Objectives: Combating Sulfonylurea Induced Hypoglycemia ... · her other laboratory values are...
19
Combating Sulfonylurea‐Induced Hypoglycemia. Octreotide to the Rescue! Patrick Dougherty, PharmD, BCPS Assistant Professor of Pharmacy Practice ‐ Emergency Medicine University of Maryland Eastern Shore School of Pharmacy & Health Professions Princess Anne, MD Objectives: • Describe the statistics and characteristics of sulfonylurea poisonings. • Explain the mechanisms of action of sulfonylureas and octreotide as an antidote. • Explain the mechanism of sulfonylurea‐induced recurrent hypoglycemia. • Evaluate the clinical evidence behind the use of octreotide as an antidote for sulfonylurea poisoning. • Create a medication therapy plan for managing a patient with sulfonylurea‐induced hypoglycemia. Background: Exposures of Sulfonylureas • American Association of Poison Control Centers (AAPCC) 2012 Annual Report • 4,206 exposures involved sulfonylureas • ≤ 5 years old – 850 cases (20%) • 1,449 cases unintentional (34%) • 66 adverse reactions • 1,291 cases treated in a health care facility • Included in 1 death Mowry, et al. 2012 Annual Report of the AAPCC’s NPDS. Clinical Toxicology. 2013;949-1229. Background: SFUs • 1 st generation: • Acetohexamide • Chlorpropamide • Tolazamide • Tolbutamide • 2 nd /3 rd generation: • Glipizide • Glyburide • Glimepiride Carr R, et al. Octreotide for Sulfonylurea-Induced Hypoglycemia Following Overdose. Ann Pharmacother. 2002;36:1727-32. Background: SFUs • Times to peak: 1‐12 hours • Half‐lives: 3‐76 hours • Durations of action: 6‐60 hours • Weakly active hepatic metabolites • Negligible fecal elimination • Extended‐release formulations • Combination products Carr R, et al. Octreotide for Sulfonylurea-Induced Hypoglycemia Following Overdose. Ann Pharmacother. 2002;36:1727-32. Glatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology. 2012;795-804. Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology, Toxicity, and Treatment. Ann Emerg Med. 2001;38:68-78. Evidence of Toxicity: • 2‐year old girl found with father’s glipizide XL 10 mg • Pediatrician: “observe for changes in behavior” • 4 hours later lethargy to emergency department (ED) • Serum glucose concentration (SGC): 39 mg/dL • 2 mL/kg D50W, food & juice • 1 hour later lethargy, 47 mg/dL • Admission of 2 days Little GL, et al. Are One or Two Dangerous? Sulfonylurea Exposure in Toddlers. J Emerg Med. 2005;28(3):305-10. 2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes © 2014 American Society of Health-System Pharmacists 1
Transcript of Objectives: Combating Sulfonylurea Induced Hypoglycemia ... · her other laboratory values are...

Combating Sulfonylurea‐Induced Hypoglycemia. Octreotide to the
Rescue!Patrick Dougherty, PharmD, BCPS
Assistant Professor of Pharmacy Practice ‐ Emergency MedicineUniversity of Maryland Eastern Shore School of Pharmacy & Health Professions
Princess Anne, MD
Objectives:
• Describe the statistics and characteristics of sulfonylurea poisonings.
• Explain the mechanisms of action of sulfonylureas and octreotide as an antidote.
• Explain the mechanism of sulfonylurea‐induced recurrent hypoglycemia.
• Evaluate the clinical evidence behind the use of octreotide as an antidote for sulfonylurea poisoning.
• Create a medication therapy plan for managing a patient with sulfonylurea‐induced hypoglycemia.
Background: Exposures of Sulfonylureas
• American Association of Poison Control Centers (AAPCC) 2012 Annual Report
• 4,206 exposures involved sulfonylureas
• ≤ 5 years old – 850 cases (20%)
• 1,449 cases unintentional (34%)
• 66 adverse reactions
• 1,291 cases treated in a health care facility
• Included in 1 deathMowry, et al. 2012 Annual Report of the AAPCC’s NPDS. Clinical Toxicology. 2013;949-1229.
Background: SFUs
• 1st generation:
• Acetohexamide
• Chlorpropamide
• Tolazamide
• Tolbutamide
• 2nd/3rd generation:
• Glipizide
• Glyburide
• Glimepiride
Carr R, et al. Octreotide for Sulfonylurea-Induced Hypoglycemia Following Overdose. Ann Pharmacother. 2002;36:1727-32.
Background: SFUs
• Times to peak: 1‐12 hours
• Half‐lives: 3‐76 hours
• Durations of action: 6‐60 hours
• Weakly active hepatic metabolites
• Negligible fecal elimination
• Extended‐release formulations
• Combination products
Carr R, et al. Octreotide for Sulfonylurea-Induced Hypoglycemia Following Overdose. Ann
Pharmacother. 2002;36:1727-32.
Glatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology.
2012;795-804.
Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology,
Toxicity, and Treatment. Ann Emerg Med. 2001;38:68-78.
Evidence of Toxicity:• 2‐year old girl found with father’s glipizide XL 10 mg
• Pediatrician: “observe for changes in behavior”
• 4 hours later lethargy to emergency department (ED)
• Serum glucose concentration (SGC): 39 mg/dL
• 2 mL/kg D50W, food & juice
• 1 hour later lethargy, 47 mg/dL
• Admission of 2 days
Little GL, et al. Are One or Two Dangerous? Sulfonylurea Exposure in Toddlers. J Emerg Med. 2005;28(3):305-10.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 1

Evidence of Toxicity:
• Life‐threatening hypoglycemia in poisoning/overdose (OD)
• 30% of pediatric exposures hypoglycemia
• All potential SFU ingestions by young children refer to ED
• Toxicity from accidental or intentional ingestion; hepatic or renal impairment; adverse effect
Glatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology. 2012;795-804.
Little GL, et al. Are One or Two Dangerous? Sulfonylurea Exposure in Toddlers. J Emerg Med. 2005;28(3):305-10.
Spiller HA, et al. Prospective Multicenter Study of Sulfonylurea Ingestion in Children. J Pediatr. 1997;131(1):141-6
Pharmacology of SFUs• Agonize SFU‐receptor subunit on K+ channel
• Stimulate depolarization of pancreatic β cells• Prevent efflux of K+ through ATP‐mediated channel
• Changes in membrane potential influx of Ca++
• Ca++ activates enzymes for insulin production & secretion
• Regardless of plasma glucose concentration
• Greater pharmacologic effects, longer durations of action in OD
Bosse GM. Antidiabetics and Hypoglycemics. In: Nelson LS, et al, editors. Goldfrank’s Toxicologic
Emergencies. 9th ed. New York: McGraw-Hill;2011. chapter 48.
Doyle ME, et al. Pharmacological Agents that Directly Modulate Insulin Secretion. Pharmacol Rev.
2003;55:105-31.
Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology, Toxicity, and
Treatment. Ann Emerg Med. 2001;38:68-78.
Pharmacology of SFUs
Bosse GM. Antidiabetics and Hypoglycemics. In: Flomenbaum NE, et al, editors. Goldfrank’s Toxicologic Emergencies. 8th ed. New York: McGraw-Hill; 2002. p.749-63.
SFU‐Induced Recurrent Hypoglycemia (SIRH):
• MS: 68‐year old female
• Overdose of glyburide
• Lethargic & confused; SGC = 35 mg/dL
• What do you want to do for MS? How do you want to monitor for its effectiveness?
• Dextrose!
• Serum glucose concentrations q hour!
SIRH Mechanism: SFU‐Induced Recurrent Hypoglycemia:
• What do you want to do for MS?
• What are the pharmacologic options?
• Dextrose!
• Glucagon?
• Diazoxide?
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 2

Octreotide:
• Long‐acting somatostatin analog
• FDA approvals:
• Acromegaly, metastatic carcinoid, vasoactive intestinal secreting tumors
• Suppresses secretion of hormones:
• Gastrin, Cholecystokinin, Growth Hormone, TSH, Glucagon, Insulin
• AAPCC 2012 Annual Report:
• Administered in 356 cases (70% in ≥ adults)Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology, Toxicity,
and Treatment. Ann Emerg Med. 2001;38:68-78.
Lheureux PE, et al. Bench-to-Bedside Review: Antidotal Treatment of Sulfonylurea-Induced
Hypoglycemia with Octreotide. Critical Care. 2005;9:543-9.
Mowry, et al. 2012 Annual Report of the AAPCC’s NPDS. Clinical Toxicology. 2013;949-1229.
Octreotide:• Mechanism of action as antidotal therapy:
• Agonist at somatostatin‐receptor on voltage‐gated Ca++ channels at pancreatic β cells
• Closing of Ca++ channels decrease influx of Ca++ decrease activation of enzymes for insulin production & secretion
• “Downstream” of SFU agonism
Glatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology. 2012;795-
804.
Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology, Toxicity,
and Treatment. Ann Emerg Med. 2001;38:68-78.
Lheureux PE, et al. Bench-to-Bedside Review: Antidotal Treatment of Sulfonylurea-Induced
Hypoglycemia with Octreotide. Critical Care. 2005;9:543-9.
Bosse GM. Antidiabetics and Hypoglycemics. In: Flomenbaum NE, et al, editors. Goldfrank’s Toxicologic Emergencies. 8th ed. New York: McGraw-Hill; 2002. p.749-63.
Octreotide
Mechanism of Octreotide:
Octreotide:• Peak effect: 30 minutes (subcutaneous)• Elimination half‐life: 1.5 hours• Duration of action: 6‐12 hours subcutaneous, 4 hours IV
• Dosing:• 50 mcg subcutaneously every 6 hours until resolution of
hypoglycemia• Pediatric: 4‐5 mcg/kg/d divided every 6 hours up to adult
dose (1 mcg/kg per dose)• Can be increased to 100 mcg; wide therapeutic windowGlatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology.
2012;795-804.
Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology,
Toxicity, and Treatment. Ann Emerg Med. 2001;38:68-78.
Lheureux PE, et al. Bench-to-Bedside Review: Antidotal Treatment of Sulfonylurea-Induced
Hypoglycemia with Octreotide. Critical Care. 2005;9:543-9.
Octreotide:• Antidotal use:
• Treat recurrent hypoglycemia induced by SFUs & refractory to administration of intravenous dextrose
• Adverse effects:
• Hyperglycemia…
• Nausea, abdominal pain, diarrhea, flatulence
• Bradycardia, prolonged QTc with long term use
Glatstein M. et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology.
2012;795-804.
Harrigan RA, et al. Oral Agents for the Treatment of Type 2 Diabetes Mellitus: Pharmacology,
Toxicity, and Treatment. Ann Emerg Med. 2001;38:68-78.
Lheureux PE, et al. Bench-to-Bedside Review: Antidotal Treatment of Sulfonylurea-Induced
Hypoglycemia with Octreotide. Critical Care. 2005;9:543-9.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 3
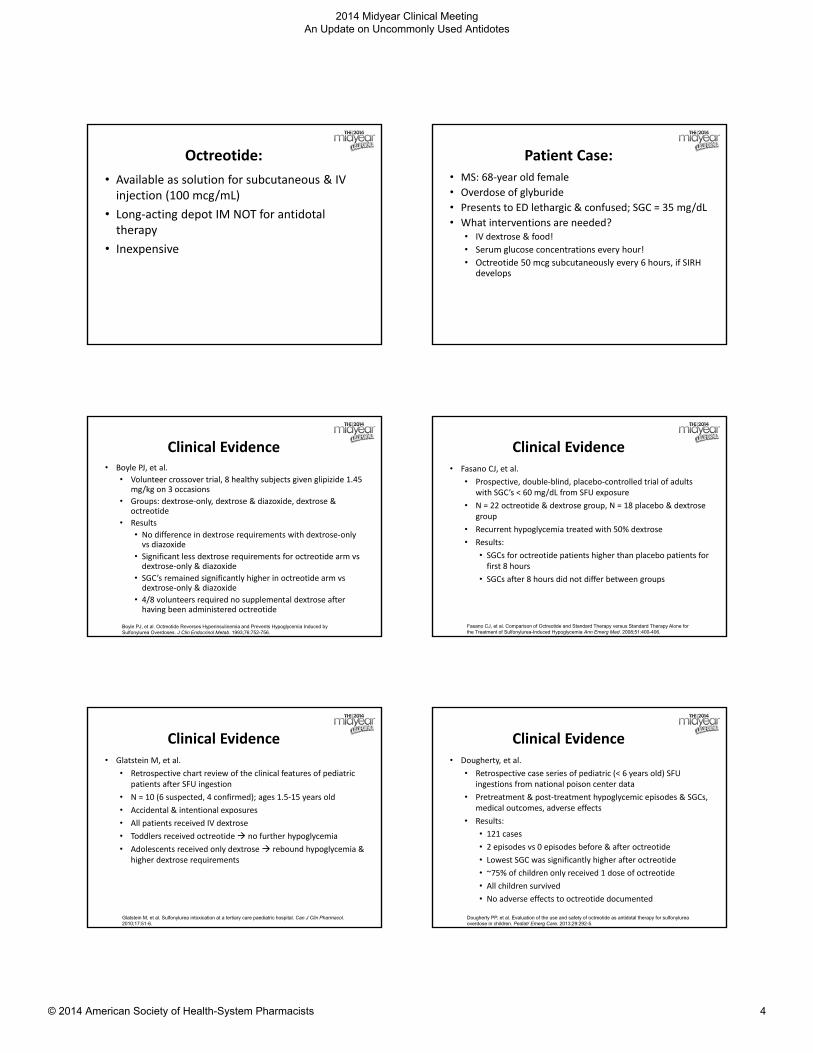
Octreotide:
• Available as solution for subcutaneous & IV injection (100 mcg/mL)
• Long‐acting depot IM NOT for antidotal therapy
• Inexpensive
Patient Case:• MS: 68‐year old female
• Overdose of glyburide
• Presents to ED lethargic & confused; SGC = 35 mg/dL
• What interventions are needed?• IV dextrose & food!
• Serum glucose concentrations every hour!
• Octreotide 50 mcg subcutaneously every 6 hours, if SIRH develops
Clinical Evidence• Boyle PJ, et al.
• Volunteer crossover trial, 8 healthy subjects given glipizide 1.45 mg/kg on 3 occasions
• Groups: dextrose‐only, dextrose & diazoxide, dextrose & octreotide
• Results
• No difference in dextrose requirements with dextrose‐only vs diazoxide
• Significant less dextrose requirements for octreotide arm vs dextrose‐only & diazoxide
• SGC’s remained significantly higher in octreotide arm vs dextrose‐only & diazoxide
• 4/8 volunteers required no supplemental dextrose after having been administered octreotide
Boyle PJ, et al. Octreotide Reverses Hyperinsulinemia and Prevents Hypoglycemia Induced by Sulfonylurea Overdoses. J Clin Endocrinol Metab. 1993;76:752-756.
Clinical Evidence• Fasano CJ, et al.
• Prospective, double‐blind, placebo‐controlled trial of adults with SGC’s < 60 mg/dL from SFU exposure
• N = 22 octreotide & dextrose group, N = 18 placebo & dextrose group
• Recurrent hypoglycemia treated with 50% dextrose
• Results:
• SGCs for octreotide patients higher than placebo patients for first 8 hours
• SGCs after 8 hours did not differ between groups
Fasano CJ, et al. Comparison of Octreotide and Standard Therapy versus Standard Therapy Alone for the Treatment of Sulfonylurea-Induced Hypoglycemia Ann Emerg Med. 2008;51:400-406.
Clinical Evidence• Glatstein M, et al.
• Retrospective chart review of the clinical features of pediatric patients after SFU ingestion
• N = 10 (6 suspected, 4 confirmed); ages 1.5‐15 years old
• Accidental & intentional exposures
• All patients received IV dextrose
• Toddlers received octreotide no further hypoglycemia
• Adolescents received only dextrose rebound hypoglycemia & higher dextrose requirements
Glatstein M, et al. Sulfonylurea intoxication at a tertiary care paediatric hospital. Can J Clin Pharmacol. 2010;17:51-6.
Clinical Evidence• Dougherty, et al.
• Retrospective case series of pediatric (< 6 years old) SFU ingestions from national poison center data
• Pretreatment & post‐treatment hypoglycemic episodes & SGCs, medical outcomes, adverse effects
• Results:
• 121 cases
• 2 episodes vs 0 episodes before & after octreotide
• Lowest SGC was significantly higher after octreotide
• ~75% of children only received 1 dose of octreotide
• All children survived
• No adverse effects to octreotide documented
Dougherty PP, et al. Evaluation of the use and safety of octreotide as antidotal therapy for sulfonylurea overdose in children. Pediatr Emerg Care. 2013;29:292-5.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 4

Clinical Evidence• Recent Case Reports ‐ Adults
• Adverse effect of therapeutic use of SFU:
• Arora A. Hypoglycaemia begets hypoglycaemia. BMJ. 2013;28:2013.
• Barkin JA, et al. Octreotide: a novel therapy for refractory sulfonylurea‐induced hypoglycemia. Pancreas. 2013;42:722‐3.
• Gonzalez RR, et al. Octreotide therapy for recurrent refractory hypoglycemia due to sulfonylurea in diabetes‐related kidney failure. Endocr Pract. 2007;13:417‐423.
• Vallurupalli S. Safety of subcutaneous octreotide in patients with sulfonylurea‐induced hypoglycemia and congestive heart failure. Ann Pharmacother. 2010: 44:387‐90
Clinical Evidence• Recent Case Reports – Pediatrics
• Cerebral edema:
• Llomado R, et al. Continuous octreotide infusion for sulfonylurea‐induced hypoglycemia in a toddler. J Emerg Med. 2013;46:209‐13.
• Delayed hypoglycemia:
• Pelavin PI, et al. Extended‐release glipizide overdose presenting with delayed hypoglycemia and treated with subcutaneous octreotide. J Pediatr Endocrinol Metab. 2009;22:171‐5.
Clinical Evidence• Review articles
• Dougherty PP, et al. 2010
• Sufficient evidence to recommend the use of octreotide with supplemental dextrose for the treatment of sulfonylurea‐induced hypoglycemia.
• Glatstein M, et al. 2012
• Limited, available data suggest that octreotide should be considered first‐line therapy in all cases (pediatric & adult) of SFU poisoning with evidence of hypoglycemia.
• Octreotide may need to be re‐dosed to prevent recurrent hypoglycemia.
Dougherty PP, et al. Octreotide’s role in the management of sulfonylurea-induced hypoglycemia. J Med Toxicol. 2010;6:199-206.
Glatstein M, et al. Octreotide for the treatment of sulfonylurea poisoning. Clinical Toxicology. 2012;50:795-804.
Objectives:• Describe the statistics and characteristics of sulfonylurea poisonings.
• Explain the mechanisms of action of sulfonylureas and octreotide as an antidote.
• Explain the mechanism of sulfonylurea‐induced recurrent hypoglycemia.
• Evaluate the clinical evidence behind the use of octreotide as an antidote for sulfonylurea poisoning.
• Create a medication therapy plan for managing a patient with sulfonylurea‐induced hypoglycemia.
BN is a 24 year‐old female who intentionally ingested 20 tablets of glipizide 10 mg in a suicidal gesture approximately 2 hours ago. She presents to the ED and is lethargic,
diaphoretic, and tremulous. Her serum glucose concentration is found to be 30 mg/dL. All of her other laboratory values are unremarkable.
Which of the following medication therapy plans is most appropriate to recommend for BN
at this time?
Administer dextrose 25 g orally and re‐administer if she becomes hypoglycemic, along with an IV infusion of 5% dextrose.
Administer dextrose 25 g IV bolus and re‐administer if she becomes hypoglycemic, along with an IV infusion of 5% dextrose.
Administer glucagon 1 mg IV for correction of her hypoglycemia, along with an IV infusion of 5% dextrose.
Administer octreotide 50 mcg subcutaneously for correction of her hypoglycemia, along with an IV infusion of 5% dextrose.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 5

Administer dextrose 25 g orally and re‐administer if she becomes hypoglycemic, along with an IV infusion of 5% dextrose.
Administer dextrose 25 g IV bolus and re‐administer if she becomes hypoglycemic, along with an IV infusion of 5% dextrose.
Administer glucagon 1 mg IV for correction of her hypoglycemia, along with an IV infusion of 5% dextrose.
Administer octreotide 50 mcg subcutaneously for correction of her hypoglycemia, along with an IV infusion of 5% dextrose.
Despite your initial recommendation & intervention, BN’s serum glucose concentration decreases to 25 mg/dL one hour later and she is found to be
lethargic and slow to respond.
Which of the following medication regimens is most appropriate to administer to BN at this time?
Administer dextrose 25 g orally along with octreotide 50 mcg subcutaneously followed by 3 more doses each 2 hours apart.
Administer dextrose 25 g IV along with glucagon 1 mg IV followed by 3 more doses each 3 hours apart.
Administer dextrose 25 g IV along with 50 mcg of octreotide subcutaneously followed by 3 more doses each 6 hours apart.
Administer dextrose 25 g orally along with glucagon 1 mg IV followed by 3 more doses each 6 hours apart.
Administer dextrose 25 g orally along with octreotide 50 mcg subcutaneously followed by 3 more doses each 2 hours apart.
Administer dextrose 25 g IV along with glucagon 1 mg IV followed by 3 more doses each 3 hours apart.
Administer dextrose 25 g IV along with 50 mcg of octreotide subcutaneously followed by 3 more doses each 6 hours apart.
Administer dextrose 25 g orally along with glucagon 1 mg IV followed by 3 more doses each 6 hours apart.
BN is admitted to the hospital for treatment of her overdose. Which of the following set of instructions is appropriate for how to manage the
care of BN?
Monitor her SGCs every hour during treatment and gradually titrate down the 5% dextrose IV.
Monitor her SGCs every 3 hours during treatment and administer 25 g of 50% dextrose IV if hypoglycemia recurs.
Monitor her SGCs every hour during treatment and administer glucagon 1 mg IV if hypoglycemia recurs.
Monitor her SGCs only after she orally consumes dextrose‐containing food and administer 25 g of 50% dextrose IV if hypoglycemia recurs.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 6

Monitor her SGCs every hour during treatment and gradually titrate down the 5% dextrose IV.
Monitor her SGCs every 3 hours during treatment and administer 25 g of 50% dextrose IV if hypoglycemia recurs.
Monitor her SGCs every hour during treatment and administer glucagon 1 mg IV if hypoglycemia recurs.
Monitor her SGCs only after she orally consumes dextrose‐containing food and administer 25 g of 50% dextrose IV if hypoglycemia recurs.
Key Takeaways• Key Takeaway #1
• Octreotide should be considered as antidotal therapy for SFU‐induced hypoglycemia (for both therapeutic‐use or overdose) refractory to the administration of dextrose.• Perhaps even first‐line?
• Key Takeaway #2• For patients with prolonged SFU‐induced hypoglycemia,
multiple doses of octreotide may be necessary.• Key Takeaway #3
• Octreotide can be safely given to pediatric patients experiencing SFU‐induced hypoglycemia refractory to the administration of dextrose.
Combating Sulfonylurea‐Induced Hypoglycemia. Octreotide to the
Rescue!Patrick Dougherty, PharmD, BCPSEmail: [email protected],
“HIE” Dose Insulin for Calcium‐Channel Blocker Overdose
Adrienne Perotti, Pharm D, BCPSClinical Specialist in Emergency Medicine/Toxicology
Presence Saints Mary and Elizabeth Medical Center, Chicago, IL
Objectives
• Define the morbidity and mortality of toxin induced cardiogenic shock
• Describe the pathophysiology of toxin induced cardiogenic shock due to calcium channel blocker (CCB) or Beta Blocker (BB) overdose.
• Discuss the use of high dose insulin‐euglycemia (HIE) in toxin induced cardiogenic shock due to CCB or BB overdose
• List the use of (HIE) in other toxins
Case Report• 17 yo F PA is presenting to the ED 3 hours post ingestion of
300 mg amlodipine tablets.• Vitals:
• HR 45, BP: 80/40, RR: 18, Wt: 55 kg• Physical Exam:
• She is awake but sleepy, diaphoretic with has active bowel sounds. Her extremities are cold with slow capillary refill.
• Current Treatments:• 2L NS fluid bolus given with 3rd L infusing• 3 mg atropine given IV• 2 gm of IV calcium chloride given• Norepinephrine IV infusion was started and is currently running at 10mcg/min
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 7

Introduction
• NPDS 2012 data
• Cardiovascular drug exposures account for 103,922/yr
• 2nd largest cause of overdose fatalities
• Majority due to Beta‐blockers (BBs) and Calcium channel blockers (CCBs)
• 3rd largest increase since last year
Mowry JB, et al. Clinical Toxicology(2013), 51:949‐1229.
Mechanism of Toxicity
Calcium Channel Blockers
• Bind to L‐type voltage sensitive calcium channels and prevent the transport of Ca2+
into cell
• Decreases chronotropicand inotropic effects in the myocardium
• Disrupts peripheral vascular resistance and regulation
• Block insulin release in β‐islet cells
Beta Blockers
• Antagonize beta‐adrenergic receptors which disrupt calcium channel influx into cell and release from the sarcoplasmic reticulum
• Decreases chronotropic and inotropic effects in the myocardium
• Disrupts peripheral vascular resistance and regulation
• Prevents gluconeogenesis and glycogenolysis
Kerns W. Emerg Med Clin N Am (2007), 25:309‐331.
Shepherd G. Am J Health‐Syst Pharm.2006;63:1828‐35.
Clinical Presentation
• Severity of symptoms is dependent on the patient and the amount of drug ingested
• Elderly
• Children
• Multiple co‐morbidities
• Hx of CHF, MI, myocardial dysfunction
• Multiple medications ingested
• Immediate release versus Sustained Release
Shepherd G. Am J Health‐Syst Pharm.2006;63:1828‐35.
Clinical Presentation
CCBs
• Bradycardia
• Dysrhythmias
• Hypotension
• Hyperglycemia
• Pulmonary Edema
• Cardiogenic Shock
• Cardiac Arrest
BBs
• Bradycardia
• Dysrhythmias
• Hypotension
• Hypoglycemia
• Bronchospasm
• Cardiogenic Shock
• Seizures
Shepherd G. Am J Health‐Syst Pharm.2006;63:1828‐35.
What is the most common presentation of a CCB & BB toxicity?
Tachycardia/Hypertension
Bradycardia/Hypertension
Tachycardia/Hypotension
Bradycardia/Hypotension
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 8

Traditional Therapy
• Supportive care
• Fluids
• Often effective in treating mild toxicity
• 10‐40 ml/kg bolus; repeat if necessary
• Caution in patients with CHF, renal dysfunction or signs of pulmonary edema
• Atropine
• Blocks parasympathetic pathway
• 0.5‐1mg q2‐3 min; max 3 mg
• Clinically ineffective in severe casesDeRoos FJ. Calcium Channel Blockers. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:884‐892.Brubacher JR. β‐Adrenergic Antagonistss. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:896‐909.
Traditional Therapy• Calcium
• Competes to override the voltage gated calcium channels to increase intracellular calcium
• Shown to reverse bradycardia and hypotension
• Dosing: 13‐25 mEq bolus with continuous infusion of 0.5mEq/kg/h
• Issues
• Often short lived and cannot overcome blockade in severe overdose
• Careful monitoring of serum calcium and phosphorous levels
DeRoos FJ. Calcium Channel Blockers. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:884‐892.Brubacher JR. β‐Adrenergic Antagonistss. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:896‐909.
Traditional Therapy• Vasopressors/Inotropes
• Beta‐Adrenergic agonists can facilitate cyclic AMP and increase calcium channel opening
• Alpha‐Adrenergic agonist peripherally can also activate receptor‐activated calcium channels
• Phosphodiesterase Inhibitors can prevent the degredation of cyclic AMP
• Conflicting data on effectiveness• May actually depress cardiac output by increasing oxygen demand and systemic vascular resistance
• Increased risk of tissue ischemia
DeRoos FJ. Calcium Channel Blockers. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:884‐892.Brubacher JR. β‐Adrenergic Antagonistss. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:896‐909.
Traditional Therapy
• Glucagon
• Stimulates cAMP through a separate G‐coupled protein receptor
• Creates positive inotropic and chronotropic effects
• Bolus of 50‐150 mcg/kg followed by infusion of 1‐10 mg/hr
• Nausea and vomiting occurs at the higher doses
• Case reports of ineffectivenessDeRoos FJ. Calcium Channel Blockers. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:884‐892.Brubacher JR. β‐Adrenergic Antagonistss. In Goldfrank’s Toxicologic Emergencies‐9th Edition., 2011:896‐909.
AC
Ca++
Ca++
Ca++
Ca++
Ca++
Troponin
Gs
β1
AerobicMetabolism
GlucoseGlucose
Glucose
Glucose
ATP
cAMP
Ca++ Ca++
Ca++
Ca++
Ca++
Ca++Ca++
EPI
Glucagon
PKA
Ca++
Ca++
Ca++
PDE
Ca++
Amrinone
Sarcoplasmic reticulum
1 23
4
Back to our Case• PA is now in the PICU. We are 10 hours post ingestion. PA
is currently on BIPAP for pulmonary edema and respiratory distress.• Current vitals: HR 55, BP: 85/45 mmHg, RR 30 and pt. is
currently altered and nauseous and retching • Current medications:
• Norepinephrine IV infusion at 30 mcg/min• Vasopressin IV infusion at 0.4 units/min• Phenylephrine IV infusion at 150 mcg/min• Hydrocortisone 100 mg IVP q8h• 9 L NS total has been given and is currently on 150 ml/hr NS infusion
• Glucagon IV infusion is at 10 mg/hr after a 10 mg bolus
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 9

What would you do in this scenario?
Increase phenylephrine drip to 200 mcg/min
Increase glucagon to 15 mg/hr
Add dobutamine at 1 mcg/kg/min
Call local poison center for HIE protocol
High Dose Insulin/Euglycemia (HIE)
• Mechanism of Action
• Provides intracellular transport of glucose to cardiac and skeletal muscle
• Preferred energy source in stressed myocardium
• Enhances inotropic effects
• Enhances endothelial nitric oxide synthase causing vascular dilation
• Enhances microvascular perfusionEngebretsen Km, et al. Clinical Toxicology (2011), 49:277‐283
Shepherd G. Am J Health‐Syst Pharm.2006;63:1828‐35.
Efficacy of HIE
Kline JA, et al. 1993
• Canine model
• Verapamil toxicity
• Compared saline, epinephrine, glucagon, calcium, or HIE
• Results (Survival)
• Saline: 0/6
• Epinephrine: 4/6
• Glucagon: 3/6
• Calcium: 3/6
• HIE: 6/6
Kerns W 2nd, et al. 1997
• Porcine model
• Propranolol toxicity
• Compared vasopressin with epinephrine, or HIE
• Results (Survival)
• Vasopressin/epinephrine
• 0/5
• HIE: 5/5
Kline JA, Tomaszewski CA, Schroeder JD, Raymond RM. J Pharmcol Exp Ther (1993), 267:744‐750.Kerns W 2ndet al. Ann Emerg Med (1997), 29:748‐757.
Efficacy of HIE• Yuan TH, et al. 1999
• Case Series (N=5 patients)• 4 verapamil• 1 amlodipine/atenolol
• Survival: 5• Average insulin dose: 0.5 units/kg/h• All had improved blood pressure and heart rate within 1 hour of therapy
• Adverse Events• Transient hypoglycemia: 4• Hypokalemia: 3• Hypomagnesemia: 3• Hypophosphatemia: 3
Yuan TH, et al. Clinical Toxicology (1999), 37:463‐474.
Efficacy of HIE
• Greene SL, et al. 2007
• Prospective observational study of an HIE protocol (N=7)
• CCB with SBP <90 mmHg despite other traditional therapies
• Loading dose: 25 gm dextrose IV followed by 1 unit/kg short‐acting insulin IV
• Maintenance dose: 0.5‐2.0 units/kg/hrGreene SL, et al. Intensive Care Med (2007), 33:2019‐2024.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 10

Efficacy of HIE
• Greene SL, et al. 2007
• Results
• Survival 6/7• Bolus insulin: 3 patients
• Improvement in blood pressure within 60 min
• Adverse events• Hypoglycemia: 1
• Hypokalemia: 2
Greene SL, et al. Intensive Care Med (2007), 33:2019‐2024.
HIE Treatment
• Standard protocol
• Initial bolus: 1 unit/kg
• Continuous infusion: 0.5‐10 units/kg/hr
• Titrate every 5 minutes
• Goal
• Maintain perfusion
• MAP, BP may not be obtainable
• Assess peripheral pulses, urine output, lactate levels
• Non invasive cardiac outputEngebretsen Km, et al. Clinical Toxicology (2011), 49:277‐283
HIE Treatment• Supportive measures
• Maintain blood glucose (BG) levels >100 mg/dL
• Check every 10 min during titration then hourly
• Continuous 5‐10% dextrose in ½ NS infusion at 80% maintenance
• Bolus of 25 gm of dextrose if BG <200 mg/dL
• Supplement and monitor potassium
• Check every hour during titration and then every 6 hours
• Monitor magnesium and phosphorous
Engebretsen Km, et al. Clinical Toxicology (2011), 49:277‐283
Back to Case PA
• HIE was started 13 hours post presentation
• 10 unit bolus of IV regular insulin
• BG >300 mg/dL
• Regular Insulin infusion started at 0.1 unit/kg/hr and titrated up to 1 unit/kg/hrwithin the hour
• 6 hours post HIE initiation
• Glucagon, hydrocortisone, phenylephrine, vasopressin discontinued
• Norepinephrine titrated to 5 mcg/min
What is the mechanism of action of HIE in toxin induced cardiogenic shock?
Enhances inotropic effects
Acts as a vasopressor
Enhances microvascular perfusion
Both A and C
Evidence of HIE in Other Cases of Toxin‐Induced Cardiogenic Shock
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 11

Holger JS et al. 2011• Retrospective chart review post implementation of toxin‐induced cardiogenic shock• N=12• All multiple co‐ingestions
• CCB: amlodipine, verapamil, diltiazem• BB: metoprolol, propranolol, atenolol, nebivolol• Antidepressants/Antipsychotics: citalopram, loxapine, buproprion, amitriptyline, escitalopram, venlafaxine, quetiapine
• Antihypertensives: quinapril, Lisinopril, furosemide
• Other: carbamazepine, tramadol, diphenhydramine, amiodarone
Holger JS, et al. Clinical Toxicology (2011), 49:653‐658
Holger JS et al. 2011• Protocol
• 20‐40 ml/kg NS bolus over 1 hour• Maintenance goal urine output 0.5 ml/kg/hr
• Calcium IV infused for goal ionized Calcium of 2 mmol/L
• Regular insulin bolus 1 unit/kg • Bolus dextrose if BG <200 mg/dL
• Regular insulin infusion• Initial: 1 unit/kg/h• Titrate: 1‐2 units/kg/h every 10‐15 minutes
• Max: 10 units/kg/h
Holger JS, et al. Clinical Toxicology (2011), 49:653‐658
Holger JS et al. 2011
• Results (N=12)
• Survival: 11/12
• Vasopressor use prior to HIE: (N=7)
• All were tapered off after HIE initiation
• Increase in BP>10 mmHg: 10/12
• Adverse events
• Hypoglycemia: 6/12
• Hypokalemia: 3/12
Holger JS, et al. Clinical Toxicology (2011), 49:653‐658
HIE can be used in toxin‐induced cardiogenic shock due to CCB and BB overdoses only.
True
False
Conclusion
• CCB and BB overdoses are common causes of toxin‐induced cardiogenic shock
• HIE use has been demonstrated effective in animal and human case studies for CCB and BB overdose when other traditional therapies have failed
• HIE should be considered earlier rather than later in the treatment of toxin‐induced cardiogenic shock
Key Takeaways• Key Takeaway #1
• HIE should be considered early in therapy in toxin‐induced cardiogenic shock due to CCB or BB overdose. In other toxin‐induced cardiogenic shock HIE should be considered, especially if traditional measures have failed.
• Key Takeaway #2• HIE protocol should be implemented in your hospital for cases of toxin‐induced cardiogenic shock
• Key Takeaway #3• Consult your local poison center for protocol recommendations at 1‐800‐222‐1222
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 12

Special Thanks
• Special thank you to Dr. Greene Shepherd for letting me use his cell slides and pictures along with ASHP.
“HIE” Dose Insulin for Calcium‐Channel Blocker Overdose
Adrienne Perotti, Pharm D, BCPSClinical Specialist in Emergency Medicine/Toxicology
Presence Saints Mary and Elizabeth Medical Center, Chicago, IL
Throwing the “Lipid Sink” at Toxicological‐Induced Cardiac Arrest
Bryan D. Hayes, PharmD, DABAT, FAACTClinical Pharmacy Specialist, EM & Toxicology
University of Maryland Medical CenterBaltimore, MD
“A 17 year‐old girl develops seizures, followed shortly by cardiovascular collapse, about 9 hours after ingesting full bottles of bupropion and lamotrigine.
“Resuscitation is attempted for more than one hour without sustained return of intact circulation.
“An anesthesiologist attending her for airway management suggests a novel antidotal therapy.”
Sirianni A, et al. Ann Emerg Med 2008;51(4):412‐5.
ED
Sirianni A, et al. Ann Emerg Med 2008;51(4):412‐5.
ICU
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 13

Sirianni A, et al. Ann Emerg Med 2008;51(4):412‐5.
Time Course
http://www.medline.com/media/catalog/sku/bhl/300x300/BHL2B6022_HRE01.JPG
www.lipidrescue.org
Guy Weinberg, MD
Lipid in Overdose?
Local Anesthetic
Non‐Local Anesthetic
Adult > 25 > 40
Pediatric > 7 > 7
Animal Numerous Numerous
Meeting Abstracts
Numerous Numerous
Supporting DataSupporting Data
Cave G, et al. Emerg Med Australas 2011;23(2):123‐41.Presley JD, et al. Ann Pharmacother 2013;47:735‐43.
<a href="https://www.flickr.com/photos/89334594@N07/8450190120/">infocux Technologies</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by‐nc/2.0/">cc</a>
Courtesy of scancrit.com
Lipid Sink
Weinberg GL. Anesthesiology 2012;117(1):180‐7.<a href="https://www.flickr.com/photos/25722571@N08/5579852238/">JaseCurtis</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by/2.0/">cc</a> French D, et al. Clin Toxicol 2011;49(4):340‐4.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 14

Fettiplace MR, et al. Crit Care Med 2013;41:e156‐62.Harvey M, et al. Br J Anaesth 2014;112(4):622‐5.
↑ FA Oxidation
Altered Ca2+
Homeostasis
Ion‐Channel Effects
http://heartresearch.org.uk/sites/default/files/pageimages/Heart%20iStock%20pic%20(1).jpg
T1/2 30‐60 min
MPS
<a href="https://www.flickr.com/photos/53552950@N00/2283676770/">ToniVC</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by‐nc‐nd/2.0/">cc</a>
CCB
BB
TCA
Local Anesthetic
Other<a href="https://www.flickr.com/photos/68387408@N00/142789779/">erix!</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by/2.0/">cc</a>
“Given the uncertainty of its beneficial effect in human poisonings, it is the opinion of the ACMT that there are no standard of care requirements to use, or to choose not to use, LRT.
“However, in circumstances where there is serious hemodynamic, or other, instability from a xenobiotic with a high degree of lipid solubility, LRT is viewed as a reasonable consideration for therapy, even if the patient is not in cardiac arrest.”
J Med Toxicol 2011;7:81‐2.
“…it may be reasonable to consider 1.5 mL/kg of 20% long‐chain fatty acid emulsion as an initial bolus, repeated every 5 minutes until cardiovascular stability is restored. After the patient is stabilized, some papers suggest a maintenance infusion of 0.25 mL/kg per minute for at least 30 to 60 minutes. A maximum cumulative dose of 12 mL/kg has been proposed.”
Vanden Hoek TL, et al. Circulation 2010;122(suppl 3):S829‐61.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 15

0.25 mL/kg/min0.25 mL/kg/min
J Med Toxicol 2011;7:81‐2.
1.5 mL/kg1.5 mL/kg
http://www.medline.com/media/catalog/sku/bhl/300x300/BHL2B6022_HRE01.JPG
TBW vs. LBWTBW vs. LBW
AdministrationAdministration
Neal JM, et al. Reg Anesth Pain Med 2010;112(2)277‐8.
https://www.flickr.com/photos/aussiegall/4348697776/
BPBP
HRHR
J Med Toxicol 2011;7:81‐2.Downes MA, et al. Emerg Med Australas 2014;26(3):286‐90.
<a href="https://www.flickr.com/photos/8294958@N03/3650559857/">digitalnoise</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by‐nc‐sa/2.0/">cc</a>
AllergyAllergy
PancreatitisPancreatitis
ALIALI
Fat emboliFat emboli
Levine M, et al. J Med Toxicol 2014;10:10‐4.Abdelmalek D, et al. Am J Ther 2013 Oct 3. [Epub ahead of print]Shenoy U, et al. Paediatr Anaesth 2014;24(3):332‐4.
Toxin releaseToxin release
DVTDVT
<a href="https://www.flickr.com/photos/31158400@N06/8575837986/">Gabludlow</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by‐nc‐nd/2.0/">cc</a>
Grunbaum AM, et al. Clin Toxicol 2012;50(9):812‐7.Cocchio C, et al. SOJ Pharm PharmSci 2014; 1(1): 3.
Lab interference
Lab interference
Stability with resus medsStability with resus meds
<a href="https://www.flickr.com/photos/103557556@N08/14152551068/">ssoloveys</a> via <a href="http://compfight.com">Compfight</a> <a href="https://creativecommons.org/licenses/by‐nc‐nd/2.0/">cc</a> Cocchio C, et al. SOJ Pharm PharmSci 2014;1(1):3.
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 16

Cole JB, et al. J Med Toxicol 2014; 10(3):307‐10.
Asystole?Asystole?
http://upload.wikimedia.org/wikipedia/commons/c/c7/Pacemaker_dependent_asystole.jpg
46 y/o 46 y/o GCS 3GCS 3 78/50 mmHg78/50 mmHg
What is the 1st line therapy?
Lipid emulsion
Norepinephrine
Sodium bicarbonate
Physostigmine
What is the 1st line therapy?
Lipid emulsion
Norepinephrine
Sodium bicarbonate
Physostigmine
1st Line1st Line
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 17

The patient weighs 85 kg. What is the 20% lipid emulsion dose?
1.5 mL/kg (LBW)
1.5 mL/kg (TBW)
100 mL
A, B, and C are all ok
The patient weighs 85 kg. What is the 20% lipid emulsion dose?
1.5 mL/kg (LBW)
1.5 mL/kg (TBW)
100 mL
A, B, and C are all ok
Non‐traditional use of lipid
Non‐traditional use of lipid
Stock in UBCsStock in UBCs
CompatibilityCompatibility
Lipid emulsion is a viable treatment option for critically ill overdose patients
_
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 18

Bryan D. Hayes, PharmD, DABAT, FAACTE‐mail: [email protected]: @PharmERToxGuy
ALiEM.com
2014 Midyear Clinical Meeting An Update on Uncommonly Used Antidotes
© 2014 American Society of Health-System Pharmacists 19