
DR. UMESH KHANNA MUMBAI NASH and nonalcoholic liver disease NASH – NonAlcoholic SteatoHepatitis.

Obstructive Sleep Apnea and Hypoxemia Are Associated with AdvancedLiver Histology in Pediatric Nonalcoholic Fatty Liver Disease
Shikha S. Sundaram, MD, MSCI1, Ronald J. Sokol, MD1, Kelley E. Capocelli, MD2, Zhaoxing Pan, PhD3, Jillian S. Sullivan, MD1,
Kristen Robbins1, and Ann C. Halbower, MD4
Objective To determine whether obstructive sleep apnea (OSA) and/or nocturnal hypoxemia are associated withthe severity of liver injury in patients with pediatric nonalcoholic fatty liver disease (NAFLD).Study design Obese children aged 10-18 years with liver biopsy–proven NAFLD were enrolled. Demographic,clinical, and laboratory data were collected, polysomnographywas performed, and liver histology was scored. Sub-jects were divided into those with OSA/hypoxemia and those without OSA/hypoxemia for analysis.Results Of 25 subjects with NAFLD, OSA/hypoxemia was present in 15 (60%) (mean age, 12.8 � 1.9 years; 68%male; 88% Hispanic; mean body mass index z-score, 2.3 � 0.3). Subjects with and without OSA/hypoxemia hadsimilar levels of serum aminotransferases, serum lipids, and inflammatory and insulin resistance markers. Althoughthere were no differences between groups in the histological severity of steatosis, inflammation, ballooning degen-eration, NAFLD activity score, or histological grade, subjects with OSA/hypoxemia had significantly more severehepatic fibrosis. Moreover, oxygen saturation nadir during polysomnography was related to hepatic fibrosis stage(r = �0.49; P = .01) and aspartate aminotransferase level (r = 0.42; P < .05). Increasing percentage of time withoxygen saturation #90% was related to NAFLD inflammation grade (r = 0.44; P = .03), degree of hepatic steatosis(r =�0.50; P = .01), NAFLD activity score (r = 0.42; P = .04), aspartate aminotransferase level (r = 0.56; P = .004), andalanine aminotransferase level (r = 0.44; P = .03).Conclusion Moderate OSA/hypoxemia is common in pediatric patients with biopsy-proven NAFLD. OSA andthe severity/duration of hypoxemia are associated with biochemical and histological measures of NAFLD severity.(J Pediatr 2014;164:699-706).
See editorial, p 684 andrelated article, p 707
onalcoholic fatty liver disease (NAFLD) is a clinicopathological condition characterized by abnormal lipid deposition
N in hepatocytes in the absence of excess alcohol intake. The most common chronic liver disease affecting both childrenand adults, NAFLD is associated with the obesity epidemic.1 NAFLD comprises a spectrum of diseases, ranging from
isolated hepatic steatosis to nonalcoholic steatohepatitis (NASH), defined as steatosis, hepatocyte ballooning, and inflamma-tion, which can be associated with fibrosis and may progress to cirrhosis.1
NAFLD affects up to 9.6% of all children and 38% of obese children.2 Although isolated hepatic steatosis may have nosignificant consequences, NASH may progress to liver fibrosis and cirrhosis in approximately 20% of cases and is associatedwith hepatocellular carcinoma in adults.1,3 Risk factors for pediatric NAFLD include Hispanic race, male sex, insulin resistance,and obesity.4
From the 1Section of Gastroenterology, Hepatology, andNutrition, Department of Pediatrics and the DigestiveHealth Institute, Children’s Hospital Colorado and
2
Obstructive sleep apnea (OSA), characterized by recurrent partial or completeupper airway obstruction during sleep, affects 1.2%-5.7% of the general pediatricpopulation.5-12 In addition, a relationship between obesity and OSA has beendemonstrated in 2 large population-based studies using polysomnography.5,10
UniversityofColoradoSchool ofMedicine; DepartmentofPathology, Children’s Hospital Colorado and University ofColoradoSchoolofMedicine; 3DepartmentofBiostatisticsand Informatics, Colorado School of Public Health; and4Pulmonary Section, Department of Pediatrics, Children’sHospital Colorado and University of Colorado School ofMedicine, Aurora, CO
Supported by the National Institutes of Health (NIH; K23DK085150-02), the Ruth L. Kirschstein NationalResearch Service Award (5T32DK067009), CysticFibrosis Foundation Clinical Fellowship Award (GEI-DER08B0), and NIH/National Center for AdvancingTranslational Sciences Colorado (Clinical and Transla-tional Science Award UL1TR000154). Its contents are theauthors’ sole responsibility and do not necessarilyrepresent official NIH views. The authors declare noconflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2014 Mosby Inc.
All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2013.10.072
AHI Apnea hypopnea index
ALT Alanine aminotransferase
AST Aspartate aminotransferase
BMI Body mass index
HPF High-power field
NAFLD Nonalcoholic fatty liver disease
NAS Nonalcoholic fatty liver disease activity score
NASH Nonalcoholic steatohepatitis
OSA Obstructive sleep apnea
REM Rapid eye movement
SaO2 Oxygen saturation
699

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 164, No. 4
Symptoms of OSA include daytime sleepiness, poor schoolperformance, and snoring, though many children are asymp-tomatic. Affected patients experience repeated episodes ofnocturnal hypoxemia alternating with normoxia (so-called“chronic intermittent hypoxemia”), resembling the patho-physiological mechanisms involved in ischemia/reperfusiontissue injury.13,14
The relationship between NAFLD and OSA extendsbeyond their simple coexistence as obesity-related comorbid-ities. Obese mice fed a high-fat and high-cholesterol dietdevelop steatosis and, when exposed to chronic intermittenthypoxia, demonstrate significant increases in alanine amino-transferase (ALT) level, hepatic inflammation, andfibrosis.15,16 Elevated serum aminotransferase (ALT andaspartate aminotransferase [AST]) levels are present in20%-50% of adults with OSA,11-13 and there is an increasedprevalence of OSA in adults with NASH. In addition,morbidly obese adults with moderate to severe OSA and hyp-oxemia have more histologically severe hepatic inflammationcompared with those with OSA without hypoxemia.17
Precious little is known about the relationship of sleep-disordered breathing and pediatric NAFLD, however. A sin-gle study from a selected sleep medicine clinic populationfound OSA in 91% of obese children with elevated serumaminotransferase levels, although liver histology was notevaluated.18,19
Given that oxidative stress induced by hypoxia/reoxygena-tion is a potential factor in the progression from fatty liver toNASH, we conducted the present study to explore the rela-tionship between pediatric NAFLD and sleep-disorderedbreathing. We hypothesized that OSA and/or nocturnal hyp-oxemia would be associated with the severity of biochemicalor histological evidence of liver injury in patients with pedi-atric NAFLD.
Methods
Pediatric patients receiving care at the Children’s HospitalColorado Pediatric Liver Center between June 2009 andJanuary 2013 were enrolled if they had suspected NAFLDand were scheduled to undergo a clinically indicated liverbiopsy (Figure 1; available at www.jpeds.com). In ourcenter, NAFLD is suspected in overweight or obesechildren (body mass index [BMI] >85% for age and sex)with chronically elevated serum aminotransferase levels andnegative screening results for Wilson disease, autoimmunehepatitis, viral hepatitis, and alpha-1 antitrypsin deficiency.
The study subjects were males and females aged 8-18 yearsand at Tanner stage 2-4. This Tanner stage range was chosento minimize variations in insulin sensitivity that couldpossibly confound the interpretation of potential associa-tions between OSA/hypoxia and NAFLD. Exclusion criteriaincluded a history of Wilson disease, alpha-1 antitrypsindeficiency, viral hepatitis, autoimmune hepatitis, anotherknown chronic liver disease, or cholelithiasis, as well as theuse of anticonvulsants, sedatives, oral or intravenous ste-roids, drugs that promote or reduce insulin resistance
700
(including insulin sensitizers, thiazolidenediones, andmetformin), or medications known to induce hepatic steato-sis (eg, steroids, amiodarone, total parenteral nutrition) inthe previous 2 weeks. Additional exclusion criteria includedcurrent use of continuous positive airway pressure, insulin-dependent diabetes, regular tobacco or alcohol use, a neuro-muscular disorder, or a genetic or craniofacial abnormality.This study was approved by the Colorado Multiple Institu-tional Review Board. Informed consent was obtained fromparents/guardians, and written assent was obtained fromall subjects.Demographic and medical history data, including results
of clinical testing for autoimmune hepatitis, alpha-1 anti-trypsin deficiency, Wilson disease, and viral hepatitis, andabdominal ultrasound or computed tomography imagingdata were obtained. Subjects were asked about clinical symp-toms of sleep apnea (ie, snoring, witnessed apnea, nonrestor-ative sleep, and daytime sleepiness). Height, weight, andwaist and hip circumferences were measured, and BMI wascalculated. BMI z-scores were determined based on age andsex using Centers for Disease Control and Preventiondata.20 Waist measurements were obtained at the midpointbetween the highest point of the iliac crest and the lowestpart of the costal margin. Hip measurements were obtainedat the fullest part of the hips.Liver biopsy specimens were obtained for clinical indica-
tions by a standard percutaneous technique. Liver histology(hematoxylin and eosin and Masson trichrome stain) wasreviewed and scored by a single pediatric pathologist blindedto patient information. Biopsy specimens with histologicallyconfirmed NAFLD (defined as$5% of hepatocytes contain-ing macrovesicular fat) were assigned a grade of necroinflam-mation (0-3) and a stage of fibrosis (0-4) based on thestandard histological criteria of Brunt et al.21 Biopsy speci-mens were also scored for the following criteria establishedby the NASH Clinical Research Network22: steatosis (grade0, <5 % of hepatocytes containing macrovesicular fat; grade1, 5%-33%; grade 2, 34%-66%; grade 3, >66%); lobularinflammation (grade 0, no foci of inflammation; grade 1,<2 foci per high-power field [HPF]; grade 2, 2-4 foci perHPF; grade 3, >4 foci per HPF); ballooning degeneration(grade 0, none; grade 1, few balloon cells; grade 2, many/prominent balloon cells). An NAFLD activity score (NAS)was calculated by summing the scores for steatosis, lobularinflammation, and ballooning degeneration.22 Fibrosis wasscored as stage 0 (none), stage 1a (mild perisinusoidal), stage1b (moderate perisinusoidal), stage 1c (portal/periportalfibrosis only), stage 2 (zone 3 and periportal), stage 3(bridging fibrosis), or stage 4 (cirrhosis).20 Subjects werealso classified as type 1 NASH (classic adult pattern), type 2NASH (portal-based), or an overlap of the 2 NASH histolog-ical subtypes.23
Subjects with histologically confirmed NAFLD underwenta standard multichannel sleep study (polysomnography),which was scored by a research-trained technician and inter-preted by a single sleep medicine physician, both of whomwere masked to liver biopsy results. The following data were
Sundaram et al

April 2014 ORIGINAL ARTICLES
analyzed: total sleep time, percent of rapid eye movement(REM) sleep, apnea/hypopnea index (AHI), oxygen nadir,percent of time at an oxygen saturation (SaO2) #90% and#95%, end-tidal CO2 time >50mmHg, oxygen desaturationindex (the drop in SaO2 to below 95% as discerned by pulseoximetry), and arousal index. The presence of OSA wasdefined as an AHI >1.0, indicating total apneas and hypo-pneas per hour of total sleep time.24,25 Apnea was defined ascessation of airflow over 2 or more attempted respiratorycycles, and hypopnea was defined as a decrease in nasal pres-sure of$50%, with a corresponding decrease in SaO2 of$3%and/or arousal. Hypoxemia was defined as SaO2 <90% for$1% of total sleep time.
The morning after the sleep study, fasting blood specimenswere obtained for ALT, AST, gamma glutamyl transpepti-dase, ultrasensitive C-reactive protein, lipid profile (ie, totalcholesterol, triglycerides, and high-density lipoprotein),glucose, and insulin. Fasting glucose and insulin levels wereused to estimate insulin resistance at baseline using the ho-meostasis model assessment of insulin resistance.26
Statistical analyses were performed using SAS 9.3 (SASInstitute, Cary, North Carolina). Descriptive statistics arepresented as mean � SD for continuous measures and asnumber and percentage for categorical responses. The2-sample t test, c2 test, or Fisher exact test was used as appro-priate to assess the differences between subjects with andwithout OSA/hypoxemia. The Pearson correlation coeffi-cient was applied to quantify the correlations of ALT level,AST level, and histological parameters with polysomno-graphic parameters. Arcsine-root transformation was appliedto proportional-type polysomnography data, such as percenttime with SaO2 <90%; results, however, are presented in theoriginal scale for ease of interpretation. A P value <.05 wasconsidered to indicate statistical significance.
Results
The study group comprised 25 obese subjects with liverbiopsy-confirmed NAFLD. Their mean age was 12.8 � 1.9years, 17 were male (68%), 22 were Hispanic (88%), with amean BMI z score of 2.3 � 0.3 (Table). There were nodifferences in personal or family history of diabetes,hypertension, autoimmune disease, liver disease, OSA, orobesity between the subjects with OSA/hypoxemia andthose without OSA/hypoxemia (Table). The 2 groups ofsubjects had similarly elevated levels of ALT, AST,triglycerides, high-density lipoprotein, and inflammatorymarkers, along with evidence of insulin resistance (Table);however, total serum cholesterol concentration was higherin those with OSA/hypoxemia (P = .03). None of thesubjects had evidence of gallstone disease on abdominalimaging.
Fifteen subjects (60%) met the study criteria for OSA and/or hypoxemia, including 1 with isolated hypoxemia, 4 withisolated OSA, and 10 with both OSA and hypoxemia. Thesubjects with confirmed OSA/hypoxemia reported moresnoring (P = .045), but otherwise had similar symptoms of
Obstructive Sleep Apnea and Hypoxemia Are Associated with AdLiver Disease
sleep-disordered breathing as those without OSA/hypoxemia(Table). The polysomnograms were of adequate durationand the time spent in REM sleep (>12% of total sleeptime) was adequate for these to be considered valid studies(Table), with similar mean total sleep time and percentREM sleep in the 2 groups. The mean AHI was 9.7 � 7.8subjects with OSA/hypoxemia, compared with 1.0 � 0.7 insubjects without OSA/hypoxemia (P = .0007), indicatingmoderate to severe OSA in the affected subjects. Thesubjects with OSA/hypoxemia also had significantly loweroxygen nadirs (81.7% � 5.1% vs 88.3% � 3.4%; P = .002)and percentage of sleep time with an SaO2 <90% (3.5% �4.5% vs 0.4% � 0.8%; P = .03) compared with thosewithout OSA/hypoxemia. These differences were notexplained by differences in age, sex, ethnicity, BMI, orclinical symptoms (P = not significant for all).Of the 25 enrolled subjects with NAFLD, 64% had defini-
tive NASH (NAS $5). There was no difference in the preva-lence of OSA/hypoxemia between subjects with definitiveNASH and those without definitive NASH. Liver histologyanalysis revealed no significant differences in the severity ofsteatosis, inflammation, ballooning degeneration, NAS(mean NAS, 4.93 � 1.2 vs 4.9 � 1.1), or histological grade(Figure 2, A); however, the subjects with OSA/hypoxemiahad significantly more advanced hepatic fibrosis (Figure 2,B). More than one-half (53%) of the subjects with OSA/hypoxemia had stage 2 or greater fibrosis, compared with10% of those without OSA/hypoxemia (P = .03). Therewere no differences in the distribution of type 1 and type 2NASH patterns between those with OSA/hypoxemia andthose without OSA/hypoxemia.Wenext examined the relationship (ie, r values) between key
polysomnography measurements and AST and ALT in allenrolled subjects. We found a significant correlation betweenworsening oxygen nadir and elevated AST level (r = �0.42; P= .04), along with a trend toward a significant relationshipwith ALT level (r = �0.36; P = .08) (Figure 3, A and B). Anincreasing percentage of time with an SaO2 #90%was associated with higher AST (r = 0.56; P = .004) and ALT(r = 0.44; P = .03) levels (Figure 3, C and D). There were nocorrelations between other results of the sleep study (ie, AHIand arousal index) and either AST or ALT level.We next examined the relationships between polysom-
nography measurements and histological parameters. Weidentified a significant correlation between NAFLD fibrosisstage and worsening oxygen nadir (r = �0.49; P = .01;Figure 3, E), along with a trend toward a significantassociation with the percentage of time with an SaO2
#95% (r = 0.37; P = .08). An increasing percentage oftime with an SaO2 #90% (r = 0.43; P = .03; Figure 3, F)or #95% (r = 0.46; P = .02) was associated with a higherNAFLD inflammation grade. In addition, increasingpercentages of time with SaO2 #90% (r = 0.40; P = .05)and #95% (r = 0.58; P = .002) were significantlyassociated with the degree of hepatic steatosis (Figure 3,G). Similarly, significant correlations were seen betweenNAS and increasing percentages of time with an SaO2
vanced Liver Histology in Pediatric Nonalcoholic Fatty 701
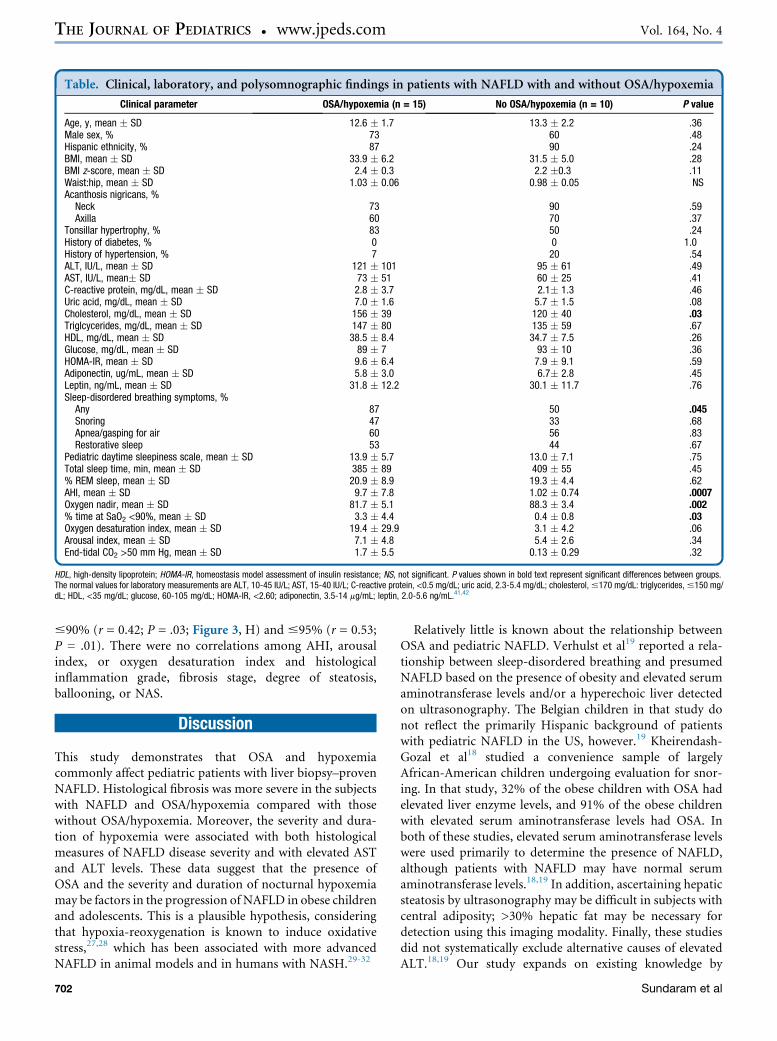
Table. Clinical, laboratory, and polysomnographic findings in patients with NAFLD with and without OSA/hypoxemia
Clinical parameter OSA/hypoxemia (n = 15) No OSA/hypoxemia (n = 10) P value
Age, y, mean � SD 12.6 � 1.7 13.3 � 2.2 .36Male sex, % 73 60 .48Hispanic ethnicity, % 87 90 .24BMI, mean � SD 33.9 � 6.2 31.5 � 5.0 .28BMI z-score, mean � SD 2.4 � 0.3 2.2 �0.3 .11Waist:hip, mean � SD 1.03 � 0.06 0.98 � 0.05 NSAcanthosis nigricans, %Neck 73 90 .59Axilla 60 70 .37
Tonsillar hypertrophy, % 83 50 .24History of diabetes, % 0 0 1.0History of hypertension, % 7 20 .54ALT, IU/L, mean � SD 121 � 101 95 � 61 .49AST, IU/L, mean� SD 73 � 51 60 � 25 .41C-reactive protein, mg/dL, mean � SD 2.8 � 3.7 2.1� 1.3 .46Uric acid, mg/dL, mean � SD 7.0 � 1.6 5.7 � 1.5 .08Cholesterol, mg/dL, mean � SD 156 � 39 120 � 40 .03Triglcycerides, mg/dL, mean � SD 147 � 80 135 � 59 .67HDL, mg/dL, mean � SD 38.5 � 8.4 34.7 � 7.5 .26Glucose, mg/dL, mean � SD 89 � 7 93 � 10 .36HOMA-IR, mean � SD 9.6 � 6.4 7.9 � 9.1 .59Adiponectin, ug/mL, mean � SD 5.8 � 3.0 6.7� 2.8 .45Leptin, ng/mL, mean � SD 31.8 � 12.2 30.1 � 11.7 .76Sleep-disordered breathing symptoms, %Any 87 50 .045Snoring 47 33 .68Apnea/gasping for air 60 56 .83Restorative sleep 53 44 .67
Pediatric daytime sleepiness scale, mean � SD 13.9 � 5.7 13.0 � 7.1 .75Total sleep time, min, mean � SD 385 � 89 409 � 55 .45% REM sleep, mean � SD 20.9 � 8.9 19.3 � 4.4 .62AHI, mean � SD 9.7 � 7.8 1.02 � 0.74 .0007Oxygen nadir, mean � SD 81.7 � 5.1 88.3 � 3.4 .002% time at SaO2 <90%, mean � SD 3.3 � 4.4 0.4 � 0.8 .03Oxygen desaturation index, mean � SD 19.4 � 29.9 3.1 � 4.2 .06Arousal index, mean � SD 7.1 � 4.8 5.4 � 2.6 .34End-tidal CO2 >50 mm Hg, mean � SD 1.7 � 5.5 0.13 � 0.29 .32
HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance; NS, not significant. P values shown in bold text represent significant differences between groups.The normal values for laboratory measurements are ALT, 10-45 IU/L; AST, 15-40 IU/L; C-reactive protein, <0.5 mg/dL; uric acid, 2.3-5.4 mg/dL; cholesterol,#170 mg/dL: triglycerides,#150 mg/dL; HDL, <35 mg/dL; glucose, 60-105 mg/dL; HOMA-IR, <2.60; adiponectin, 3.5-14 mg/mL; leptin, 2.0-5.6 ng/mL.41,42
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 164, No. 4
#90% (r = 0.42; P = .03; Figure 3, H) and #95% (r = 0.53;P = .01). There were no correlations among AHI, arousalindex, or oxygen desaturation index and histologicalinflammation grade, fibrosis stage, degree of steatosis,ballooning, or NAS.
Discussion
This study demonstrates that OSA and hypoxemiacommonly affect pediatric patients with liver biopsy–provenNAFLD. Histological fibrosis was more severe in the subjectswith NAFLD and OSA/hypoxemia compared with thosewithout OSA/hypoxemia. Moreover, the severity and dura-tion of hypoxemia were associated with both histologicalmeasures of NAFLD disease severity and with elevated ASTand ALT levels. These data suggest that the presence ofOSA and the severity and duration of nocturnal hypoxemiamay be factors in the progression of NAFLD in obese childrenand adolescents. This is a plausible hypothesis, consideringthat hypoxia-reoxygenation is known to induce oxidativestress,27,28 which has been associated with more advancedNAFLD in animal models and in humans with NASH.29-32
702
Relatively little is known about the relationship betweenOSA and pediatric NAFLD. Verhulst et al19 reported a rela-tionship between sleep-disordered breathing and presumedNAFLD based on the presence of obesity and elevated serumaminotransferase levels and/or a hyperechoic liver detectedon ultrasonography. The Belgian children in that study donot reflect the primarily Hispanic background of patientswith pediatric NAFLD in the US, however.19 Kheirendash-Gozal et al18 studied a convenience sample of largelyAfrican-American children undergoing evaluation for snor-ing. In that study, 32% of the obese children with OSA hadelevated liver enzyme levels, and 91% of the obese childrenwith elevated serum aminotransferase levels had OSA. Inboth of these studies, elevated serum aminotransferase levelswere used primarily to determine the presence of NAFLD,although patients with NAFLD may have normal serumaminotransferase levels.18,19 In addition, ascertaining hepaticsteatosis by ultrasonography may be difficult in subjects withcentral adiposity; >30% hepatic fat may be necessary fordetection using this imaging modality. Finally, these studiesdid not systematically exclude alternative causes of elevatedALT.18,19 Our study expands on existing knowledge by
Sundaram et al
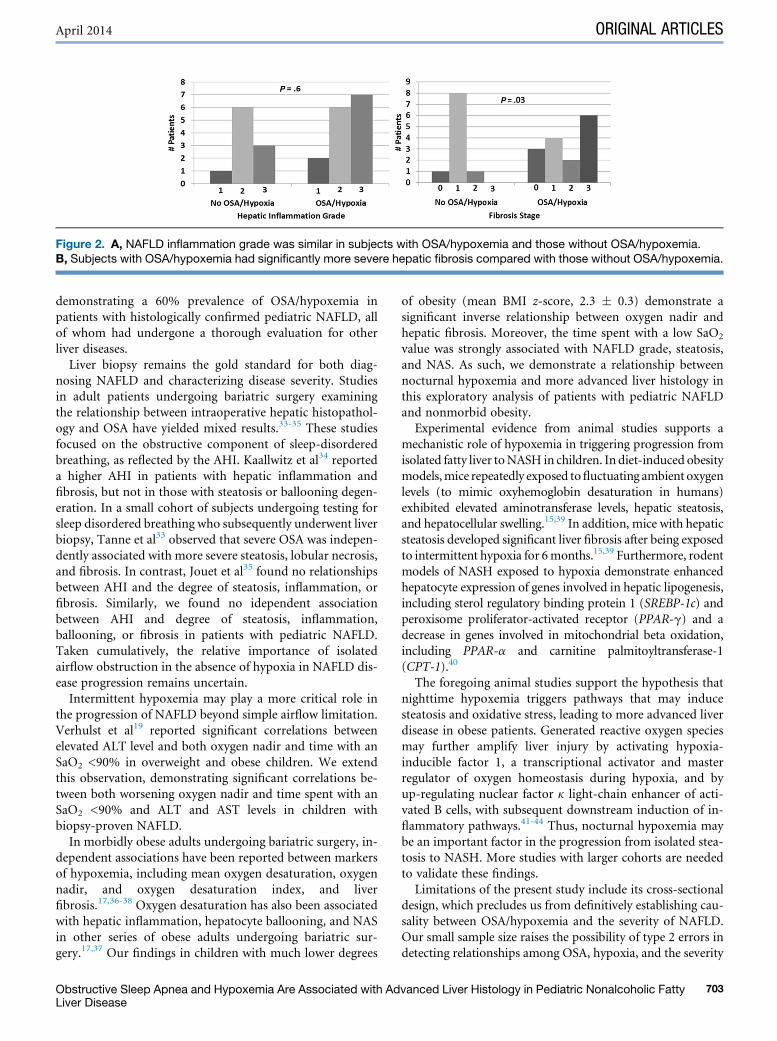
Figure 2. A, NAFLD inflammation grade was similar in subjects with OSA/hypoxemia and those without OSA/hypoxemia.B, Subjects with OSA/hypoxemia had significantly more severe hepatic fibrosis compared with those without OSA/hypoxemia.
April 2014 ORIGINAL ARTICLES
demonstrating a 60% prevalence of OSA/hypoxemia inpatients with histologically confirmed pediatric NAFLD, allof whom had undergone a thorough evaluation for otherliver diseases.
Liver biopsy remains the gold standard for both diag-nosing NAFLD and characterizing disease severity. Studiesin adult patients undergoing bariatric surgery examiningthe relationship between intraoperative hepatic histopathol-ogy and OSA have yielded mixed results.33-35 These studiesfocused on the obstructive component of sleep-disorderedbreathing, as reflected by the AHI. Kaallwitz et al34 reporteda higher AHI in patients with hepatic inflammation andfibrosis, but not in those with steatosis or ballooning degen-eration. In a small cohort of subjects undergoing testing forsleep disordered breathing who subsequently underwent liverbiopsy, Tanne et al33 observed that severe OSA was indepen-dently associated with more severe steatosis, lobular necrosis,and fibrosis. In contrast, Jouet et al35 found no relationshipsbetween AHI and the degree of steatosis, inflammation, orfibrosis. Similarly, we found no idependent associationbetween AHI and degree of steatosis, inflammation,ballooning, or fibrosis in patients with pediatric NAFLD.Taken cumulatively, the relative importance of isolatedairflow obstruction in the absence of hypoxia in NAFLD dis-ease progression remains uncertain.
Intermittent hypoxemia may play a more critical role inthe progression of NAFLD beyond simple airflow limitation.Verhulst et al19 reported significant correlations betweenelevated ALT level and both oxygen nadir and time with anSaO2 <90% in overweight and obese children. We extendthis observation, demonstrating significant correlations be-tween both worsening oxygen nadir and time spent with anSaO2 <90% and ALT and AST levels in children withbiopsy-proven NAFLD.
In morbidly obese adults undergoing bariatric surgery, in-dependent associations have been reported between markersof hypoxemia, including mean oxygen desaturation, oxygennadir, and oxygen desaturation index, and liverfibrosis.17,36-38 Oxygen desaturation has also been associatedwith hepatic inflammation, hepatocyte ballooning, and NASin other series of obese adults undergoing bariatric sur-gery.17,37 Our findings in children with much lower degrees
Obstructive Sleep Apnea and Hypoxemia Are Associated with AdLiver Disease
of obesity (mean BMI z-score, 2.3 � 0.3) demonstrate asignificant inverse relationship between oxygen nadir andhepatic fibrosis. Moreover, the time spent with a low SaO2
value was strongly associated with NAFLD grade, steatosis,and NAS. As such, we demonstrate a relationship betweennocturnal hypoxemia and more advanced liver histology inthis exploratory analysis of patients with pediatric NAFLDand nonmorbid obesity.Experimental evidence from animal studies supports a
mechanistic role of hypoxemia in triggering progression fromisolated fatty liver toNASH in children. In diet-induced obesitymodels,mice repeatedly exposed tofluctuating ambient oxygenlevels (to mimic oxyhemoglobin desaturation in humans)exhibited elevated aminotransferase levels, hepatic steatosis,and hepatocellular swelling.15,39 In addition, mice with hepaticsteatosis developed significant liver fibrosis after being exposedto intermittent hypoxia for 6months.15,39 Furthermore, rodentmodels of NASH exposed to hypoxia demonstrate enhancedhepatocyte expression of genes involved in hepatic lipogenesis,including sterol regulatory binding protein 1 (SREBP-1c) andperoxisome proliferator-activated receptor (PPAR-g) and adecrease in genes involved in mitochondrial beta oxidation,including PPAR-a and carnitine palmitoyltransferase-1(CPT-1).40
The foregoing animal studies support the hypothesis thatnighttime hypoxemia triggers pathways that may inducesteatosis and oxidative stress, leading to more advanced liverdisease in obese patients. Generated reactive oxygen speciesmay further amplify liver injury by activating hypoxia-inducible factor 1, a transcriptional activator and masterregulator of oxygen homeostasis during hypoxia, and byup-regulating nuclear factor k light-chain enhancer of acti-vated B cells, with subsequent downstream induction of in-flammatory pathways.41-44 Thus, nocturnal hypoxemia maybe an important factor in the progression from isolated stea-tosis to NASH. More studies with larger cohorts are neededto validate these findings.Limitations of the present study include its cross-sectional
design, which precludes us from definitively establishing cau-sality between OSA/hypoxemia and the severity of NAFLD.Our small sample size raises the possibility of type 2 errors indetecting relationships among OSA, hypoxia, and the severity
vanced Liver Histology in Pediatric Nonalcoholic Fatty 703

Figure 3. Correlations between key polysomnographic paraemteres and AST, ALT, and liver histology in subjects with NAFLD.A, Lower SaO2 nadir correlated with higher AST. B, Lower SaO2 nadir trended to correlate with higher ALT. C, Greater time withan SaO2 <90% correlated with higher AST. D, Greater time with an SaO2 <90% correlated with higher ALT. E, Lower SaO2 nadircorrelated with higher fibrosis stage. F, Greater time with an SaO2 <90% correlated with higher inflammation grade. G, Greatertime with an SaO2 <90% correlated with higher degree of steatosis. H,Greater time with an SaO2 <90% correlated with a worseNAS. Regression lines were calculated by arcsine-root transformation.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 164, No. 4
704 Sundaram et al

April 2014 ORIGINAL ARTICLES
of NAFLD. Although this largely Hispanicmale cohort of sub-jects reflects the demographics of pediatric NAFLD in the US,these findingsmight not be generalizable to other populations.In addition, our samplemaybebiased towardmore severe liverdisease, given that all enrolled subjects underwent liver biopsyanalysis for clinical indications that included chronicallyelevated serum aminotransferase levels. Further longitudinalstudies are needed to evaluate the effect of treatment ofnocturnal hypoxemia on the severity of NAFLD.
In conclusion, our study demonstrates that OSA/hypox-emia is common in pediatric patients with liver biopsy–proven NAFLD and is associated with more advanced liverinjury and histological disease. Further investigation intothe possible effects prevention or treatment of hypoxia on pa-tients with NAFLD is indicated. n
Submitted for publication May 15, 2013; last revision received Sep 25, 2013;
accepted Oct 24, 2013.
Reprint requests: Shikha S. Sundaram, MD, MSCI, Associate Professor of
Pediatrics, Digestive Health Institute, Children’s Hospital Colorado, 13123 E
16th Ave, B290, Aurora, CO 80045. E-mail: shikha.sundaram@
childrenscolorado.org
References
1. Brunt EM. Nonalcoholic steatohepatitis: definition and pathology.
Semin Liver Dis 2001;21:3-16.
2. Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C.
Prevalence of fatty liver in children and adolescents. Pediatrics 2006;
118:1388-93.
3. Angulo P.Nonalcoholic fatty liver disease.N Engl JMed 2002;346:1221-31.
4. Schwimmer JB. Definitive diagnosis and assessment of risk for nonalco-
holic fatty liver disease in children and adolescents. Semin Liver Dis
2007;27:312-8.
5. Li AM, So HK, Au CT, Ho C, Lau J, Ng SK, et al. Epidemiology of
obstructive sleep apnoea syndrome in Chinese children: a two-phase
community study. Thorax 2010;65:991-7.
6. Gislason T, Benediktsdottir B. Snoring, apneic episodes, and nocturnal
hypoxemia among children 6 months to 6 years old: an epidemiologic
study of lower limit of prevalence. Chest 1995;107:963-6.
7. Mallory GB Jr, Fiser DH, Jackson R. Sleep-associated breathing disorders
in morbidly obese children and adolescents. J Pediatr 1989;115:892-7.
8. Marcus CL, Curtis S, Koerner CB, Joffe A, Serwint JR, Loughlin GM.
Evaluation of pulmonary function and polysomnography in obese chil-
dren and adolescents. Pediatr Pulmonol 1996;21:176-83.
9. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep
apnea: a population health perspective. Am J Respir Crit Care Med
2002;165:1217-39.
10. Bixler EO, Vgontzas AN, Lin HM, Liao D, Calhoun S, Vela-Bueno A,
et al. Sleep- disordered breathing in children in a general population
sample: prevalence and risk factors. Sleep 2009;32:731-6.
11. O’Brien LM, Holbrook CR, Mervis CB, Klaus CJ, Bruner JL, Raffield TJ,
et al. Sleep and neurobehavioral characteristics of 5- to 7-year-old children
with parentally reported symptoms of attention-deficit/hyperactivity dis-
order. Pediatrics 2003;111:554-63.
12. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, et al.
Diagnosis and management of childhood obstructive sleep apnea syn-
drome. Pediatrics 2012;130:e714-55.
13. Henrion J, Colin L, Schapira M, Heller FR. Hypoxic hepatitis caused by
severe hypoxemia from obstructive sleep apnea. J Clin Gastroenterol
1997;24:245-9.
14. Mathurin P, Durand F, Ganne N, Mollo JL, Lebrec D, Degott C, et al.
Ischemic hepatitis due to obstructive sleep apnea. Gastroenterology
1995;109:1682-4.
Obstructive Sleep Apnea and Hypoxemia Are Associated with AdLiver Disease
15. Savransky V, Bevans S, Nanayakkara A, Li J, Smith PL, Torbenson MS,
et al. Chronic intermittent hypoxia causes hepatitis in a mouse model of
diet-induced fatty liver. Am J Physiol Gastrointest Liver Physiol 2007;
293:G871-7.
16. Drager LF, Li J, Reinke C, Bevans-Fonti S, Jun JC, Polotsky VY. Intermit-
tent hypoxia exacerbates metabolic effects of diet-induced obesity.
Obesity 2011;19:2167-74.
17. Polotsky VY, Patil SP, Savransky V, Laffan A, Fonti S, Frame LA, et al.
Obstructive sleep apnea, insulin resistance, and steatohepatitis in severe
obesity. Am J Respir Crit Care Med 2009;179:228-34.
18. Kheirandish-Gozal L, Sans Capdevila O, Kheirandish E, Gozal D.
Elevated serum aminotransferase levels in children at risk for obstructive
sleep apnea. Chest 2008;133:92-9.
19. Verhulst SL, Jacobs S, Aerts L, Schrauwen N, Haentjens D, Rooman RP,
et al. Sleep-disordered breathing: a new risk factor of suspected fatty liver
disease in overweight children and adolescents? Sleep Breath 2009;13:
207-10.
20. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM,
Guo SS, Wei R, et al. CDC growth charts: United States. Adv Data
2000;314:1-27.
21. Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-Tetri BA,
Bacon BR. Nonalcoholic steatohepatitis: a proposal for grading
and staging the histological lesions. Am J Gastroenterol 1999;94:
2467-74.
22. Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ,
Cummings OW, et al. Design and validation of a histological scoring sys-
tem for nonalcoholic fatty liver disease. Hepatology 2005;41:1313-21.
23. Schwimmer JB, Behling C, Newbury R, Deutsch R, Nievergelt C,
Schork NJ, et al. Histopathology of pediatric nonalcoholic fatty liver dis-
ease. Hepatology 2005;42:641-9.
24. Halbower AC, Ishman SL, McGinley BM. Childhood obstructive sleep-
disordered breathing: a clinical update and discussion of technological
innovations and challenges. Chest 2007;132:2030-41.
25. Montgomery-Downs HE, O’Brien LM, Gulliver TE, Gozal D. Polysom-
nographic characteristics in normal preschool and early school-aged
children. Pediatrics 2006;117:741-53.
26. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF,
Turner RC. Homeostasis model assessment: insulin resistance and
beta-cell function from fasting plasma glucose and insulin concentra-
tions in man. Diabetologia 1985;28:412-9.
27. Lavie L. Obstructive sleep apnoea syndrome: an oxidative stress disorder.
Sleep Med Rev 2003;7:35-51.
28. Yamauchi M, Nakano H, Maekawa J, Okamoto Y, Ohnishi Y, Suzuki T,
et al. Oxidative stress in obstructive sleep apnea. Chest 2005;127:1674-9.
29. Albano E, Mottaran E, Occhino G, Reale E, Vidali M. Review article: role
of oxidative stress in the progression of non-alcoholic steatosis. Aliment
Pharmacol Ther 2005;22(Suppl 2):71-3.
30. Nobili V, Parola M, Alisi A, Marra F, Piemonte F, Mombello C, et al.
Oxidative stress parameters in paediatric non-alcoholic fatty liver dis-
ease. Int J Mol Med 2010;26:471-6.
31. Rector RS, Thyfault JP, Uptergrove GM, Morris EM, Naples SP,
Borengasser SJ, et al. Mitochondrial dysfunction precedes insulin resis-
tance and hepatic steatosis and contributes to the natural history of
non-alcoholic fatty liver disease in an obese rodent model. J Hepatol
2010;52:727-36.
32. Rolo AP, Teodoro JS, Palmeira CM. Role of oxidative stress in the path-
ogenesis of nonalcoholic steatohepatitis. Free Radic Biol Med 2012;52:
59-69.
33. Tanne F, Gagnadoux F, Chazouilleres O, Fleury B, Wendum D,
Lasnier E, et al. Chronic liver injury during obstructive sleep apnea. Hep-
atology 2005;41:1290-6.
34. Kallwitz ER, Herdegen J, Madura J, Jakate S, Cotler SJ. Liver enzymes
and histology in obese patients with obstructive sleep apnea. J Clin Gas-
troenterol 2007;41:918-21.
35. Jouet P, Sabate JM, Maillard D, Msika S, Mechler C, Ledoux S, et al.
Relationship between obstructive sleep apnea and liver abnormalities
in morbidly obese patients: a prospective study. Obes Surg 2007;17:
478-85.
vanced Liver Histology in Pediatric Nonalcoholic Fatty 705

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 164, No. 4
36. Newton JL, Day CP, Gibson G, Tomlinson M, Henderson E. Recurrent
nocturnal hypoxemia is associated with progressive non-alcoholic fatty
liver disease (NAFLD). Hepatology 2008;48(4 Suppl):808A.
37. Aron-Wisnewsky J, Minville C, Tordjman J, Levy P, Bouillot JL,
Basdevant A, et al. Chronic intermittent hypoxia is a major trigger for
non-alcoholic fatty liver disease in the morbidly obese. J Hepatol 2012;
56:225-33.
38. Mishra P, Nugent C, Afendy A, Bai C, Bhatia P, Afendy M, et al. Ap-
noeic-hypopnoeic episodes during obstructive sleep apnoea are associ-
ated with histological nonalcoholic steatohepatitis. Liver Int 2008;28:
1080-6.
39. Savransky V, Nanayakkara A, Vivero A, Li J, Bevans S, Smith PL, et al.
Chronic intermittent hypoxia predisposes to liver injury. Hepatology
2007;45:1007-13.
50 Years Ago in THE JOURNAL OF PEDIATRICS
706
40. Piguet AC, Stroka D, Zimmermann A, Dufour JF. Hypoxia aggravates
non-alcoholic steatohepatitis in mice lacking hepatocellular PTEN.
Clin Sci 2010;118:401-10.
41. Culver C, Sundqvist A, Mudie S, Melvin A, Xirodimas D, Rocha S.
Mechanism of hypoxia-induced NF-kappaB. Mol Cell Biol 2010;30:
4901-21.
42. Dimova EY, Kietzmann T. Hypoxia-inducible factors: post-translational
crosstalk of signaling pathways. Methods Mol Biol 2010;647:215-36.
43. He G, Karin M. NF-kappaB and STAT3: key players in liver inflamma-
tion and cancer. Cell Res 2011;21:159-68.
44. Qu A, Taylor M, Xue X, Matsubara T, Metzger D, Chambon P, et al.
Hypoxia-inducible transcription factor 2alpha promotes steatohepatitis
through augmenting lipid accumulation, inflammation, and fibrosis.
Hepatology 2011;54:472-83.
The Roentgen Appearance of the Chest in Acute Glomerulonephritis in ChildrenKirkpatrick JA, Fleisher DS. J Pediatr 1964;64:492-8
Kirkpatrick and Fleishermade a novel radiographic observation in childrenwith acute glomerulonephritis (AGN) andrespiratory distress admitted to St Christopher’s Hospital for Children in the later 1950s, and then systematically
studiedpatientswithAGNbothwith andwithout respiratory symptoms.This report includes the 76 childrenhospitalizedbetween 1956 and 1961. Patients had proven or presumed postinfectious (usually poststreptococcal) AGN. Sixty-five ofthe 76 patients (86%) had abnormalities noted on plain chest radiograph, most frequently cardiomegaly and pulmonaryvascular prominence, indistinctness, and varying degrees of pulmonary edema. Although not pathognomonic, thenuanced finding of pulmonary vascular abnormalities out of proportion to cardiomegaly, suggesting pathophysiologybeyond mere volume overload and distinct from primary cardiac dysfunction, has diagnostic value. Not all patientswith the radiographic findings had hypertension, skin edema, renal failure, or even hematuria at the time of the radio-graphic observations.
It is not entirely clear whether the pulmonary edema in AGN is related to arterial hypertension, increased capillarypermeability, excessive renal reabsorption of sodium and water, some other factors, or a combination of factors.
At the time of this report, 15 or more new cases of AGN were admitted annually at St Christopher’s Hospital. Thiswriter “teethed” on these cases and other spectacular observations of John Kirkpatrick (who later became Chief ofRadiology at the Children’s Hospital Boston). With the rate of AGN diminishing to only 1 or 2 cases annually atSt Christopher’s Hospital—with familiarity and recognition by house staff and younger physicians and radiologistswaning as well—the simple radiographic findings in more than one enigmatic case have led this writer to raise theunsuspected correct diagnosis of AGN, validating our venerated mentor’s concluding line in this 50-year-old article:“These roentgen findings add another dimension to the spectrum of this disease and can be of diagnostic value.”
Sarah S. Long, MDDepartment of Pediatrics
St Christopher’s Hospital for ChildrenPhiladelphia, Pennsylvania
http://dx.doi.org/10.1016/j.jpeds.2013.10.039
Sundaram et al

Figure 1. A CONSORT diagram of subject enrollment into the study. CPAP, continuous positive airway pressure.
April 2014 ORIGINAL ARTICLES
Obstructive Sleep Apnea and Hypoxemia Are Associated with Advanced Liver Histology in Pediatric Nonalcoholic FattyLiver Disease
706.e1


















