the staffing and level of experience of the junior doctors to whom they provide support on the wards.
Acute Oncology initiatives are being implemented nationwide and not only changing the way in which
clinical care for cancer patients is being delivered but also having a potential impact on training. A preliminary assessment of these aspects was investigated in the 2009 ORF survey but the current survey hopefully provides more robust data about trainee experience and views. In July 2011 the Royal College of Radiologists‟ issued guidance on the role of clinical oncologists in Acute Oncology Services (http://www.rcr.ac.uk/docs/oncology/pdf/Acute_Oncology_July_2011.pdf)
Trainees were asked about on-call arrangements in their local departments. In March 2011 the Royal
College of Radiologists issued guidance about Clinical Oncology trainee involvement in Hospital at Night schemes, in which Oncology registrars are expected to provide night time cover at medical registrar level for non-Oncology patients (http://www.rcr.ac.uk/docs/oncology/pdf/H@N%20guidance%20March%202011%20Final.pdf).
In the current survey, detailed questions were asked of trainees in regions participating in Hospital at
Night rotas (H@N) to gather further data about the impact of the scheme on training, morale and patient safety.
In 2011, with the implementation of nationally co-ordinated recruitment, the annual intake of ST3‟s
occurs in August/September of each year. If there are gaps in the rota outwith this time, these gaps can be filled by LAT or LAS appointments. However, such positions are notoriously difficult to recruit to and often remain unfilled. This survey confirms that unfilled registrar posts are an issue for many training schemes, with half of trainees (50.2%) not having had a full complement of clinical oncology trainees in their hospital over the 6 month period preceding the survey. Hopefully this will be less of an issue in 2012, as there will be a second round of nationally coordinated recruitment in November in 2012.
Figure 4.1 Trainees were asked to indicate the reasons for lack of full complement of Clinical
Oncology trainees
25.9%
29.1%
30.5%
8.2% 5.0% 1.4%
Trainee on OOPE with no replacement appointed
Maternity leave with no replacement appointed
Lack of LAT/LAS posts being filled
Long-term sick leave with no replacement appointed
Hospital financial cutback in staff numbers
Other

18
4.1 Management of Oncology In-patients Trainees were asked questions about the management of Oncology in-patients in their posts,
particularly about the level of registrar and consultant involvement in in-patient care. The majority of trainees (81.8%) contribute to the in-patient care of patients belonging to at least two consultants/teams with consultants/teams reviewing all their in-patients at least once a week, according to 88% of respondents. However only 38.7% of trainees reported that new admissions were reviewed by a consultant within 24 hours of admission.
Figure 4.2 Trainees were asked how many ward rounds they performed with the attending consultant
for the relevant patient
Zero
One
Two
Three
Four or more
Figure 4.3 Trainees were asked how many ward rounds they performed a week independent of
consultant supervision
Zero
One
Two
Three
Four or more
There was variation in the number of hours per week spent by trainees in reviewing patients on the
ward but 84.4% of trainees spent up to 6 hours in doing so, with a minority (15.6%) spending a longer time than this. Less than one third of trainees were required to attend the ward during radiotherapy planning sessions.
Over the past few years, a significant number of hospitals have implemented a formal system, in
which specialty trainees take turns to be primarily based on the Oncology ward for a week or more in succession. This is often referred to as an Oncology Ward Registrar rota. The current survey indicates that 25.7% of trainees are currently involved in such a system, a similar proportion to that identified in the 2009 ORF survey.

19
Figure 4.4 Trainees involved in an Oncology Ward Registrar rota were asked how many weeks they were involved in this rota on average during a six month period
1 week
2 weeks
3 weeks
4 weeks
5 weeks
6 weeks or more
Overall, the majority of trainees think that the Oncology Ward Registrar system is unhelpful for
training purposes. Figure 4.5 Trainees were asked for their views on statements made about an Oncology Ward
Registrar system
Strongly disagree
Disagree Agree Strongly agree
The system is educational and improves Clinical Oncology training
17.4% 50.7% 30.4% 1.4%
The system strengthens training by releasing the non-cover registrars for teaching or planning sessions
9.7% 47.6% 40.1% 2.6%
The system adversely affects training by reducing overall training opportunities
1.9% 35.3% 50.2% 12.6%
Half of respondents (50.2%) thought that increasing ward cover was required due to an increasing
lack of experience by junior ward doctors. Extensive feedback was provided regarding examples in support of this. Many trainees reported that junior doctors on the ward were inexperienced in procedures such as ascitic or pleural drain insertion and registrar involvement was frequently required for their performance. Respondents also cited the relative lack of general medical experience of foundation year doctors and associated lack of competence or confidence in managing acutely unwell patients resulting in a greater requirement for supervision by a registrar. Some trainees reported that ward juniors required registrar guidance on basic medical management decisions such as the appropriate prescription of fluids, anti-emetics or opiates.
4.2 Acute Oncology Trainees were asked about the presence of an Acute Oncology Service within their department.
34.2% of trainees reported the existence of an Acute Oncology Service within their Department and in 78.3% cases trainees took part in delivering this service. 71.7% of trainees thought that there had been an improvement in the quality of in-patient care since the introduction of an Acute Oncology service.
General comments were invited about Acute Oncology. Many trainees commented that the Acute
Oncology service in their centre was in its early days and still evolving. There is clearly a lot of variation in the form which Acute Oncology Services take in different hospitals. Two areas of concern that were repeatedly expressed by trainees were the shortage of staff to cover the Acute Oncology service and problems created by the shortage of beds. In some centres the service is Consultant led but in others it is highly dependent on specialty registrars and has increased their level of service
20
commitment. Some trainees felt that there was a conflict between the need for site specialty training and involvement in the Acute Oncology service. Whilst it is recognised that such a service can improve patient care, there is scope for organisational improvement and this system should not over-burden trainees.
4.3 On-call Commitments More than three quarters of trainees are involved in an out of hours on call rota that covers clinical
oncology, medical oncology +/- haematology patients. Figure 4.6 Trainees were asked about the frequency of their on-call commitment
6.1%
38.4%
44.1%
11.4%
1 night in up to 5
1 in 5-10
1 in 10-15
1 in more than 15
12.3% of trainees stated that they participate in a separate Monday to Friday “evening shift” cover for
linear accelerators that are scheduled to work beyond 5pm. The frequency of this on call rota commitment was 1 in 5-10 for more than half of respondents.
4.4 Hospital at Night (H@N) In the 2009 ORF Survey Report it was of concern that a small proportion of trainees were taking part
in a general medicine/“Hospital at Night” rota. Since the publication of this report, the Royal College of Radiologists has issued guidance on the employment of Clinical Oncology Registrars in “Hospital at Night” teams. The 2011 ORF Survey included detailed questions on this issue to gather more data on the appropriateness of Clinical Oncology trainee involvement in a general medicine/”Hospital at night” rota and the impact of such involvement on Clinical Oncology training.
5.9% of trainees responding to the survey have been involved in a “Hospital at Night” rota with 80% of
those trainees also participating in a separate Oncology registrar on-call rota. Currently, Oxford and South East Scotland remain the only two regions involved in the Hospital at night scheme.
Impact on Clinical Oncology Training Trainees were asked about the total number of months to date, during which they had participated in
“Hospital at Night”. The survey identified that involved trainees had participated in the rota for a median of 9.5 months (range 1 month to 24 months), losing a median of 10 days of routine Clinical Oncology work through participation. About a third of participants had also lost days of study leave through participation in Hospital at Night.
One concern about Clinical Oncology registrar involvement in Hospital at Night rotas is that this may
conflict with preparation for the FRCR Examinations. The FRCR Examinations are recognised to be demanding and require a significant amount of trainee preparation outside working hours, as well as focused specialist training on the job. 80% of trainees involved in Hospital at Night rotas were preparing for the exams (within 6 months of the exam date) whilst participating, with two thirds preparing for the FRCR Part 1 exam and 13% preparing for the final FRCR exam.

21
Figure 4.7 Trainees were asked if they were preparing for FRCR exams whilst participating in H@N
66.7%
20.0%
13.3%
Yes, First FRCR
Yes, Final FRCR
No
Figure 4.8 Trainees were asked to what extent they agreed with the following statement about H@N
Strongly disagree
Disagree Agree Strongly Agree
Participation in H@N has been beneficial to my Clinical Oncology Training
86.7% 13.3% 0% 0%
Appropriateness of Clinical Oncology Trainee Involvement 52.4% of those trainees involved in Hospital at Night had participated during Year 1 of Clinical
Oncology training but nearly half had participated in Years 2 or 3, which is of concern, given the Royal College of Radiologists‟ recommendation that where trainees are involved in Hospital at Night rotas, this should be restricted to ST3 level or the first year of Specialty.
Figure 4.9 Trainees were asked which years of training they had participated in a H@N rota
Year 1
Year 2
Year 3
Year 4
Year 5
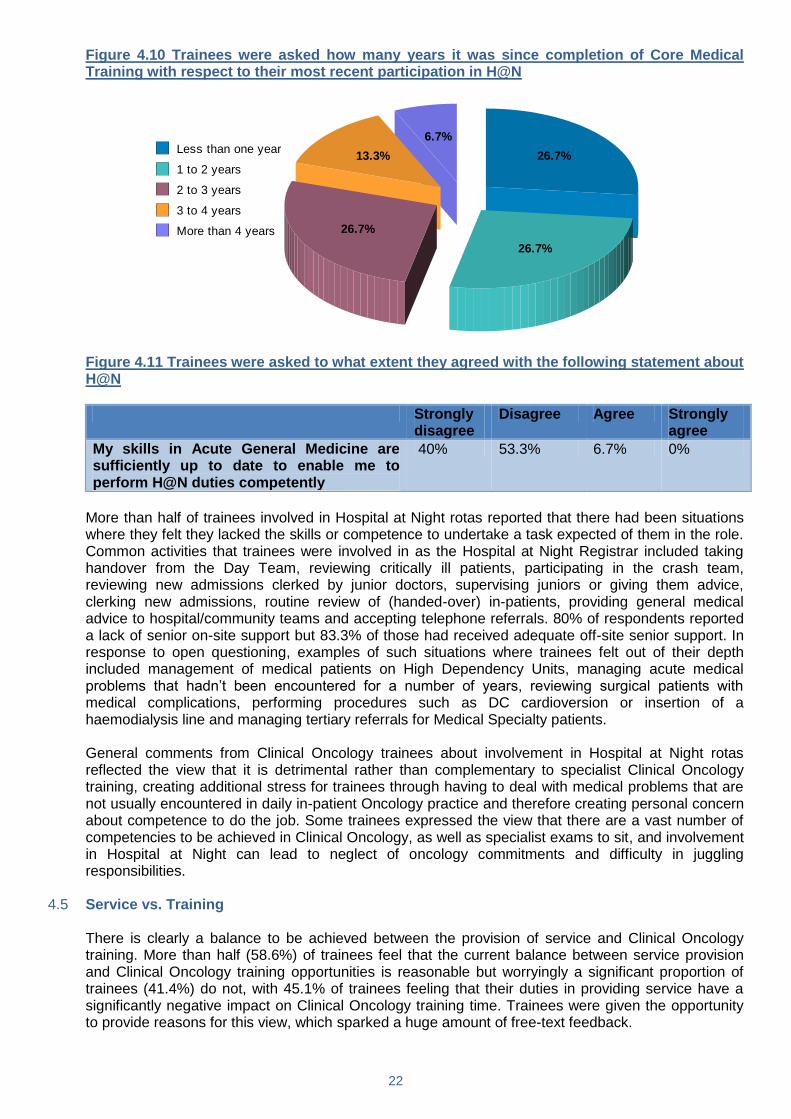
It is recognised by the Royal College of Radiologists that where Clinical Oncology trainees are
involved in Hospital at Night rotas, ideally they should have completed Core Medical Training in the recent past as they will become deskilled in the management of acutely ill non-Oncology patients as time elapses from the training and exposure provided by Core Medical Training. This survey identified that three quarters of trainees involved were more than 12 months beyond Core Medical Training at the time of their involvement; worryingly 20% were more than 3 years out from Core Medical Training. However, only 6.7% of hospitals had provided trainees with training updates in Acute General Medicine. None of the trainees had been provided with additional study leave or additional study budget for training sessions in Acute General Medicine, over those provided for Clinical Oncology training.
22
Figure 4.10 Trainees were asked how many years it was since completion of Core Medical Training with respect to their most recent participation in H@N
26.7%
26.7%
26.7%
13.3%
6.7%
Less than one year
1 to 2 years
2 to 3 years
3 to 4 years
More than 4 years
Figure 4.11 Trainees were asked to what extent they agreed with the following statement about
H@N
Strongly disagree
Disagree Agree Strongly agree
My skills in Acute General Medicine are sufficiently up to date to enable me to perform H@N duties competently
40% 53.3% 6.7% 0%
More than half of trainees involved in Hospital at Night rotas reported that there had been situations
where they felt they lacked the skills or competence to undertake a task expected of them in the role. Common activities that trainees were involved in as the Hospital at Night Registrar included taking handover from the Day Team, reviewing critically ill patients, participating in the crash team, reviewing new admissions clerked by junior doctors, supervising juniors or giving them advice, clerking new admissions, routine review of (handed-over) in-patients, providing general medical advice to hospital/community teams and accepting telephone referrals. 80% of respondents reported a lack of senior on-site support but 83.3% of those had received adequate off-site senior support. In response to open questioning, examples of such situations where trainees felt out of their depth included management of medical patients on High Dependency Units, managing acute medical problems that hadn‟t been encountered for a number of years, reviewing surgical patients with medical complications, performing procedures such as DC cardioversion or insertion of a haemodialysis line and managing tertiary referrals for Medical Specialty patients.
General comments from Clinical Oncology trainees about involvement in Hospital at Night rotas
reflected the view that it is detrimental rather than complementary to specialist Clinical Oncology training, creating additional stress for trainees through having to deal with medical problems that are not usually encountered in daily in-patient Oncology practice and therefore creating personal concern about competence to do the job. Some trainees expressed the view that there are a vast number of competencies to be achieved in Clinical Oncology, as well as specialist exams to sit, and involvement in Hospital at Night can lead to neglect of oncology commitments and difficulty in juggling responsibilities.
4.5 Service vs. Training There is clearly a balance to be achieved between the provision of service and Clinical Oncology
training. More than half (58.6%) of trainees feel that the current balance between service provision and Clinical Oncology training opportunities is reasonable but worryingly a significant proportion of trainees (41.4%) do not, with 45.1% of trainees feeling that their duties in providing service have a significantly negative impact on Clinical Oncology training time. Trainees were given the opportunity to provide reasons for this view, which sparked a huge amount of free-text feedback.

23
The most common concern of trainees is that there is a lack of protected radiotherapy planning time in their weekly schedule. Where fixed planning sessions do exist, the experience of some trainees is that they frequently miss these sessions due to requirements to cover non-timetabled clinics or to attend the ward or chemotherapy unit to deal with patient problems. There is a general feeling that radiotherapy training is not prioritised within departments and planning time is being eroded at the expense of providing other elements of the Oncology Service. Another commonly expressed view was that outpatient clinics are very busy, sometimes over booked or understaffed, limiting opportunity for discussion of cases with consultants. Some trainees are required to spend a high proportion of their time doing clinics, which restricts involvement in other training opportunities. Registrars reported in the free text that they were covering up to 7 clinics a week. Whilst some trainees reported that they gained valuable training whilst providing service, others felt that their “on the job” training was inadequate. In some cases this was because consultants were frequently absent and feedback on patient management was scarce. Some trainees recognised that their training experience was variable dependent on the consultant they were working with. It was suggested that trainees should be allocated to work with consultants who were interested in training and willing to teach, rather than those with the busiest clinics.
Many trainees are being asked to cover the workload of other staff; for example staff grades on
annual or sick leave, cross cover of other registrars on leave or unfilled posts. The increasing number of consultants and decreasing number of trainees means that in some hospitals trainees are expected to care for patients belonging to multiple consultants. Some trainees report that the implementation of a Ward registrar system, Hospital at Night rota or Acute Oncology Service has further reduced time and opportunities to gain out-patient oncology experience. Additionally some trainees do not have any formal teaching scheduled in their timetable and where this does exist it is not always bleep-free.
Key Points
Half of trainees report not having a full complement of Clinical Oncology trainees in their hospital over the 6 months preceding the survey
Only 38.7% of trainees report that new admissions were reviewed by a consultant within 24 hours of admission
The vast majority of trainees spend up to 6 hours a week reviewing ward patients
Most trainees feel that the Oncology Ward Registrar system is unhelpful for training purposes
There is a general feeling that there is a shortage of staff to cover the Acute Oncology service
71.7% of trainees felt that there has been an improvement in the quality of patient care since the introduction of an Acute Oncology service
Not a single trainee felt that participation in H@N was beneficial to their Clinical Oncology training
3/4 of trainees involved in H@N were more than 12 months beyond Core Medical Training
Over 90% of trainees involved in H@N did not feel that their skills in acute general medicine were sufficiently up to date to enable them to perform H@N duties competently
With regards to service versus training, the biggest concern of trainees is the lack of protected radiotherapy planning time in their weekly schedule
Trainees feel that they should be allocated to work with consultants who are interested and willing to teach rather than those with the busiest clinics
24
5 Research and Out of Programme Activities Clinical oncology is an academic speciality and increasing numbers of trainees choose to
complement their clinical training with time out of programmed training, spent in dedicated research activities or in developing advanced technology skills, either within the UK or abroad. Time spent out of programme can be hugely beneficial, on a number of levels, as well as enjoyable and rewarding. This period of time is known as out of programme activities/experience (OOPA/OOPE) and is rigorously planned between the trainee, the head of their training programme, the College and the GMC. A number of Academic Clinical Fellowships have been introduced in recent years and the intention is to further encourage the expansion of a high quality clinical academic workforce.
Respondents were asked about their previous, ongoing and future plans to spend a period of time out
of programme. Detailed information regarding the nature and quality of their activity and organisational practicalities was acquired, and future career intentions were also assessed. The following is a summary of the key points, and the more detailed data will be utilised further at a later date, incorporated into guidance for organising OOPE on the RCR website.
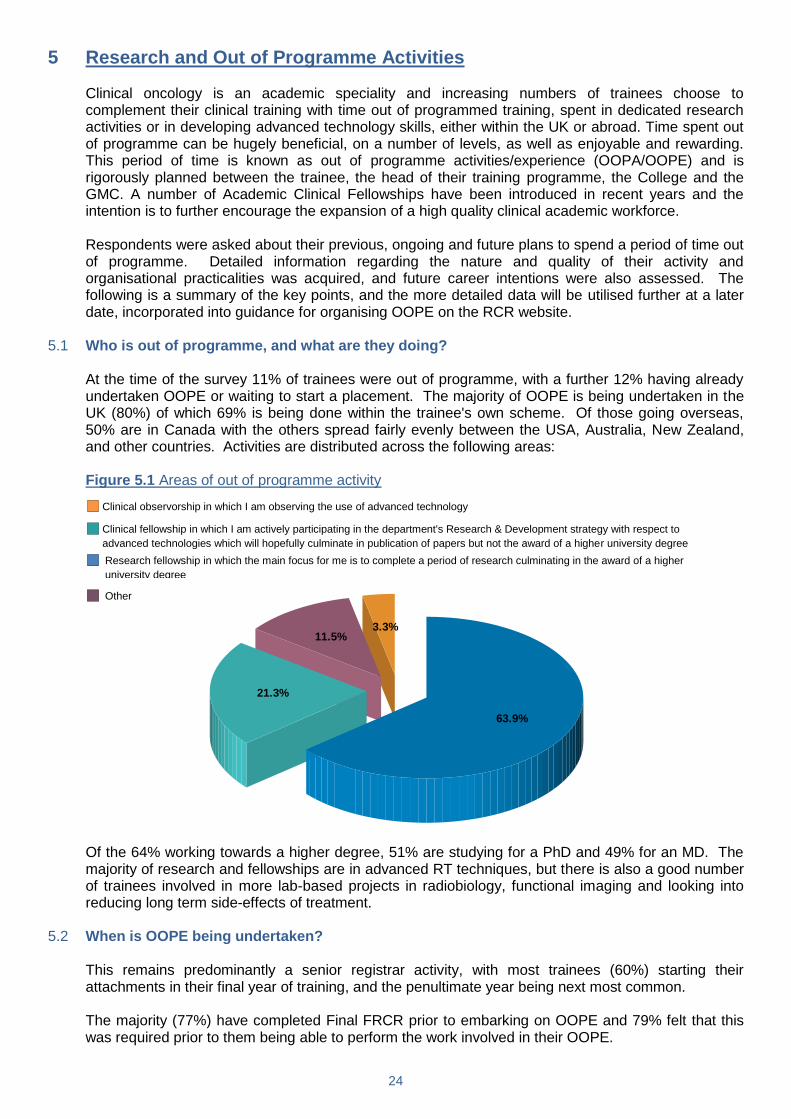
5.1 Who is out of programme, and what are they doing? At the time of the survey 11% of trainees were out of programme, with a further 12% having already
undertaken OOPE or waiting to start a placement. The majority of OOPE is being undertaken in the UK (80%) of which 69% is being done within the trainee's own scheme. Of those going overseas, 50% are in Canada with the others spread fairly evenly between the USA, Australia, New Zealand, and other countries. Activities are distributed across the following areas:
Figure 5.1 Areas of out of programme activity
63.9%
21.3%
11.5%3.3%
Of the 64% working towards a higher degree, 51% are studying for a PhD and 49% for an MD. The
majority of research and fellowships are in advanced RT techniques, but there is also a good number of trainees involved in more lab-based projects in radiobiology, functional imaging and looking into reducing long term side-effects of treatment.
5.2 When is OOPE being undertaken? This remains predominantly a senior registrar activity, with most trainees (60%) starting their
attachments in their final year of training, and the penultimate year being next most common. The majority (77%) have completed Final FRCR prior to embarking on OOPE and 79% felt that this
was required prior to them being able to perform the work involved in their OOPE.
Clinical observorship in which I am observing the use of advanced technology
Clinical fellowship in which I am actively participating in the department's Research & Development strategy with respect to
advanced technologies which will hopefully culminate in publication of papers but not the award of a higher university degree Research fellowship in which the main focus for me is to complete a period of research culminating in the award of a higher
university degree
Other
25
For those studying for an MD or PhD, the average time out of programme is 35 months, while for
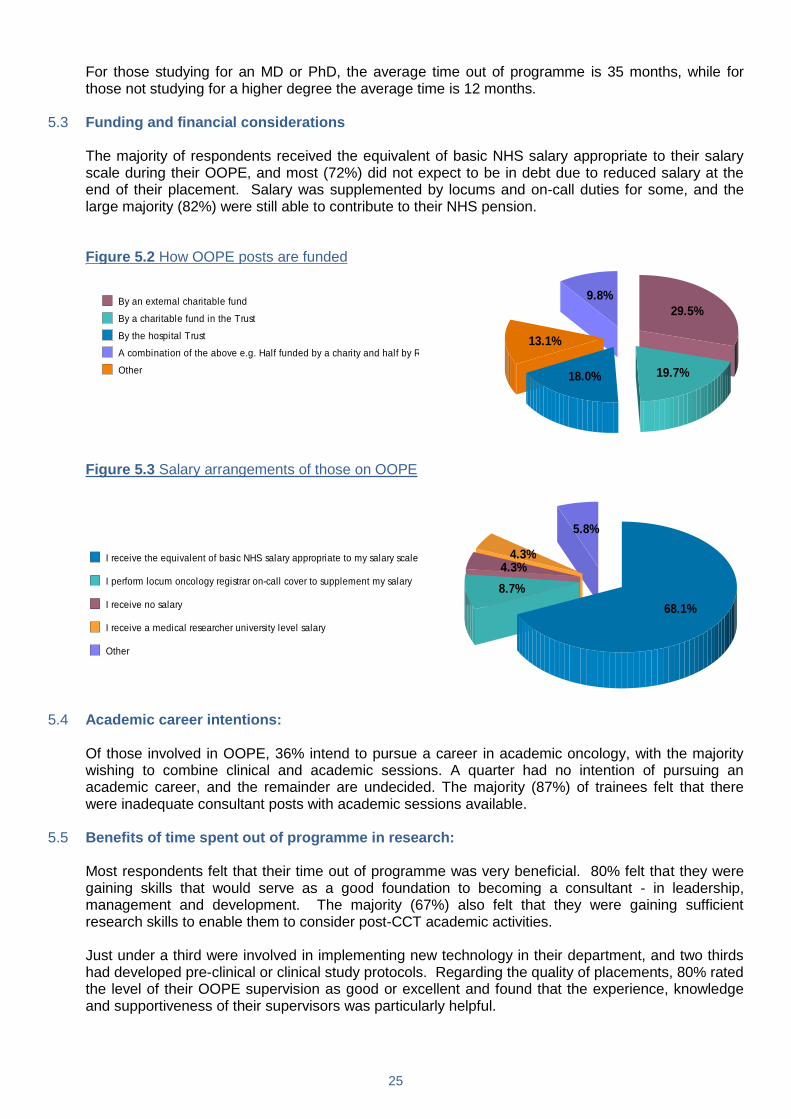
those not studying for a higher degree the average time is 12 months. 5.3 Funding and financial considerations The majority of respondents received the equivalent of basic NHS salary appropriate to their salary
scale during their OOPE, and most (72%) did not expect to be in debt due to reduced salary at the end of their placement. Salary was supplemented by locums and on-call duties for some, and the large majority (82%) were still able to contribute to their NHS pension.
Figure 5.2 How OOPE posts are funded
29.5%
19.7%18.0%
13.1%
9.8%
By an external charitable fund
By a charitable fund in the Trust
By the hospital Trust
A combination of the above e.g. Half funded by a charity and half by R&D
Other
Figure 5.3 Salary arrangements of those on OOPE
68.1%
8.7%
4.3%4.3%
5.8%
I receive the equivalent of basic NHS salary appropriate to my salary scale
I perform locum oncology registrar on-call cover to supplement my salary
I receive no salary
I receive a medical researcher university level salary
Other
5.4 Academic career intentions: Of those involved in OOPE, 36% intend to pursue a career in academic oncology, with the majority
wishing to combine clinical and academic sessions. A quarter had no intention of pursuing an academic career, and the remainder are undecided. The majority (87%) of trainees felt that there were inadequate consultant posts with academic sessions available.
5.5 Benefits of time spent out of programme in research: Most respondents felt that their time out of programme was very beneficial. 80% felt that they were
gaining skills that would serve as a good foundation to becoming a consultant - in leadership, management and development. The majority (67%) also felt that they were gaining sufficient research skills to enable them to consider post-CCT academic activities.
Just under a third were involved in implementing new technology in their department, and two thirds
had developed pre-clinical or clinical study protocols. Regarding the quality of placements, 80% rated the level of their OOPE supervision as good or excellent and found that the experience, knowledge and supportiveness of their supervisors was particularly helpful.

26
5.6 Respondents not currently spending time out of programme Of those respondents not out of programme, most (95%) would consider participating in fellowships
to gain training in new skills either at home or abroad, and 6% of all respondents had applied for research or clinical fellowship at some point. 61% hoped to undertake OOPE in the future but had not yet organised a placement.
The percentage of those with no intention of pursuing a period of OOPE was significantly less that 2
years ago (16% compared to 40%) and for these trainees, most common reasons were (in order of magnitude) personal/family, extended training time, financial considerations and pressure to pass FRCR.
Figure 5.4 Intentions of those not currently out of programme
I have already completed a period of OOPE
I have an OOPE placement arranged but have not yet started it
I hope to undertake a period of OOPE in the future but have not yet arranged anything
I have not done, and do not intend to undertake, a period of OOPE
5.7 General points regarding research and OOPE
Academic work during full time clinical training: Whilst 62% of respondents felt that research activity was encouraged (with 38% reporting discouragement), only 12% felt that they had adequate time available to dedicate to research projects.
Areas of interest: Respondents felt strongly that radiobiology and clinical radiotherapy research were poorly represented in the opportunities available, with clinical radiotherapy research being the area that the majority (60%) found most interesting.
Posters and publications in oncology: Just over two thirds of respondents had published posters or publications in oncology, with one third owning 1-2 posters or publications and another third having 3 or more published pieces of work. Just under a third had no publications or posters.
5.8 Responses to open questions There were many comments about the joys and frustrations of combining clinical work with research
and OOPE.
Research: Many respondents commented that although they had entered training with high hopes of participating in research, and indeed that they feel it should be “desirable” or “essential” there seem to be a number of barriers to this. The pressures associated with completing FRCR were mentioned frequently, and the seeming lack of time once this is completed to then organise a period of research before CCT. There is also a feeling of there being little funding and opportunity in the areas which most interest people, and difficulty in finding out about opportunities for research. It is

27
felt that most placements are found by word of mouth, and this is backed up by the survey as only 20% of positions were found by a job advert. There were several comments suggesting that as with Medical Oncology, a period of time in research should become more the norm, but another commented that “research for research's sake” can be a harmful pressure.
Out of programme activities: Several respondents took the time to describe how much they have enjoyed OOPE and how it has given them the time and freedom to pursue areas of interest that are difficult to cover in a busy job. However, there is an overall feeling that access to information regarding placements is rather patchy, and some comment on the process seeming rather “secretive” and difficult to organise.
Key Points
There is clearly a great amount of interest amongst trainees in spending time away from their routine clinical job to learn new skills and techniques (95% of respondents expressing an interest). This perhaps reflects the uneven distribution of new technology across the country, and the difficulty in gaining adequate exposure to these techniques as a trainee. With advanced radiotherapy techniques only being available in certain centres, how best to ensure all trainees receive adequate exposure to these is unclear but OOPE clearly has a role to play.
This obvious enthusiasm for a deeper experience or time spent in research is clearly not translating into all of these trainees actualising these aspirations and accessing fellowship or research opportunities.
There is an obvious need for better information regarding organising effective OOPE, and the ORF aims to establish a database of OOPE placements which will be accessible via the RCR website. This will enable trainees who have undertaken OOPE to provide information on placements and the practicalities of organising these, and those offering fellowships to advertise them to a broader audience.

28
6 Royal College of Radiologists & the Oncology Registrars’ Forum The vast majority of trainees (93%) agreed or strongly agreed that the work of the RCR is essential in
providing leadership and promoting education for clinical oncologists, and 81% regularly read the Clinical Oncology journal provided to the college members. Fewer trainees regularly use the website (65%) or read the RCR‟s e-bulletins (57%). Over 90% believe that the work of the RCR is of relevance to them.
When asked specifically about the Oncology Registrars‟ Forum (ORF), 97% of trainees agreed that
the forum‟s role is to promote and support clinical oncology training and experience. A third of trainees, however, were not aware that the ORF had a dedicated section of the RCR‟s website, and only 33% had used the ORF‟s online resources. A similar number of trainees (35%) felt that the online resources had been useful.
Figure 6.1 Trainees were asked if they were aware of the ORF‟s section of the College‟s website
10.4%
56.7%
28.0%
4.9%
Strongly agree
Agree
Disagree
Strongly disagree
Figure 6.2 Trainees were asked if they had used the ORF‟s online resources
4.1%
28.4%
60.4%
7.1%
Strongly agree
Agree
Disagree
Strongly disagree
Trainees‟ suggestions for the ORF‟s online role included providing information on exams including
practice questions, providing information for new trainees and information regarding research and OOPE opportunities. These are all areas which have been or are due to be updated on the RCR‟s website – further feedback from trainees is welcome and valued. General feedback regarding the role and value of the ORF within the RCR was positive.
Key Points
Most trainees are aware of the roles of the RCR and the ORF
Awareness of the ORF section of the RCR website needs to improve
Most trainee suggestions for the role of the ORF‟s online resource have either already been provided or are in the process of being developed.

29
7 Career and Work-Life Balance and Less than Full-Time Training
7.1 The future Trainees were asked if they were confident about obtaining a consultant post in clinical oncology at
the end of their training, and the answers reflected a 50:50 split of opinions. 69.8% felt it would be more common for people to move between consultant jobs in the future. 65.3% felt that a sub-consultant grade was likely to be created but 74.2 % felt that this was not appropriate to new styles of training. 32.4 % stated that they would rather be unemployed for a period of time, than take a sub-consultant post.
7.2 Recruitment 20.1% were recruited via the nationally coordinated recruitment process and for 98% clinical oncology
had been their first choice of speciality. 72.2% had been offered a post in their first choice of deanery. For the rest, just over half got their second choice, and roughly a quarter got their third and fourth choices.
7.3 Less-than-full-time training (LTFT) 14.7% of respondents are currently working LTFT. An additional 4.3% had previously worked LTFT
and 10.4% are intending to train part-time in the future. 1.7% would like to work LTFT but the opportunity is not available to them. 12% of respondents intend to work LTFT as a consultant.
Of those currently working LTFT, just over a quarter had commenced LTFT training in each of years
1-3, with a small number becoming part time in years 4-5. 63.3% work 6 sessions per week, with 12.2% working seven sessions, and 18.4% working 8 sessions per week. Current working patterns indicated the vast majority are working either reduced sessions in a full time post, or a job/slot share.
Figure 7.1 Trainees currently training LTFT were asked what their current working arrangement was
Supernumary
Job Share
Reduced sessions in a full-time post
Other
The „Other‟ section includes trainees doing OOPE part-time, and those in clinical lecturer posts.
Supporting what was suspected anecdotally, very few felt that trying to cover a full-time job in reduced sessions was the optimal way to train LTFT. 34.7% felt supernumerary training was optimal and 51% felt a job-share was optimal. Many respondents left comments such as „I would prefer job-sharing because you are not “dumping on your full-time colleagues and can hand things over to your other half” and “Doing a full-time job in reduced sessions is impossible!”
75.5% of LTFT trainees felt they could achieve a balanced mix of service and training in their jobs.
For those where this was not the case, free text comments mostly revolved around feeling that you needed to „make up‟ for the lack of service provision on your days off by limiting time for teaching, audit and research.
The vast majority (91.8%) had no problems accessing LTFT training. 2.6% of all respondents were
currently on maternity leave, and 71.4% of these were intending to take the full 12 months off.

30
7.4 Leaving oncology A quarter of trainees had considered leaving oncology, and 41.2% of these had considered leaving
medicine all together. For those who had considered changing speciality, the most common speciality that they have considered was General Practice, with a small number considering general medicine, radiology, pathology and palliative care
7.5 Work-life balance and morale For most people, they felt their work-life balance was OK, good or excellent (84.3%). However, a
small proportion felt their work-life balance was poor or very poor. The work-life balance scores were slightly better for LTFT trainees, compared with full-time trainees.
Figure 7.2 Trainees were asked to rate their work/life balance and their morale
How would you rate your work/life balance at present?
How would you rate your morale at present?
Overall, 85% felt their morale was excellent, good or OK, with the proportions reporting low morale
very similar to those reporting poor work-life balance. The free text comments underline the difficulties of studying for the exam whilst still performing at work, the conflict between wanting to do a good job and wanting to see your spouse/children, and the anxiety of the forthcoming consultant job situation.
Key Points
A third of trainees would rather have a period of unemployment than accept a sub consultant post
98% of trainees appointed via the nationally co-ordinated recruitment process had selected clinical oncology as their first choice specialty
With regards to LTFT trainees, a third felt that supernumerary training was optimal and a half preferred job sharing
Over 90% of LTFT trainees had no problem accessing such training
The vast majority of trainees felt that their work/life balance and morale was OK, good or excellent.

31
8 Demographics Just over half of the trainees responding to the survey (58%) were female and 82% were aged
between 30 and 40 – very similar to 2009. 13.8% were currently undertaking some form of out of programme experience. 32% had passed the final FRCR exam, a further 38% had passed the first FRCR exam and the remaining 30% were yet to pass the first FRCR exam. Trainees responding to the survey were roughly evenly distributed by year of training. Only a small minority (4%) of respondents were training within Academic Clinical Fellow posts.
68% of trainees have commenced training during or after 2007 when the Modernising Medical
Careers system was introduced. 29% of trainees are currently using the pre-2007 Clinical Oncology training curriculum. Only 16% stated that they are using the 2007 curriculum, and 49% are using the new 2010 curriculum.
Trainees yet to pass the final FRCR exam who have continued to use earlier versions of the
curriculum cited various reasons, including a feeling that „switching‟ would create additional time pressures at work, a lack of awareness of the new curriculum or any clear benefit provided by switching, and a reluctance to change in the later years of training. A number of trainees stated that they had not been provided with any information on the new curriculum and were unsure as to whether it was necessary for them to change.
9 Conclusion The 2011 ORF survey is the most comprehensive survey to date of Clinical Oncology trainees with a
71.5% response rate. This has enabled us to produce the above report which is a thorough evaluation of current Clinical Oncology training in the UK. As with the 2009 survey, this report will be widely disseminated throughout the UK to trainees and trainers and will be discussed at the appropriate RCR meetings as we constantly strive to improve training.
The ORF would like to thank all those involved in designing the survey and analysing the results as
well as those who took the time to complete the survey. Work on the next survey has already begun. While we still wish to cover a wide variety of topics, we plan to try to make some of the questions more focused which will hopefully reduce the amount of time required to complete it and improve our response rates even further.
32
Appendix
List of Tables and Charts
Figure Type Content Page Number
Education
1.1 Chart Bleep free teaching 4
1.2 Chart Supervisor support to attend teaching sessions 5
1.3 Chart Time dedicated to formal teaching 5
1.4 Table Usefulness of different teaching formats 5
1.5 Chart Image interpretation 6
1.6 Table Quality of practical experience 7
1.7 Chart Prescribing of chemotherapy 7
1.8 Chart Competence in conventional simulator planning 9
1.9 Chart Competence in virtual simulator planning 9
1.10 Chart Competence in CT planning 9
Examinations
2.1 Chart Percentage of SBA questions answered in the First FRCR Examination 11
2.2 Chart Percentage of SBA questions answered in the Final FRCR Part A Exam 12
Training Programmes & Assessment Practices
3.1 Chart Rating of training programmes 13
3.2 Table Levels of support 13
3.3 Table Assessment and appraisal experience 14
3.4 Chart Frequency of ePortfolio usage 14
3.5 Table Frequency of workplace based assessment usage 14
3.6 Table Attributes of workplace based assessments 15
3.7 Table Audit 15
3.8 Chart Annual study budgets 16
3.9 Chart Additional qualifications undertaken 16
Regional Clinical Oncology Service Commitments
4.1 Chart Reasons for gaps in training rotas 17
4.2 Chart Ward rounds performed with the attending consultant 18
4.3 Chart Ward rounds performed independent of consultant supervision 18
4.4 Chart Time spent on an Oncology Ward Registrar rota 19
4.5 Table Views on Oncology Ward Registrar systems 19
4.6 Chart Frequency of on-call commitment 20
4.7 Chart Hospital at Night and exams 21
4.8 Table Hospital at Night and benefit to training 21
4.9 Chart Years of training involved in Hospital at Night 21
4.10 Chart Hospital Night and years since completion of core medical training 22
4.11 Table Hospital at Night and acute general medical skills 22
Research & Out of Programme Activities
5.1 Chart Areas of out of programme activities 24
5.2 Chart Funding of out of programme posts 25
5.3 Chart Salary arrangements of those out of programme 25
5.4 Chart Intentions of those not currently out of programme 26
Royal College of Radiologists & the Oncology Registrars’ Forum
6.1 Chart Awareness of the ORF section of the College website 28
6.2 Chart Usage of the ORF section of the College website 28
Career, Work/Life Balance & Less than Full-Time Training
7.1 Chart Less than full time working arrangements 29
7.2 Chart Work/life balance and morale 30