Insights into Nonalcoholic Fatty-Liver Disease Heterogeneity
14
Insights into Nonalcoholic Fatty-Liver Disease Heterogeneity Marco Arrese, MD 1,2 Juan P. Arab, MD 1,2 Francisco Barrera, MD 1,2 Benedikt Kaufmann, MD 3 Luca Valenti, MD 4 Ariel E. Feldstein, MD 3 1 Department of Gastroenterology, Escuela de Medicina, Ponti ficia Universidad Católica de Chile, Santiago, Chile 2 Centro de Envejecimiento y Regeneración (CARE), Departamento de Biología Celular y Molecular, Facultad de Ciencias Biologicas, Pontificia Universidad Catolica de Chile, Santiago, Chile 3 Department of Pediatric Gastroenterology, Rady Children’s Hospital, University of California San Diego, California 4 Department of Pathophysiology and Transplantation, Universita degli Studi di Milano, Translational Medicine, Department of Transfusion, Medicine and Hematology, Fondazione IRCCS Ca’ Granda, Pad Marangoni, Milan, Italy Semin Liver Dis 2021;41:421–434. Address for correspondence Marco Arrese, MD, Department of Gastroenterology, Escuela de Medicina, Ponti ficia Universidad Católica de Chile, Diagonal Paraguay #362, 8330077 Santiago, Chile (e-mail: [email protected]). Ariel E. Feldstein, MD, Division of Pediatric Gastroenterology Hepatology and Nutrition, UCSD 3020 Children’s Way, MC 5030, San Diego, CA 92103-8450 (e-mail: [email protected]). Nonalcoholic fatty-liver disease (NAFLD) is currently con- sidered the commonest liver disease worldwide with an estimated global prevalence of 25%. 1,2 The acronym refers to a range of hepatic histological alterations including isolated steatosis (also referred as NAFL), non-alcoholic streatohepatitis (NASH which is hallmarked by the pres- ence of hepatocellular injury accompanied by inflamma- tion and variable degrees of fibrosis), and cirrhosis. 3 Importantly, NAFLD is a risk factor for hepatocellular carcinoma (HCC) development even in the absence of cirrhosis. 4 NAFLD relevance is underscored by data point- ing to NAFLD as the most fast-growing cause of cirrhosis and the need liver transplantation in the United States. 5 Moreover, epidemiological figures are worrisome as, according to epidemiological modeling, NAFLD burden is expected to grow in the coming decades burdening health care systems and causing substantial economic costs and compromising individual health, determining significant morbidity and mortality. 6 To date, dietary caloric restriction and exercise are the cornerstone of NAFLD therapy, and although these measures have been proven to be efficacious, therapeutic goals are difficult to achieve or sustain. 7–9 Unfortunately, no Food and Drug Administration (FDA)-approved therapies for NAFLD Keywords ► nonalcoholic fatty- liver disease ► steatosis ► cirrhosis ► fibrosis ► nonalcoholic ► steatohepatitis ► NAFLD ► NASH ► metabolic syndrome ► heterogeneity Abstract The acronym nonalcoholic fatty-liver disease (NAFLD) groups a heterogeneous patient population. Although in many patients the primary driver is metabolic dysfunction, a complex and dynamic interaction of different factors (i.e., sex, presence of one or more genetic variants, coexistence of different comorbidities, diverse microbiota composi- tion, and various degrees of alcohol consumption among others) takes place to determine disease subphenotypes with distinct natural history and prognosis and, eventually, different response to therapy. This review aims to address this topic through the analysis of existing data on the differential contribution of known factors to the pathogenesis and clinical expression of NAFLD, thus determining the different clinical subphenotypes observed in practice. To improve our understanding of NAFLD heterogeneity and the dominant drivers of disease in patient subgroups would predictably impact on the development of more precision-targeted therapies for NAFLD. published online July 7, 2021 DOI https://doi.org/ 10.1055/s-0041-1730927. ISSN 0272-8087. © 2021. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/ licenses/by-nc-nd/4.0/) Thieme Medical Publishers, Inc., 333 Seventh Avenue, 18th Floor, New York, NY 10001, USA THIEME 421 Published online: 2021-07-07
Transcript of Insights into Nonalcoholic Fatty-Liver Disease Heterogeneity

Insights into Nonalcoholic Fatty-Liver DiseaseHeterogeneityMarco Arrese, MD1,2 Juan P. Arab, MD1,2 Francisco Barrera, MD1,2 Benedikt Kaufmann, MD3
Luca Valenti, MD4 Ariel E. Feldstein, MD3
1Department of Gastroenterology, Escuela de Medicina, PontificiaUniversidad Católica de Chile, Santiago, Chile
2Centro de Envejecimiento y Regeneración (CARE), Departamento deBiología Celular y Molecular, Facultad de Ciencias Biologicas,Pontificia Universidad Catolica de Chile, Santiago, Chile
3Department of Pediatric Gastroenterology, Rady Children’sHospital, University of California San Diego, California
4Department of Pathophysiology and Transplantation, Universitadegli Studi di Milano, Translational Medicine, Department ofTransfusion, Medicine and Hematology, Fondazione IRCCS Ca’Granda, Pad Marangoni, Milan, Italy
Semin Liver Dis 2021;41:421–434.
Address for correspondence Marco Arrese, MD, Department ofGastroenterology, Escuela de Medicina, Pontificia UniversidadCatólica de Chile, Diagonal Paraguay #362, 8330077 Santiago, Chile(e-mail: [email protected]).
Ariel E. Feldstein, MD, Division of Pediatric GastroenterologyHepatology and Nutrition, UCSD 3020 Children’s Way, MC 5030, SanDiego, CA 92103-8450(e-mail: [email protected]).
Nonalcoholic fatty-liver disease (NAFLD) is currently con-sidered the commonest liver disease worldwide with anestimated global prevalence of 25%.1,2 The acronym refersto a range of hepatic histological alterations includingisolated steatosis (also referred as NAFL), non-alcoholicstreatohepatitis (NASH which is hallmarked by the pres-ence of hepatocellular injury accompanied by inflamma-tion and variable degrees of fibrosis), and cirrhosis.3
Importantly, NAFLD is a risk factor for hepatocellularcarcinoma (HCC) development even in the absence ofcirrhosis.4 NAFLD relevance is underscored by data point-ing to NAFLD as the most fast-growing cause of cirrhosis
and the need liver transplantation in the United States.5
Moreover, epidemiological figures are worrisome as,according to epidemiological modeling, NAFLD burden isexpected to grow in the coming decades burdening healthcare systems and causing substantial economic costs andcompromising individual health, determining significantmorbidity and mortality.6
To date, dietary caloric restriction and exercise are thecornerstone of NAFLD therapy, and although these measureshave been proven to be efficacious, therapeutic goals aredifficult to achieve or sustain.7–9 Unfortunately, no Food andDrug Administration (FDA)-approved therapies for NAFLD
Keywords
► nonalcoholic fatty-liver disease
► steatosis► cirrhosis► fibrosis► nonalcoholic► steatohepatitis► NAFLD► NASH► metabolic syndrome► heterogeneity
Abstract The acronym nonalcoholic fatty-liver disease (NAFLD) groups a heterogeneous patientpopulation. Although in many patients the primary driver is metabolic dysfunction, acomplex and dynamic interaction of different factors (i.e., sex, presence of one or moregenetic variants, coexistence of different comorbidities, diverse microbiota composi-tion, and various degrees of alcohol consumption among others) takes place todetermine disease subphenotypes with distinct natural history and prognosis and,eventually, different response to therapy. This review aims to address this topicthrough the analysis of existing data on the differential contribution of known factorsto the pathogenesis and clinical expression of NAFLD, thus determining the differentclinical subphenotypes observed in practice. To improve our understanding of NAFLDheterogeneity and the dominant drivers of disease in patient subgroups wouldpredictably impact on the development of more precision-targeted therapies forNAFLD.
published onlineJuly 7, 2021
DOI https://doi.org/10.1055/s-0041-1730927.ISSN 0272-8087.
© 2021. The Author(s).This is an open access article published by Thieme under the terms of the
Creative Commons Attribution-NonDerivative-NonCommercial-License,
permitting copying and reproduction so long as the original work is given
appropriate credit. Contents may not be used for commercial purposes, or
adapted, remixed, transformed or built upon. (https://creativecommons.org/
licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc., 333 Seventh Avenue, 18th Floor,New York, NY 10001, USA
THIEME
421
Published online: 2021-07-07

are currently available. Clinical trials conducted so far with amyriad of investigational agents have shown relatively lowrates of response compared with placebo.10 The latter maybe related to several factors11 with disease heterogeneitybeing a relevant aspect. In fact, inclusion criteria for most ofclinical studies is usually based mainly on histological diag-nosis of NAFLD which result in mixed population ofpatients.12 Thus, more granular data on the effectivenessof new therapies in NAFLD subgroups is needed to create theproper grounds for personalized or precision medicineapproaches in the near future.13–15
As mentioned above, the NAFLD acronym groups a het-erogeneous patient population. NAFLD clinical expressionresults from a complex and multilayered dynamic interac-tion of different factors including sex,16 presence of severalgenetic variants,17 coexistence of different comorbidities,18
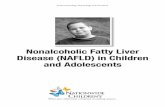
diverse microbiota composition,19–21 and various degrees ofalcohol consumption22 among others. This complex interac-tion results in several disease subphenotypes with distinctnatural history and prognosis and, eventually, differentresponse to therapy (►Fig. 1). Of note, NAFLD heterogeneity
was one of the reasons argued by an expert panel thatsuggested to replace NAFLD by a new acronym derivedfrom the initial letters of metabolic (dysfunction)-associatedfatty-liver disease (i.e., MAFLD). NAFLD renaming was pro-posed aiming to better capture themain driver of the diseasein themajority of patients.23,24However, this suggestion hadnot been universally accepted and a debate on the matter isongoing.25,26 In the present review, we aim to address theissue of NAFLDheterogeneity through the analysis of existingdata on the differential contribution of known factors to theclinical expression of NAFLD. The impact of better decipher-ingNAFLDheterogeneity and the dominant drivers of diseasein patient subgroups on the development of more targetedtherapies for NAFLD is also highlighted.
Role of Genetic Determinants
NAFLD has a strong heritability and during the last year’sgenome-wide association studies (GWAS) have allowed thediscovery of the main common genetic determinants of thiscondition and of the susceptibility to hepatic fat
Fig. 1 The acronym nonalcoholic fatty-liver disease (NAFLD) groups a heterogeneous patient population. The different phenotypes observed inclinical practice stem from a complex and dynamic interaction of different factors (age, sex, reproductive status, presence of one or moregenetic variants and epigenetic factors, a diverse microbiota composition, coexistence of different comorbidities, the degree of alcoholconsumption, and muscle mass and physical activity among other). These variables critically influence NAFLD development and progression.Disease heterogeneity imply that pathophysiological mechanisms underlying NAFLD may have different hierarchy or trajectory in differentpatients defining different subphenotypes which may be relevant to molecular pathway-based therapies. NAFLD heterogeneity may alsoinfluence natural history and prognosis and, eventually, response to therapy.
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.422

accumulation.17 Their common pathogenic mechanismturned out to be the alteration of hepatocellular lipid han-dling, favoring on one hand retention in lipid droplets oversecretion within very-low density lipoproteins and on theother hand synthesis over catabolism.27 Increased quantityand altered composition of lipids determines lipotoxicityand potentially progressive liver disease.27
Identification of patatin-like phospholipase domain-con-taining 3 (PNPLA3) p.I148M and transmembrane 6 super-family member 2 (TM6SF2) p.E167K, as the main riskvariants, allowed soon to pinpoint a subset of patientscarrying multiple variants who are at higher risk of pro-gression to the hepatic rather than to the cardiometaboliccomplications of NAFLD.14,17,28,29 Due to the increasedpower of studies conducted in large population-basedcohorts, the number of NAFLD risk variants is now increas-ing by the day.30–33 We are therefore presently moving to amodel where, across the continuum of the distribution ofthe inherited predisposition to NAFLD in the population, thedevelopment of polygenic risk scores (PRS) can stratify therisk of this condition and of liver-related complica-tions.30,31,34–36 For example, “high” PRS can predict theevolution to cirrhosis and HCC independently of classicalrisk factors in individuals with dysmetabolism and/orNAFLD, potentially being able to aid in the clinical manage-ment and in the design of referral pathways.35
On the other hand, it has become clear that the maincommon risk variant and PRS cannot discriminate accuratelybetween “metabolic” and “genetic” NAFLD.28 Vice versa, veryrobust evidencehas accumulated that increased adiposity, anddysmetabolism is the main trigger for the phenotypic expres-sion of this genetic predisposition; the higher the body massindex, the higher the risk of liver disease in carriers of NAFLDrisk variants.30,35,37,38 In addition, genetic predisposition toNAFLD contributes to insulin resistance via inducing liverinjury.34 Finally, the main genetic risk variants in PNPLA3and TM6SF2 are similarly enriched in “overweight/obese”versus “lean”NAFLD.39,40 Indeed, central adipose tissue distri-bution, genetic causes of insulin resistance,37 and other factorspredisposing to hepatic fat accumulation canvicariate the roleofexcess adiposityamong thesmall fractionof lean individualswho develop NAFLD.
Excess intake of alcohol is another key determinant of thephenotypic expression of NAFLD risk variants17,30 which arealso the main genetic risk factors of alcoholic liver disease.41
Fructose intake, chronic hepatitis C, and iron accumulationare additional triggers of liver disease.42–44 This new evi-dence suggests that several conditions that were previouslyconsidered as separated diseases share major pathogenicmechanism of liver damage centered on fat accumulationand lipotoxicity which are initiated by specific but oftenconcomitant insults. Themost frequent is the combination ofobesity, excessive alcohol, and genetic predisposition. Envi-ronmental and toxic insults may further push this deleteri-ous mix toward liver disease. As such, genetics has clearlyhighlighted that clinical heterogeneity should perhaps be thebest considered in the overall context of fatty-liver diseasesthan in NAFLD per se.
However, there is initial evidence from the first nextgeneration sequencing studies that rare genetic variantswith a large impact on hepatic fat can predispose to NAFLDirrespective of dysmetabolism.14,45 For example, carriage ofapolipoprotein B (APOB) variants predispose to severeNAFLD, cirrhosis, and HCC in nonobese individuals.45,46
This subset of patients is at low risk of cardiovascular diseasedue to reduced circulating lipoproteins andmayalso possiblybenefit from vitamin E supplementation due to malabsorp-tion of lipophilic vitamins.45–47
There is additional evidence that the genetic setup ofNAFLD can influence the profile of extrahepatic organdamage and the response to therapy. Thanks to the recentdiscoveries in NAFLD genetics,14,17,28,29 the frontier ofdisease phenotyping can move away from the “metabolicvs. genetic” simplistic dichotomy, toward a subclassificationintegrated with the clinical risk factors and based oncombined environmental-genetic pathways underlying dis-ease predisposition. The challenge ahead will be to developreliable clusters of genetic variants that predict diseasesubtypes. Based on the current knowledge at least threegroups can be identified. The first is defined by the presenceof high genetic risk of obesity and insulin resistance37,48 inthe absence of specific risk determinants of liver injury(“insulin-resistant fatty-liver disease”). This roughly corre-sponds to the previous classification of “metabolic NAFLD,”at high risk of cardiometabolic complications, but lower riskof liver-related events. Among the specific determinants ofliver involvement in individuals with dysmetabolism, agroup of genetic variants including those in glucokinaseregulator (GCKR) that facilitate fat accumulation by divert-ing carbon substrates from glucose metabolism to lipidsynthesis (de novo lipogenesis [DNL]) can define “enhancedlipogenesis fatty-liver disease,” at high risk of dyslipide-mia.17,49 Insulin-resistant patients carrying these variantsmay possibly benefit from approaches reducing lipogenesis,such as statins and omega-3 fatty acids.14,50 A pathophysi-ological distinct subset (“impaired lipid remodeling fattyliver disease”) is represented by those with a high burden ofgenetic variants, including those in PNPLA3, TM6SF2, mem-brane bound O-acyl transferase (MBOAT7), and APOB,impairing lipid remodeling and secretion and favoring lip-otoxicity. These patients are at a particularly high risk ofliver-related complications, including hepatocellular carci-noma before cirrhosis development.14 They develop type-2diabetes,34,48 but are relatively protected from cardiovas-cular disease.14,35 From a therapeutic point of view, theyrespond well to weight loss, but when they carry thePNPLA3 variant do not benefit from statins and are atincreased risk of liver injury due to enhanced hepatic lipidaccumulation during insulin therapy (reviewed by Cespiatiet al14).
Overall, the newest research developments have sug-gested new possibilities to integrate, rather than opposethe genetic markers with clinical information to improvefatty-liver disease classification and management. The effi-cacy and cost effectiveness of this approach remains to beproven before wide implementation can be advised.
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 423

Differential Contribution of PathogeneticPathways
NAFLD pathogenesis is associated with a wide spectrum ofaberrant cellular and molecular mechanisms.51–53 As de-scribed above, genetic54 and metabolic55 alterations are keydrivers of the development of NAFLD resulting in an envi-ronment that favors hepatic fat accumulation and toxic lipidmetabolites via an increase in circulating free fatty acidsreleased from a dysfunctional inflamed adipose tissue56,57
and an increased DNL in hepatocytes.58,59 These changesmay lead to a state of “lipotoxicity” that triggers hepatocel-lular stress and consequently may result in liver injury andcell death, activating a sterile liver inflammatory re-sponse51,53,60 and ultimately liver fibrogenesis contributingto disease progression. Themechanisms thought to be at playin NAFLD pathogenesis may act in a sequential or parallelfashion andwith different hierarchieswithin the spectrumofdisease and over time.57,60 Thus, it is likely that the observedheterogeneity of NAFLD in the clinic, where some patientsdevelop isolated steatosis, whereas others develop NASHandadvanced chronic liver disease stems from a differentialcontribution of pathogenetic pathways,60,61 as well asfrom the activation or deactivation of redundant mecha-nisms. Also, it is likely that, besides genes, many factorsincluding diet, exercise, sex, age, and coexistence of obesityand type 2 diabetes mellitus (T2DM) among others, criticallyinfluence disease pathogenesis in a given patient.15 Howev-er, to dissect the precise contribution of each pathway toNAFLD development and progression is difficult due tolimitations of available animal models62,63 or lack of robusthuman data. Remarks on potentially relevant pathogenicdifferences among NAFLD patients are provided below.
One important mechanism underlying NAFLD develop-ment is an upregulated DNL which has been reported to bethree-fold increased compared with control patients.58 In-terestingly, DNL rates are influenced by age and sex, and thispathway may be pathogenically more relevant in older andmale patients than others.64,65
A previously overlooked player in NAFLD pathogenesisis the skeletal muscle. Several studies have underscoredthat sarcopenia (i.e., decreased muscle mass) or adversemuscle composition (i.e., low muscle volume and musclefat infiltration or myosteatosis) may influence both NAFLDdevelopment and progression.66–68 Although importantmethodological differences exist across published studies,not all patients with NAFLD exhibit muscle alterations and itis likely that this pathogenic factor be more relevant inparticular populations, such as nonobese or lean NAFLD, aswell as older patients inwhich sarcopenia ismore frequent.69
Activation of the innate immune system has been impli-cated in NAFLD progression.70,71 After liver damage, a phys-iological immune response is key for resolution of theinjurious process, liver regeneration and restauration of ahealthy liver state, while an exuberant and persistent innateimmune response may lead to chronic liver inflammation. Inthe context of NAFLD, an imbalance of the cross-talk of thegut microbiome and the liver, known as the gut-liver axis, as
well as occurrence of hepatocyte cell injury and death aretwo key upstream triggers of a persistent pathogenic innateimmune response.57,71 Intestinal dysbiosis, defined as theimbalance between resident microbial communities thatdisturb the symbiotic relationship between gut microbesand the host, and an increased intestinal permeability maylead to a pathological translocation of microbial products tothe liver via the portal vein.19,20 In this setting, pathogen-associated molecular patterns (PAMPs) are recognized byselective pattern recognition receptors, mainly toll-likereceptors, in the liver and cause a chronic innate immuneresponse. In addition, microbiota-derived metabolites suchas modified bile acids, choline, and ethanol alter hepaticmetabolism and trigger an inflammatory response.72 Theabove-mentioned mechanisms may be at play in only afraction of individuals with NAFLD. In fact, clinical studieshave uncovered that only a subset of NAFLD patients presentwith dysbiosis and/or a dysfunction in the gut barrier.19,72
These findings point that in addition to the genetic andmetabolic modifiers, assessment of microbiome profile,and or intestinal permeability may allow for a more preciseclassification and risk stratification of NAFLD patients todefine an adequate therapeutic intervention.72–74
In certain settings, the immune system may be activatedby other stimuli and contribute to NAFLD development andprogression. This may be the case for the association ofNAFLD with some immune-mediated inflammatory disor-ders, such as psoriasis75,76 and suppurative hidradenitis,77
which are associated to a low-grade systemic inflammatorystate. Of note, Psoriasis patients exhibit significantly in-creased serum levels of proinflammatory cytokines such astumor necrosis factor-a (TNF-a) interleukin (IL)-6 and re-duced levels of the anti-inflammatory adipokine, adiponec-tin than matched controls.78 Also, psoriasis patients withNAFLD have higher serum levels of C-reactive protein (CRP)and have an increased prevalence of advanced liver fibro-sis.79 In the same line, patientswith suppurative hidradenitisexhibit a high prevalence of NAFLD independently of classicmetabolic risk factors.80 However, it remains difficult todissect whether the underlying systemic inflammation ob-served in psoriasis and suppurative hidradenitis is a majorcontributor to NAFLD development and progression giventhe frequent coexistence of obesity in these patient popula-tions.76,81 Interestingly, an imbalance in T-cell subtypes, likeTh17/Treg, leading to an IL-17–mediated inflammation maybe a common pathogenic link in this regard.76,82
Hepatocyte cell death as a result of lipotoxicity is anotherkey driver of the progression of NAFLD. Cellular release ofdamage-associated molecular patterns (DAMPs) by dam-aged71 or stressed hepatocytes are recognized by the innateimmune system and may trigger chronic liver inflamma-tion.60,83 Recently pyroptosis has been identified as a novelform of programmed cell death in NAFLD and NASH. Pyrop-tosis is characterized by the activation and assembly ofmultiprotein complexes, called inflammasomes. The moststudied one is the nucleotide-binding domain, leucine-rich–repeat (NLR) family, pyrin domain containing 3 (NLRP3)inflammasome. Once activated, the NLRP3 inflammasome
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.424

cleaves procaspase-1 to its mature form caspase-1 thatsubsequently cleaves IL-1β, IL-18, and gasdermin D. IL-1band IL-18 are highly proinflammatory cytokines that arereleased into the extracellular space partly through gasder-min D formed transmembrane pores.60,84 NLRP3 was shownto promote NASH and liver fibrosis in various mousemodels.Genetic constitutive overactivation of the NLRP3 inflamma-some causes pyroptosis, inflammation, and fibrosis in theliver, while global NLRP3 knock out mice show less inflam-mation and liver fibrosis in models of diet inducedNASH.85,86 Human data on the contribution of NLRP3 toNAFLD development and progression is scarce; thus, futuretranslational studies to examine the human relevance ofthese pathways to NAFLD heterogeneity are warranted.
As described above, PAMPs and DAMPs activate andsustain a pattern recognition receptor-mediated innate im-mune response characteristic for NAFLD. Once activated, acomplex intercellular cross-talk between the different innateimmune cells, mainly macrophages, neutrophils, naturalkiller cells, and T-cells, as well as hepatocytes and hepaticstellate cells (HSCs), defines the progression to steatohepa-titis and fibrosis. Macrophages are known to play a crucialrole in orchestrating immune response and the recruitmentof further immune cells.87 Kupffer’s cells, the resident livermacrophages, are dominant over monocytes and monocyte-derived macrophages (MoMFs) in a healthy liver. However,after liver injury, both monocytes and subsequently MoMFsare rapidly recruited to the liver.88 The functional plasticityof macrophages was historically subclassified in the twopolarizations, proinflammatory-type M1 and anti-inflam-matory-type M2. This classification was shown to lackaccuracy of the macrophage activation program. Instead,during liver injury, macrophages display wide gene expres-sion profiles that led to the identification of different sub-populations of macrophages. The new technology of single-cell RNA sequencing (scRNA-seq) revealed an accumulationof MoMF in murine livers in a diet-induced NASH model.89
The population of MoMF was further subclassified in thethree clusters MoMF I to III with each cluster characterizedby particular marker genes. Interestingly, similar subpopu-lations of bonemarrowmonocyteswere also detected. Thesefindings indicate a NAFLD gene signature in myeloid leuko-cytes in both liver and bone marrow.88 Another study usingscRNA-seq identified further subpopulations of macro-phages in NASH characterized by the expression of Trem2,termed NASH-associated macrophages. In human samples,Trem2 expression correlated with the severity of NAFLDactivity score and the extent of fibrosis. Therefore, markersof NASH-associated macrophages may function as potentialnovel key classifiers of NAFLD/NASH phenotypes.90 Thespecific role of Kupffer’s cells during the progression ofNAFLD to NASH has continued to evolve. Recent evidencehas uncovered a reduction of mature Kupffer’s cell popula-tion during this process due to increased Kupffer’s cell death.Monocyte-derived macrophages are then able to enter thestage of differentiation into Kupffer’s cells. While Kupffer’scell acts mainly by facilitating hepatocyte triglyceride accu-mulation, MoMFs are more proinflammatory.91,92 A better
understanding and profiling of the immune cell niche duringNAFLD and NASH may provide a precision medicine ap-proach to the current pathological scoring of inflammationand allow for risk stratification and identify patients morelikely to have a progressive disease versus those who willhave a nonprogressive liver phenotype.
Liver fibrosis is the critical pathological feature that pre-dicts liver-related outcome in NASH.93,94 Various cytokinesactivate HSCs and their transformation toward collagen se-cretingmyofibroblasts (MFB) which are key for triggering andprogression of liver fibrosis as in other hepatic diseases.95
However, considering the disturbed metabolic milieu presentin NAFLD, it is likely, although not certain that a myriad ofdisease-specific mechanisms may be at play (recentlyreviewed by Schwabe et al).96 Interestingly, a recent studyinvestigating the population of activated HSCs in liver fibrosisrevealed various clusters of MFBs, suggesting the existence ofheterogeneity within the fibrogenic cell population. While allclusters showed a high expression of collagen, the ability tosecret chemokines to modulate inflammation was limited tocertain clusters.97 Another study uncovered specific liverzonation of HSCs, classifying them into portal vein-associatedHSCs (PaHSCs) and central vein-associated HSCs (CaHSCs).Notably, CaHSCs were identified as the dominant pathogeniccollagen-producing cells. The lysophosphatidic acid receptor 1(LPAR1) is upregulated in NASH patients and selectivelyexpressed in CaHSCs but not PaHSCs and NPCs. Pharmacologi-cal inhibition of LPAR1 in a murine NASHmodel has shown toameliorate liver fibrosis.98 These findings underline the com-plexityanddiversityofHSCs in the contextof the pathogenesisof liverfibrosis ingeneral and inNAFLD inparticular.96 Furtherstudies are warranted to investigate whether certain subpo-pulations of HSCs favor remodeling after liver injury or trig-gering liver fibrosis. These studies may allow to identifypatients with fibrotic NASH that are at particular risk ofworsening of fibrosis versus those that are more likely toshow a robust wound healing response with potential forspontaneous improvement of fibrosis. In summary, thesenovel studies dissecting the distinct immune cell and HSCniche may allow to provide two additional groups to the onesdescribed in the previous section including an “Inflammatoryfatty liver disease” and a “profibrotic fatty-liver disease.” Thisclassification may be central to identify patients withNAFLD/NASH that are at particular risk for diseaseprogressionor “rapid progressors,” a subphenotype that represents thecentral target for therapeutic intervention.
Heterogeneity of Clinical Disease
In the clinical arena, NAFLD patients present withdiverse features. Sources of heterogeneity that can beconsidered in the clinic at present time are multiple andinclude age, sex, cardiometabolic comorbidities, ethnicity,endocrine status, as well as alcohol and tobaccoconsumption.23
Considerations on the influence of age and sex in NAFLDclinical presentation and prognosis has been reviewed else-where,99–101 underscoring that while pediatric patients may
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 425

have a different natural history and unique susceptibilities,as well as more severe long-term consequences,101 olderpatients exhibit an increased prevalence and severity ofNAFLD.102 With regard to sex, NAFLD is considered a sexu-ally dimorphic disease with clear differences between maleand females with the latter being protected of severe fibroticdisease during premenopausal stage.103
Being a multisystem disease, NAFLD is commonly associ-ated with metabolic features, with a prevalence of 80% ofobesity, 72% dyslipidemia, and 44% of T2DM.1,104 Althoughthe combination of these features acts in an additive mannerto promote NAFLD progression, T2DM is the feature moststrongly and consistently associated with a more severedisease and progression.105–107 Considering the ominouseffect of T2DM on liver disease progression and extrahepaticcomplications (i.e., cardiovascular disease, cancer risk, andchronic kidney disease), most guidelines recommendpatients that NAFLD need to be screened and treated formetabolic comorbidities.3,108,109 In addition, while obesity isalso considered a risk factor for disease progression,107,110
lean patients with NAFLD have been increasingly recognizedas being at risk of progression to advanced liver disease, aswell as of developing metabolic comorbidities, and cardio-vascular disease with impact in overall and liver-relatedmortality.111,112 Lean patients account for 20 to 30% ofNAFLD patients.113 The same as obese NAFLD, its presenceis associated with presence of metabolic comorbidities,increased visceral adiposity and unfavorable genetic poly-morphisms.114Of note, lean NAFLD is not a benign condition,since it is independently associated with increased overalland cardiovascular mortality.115
Ethnicity is an important aspect in NAFLD heterogeneity.Several studies describe Hispanic Latino population to be atthe highest risk for development of NAFLD, whereas non-Hispanic Black and non-Hispanic Asian population are atlowest risk.116 In the United States, most of this risk isexplained specifically by Mexican American population(50% NAFLD prevalence, compared with only 30% of preva-lence in other Hispanic populations). The cause for theseethnicity differences is probably explained by genetic andsociocultural factors including diet, exercise, alcohol con-sumption, education, family income, and quality of life.Interestingly, novel data suggest that advanced fibrosisassessed by noninvasive serum test is more prevalent innon-Hispanic black (28.5%) and non-Hispanic white popu-lations (25.8%) compared with Mexican American (10.8%)and Asian non-Hispanic population (2.65%).117 Indeed, fur-ther studies are needed to validate and explore thesefindings.
Sex differences is another important factor to be consid-ered in NAFLD heterogeneity. It has been repeatedly shownthat female patients at reproductive age have a significantlylower NAFLD prevalence and severity118 which may beexplained by a myriad of sex differences in the pathobiologyof NAFLD (e.g., different storing of surplus calories, differen-tial activation of hepatic DNL, and sex-specific in mitochon-drial function and immune responses among others).99 Aftermenopause, sex differences are reduced in NAFLD and, in
fact, womenhave a higher riskof advancedfibrosis thanmen,especially after age 50 years,119 suggesting that estrogencould be a protector factor for NAFLD.99,118 Again, sociocul-tural characteristics are likely to be involved in sex differ-ences in NAFLD risk.
Obstructive sleep apnea (OSA) is a common complica-tion of obesity, inducing repetitive cycles of hypoxia andreoxygenation. Presence of OSA is associated with in-creased liver steatosis, inflammation, and fibrosis.120,121
Unfortunately, trials evaluating OSA therapy with continu-ous positive airway pressure (CPAP) have shown noncon-clusive results in reducing liver fibrosis of NAFLDpatients.120,122
Alcohol consumption has classically been considered anexclusion criterion for NAFLD. However, it has been increas-ingly recognized that a group of patients may present a dualetiology (i.e., alcoholic and nonalcoholic) of their fatty-liverdisease.22 Recent population based longitudinal studiesdemonstrate that even mild consumption of alcohol canhave a synergistic effect when combined with obesity, insu-lin resistance, and metabolic dysfunction to increase risk ofcirrhosis and hepatocellular carcinoma.22 In this context, therenaming of NAFLD into MAFLD proposes a set of positivecriteria for diagnosis and does not consider the exclusion ofalcohol consumption as a prerequisite criterion fordiagnosis.23,24
Among other relevant factors that may modulate diseasedevelopment and severity are presence of skin inflammatorydisorders, such as psoriasis and suppurative hidradenitis,hypothyroidism, polycystic ovarian syndrome, and peri-odontitis, all of which have been associated with increasedprevalence of NAFLD.123
Besides systemic comorbidities, patients with NAFLDrepresent a wide spectrum of liver disease severity. In theprevious decade, emphasis was made in a dichotomic differ-entiation between those patients with isolated steatosis andthose with NASH. More recently, emphasis is made onpatientswithNASHand liver fibrosis as the latter histologicalfeature has been shown to be a major prognostic determi-nant in NAFLD patients.94 Natural history studies, as well asstudies examining patients on the placebo arms of drugclinical trials, using paired biopsies, showed that evolutionof NAFLD/NASH overtime is highly dynamic and that, al-though NASH has a higher risk of fibrosis progression anddevelopment of cirrhosis than non-NASH patients, someindividuals will have spontaneous improvement whilesome patients with isolated steatosis could also progressto NASH and cirrhosis.124–131 Current data support the ideathat approximately 20 to 25% of patients with isolatedsteatosis will progress to NASH, and from those, approxi-mately 20 to 40% will progress to advanced fibrosis andcirrhosis. Additionally, 5 to 7% of NASH-cirrhotic patientswill develop HCC.56 Thus, identifying the group of patientswho most likely will progress to advanced fibrosis is aprimary goal of NAFLD/NASH-related research. In thisregard, those at higher risk are patients with metabolicabnormalities, such as T2DM, metabolic syndrome, andobesity.2,132
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.426

Most natural history studies of NAFLD have assessed liver--related morbidity and mortality in relation to a singletime-point evaluation of histology to identify riskfactors.124,131,133–135 In spite of their intrinsic selection bias,paired-biopsy studies are informative regarding identificationof factors associated with disease progression.125,126,128–130
In these studies, the main risk factors for presence of NAFLDare metabolic abnormalities such as T2DM, metabolic syn-drome, and obesity.136–138 Regarding predictors of fibrosisprogression, studies have shown that the best predictors arehistological parameters including hepatocellular ballooningdegeneration and inflammation associated with age inpatients with NASH.130 As mentioned above, the presence offibrosis on initial biopsy or progression of fibrosis on serialbiopsies appears tobethemost prominenthistologicpredictorof overall mortality and liver-related outcomes.139–141 Duringthe last decade, efforts havebeenmade to identify noninvasivesurrogates of liver biopsy that can be followed over time.Serum aminotransferase levels are good predictors of im-provement of NASH in clinical trials.10 Likewise, markers ofcell death including soluble cytokeratin-18 (CK-18) forms(total and fragmented) have been shown to be good diagnosticmarkers of NASH and predict response to therapeutic inter-ventions but currently remain a research tool and are notclinically available.142,143 Other circulating markers such asproinflammatorymarkers, including circulating levels of cyto-kines (onlinTNF-a, IL-6, IL-8, andCRP),orothermolecules, suchas adiponectin, have shown inconsistent results in part due tothe challengeswith the sensitivity of the assays used to detectchanges in blood.143–146 To identify patients who already areprogressingandpatients at early stagesoffibrosis, noninvasivescores have been developed. Among them, the NAFLD FibrosisScore, Fibrosis-4 (FIB-4), and Hepamet are nonexpensive,noncommercial, and easily available.147–152 The enhancedliver fibrosis (ELF) test is a commercial panel that combinesvarious constituents of collagen matrix deposition and turn-over.153 Additionally, imaging assessment of steatosis andfibrosis has been developed as a noninvasive method andhas focused mainly on transient elastography (TE) with con-trolled attenuation parameter (CAP) and magnetic resonanceimaging (MRI)-based technologies.153–158 Details on modernconcepts about noninvasive assessment of hepaticfibrosis canbe found in recent in-depth reviews on the topic.159,160
Implications for Clinical Practice andResearch
The differential contribution of genetic/epigenetic, environ-mental, and metabolic factors deters a significant interpa-tient variation regarding the major driver of disease(►Fig. 2). Proper consideration of NAFLD heterogeneity isrelevant for both clinical practice and research. In the clinicalarena, a more precise patient phenotyping could allow to amore granular grouping of patients to better stratify theminto those at higher risk of adverse outcomes. Also, a betterphenotyping would allow the implementation of tailoredtreatment approaches in line with concepts of precisionmedicine or individualized care.13,15,161 Since the degree
of liver fibrosis has been shown to be closely related to liver-related mortality,93,94 assessment of this variable is nowconsidered crucial in patient stratification and should beperformedwith the available noninvasive tools.159However,most of these tools are not able to distinguish those patientsthat show a strong wound healing response and thus morelikely to have a resolutive phenotype with spontaneousregression of fibrosis versus those that will have a strongfibrogenic response andwill more likely show progression offibrosis. The challenge for the future will be to develop deepphenotyping approaches that also takes into considerationthese processes in a given patient, and incorporates associ-ated comorbidities, race, genetic and epigenetic influences,and environmental factors.10,162 Thus, clinical variablesknown to be associated with rapid disease progression,such as T2DM, arterial hypertension, severe obesity, andworseningmetabolic health (i.e., presence of disglycemia andhaving one or more components of metabolic syndrome),should be factor in association with molecular and cellularprofiling of liver phenotypes and if present, may confer thelabel of “high-risk” NAFLD/NASH163,164 which may implyhigher risk of all-cause mortality, as well as of fibrosis,cirrhosis, and HCC.165 In addition, consideration on differ-ences linked to age, sex, and hormonal status may be provenrelevant given that these factors may influence NAFLDnatural history, as well as the performance of several diag-nostic tools.15 With regard to genetic factors, routine geno-typing of genetic variants known to influence NAFLD has notyet been proven to be cost effective but likely will contributeto individualized management when used integrated withall pertinent clinical information14,166 (see section Role ofGenetic Determinants). Finally, detailed phenotyping of be-havioral (i.e., physical activity and diet), alcohol use, andsocioeconomic factors, as well as of muscle mass and com-position (i.e., using MRI techniques), could aid in betterdefining NAFLD patient cohorts.
From a therapeutic standpoint, NAFLD heterogeneityshould be considered when structuring a therapeutic planfor disease management. As previously outlined in severalclinical guidelines or position papers released and endorsedby several scientific societies or expert panels,3,108,167 life-style modifications remain the cornerstone of NAFLD man-agement and are indicated in all patients.7 Of note, sexdifferences in the response to lifestyle changes have beenobserved in several studies. Interestingly in the most-citedstudy assessing lifestyle interventions in NAFLD,168 menshowed a greater histological improvement than womenafter weight loss. In this study, male sex was one of thefactors predicting beneficial histological response followinga relativelymodest weight loss (between 7 and 10%), while inwomen, a more substantial weight loss (> 10%) was requiredto achieve a significant histological improvement.168,169 Thus,based in these observations, women may require additionalsupport to achieve the goals to be achieved after introductionof lifestyle changes. In contrast, patients carrying the p.I148Mvariant of the PNAPL3 gene exhibit a better response tolifestyle modification and bariatric surgery than patientsnot carrying the variant.170–172 This information may be of
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 427

aid when considering obesity surgery in NAFLD patients.The same applies to the possibility of applying tailoredcardiovascular risk management in patient subgroups aspatients with the p.I148M variant of PNAPL3, as well asthose with the TM6SF2 E167K gene variant, exhibit a lowerrisk of cardiovascular disease compared with noncarriers.17
Finally, tailored HCC screening may be envisioned for somepatients using genetic information as use of PRS, as shown byBianco et al in a recent paper in which PNPLA3–TM6SF2–GCKR–MBOAT7 were combined, may improve HCC risk strat-ification in NAFLD.173
With regard to interpatient variability to therapeuticagents, available information is scarce. It is likely thatbetter and more detailed assessment of certain specificpathways could be of help in selecting therapeutic agents.This could be made with the use of metabolomics174,175
or other system biology tools. Thus, if DNL is shown to beoveractive,65 specific use of agents targeting this path-way, such as acetyl-CoA carboxylase (ACC) inhibitors,could be indicated.174,175 Also, if appropriate tools toassess intestinal dysbiosis19 are available, gut micro-biome-targeted therapies could be also used only in thosewith altered microbial composition. Finally, drugs thatimprove dyslipidemia or decrease cardiovascular diseasemay be more effective for those patients with a moreprofound derangement of metabolic health such aspatients with concurrent T2DM and NAFLD. In the latterpopulation, one should also consider the potential bene-fits of antidiabetic drugs, such as pioglitazone and sodi-um-glucose cotransporter-2 (SGLT2) inhibitors,176,177 orthe preferential use of the glucagon-like peptide 1 (GLP-1) receptor agonists, such as liraglutide or semaglutide,with potentially beneficial impact on liver histology and
cardiovascular outcomes in this particular patientpopulation.178–181
Finally, consideration of psychosocial factors in theevaluation of any given patient is also relevant for NAFLDmanagement and should be part of a comprehensivephenotyping approach. These factors might influence mo-tivation to both adopt and sustain lifestyle changes. In thisregard, necessary support to patients’ efforts throughhealth coaching and/or motivational interventions is keyto successful adherence to any program aimed at natural-izing physical activity in daily life.
The impact of NAFLD heterogeneity in therapeutic clinicaltrials has been also emphasized recently.12,23 Precise strati-fication of patient cohorts, included in a given study, is a keywhen assessing therapeutic response in a complex diseasesuch as NAFLD. The suboptimal responses observed in sev-eral clinical trials of different drugs may be in part due to thefact that disease heterogeneity was not taken into consider-ation.11,182 In their recent review on the matter Ampueroand Romero-Gomez concluded that clinical trial reportingfor NAFLD has been suboptimal with no detailed mention ofdysmetabolic comorbidities or proper recording of dailydietary and exercise habits. These authors suggest that futuretrials should carefully consider the presence of comorbiditiesexpected to impact on the treatment response (trying tokeep similar proportion of patients in the different arms of agiven trial), as well as proper recording of alcohol intake andexercise both during the trial and not only at entry, whichwill improve capturing of the effects of these variables intreatment responses. Also, adoption of innovative trialsdesigns to study novel NAFLD treatments, such as theadaptative, umbrella, or basket strategies, could be usefulto improve trial efficiency.12,23
Fig. 2 The differential contribution of genetic/epigenetic, environmental and metabolic factors deters a significant interpatient variationregarding the major driver of disease. Circles depict three hypothetical patients that exhibit a different predominance of the three above-mentioned factors. While patient 1 has environmental factors (e.g., poor diet and/or physical activity) as main driver of disease, patients 2 and 3has a mixed predominance of genetic factors and metabolic derangement as determinants of their phenotypes. Better distinction of maindrivers in each patient may help to implementation of individualized or precision medicine approaches in nonalcoholic fatty-liver disease(NAFLD) management (adapted from Eslam et al).23
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.428

Conclusion and Outlook
NAFLD groups a heterogeneous patient population. The het-erogeneity of NAFLD is reflected by the fact that somepatientsdevelop only steatosis, whereas others develop hepatocyteinjury, steatohepatitis, and progressive liver fibrosis and,ultimately, cirrhosis. The interaction of different factors (e.g.,sex, presence of one or more genetic variants, coexistence ofdifferent comorbidities such as obesity and T2DM, diversemicrobiota composition, and various degrees of alcohol con-sumption) critically influence different disease pathways todetermine disease subphenotypeswith distinct natural histo-ry and prognosis and potentially different response to treat-ment. The recent proposal of NAFLD, renaming into MAFLDthat sets positive criteria for diagnosis,24 has been generallywelcomed by the scientific community, although debate isongoing.25 The use of MAFLD may be a step forward inaddressing disease heterogeneity by grouping a more homog-enouspatient populationwithmoreseveremetabolic and liverdisease (i.e., presence of significant fibrosis).183–185 In addi-tion, differentiationof threesubgroups (i.e., obeseMAFLD, leanMAFLD, and diabeticMAFLD) that may have different progno-sis and could be appraised differently, may be also relevant.However, further discussion is necessary and consensus needsto be reached on this matter.26,184
Taking into account, disease heterogeneity is relevant bothclinically, to apply more individualized approaches in NAFLDdiagnosis and treatment, and to drug development due to theneed of including more homogeneous patient populations inclinical trials. In addition to clinical factors, availability ofmodern tools to define activation of DNL with metabolomics,development of accurate biomarkers of inflammatory, celldeath or liver fibrosis pathways activation, better detectionof presence of dysbiosis assisted by the use of microbiotasignatures, or evaluationofgenetic riskofcirrhosisorHCCwithPRS would surely impact our ability to discriminate patients’subgroups and stratify them according to their risks of pooroutcomes. This alsowould help to select themost appropriatetreatment for a given patient following the precisionmedicineprinciples.13,15 Thus, in the future, it can be envisaged thatprecise phenotyping of pathogenic pathways would lead toselect a specific drug10 or that a genetic treatment27,186 couldbe chosen based on global ethnic-specific genetic information.Also, it is likely that principles of precision nutrition187 andprecision exercise188 would apply to patient management toincrease thetherapeuticefficacyof lifestyles changes inNAFLDmanagement.
Indeed, further research is needed to improve our under-standing of NAFLD heterogeneity. Building of large biobanksfrom well-characterized patient populations integratingclinical, genetic, biomarkers, and OMICs information is keyto this end. The use of artificial intelligence approaches offersthe opportunity to combine and decode this information todevelop useful algorithms for patient stratification andman-agement. A better definition of the dominant drivers ofdisease in patient subgroups would predictably impact onthe development of more precision-targeted therapies forNAFLD.
Main Concepts and Learning Points
• Nonalcoholic fatty-liver disease (NAFLD) is an umbrellaterm that groups a heterogeneous patient population.
• NAFLD heterogeneity is influenced by multiple variablesincluding age, sex, presence of one or more geneticvariants, coexistence of different comorbidities, diversemicrobiota composition, and various degrees of alcoholconsumption among other factors.
• The heterogeneous nature of NAFLD results from a differ-ent hierarchy or trajectory of pathophysiological mecha-nisms that determine several disease subphenotypeswithdistinct natural history and prognosis and, eventually,different response to therapy.
• Proper consideration of NAFLD heterogeneity is relevantfor both clinical practice to implement individualizedmedicine approaches, as well as for clinical research, toimprove clinical trials efficiency.
• The recent renaming of NAFLD intoMAFLD (i.e., metabolic[dysfunction]-associated fatty-liver disease) is a step for-ward in taking into account NAFLD heterogeneity bysetting specific diagnostic criteria and grouping patientswith disturbedmetabolic health. However, more researchis needed to refine discrimination of subtypes of thedisease.
AbbreviationsACC, acetyl-CoA carboxylase; APOB, apolipoprotein B;CaHSCs, central vein-associated HSCs; CRP, C-reactiveprotein; DAMPs, damage-associated molecular patterns;DNL, de novo lipogenesis; GCKR, glucokinase regulator;GWAS, genome-wide association studies; HCC, hepato-cellular carcinoma; HSC, hepatic stellate cells; IL, inter-leukin; MBOAT7, membrane bound O-acyl transferase;MoMFs, monocyte-derived macrophages; NAFLD, nonal-coholic fatty-liver disease; NAFL, nonalcoholic fatty-liver;NASH, nonalcoholic steatohepatitis; NLRP3, NLR familypyrin domain containing 3; PaHSCs, portal vein-associat-ed HSCs; PAMPs, pathogen-associated molecular pat-terns; PNPLA3, patatin-like phospholipase domain-containing 3; PRS, polygenic risk scores; scRNA-seq, singlecell RNA sequencing; TDM2, type 2 diabetes mellitus;TM6SF2: transmembrane 6 superfamily member 2; TNF-a, tumor necrosis factor-a.
Funding SourcesThis work was funded, in part, by grants from the FondoNacional De Ciencia y Tecnología de Chile (FONDECYT no.:1191145 to M.A., no.:1200227 to J.P.A., and no.:1191183to F.B.), the Comisión Nacional de Investigación, Ciencia yTecnología (CONICYT, AFB170005, CARE, Chile, UC). M.A.is part of the European-Latin American ESCALON consor-tium funded by the European Union’s Horizon 2020Research and Innovation Program under grant agreementno. 825510. A.E.F. was supported was by NIH grants R01DK113592 and R01 AA024206. L.V. was supported byproject grants from MyFirst Grant AIRC n.16888, RicercaFinalizzata Ministero della Salute RF-2016–02364358
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 429

(“Impact of whole exome sequencing on the clinicalmanagement of patients with advanced nonalcoholicfatty-liver and cryptogenic-liver disease”), Ricerca cor-rente Fondazione IRCCS Ca’ Granda Ospedale MaggiorePoliclinico, the European Union (EU) Program Horizon2020 (under grant agreement No. 777377) for the projectLITMUS- “Liver Investigation: Testing Marker Utility inSteatohepatitis,” Program “Photonics” under grant agree-ment “101016726” for the project “REVEAL: Neuronalmicroscopy for cell behavioural examination and manip-ulation,” Gilead_IN-IT-989–5790 “Developing a model ofcare for risk stratification and management of diabeticpatients with non-alcoholic fatty-liver disease (NAFLD),”Fondazione IRCCS Ca’ Granda “Liver BIBLE” PR-0391,Fondazione IRCCS Ca’ Granda core COVID-19 Biobank(RC100017A).
Conflict of InterestThe authors declare that they have no conflict of interestrelevant to the present study. L.V. has received speakingfees fromMSD, Gilead, AlfaSigma, and AbbVie, served as aconsultant for Gilead, Pfizer, AstraZeneca, Novo Nordisk,Intercept, Diatech Pharmacogenetics and Ionis Pharma-ceuticals, and received research grants from Gilead.
References1 Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, WymerM.
Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes.Hepatology 2016;64(01):73–84
2 Cotter TG, Rinella M. Nonalcoholic fatty liver disease 2020: thestate of the disease. Gastroenterology 2020;158(07):1851–1864
3 Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis andmanagement of nonalcoholic fatty liver disease: Practice guid-ance from the American Association for the Study of LiverDiseases. Hepatology 2018;67(01):328–357
4 Huang DQ, El-Serag HB, Loomba R. Global epidemiologyof NAFLD-related HCC: trends, predictions, risk factors andprevention. Nat Rev Gastroenterol Hepatol 2021;18(04):223–238
5 Younossi ZM, Marchesini G, Pinto-Cortez H, Petta S. Epidemiol-ogy of nonalcoholic fatty liver disease and nonalcoholic steato-hepatitis: implications for liver transplantation. Transplantation2019;103(01):22–27
6 Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling theepidemic of nonalcoholic fatty liver disease demonstrates anexponential increase in burden of disease. Hepatology 2018;67(01):123–133
7 Younossi ZM, Corey KE, Lim JK. AGA clinical practice update onlifestyle modification using diet and exercise to achieve weightloss in the management of nonalcoholic fatty liver disease:expert review. Gastroenterology 2021;160(03):912–918
8 Thorp A, Stine JG. Exercise as medicine: the impact of exercisetraining on nonalcoholic fatty liver disease. Curr Hepatol Rep2020;19(04):402–411
9 Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLDwith diet, physical activity and exercise. J Hepatol 2017;67(04):829–846
10 Vuppalanchi R, Noureddin M, Alkhouri N, Sanyal AJ. Therapeuticpipeline in nonalcoholic steatohepatitis. Nat Rev GastroenterolHepatol 2021
11 Ratziu V, Friedman SL. Why do so many NASH trials fail?Gastroenterology 2020:S0016-5085(20)30680-6
12 Ampuero J, Romero-GomezM. Stratification of patients in NASHclinical trials: a pitfall for trial success. JHEP Rep 2020;2(05):100148
13 Sookoian S, Pirola CJ. Precision medicine in nonalcoholic fattyliver disease: New therapeutic insights from genetics and sys-tems biology. Clin Mol Hepatol 2020;26(04):461–475
14 Cespiati A, Youngson NA, Tourna A, Valenti L. Genetics andepigenetics in the clinic: precision medicine in the managementof fatty liver disease. Curr Pharm Des 2020;26(10):998–1009
15 Lonardo A, Arab JP, ArreseM. Perspectives on precisionmedicineapproaches toNAFLDdiagnosis andmanagement. Adv Ther 2021(e-pub ahead of print). Doi: 10.1007/s12325-021-01690-1
16 Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, et al. Sex and gender:modifiers of health, disease, and medicine. Lancet 2020;396(10250):565–582
17 Trépo E, Valenti L. Update on NAFLD genetics: from new variantsto the clinic. J Hepatol 2020;72(06):1196–1209
18 Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol2015;62(1, suppl):S47–S64
19 Sharpton SR, Schnabl B, Knight R, Loomba R. Current concepts,opportunities, and challenges of gut microbiome-based person-alized medicine in nonalcoholic fatty liver disease. Cell Metab2021;33(01):21–32
20 Arab JP, ArreseM, Shah VH. Gutmicrobiota in non-alcoholic fattyliver disease and alcohol-related liver disease: current conceptsand perspectives. Hepatol Res 2020;50(04):407–418
21 Jiang L, Schnabl B. Gut microbiota in liver disease: what do weknowandwhat dowe not know? Physiology (Bethesda) 2020;35(04):261–274
22 Idalsoaga F, Kulkarni AV, Mousa OY, Arrese M, Arab JP. Non-alcoholic fatty liver disease and alcohol-related liver disease:two intertwined entities. Front Med (Lausanne) 2020;7:448
23 Eslam M, Sanyal AJ, George JInternational Consensus Panel.MAFLD: a consensus-driven proposed nomenclature for meta-bolic associated fatty liver disease. Gastroenterology 2020;158(07):1999–2014.e1
24 Eslam M, Newsome PN, Sarin SK, et al. A new definition formetabolic dysfunction-associated fatty liver disease: an inter-national expert consensus statement. J Hepatol 2020;73(01):202–209
25 Younossi ZM, Rinella ME, Sanyal AJ, et al. From NAFLD toMAFLD:implications of a premature change in terminology. Hepatology2021;73(03):1194–1198
26 Ratziu V, Rinella M, Beuers U, et al. The times they are a-changin’(for NAFLD as well). J Hepatol 2020;73(06):1307–1309
27 Romeo S, Sanyal A, Valenti L. Leveraging human genetics toidentify potential new treatments for fatty liver disease. CellMetab 2020;31(01):35–45
28 Yki-Järvinen H. Non-alcoholic fatty liver disease as a cause and aconsequence of metabolic syndrome. Lancet Diabetes Endocri-nol 2014;2(11):901–910
29 Dongiovanni P, Petta S, Maglio C, et al. Transmembrane 6superfamily member 2 gene variant disentangles nonalcoholicsteatohepatitis from cardiovascular disease. Hepatology 2015;61(02):506–514
30 Emdin CA, Haas M, Ajmera V, et al. Association of geneticvariation with cirrhosis: a multi-trait genome-wide associationand gene-environment interaction study. Gastroenterology2021;160(05):1620–1633.e13
31 Jamialahmadi O, Mancina RM, Ciociola E, et al. Exome-wideassociation study on alanine aminotransferase identifies se-quence variants in the GPAM and APOE associated with fattyliver disease. Gastroenterology 2021; 160(05):1634–1646.e7
32 Emdin CA, Haas ME, Khera AV, et al; Million Veteran Program. Amissense variant in mitochondrial amidoxime reducing
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.430

component 1 gene and protection against liver disease. PLoSGenet 2020;16(04):e1008629
33 Abul-Husn NS, Cheng X, Li AH, et al. A protein-truncatingHSD17B13 variant and protection from chronic liver disease. NEngl J Med 2018;378(12):1096–1106
34 Dongiovanni P, Stender S, Pietrelli A, et al. Causal relationship ofhepatic fat with liver damage and insulin resistance in nonalco-holic fatty liver. J Intern Med 2018;283(04):356–370
35 Bianco C, Jamialahmadi O, Pelusi S, et al. Non-invasive stratifica-tion of hepatocellular carcinoma risk in non-alcoholic fatty liverusing polygenic risk scores. J Hepatol 2021;74(04):775–782
36 Gellert-Kristensen H, Richardson TG, Davey Smith G, Nordest-gaard BG, Tybjaerg-Hansen A, Stender S. Combined effect ofPNPLA3, TM6SF2, and HSD17B13 variants on risk of cirrhosisand hepatocellular carcinoma in the general population. Hep-atology 2020;72(03):845–856
37 Stender S, Kozlitina J, Nordestgaard BG, Tybjærg-Hansen A,Hobbs HH, Cohen JC. Adiposity amplifies the genetic risk of fattyliver disease conferred by multiple loci. Nat Genet 2017;49(06):842–847
38 Barata L, Feitosa MF, Bielak LF, et al. Insulin resistance exacer-bates genetic predisposition to nonalcoholic fatty liver disease inindividuals without diabetes. Hepatol Commun 2019;3(07):894–907
39 Wei JL, Leung JC, Loong TC, et al. Prevalence and severity ofnonalcoholic fatty liver disease in non-obese patients: a popula-tion study using proton-magnetic resonance spectroscopy. Am JGastroenterol 2015;110(09):1306–1314, quiz 1315
40 Fracanzani AL, Petta S, Lombardi R, et al. Liver and cardiovasculardamage in patients with lean nonalcoholic fatty liver disease,and associationwith visceral obesity. Clin Gastroenterol Hepatol2017;15(10):1604–1611.e1
41 Valenti LVC, Baselli GA. Genetics of nonalcoholic fatty liverdisease: a 2018 update. Curr PharmDes 2018;24(38):4566–4573
42 Valenti L, Nobili V. PNPLA3 I148M polymorphism and liverdamage in obese children. J Pediatr 2011;159(05):876
43 Valenti L, Rumi M, Galmozzi E, et al. Patatin-like phospholipasedomain-containing 3 I148M polymorphism, steatosis, and liverdamage in chronic hepatitis C. Hepatology 2011;53(03):791–799
44 Dongiovanni P, Donati B, Fares R, et al. PNPLA3 I148M polymor-phism and progressive liver disease.World J Gastroenterol 2013;19(41):6969–6978
45 Pelusi S, Baselli G, Pietrelli A, et al. Rare pathogenic variantspredispose to hepatocellular carcinoma in nonalcoholic fattyliver disease. Sci Rep 2019;9(01):3682
46 Cefalù AB, Pirruccello JP, Noto D, et al. A novel APOB mutationidentified by exome sequencing cosegregates with steatosis,liver cancer, and hypocholesterolemia. Arterioscler ThrombVasc Biol 2013;33(08):2021–2025
47 Valenti L, Romeo S. Editorial: new insights into the relationshipbetween the intestine and non-alcoholic fatty liver-is “fatty gut”involved in disease progression? Aliment Pharmacol Ther 2017;46(03):377–378
48 Liu Z, Zhang Y, Graham S, et al. Causal relationships betweenNAFLD, T2D and obesity have implications for disease subphe-notyping. J Hepatol 2020;73(02):263–276
49 Speliotes EK, Yerges-Armstrong LM,Wu J, et al; NASHCRNGIANTConsortium MAGIC Investigators GOLD Consortium. Genome-wide association analysis identifies variants associated withnonalcoholic fatty liver disease that have distinct effects onmetabolic traits. PLoS Genet 2011;7(03):e1001324
50 Dongiovanni P, Petta S, Mannisto V, et al. Statin use and non-alcoholic steatohepatitis in at risk individuals. J Hepatol 2015;63(03):705–712
51 Arab JP, Arrese M, Trauner M. Recent insights into the pathogen-esis of nonalcoholic fatty liver disease. Annu Rev Pathol 2018;13:321–350
52 Brunt EM, Wong VW, Nobili V, et al. Nonalcoholic fatty liverdisease. Nat Rev Dis Primers 2015;1:15080
53 Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ.Mechanisms of NAFLD development and therapeutic strategies.Nat Med 2018;24(07):908–922
54 Sookoian S, Pirola CJ, Valenti L, Davidson NO. Genetic pathwaysin nonalcoholic fatty liver disease: insights from systems biolo-gy. Hepatology 2020;72(01):330–346
55 Bence KK, BirnbaumMJ. Metabolic drivers of non-alcoholic fattyliver disease. Mol Metab 2020 (e-pub ahead of print). Doi:10.1016/j.molmet.2020.101143
56 Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogen-esis of non-alcoholic fatty liver disease (NAFLD). Metabolism2016;65(08):1038–1048
57 Tilg H, Adolph TE, Moschen AR. Multiple parallel hits hypothesisin nonalcoholic fatty liver disease - revisited after a decade.Hepatology 2021;73(02):833–842
58 Lambert JE, Ramos-Roman MA, Browning JD, Parks EJ. Increasedde novo lipogenesis is a distinct characteristic of individualswith nonalcoholic fatty liver disease. Gastroenterology 2014;146(03):726–735
59 Smith GI, ShankaranM, YoshinoM, et al. Insulin resistance driveshepatic de novo lipogenesis in nonalcoholic fatty liver disease. JClin Invest 2020;130(03):1453–1460
60 Schuster S, Cabrera D, Arrese M, Feldstein AE. Triggering andresolution of inflammation in NASH. Nat Rev GastroenterolHepatol 2018;15(06):349–364
61 Parthasarathy G, Revelo X, Malhi H. Pathogenesis of nonalcoholicsteatohepatitis: an overview. Hepatol Commun 2020;4(04):478–492
62 Buyco DG, Martin J, Jeon S, Hooks R, Lin C, Carr R. Experimentalmodels of metabolic and alcoholic fatty liver disease. World JGastroenterol 2021;27(01):1–18
63 Ipsen DH, Lykkesfeldt J, Tveden-Nyborg P. Animal models offibrosis in nonalcoholic steatohepatitis: do they reflect humandisease? Adv Nutr 2020;11(06):1696–1711
64 Pramfalk C, Pavlides M, Banerjee R, et al. Sex-specific differencesin hepatic fat oxidation and synthesis may explain the higherpropensity for NAFLD in men. J Clin Endocrinol Metab 2015;100(12):4425–4433
65 Paglialunga S, Dehn CA. Clinical assessment of hepatic de novolipogenesis in non-alcoholic fatty liver disease. Lipids Health Dis2016;15(01):159
66 Fernández-Mincone T, Contreras-Briceño F, Espinosa-RamírezM, et al. Nonalcoholic fatty liver disease and sarcopenia: patho-physiological connections and therapeutic implications. ExpertRev Gastroenterol Hepatol 2020;14(12):1141–1157
67 Cabrera D, Ruiz A, Cabello-Verrugio C, et al. Diet-induced nonal-coholic fatty liver disease is associated with sarcopenia anddecreased serum insulin-like growth factor-1. Dig Dis Sci2016;61(11):3190–3198
68 Chakravarthy MV, Siddiqui MS, Forsgren MF, Sanyal AJ. Harness-ing muscle-liver crosstalk to treat nonalcoholic steatohepatitis.Front Endocrinol (Lausanne) 2020;11:592373
69 Kashiwagi K, Takayama M, Fukuhara K, et al. A significantassociation of non-obese non-alcoholic fatty liver disease withsarcopenic obesity. Clin Nutr ESPEN 2020;38:86–93
70 Cai J, ZhangXJ, LiH.Theroleof innate immunecells innonalcoholicsteatohepatitis. Hepatology 2019;70(03):1026–1037
71 Arrese M, Cabrera D, Kalergis AM, Feldstein AE. Innate immunityand inflammation in NAFLD/NASH. Dig Dis Sci 2016;61(05):1294–1303
72 Chu H, Duan Y, Yang L, Schnabl B. Small metabolites, possible bigchanges: a microbiota-centered view of non-alcoholic fatty liverdisease. Gut 2019;68(02):359–370
73 Porras D, Nistal E, Martínez-Flórez S, González-Gallego J, García-Mediavilla MV, Sánchez-Campos S. Intestinal microbiota
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 431

modulation in obesity-related non-alcoholic fatty liver disease.Front Physiol 2018;9:1813
74 Tripathi A, Debelius J, Brenner DA, et al. The gut-liver axis and theintersection with the microbiome. Nat Rev Gastroenterol Hep-atol 2018;15(07):397–411
75 Candia R, Ruiz A, Torres-Robles R, Chávez-Tapia N, Méndez-Sánchez N, Arrese M. Risk of non-alcoholic fatty liver diseasein patients with psoriasis: a systematic review and meta-analy-sis. J Eur Acad Dermatol Venereol 2015;29(04):656–662
76 Heitmann J, Frings VG, Geier A, Goebeler M, Kerstan A. Non-alcoholic fatty liver disease and psoriasis - is there a sharedproinflammatory network? J Dtsch Dermatol Ges 2021
77 Damiani G, Leone S, Fajgenbaum K, et al. Nonalcoholic fatty liverdisease prevalence in an Italian cohort of patients with hidra-denitis suppurativa: a multi-center retrospective analysis.World J Hepatol 2019;11(04):391–401
78 van der Voort EA, Koehler EM, Dowlatshahi EA, et al. Psoriasis isindependently associatedwith nonalcoholic fatty liver disease inpatients 55 years old or older: results from a population-basedstudy. J Am Acad Dermatol 2014;70(03):517–524
79 van der Voort EA, Koehler EM, Nijsten T, et al. Increased preva-lence of advanced liver fibrosis in patients with psoriasis: across-sectional analysis from the rotterdam study. Acta DermVenereol 2016;96(02):213–217
80 Durán-Vian C, Arias-Loste MT, Hernández JL, et al. High preva-lence of non-alcoholic fatty liver disease among hidradenitissuppurativa patients independent of classic metabolic risk fac-tors. J Eur Acad Dermatol Venereol 2019;33(11):2131–2136
81 Prussick RB, Miele L. Nonalcoholic fatty liver disease in patientswith psoriasis: a consequence of systemic inflammatory bur-den? Br J Dermatol 2018;179(01):16–29
82 He B, Wu L, Xie W, et al. The imbalance of Th17/Treg cells isinvolved in the progression of nonalcoholic fatty liver disease inmice. BMC Immunol 2017;18(01):33
83 Luedde T, Kaplowitz N, Schwabe RF. Cell death and cell deathresponses in liver disease: mechanisms and clinical relevance.Gastroenterology 2014;147(04):765–783.e4
84 Wree A, Holtmann TM, Inzaugarat ME, Feldstein AE. Noveldrivers of the inflammatory response in liver injury and fibrosis.Semin Liver Dis 2019;39(03):275–282
85 Wree A, Eguchi A, McGeough MD, et al. NLRP3 inflammasomeactivation results in hepatocyte pyroptosis, liver inflammation,and fibrosis in mice. Hepatology 2014;59(03):898–910
86 Wree A, McGeough MD, Peña CA, et al. NLRP3 inflammasomeactivation is required for fibrosis development in NAFLD. J MolMed (Berl) 2014;92(10):1069–1082
87 Krenkel O, Tacke F. Liver macrophages in tissue homeostasis anddisease. Nat Rev Immunol 2017;17(05):306–321
88 Krenkel O, Hundertmark J, Abdallah AT, et al. Myeloid cells inliver and bone marrow acquire a functionally distinct inflam-matory phenotype during obesity-related steatohepatitis. Gut2020;69(03):551–563
89 Chu AL, Schilling JD, King KR, Feldstein AE. The power of single-cell analysis for the study of liver pathobiology. Hepatology2021;73(01):437–448
90 Xiong X, Kuang H, Ansari S, et al. Landscape of intercellularcrosstalk in healthy and NASH liver revealed by single-cellsecretome gene analysis. Mol Cell 2019;75(03):644–660.e5
91 Daemen S, Gainullina A, Kalugotla G, et al. Dynamic shifts in thecomposition of resident and recruited macrophages influencetissue remodeling in NASH. Cell Rep 2021;34(02):108626
92 Tran S, Baba I, Poupel L, et al. Impaired Kupffer cell self-renewalalters the liver response to lipid overload during non-alcoholicsteatohepatitis. Immunity 2020;53(03):627–640.e5
93 Vilar-Gomez E, Calzadilla-Bertot L,Wai-SunWong V, et al. Fibrosisseverity as a determinant of cause-specific mortality in patientswith advanced nonalcoholic fatty liver disease: a multi-nationalcohort study. Gastroenterology 2018;155(02):443–457.e17
94 Ekstedt M, Hagström H, Nasr P, et al. Fibrosis stage is thestrongest predictor for disease-specific mortality in NAFLD afterup to 33 years of follow-up. Hepatology 2015;61(05):1547–1554
95 Kisseleva T, Brenner D. Molecular and cellular mechanisms ofliver fibrosis and its regression. Nat Rev Gastroenterol Hepatol2021;18(03):151–166
96 Schwabe RF, Tabas I, Pajvani UB. Mechanisms of fibrosis devel-opment in nonalcoholic steatohepatitis. Gastroenterology 2020;158(07):1913–1928
97 Krenkel O, Hundertmark J, Ritz TP, Weiskirchen R, Tacke F. Singlecell RNA sequencing identifies subsets of hepatic stellate cellsand myofibroblasts in liver fibrosis. Cells 2019;8(05):E503
98 Dobie R, Wilson-Kanamori JR, Henderson BEP, et al. Single-celltranscriptomics uncovers zonation of function in the mesen-chyme during liver fibrosis. Cell Rep 2019;29(07):1832–1847.e8
99 Lonardo A, Nascimbeni F, Ballestri S, et al. Sex differences innonalcoholic fatty liver disease: state of the art and identifica-tion of research gaps. Hepatology 2019;70(04):1457–1469
100 Bertolotti M, Lonardo A, Mussi C, et al. Nonalcoholic fatty liverdisease and aging: epidemiology to management. World J Gas-troenterol 2014;20(39):14185–14204
101 Vittorio J, Lavine JE. Recent advances in understanding andmanaging pediatric nonalcoholic fatty liver disease. F1000 Res2020;9:9
102 Golabi P, Paik J, Reddy R, Bugianesi E, Trimble G, Younossi ZM.Prevalence and long-term outcomes of non-alcoholic fatty liverdisease among elderly individuals from the United States. BMCGastroenterol 2019;19(01):56
103 Yang JD, Abdelmalek MF, Pang H, et al. Gender and menopauseimpact severity of fibrosis among patients with nonalcoholicsteatohepatitis. Hepatology 2014;59(04):1406–1414
104 Petroni ML, Brodosi L, Bugianesi E, Marchesini G. Management ofnon-alcoholic fatty liver disease. BMJ 2021;372:m4747
105 Kanwal F, Kramer JR, Li L, et al. Effect of metabolic traits on therisk of cirrhosis and hepatocellular cancer in nonalcoholic fattyliver disease. Hepatology 2020;71(03):808–819
106 Younossi ZM, Golabi P, de Avila L, et al. The global epidemiol-ogy of NAFLD and NASH in patients with type 2 diabetes: Asystematic review and meta-analysis. J Hepatol 2019;71(04):793–801
107 Jarvis H, Craig D, Barker R, et al. Metabolic risk factors andincident advanced liver disease in non-alcoholic fatty liverdisease (NAFLD): A systematic review and meta-analysis ofpopulation-based observational studies. PLoS Med 2020;17(04):e1003100
108 Arab JP, Dirchwolf M, Álvares-da-Silva MR, et al. Latin AmericanAssociation for the study of the liver (ALEH) practice guidance forthe diagnosis and treatment of non-alcoholic fatty liver disease.Ann Hepatol 2020;19(06):674–690
109 Tsochatzis EA, Newsome PN. Non-alcoholic fatty liver diseaseand the interface between primary and secondary care. LancetGastroenterol Hepatol 2018;3(07):509–517
110 Lu FB, Hu ED, Xu LM, et al. The relationship between obesity andthe severity of non-alcoholic fatty liver disease: systematicreview and meta-analysis. Expert Rev Gastroenterol Hepatol2018;12(05):491–502
111 Younes R, Govaere O, Petta S, et al. Caucasian lean subjects withnon-alcoholic fatty liver disease share long-term prognosis ofnon-lean: time for reappraisal of BMI-driven approach? Gut2021 (e-pub ahead of print). Doi: 10.1136/gutjnl-2020-322564
112 Ye Q, Zou B, Yeo YH, et al. Global prevalence, incidence, andoutcomes of non-obese or lean non-alcoholic fatty liver disease:a systematic review and meta-analysis. Lancet GastroenterolHepatol 2020;5(08):739–752
113 Lu FB, Zheng KI, Rios RS, Targher G, Byrne CD, Zheng MH. Globalepidemiology of lean non-alcoholic fatty liver disease: a system-atic review and meta-analysis. J Gastroenterol Hepatol 2020;35(12):2041–2050
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.432

114 Younes R, Bugianesi E. NASH in lean individuals. Semin Liver Dis2019;39(01):86–95
115 Golabi P, Paik J, Fukui N, Locklear CT, de Avilla L, Younossi ZM.Patients with lean nonalcoholic fatty liver disease are metaboli-cally abnormal and have a higher risk formortality. Clin Diabetes2019;37(01):65–72
116 Younossi Z, Anstee QM,Marietti M, et al. Global burden of NAFLDand NASH: trends, predictions, risk factors and prevention. NatRev Gastroenterol Hepatol 2018;15(01):11–20
117 Le MH, Yeo YH, Cheung R, Wong VW, Nguyen MH. Ethnicinfluence on nonalcoholic fatty liver disease prevalence andlack of disease awareness in the United States, 2011-2016. JIntern Med 2020;287(06):711–722
118 Lonardo A, Suzuki A. Focus on Clinical Aspects and Implicationsfor Practice and Translational Research. Sexual dimorphism ofNAFLD in adults. J Clin Med 2020;9(05):E1278
119 Balakrishnan M, Patel P, Dunn-Valadez S, et al. Women have alower risk of nonalcoholic fatty liver disease but a higher risk ofprogression vs men: a systematic review andmeta-analysis. ClinGastroenterol Hepatol 2021;19(01):61–71.e15
120 Parikh MP, Gupta NM, McCullough AJ. Obstructive sleep apneaand the liver. Clin Liver Dis 2019;23(02):363–382
121 Hernández A, Geng Y, Sepúlveda R, et al. Chemical hypoxiainduces pro-inflammatory signals in fat-laden hepatocytes andcontributes to cellular crosstalk with Kupffer cells throughextracellular vesicles. Biochim Biophys Acta Mol Basis Dis2020;1866(06):165753
122 Mesarwi OA, Loomba R, Malhotra A. Obstructive sleep apnea,hypoxia, and nonalcoholic fatty liver disease. Am J Respir CritCare Med 2019;199(07):830–841
123 Rosato V, Masarone M, Dallio M, Federico A, Aglitti A, Persico M.NAFLD and extra-hepatic comorbidities: current evidence on amulti-organmetabolic syndrome. Int J Environ Res Public Health2019;16(18):E3415
124 Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC,McCullough AJ. Nonalcoholic fatty liver disease: a spectrum ofclinical and pathological severity. Gastroenterology 1999;116(06):1413–1419
125 Pelusi S, Cespiati A, Rametta R, et al. Prevalence and risk factors ofsignificant fibrosis in patients with nonalcoholic fatty liverwithout steatohepatitis. Clin Gastroenterol Hepatol 2019;17(11):2310–2319.e6
126 Kleiner DE, Brunt EM, Wilson LA, et al; Nonalcoholic Steatohe-patitis Clinical Research Network. Association of histologicdisease activity with progression of nonalcoholic fatty liverdisease. JAMA Netw Open 2019;2(10):e1912565
127 Ekstedt M, Franzén LE, Mathiesen UL, Kechagias S. Low clinicalrelevance of the nonalcoholic fatty liver disease activity score(NAS) in predicting fibrosis progression. Scand J Gastroenterol2012;47(01):108–115
128 Pais R, Charlotte F, Fedchuk L, et al; LIDO Study Group. Asystematic review of follow-up biopsies reveals disease progres-sion in patients with non-alcoholic fatty liver. J Hepatol 2013;59(03):550–556
129 Wong VW, Wong GL, Choi PC, et al. Disease progression of non-alcoholic fatty liver disease: a prospective studywith paired liverbiopsies at 3 years. Gut 2010;59(07):969–974
130 Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH. Systematicreview of risk factors for fibrosis progression in non-alcoholicsteatohepatitis. J Hepatol 2009;51(02):371–379
131 Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R.Fibrosis progression in nonalcoholic fatty liver vs nonalcoholicsteatohepatitis: a systematic review and meta-analysis ofpaired-biopsy studies. Clin Gastroenterol Hepatol 2015;13(04):643–654.e1, 9, quiz e39–e40
132 Cariou B, Byrne CD, Loomba R, Sanyal AJ. Nonalcoholic fatty liverdisease as a metabolic disease in humans: a literature review.Diabetes Obes Metab 2021;23(05):1069–1083
133 McPherson S, Hardy T, Henderson E, Burt AD, Day CP, AnsteeQM. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for progno-sis and clinical management. J Hepatol 2015;62(05):1148–1155
134 Teli MR, James OF, Burt AD, Bennett MK, Day CP. The naturalhistory of nonalcoholic fatty liver: a follow-up study. Hepatology1995;22(06):1714–1719
135 Powell EE, Cooksley WG, Hanson R, Searle J, Halliday JW, PowellLW. The natural history of nonalcoholic steatohepatitis: afollow-up study of forty-two patients for up to 21 years.Hepatology 1990;11(01):74–80
136 Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohe-patitis: Mayo Clinic experiences with a hitherto unnamed dis-ease. Mayo Clin Proc 1980;55(07):434–438
137 Adler M, Schaffner F. Fatty liver hepatitis and cirrhosis in obesepatients. Am J Med 1979;67(05):811–816
138 Wanless IR, Lentz JS. Fatty liver hepatitis (steatohepatitis) andobesity: an autopsy study with analysis of risk factors. Hepatol-ogy 1990;12(05):1106–1110
139 Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver fibrosis, but noother histologic features, is associated with long-term outcomesof patients with nonalcoholic fatty liver disease. Gastroenterol-ogy 2015;149(02):389–97.e10
140 Younossi ZM, Stepanova M, Rafiq N, et al. Pathologic criteria fornonalcoholic steatohepatitis: interprotocol agreement and abil-ity to predict liver-related mortality. Hepatology 2011;53(06):1874–1882
141 Kim D, Kim WR, Kim HJ, Therneau TM. Association betweennoninvasive fibrosis markers and mortality among adults withnonalcoholic fatty liver disease in the United States. Hepatology2013;57(04):1357–1365
142 Vuppalanchi R, Jain AK, Deppe R, et al. Relationship betweenchanges in serum levels of keratin 18 and changes in liverhistology in children and adults with nonalcoholic fatty liverdisease. Clin Gastroenterol Hepatol 2014;12(12):2121–30.e1, 2
143 Feldstein AE, Wieckowska A, Lopez AR, Liu YC, Zein NN, McCul-lough AJ. Cytokeratin-18 fragment levels as noninvasive bio-markers for nonalcoholic steatohepatitis: a multicentervalidation study. Hepatology 2009;50(04):1072–1078
144 Wong VW, Hui AY, Tsang SW, et al. Metabolic and adipokineprofile of Chinese patients with nonalcoholic fatty liver disease.Clin Gastroenterol Hepatol 2006;4(09):1154–1161
145 Musso G, Gambino R, Durazzo M, et al. Adipokines in NASH:postprandial lipid metabolism as a link between adiponectinand liver disease. Hepatology 2005;42(05):1175–1183
146 Hui JM, Hodge A, Farrell GC, Kench JG, Kriketos A, George J.Beyond insulin resistance in NASH: TNF-alpha or adiponectin?Hepatology 2004;40(01):46–54
147 Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: anoninvasive system that identifies liver fibrosis in patients withNAFLD. Hepatology 2007;45(04):846–854
148 Sterling RK, Lissen E, Clumeck N, et al; APRICOT Clinical Inves-tigators. Development of a simple noninvasive index to predictsignificant fibrosis in patients with HIV/HCV coinfection. Hep-atology 2006;43(06):1317–1325
149 Angulo P, Bugianesi E, Bjornsson ES, et al. Simple noninvasivesystems predict long-term outcomes of patients with nonalco-holic fatty liver disease. Gastroenterology 2013;145(04):782–9.e4
150 McPherson S, Stewart SF, Henderson E, Burt AD, Day CP. Simplenon-invasive fibrosis scoring systems can reliably exclude ad-vanced fibrosis in patients with non-alcoholic fatty liver disease.Gut 2010;59(09):1265–1269
151 Harrison SA, Oliver D, Arnold HL, Gogia S, Neuschwander-TetriBA. Development and validation of a simple NAFLD clinicalscoring system for identifying patients without advanced dis-ease. Gut 2008;57(10):1441–1447
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al. 433

152 Ampuero J, Pais R, Aller R, et al; HEPAmet Registry. Developmentand validation of hepamet fibrosis scoring system-a simple,noninvasive test to identify patients with nonalcoholic fattyliver disease with advanced fibrosis. Clin Gastroenterol Hepatol2020;18(01):216–225.e5
153 Castera L, Friedrich-Rust M, Loomba R. Noninvasive assessmentof liver disease in patients with nonalcoholic fatty liver disease.Gastroenterology 2019;156(05):1264–1281.e4
154 Chen J, Talwalkar JA, Yin M, Glaser KJ, Sanderson SO, Ehman RL.Early detection of nonalcoholic steatohepatitis in patients withnonalcoholic fatty liver disease by using MR elastography. Radi-ology 2011;259(03):749–756
155 Noureddin M, Lam J, Peterson MR, et al. Utility of magneticresonance imaging versus histology for quantifying changes inliver fat in nonalcoholic fatty liver disease trials. Hepatology2013;58(06):1930–1940
156 European Association for Study of Liver Asociacion Latinoamer-icana para el Estudio del Higado. EASL-ALEH clinical practiceguidelines: non-invasive tests for evaluation of liver diseaseseverity and prognosis. J Hepatol 2015;63(01):237–264
157 Tapper EB, Challies T, Nasser I, Afdhal NH, Lai M. The perfor-mance of vibration controlled transient elastography in a UScohort of patients with nonalcoholic fatty liver disease. Am JGastroenterol 2016;111(05):677–684
158 Chen J, Yin M, Talwalkar JA, et al. Diagnostic performance of MRelastography and vibration-controlled transient elastography inthe detection of hepatic fibrosis in patients with severe tomorbid obesity. Radiology 2017;283(02):418–428
159 Adams LA, Chan WK. Noninvasive tests in the assessment ofNASH and NAFLD fibrosis: now and into the future. Semin LiverDis 2020;40(04):331–338
160 Loomba R, Adams LA. Advances in non-invasive assessment ofhepatic fibrosis. Gut 2020;69(07):1343–1352
161 Subramanian M, Wojtusciszyn A, Favre L, et al. Precision medi-cine in the era of artificial intelligence: implications in chronicdisease management. J Transl Med 2020;18(01):472
162 Sanyal AJ. Past, present and future perspectives in nonalcoholicfatty liver disease. Nat Rev Gastroenterol Hepatol 2019;16(06):377–386
163 Arrese M, Barrera F, Triantafilo N, Arab JP. Concurrent nonalco-holic fatty liver disease and type 2 diabetes: diagnostic andtherapeutic considerations. Expert Rev Gastroenterol Hepatol2019;13(09):849–866
164 Paik JM, Deshpande R, Golabi P, Younossi I, Henry L, Younossi ZM.The impact of modifiable risk factors on the long-term outcomesof non-alcoholic fatty liver disease. Aliment Pharmacol Ther2020;51(02):291–304
165 Saiman Y, Hooks R, Carr RM. High-risk groups for non-alcoholicfatty liver and non-alcoholic steatohepatitis development andprogression. Curr Hepatol Rep 2020;19:412–419
166 Koo BK, Joo SK, Kim D, et al. Development and validation of ascoring system, based on genetic and clinical factors, to deter-mine risk of steatohepatitis in asian patients with nonalcoholicfatty liver disease. Clin Gastroenterol Hepatol 2020;18(11):2592–2599.e10
167 European Association for the Study of the Liver (EASL) EuropeanAssociation for the Study of Diabetes (EASD) European Associa-tion for the Study of Obesity (EASO) EASL-EASD-EASO ClinicalPractice Guidelines for the management of non-alcoholic fattyliver disease. J Hepatol 2016;64(06):1388–1402
168 Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al.Weight loss through lifestyle modification significantly reducesfeatures of nonalcoholic steatohepatitis. Gastroenterology 2015;149(02):367–78.e5, quiz e14–e15
169 Bhogal MS, Langford R. Gender differences in weight loss;evidence from a NHSweight management service. Public Health2014;128(09):811–813
170 Shen J, Wong GL, Chan HL, et al. PNPLA3 gene polymorphism andresponse to lifestyle modification in patients with nonalcoholicfatty liver disease. J GastroenterolHepatol 2015;30(01):139–146
171 Krawczyk M, Jiménez-Agüero R, Alustiza JM, et al. PNPLA3 p.I148M variant is associated with greater reduction of liver fatcontent after bariatric surgery. Surg Obes Relat Dis 2016;12(10):1838–1846
172 Luukkonen PK, Qadri S, Lehtimäki TE, et al. The PNPLA3-I148Mvariant confers an antiatherogenic lipid profile in insulin-resistant patients. J Clin Endocrinol Metab 2021;106(01):e300–e315
173 Bianco C, Jamialahmadi O, Pelusi S, et al. Non-invasive stratifi-cation of hepatocellular carcinoma risk in non-alcoholic fattyliver using polygenic risk scores. J Hepatol 2021;74(04):775–782
174 Mato JM, Alonso C, NoureddinM, Lu SC. Biomarkers and subtypesof deranged lipidmetabolism in non-alcoholic fatty liver disease.World J Gastroenterol 2019;25(24):3009–3020
175 Alonso C, Fernández-Ramos D, Varela-Rey M, et al. Metabolomicidentification of subtypes of nonalcoholic steatohepatitis.Gastroenterology 2017;152(06):1449–1461.e7
176 Xing B, Zhao Y, Dong B, Zhou Y, LvW, ZhaoW. Effects of sodium-glucose cotransporter 2 inhibitors on non-alcoholic fatty liverdisease in patients with type 2 diabetes: a meta-analysis ofrandomized controlled trials. J Diabetes Investig 2020;11(05):1238–1247
177 Blazina I, Selph S. Diabetes drugs for nonalcoholic fatty liverdisease: a systematic review. Syst Rev 2019;8(01):295
178 Lv X, Dong Y, Hu L, Lu F, Zhou C, Qin S. Glucagon-like peptide-1receptor agonists (GLP-1 RAs) for the management of nonalco-holic fatty liver disease (NAFLD): a systematic review. EndocrinolDiabetes Metab 2020;3(03):e00163
179 Mantovani A, Byrne CD, Scorletti E, Mantzoros CS, Targher G.Efficacy and safety of anti-hyperglycaemic drugs in patientswithnon-alcoholic fatty liver disease with or without diabetes: Anupdated systematic review of randomized controlled trials.Diabetes Metab 2020;46(06):427–441
180 Mantovani A, Petracca G, Csermely A, Beatrice G, Targher G.Sodium-Glucose cotransporter-2 inhibitors for treatment ofnonalcoholic fatty liver disease: a meta-analysis of randomizedcontrolled trials. Metabolites 2020;11(01):22
181 WongC, YaowCYL, Ng CH, et al. Sodium-glucose co-transporter 2inhibitors for non-alcoholic fatty liver disease in asian patientswith type 2 diabetes: a meta-analysis. Front Endocrinol (Lau-sanne) 2021;11:609135
182 Drenth JPH, Schattenberg JM. The nonalcoholic steatohepatitis(NASH) drug development graveyard: established hurdles andplanning for future success. Expert Opin Investig Drugs 2020;29(12):1365–1375
183 Lin S, Huang J, Wang M, et al. Comparison of MAFLD and NAFLDdiagnostic criteria in real world. Liver Int 2020;40(09):2082–2089
184 Wai-Sun Wong V, Kanwal F. On the proposed definition ofmetabolic-associated fatty liver disease. Clin Gastroenterol Hep-atol 2021;19(05):865–870
185 Yamamura S, Eslam M, Kawaguchi T, et al. MAFLD identifiespatients with significant hepatic fibrosis better than NAFLD.Liver Int 2020;40(12):3018–3030
186 Lindén D, Ahnmark A, Pingitore P, et al. Pnpla3 silencing withantisense oligonucleotides ameliorates nonalcoholic steatohe-patitis and fibrosis in Pnpla3 I148M knock-in mice. Mol Metab2019;22:49–61
187 Kaiser J. NIH’s ‘precision nutrition’ bet aims for individualizeddiets. Science 2021;371(6529):552
188 Ross R, Goodpaster BH, Koch LG, et al. Precision exercise medi-cine: understanding exercise response variability. Br J SportsMed 2019;53(18):1141–1153
Seminars in Liver Disease Vol. 41 No. 4/2021 © 2021. The Author(s).
Nonalcoholic Fatty-Liver Disease Heterogeneity Arrese et al.434