Obstructing colonic cancer: the role of primary anastomosis · colonic obstruction in 10-30% cases...
52
Obstructing colonic cancer: the role of primary anastomosis Korhan Taviloglu, MD Department of Surgery Florence Nightingale Hospital, Istanbul, Turkey www.taviloglu.com 1 6th Congress of Hellenic Society of Trauma and Emergency Surgery – 17-19 February, 2011, Thessaloniki, Greece
Transcript of Obstructing colonic cancer: the role of primary anastomosis · colonic obstruction in 10-30% cases...

Obstructing colonic cancer: the role of primary
anastomosis Korhan Taviloglu, MD
Department of Surgery Florence Nightingale Hospital,
Istanbul, Turkey www.taviloglu.com
1
6th Congress of Hellenic Society of Trauma and Emergency Surgery – 17-19 February, 2011,
Thessaloniki, Greece
2

3
4
• Malignant tumors of the large bowel develop
colonic obstruction in 10-30% cases .
• Surgical decompression W colostomy and W
or WO resection and eventual re-anastomosis
is the traditional treatment of choice.
• Endoscopic decompression stents can allow
urgent stabilization for patients with malignant
obstruction requiring surgical palliation.
Al Samaraee et al, J Gastrointest Canc (2010)
Backgorund
5
• Cancer is the 2nd most common cause of bowel obstruction in adults
• Cancer-associated bowel obstruction is most frequently related to malignancies of gastrointestinal or ovarian origin (40 % incidence in advanced disease)
• Colonic cancer is the 2nd cancer killer in the USA
Colonic cancer obstruction

6
• Localization: Recto-sigmoid area (86 %), descending colon (11%), transverse colon (2 %), ascending colon (0.5 %)
• Duke’s A: 4 % • Distant metastases: 15 %
Sebastian S. Am J Gastroenterol 2004
Colonic cancer obstruction

7
• Intraluminal colonic tumor
• Intraperitoneal carcinomatosis associated with advanced or recurrent ovarian cancer with extrinsic compression
• Impaired GI motility as a result of tumor infiltration of mesenteric structures, bowel musculature or celiac plexus and associated edema
Colonic obstruction causes

8
• Peritumor inflammatory edema
• Fecal impaction
• Obstipation from opioids or anticholinergics
• Dysmotility as a result of autonomic failure or paraneoplastic autoimmunity
• Adhesions from previous surgery
Colonic obstruction causes

9
• For lesions of the right colon: right hemicolectomy with ileo-colic anastomosis
• 10% of these right sided anastomoses may leak
• Several alternatives for left colonic obstruction
Surgical alternatives for obstructing carcinoma of the colon
10
• The presence of strangulation carries a 30% mortality rate and, when suspected, surgical management must be considered emergently.
• Partial, non-strangulated obstruction is initially managed by medical means: bowel rest with NG suction, antiemetics, analgesics, and IV fluids.
Surgical decision making for obstructing carcinoma of the colon

11
1. Resection & primary anastomosis 2. Resection & anastomosis w proximal stoma 3. Hartmann’s procedure 4. Diverting colostomy / ileostomy 5. Colostomy & mucous fistula 6. Subtotal colectomy 7. Surgical bypass 8. Palliative stenting 9. Stenting as a bridge to surgery
Surgical alternatives for obstructing carcinoma of the colon

12
Hospital stay (days)
Morbidity %
Mortality %
Hartmann 17-30 20-30 6 - 12
Subtotal colectomy
10-20 6-44 6
Colostomy 30-55 20-40 2-15
Surgical alternatives for obstructing carcinoma of the colon
13
• 70-80 % undergo resection of the tumor in the 1st operation
• Hospital stay: 30-55 days • 25 % of patients prefer closure of the
stoma • Mortality: 2-15 % • Morbidity 20-40 %
Colostomy

14
• Welch et al (1973): a 2 % mortality for colostomy, 60 % for primary resection
• Ohman et al (1982): 5% mortality for colostomy & 14 % for primary resection
• It has been proposed that increased fecal load may not cause any increase in the rate of anastomotic leakage (Schrock, 1973; Irving- 1987)
Colostomy vs. primary anastomosis
15
• Many authors proposed primary resection with immediate anastomosis as the ideal treatment of obstructing colo-rectal carcinoma
• Leakage rate: 2-5 % • Mortality rate: 3-10 %
Primary anastomosis

16
• Surgical units headed by specialist (colo-rectal) consultants choose primary resection and anastomosis in 67% cases as compared to 41% by units headed by non-specialist consultants (p<0.05, significant).
(Darby, 1992)
Primary anastomosis
17
• A safer option with acceptable mortality and morbidity
• However reversal of the Hartmann’s procedure is a major task with a higher morbidity and mortality compared to a loop stoma
• Major morbidity occurs in 30% and mortality rate is 6% to 12%, hospital stay 17-30 days
• Therefore; some groups favor, colostomy & mucous fistula, following primary resection
Hartmann’s procedure

18
• No stoma problem • One stage procedure • Shorter hospital stay • Removes sychronous
proximal neoplasms & reduced risk of metachronous lesions
• Increase in the operating time
• Debilitating PO diarrhea and fecal incontinence in the elderly patients.
Advantages Disadvantages
Subtotal colectomy

19
Proximal colon adenocarcinoma (n: 1,492)
• Proximal colonic ca. W obstruction 306 patients (20.5 %)
• Proximal colonic ca. WO obstruction 1,186 patients (79.5
%)
Outpatient visits every 3-6 months
Mean follow-up period 77.7 months

20
Chin et al. Int Jcolorectal Dis, 2010
Better

21
Chin et al. Int Jcolorectal Dis, 2010

• Stent insertion may decompress the obstructed colon, allowing optimal colonic cleansing and subsequent colon resection.
• After colonic decompression, laparoscopic resection also has had been reported.
22
Stipa et al. Surg Endosc, 2008

23

• Colonic stenting as a bridge to surgery is more effective
and less (3,135 USD) costly than surgery in the
treatment of emergent, malignant left colonic
obstruction.
• The benefits are most pronounced in high-risk patients
and are diminished by increases in stent placement
failure rates and perforation rates.
• In low-risk patients, the benefits are more modest and
may not outweigh the risks.
24 Govindarajan et al, Dis Colon Rectum 2007

• Average monthly cost of a newly created stoma was
higher than that of a chronic stoma because of more
frequent home nursing visits.
• The time period associated with a newly created
stoma was defined from the creation of the colostomy
up to the time when stoma closure would be
attempted (3 or 6 months).
25
Govindarajan et al, Dis Colon Rectum 2007

26

27
Colonic obstruction – Endoscopy

28
• Temporary stents • Permanent stents (self expandable wallstent)
Colonic obstruction – Endoscopy

29
Shin et al, JASCRS 2008
30
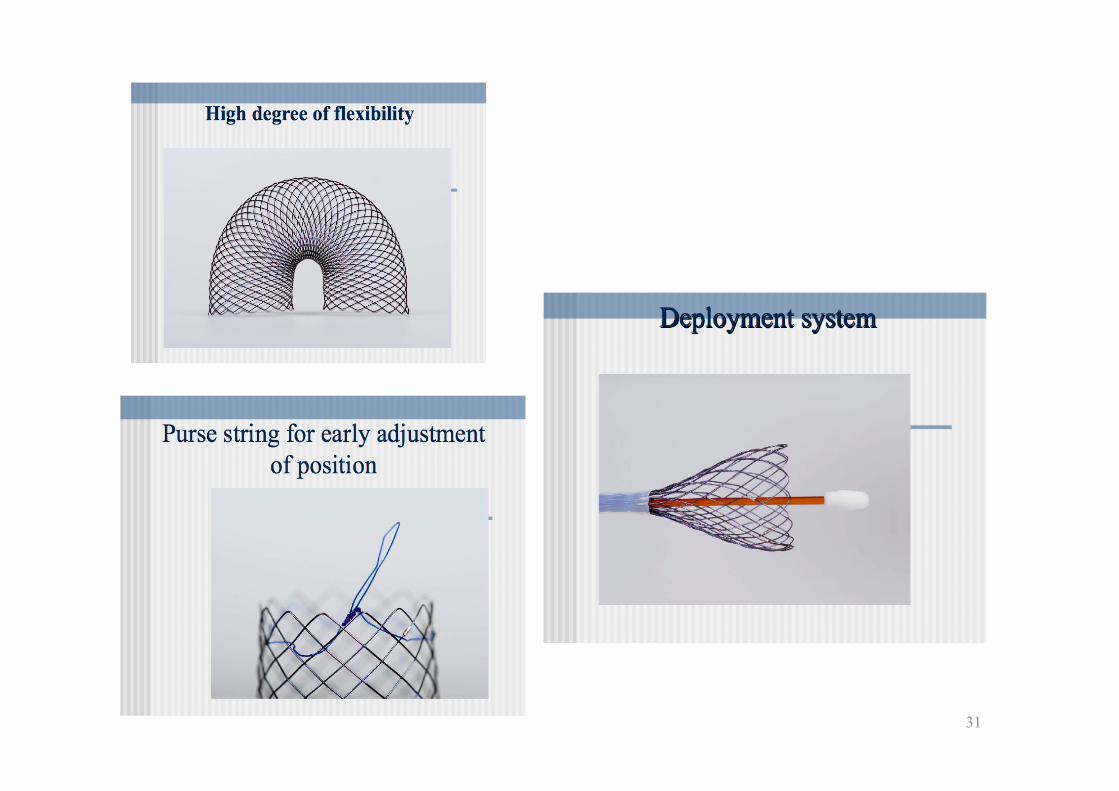
31

32

33
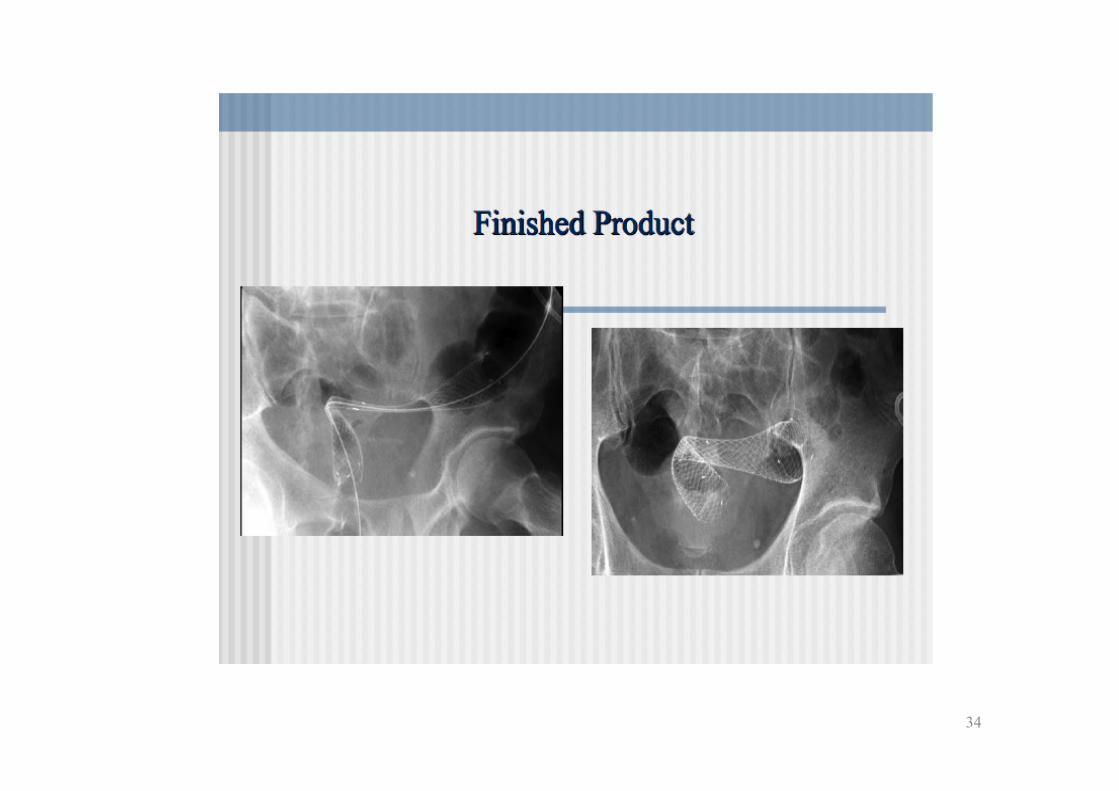
34

35
Shin et al, JASCRS 2008

36
Early complications - Stent placement failure / malplacement (6-10 %) - Migration (10-25 %) - Perforation (5 %) - Mortality 0.6 %
Late complications (25 %) - Stent re-obstruction (tumor or fecaloma) – 5-10 % - 2nd stent placement??? - Fecal incontinence - Perforation
Stent related complications

37
• A review of 54 publications - 1,198 patients
• Mortality rate 0.5 %
• Clinical success rate: 94 %
• Technical success rate: 91 %
• Clinical success as a bridge to surgery: 72 %
• Palliative & bridge to surgery results are
similar Sebastian S. Am J Gastroenterol 2004
Analysis of stenting results for obstructing colonic tumors

38
Stent diameter
(mm)
Length delivery catheter
(cm)
Delivery catheter size (F)
Material
Z® 25 40 31 Stainless steel
Memotherm®
25,30 120 14.5 Nitinol
Enteral wallflex®
18,20,22 136, 266 10 Nitinol
Precision ultraflex®
30 69 / 90 / 120
16 Nitinol
Corectcoil® 16,20 80 32 Nitinol Choostent®
22 75 / 120 12 Nitinol
Niti – S 20,22,24 100 24 Nitinol
Self expandable metallic stents

39

40
41
• Stent insertion succesful in 226 /244 patients (93 %)
• Mean length of hospital stay, 7 days less in the stent group
• Less mortality in stenting (p=0.03) • Less complications in stenting (p< 0.001) • Less stoma formation in stenting
(p< 0.001) Tilney et al, Surg Endosc 2007.
Colon stenting vs. surgery for malignant colon obstruction

42
• Duke’s stage • ASA stage • Advanced nodal involvement • pre-treatment CEA levels • Perforation • Obstruction
Serafini, 1998 Wagman, 1990 Carraro 2001
Poor prognosis

43
• Age • ASA grade • Operative urgency • Dukes’ stage
Predictors of outcome
Tekkis PP, et al. Ann Surg 2004, 204: 76–81.

44
• In a 80 year old patient with an unresectable obstructed colonic tumor, mortality rate is > 70 %
• ‘’Only stenting may be a better treatment option.’’
Palliative stenting in malignant colonic obstruction

45
46
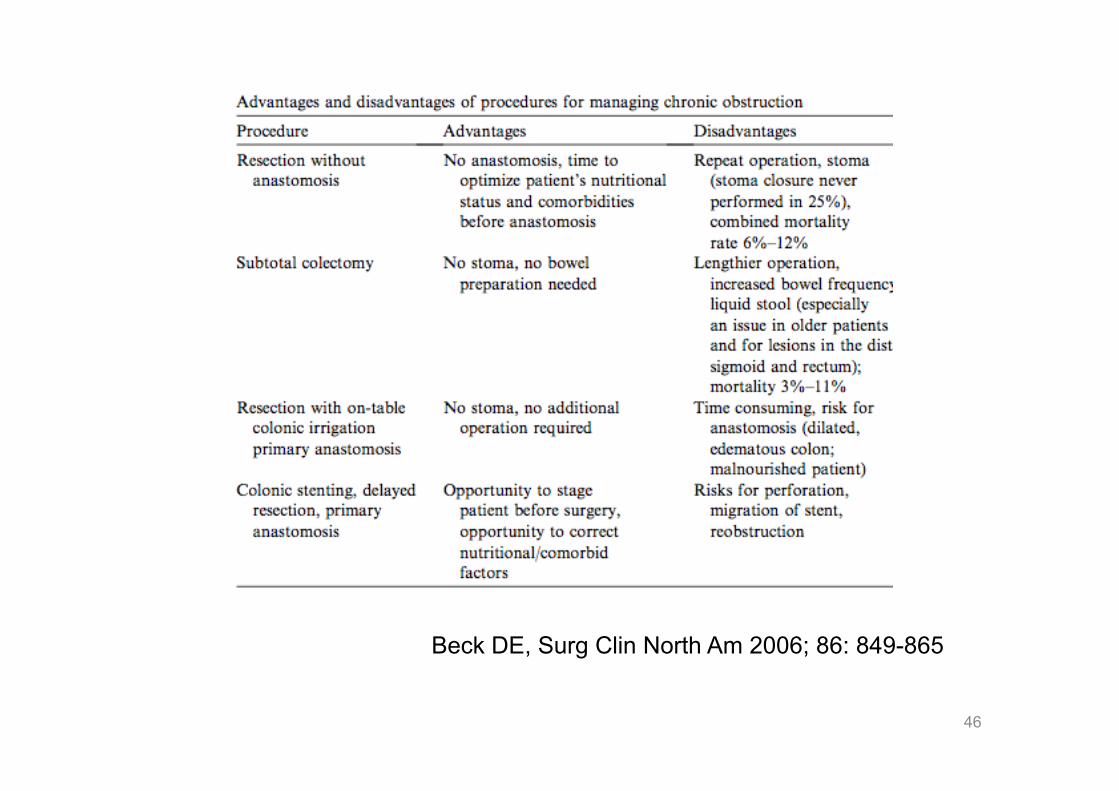
Beck DE, Surg Clin North Am 2006; 86: 849-865

47
Loop colostomy vs. Hartmann’s procedure
• There is only one RCT study, by Kronborg et al in 1995 • Compares emergency colostomy with three stages
procedure (58 patients) versus HP (63 patients) for obstructing colonic tumors.
• No difference in terms of mortality & morbidity rate, recurrence rate and cancer specific survival
• This RCT has some important limitations due to methodological flaws: no prior sample size estimation; a 15-year accrual period; procedures being performed by 36 attending and training surgeons; incomplete follow up; heterogeneous underlying pathology (with non-malignant strictures accounting for 14% of cases).
48 Kronborg O: Int J Colorectal Dis 1995, 10: 1–5.

Hartmann’s procedure (HP) vs. primary
resection and anastomosis (PRA) • There are no RCT’s comparing HP and
PRA; thus neither grade A and B evidence are available.
• HP offers no overall survival benefit compared to segmental colonic resection with primary anastomosis in obstructing left colon cancer (Grade of recommendation 2C+); HP should be considered in patients with high surgical risk (Grade of recommendation 2C)
49
Ansolini L, et al. WJES 2010, 5:29

Total or subtotal colectomy (TC)
vs segmental colectomy (SC)
• There is only one RCT, write out SCOTIA study group (Subtotal Colectomy versus on Table Irrigation and Anastomosis) in 1995, that compared the TC (47 patients) vs. SC (44 patients) and ICI.
• There were no differences in mortality, overall morbidity and rates of infection.
• In regard of long-term outcomes, patients undergoing TC were noted to have a statistically higher number of daily bowel movements compared to ICI/SC. The authors concluded that SC following ICI should be therefore preferred to TC.
50 Br J Surg 1995, 82: 1622–1627.

51
• For the treatment of obstructing colonic tumors, colonic stenting should be the first choice of treatment as a bridge for surgery.
• If stenting is not succesful, or in the presence of a complication, primary resection and anastomosis may be the treatment option in experienced centers.
‘’CONCLUSION’’

Thank you! Korhan Taviloglu
Department of Surgery Florence Nightingale Hospital,
Istanbul, Turkey www.taviloglu.com
52 www.taviloglu.com
6th Congress of Hellenic Society of Trauma and Emergency Surgery – 17-19 February, 2011,
Thessaloniki, Greece