Population Status and Natural Localities of Rhodiola rosea ...

NON-PRESCRIPTION
THERAPIES FOR
IMPROVED HEALTH

Jeffrey P. Leake, M.D., D.A.B.A.,CPT
AMMEF Course Director

GENERAL PRINCIPLES Botanical or natural compounds that enhance biological function can be
valuable elements in an overall health promotion strategy
Many are herbs used for centuries in Chinese or Ayurvedic (longevity
knowledge) medicine
Many are biological compounds found naturally in humans (amino acids, co-
factors, vitamins and minerals
Rigorous clinical trials are often lacking.
Studies are often small and short in length of follow up
Most do not contain control groups

GENERAL PRINCIPLES
……..there would be general agreement to the effect that nutrition is important,
despite the fact that the still growing number of failed trials of individual nutrients
might suggest that no nutrient actually made much of a difference, a conclusion
that is absurd on its face and ought to have alerted us to the possibility that
there was something wrong with how we were investigating the matter. To
provide the proof needed to sustain revised intake recommendations, we shall
have to find a design better suited to nutrients than the randomized controlled
trial as currently implemented, and we need to develop a series of global
indices, nutrient by nutrient, which better capture the polyvalent nature of most
nutrients
Nutrients, Endpoints, and the Problem of Proof
Robert P. Heaney*
J. Nutr. September 1, 2008 vol. 138 no. 9 1591-1595

GENERAL PRINCIPLES
Nutrients and other bioactive food components are not drugs, and several
distinguishing characteristics are overlooked in the design and/or interpretation
of nutrition research. Unlike drugs, nutrients work in complex networks, are
homeostatically controlled, and cannot be contrasted to a true placebo group.
The beneficial effects of nutrients are small and can take decades to manifest.
A Commentary on the Nutrient-Chronic Disease Relationship and the New
Paradigm of Evidence-Based Nutrition
Natural Medicine Journal 12/1/2010
Andrew Shao, PhD, and Douglas Mackay, ND

Comparison between the Daily Values (DV) and the Dietary Reference Intakes (RDA or AI) for Adults
Micronutrient DV RDA or AI for Adult
Males (amount/day) RDA or AI for Adult
Females (amount/day)
Biotin 300 mcg 30 mcg 30 mcg
Folate 400 mcg 400 mcga 400 mcga
Niacin 20 mg 16 mgb 14 mgb
Pantothenic Acid 10 mg 5 mg 5 mg Riboflavin 1.7 mg 1.3 mg 1.1 mg Thiamin 1.5 mg 1.2 mg 1.1 mg
Vitamin A 5,000 IU 3,000 IUc 2,333 IUc
Vitamin B6 2 mg 1.3-1.7 mg 1.3-1.5 mg
Vitamin B12 6 mcg 2.4 mcgd 2.4 mcgd
Vitamin C 60 mg 90 mg 75 mg Vitamin D 400 IU 600-800 IU 600-800 IU
Vitamin E 30 IU 22.5-33 IUe 22.5-33 IUe
Vitamin K 80 mcg 120 mcg 90 mcg
Calcium 1,000 mg 1,000-1,200 mg 1,000-1,200 mg Chloride 3,400 mg 1,800-2,300 mg 1,800-2,300 mg Chromium 120 mcg 30-35 mcg 20-25 mcg Copper 2 mg 900 mcg 900 mcg Iodine 150 mcg 150 mcg 150 mcg Iron 18 mg 8 mg 8-18 mg Magnesium 400 mg 400-420 mg 310-320 mg Manganese 2 mg 2.3 mg 1.8 mg Molybdenum 75 mcg 45 mcg 45 mcg Phosphorus 1,000 mg 700 mg 700 mg Potassium 3,500 mg 4,700 mg 4,700 mg Selenium 70 mcg 55 mcg 55 mcg Zinc 15 mg 11 mg 8 mg Cholinef None established 550 mg 425 mg

GENERAL PRINCIPLES
Standardization of purity and potency among over the counter products is highly
variable
Drug interactions and side effects are often underappreciated
Toxicity possible
IT IS IMPERATIVE THAT NUTRITIONAL SUPPLEMENTS BE
SOURCED ONLY FROM HIGH QUALITY, RELIABLE
MANUFACTURERS

General Categories
1. Vitamins & Minerals
2. Cardiovascular
3. Anti Inflammatories/Antioxidants
4. Adrenal Adaptogens
5. Energy Enhancers
6. Hormone Modulators
7. Glycemic Agents/Insulin Sensitizers
8. Liver Support
9. Fat Oxidization Enhancers

Adrenal Adaptogens
1. Rhodiola Rosea 2. Ashwagandha 3. Licorice Root 4. DHEA 5. Phoshatidylserine

Fat Oxidation Enhancers
1. Green Tea
2. Carnitine
3. Conjugated Linoleic Acid

Anti Inflammatories &Anti-oxidants
1. N-Acetylcysteine
2. Carnitine
3. Tumeric/Curcumin
4. Marine Fish Oil
5. Co Enzyme Q 10
6. Alpha Lipoic Acid
7. Grape Seed
8. Boswellia

Liver Support
1. Milk Thistle
2. Alpha Lipoic Acid

Hormone Modulators
1. Di-Indolymethane
2. Sal Palmetto
3. Phoshatidylserine

Cardiovascular
1. Marine Fish Oil
2. Co Enzyme Q 10
3. Magnesium
4. B vitamins
5. Alpha Lipoic Acid
6. Grape Seed
7. L-Arginine
Energy Enhancers
1. Co-Enzyme Q-10
2. PQQ
3. Rhodiola Rosea
4. Ashwagandha
5. Green Tea

Glycemic Agents/Insulin Sensitizers
1. Vitamin D
2. Folic Acid
3. Cinnamon

ADRENAL FUNCTION & SUPPORT
Symptoms of Hypoadrenalism include:
1. Fatigue
2. Weakness
3. Anorexia
4. Nausea
5. Vomiting
6. Weight Loss
7. Salt Craving
8. Hypotension (Orthostatic)
9. Hypoglycemia
10. Skin Hyperpigmentation
11. Loss Of Body Hair
12. Poor Tolerance To Stress

ADRENAL FUNCTION & SUPPORT
Mild Hypoadrenalism can be diagnosed by the Cortosyn or ATCH Stimulation Test
Measure Serum A.M. Cortisol level. If low or low normal and symptomatic, then
administer 25 Units Cortosyn I.M.
Failure to double Cortisol level in 30 minutes is positive for mild Hypoadrenalism
No compelling evidence exists that Salivary Cortisol Levels can assess Adrenal
function accurately
24 hour urinary cortisol levels can fluctuate 64% depending on hydration
(probably effects salivary levels, too)
Do not administer L tryptophan to hypoadrenal patients – increases toxicity

ADRENAL FUNCTION & SUPPORT
CORTISOL THERAPY; Administer Cortef 5 mgs QID before meals and at bedtime ( with milk or antacid) DHEA THERAPY: Patients with Hypoadrenalism may have low DHEA (particularly women)
ADRENAL SUPPORT: Various vitamins, minerals and adrenal adaptogenic herbs can be used to support adrenal function in lieu of Cortef Glycrrhiza glabra (licorice root), Vitamin C, Pantothenic Acid (B5), Rhodiola Rosea, Ashwaghanda, Phosphotidylserine, Selenium
SAFE USES OF CORTISOL William Jeffries

Rhodiola Rosea
Native to eastern Siberia, Rhodiola Rosea has been used in Russian traditional
medicine for centuries, as it is known for its adaptogenic activity (increases the
body’s resistance to stress and aids mental function).
Rhodiola’s adaptogenic activity relieves mental stress. 44
The extract can prevent behavioral and physiological changes that are often associated
with chronic stress.45
A single dose of rhodiola has been shown to stimulate the central nervous system to
balance mood and behavior.29
One study observed the effects of rhodiola extract on 56 healthy physicians that were
suffering from fatigue during night shifts. After two weeks of rhodiola supplementation, the
study found a significant improvement in energy levels among individuals taking the extract.
Researchers suggested rhodiola can decrease fatigue during stressful conditions.46
Another study recruited students to take rhodiola for 20 days during an examination period.
Results indicated students taking rhodiola had more physical and mental endurance, when
compared to the placebo group.47

Rhodiola Rosea
A six-week study recruited individuals with mood ailments to take rhodiola extract,
finding mood, sleep, and emotions improved in subjects taking rhodiola extract.48
Similarly, rhodiola may alleviate chronic anxiety, as a ten-week study demonstrated
it significantly reduced anxiety among individuals taking the extract.49
Furthermore, the stress-relieving effects have been extended to stress-related
cardiovascular ailments, as rhodiola can inhibit cardiovascular damage.50
44 Perfumi M, Mattioli L. Adaptogenic and central nervous system effects of single doses of 3% rosavin and 1% salidroside Rhodiola rosea L. extract in mice. Phytother Res. 2007; 21(1):
37-43. 45 Mattioli L, Funari C, Perfumi M. Effects of Rhodiola rosea L. extract on behavioural and physiological alterations induced by chronic mild stress in female rats. J Psychopharmacol. 2008
May 30. 46 Darbinyan V, Kteyan A, Panossian A, Gabrielian E, Wikman G, Wagner H. Rhodiola rosea in stress induced fatigue-a double blind cross-over study of a standardized extract SHR-5
with a repeated low-dose regimen on the mental performance of healthy physicians during night duty. Phytomedicine. 2000; 7(5): 365-371. 47 Spasov AA, Wikman GK, Mandrikov VB, et al. A double-blind, placebo-controlled pilot study of the stimulating and adaptogenic effect of Rhodiola rosea SHR-5 extract on the fatigue of
students caused by stress during an examination period with a repeated low-dose regimen.
Phytomedicine. 2000; 7(2): 85-89. 48 Darbinyan V, Aslanyan G, Amroyan E, Gabrielyan E, et al. Clinical trial of Rhodiola rosea L. extract SHR-5 in the treatment of mild to moderate depression. Nord J Psychiatry. 2007;
61(5): 343-348. 49 Bystritsky A, Kerwin L, Feusner JD. A pilot study of Rhodiola rosea (Rhodax) for generalized anxiety disorder (GAD). J Altern Complement Med. 2008; 14(2): 175-180. 50 Maslova LV, Kondrat’ev B, Maslov LN, Lishmanov I. The cardioprotective and antiadrenergic activity of an extract of Rhodiola rosea in stress. Eksp Klin Farmakol. 1994; 57(6): 61-63.

Ashwagandha
Commonly used in Ayurvedic medicine to strengthen physical and mental stamina
Ashwagandha is a nightshade plant native to India, Bangladesh, and Sri Lanka.4
Can significantly improve antioxidant activity to lessen the formation of oxidative stress in the body.5
One study suggested ashwagandha had neuroprotective effects, as it produced a significant reduction in
the proliferation of degenerating cells.6
Can enhance cognition and memory that may be suppressed during stress, by aiding acetylcholine
neurotransmitter function.7
Ashwagandha’s adaptogenic activity can aid the stress response. A three-month study recruited 17
participants to take ashwagandha to see how the herb affected their ability to cope with stress.
Researchers found that ashwagandha significantly improved subjects’ stress response, without adverse
effects on the liver or kidneys.8
4 Kulkarni SK, Dhir A. Withania somnifera: An Indian ginseng. Prog Neurophyscho Biol Psych. 2008; 32(5):1093-1105. 5 Sankar SR, Manivasagam T, Krishnamurti A, Ramanathan M. The neuroprotective effect of Withania somnifera root extract in MPTP-intoxicated mice: an analysis of behavioral and
biochemical variables. Cell Mol Biol Lett. 2007; 12(4):473-481. 6 Jain S, Shukla SD, Sharma K, Bhatnagar M. Neuroprotective effects of Withania somnifera Dunn in hippocampal sub-regions of female albino rat. Phytother Res. 2001; 15(6): 544-548.
7 Schliebs R, Liebmann A, Bhattacharya SK, Kumar A, et al. Systemic administration of defined extracts from Withania somnifera (Indian Ginseng) and Shilajit differentially affects
cholinergic but not glutamatergic and GABAergic markers in rat brain. Neurochem Int. 1997; 30(2):181-190. 8 Seely D, Singh R. Adaptogenic potential of a polyherbal natural health product: Report on a longitudinal clinical trial. Evid Based Complement Alternat Med. 2007; 4(3):375-380.

Glycyrrhiza glabra/Licorice root
Potentiates the effects of glucocorticoids and mineralocorticoids by slowing
their rate of catabolism
Adverse effects include hypotension and hypokalemia
Increase intake of fruits and vegetables when administering
Do not use with patients taking glucocorticoids or mineralocorticoids
Large doses may lower DHEA and Testosterone
Effects are cumulative with continued use
Dose is 2 to 6 drops of a 1:1 or 1:2 tincture BID
Nutritional Medicine Alan R. Gaby page 1119

Phoshatidylserine
Phosphatidylserine (PS) is a naturally occurring phospholipid nutrient that is most
concentrated in organs with high metabolic activity, such as the brain, lungs, heart, liver,
and skeletal muscle.
PS is located mainly in the internal layer of the cell membrane and has a variety of unique
regulatory and structural functions.
PS modulates the activity of receptors, ion channels, enzymes and signaling molecules
and is involved in governing membrane fluidity [1]. T
Traditionally, PS supplements were derived from bovine cortex (BC-PS); however, due to
the potential transfer of infectious diseases, soy-derived PS (S-PS) has been established
as a safe alternative [2].
PS has been shown to improve a variety of brain functions that tend to decline with age [3].
In recent studies, PS has been shown to enhance mood in a cohort of young people during
mental stress [4] and to improve accuracy during tee-off by increasing the golfer's stress
resistance [5].

Phosphatidylserine
1. Pepeu G, Pepeu IM, Amaducci L: A review of phosphatidylserine pharmacological and clinical effects. Is
phosphatidylserine a drug for the ageing brain? Pharmacol Res 1996, 33:73-80.
2. Jorissen BL, Brouns F, van Boxtel MP, Riedel WJ: Safety of soy-derived phosphatidylserine in elderly people. Nutr
Neurosci 2002, 5:337-343.
3. Crook TH, Tinklenberg J, Yesavage J, Petrie W, Nunzi MG, Massari DC: Effects of Phosphatidylserine in age-
associated memory impairment.
Neurol 1991, 41(5):644-649.
4. Benton D, Donohoe RT, Sillance B, Nabb S: The Influence of phosphatidylserine supplementation on mood and heart
rate when faced with an acute stressor.
Nutr Neurosci 2001, 4(3):169-178
5. Jäger R, Purpura M, Geiss K-R, Weiß M, Baumeister J, Amatulli F, Schröder L, Herwegen H: The effect of
phosphatidylserine on golf performance.
J Int Soc Sports Nutr 2007, 4:23. PubMed Abstract | BioMed Central

The effects of phosphatidylserine on endocrine response to moderate
intensity exercise
Michael A Starks1, Stacy L Starks1, Michael Kingsley2, Martin Purpura3 and Ralf Jäger3*
Background Previous research has indicated that phosphatidylserine (PS) supplementation has the potential to attenuate
the serum cortisol response to acute exercise stress. Equivocal findings suggest that this effect might be dose dependent.
This study aimed to examine the influence of short-term supplementation with a moderate dose of PS (600 mg per day) on
plasma concentrations of cortisol, lactate, growth hormone and testosterone before, during, and following moderate intensity
exercise in healthy males.
Methods 10 healthy male subjects participated in the study. Each subject was assigned to ingest 600 mg PS or placebo per
day for 10 days using a double-blind, placebo-controlled, crossover design. Serial venous blood samples were taken at rest,
after a 15 minute moderate intensity exercise protocol on a cycle ergometer that consisted of five 3-minute incremental
stages beginning at 65% and ending at 85% VO2 max, and during a 65 minute passive recovery. Plasma samples were
assessed for cortisol, growth hormone, testosterone, lactate and testosterone to cortisol ratio for treatment (PS or placebo).
Results Mean peak cortisol concentrations and area under the curve (AUC) were lower following PS (39 ± 1% and 35 ± 0%,
respectively) when compared to placebo (p < 0.05). PS increased AUC for testosterone to cortisol ratio (184 ± 5%) when
compared to placebo (p < 0.05). PS and placebo supplementation had no effect on lactate or growth hormone levels.
Conclusion The findings suggest that PS is an effective supplement for combating exercise-induced stress and preventing
the physiological deterioration that can accompany too much exercise. PS supplementation promotes a desired hormonal
status for athletes by blunting increases in cortisol levels.
Journal of the International Society of Sports Nutrition 2008, 5:11

S-PS significantly decreased cortisol (35 ± 0%, p < 0.01) and increased
testosterone (37 ± 5%, p = 0.02) AUC levels and testosterone to cortisol ratio
(184 ± 5%, p = 0.02) in comparison to placebo.
The results of this study suggest that 600 mg/d of S-PS might have the potential to
avert an overtrained state
Starks et al. Journal of the International Society of Sports Nutrition 2008 5:11 2783-5

Cortisol, testosterone, lactate and growth hormone response to exercise
after 10 days of oral treatment with 600 mg S-PS or placebo (pre-exercise
phase -30 to 0 minutes, exercise phase: 0 to 15 minutes, recovery phase 16
to 80 minutes).
Starks et al. Journal of the International Society of Sports Nutrition 2008 5:11 2783-5

5-HYDROXYTRYPTOPHAN/5-HTP
5-HTP is a natural compound that comes from the seeds of Griffonia simplicifolia,
trees mainly found in West Africa
As an intermediate L-tryptophan metabolite, 5-HTP easily bypasses the blood-
brain barrier and is highly effective in entering the blood stream for available use
(70% of oral 5-HTP enters the blood stream).1
Mood Balance
Low serotonin levels are significantly related to a low, sad mood.
5-HTP stimulates the production of serotonin in the brain to enhance mood. 3,4,5
When 5-HTP was compared with the administration fluvoxamine, (36 subjects
over six weeks) both treatment groups had similar results with a 50%
improvement in mood;2

5-HYDROXYTRYPTOPHAN/5-HTP
Sleep Disturbances
A study conducted by the University of Rome found 5-HTP reduced night terrors in
children.
Forty-five children participated in the study finding 93.5% of the treatment group
had a reduced amount of night terrors after one-month in the treatment group,
while 83.9% were night terror-free after six-months of treatment.6

5-HYDROXYTRYPTOPHAN/5-HTP
Chronic tension headaches
In a double-blind study recruited 65 patients with headaches finding subjects that
took 5-HTP supplementation used less pain relievers and had a reduction in the
number of headaches after two weeks of treatment, in comparison to the placebo
group.7
Compared 5-HTP to Propranolol, 39 patients in a double-blind trial and found a
significant reduction in headaches among both the 5-HTP and Propranolol groups
over a four-month period suggesting 5-HTP is a safe alternative to other
therapies.8
5-HYDROXYTRYPTOPHAN/5-HTP
Weight Management
5-HTP is an effective source for appetite control.9
One study found an increase in serotonin levels reduced carbohydrate cravings
and curbed the appetite of 20 obese patients participating in a six-week, double-
blind study.10
Patients with blood sugar problems usually have low brain serotonin levels.
A two-week, double-blind study of 20 overweight subjects with insulin resistance
found oral 5-HTP normalized eating behaviors and reduced excessive energy
intake.11
5-HTP can reduce excessive food consumption that can be generated by
anxiety.12

5-HYDROXYTRYPTOPHAN/5-HTP
Dosage:
Up to 300 mg in three divided doses per day. Do not exceed 900 mg per day.
As part of weight loss programs, it is recommended that 5-HTP be taken 20
minutes before each meal, to act as a natural appetite suppressant and reduce
the craving for carbohydrates. Start at 100 mg three times per day. If after four
weeks the desired results are not achieved, increase the dosage to 200 mg three
times per day

5-HYDROXYTRYPTOPHAN/5-HTP 1 Birdsall, TC. 5-hydroxytryptophan: a clinically- effective serotonin precursor. Altern Med Rev. 1998; 3:271-280.
2 Poldinger, W, Calanchini, B, Schwarz ,W. A functional-dimensional approach to depression: serotonin deficiency as a target syndrome in a
comparison of 5-hydroxytryptophan and fluvoxamine. Psychopathology. 1991;24:53-81.
3 Van Praag, HM, Korf, J, Dols, LC, Schut, T. A pilot study of the predictive value of the probenecid test in application of 5-hydroxytryptophan as
antidepressant. Psychopharmacologia. 1972;25:14-21.
4 Van Praag HM. Central monamine metabolism in depression. II. Comp Psychiat. 1980; 21:44-54.
5 Van Praag HM. Management of depression with serotonin precursors. Biol Psychiatry. 1981;16:291-310.
6 Bruni, O, Ferri, R, Miano, S, Verillo, E. L -5-Hydroxytryptophan treatment of sleep terrors in children. Eur J Pediatr. 2004; 163(7):402-407.
7 Ribeiro, CA. L- 5-hydroxytryptophan in the prophylaxis of chronic tension-type headache : A double-blind, randomized, placebo-controlled study. For
the Portugese Head Study. Headache, 2000; 40:451-456.
8 Maissen CP, et al. Comparison of the effect of 5-hydroxytryptophan and propranolol in the interval treatment of migraine. Schweiz Med Wochenschr.
1991; 121:1585-1590.
9 Halford, JC, Harraold, JA, Boyland, EJ, Lawton, CL, Blundell, JE. Serotonergic drugs: Effects on appetite expression and use for the treatment of
obesity. Drugs. 2007; 67(1):27-55.
10 Cangiano, C, Ceci, F, Cascino, A, et al. Eating behavior and adherence to dietary prescriptions in obese adult subjects treated with 5-
hydroxytryptophan. Am J Clin Nutr. 1992 Nov; 56(5):863-867.
11 Cangiano, C, Laviano, A, Del Ben, M, et al. Effects of oral 5-hydroxy-tryptophan on energy intake and macronutrient selection in non-insulin
dependent diabetic patients. Int J Obes Relat Metab Disord. 1998 Jul; 22(7):648-654.
12 Amer, A, Breu, J, McDermott, J, et al. 5-Hydroxy-L-tryptophan suppresses food intake in food-deprived and stressed rats. Pharm Biochem and
Behavior. 2004 Jan; 77(1):137-143.

N-ACETYLCYSTEINE
Derivative of amino acid cysteine – more stable than cysteine (which oxidizes to
inactive cystine)
Readily absorbed and most converted to cysteine
Cysteine is a precursor to the antioxidant glutathione (cysteine availability is often
the rate limiting step)
In contrast to glutathione (which can enter the cell) supplementation, NAC can
enter the cell and then be converted to glutathione
It is also a free radical scavenger in it’s own right
It contains a free sulfhydryl group that can cleave disulfide bonds (which may
lower homocysteine levels)
Dose range is 600 mgs to 1200 mgs per day

Carnitine
Carnitine is a quaternary amine that facilitates transport of fatty acids into
mitochondria
Has demonstrated antioxidant functions and supports immune function
Carnitine deficiency may result in fatigue, muscle weakness, lipid accumulation in
muscle, fatty liver and hypoglycemia
Only the L-isomer is active
Is synthesized in the liver, kidney and brain from lysine and required Vitamin C,
methionine, Fe++, and B6 and niacin
Well tolerated with mild GI symptoms the major side effect – may cause an
unpleasant body odor
Statins may reduce levels
Dose is typically 1 – 2 grams per day

An Acute Increase in Skeletal Muscle Carnitine Content Alters Fuel
Metabolism in Resting Human Skeletal Muscle
Francis B. Stephens, Dumitru Constantin-Teodosiu, David Laithwaite, Elizabeth J. Simpson, and Paul L. Greenhaff
Context: Carnitine plays an essential role in the integration of fat and carbohydrate oxidation in skeletal muscle, which is
impaired in obesity and type 2 diabetes.
Objective: The aim of the present study was to investigate the effect of an increase in skeletal muscle total carnitine (TC)
content on muscle fuel metabolism
Design: A 5-h iv infusion of saline (control) or L-carnitine was administered while serum insulin was maintained at a
physiologically high concentration during two randomized visits.
Participants: Seven healthy, nonvegetarian young men (body mass index, 26.1 1.6 kg/m2) participated in the present study
at the University of Nottingham.
Main Outcome Measures: Skeletal muscle pyruvate dehydrogenase complex (PDC) activity and associated muscle
metabolites were measured.
Results: The combination of hypercarnitinemia (600 mol/liter) and hyperinsulinemia (160 mU/liter) increased muscle TC
content by 15% (P 0.01) and was associated with decreased pyruvate dehydrogenase complex activity (P0.05) and muscle
lactate content (P0.05) by 30 and 40%, respectively, and an overnight increase in muscle glycogen (P0.01) and long-chain
acyl-coenzymeAcontent (P0.05) by 30 and 40%, respectively, compared with control.
Conclusions: These results suggest that an acute increase in human skeletal muscle TC content results in an inhibition of
carbohydrate oxidation in conditions of high carbohydrate availability, possibly due to a carnitine-mediated increase in fat
oxidation. These novel findings may have important implications for our understanding of the regulation of muscle fat
oxidation, particularly during exercise, when carnitine availability may limit fat oxidation, and in obesity and type 2 diabetes
where it is known to be impaired.
(J Clin Endocrinol Metab 91: 5013–5018, 2006)

EFFECTS OF A COMBINATION OF BETA CAROTENE AND VITAMIN A ON
LUNG CANCER AND CARDIOVASCULAR DISEASE
GILBERT S. OMENN , M.D., PH.D., GARY E. GOODMAN , M.D., M.S., MARK D. THORNQUIST , PH.D., JOHN BALMES
, M.D., MARK R. CULLEN, M.D., ANDREW GLASS , M.D., JAMES P. KEOGH , M.D., FRANK L. MEYSKENS, JR., M.D.,
BARBARA VALANIS , DR.P.H., JAMES NH. WILLIAMS, JR., M.D., SCOTT BARNHART , M.D., M.P.H., AND SAMUEL
HAMMAR , M.D.
Background. Lung cancer and cardiovascular disease are major causes of death in the United States. It has been proposed
that carotenoids and retinoids are agents that may prevent these disorders.
Methods. We conducted a multicenter, randomized, double-blind, placebo-controlled primary prevention trial — the Beta-
Carotene and Retinol Efficacy Trial — involving a total of 18,314 smokers, former smokers, and workers exposed to
asbestos. The effects of a combination of 30 mg of beta carotene per day and 25,000 IU of retinol (vitamin A) in the form of
retinyl palmitate per day on the primary end point, the incidence of lung cancer, were compared with those of placebo.
Results. A total of 388 new cases of lung cancer were diagnosed during the 73,135 person-years of followup (mean length
of follow-up, 4.0 years). The active-treatment group had a relative risk of lung cancer of 1.28 (95 percent confidence
interval, 1.04 to 1.57; P 0.02), as compared with the placebo group. There were no statisticallysignificant differences in the
risks of other types of cancer. In the active-treatment group, the relative risk of death from any cause was 1.17 (95 percent
confidence interval, 1.03 to 1.33); of death from lung cancer, 1.46 (95 percent confidence interval, 1.07 to 2.00); and of
death from cardiovascular disease, 1.26 (95 percent confidence interval, 0.99 to 1.61). On the basis of these findings, the
randomized trial was stopped 21 months earlier than planned; follow-up will continue for another 5 years.
Conclusions. After an average of four years of supplementation, the combination of beta carotene and vitamin
A had no benefit and may have had an adverse effect on the incidence of lung cancer and on the risk of death from
lung cancer, cardiovascular disease, and any cause in smokers and workers exposed to asbestos.
(N Engl J Med 1996;334:1150-5.)

Ferritin Concentrations, Metabolic Syndrome, and Type 2 Diabetes in Middle-
Aged and Elderly Chinese
Liang Sun, Oscar H. Franco, Frank B. Hu, Lu Cai, Zhijie Yu, Huaixing Li, Xingwang Ye, Qibin Qi,
Jing Wang, An Pan, Yong Liu, and Xu Lin Key
Context: Elevated ferritin concentrations frequently cluster with well-established risk factors of diabetes including obesity,
metabolic syndrome, chronic inflammation, and altered circulating adipokines. Few studies, however, have systematically
evaluated the effect of these risk factors on ferritin-diabetes association, particularly in Chinese populations.
Objective: We aimed to investigate, in a middle-aged and elderly Chinese population, whether elevated ferritin
concentrations are associated with higher risk of metabolicsyndromeandtype2diabetes and to what extent the associations
were influenced by obesity, inflammation, and adipokines.
Design and Methods: We conducted a population-based, cross-sectional survey of 3289 participants aged 50–70 yr in
Beijing and Shanghai in 2005. Fasting plasma ferritin, glucose, insulin, lipid profile, glycohemoglobin, inflammatory markers,
adipokines, and dietary profile were measured.
Results: Median ferritin concentrations were 155.7 ng/ml for men and 111.9 ng/ml for women. After multiple adjustment, the
odds ratios (ORs) were substantially higher for type 2 diabetes (OR 3.26, 95% confidence interval 2.36–4.51) and metabolic
syndrome OR 2.80 (95% confidence interval 2.24–3.49) in the highest ferritin quartile compared with those in the lowest
quartile. These associations remained significant after further adjustment for dietary factors, body mass index, inflammatory
markers, and adipokines.
Conclusions: Elevated circulating ferritin concentrations were associated with higher risk of type 2 diabetes and metabolic
syndrome in middle-aged and elderly Chinese independent of obesity, inflammation, adipokines, and other risk factors. Our
data support the crucial role of iron overload for metabolic diseases, even in a country with relatively high prevalence of iron
deficiency.
(J Clin Endocrinol Metab 93: 4690–4696, 2008)

Vitamin D
Recently, several epidemiological studies have reported increasing prevalence of
alarming rates of low serum 25-OH vitamin D levels among seemingly healthy
populations, especially in the elderly in the Western industrialized world.
Vitamin D receptors are ubiquitous, being found on several tissues including, gut,
adipose tissues, cardiac and skeletal muscles
Both cross-sectional and prospective studies point out that vitamin D insufficiency
(20–29 ng/ml) and deficiency (less than 20 ng/ml) have direct and indirect effects
on insulin secretion and insulin action. In this regard, vitamin D has been directly
linked to the development of type 2 diabetes and type 1 diabetes, but the
mechanism(s) remains controversial (1)
A large cross-sectional study that both low serum 25-OH vitamin D and 1,25-
hydroxy vitamin D were associated with higher prevalence of myocardial
dysfunction, deaths due to heart failure, and sudden cardiac death. (2)
(1) Alvarez JA, Ashraf A 2010 Role of vitamin D in insulin secretion andinsulin sensitivity for glucose homeostasis. Int J Endocrinol 2010: 351385 (2) Pilz S, Ma¨ rz W, Wellnitz B, Seelhorst U, Fahrleitner-Pammer A, Dimai HP, Boehm BO, Dobnig H 2008 Association of vitamin D deficiency with heart failure and sudden cardiac death in a large crosssectional study of patients referred for coronary angiography. J Clin Endocrinol Metab 93:3927–3935

Vitamin D
Vitamin D supplementation improves cytokine profiles in patients with
congestive heart failure in a double-blind, randomized, placebo-controlled trial.
In their study, IL-10 was higher after vitamin D supplementation, whereas TNF-
alpha was not changed. The authors concluded that vitamin D reduces the
inflammatory milieu in congestive heart failure patients and suggested that the
vitamin D–PTH axis may be involved in the progression of congestive heart
failure.
A cross sectional and prospective study reported that in individuals with vitamin
D deficiency (15 ng/ml) have a 62%increase in the first incidence of a
cardiovascular disease event, especially in patients with hypertension.
1)Schleithoff SS, Zittermann A, Tenderich G, Berthold HK, Stehle P, Koerfer R 2006 Vitamin D supplementation improves cytokine profiles
in patients with congestive heart failure: a double-blind, randomized, placebo-controlled trial. Am J Clin Nutr 83:754–759
(2) Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin EJ, D’Agostino RB, Wolf M, Vasan RS 2008 Vitamin D
deficiency and risk of cardiovascular diseases. Circulation 117: 503–511

Systematic Review: Vitamin D and Cardiometabolic Outcomes
Anastassios G. Pittas, MD, MS; Mei Chung, MPH; Thomas Trikalinos, MD; Joanna Mitri, MD; Michael Brendel, BA; Kamal Patel, MPH;
Alice H. Lichtenstein, DSc; Joseph Lau, MD; and Ethan M. Balk, MD, MPH
Background: Vitamin D may modify risk for cardiometabolic outcomes (type 2 diabetes, hypertension, or cardiovascular
disease).
Purpose: To examine the association between vitamin D status, including the effect of vitamin D supplementation, and
cardio-metabolic outcomes in generally healthy adults.
Data Sources: English-language studies in MEDLINE (inception to 4 November 2009) and the Cochrane Central Register of
Controlled Trials (fourth quarter of 2009).
Study Selection: 11 reviewers screened citations to identify longitudinal cohort studies that reported associations between
vitamin D status and cardio-metabolic outcomes, including randomized trials of vitamin D supplementation.
Data Extraction: 5 independent reviewers extracted data about study conduct, participant characteristics, outcomes, and
quality. Differences were resolved by consensus.
Data Synthesis: 13 observational studies (14 cohorts) and 18 trials were eligible. Three of 6 analyses (from 4 different
cohorts) reported a lower incident diabetes risk in the highest versus the lowest vitamin D status groups. Eight trials found no
effect of vitamin D supplementation on glycemia or incident diabetes. In meta-analysis of 3 cohorts, lower 25-hydroxyvitamin
D concentration was associated with incident hypertension (relative risk, 1.8 [95% CI, 1.3 to 2.4]). In meta-analyses of 10
trials, supplementation non-significantly reduced systolic blood pressure (weighted mean difference, 1.9 mm Hg [CI, 4.2 to
0.4 mm Hg]) and did not affect diastolic blood pressure (weighted mean difference, 0.1 mm Hg [CI, 0.7 to 0.5 mm Hg]). Lower
25-hydroxyvitamin D concentration was associated with incident cardiovascular disease in 5 of 7 analyses (6 cohorts). Four
trials found no effect of supplementation on cardiovascular outcomes.
Limitations: Studies included primarily white participants. Observational studies were heterogeneous. Several trials reported
post hoc analyses.
Conclusion: The association between vitamin D status and cardiometabolic outcomes is uncertain. Trials showed no
clinically significant effect of vitamin D supplementation at the dosages given. Ann Intern Med. 2010;152:307-314.

Vitamin D and Cardiovascular Outcomes: A Systematic Review and
Meta-Analysis
Mohamed B. Elamin, Nisrin O. Abu Elnour, Khalid B. Elamin, Mitra M. Fatourechi, Aziz A. Alkatib, Jaime P. Almandoz, Hau Liu, Melanie A. Lane,
Rebecca J. Mullan, Ahmad Hazem, Patricia J. Erwin, Donald D. Hensrud, Mohammad Hassan Murad, and Victor M. Montori
Context: Several studies found association between vitamin D levels and hypertension, coronary
artery calcification, and heart disease.
Objective: The aim of this study was to summarize the evidence on the effect of vitamin D on
cardiovascular outcomes.
Design and Methods: We searched electronic databases from inception through August 2010 for
randomized trials. Reviewers working in duplicate and independently extracted study characteristics,
quality, and the outcomes of interest. Random-effects meta-analysis was used to pool the relative risks
(RR) and the weighted mean differences across trials.
Results: We found 51 eligible trials with moderate quality. Vitamin D was associated with nonsignificant
effects on the patient-important outcomes of death [RR, 0.96; 95% confidence interval (CI), 0.93, 1.00; P
0.08], myocardial infarction (RR, 1.02; 95% CI, 0.93, 1.13; P 0.64), and stroke
(RR, 1.05;95%CI, 0.88, 1.25; P0.59). These analyses were associated with minimal heterogeneity. There
were no significant changes in the surrogate outcomes of lipid fractions, glucose, or diastolic or systolic
blood pressure. The latter analyses were associated with significant heterogeneity, and the pooled
estimates were trivial in absolute terms.
Conclusions: Trial data available to date are unable to demonstrate a statistically significant
reduction in mortality and cardiovascular risk associated with vitamin D. The quality of the
available evidence is low to moderate at best.
(J Clin Endocrinol Metab 96: 0000–0000, 2011)

Circulating 25-Hydroxyvitamin D Levels and Frailty Status in Older Women
Kristine E. Ensrud, Susan K. Ewing, Lisa Fredman, Marc C. Hochberg, Jane A. Cauley, Teresa A. Hillier, Steven R. Cummings, Kristine Yaffe, and
Peggy M. Cawthon
Context: Vitamin D deficiency and frailty are common with aging, but the association between these conditions is uncertain.
Objective: To determine the association between 25-hydroxyvitamin D (25(OH)D) levels and prevalent and incident frailty
status among older women.
Design: Cross-sectional and longitudinal analyses of a prospective cohort study.
Participants: 6307 women aged 69 years.
Main Outcome Measures: Frailty status classified as robust, intermediate stage, or frail at baseline;and robust,
intermediate stage, frail, or dead (all-cause mortality) at follow-up an average of 4.5 years later.
Results: At baseline, there was a U-shaped association between 25(OH)D level and odds of frailty with the lowest risk
among women with levels 20.0–29.9 ng/ml (referent group). Compared with this group, the odds of frailty were higher
among those with levels15.0 ng/ml [multivariable odds
ratio (MOR) 1.47, 95% confidence interval (CI), 1.19–1.82], those with levels 15.0–19.9 ng/ml (MOR 1.24, 95% CI 0.99–
1.54), and those with levels 30 ng/ml (MOR 1.32, 95% CI 1.06–1.63). Among 4551 nonfrail women at baseline, the odds of
frailty/death (vs. robust/intermediate) at follow-up
appeared higher among those with levels 15.0–19.9 ng/ml (MOR 1.21, 95% CI 0.99–1.49), but the CI overlapped 1.0. The
odds of death (vs. robust/intermediate/frail at follow-up) was higher among those with levels15.0 ng/ml (MOR 1.40, 95% CI
1.04–1.88) and those with levels 15.0–19.9 ng/ml (MOR 1.30, 95% CI 0.97–1.75), although the latter association did not
quite reach significance.
Conclusion: Lower (20 ng/ml) and higher (30 ng/ml) levels of 25(OH)D among older women were moderately associated
with a higher odds of frailty at baseline. Among non-frail women at baseline, lower levels (20 ng/ml) were modestly
associated with an increased risk of incidentfrailty or death at follow-up.
(J Clin Endocrinol Metab 95: 5266–5273, 2010)
REVIEW: The Role of Vitamin D and Calcium in Type 2 Diabetes. A
Systematic Review and Meta-Analysis
Anastassios G. Pittas, Joseph Lau, Frank B. Hu, and Bess Dawson-Hughes
Context: Altered vitamin D and calcium homeostasis may play a role in the development of type 2
diabetes mellitus (type 2 DM).
Evidence Acquisition and Analyses: MEDLINE review was conducted through January 2007 for
observational studies and clinical trials in adults with outcomes related to glucose homeostasis. When data
were available to combine, meta-analyses were performed, and summary odds ratios (OR) are presented.
Evidence Synthesis: Observational studies show a relatively consistent association between low vitamin
D status, calcium or dairy intake, and prevalent type 2 DM or metabolic syndrome [OR (95% confidence
interval): type 2 DM prevalence, 0.36 (0.16–0.80) among nonblacks for highest vs. lowest 25-
hydroxyvitamin D; metabolic syndrome prevalence, 0.71 (0.57– 0.89) for highest vs. lowest dairy intake].
There are also inverse associations with incident type 2 DM or metabolic syndrome [OR (95% confidence
interval): type 2 DM incidence, 0.82 (0.72– 0.93) for highest vs. lowest combined vitamin D and calcium
intake; 0.86 (0.79–0.93) for highest vs. lowest dairy intake]. Evidence from trials with vitamin D and/or
calcium supplementation suggests that combined vitamin D and calcium supplementation may have a role
in the prevention of type 2 DM only in populations at high risk (i.e. glucose intolerance). The available
evidence is limited because most observational studies are cross-sectional and did not adjust for important
confounders, whereas intervention studies were short in duration, included few subjects, used a variety of
formulations of vitamin D and calcium, or did post hoc analyses.
Conclusions: Vitamin D and calcium insufficiency may negatively influence glycemia, whereas
combined supplementation with both nutrients may be beneficial in optimizing glucose
metabolism. (J ClinEndocrinol Metab 92: 2017–2029, 2007)

Conclusions
Vitamin D
The last year in clinical vitamin D research has confirmed the presence of a worldwide problem with vitamin D depletion, a
problem that appears to be worsening. Large-scale population studies bear out long-held concerns that low serum 25OHD
levels are associated with a number of adverse outcomes in the human musculoskeletal, innate immune, and cardiovascular
systems; in fact, low vitamin D levels are significantly associated with all-cause mortality in the U.S. population. It is
hypothesized that the rise in global obesity contributes to the worsening of the problem of vitamin D insufficiency/deficiency,
amplifying adverse impacts on the host skeleton, immuno-reactivity to microbes, and metabolic status. Because of its
frequency, its ease of detection, its associated adverse outcomes, and the straightforward, inexpensive and effective means
by which is can be treated, vitamin D insufficiency should be sought especially when evaluating and treating osteoporotic,
otherwise immuno-compromised, and obese subjects.
Finally, it should be remembered that treatment of vitamin D insufficiency/deficiency has two phases:
1) restoration of 25OHD levels to more than 30 ng/ml; and
2) 2) maintenance of the serum 25OHD in that range.
Adams and Hewison Update in Vitamin D J Clin Endocrinol Metab, February 2010, 95(2):471–478
OPTIMAL TARGET VIT D3 = 40 – 70 NGS/ML
Clinical Endocrinology
Volume 75, Issue 5, pages 575-584, 4 OCT 2011

Homocysteine
Homocysteine is a sulfur-containing amino acid generated during
metabolism of the essential amino acid methionine.
It is in turn metabolized by 1 of 2 pathways: through transsulfuration by the
vitamin B6–dependent cystathionine β-synthase in hepatic cells or via
remethylation to methionine in nonhepatic cells.
Hyperhomocysteinemia promotes inflammation by increasing expression of
vascular cell adhesion molecule 1 (VCAM1) and tumor necrosis factor-α and
increases oxidative modification of low-density lipoproteins, thereby
promoting uptake of low-density lipoprotein cholesterol by macrophages.
Mayo Clin Proc. • November 2008;83(11):1200-1202

Homocysteine
Homocysteine has been shown to activate platelets and promote expression of the CD40/CD40 ligand from activated platelets. The CD40/CD40 ligand engagement on the surface of endothelial cells, smooth muscle cells, or macrophages triggers an additional inflammatory response, characterized by the release of inflammatory cytokines (interleukins 1B, 6, 8, 12) and chemokines (chemokine [C-C motif] ligand 2 [CCL2]) as well as expression of adhesion molecules (E selectin, VCAM1, Pselectin).
Hyperhomocysteinemia also increases concentrations of procoagulant tissue factor and reduces antithrombin III activity. This, in addition to the findings of enhanced activation of metalloproteinases after increases in homocysteine, suggests a predisposition to plaque rupture and thrombosis.
Mayo Clin Proc. • November 2008;83(11):1200-1202

Homocysteine
Homocysteine is elevated in kidney disease, and renal dysfunction is a recognized
risk factor for CV disease.
The kidneys have an important role in homocysteine metabolism; as renal function
declines, homocysteine concentrations increase.
In a recent post hoc analysis of the Vitamins to Prevent Stroke (VITATOPS) trial,
adjustment for renal function eliminated the relationship between total
homocysteine and carotid intima medial thickness as well as flow-mediated
dilatation of the brachial artery.
These findings suggest that renal dysfunction may account for the
epidemiologic association between mild hyperhomocysteinemia and
increased CV risk and that lowering homocysteine levels with B vitamins
would not eliminate the relationship between renal function and CV risk.
Thus, mild hyperhomocysteinemia may be a risk marker, rather than a risk
factor
Mayo Clin Proc. • November 2008;83(11):1200-1202

Homocysteine
Elevated homocysteine levels are associated with an increased risk
of CV events, but B vitamins may not provide a preventive benefit in patients with
mild homocysteinemia
Studies must take into account renal function when evaluating the pathogenicity of
homocysteine, as well as therapies for reducing homocysteine levels other than B
vitamins (eg, novel future therapies, as well as various combinations of exercise
training, methionine restriction, and use of betaine-homocysteine
methyltransferase and N-acetylcysteine).

Homocysteine and folate as risk factors for dementia and Alzheimer Disease
Giovanni Ravaglia, Paola Forti, Fabiola Maioli, Mabel Martelli, Lucia Servadei, Nicoletta Brunetti, Elisa Porcellini, and Federico Licastro
Background: In cross-sectional studies, elevated plasma total homocysteine (tHcy) concentrations have been associated with cognitive impairment and dementia. Incidence studies of this issue are few and have produced conflicting results.
Objective: We investigated the relation between high plasma tHcy concentrations and risk of dementia and Alzheimer disease (AD) in an elderly population.
Design: A dementia-free cohort of 816 subjects (434 women and 382 men; mean age: 74 y) from an Italian population-based study constituted our study sample. The relation of baseline plasma tHcy to the risk of newly diagnosed dementia and AD on follow-up was examined. A proportional hazards regression model was used to adjust for age, sex, education, apolipoprotein E genotype, vascular risk factors, and serum concentrations of folate and vitamin B-12.
Results: Over an average follow-up of 4 y, dementia developed in 112 subjects, including 70 who received a diagnosis of AD. In the subjects with hyperhomocysteinemia (plasma tHcy 15 mol/L), the hazard ratio for dementia was 2.08 (95% CI: 1.31, 3.30; P 0.002). The corresponding hazard ratio for AD was 2.11 (95% CI: 1.19, 3.76; P 0.011). Independently of hyperhomocysteinemia and other confounders, low folate concentrations (11.8 nmol/L) were also associated with an increased risk of both dementia (1.87; 95% CI: 1.21, 2.89; P 0.005) and AD (1.98; 95% CI: 1.15, 3.40; P 0.014), whereas the association was not significant for vitamin B-12.
Conclusions: Elevated plasma tHcy concentrations and low serum folate concentrations are independent predictors of the development of dementia and AD.
Am J Clin Nutr 2005;82:636–43.

Homocysteine or Renal Impairment Which Is the Real Cardiovascular Risk
Factor?
Kathleen Potter, Graeme J. Hankey, Daniel J. Green, John W. Eikelboom, Leonard F. Arnolda
Objective—The purpose of this study was to determine whether adjustment for renal function eliminates
the relationship between total plasma homocysteine (tHcy) and vascular risk, assessed by carotid intima
medial thickness (CIMT) and flow-mediated dilation (FMD) of the brachial artery.
Methods and Results—We used cross-sectional data from 173 stroke patients treated with B-vitamins
(folic acid 2 mg, vitamin B6 25 mg, and vitamin B12 0.5 mg) or placebo in a randomized double-blinded
trial to test the relationships between posttreatment tHcy, cystatin C (a marker of glomerular filtration rate),
estimated glomerular filtration rate (eGFR, Modification of Diet in Renal Disease equation) creatinine,
CIMT, and FMD in stepwise and multivariable regression models. The strong linear relationship between
tHcy and cystatin C was not altered by long-term B-vitamin treatment. tHcy lost significance as a predictor
of the vascular measurements after adjustment for any single marker of renal function. Cystatin C, but not
tHcy, was a significant independent predictor of FMD after adjustment for age, sex, smoking, systolic blood
pressure, high-density lipoprotein cholesterol, and treatment group.
Conclusions—Adjusting for renal function eliminates the relationship between tHcy and CIMT and FMD,
supporting the hypothesis that elevated tHcy is a marker for renal impairment rather than an independent
cardiovascular risk factor.
(Arterioscler Thromb Vasc Biol. 2008;28:1158-1164)

L-Folic Acid Supplementation in Healthy Postmenopausal Women: Effect on
Homocysteine and Glycolipid Metabolism
Paola Villa, Concetta Perri, Rosanna Suriano, Francesco Cucinelli, Simona Panunzi, Micaela Ranieri, Cristina Mele, and Antonio Lanzone
Context: Hyperhomocysteinemia as well as alterations of glycemic and lipidic metabolism are recognized as risk factors for
cardiovascular diseases.
Objective: The aim of this study was to examine the effect of L-folic acid supplementation on homocysteine (Hcy) and
related thiols, such as cysteine (Cys) and Cys-glycine (Cys-Glyc) pathways and their relationship to glucose, insulin, and
lipidic metabolism in normoinsulinemic postmenopausal women.
Design: This study was a randomized placebo, not double-blind, trial.
Setting: The study was performed in an academic research center.
Patients or Other Participants: Twenty healthy postmenopausal women were selected. No patient was taking drugs
known to affect lipid or glucose metabolism.
Intervention(s): Patients underwent two hospitalizations before and after 8 wk of L-acid folic (7.5 mg/d) or placebo
administration. The glycemic metabolism was studied by an oral glucose tolerance test and a hyperinsulinemic euglycemic
clamp. Hcy metabolism was studied by a standardized oral methionine-loading test.
Main Outcome Measure(s): Hcy, Cys, and Cys-Glyc, basally and after a methionine loading test, were measured. Basal
insulin, glucose, and peptide C levels as well as area under the curve for insulin, area under the curve for peptide, hepatic
insulin extraction, and metabolic index were assayed. The total cholesterol, high-density lipoprotein (HDL) cholesterol, and
low-density lipoprotein (LDL) cholesterol levels and the cholesterol/HDL and LDL/HDL ratios were also measured.
Results: The total basal Hcy concentration and the plasma postmethionine loading Hcy values were significantly decreased
(P 0.01) in L-folic acid-treated patients, whereas postmethionine loading Cys- Glyc levels were markedly increased (P
0.02). Furthermore, L-folic acid intake induced a significant improvement in carbohydrate metabolism through an increase in
fractional hepatic insulin extraction (P 0.05) and peripheral insulin sensitivity (P 0.02) in normoinsulinemic women. HDL
levels considerably increased, inducing an improvement in other atherosclerotic indexes, such as cholesterol/ HDL and
LDL/HDL ratios (P 0.03).
Conclusions: These results show that folic acid supplementation lowers plasma Hcy levels and improves insulin and lipid
metabolism, reducing the risk of cardiovascular disease.
(J Clin Endocrinol Metab 90: 4622–4629, 2005)

The Prevalence of Vitamin B12 Deficiency in Patients with Type 2 Diabetes: A
Cross-Sectional Study
Matthew C. Pflipsen, MD, Robert C. Oh, MD, MPH, Aaron Saguil, MD, MPH,
Dean A. Seehusen, MD, MPH, FAAFP, and Richard Topolski, PhD
Purpose: The purpose of this study is to define the prevalence of vitamin B12 deficiency in a type 2 diabetic
population within a primary care practice. Metformin use and advanced age are associated with vitamin B12
deficiency and often present in type 2 diabetic patients, yet the prevalence of vitamin B12 deficiency in the diabetic
population is unknown.
Methods: We conducted a cross-sectional study of 203 outpatient type 2 diabetic patients at a large military
primary care clinic. Patients completed a survey and had B12 levels measured. Patients with borderline B12 levels
also had methylmalonic acid and homocysteine levels drawn. Serum B12 levels <100 pg/mL or serum B12 levels of
100 to 350 pg/mL with elevation of serum methylmalonic acid >243 nmol/L or homocysteine >11.9 nmol/L defined
B12 deficiency. Descriptive statistics described frequency and means. 2 and student’s t tests were used to analyze
associations between categorical and continuous variables, respectively. Multivariate logistical regression
identified covariates independently associated with B12 deficiency.
Results: Twenty-two percent (n 44) of diabetic patients had metabolically confirmed B12 deficiency. Patients on
metformin had lower serum B12 levels (425.99 pg/mL vs 527.49 pg/mL; P .012) and were at increased risk for B12
deficiency (P .04), as defined by a serum B12 level <350 pg/mL. Prevalence of B12 deficiency was significantly
lower for patients using a multivitamin (odds ratio, 0.31; 95% CI, 0.15– 0.63).
Conclusions: Our results found a 22% prevalence of metabolically confirmed B12 deficiency in the primary care
type 2 diabetic population. Although further research needs to be performed to determine the clinical implications
of our findings, B12 deficiency should be considered in type 2 diabetic patients, especially those taking metformin.
Furthermore, a daily multivitamin may protect against B12 deficiency.
(J Am Board Fam Med 2009;22:528 –534.)

High-Dose B-Vitamin Supplementation and Progression of Subclinical
Atherosclerosis: A Randomized Controlled Trial
Howard N. Hodis, MD1,2,3,4, Wendy J. Mack, PhD1,2, Laurie Dustin, MS1,2, Peter R. Mahrer,
MD5, Stanley P. Azen, PhD1,2, Robert Detrano, MD6, Jacob Selhub, PhD7, Petar Alaupovic,
PhD8, Chao-ran Liu, MD1,3, Ci-hua Liu, MD1,3, Juliana Hwang, PharmD1,4, Alison G. Wilcox,
Background and Purpose—Although plasma total homocysteine (tHcy) levels are associated with cardiovascular disease
(CVD), it remains unclear whether homocysteine is a cause or a marker of atherosclerotic vascular disease. We determined
whether reduction of tHcy levels with B-vitamin supplementation reduces subclinical atherosclerosis progression.
Methods—In this double-blind clinical trial, 506 participants 40–89 years of age with an initial tHcy >8.5 μmol/L without
diabetes and CVD were randomized to high-dose B-vitamin supplementation (folic acid 5 mg + vitamin B12 0.4 mg + vitamin
B6 50 mg) or matching placebo for 3.1 years. Subclinical atherosclerosis progression across 3 vascular beds was assessed
using highresolution B-mode ultrasonography to measure carotid artery intima-media thickness (primary outcome) and
multidetector spiral computed tomography to measure aortic and coronary artery calcium (secondary outcome).
Results—Although the overall carotid artery intima-media thickness progression rate was lower with B-vitamin
supplementation than with placebo, statistically significant between-group differences were not found (p=0.31). However,
among subjects with baseline tHcy≥9.1 μmol/L, those randomized to B-vitamin supplementation had a statistically significant
lower average rate of carotid artery intima-media thickness progression compared with placebo (p=0.02); among subjects
with a baseline tHcy <9.1 μmol/L there was no significant treatment effect (p-value for treatment interaction=0.02). B-vitamin
supplementation had no effect on progression of aortic or coronary artery calcification overall or within subgroups.
Conclusion—High-dose B-vitamin supplementation significantly reduces progression of early stage subclinical
atherosclerosis (carotid artery intima-media thickness) in well-nourished healthy B-vitamin “replete” individuals at
low-risk for CVD with a fasting tHcy >9.1 μmol/L.
Stroke. 2009 March ; 40(3): 730–736.
Serum B Vitamin Levels and Risk of Lung Cancer
Context B vitamins and factors related to 1-carbonmetabolism help to maintain DNA integrity and regulate gene expression
and may affect cancer risk.
Objective To investigate if 1-carbon metabolism factors are associated with onset of lung cancer.
Design, Setting, and Participants The European Prospective Investigation into Cancer and Nutrition (EPIC) recruited 519
978 participants from 10 countries between 1992 and 2000, of whom 385 747 donated blood. By 2006, 899 lung cancer
cases were identifiedand1770control participants were individually matched by country, sex, date of birth, and date of blood
collection. Serum levels were measured for 6 factors of 1-carbon metabolism and cotinine.
Main Outcome Measure Odds ratios (ORs) of lung cancer by serum levels of 4 B vitamins (B2, B6, folate [B9], and B12),
methionine, and homocysteine.
Results Within the entire EPIC cohort, the age-standardized incidence rates of lung cancer (standardized to the world
population, aged 35-79 years) were 6.6, 44.9, and 156.1 per100 000person-yearsamongnever, former, and current smokers
for men, respectively. The corresponding incidence rates forwomenwere7.1, 23.9,and100.9per100 000personyears,
respectively. After accounting for smoking, a lower risk for lung cancer was seen for elevated serum levels of B6 (fourth vs
first quartile OR, 0.44;95%confidence interval [CI], 0.33-0.60; P for trend.000001), as well as for serum methionine (fourth
vs first quartile OR, 0.52; 95% CI, 0.39-0.69; P for trend.000001). Similar and consistent decreases in risk were observed in
never, former, and current smokers, indicating that results were not due to confounding by smoking. The magnitude of risk
was also constant with increasing length of follow-up, indicating that the associationswerenot explainedbypreclinical
disease. A lower risk was also seen for serum folate (fourth vs first quartile OR, 0.68;95%CI, 0.51- 0.90; P for trend =.001),
although this was apparent only for former and current smokers. When participants were classified by median levels of
serum methionine and B6, having above-median levels of bothwasassociated with a lower lung cancer risk overall (OR,
0.41; 95% CI, 0.31-0.54), as well as separately among never (OR, 0.36; 95% CI, 0.18-0.72), former(OR,0.51;95%CI, 0.34-
0.76),andcurrent smokers(OR,0.42;95%CI, 0.27-0.65).
Conclusion Serum levels of vitamin B6 and methionine were inversely associated with risk of lung cancer.
JAMA. 2010;303(23):2377-2385
Dietary Folate and Vitamin B6 and B12 Intake in Relation to Mortality From
Cardiovascular Diseases Japan Collaborative Cohort Study
Renzhe Cui, MD; Hiroyasu Iso, MD; Chigusa Date, MD; Shogo Kikuchi, MD; Akiko Tamakoshi, MD;
for the Japan Collaborative Cohort Study Group
Background and Purpose—The association of dietary folate and B vitamin intakes with risk of
cardiovascular disease is controversial, and the evidence in Asian populations is limited.
Methods—A total of 23 119 men and 35 611 women, age 40 to 79 years, completed a food frequency
questionnaire in the Japan Collaborative Cohort Study. During the median 14-year follow-up, there were
986 deaths from stroke, 424 from coronary heart disease, and 2087 from cardiovascular disease.
Results—Dietary folate and vitamin B6 intakes were inversely associated with mortality from heart failure
for men and with mortality from stroke, coronary heart disease, and total cardiovascular disease for
women. These inverse associations did not change materially after adjustment for cardiovascular risk
factors. No association was found between vitamin B12 intake and mortality risk.
Conclusions—High dietary intakes of folate and vitamin B6 were associated with reduced risk of mortality
from stroke, coronary heart disease, and heart failure among Japanese.
(Stroke. 2010;41:00-00.)

Folate, Vitamin B12, and Homocysteine as Risk Factors for Cognitive
Decline in the Elderly
Jae-Min Kim, MD, PhD, Sung-Wan Kim, MD, PhD, Il-Seon Shin, MD, PhD, Su-Jin Yang, MD, PhD, Woo-Young Park,
MD, Sung-Jin Kim, MD, Hee-Young Shin, MD, PhD, Jin-Sang Yoon, MD, PhD
Objective Cross-sectional studies have shown that the dysregulation of one-carbon metabolism is associated with cognitive
impairment. However, the findings of longitudinal studies investigating this association have been inconsistent. This study
investigated the prospective associations between cognitive decline and the levels of folate, vitamin B12 and homocysteine
both at baseline and over course of the study period.
Methods A total of 607 (83%) elderly individuals were selected from a group of 732 elderly individuals without dementia at
baseline and followed over a 2.4-year study period. The Mini-Mental State Examination (MMSE) was administered to the
subjects, and the serum levels of folate, vitamin B12 and homocysteine were assayed both at baseline and at followup
examinations. Covariates included demographic data, disability, depression, alcohol consumption, physical activity, vascular
risk factors, serum creatinine level, vitamin intake, and apolipoprotein E genotype.
Results Cognitive decline was associated with decreasing quintiles of folate at baseline, a relative decline in folate and an
increase in homocysteine across the two examinations after adjustment for relevant covariates.
Conclusion These results suggest that folate and homocysteine are involved in the etiology
of cognitive decline in the elderly.
Psychiatry Invest 2008;5:36-40

Vitamin B12, cognition, and brain MRI measures A cross-sectional
examination
C.C. Tangney, PhD, N.T. Aggarwal, MD, H. Li, MS, R.S. Wilson, PhD, C. DeCarli, MD, D.A. Evans,
MD and M.C. Morris, ScD
Objective: To investigate the interrelations of serum vitamin B12 markers with brain volumes, cerebral
infarcts, and performance in different cognitive domains in a biracial population sample cross-sectionally.
Methods: In 121 community-dwelling participants of the Chicago Health and Aging Project, serum markers
of vitamin B12 status were related to summary measures of neuropsychological tests of 5 cognitive
domains and brain MRI measures obtained on average 4.6 years later among 121 older adults.
Results: Concentrations of all vitamin B12–related markers, but not serum vitamin B12 itself, were
associated with global cognitive function and with total brain volume. Methylmalonate levels were
associated with poorer episodic memory and perceptual speed, and cystathionine and 2-methylcitrate with
poorer episodic and semantic memory. Homocysteine concentrations were associated with decreased total
brain volume. The homocysteine-global cognition effect was modified and no longer statistically significant
with adjustment for white matter volume or cerebral infarcts. The methylmalonate-global cognition effect
was modified and no longer significant with adjustment for total brain volume.
Conclusions: Methylmalonate, a specific marker of B12 deficiency, may affect cognition by reducing total
brain volume whereas the effect of homocysteine (nonspecific to vitamin B12 deficiency) on cognitive
performance may be mediated through increased white matter hyperintensity and cerebral infarcts. Vitamin
B12 status may affect the brain through multiple mechanisms.
Neurology September 27, 2011 vol. 77 no. 13 1276-1282

Trimethylglycine [betaine]
Trimethylglycine (TMG), commonly known as betaine, is naturally produced in
the body to diminish hazardous homocysteine levels. TMG converts
homocysteine into methionine, which is an essential amino acid for healthy hair,
skin, and nails.
Betaine reduces homocysteine levels and restores SAMe production.1 Betaine
increased SAMe (a L-methionine metabolite) levels in rats with fatty livers. The
increase of SAMe decreased fat accumulation in the liver and aided the
production of glutathione, a strong antioxidant that prevents free radical
damage.2
Betaine is effective in lowering homocysteine levels.3 and can lower
homocysteine levels up to 20% in healthy subjects.4
Betaine supplementation (500 mg) was administered to healthy male subjects
(19-40 years old) finding homocysteine levels were reduced 4 to 6 hours after
intake. Researchers concluded betaine’s ability to augment L-methionine
production decreased homocysteine concentrations.5

Trimethylglycine [betaine]
Homocysteine levels decreased in healthy volunteers with normal body weight
after a single-dose of betaine (3 or 6 g) was administered two hours prior to
evaluation.6
Betaine supplementation decreased homocysteine levels in 42 obese subjects (6
g/day, but had no effects on fat mass.7
Dose: 500 to 1000 mgs daily
1 Kharbanda, KK. Role of transmethylation reactions in alcoholic liver disease. World J Gastroenterol. 2007 Oct;
13(37):4947-4954. 2 Barak, AJ, Beckenhauer, HC, Tuma, DJ. S-adenosylmethionine generation and prevention of alcoholic fatty liver by
betaine. Alcohol. 1994; 11:501-503. 3 Guthikonda, S, Haynes, WG. Homocysteine: role and implications in atherosclerosis. Curr Atheroscler Rep. 2006 Mar;
8(2):100-106. 4 Olthof, MR, Verhoef, P. Effects of betaine intake on plasma homocysteine concentrations and consequences for health.
Curr Drug Metab. 2005 Feb; 6(1):15-22. 5 Atkinson, W, Elmslie, J, Lever, M, et al. Dietary and supplementary betaine: acute effects on plasma betaine and
homocysteine concentrations under standard and postmethionine load conditions in healthy male subjects. Am J Clin
Nutr. 2008 Mar; 87(3):577-585. 6Schwab, U, Torronen, A, et al. Orally administered betaine has an acute and dose-dependent effect on serum betaine
and plasma homocysteine concentrations in healthy humans. J Nutr. 2006 Jan; 136(1):34-38. 7 Schwab, U, Torronen, A, et al. Betaine supplementation decreases plasma homocysteine concentrations but does not
affect body weight, body composition, or resting e

L-Theanine - [GREEN TEA]
Uses;
1. Stress Relief
2. Mood Balance
3. Premenstrual Syndrome
4. Immune Function
Dosage: 50 mgs to 200 mgs per day

GREEN TEA
Green Tea is rich in catechin polyphenols, particularly epigallocatechin gallate
(EGCG), which has thermogenic and fat oxidizing capabilities. Green Tea has
been an effective aid for fat oxidation, weight management, and insulin
sensitivity.15
Men and women with excessive visceral fat were given Green Tea for 12 weeks
finding a decrease in fat and overall body weight was greater than the control
group.16
Glucose tolerance and fat oxidation were measured in moderate-intensity
exercise subjects taking Green Tea extract. Results indicated fat oxidation levels
(17%) and glucose sensitivity (13%) were higher after taking Green Tea extract,
when compared to the placebo.

GREEN TEA
Combining Green Tea extract with an exercise routine increased fat oxidation in the liver and skeletal
muscles, and decreased weight in mice consuming a high-fat diet.17
Furthermore, Green Tea extract stimulated fat oxidation to improve exercise endurance capacity in mice.
Researchers indicated exercise endurance was 30% higher in mice taking Green Tea extract, as metabolic
capacity and fat utilization increased to improve skeletal muscle energy.18, 19
15 Venables, MC, Hulston, CJ, Cox, HR, Jeukendrup, AE. Green Tea extract ingestion, fat oxidation, and
glucose tolerance in healthy humans. Am J Clin Nutr. 2008 Mar; 87(3):778-784. 16 Nagao, T, Hase, T, Tokimitsu, I. A Green Tea extract high in catechins reduces body fat and
cardiovascular risks in humans. Obesity. 2007 Jun; 15(6):1473-1483. 17 Shimotoyodome, A, Haramizu, S, Inaba, M, et al. Exercise and Green Tea extract stimulate fat oxidation
and prevent obesity in mice. Med Sci Sports Exerc. 2005 Nov; 37(11):1884-1892. 18 Murase, T, Haramizu, S, et al. Green Tea extract improves endurance capacity and increases muscle
lipid oxidation in mice. Am J Physiol Regul Integr Comp Physiol. 2005 Mar; 288(3):R708:715. 19 Murase, T, Haramizu, S, et al. Green Tea extract improves running endurance in mice by stimulating lipid
utilization during exercise. Am J Physiol Regul Integr Comp Physiol. 2006 Jun; 290(6):R1550-1556.

L-Theanine
Naturally found in green tea, L-Theanine makes up 50% of the amino acid
properties in this plant.
L-Theanine increases alpha-brain wave activity and decreases beta waves to
promote optimal brain function.
Unlike other relaxants that cause drowsiness, alpha-brain wave activity is
associated with relaxation. This effect can calm the mind, while improving mental
awareness and mood. L-Theanine can also alleviate mood changes, cramps and
irritability associated with the menstrual cycle
It can reduce the heart rate in participants exposed to stress related tasks1, while
the calming effects may also impact blood pressure.

L-Theanine
48 healthy adults were 200 mg of L-Theanine, 250 mg of caffeine, both, or a
placebo. Blood pressure was monitored before administration and 40 minutes
after intake. Results indicated L-Theanine reduced blood pressure levels that
were raised by caffeine, concluding L-Theanine may be useful in balancing blood
pressure and reducing anxiety.2
A double-blind study investigated mental and mood effects of 250 mg/day of L-
Theanine, in combination with 150 mg/day of caffeine from green tea. Results
indicated the combination improved mental alertness and reduced fatigue.9
L-Theanine fights against neurotoxins and oxidative stress that can damage the
nervous system. One study found L-Theanine reduced the effects of oxidative
stress in the brain and inhibited the death of neuronal cells that leads to nervous
system dysfunction.10

L-Theanine
30 mg of L-Theanine stimulated alpha brain waves that lead to a positive mood
and improved cognition.3 The same researchers extended the study finding L-
Theanine enhanced mental performance and attention span in healthy volunteers
that consumed decaffeinated green tea with a high content of L-Theanine and
theogallin (a polyphenol found in tea).4
Women with premenstrual symptoms were recruited for a twelve-week study to
observe the effects of 200 mg/day of L-Theanine on mood swings, irritability,
crying, etc. The study found L-Theanine reduced premenstrual symptoms in
women supplementing with L-Theanine, when compared to the placebo group.5

L-Theanine
L-Theanine has been investigated as an aid for the immune system. A double-blind study of
healthy adults (18-70 years old) reviewed the effects of green tea capsules on gammadelta
T cell function (cells that fight infections) being administered for three months. Subjects
taking the supplement had more T cell proliferation and fewer illnesses. Researchers
concluded green tea capsules are a safe, effective treatment against cold and flu
symptoms.11
Individuals exclusively taking L-Theanine had less cold and flu symptoms, as gammadelta T
cell function improved.12
1 Kimura, K, Ozeki, M, Juneja, LR, Ohira, H. L-Theanine reduces psychological and physiological stress responses. Biol Psychol. 2007; 74(1):39-45. 2 Rogers, PJ, Smith, JE, Heatherley, SV, Pleydell-Pearce, CW. Time for tea: mood, blood pressure and cognitive performance effects of caffeine and theanine administered alone and
together. Psychopharmacology. 2008 Jan; 195(4):569-577. 3 Dimpfel, W, Kler, A, Kriesl, E, Lehnfeld, R. Theogallin and L-Theanine as active ingredients in decaffeinated green tea extract: II. Characterization in the freely moving rat by means
of quantitative field potential analysis. J Pharm Pharmacol. 2007 Oct; 59(10):1397-1403. 4 Dimpfel, W, Kler, A, et al. Source density analysis of the human EEG after ingestion of a drink containing decaffeinated extract of green tea enriched with L-Theanine and theogallin. Nutr Neurosci. 2007; 10(3-4):169-180. 5 Timmcke Quilici, J, Juneja, L, Kapoor, MP. Efficacy and Short-Term Safety of L-Theanine in Randomized, Double-Blind, Parallel-Group Study. The FASEB Journal. 2008; 22:760. 6 Nobre, AC, Rao, A, Owen, GN. L-Theanine, a natural constituent in tea, and its effect on mental state. Asia Pac J Clin Nutr. 2008; 17(1):167-168. 7 Nathan, PJ, Lu, K, et al. The neuropharmacology of L-Theanine(N-ethyl-L-glutamine): a possible neuroprotective and cognitive enhancing agent. J Herb Pharmacother. 2006; 6(2):21-30. 8 Yamada, T, Terashima, T, Honma, H, et al. Effects of Theanine, a unique amino acid in tea leaves, on memory in a rat behavioral test. Biosci Biotechnol Biochem. 2008 May;
72(5):1356-1359. 9 Haskell, CF, Kennedy, DO, Milne, AL, et al. The effects of L-Theanine, caffeine and their combination on cognition and mood. Biol Psychol. 2008 Feb; 77(2):113-122. 10 Cho, HS, Kim, S, et al. Protective effect of the green tea component, L-Theanine on environmental toxins-induced neuronal cell death. Neurotoxicology. 2008 Jul; 29(4):656-662.
11 Rowe, CA, Nantz, MP, Bukowski, JF, Percival, SS. Specific formulation of Camellia sinensis prevents cold and flu symptoms and enhances gamma,delta T cell function: a
randomized, double-blind, placebo-controlled study. J Am Coll Nutr. 2007 Oct; 26(5):445-452. 12 Bukowski, JF, Percival, SS. L-Theanine intervention enhances human gammadeltaT lymphocyte function. Nutr Rev. 2008 Feb; 66(2):96-102.
COENZYME Q 10
Indications:
1. Cardiovascular Health
2. Energy production
3. Neurological Health
4. Blood Sugar Stabilization
5. Skin health
Dosage Up to 600 mgs per day

COENZYME Q 10
Coenzyme Q10 (Ubiquinone), is found in every living organism, as each cell
depends on it to create energy.
The body naturally forms CoQ10, but production starts to decrease around 30
years old.
CoQ10 is a crucial antioxidant that neutralizes free radicals and regenerates the
production of vitamin
CoQ10 is an aid in several aspects of heart health; such as preventing cholesterol
oxidation, especially in balancing LDL cholesterol levels.
CoQ10 benefits blood pressure by lowering systolic and diastolic levels without
significant side effects.1,2,3 A meta-analysis of 12 clinical trials (362 patients)
showed systolic blood pressure could decrease up to 17 mm Hg, while diastolic
blood pressure could decrease up to 10 mm Hg with CoQ10 supplementation.4

COENZYME Q 10
60 mg per day of CoQ10 safely lowered systolic blood pressure by 7.3 mm Hg in twelve-
weeks.5
CoQ10 is viewed as a safe addition to standard heart treatments.6
90 mg per day of CoQ10, in conjunction with 5 gm per day of phospholipids (lecithin)
decreased systolic and diastolic blood pressure, along with total and LDL cholesterol in four-
weeks.7
Supplementing CoQ10 can relieve side effects associated with various heart treatments.
CoQ10 can reduce muscle pain associated with statin drug use.
Patients were given CoQ10 (100 mg per day) or vitamin E (400 IU per day) for 30 days. Pain
severity decreased by 40%, and pain interference with daily activities decreased by 38% in
the CoQ10 group. In contrast, pain was not relieved in the vitamin E group.8
Another study indicated CoQ10 supplementation improved diastolic function that is often
worsened with statin therapy.9

COENZYME Q 10
CoQ10 aids athletes’ energy demands. Subjects supplemented with 100 to 300
mg per day of CoQ10 one week prior to a workload trial experienced less fatigue
and improved athletic performance during the workload.10
Supplementing 300 mg/d of CoQ10 decreased exercise-induced muscle injuries
among Japanese Kendo athletes training 5 to 6 hours each day.11
Supplementing with 200 mg of CoQ10 rapidly restores CoQ10 levels in the
muscles and reduces oxidative stress. Subjects that received an acute dose (one
time dose) of 200 mg had a higher CoQ10 muscle concentration and lower levels
of oxidative stress in the muscle. The same study found subjects receiving a
chronic dose (fourteen-days, 200 mg per day) improved their workout capacity, as
they experienced less fatigue.12
Researchers are exploring the benefits CoQ10 on improving energy expenditure
in the brain and hindering the effects of neurological ailments. After two months of
CoQ10 supplementation (100 to 200 mg per day), energy expenditure in the brain
can increase by 29%.13

COENZYME Q 10
A study conducted by the University of California at San Diego randomly
assigned 80 patients with early stages of neurological degeneration to receive
300, 600 or 1200 mg of CoQ10 each day, or a placebo. After 10 months of
research, the study found that patients receiving the 1200 mg dose had a 44%
slower rate of decline, when compared to the placebo group.14
A twelve-week study found that patients with blood sugar imbalances could
stabilize their blood levels by supplementing with 200 mg of CoQ10 per day.15
Another study found ketone levels that are associated with unstable blood
sugar were lowered in more than half of patients that received 120 mg of
CoQ10 for up to eighteen-weeks.16

COENZYME Q 10
CoQ10 is naturally found in the skin with vitamins A, C, and E; but its overall
production diminishes with age leaving skin susceptible to oxidative damage
caused by free radicals. Research suggests CoQ10 can repair and protect the
skin from oxidative damage that accelerates skin aging.
In combination with carotenoids, topical CoQ10 has been shown to be a potent
anti-inflammatory that is easily absorbed through the skin to discourage
premature aging.17
Along with reducing oxidative stress, another study found topical CoQ10
improves the appearance of the skin by decreasing wrinkle depth.18

COENZYME Q 10
1 Rosenfeldt, F. et al. Systematic review of effect of coenzyme Q10 in physical exercise, hypertension and heart failure. Biofactors. 2003; 18(1-
4):91-100.
2 Houston, M.C. The role of vascular biology, nutrition and nutraceuticals in the prevention and treatment of hypertension. JANA.2002; S1:5-71.
3 Tran, MT, Mitchell, TM, et al. Role of coenzyme Q10 in chronic heart failure, angina, and hypertension. Pharmacotherapy. 2001 Jul; 21(7):797-
806.
4 Rosenfeldt, F., Haas, S., Krum, H., et al. Coenzyme Q10 in the treatment of hypertension: a meta-analysis of the clinical trials. J Hum
Hypertension. 2007 Apr; 21(2):297-306.
5 Burke, B., Neuenschwander, R., Olson, R. Randomized, double-blind, placebo-controlled trial of coenzyme Q10 in isolated systolic hypertension.
South Med Journal. 2001; 94(11):1112-1117.
6 Pepe, S, Marasco, S, Haas, S, et al. Coenzyme Q10 in cardiovascular disease. Mitochondrion. 2007; S154-167.
7 Eshginia, S, Gapparov, M. The influence of phospholipids food and antioxidant at patients with hypertension. Vopr Pitan. 2006; 75(2):37-39.
8 Caso, G, Kelly, P, et al. Effect of coenzyme q10 on myopathic symptoms in patients treated with statins. Am J Cardiol. 2007 May; 99(10):1409-
1412.
9 Silver, MA, Langsjoen, PH, et al. Effect of atorvastatin on left ventricular diastolic function and ability of coenzyme Q10 to reverse that dysfunction.
Am J Cardiol. 2004 Nov; 94(10):1306-1310.
10 Mizuno, K, et al. Antifatigue effects of coenzyme Q10 during physical fatigue. Nutrition. 2008 Apr;24(4):293-299.
11 Kon, M et al. Reducing exercise-induced muscular injury in kendo athletes with supplementation of coenzyme Q10. British Jour Nutr. 2008 Feb;
20:1-7.
12 Cooke, M, Iosia, M, Buford, T, et al. Effects of acute and 14-day coenzyme Q10 supplementation on exercise performance in both trained and
untrained individuals. J Int Soc Sports Nutr. 2008 Mar;5:8.
13 Matthews, R T, Yang, L, Browne, S, Baik, M, Beal, MF. Coenzyme Q10 administration increases brain mitochondrial concentrations and exerts
neuroprotective effects. Proceedings National Academy of Sciences. 1998 Jul; 95(15):8892-8897.
14 Shults, CW, Oakes, D, Kieburtz, K, et al. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch
Neurol. 2002; 59(10):1541-1550.
15 Hodgson, JM, Watts, GF, Playford, DA, Burke, V, Croft, KD. Coenzyme Q10 improves blood pressure and glycaemic control in a controlled trial
in subjects with type 2 diabetes. Eur J Clin Nutr. 2002 Nov; 56(11):1137-1142.
16 Gaby, AR. The role of coenzyme Q10 in clinical medicine: Part II. Cardiovascular disease, hypertension, diabetes mellitus and infertility. Altern
Med Rev. 2001 Sept; 1(3):168-175.
17 Fuller, B, Smith, D, et al. Anti-inflammatory effects of CoQ10 and colorless carotenoids. J Cosmet Dermatol. 2006 Mar; 5(1):30-38.
18 Hoppe, U, Bergemann, J, Diembeck, W, et al. Coenzyme Q10, a cutaneous antioxidant and energizer. Biofactors. 1999; 9(2-4):371-378.

COENZYME Q 10
In healthy individuals, CoQ10 is created from tyrosine (or phenylalanine) and mevalonate.1
As we age, CoQ10 levels decline leading to greater oxidative stress, aging, and disease.2
CoQ10 is an essential antioxidant that is needed to regenerate other antioxidants, stimulate
cellular growth, and inhibit cell death. Studies show that CoQ10 can benefi t heart health by
supporting healthy blood pressure levels.3,4,5
CoQ10 levels decrease dramatically when individuals are taking statin drugs. CoQ10
supplementation is a safe and effective way to restore deficiencies.
Similar to the high-energy demands found in the heart, the brain relies on cellular energy for
optimal mitochondrial function. After two months of CoQ10 supplementation (100 to 200 mg
per day), energy expenditure in the brain can increase by 29%.6 A study conducted by the
University of California at San Diego randomly assigned 80 patients with early stages of
neurological degeneration to receive 300, 600 or 1200 mg of CoQ10 each day, or a placebo.
After 10 months of research, the study found that patients receiving the 1200 mg dose had a
44% slower rate of decline, when compared to the placebo group.7
COENZYME Q 10
CoQ10 is also beneficial to help athletes meet energy demands
Researchers have observed that CoQ10 supplementation can improve athletic
performance and decrease exercise induced muscle injuries.8,9
Supplementing with CoQ10 reduces oxidative stress in the muscles to decrease
levels of fatigue.10 Unstable bloodsugar levels can occur from a CoQ10
deficiency, as this nutrient influence’s glucose assimilation.
A twelve-week study found that patients with type 2 diabetes could stabilize their
blood levels by supplementing with 200 mg of CoQ10 per day.11

COENZYME Q 10
1Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr. 2001 Dec;20(6):591-598.
2Willis R, Anthony M, Sun L, Honse Y, Qiao G. Clinical implications of the correlation between coenzyme Q10 and vitamin B6 status. Biofactors.
1999;9(2-4):359-363.
3Rosenfeldt, F. et al. Systematic review of effect of coenzyme Q10 in physical exercise, hypertension and heart failure. Biofactors. 2003; 18(1- 4):91-
100.
4Houston, M.C. The role of vascular biology, nutrition and NUTRAceuticals
in the prevention and treatment of hypertension. JANA.2002; S1:5-71.
5Tran, MT, Mitchell, TM, et al. Role of coenzyme Q10 in chronic heart failure, angina, and hypertension. Pharmacotherapy. 2001 Jul; 21(7):797- 806.
6Matthews, R T, Yang, L, Browne, S, Baik, M, Beal, MF. Coenzyme Q10 administration increases brain mitochondrial concentrations and exerts
neuroprotective effects. Proceed Nat Academy of Sciences. 1998 Jul; 95(15):8892-8897.
7Shults, CW, Oakes, D, Kieburtz, K, et al. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline.
Arch Neurol. 2002; 59(10):1541-1550.
8Mizuno, K, et al. Antifatigue effects of coenzyme Q10 during physical fatigue. Nutrition. 2008 Apr;24(4):293-299.
9Kon, M et al. Reducing exercise-induced muscular injury in kendo athletes with supplementation of coenzyme Q10. British Jour Nutr. 2008 Feb; 20:1-
10Cooke, M, Iosia, M, Buford, T, et al. Effects of acute and 14-day coenzyme Q10 supplementation on exercise performance in both trained
and untrained individuals. J Int Soc Sports Nutr. 2008 Mar;5:8.
11Hodgson, JM, Watts, GF, Playford, DA, Burke, V, Croft, KD. Coenzyme Q10 improves blood pressure and glycaemic control in a controlled trial in
subjects with type 2 diabetes. Eur J Clin Nutr. 2002 Nov; 56(11):1137-1142.

PQQ/Pyrroloquinoline quinone PQQ supports mitochondrial health and cellular energy production, and to protect
the body from oxidative stress
PQQ stimulates the spontaneous growth of new mitochondria in aging cells, and
activates genes that govern mitochondrial reproduction, protection, and repair.
PQQ is especially effective in neutralizing superoxide and hydroxylradicals,[1][2] two
prominent causes of mitochondrial dysfunction.
PQQ not only protects mitochondria from oxidative stress—it promotes the
spontaneous generation of new mitochondria within aging cells, a process known
as mitochondrial biogenesis.[3] The implications of this revelation for human health
and longevity are significant because the only other known methods proven to
stimulate mitochondiral biogenesis in aging humans are intense aerobic
exercise,[4] strict caloric restriction,[5] and certain medications such as
thiazolidinediones[6] and the diabetes drug metformin.[7]

PQQ/Pyrroloquinoline quinone
PQQ is a potent neuroprotective nutrient that has been shown to protect
memory and cognition in both aging animals and humans.[8]9]
It has been shown to reverse cognitive impairment caused by chronic oxidative
stress in pre-clinical models and improve performance on memory tests.[10]
PQQ supplementation stimulates the production and release of nerve growth
factor in cells that support neurons in the brain,[11] a possible explanation for the
marked improvement of memory function it produces in aging humans and rats

PQQ/Pyrroloquinoline quinone
PQQ has been shown to promote memory, attention, and cognition in humans.
In a double-blind, placebo-controlled clinical trial conducted in Japan in 2007,
supplementation with 20 mg per day of PQQ resulted in improvements on tests of
higher cognitive function in a group of 71 middle-aged and elderly people aged
between 40-70, who outperformed the placebo group by more than twofold in their
standardized memory tests. [12]
Results of the study also suggest a synergistic relationship between PQQ and the
nutrient coenzyme Q10 (CoQ10), which further amplified performance on
standardized memory tests when subjects also took 300 mg per day of CoQ10. No
adverse effects were linked to the supplementation, and the results demonstrated
that PQQ, especially when combined with CoQ10, can be used to improve mental
status and quality of life in older patients, and help slow or prevent age-related
cognitive decline in middle-age patients.

PQQ/Pyrroloquinoline quinone
1 ^ Hara, H; Hiramatsu, H; Adachi, T (2007 Mar). "Pyrroloquinoline quinone is a potent neuroprotective nutrient against 6-
hydroxydopamine-induced neurotoxicity". Neurochemical Research 32 (3): 489–95.
2 ^ Urakami, T; Yoshida, C; Akaike, T; Maeda, H; Nishigori, H; Niki, E (1997). "Synthesis of monoesters of pyrroloquinoline
quinone and imidazopyrroloquinoline, and radical scavenging activities using electron spin resonance in vitro and
pharmacological activity in vivo". Journal of nutritional science and vitaminology 43 (1): 19–33.
3^ Chowanadisai, W; Bauerly, KA; Tchaparian, E; Wong, A; Cortopassi, GA; Rucker, RB (2010 Jan). "Pyrroloquinoline
quinone stimulates mitochondrial biogenesis through cAMP response element-binding protein phosphorylation and
increased PGC-1alpha expression". Journal of Biological Chemistry 285 (1): 142–52.
4^ Lanza, IR; Sreekumaran Nair, K (2010 Aug). "Regulation of skeletal muscle mitochondrial function: genes to proteins".
Acta Physiologica 199 (4): 529–47.
5^ Spindler, SR (2010 Jul). "Caloric restriction: from soup to nuts". Ageing Research Reviews 9 (3): 324–53.
6^ Fujisawa, K.; Nishikawa, T.; Kukidome, D.; Imoto, K.; Yamashiro, T.; Motoshima, H.; Matsumura, T.; Araki, E. (2009).
"TZDs reduce mitochondrial ROS production and enhance mitochondrial biogenesis". Biochemical and Biophysical
Research Communications 379 (1): 43–48.
7^ Suwa, M; Egashira, T; Nakano, H; Sasaki, H; Kumagai, S (2006 Dec). "Metformin increases the PGC-1alpha protein and
oxidative enzyme activities possibly via AMPK phosphorylation in skeletal muscle in vivo". Journal of Applied Physiology 101
(6): 1685–92.

PQQ/Pyrroloquinoline quinone
8^ Takatsu, H; Owada, K; Abe, K; Nakano, M; Urano, S (2009). "Effect of vitamin E on learning and memory deficit in
aged rats". Journal of nutritional science and vitaminology 55 (5): 389–93.
9^ "Effect of pyrroloquinoline quinone (PQQ) on mental status of middle-aged and elderly persons". Food Style 21 13 (7):
50–52. 2009.
10^ Ohwada, K; Takeda, H; Yamazaki, M; Isogai, H; Nakano, M; Shimomura, M; Fukui, K; Urano, S (2008 Jan).
"Pyrroloquinoline quinone (PQQ) prevents cognitive deficit caused by oxidative stress in rats". Journal of Clinical
Biochemistry and Nutrition 42: 29–34.
11^ Murase, K; Hattori, A; Kohno, M; Hayashi, K (1993). "Stimulation of nerve growth factor synthesis/secretion in mouse
astroglial cells by coenzymes". Biochemistry and molecular biology international 30 (4): 615–21.
12Effect of pyrroloquinoline quinone (PQQ) on mental status of middle-aged and elderly persons". Food Style 21 13 (7):
50–52. 2009

Grape Seed
Proanthocyanidins found in grape seeds, can stabilize LDL levels and maintain
cardiovascular health.
Common injury and free radical damage can come to the arteries after they are
cleared from plaque buildup.
Proanthocyanidins reduced the formation of free radicals and had cardioprotective
benefits in rats after restoring blood flow to the vessels.(1)
A 21-week study observed that grape seed extract decreased LDL levels and
protected the vascular endothelium (blood vessel lining) maintaining tone in the
artery walls and stabilizing blood pressure.(2)
A Greek study recruited 30 men with cardiovascular ailments to see if grape seed
extract would improve endothelial function by improving blood flow dilation in the
arteries. Results signified that subjects taking 600 mg per day of grape seed
extract had significant improvement in blood flow and endothelial function.(3)

Grape Seed
A series of studies conducted at Creighton University have indicated
proanthocyandins have remarkable benefits on heart health by optimizing several
cardiovascular functions, including endothelial function and decreased LDL levels.
Primarily, proanthocyanidins protect the heart from the dangerous formation of free
radicals and oxidative stress.(4)
Researchers administered grape extract to rats for three weeks finding the
antioxidant scavenged free radicals to significantly reduce injury associated with
ischemia-reperfusion.(5)
1 Pataki T, Bak I, Kovacs P, et al. Grape seed proanthocyanidins improved cardiac recovery during reperfusion after ischemia in isolated rat hearts.
Am J Clin Nutr. 2002 May; 75(5):894-899.
2 Yu H, Wang SE, Zhao C, Xu G. Study of anti-atherosclerosic effect of grape seed extract and its mechanism. Wei Sheng Yan Jin. 2002 Aug;
31(4):263-265.
3 Lekakis J, Rallidis LS, Andreadou I, et al. Polyphenolic compounds from red grapes acutely improve endothelial function in patients with coronary
heart disease. Eur J Cardiovasc Prev Rehabil. 2005 Dec; 12(6):596-600.
4 Bagchi D, Sen,CK, Ray SD et al. Molecular mechanisms of cardioprotection by a novel grape seed proanthocyanidin extract. Mutat Res. 2003; 523-
524:87-97.
5 Cui J, Cordis GA, Tosaki A, Maulik N, Das DK. Reduction of myocardial ischemia reperfusion injury with regular consumption of grapes. Ann NY
Acad Sci. 2002;957: 302-307.

Diindolymethane (DIM) Plant indoles, also called glucosinolates, found in cruciferous vegetables provide
health benefits to humans. Cruciferous vegetables are known for their cancer
protection.
Two such indoles provided by cruciferous vegetables are I3C (Indole 3
Carbinol) and DIM (Diindolylmethane).
Consumption of cruciferous vegetables, including broccoli, Brussels sprouts, kale,
and cauliflower, has been associated with a decreased risk of various human
cancers. The strongest associations are with cancers of the breast, endometrium,
colon, and prostate (10).
DIM is not naturally present in these plants. It gets released with the help of
enzymes upon crushing of the broccoli, cauliflower, cabbage or brussel sprouts or
during human digestion. (1,3 )

Diindolymethane (DIM)
DIM is 2 molecules of I3C combined together
Stomach acid, or HCl, can also aid the joining of two indole 3 carbinols to make
diindolylmethane. Lack of HCl will hinder one's ability to make DIM from I3C. (2)
DIM absorption can be greatly enhanced by emulsifying it with lecithin in rice
bran oil, including with it compounds that hold it in solution such as beeswax, and
finally adding fat soluble nutrients that aid absorption through the gut wall.

Diindolymethane (DIM)
It has been suggested that a low level of the 2-hydroxyestrogen metabolites (2-
OHE) and a high level of 16 alpha-hydroxyestrone (16 alpha-OHE1) is associated
with an enhanced risk of breast cancer. DIM increases 2 hydroxyestrone and
therefore improves the 2/16 hydroxyestrone ratio, making it very protective for
womenat high risk for this condition. (6)
DIM also reduces availability of 4 androstenedione for aromatization to estrone.
(7)
Diindolymethane (DIM)
DIM is more potent than I3C at protecting against mammary carcinoma due to
decreased formation of 16 alpha-hydroxyestrone from estrone. (6)
I3C,unlike DIM, raises 4-hydroxy estrogen with the potential of aggravating
cancers such as breast, endometrial and prostate cancer. I3C increases 4-
hydroxy estrogen production in animals and in humans. (8)
4-hydroxyestrogens and CYP1B1, the only CYP source of 4-hydroxy estrogen,
have both been implicated in the causation of prostate and breast cancer in
humans. 4-hydroxy estrogens and CYP1B1 are also implicated in the causation
and growth of uterine fibroid tumors and endometriosis.

Diindolymethane (DIM)

Diindolymethane (DIM)
DIM is an aromatase inhibitor. DIM helps to block the conversion of testosterone
to estrogen. (10)
DIM induces apoptosis in PC3 cells, through the mitochondrial pathway
suggesting that DIM is hopeful as a therapeutic strategy for the treatment of
androgen-independent prostate cancer. (11)
According to UC Berkeley researchers “DIM exhibits potent antiproliferative and
antiandrogenic properties in androgen-dependent human prostate cancer cells.
DIM suppresses cell proliferation of LNCaP cells and inhibits
dihydrotestosterone (DHT) stimulation of DNA synthesis.” DIM is a strong
competitive inhibitor of DHT binding to the androgen receptor.
An in vivo study in rats showed that DIM cut in half testosterone 16 alpha and 2
alpha-hydroxylation. (12)

Diindolymethane (DIM) 1. Johnson IT. Glucosinolates: bioavailability and importance to health. Int J Vitam Nutr Res. 2002 Jan;72(1):26-31.
2. McDanell R, McLean AE, Hanley AB, Heaney RK, Fenwick GR. Chemical and biological properties of indole
glucosinolates. J Agric Food Chem. 1999 Apr;47(4):1541-8.
3. Grose, KR, and Bjeldanes, LF. Oligermization of indole-3-carbinol in aqueous acid. Chem Res Toxicol 1992: 5:188-193.
(glucobrassicins): a review. Food Chem Toxicol. 1988 Jan;26(1):59-70.
4. Park JY, Shigenaga MK, Ames BN. Induction of cytochrome P4501A1 by 2,3,7,8-tetrachlorodibenzo-p-dioxin or
indolo(3,2-b)carbazole is associated with oxidative DNA damage.
5. Jensen-Jarolim E, Gajdzik L, Haberl I, Kraft D, Scheiner O, Graf J.Hot spices influence permeability of human intestinal
epithelial monolayers. J Nutr. 1998 Mar;128(3):577-81.
6. Dalessandri KM, Firestone GL, Fitch MD, Bradlow HL, Bjeldanes LF. Pilot study: effect of 3,3'-diindolylmethane
supplements on urinary hormone metabolites in postmenopausal women with a history of early-stage breast cancer. Nutr
Cancer. 2004;50(2):161-7.
7. Jellinck PH, Makin HL, Sepkovic DW, Bradlow HL. Influence of indole carbinols and growth hormone on the metabolism
of 4-androstenedione by rat liver microsomes. J Steroid Biochem Mol Biol. 1993 Dec;46(6):791-8.
8. Yoshida M, Katashima S, Ando J, Tanaka T, Uematsu F, Nakae D, Maekawa A. Dietary indole-3-carbinol promotes
endometrial adenocarcinoma development in rats initiated with N-ethyl-N'- nitro-N-nitrosoguanidine, with induction of
cytochrome P450s in the liver and consequent modulation of estrogen metabolism. Carcinogenesis. 2004 Nov;25(11):2257-
64. Epub 2004 Jul 7.
9. Shertzer HG, Sainsbury M. Intrinsic acute toxicity and hepatic enzyme inducing properties of the chemoprotectants
indole-3-carbinol and 5,10-dihydroindeno[1,2-b]indole in mice. Food Chem Toxicol. 1991 Apr;29(4):237-42..
10. Hien T. Le, Charlene M. Schaldach, Gary L. Firestone, and Leonard F. Bjeldanes. Plant-derived 3,3_-Diindolylmethane
Is a Strong Androgen Antagonist in Human Prostate Cancer Cells. Journal of Biological Chemistry Vol. 278, No. 23, Issue of
June 6, pp. 21136-21145, 2003.
11. Nachshon-Kedmi M, Yannai S, Fares FA Induction of apoptosis in human prostate cancer cell line, PC3, by 3,3'-
diindolylmethane through the mitochondrial pathway. Br J Cancer. 2004 Oct 4;91(7):1358-63.
12. Wortelboer HM, van der Linden EC, de Kruif CA, Noordhoek J, Blaauboer BJ, van Bladeren PJ, Falke HE. Effects of
indole-3-carbinol on biotransformation enzymes in the rat: in vivo changes in liver and small intestinal mucosa in comparison
with primary hepatocyte cultures. Food Chem Toxicol. 1992 Jul;30(7):589-99.
MARINE FISH OIL
Several studies have recognized the significant benefits of omega-3 fatty acids in
reducing inflammation, including chronic joint swelling and autoimmune
ailments.1
66 patients with chronic joint inflammation wee assigned to take omega-3 fats
(130 mg/day) or a placebo. Patients taking fish oil found relief from joint
tenderness.2
Diets high in omega-6 fats (vegetable, sunflower, etc.) can lead to inflammation
and various health concerns.

MARINE FISH OIL
Omega-3 fats can help to counterbalance the ratio of omega-6 fatty acids and
reduce inflammatory components.3 A clinical trial recruited 50 subjects with
chronic joint inflammation and a diet high in omega-6 fats (<10 g/day) to take
omega-3 fish oil (40 mg/day). Patients taking fish oil found a decrease in joint
inflammation.4
Fish oil contains concentrated amounts of DHA, a vital component of
phospholipids that are abundant in the brain. Optimum amounts of DHA are
important, as a deficiency can lead to mental decline. Researchers found a six-
month administration

MARINE FISH OIL
Fish oil contains concentrated amounts of DHA, a vital component of
phospholipids that are abundant in the brain. Optimum amounts of DHA are
important, as a deficiency can lead to mental decline. A six-month administration
of fish oil (1.7 g DHA/day, 0.6 g EPA/day) among individuals experiencing a mild
cognitive decline improved brain function.5
The effects of fish oil on mental function have been examined in a long-term
observational study. Subjects born in 1936 had their cognitive abilities tested in
1947, then again in 2000-2001. Individuals that took fish oil over this duration of
time had less cognitive decline than those that did not supplement with fish oil.6
Omega-3’s can stimulate the sympathetic nervous system to alleviate mental
stress among men. By taking 7.2 g/day of fish oil, adrenal activity that elicits
mental stress was suppressed in male subjects.7

MARINE FISH OIL
Fish oil can aid cognitive development in children. Mothers (98 women) took fish
oil (2.2 g DHA/day, 1.1 g EPA/day) or a placebo during pregnancy. Researchers
assessed every child’s cognitive development at 2 ½ years old finding
administration of fish oil during pregnancy was beneficial to a child’s eye and
hand coordination.8
An extensive review of studies concerning the benefits of fish oil on
cardiovascular health suggests individuals with heart complications should take
fish oil to reduce health risks.

MARINE FISH OIL
One review recommends individuals take 1,000 mg of fish oil to decrease the
risk of cardiovascular ailments.9
Another review recommends 800 mg EPA/day and 1,000 mg DHA/day.10
Furthermore, taking 2,000 mg to 4,000 mg of fish oil/day can aid cholesterol
levels.11
The American Heart Association recommends one serving of fish per day for
individuals with cardiovascular ailments to receive beneficial omega-3 fatty acids.

MARINE FISH OIL One study examined the effects of omega-3 fatty acids on cardiovascular
function during exercise training. Elite athletes (25 Australian Rules footballers)
were recruited during a five-week training to take 6 g/day of DHA or a placebo.
The study found fish oil supplementation improved cardio function and
decreased cardio risk factors.12
C-reactive protein levels can be an indication of systemic inflammation, which
leads to cardiovascular ailments. Fish oil (1,000 mg/meal) has been found to
lower C-reactive protein levels, as 33 subjects taking 1,000 mg of omega-3s (960
mg/day of EPA, 600 mg/day of DHA) had a reduction in C-reactive protein
levels.13

MARINE FISH OIL
Several studies have recognized even modest doses of fish oil (250 mg/day of
EPA and DHA) can offer cardiovascular protection. Risk factors associated with
cardiovascular complications can be reduced by 36%.14
Research has indicated 4,000 mg of omega-3s can lower triglyceride levels by
30%.15 One such study reviewed the effects of fish oil on weight loss among 324
overweight
individuals (20 to 40 years old), finding fish oil decreased triglyceride levels by
30%.16

MARINE FISH OIL
More significantly, another study found that taking 4,000 mg (465 mg EPA, 375
mg DHA per capsule) of omega-3s each day can decrease triglyceride levels by
45%.17
Overall, fish oil has significant results on triglyceride levels and supplementation
is well-tolerated to work with conventional cholesterol therapies.18
A deficiency in DHA can lead to changes in behavior and mood. One study
observed the effects of DHA on mental stress by giving 41 students fish oil (1.5 –
1.8 g DHA/day) or a placebo from the beginning of the fall semester to the
middle of final exams. Results indicated norepinephrine concentrations
significantly decreased in the DHA group (-31%) suggesting DHA could alleviate
mental stress.19
Fish oil’s mood boosting benefits were reviewed in a twelve-week trial that
recruited patients with nervous system degeneration. Results indicated subjects
taking fish oil had improvement in their mood, as omega-3 levels increased in the
blood.20

MARINE FISH OIL
Fish oil supplementation may extend to alleviating headaches. One study
recruited 27 adolescents with chronic headaches to take fish oil for two months.
Subjects reported a significant improvement in headache frequency (87%),
duration (74%), and severity (83%), while taking fish oil.22
Dosage: 4 to 6 grams per day
May augment blood thinners
Discontinue 10 to 14 days prior to surgery

MARINE FISH OIL
1 Simopoulos, AP. Omega-3 fatty acids in inflammation and autoimmune diseases. J Am Coll Nutr. 2002 Dec; 21(6):495-505. 2 Kremer, JM, Lawrence, DA, Petrillo, GF, et al. Effects of high-dose fish oil on rheumatoid arthritis after stopping
nonsteroidal antiinflammatory drugs. Clinical and immune correlates. Arthritis Rheum. 1995 Aug; 38(8):1107-1114. 3 James, MJ, Cleland, LG. Dietary n-3 fatty acids and therapy for rheumatoid arthritis. Semin Arthritis Rheum. 1997 Oct;
27(2):85-97. 4 Volker, D, Fitzgerald, P, et al. Efficacy of fish oil concentrate in the treatment of rheumatoid arthritis. J Rheumatol. 2000
Oct; 27(10):2343-2346. 5 Freund-Levi, Y, Eriksdotter-Jonhagen, M, et al. Omega-3 fatty acid treatment in 174 patients with mild to moderate
Alzheimer disease: OmegAD study: a randomized double-blind trial. Arch Neurol. 2006 Oct; 63(10):1402-1408. 6 Whalley, LJ, Fox, HC, et al. Cognitive aging, childhood intelligence, and the use of food supplements: possible involvement
of n-3 fatty acids. Am J Clin Nutr. 2004 Dec; 80(6):1650-1657. 7 Delarue, J, Matzinger, O, et al. Fish oil prevents the adrenal activation elicited by mental stress in healthy men. Diabetes
Metab. 2003 Jun; 29(3):289-295. 8 Dunstan, JA, Simmer, K, et al. Cognitive assessment of children at age 2(1/2) years after maternal fish oil supplementation
in pregnancy: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2008 Jan; 93(1):F45-50. 9 Oh, R. Practical applications of fish oil (Omega-3 fatty acids) in primary care. J Am Board Fam Pract. 2005; 18(1):28-36. 10 Anand, RG, Alkadri, M, et al. The role of fish oil in arrhythmia prevention. J Cardiopulm Rehabil Prev. 2008; 28(2):92-98. 11 Covington, MB. Omega-3 fatty acids. Am Fam Physician. 2004 Jul; 70(1):133-140. 12 Buckley, JD, Burgess, S, et al. DHA-rich fish oil lowers heart rate during submaximal exercise in elite Australian Rules
footballers. J Sci Med Sport. 2008 Jun. 13 Bowden RG, Wilson RL, Deike E, Gentile M. Fish oil supplementation lowers C-reactive protein levels independent of
triglyceride reduction in patients with end-stage renal disease. Nutr Clin Pract. 2009;24(4):508-512. 14 Mozaffarian, D. Fish and n-3 fatty acids for the prevention of fatal coronary heart disease and sudden cardiac death. Am J
Clin Nutr. 2008 Jun; 87(6):1991S-1996S. 15 Skulas-Ray AC, West SG, Davidson MH, Kris-Etherton PM. Omega-3 fatty acid concentrates in the treatment of moderate
Hypertriglyceridemia. Expert Opin Pharmacother. 2008 May;9(7):1237-1248.

Krill Oil
Krill are the world's largest animal biomass. Krill Oil extracted from these shrimp-
like crustaceans contains many nutrients essential to living creatures. Krill Oil
contains three important phospholipids;
1. phosphatidylcholine
2. Phosphatidylinositol
3. phosphatidylethanolamine.
These phospholipids contain a high proportion of EPA and DHA, and resemble
human brain phospholipids

Krill Oil
The human brain contains the most phospholipid rich membranes in the body,
especially high in DHA for membrane fluidity. Krill Oil's phospholipids naturally
contain EPA and DHA, anti-inflammatory fatty acids that hold the membranes in
healthy balance against toxic,
oxidative, and inflammatory attack. As a matter of fact, the phospholipids are
bound to astaxanthin, known to cross the blood-brain barrier!
The phospholipids in Krill, including phosphatidylcholine, are natural emulsifiers,
they facilitate the digestion and absorption of the healthy lipids in Krill Oil. While
practically all choline supplements are derived from plant sources such as soy,
choline from Krill is animal based.
Krill Oil
Omega 3 Fatty Acids are known to be sensitive to oxidation, however because
nature provided Krill with many powerful antioxidants, Krill Oil is remarkably
stable.
In addition to its high omega 3 to omega 6 profile, Krill Oil contains a rich
network of antioxidants including Vitamin E, all trans retinol Vitamin A, beta
carotene and the carotenoid relatives, canthaxanthin and astaxanthin.
These antioxidants work synergistically with other bioactive compounds in Krill
Oil to support peak functioning of the brain, liver, skin, and other organs.
Astaxanthin was found to be extremely effective at quenching singlet oxygen
radicals in membranes.11

Krill Oil
A research study performed at Tufts University in Boston found that when
astaxanthin or canthaxanthin were added to rat liver
microsomes, these antioxidants greatly inhibited radical-initiated lipid
peroxidation, equal to that of alpha-tocopherol and to a greater extent than
beta-carotene.13
Astaxanthin has also been shown to protect LDL from oxidation.1

Krill Oil Studies consistently demonstrate that marine oil improves morning stiffness
and joint tenderness in patients with rheumatoid arthritis.
Researchers believe this therapeutic benefit stems from omega-3's ability to
reduce levels of prostaglandins and leukotrienes that aggravate the
inflammation associated with rheumatoid arthritis.5,6,7
In addition to rheumatoid arthritis, studies indicate omega-3 essential fatty
acids can improve other inflammatory diseases as well including :
1. Ulcerative Colitis
2. Crohn's disease
3. Eczema
4. Acne
5. Psoriasis
6. Asthma

Krill Oil
A double-blind, controlled, randomized trial on 70 women showed that Krill Oil
dramatically improved all emotional PMS symptoms including feeling
overwhelmed, anxiety, stress, irritability, and depression.
After 45 and 90 days the Krill Oil group on 2 g per day, had statistically
significant differences in both emotional and physical symptoms including
breast tenderness, joint pain and dysmenorrhea.
The fish oil group after 90 days only had statistically significant reduction in
weight gain, swelling and abdominal pain.14 Study subjects reported using
50% fewer analgesics on a dose of 2 Krill Oil gelcaps daily.

Krill Oil 1. Iwamaoto T. et al. Inhibition of low density lipoprotein oxidation by astaxanthin.. J Atheroscler Thromb 2000;7(4):216-22 (ISSN: 1340-3478)
National Institute of Health and Nutrition, Tokyo, Japan.
2. Stone NJ, Fish consumption, fish oil: lipids and coronary heart disease. Circulation. 1996;94, 2237-2340.
3. Von Schacky C, Prophylaxis of Atherosclerosis with marine Omega-3 fatty acids. A comprehensive strategy. Annals Internal Med 107, 890-899.
1987.
4. Seidelin Kn, Myrup B, and Fischer-Hansen B. N-3 fatty acids in adipose tissue and coronary artery disease are inversely correlated. Am J Clin Nutr
55, 1117-1119. 1992.
5. Kremer J, er al, Fish oil supplementation in active rheumatoid arthritis: A double blinded, controlled cross-over study. Ann Intern Med. 106, 497-
502, 1987.
6. Van der Temple H, et al, Effects of fish oil supplementation in rheumatoid arthritis. Annals of Rheum Dis 49, 76-80. 1990.
7. Sperling R, et al, Effects of dietary supplementation with marine fish oil on leukocyte lipid mediator generation and function in rheumatoid arthritis.
Art Rheum 30, 988-997. 1987.
8. Urakaze M, Hamazaki T, Soda Y, et al. Infusion of emulsified trieicosapentaenoyl-glycerol into rabbits - the effects on platelet aggregation,
polymorphonuclear leukocyte adhesion, and fatty acid composition in plasma and platelet phospholipids. Throm Res 1986 Dec 1:44-(5): 673-82.
9. Yamashita N. et al. Inhibition of natural killer cell activity of human lymphocytes by eicosapentaenoic acid. Biochm Biophys Res Commun 1986
Aug 14;138 (3):1058-67.
10. Ruggiero-Lopez D. et al. Comparative effects of dietary corn, fish and Krill oils on intestinal glycosylation. Biochem Mol Biol Int 1994
aug;33(5):1001-10.
11. Di Mascio P, Devasagayam TP, Kaiser S, Sies H. Carotenoids, tocopherols and thiols as biological singlet molecular oxygen quenchers. Biochem
Soc Trans. 1990 Dec;18(6):1054-6.
12. Cantrell A, McGarvey DJ, Truscott TG, Rancan F, Bohm F. Singlet oxygen quenching by dietary carotenoids in a model membrane environment.
Arch Biochem Biophys. 2003 Apr 1;412(1):47-54.
13. Palozza P, Krinsky NI. Astaxanthin and canthaxanthin are potent antioxidants in a membrane model. Arch Biochem Biophys. 1992
Sep;297(2):291-5. Department of Biochemistry, Tufts University School of Medicine, Boston, Massachusetts 02111-1837.
14. Sampalis, F., M.D, PhD. et al. Evaluation of the Effects of Neptune Krill Oil™ on the Management of Premenstrual Syndrome and Dysmenorrhea.
Altern Med Rev 2003;8(2)171-179.
15. Stone, NJ. Fish consumption, fish oil: lipids and coronary heart disease. Circulation 1996;94: 2337-2340.
16. Simopoulos, AP. Omega 3 fatty acids in health and disease and in growth and development. Am J Clin Nutr 1991;54: 438-463.
17. Saynor R., Verel D, Gillot T. The long term effect of dietary supplementation with fish lipid concentrate on serum lipids, bleeding time, platelets
and angina. Atherosclerosis; 1984;50: 3-10.
Prostate Supplements
1. Sal Palmetto 2. Pygeum 3. Nettle Root 4. Lycopene

Sal Palmetto
Saw Palmetto extract comes from Saw Palmetto plants that are native to the United
States.
It can inhibit 5 alpha reductase which converts testosterone into free testosterone.
Saw Palmetto is comparable to traditional prostate treatments and is well-tolerated
among individuals with prostate ailments.1
A randomized trial recruited 92 men with urinary tract ailments related to prostate
growth to take Saw Palmetto or a placebo, concluding Saw Palmetto may have
short-term effects in improving urinary function.2
A six-month treatment recruited 85 men with prostate ailments to take Saw Palmetto
or a placebo finding the herb improved urinary tract function.3
1Gordon AE, Shaughnessy AF. Saw Palmetto for prostate disorders. Am Fam Physician. 2003 Mar 15; 67(6):1281-1283. 2Shi R, Xie Q, Gang X, et al. Effect of Saw Palmetto soft gel capsule on lower urinary tract symptoms associated with benign prostatic hyperplasia: a
randomized trial in Shanghai, China. J Urol. 2008 Feb; 179(2):610-615. 3Gerber GS, Kuznetsov D, Johnson BC, Burstein JD. Randomized, double-blind, placebo-controlled trial of Saw Palmetto in men with lower urinary tract
symptoms. Urology. 2001 Dec; 58(6):960-964; discussion 964-965.

Lycopene
Lycopene shows promising results in maintaining prostate health in several in
vitro, animal, and clinical trials.1,2,3
A meta-analysis of lycopene’s benefits on prostate health found that greater
lycopene intake was associated with healthy prostate function.4
A case-control study reviewed the relationship between antioxidant serum levels
and normal prostate function among healthy men. After thirteen years, a follow-up
included 578 men that had developed prostate ailments. Results indicated that
low lycopene levels had a significant association with the development of
abnormal prostate function.9
1 Dahan K, Fennal M, Kumar NB. Lycopene in the prevention of prostate cancer. J Soc Integr Oncol. 2008 Winter; 6(1):29-36.
2 Fraser ML, Lee AH, Binns CW. Lycopene and prostate cancer: emerging evidence. Expert Rev Anticancer Ther. 2005 Oct; 5(5):847-854.
3 Miller EC, Giovannucci E, Erdman JW Jr, et al. Tomato products, lycopene, and prostate cancer risk. Urol Clin North Am. 2002 Feb; 29(1):83-93.
4 Giovannucci E, Rimm EB, Liu Y, et al. A prospective study of tomato products, lycopene, and prostate cancer risk. J Natl Cancer Inst. 2002 Mar 6;
94(5):391-398.
9 Gann PH, Ma J, Giovannucci E, et al. Lower prostate cancer risk in men with elevated plasma lycopene levels: results of a prospective analysis.
Cancer Res. 1999 Mar 15; 59(6):1225-1230
Pygeum
A native evergreen tree that grows in South Africa, Pygeum africanum extract contains active constituents, including phytosterols (β-sitosterol, β-sitosteryl glucoside, and β-sitosterone) that benefit prostate health.
Pygeum has been shown to inhibit the growth of abnormal cells and proteins related to an inflamed prostate.1
Due to the significant increase of the annual harvest in the last decade trade in its bark has been added to Appendix II of the Convention Trade in Endangered Species (CITES). A meta-analysis reviewed studies on Pygeum and prostate health from 1966 to 2000. The review found that men taking Pygeum were twice as likely to report a reduction in symptoms related to an enlarged prostate, such as obstructed urinary tract function.2\
A two-month treatment with Pygeum extract showed improvement in urinary flow among men (50-75 years old) with enlarged prostate symptoms.3
Pygeum
Another study compared the dosage of Pygeum extract, 50 mg/twice daily to 100
mg/once daily, among 209 patients with prostate inflammation. Results indicated
both doses of Pygeum extract were equally effective and safe for
supplementation.4
One study reviewed androgen receptor activity that is associated with prostate
growth. Results indicated Pygeum was effective in inhibiting excessive androgen
activity.5
An in vitro study observed the effects of Pygeum on human prostate cells finding
the extract inhibited the proliferation of abnormal cells.6
1Shenouda NS, Sakla MS, Newton LG, et al. Phytosterol Pygeum africanum regulates prostate cancer in vitro and in vivo. Endocrine. 2007 Feb;
31(1):72-81. 2Wilt T, Ishani A, Mac Donald R, et al. Pygeum africanum for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002; (1):CD001044. 3Breza J, Dzurny O, Borowka A, et al. Efficacy and acceptability of tadenan (Pygeum africanum extract) in the treatment of benign prostatic
hyperplasia (BPH): a multicentre trial in central Europe. Curr Med Res Opin. 1998; 14(3):127-139. 4 Chatelain C, Autet W, Brackman F. Comparison of once and twice daily dosage forms of Pygeum africanum extract in patients with benign
prostatic hyperplasia: a randomized, double-blind study, with long-term open label extension. Urology. 1999 Sep; 54(3):473-478. 5 Schleich S, Papaioannou M, Baniahmad A, Matusch R. Extracts from Pygeum africanum and other ethnobotanical species with antiandrogenic
activity. Planta Med. 2006 Jul; 72(9):807-813. 6 Santa María Margalef A, Paciucci Barzanti R, Reventós Puigjaner J, et al. Antimitogenic effect of Pygeum africanum extracts on human prostatic
cancer cell lines and explants from benign prostatic hyperplasia. Arch Esp Urol. 2003 May; 56(4):369-378.

Nettle Root/Urtica dioica
Stinging Nettle has anti-inflammatory properties that benefit prostate health and
improve urinary flow.
A six-month study found that Stinging Nettle improved urinary tract function in 232
patients with inflamed prostate and urinary flow obstruction.1
A 96-week study of 219 subjects with urinary tract ailments took a Stinging
Nettle/sabal fruit combination or a placebo. Results indicated that urinary flow
improved among subjects taking the Stinging Nettle formulation.2
In patients with prostate ailments, Stinging Nettle significantly inhibited enzymatic
activity that leads to excessive cellular growth.3
Researchers have also found that the proliferation of abnormal prostate cells was
deterred by Stinging Nettle after seven days of treatment.4

Nettle Root/Urtica dioica
An animal study found Stinging Nettle reduced an enlarged prostate by 33.8% in
mice.5 The same researchers extended their study to human prostate cells finding
Stinging Nettle inhibited the excessive proliferation of prostate cells.6
An animal study found Stinging Nettle reduced an enlarged prostate by 33.8% in
mice.5 The same researchers extended their study to human prostate cells finding
Stinging Nettle inhibited the excessive proliferation of prostate cells.6
1 Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover
study. J Herb Pharmacother. 2005; 5(4):1-11. 2 Lopatkin N, Sivkov A, Schläfke S, et al. Efficacy and safety of a combination of Sabal and Urtica extract in lower urinary tract symptoms--long-term
follow-up of a placebo-controlled, double-blind, multicenter trial. Int Urol Nephrol. 2007; 39(4):1137-1146. 3 Durak I, Biri H, Devrim E, et al. Aqueous extract of Urtica dioica makes significant inhibition on adenosine deaminase activity in prostate tissue from
patients with prostate cancer. Cancer Biol Ther. 2004 Sep; 3(9):855-857. 4 Konrad L, Müller HH, Lenz C, et al. Antiproliferative effect on human prostate cancer cells by a Stinging Nettle root (Urtica dioica) extract. Planta
Med. 2000 Feb; 66(1):44-47. 5Lichius JJ, Renneberg H, Blaschek W, et al. The inhibiting effects of components of Stinging Nettle roots on experimentally induced prostatic
hyperplasia in mice. Planta Med. 1999 Oct; 65(7):666-668. 6Lichius JJ, Lenz C, Lindemann P, et al. Antiproliferative effect of a polysaccharide fraction of a 20% methanolic extract of stinging nettle roots upon
epithelial cells of the human prostate (LNCaP). Pharmazie. 1999 Oct; 54(10):768-771.

Nettle Root/Urtica dioica
1 Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind,
placebo-controlled, crossover study. J Herb Pharmacother. 2005; 5(4):1-11. 2Lopatkin N, Sivkov A, Schläfke S, et al. Efficacy and safety of a combination of Sabal and Urtica extract in lower urinary
tract symptoms--long-term follow-up of a placebo-controlled, double-blind, multicenter trial. Int Urol Nephrol. 2007;
39(4):1137-1146. 3 Durak I, Biri H, Devrim E, et al. Aqueous extract of Urtica dioica makes significant inhibition on adenosine deaminase
activity in prostate tissue from patients with prostate cancer. Cancer Biol Ther. 2004 Sep; 3(9):855-857. 4 Konrad L, Müller HH, Lenz C, et al. Antiproliferative effect on human prostate cancer cells by a Stinging Nettle root
(Urtica dioica) extract. Planta Med. 2000 Feb; 66(1):44-47. 5 Lichius JJ, Renneberg H, Blaschek W, et al. The inhibiting effects of components of Stinging Nettle roots on
experimentally induced prostatic hyperplasia in mice. Planta Med. 1999 Oct; 65(7):666-668. 6 Lichius JJ, Lenz C, Lindemann P, et al. Antiproliferative effect of a polysaccharide fraction of a 20% methanolic extract
of stinging nettle roots upon epithelial cells of the human prostate (LNCaP). Pharmazie. 1999 Oct; 54(10):768-771.

Cinnamon
Cinnamon is a small tree grown in India, Sri Lanka, and Brazil, and is one of the
oldest known spices. One teaspoon of cinnamon contains a healthy dose of
manganese, calcium, fiber, and iron. This potent spice provides many health
benefits such as: aiding digestion, improving circulation, increasing energy, and
regulating blood sugar.6
Cinnamon extract was administered to overweight patients in a water-soluble
form to determine the effects on blood sugar and body composition.
Researchers found that cinnamon significantly improved body composition and
glucose levels. It was suggested that cinnamon may decrease insulin and
cardiovascular risks associated with weight problems.7

Cinnamon
A group of researchers studied the effects of cinnamon extract on blood sugar levels after
eating a meal. Healthy subjects were recruited to consume rice pudding with or without
cinnamon. Subjects that consumed the rice pudding (300 mg) and cinnamon (6 mg) had a
lower glucose response, then subjects that did not consume cinnamon.8
A six-week study found that cinnamon extract improved glucose and insulin levels in mice
with blood sugar ailments. Researchers suggested that these effects could be associated
with cinnamon’s ability to suppress high glucose levels and slow the absorption of
carbohydrates in the small intestine.9 Additionally, cinnamon extract was administered to
rats fed a high-fructose diet for three weeks. Results indicated that cinnamon extract
improved insulin regulation, when compared to the placebo group. Researchers
suggested cinnamon extract could enhance insulin signaling to stabilize blood sugar.10
7 Ziegenfuss TN, Hofheins JE, Mendel RW, Landis J, Anderson RA. Effects of a water-soluble cinnamon extract on body composition and
features of the metabolic syndrome in pre-diabetic men and women. J Int Soc Sports Nutr. 2006; 3:45-53. 8 Hlebowicz J, Darwiche G, Bjorgell O, Almer LO. Effect of cinnamon on postprandial blood glucose, gastric emptying, and satiety in healthy
subjects. American Journal of Clinical Nutrition. 2007; 85(6):1552-1556. 9 Hyun, H., Hyun, S. H., & Choung, S. Y. Anti-diabetic effect of cinnamon extract on blood glucose in db/db mice Journal of Ethnopharmacology,
2006; 104(1/2):119-123. 10 Qin B, Nagasaki M, Ren M, Bajotto G, Oshida Y, Sato Y. Cinnamon extract prevents the insulin resistance induced by a high-fructose diet.
Horm Metab Res. 2004; 36(2):119-125.

Effectiveness of Cinnamon for Lowering Hemoglobin A1C in Patients with
Type 2 Diabetes: A Randomized, Controlled Trial
Paul Crawford, MD
Purpose: Multiple trials in the past have shown conflicting results of whether cinnamon lowers glucose
or hemoglobin A1C (HbA1C). The purpose of this study was to determine whether cinnamon lowers
HbA1C in patients with type 2 diabetes. I performed a randomized, controlled trial to evaluate whether
daily cinnamon plus usual care versus usual care alone lowers HbA1c.
Methods: I randomized 109 type 2 diabetics (HbA1C >7.0) from 3 primary care clinics caring for
pediatric, adult, and geriatric patients at a United States military base. Participants were randomly allocated
to either usual care with management changes by their primary care physician or usual care with
management changes plus cinnamon capsules, 1g daily for 90 days. HbA1c was drawn at baseline and
90 days and compared with intention-to-treat analysis. This study was approved by an institutional review
board.
Results: Cinnamon lowered HbA1C 0.83% (95% CI, 0.46 –1.20) compared with usual care alone lowering
HbA1C 0.37% (95% CI, 0.15– 0.59).
Conclusions: Taking cinnamon could be useful for lowering serum HbA1C in
type 2 diabetics with HbA1C >7.0 in addition to usual care.
(J Am Board Fam Med 2009;22:507–512.)

Alpha lipoic acid
ALA is a potent antioxidant for neutralizing free radicals and oxidative stress(1,2,)
A combination of ALA and acetyl-L-carnitine can restore mitochondrial function
and lessen the aging process by reducing oxidative stress.(3)
ALA can prevent free radical damage in the brain.(4)
ALA may be an effective aid in hindering neurodegenerative ailments.(5)
ALA has ability to scavenge lipid peroxidation, increase glutathione levels
(antioxidant in every human cell), and increase acetylcholine (an essential
nervous system messenger) to improve memory and concentration that declines
with age.(6)
ALA is a potential aid in hindering bone erosion caused by oxidative stress.(7)
ALA inhibits the formation of osteoclasts (bone-degrading cells) that are produced
in inflamed bone conditions.(8)

Alpha lipoic acid
ALA increases glutathione (a strong antioxidant) production to protect the eyes
from protein build up in the lens that causes blurred vision.(9)
75 mg/day of ALA for two months or 150 mg/day of ALA for one month could be
effective in protecting the optic nerve and stabilizing fluid pressure in the
eye.(10)
ALA improved insulin sensitivity in overweight adults after four weeks of
supplementation.(11)
ALA is also effective in reducing pain, numbness, tingling, burning sensations
associated with insulin resistance. A three-week, double blind study of 328
insulin resistant patients found ALA significantly reduced these negative nerve
effects.(12) A follow-up study found five-weeks of 600 mg/day of ALA oral
treatment was effective in reducing stabbing pain, numbness, and burning
among 181 insulin resistant patients.(13)
Alpha lipoic acid
100 mg of ALA protects the liver from injury associated with ischemia-reperfusion
(process of restoring blood circulation to blocked tissues or vessels).(14 )
In combination with Acetyl-L-Carnitine, an eight-week, double-blind study found
ALA can normalize blood pressure and vascular function by possibly reducing
oxidative stress in the mitochondria. Normal mitochondria function is needed for
optimal energy in the heart.(15)

Alpha lipoic acid
1 Ceriello, A. New insights on oxidative stress and diabetic complications may lead to a “causal” antioxidant therapy. Diabetes Care. 2003 May;
26(5):1589-1596.
2 Da Ros, R, Assaloni, R, Ceriello, A. Molecular targets of diabetic vascular complications and potential new drugs. Curr Drug Targets. 2005 Jun;
6(4):503-559.
3 Ames, BN, Liu, J. Delaying the mitochondrial decay of aging with acetylcarnitine. Ann NY Acad Sci. 2004 Nov; 1033:108-116.
4 Komeima, K, Rogers, BS, Lu, L, Campochiaro, PA. Antioxidants reduce cone cell death in a model of retinitis pigmentosa. Proc Natl Acad Sci.
2006 Jul 25; 103(30):11300-11305.
5 Packer, L, Tritschler, HJ, Wessel, K. Neuroprotection by the metabolic antioxidant alpha-lipoic acid. Free Radic Biol Med. 1997; 22(1-2):359-378.
6 Holmquist, L, Stuchbury, G, et al. Lipoic acid as a novel treatment for Alzheimer's disease and related dementias. Pharmacol Ther. 2007 Jan;
113(1):154-164.
7 Kim, HJ, Chang, EJ, Kim, HM, et al. Antioxidant alpha-lipoic acid inhibits osteoclast differentiation by reducing nuclear factor-kappaB DNA binding
and prevents in vivo bone resorption induced by receptor activator of nuclear factor-kappaB ligand and tumor necrosis factor-alpha. Free Radic Biol
Med. 2006 May; 40(9):1483-1493.
8 Ha, H, Lee, JH, Kim, HN, et al. Alpha-Lipoic acid inhibits inflammatory bone resorption by suppressing prostaglandin E2 synthesis. J Immunol.
2006 Jan; 176(1):111-117.
9 Maitra, I, Serbinova, E, Trischler, H, Packer, L. Alpha-lipoic acid prevents buthionine sulfoximine-induced cataract formation in newborn rats. Free
Radic Biol Med. 1995 Apr; 18(4): 823-829.
10 Filina, AA, Davydova, NG, Endrikhovskii, SN, Shamshinova, AM. Lipoic acid as a means of metabolic therapy of open-angle glaucoma. Vestn
Oftalmol. 1995 Oct; 111(4):6-8.
11 Kamenova, P. Improvement of insulin sensitivity in patients with type 2 diabetes mellitus after oral administration of alpha-lipoic acid. Hormones.
2006; 5(4):251-258.
12 Ziegler, D, Hanefeld, M, Ruhnau, KJ, et al. Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid. A 3-
week multicentre randomized controlled trial. Diabetologia. 1995 Dec; 38(12):1425-1433.
13 Ziegler, D, Ametov, A, Barinov, A, et al. Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial.
Diabetes Care. 2006 Nov; 29(11):2365-2370.
14 Dulundu, E, Ozel, Y, Toaloglu, U, et al. Alpha-lipoic acid protects against hepatic ischemia-reperfusion injury in rats. Pharmacology. 2007;
79(3):163-170.

Boswellia (Boswellia serrata)
118. Shah BA, Qazi GN, Taneja SC. Boswellic acids: a group of medicinally important compounds. Nat Prod Rep 2009;26:72-89.
119. Syrovets T, Buchele B, Krauss C, Laumonnier Y, Simmet T. Acetyl-boswellic acids inhibit lipopolysaccharide-mediated TNF-alpha induction in
monocytes by direct interaction with IkappaB kinases. J Immunol 2005;174:498-506.
122. Kimmatkar N, Thawani V, Hingorani L, Khiyani R. Efficacy and tolerability of Boswellia serrata extract in treatment of osteoarthritis of knee--a
randomized double blind placebo controlled trial. Phytomedicine 2003;10:3-7.
123. Sengupta K, Alluri KV, Satish AR, et al. A double blind, randomized, placebo controlled study of the efficacy and safety of 5-Loxin for treatment
of osteoarthritis of the knee. Arthritis Res Ther 2008;10:R85.
124. Gupta I, Parihar A, Malhotra P, et al. Effects of gum resin of Boswellia serrata in patients with chronic colitis. Planta Med 2001;67:391-5.
125. Gerhardt H, Seifert F, Buvari P, Vogelsang H, Repges R. [Therapy of active Crohn disease with Boswellia serrata extract H 15]. Z
Gastroenterol 2001;39:11-7. [Article in German; abstract in English]
126. Gupta I, Gupta V, Parihar A, et al. Effects of Boswellia serrata gum resin in patients with bronchial asthma: results of a double-blind, placebo-
controlled, 6-week clinical study. Eur J Med Res 1998;3:511-4.

Boswellia (Boswellia serrata)
Boswellia, also known as Indian frankincense, has long been recognized as an
herb with anti-inflammatory properties. The gum resin of boswellia contains
boswellic acids (BA), a group of pentacyclic triterpenoids that non-competitively
inhibit 5-LO activity.118
The most potent BA inhibitor of 5-LOX is 3-O-acetyl-11- keto-beta-boswellic acid
(AKBA). AKBA also downregulates TNFinduced gene expression and blocks the
activation and nuclear translocation of NF-B.118,119
Two separate double-blind, placebo-controlled studies have found administration of
boswellia extract significantly reduces
pain and stiffness and improves joint function in persons with clinically diagnosed
osteoarthritis of the knee.122,123
Clinical trials of boswellia extract involving patients with inflammatory bowel
disease and asthma have also reported symptomatic benefit.124-126

Boswellia (Boswellia serrata)
Function, pain and stiffness scores. Presented are the mean scores for (a) visual analog scale, (b) Lequesne's Functional Index, (c) Western Ontario
and McMaster Universities Osteoarthritis Index (WOMAC)-pain, (d) WOMAC-stiffness, and (e) WOMAC-functional ability in the low-dose (100 mg/day
5-Loxin®) and high-dose (250 mg/day 5-Loxin®) groups and placebo group at different time points, as indicated. Each bar represents mean
concentration ± standard deviation. In comparison with placebo, the change in scores in the treatment groups was tested for significance using
Turkey's multiple comparison test; asterisk indicates statistical significance.
Arthritis Res Ther. 2008; 10(4): R85.

Turmeric (Curcuma longa)
Turmeric has a long history of use in South and East Asian countries as both a
spice and a traditional remedy for liver ailments and inflammatory conditions.
The rhizomes of turmeric contain a number of compounds including curcuminoids
and sesquiterpenes that demonstrate antioxidant, hepatoprotective, hypoglycemic,
hypolipidemic, antiproliferative, and anti-inflammatory effects. (90-93)
Many of turmeric’s health benefits are attributed to its primary active constituent,
curcumin. This orange-yellow polyphenolic compound has been shown in vivo and
in vitro to exert a significant regulatory effect on molecular targets such as NF-_B,
TNF, COX-2, IL-1, IL-6, and a number of other inflammatory mediators.94

Tumeric (Curcuma longa)
Preliminary data from human studies indicate curcumin can favorably influence the
course of serious inflammatory conditions.
A double-blind, placebocontrolled trial was conducted to assess the effects of 2
gm/day of curcumin as an adjunct to sulfasalazine or mesalamine therapy in a
group of subjects with quiescent ulcerative colitis.
After six months, the rate of symptom recurrence in the curcumin group was
significantly lower than in the placebo group (4.65% vs 20.51%). Clinical and
endoscopic indices of disease activity were also significantly reduced by curcumin
in this study.95

Tumeric (Curcuma longa)
Despite turmeric’s therapeutic potential, its efficacy is somewhat limited by poor
bioavailability of its curcuminoid constituents.91 Recent advancements in
biotechnology have led to the development of phospholipid delivery systems that
dramatically improve the absorption of curcumin.96
Clinical trials have found curcumin-phospholipid complexes to be highly effective in
reducing symptoms associated with inflammatory conditions such as uveitis and
osteoarthritis of the knee.97-99
90. [No authors listed] Curcuma longa (turmeric). Monograph. Altern Med Rev 2001;6 Suppl:S62-6.
91. Anand P, Kunnumakkara AB, Newman RA, Aggarwal BB. Bioavailability of curcumin: problems and promises. Mol Pharm 2007;4:807-18.
92. El-Agamy DS. Comparative effects of curcumin and resveratrol on aflatoxin B(1)-induced liver injury in rats. Arch Toxicol 2010;84:389-96.
93. Gupta SK, Kumar B, Nag TC, et al. Curcumin prevents experimental diabetic retinopathy in rats through its hypoglycemic, antioxidant, and anti-
Inflammatory mechanisms. J Ocul Pharmacol Ther 2011 Feb 12. [Epub ahead of print]
94. Zhou H, Beevers CS, Huang S. The targets of curcumin. Curr Drug Targets 2011;12:332-47.
95. Hanai H, Iida T, Takeuchi K, et al. Curcumin maintenance therapy for ulcerative colitis: randomized, multicenter, double-blind, placebo-controlled trial.
Clin Gastroenterol Hepatol 2006;4:1502-6.
96. Marczylo TH, Verschoyle RD, Cooke DN, Morazzoni P, Steward WP, Gescher AJ. Comparison of systemic availability of curcumin with that of
curcumin formulated with phosphatidylcholine. Cancer Chemother Pharmacol 2007;60:171-7.
97. Allegri P, Mastromarino A, Neri P. Management of chronic anterior uveitis relapses: efficacy of oral phospholipidic curcumin treatment. Long-term
follow-up. Clin Ophthalmol 2010;4:1201-6.
98. Belcaro G, Cesarone MR, Dugall M, et al. Product-evaluation registry of Meriva®, a curcumin-phosphatidylcholine complex, for the complementary
management of osteoarthritis. Panminerva Med 2010;52(2 Suppl 1):55-62.
99. Appendino G, Belcaro G, Cesarone MR, et al. Efficacy and safety of Meriva, a curcuminphosphatidylcholine complex, during extended administration
in osteoarthritis patients. Altern Med Rev 2010;15:337-44.

Milk Thistle
Seeds of the dried milk thistle flower are rich in silymarin, a bioflavonoid
complex of three flavonolignins: silybin, silydianin, and silychristin.
Silymarin is responsible for milk thistle’s powerful protective and regenerative
activities in the liver.
Silymarin has been shown to support and enhance normal, healthy liver function
through three primary actions.
1. Binding to the outer cell membrane, preventing harmful toxins from entering
the cell.
2. Silymarin enhances levels of glutathione and superoxide dismutase,
3. Silymarin stimulates damaged liver cells to regenerate. In the cell nucleus,
silymarin augments the production ofmribosomes, stimulating protein
synthesis in the damaged cell resulting in expedited cell regeneration
Dose: 250 mgs/day

Milk Thistle
Gandon, JM, Brissot, P. Aminotransferase levels and silymarin inde novo tacrine-treated patients with Alzheimer's disease.
Dement Geriatr Cogn Disord 1999;10:181-5.
Bass, NM. Is there any use for nontraditional or alternative therapies in patients with chronic liver disease? [In Process
Citation]. Curr Gastroenterol Rep 1999;1:50-6.
Berkson, BM. A conservative triple antioxidant approach to the treatment of hepatitis C. Combination of alpha lipoic acid
(thioctic acid), silymarin, and selenium: three case histories. Med Klin 1999;94 Suppl 3:84-9.
Edwards, J, Grange, LL, Wang, M, Reyes, E. Fetoprotectivity of the flavanolignan compound siliphos against ethanol-
induced toxicity [In Process Citation]. Phytother Res 2000;14:517-21.
Farghali, H, Kamenikova, L, Hynie, S, Kmonickova, E. Silymarin effects on intracellular calcuim and cytotoxicity: a study in
perfused rat hepatocytes after oxidative stress injury. Pharmacol
Res 2000;41:231-7.
Flora, K, Hahn, M, Rosen, H, Benner, K. Milk thistle (Silybum marianum) for the therapy of liver disease [see comments].
Am J Gastroenterol 1998;93:139-43.
Kropacova, K, Misurova, E, Hakova, H. Protective and therapeutic effect of silymarin on the development of latent liver
damage. Radiats Biol Radioecol 1998;38:411-5.
Par, A, Roth, E, Rumi, G, Jr., Kovacs, Z, Nemes, J, Mozsik, G. [Oxidative stress and antioxidant defense in alcoholic liver
disease and chronic hepatitis C]. Orv Hetil 2000;141:1655-9.

Conjugated Linoleic Acid/CLA
CLA is known for its body weight management properties, which include
reducing body fat and increasing lean muscle mass.
Over 30 clinical studies have been published investigating the effect of CLA on
weight management. The trials have quite variable designs, which leads to
inconsistency. However a meta-analysis conducted in 2007 concluded CLA has
a small impact on fat mass. [1]
There are concerns that the use of CLA supplements by extremely
overweight people may tend to cause or to aggravate insulin resistance [2]

Conjugated Linoleic Acid/CLA
1 Whigham L et al. (January 2007). "Efficacy of conjugated linoleic acid for reducing fat mass:a meta-
analysis in humans". Am. J. Clin. Nutr. 85 (5): 1203–11.
2 Ulf Risérus, MMed; Samar Basu, PhD; Stefan Jovinge, MD, PhD; Gunilla Nordin Fredrikson, PhD; Johan
Ärnlöv, MD; Bengt Vessby, MD, PhD (September 2002). "Supplementation With Conjugated Linoleic Acid
Causes Isomer-Dependent Oxidative Stress and Elevated C-Reactive Protein". American Heart Association
Journals 106 (15): 1925–9.

Magnesium Orotate Magnesium is an essential mineral for calcium and potassium assimilation, nerve
and muscle impulses, enzyme reactions, heart muscle health, heart rhythm,
converting blood sugar into energy, assisting proper calcium, vitamin C, and
carbohydrate metabolism, formation of bone, and may be beneficial for anxiety,
depression, nervousness, heart disease and PMS.
Magnesium orotate is used by competitive athletes to increase endurance.
It is also used to treat symptoms of magnesium deficiency, including diabetes,
hypertension, dementia, and osteoporosis, and to treat migraines, asthma, chronic
lung disease, heart attacks, arrhythmias, blood vessel stiffness, atherosclerosis,
and high blood pressure.
Orotate salts, being neutrally charged, pass easily through cell membranes. In
effect, orotate ferries the mineral atoms into cells and tissues, producing higher
concentrations.
Dose: 500 – 1000 mgs/day

Magnesium Orotate
Recent research indicates that pharmacologic doses of oral magnesium may
improve endothelial function in individuals with cardiovascular disease.
A randomized double-blind, placebo-controlled trial in 50 men and women with
stable coronary artery disease found that six months of oral magnesium
supplementation (730 mg/day) resulted in a 12% improvement in flow-mediated
vasodilation compared to placebo (1).
Magnesium supplementation also resulted in increased exercise tolerance during
an exercise stress test compared to placebo. In another study of 42 patients with
coronary artery disease who were already taking low-dose aspirin (an inhibitor of
platelet aggregation), three months of oral magnesium supplementation (800-
1,200 mg/day) resulted in an average 35% reduction in platelet-dependent
thrombosis, a measure of the propensity of blood to clot (2).
Magnesium Orotate
Additionally, a recent study in 657 women participating in the Nurses' Health
Study reported that dietary magnesium intake was inversely associated with E-
selectin, a marker of endothelial dysfunction (3).
Cell culture studies have associated low magnesium concentrations with
endothelial dysfunction, namely inhibition of endothelial proliferation (4).
Although preliminary, these studies suggest that magnesium may be of benefit
in improving endothelial function in individuals with cardiovascular diseases.

Magnesium Orotate Magnesium depletion is commonly associated with both insulin dependent
(IDDM) and non-insulin dependent (NIDDM) diabetes mellitus.
Between 25% and 38% of diabetics have been found to have decreased
serum levels of magnesium (hypomagnesemia) (5).
Magnesium depletion has been shown to increase insulin resistance in a few
studies and may adversely affect blood glucose control in diabetes.
One study reported that dietary magnesium supplements (400 mg/day)
improved glucose tolerance in elderly individuals (6).

Magnesium Orotate
A randomized, double-blind, placebo-controlled study in 63 individuals with
type 2 diabetes and hypomagnesemia found that those taking an oral
magnesium chloride solution (2.5 g/day) for 16 weeks had improved
measures of insulin sensitivity and glycemic control compared to those
taking a placebo (7).
A small study in nine type 2 diabetic patients reported that supplemental
magnesium (300 mg/day for 30 days), in the form of a liquid, magnesium-
containing salt solution, improved fasting insulin levels but did not affect
fasting glucose levels (8).
A recent meta-analysis of nine randomized, double-blind, controlled trials
concluded that oral supplemental magnesium may lower fasting plasma
glucose levels in diabetic individuals (9).

Magnesium Orotate
1. Shechter M, Sharir M, Labrador MJ, Forrester J, Silver B, Bairey Merz CN. Oral magnesium
therapy improves endothelial function in patients with coronary artery disease. Circulation.
2000;102(19):2353-2358.
2. Shechter M, Merz CN, Paul-Labrador M, et al. Oral magnesium supplementation inhibits platelet-
dependent thrombosis in patients with coronary artery disease. Am J Cardiol. 1999;84(2):152-156.
3. Song Y, Li TY, van Dam RM, Manson JE, Hu FB. Magnesium intake and plasma concentrations of
markers of systemic inflammation and endothelial dysfunction in women. Am J Clin Nutr.
2007;85(4):1068-1074.
4. Maier JA, Malpuech-Brugere C, Zimowska W, Rayssiguier Y, Mazur A. Low magnesium promotes
endothelial cell dysfunction: implications for atherosclerosis, inflammation and thrombosis. Biochim
Biophys Acta. 2004;1689(1):13-21.

Magnesium Orotate
5. Tosiello L. Hypomagnesemia and diabetes mellitus. A review of clinical implications. Arch Intern
Med. 1996;156(11):1143-1148.
6. Paolisso G, Sgambato S, Gambardella A, et al. Daily magnesium supplements improve glucose
handling in elderly subjects. Am J Clin Nutr. 1992;55(6):1161-7.
7. Rodriguez-Moran M, Guerrero-Romero F. Oral magnesium supplementation improves insulin
sensitivity and metabolic control in type 2 diabetic subjects: a randomized double-blind controlled
trial. Diabetes Care. 2003;26(4):1147-1152.
8. Yokota K, Kato M, Lister F, et al. Clinical efficacy of magnesium supplementation in patients with
type 2 diabetes. J Am Coll Nutr. 2004;23(5):506S-509S.
9. Song Y, He K, Levitan EB, Manson JE, Liu S. Effects of oral magnesium supplementation on
glycaemic control in Type 2 diabetes: a meta-analysis of randomized double-blind controlled trials.
Diabet Med. 2006;23(10):1050-1056.

L-ARGININE
Effect of Oral L-arginine Supplementation on Blood Pressure
A Meta-analysis of Randomized, Double-blind, Placebo-controlled Trials
Jia-Yi Dong, BSc; Li-Qiang Qin, MD, PhD; Zengli Zhang, MD, PhD; Youyou Zhao, PhD; Junkuan Wang, PhD; Fabrizio
Arigoni, PhD; Weiguo Zhang, MD, PhD
Abstract and Background Previous studies suggest that L-arginine, an amino acid and a substrate of nitric oxide synthase,
may have blood pressure (BP)-lowering effect. Because some studies were performed with limited number of patients with
hypertension and therefore limited statistical power with sometimes inconsistent results, we aimed to examine the effect of
oral L-arginine supplementation on BP by conducting a meta-analysis of randomized, double-blind, placebo-controlled trials.
Methods PubMed, Cochrane Central Register of Controlled Trials, and the ClinicalTrials.gov databases were searched
through June 2011 to identify randomized, double-blind, placebo-controlled trials of oral L-arginine supplementation on BP in
humans. We also reviewed reference lists of obtained articles. Either a fixed-effects or, in the presence of heterogeneity, a
random-effects model was used to calculate the combined treatment effect.
Results We included 11 randomized, double-blind, placebo-controlled trials involving 387 participants with oral L-arginine
intervention ranging from 4 to 24 g/d. Compared with placebo, L-arginine intervention significantly lowered systolic BP by
5.39 mm Hg (95% CI −8.54 to −2.25, P = .001) and diastolic BP by 2.66 mm Hg (95% CI −3.77 to −1.54, P < .001).
Sensitivity analyses restricted to trials with a duration of 4 weeks or longer and to trials in which participants did not use
antihypertensive medications yielded similar results. Meta-regression analysis suggested an inverse, though insignificant (P =
.13), relation between baseline systolic BP and net change in systolic BP.
Conclusions This meta-analysis provides further evidence that oral L-arginine
supplementation significantly lowers both systolic and diastolic BP.
American Heart Journal. 2011;162(6):959-965

L-ARGININE Beneficial effects of a long-term oral L-arginine treatment added to a
hypocaloric diet and exercise training program in obese, insulin-resistant
type 2 diabetic patients
Pietro Lucotti,1 Emanuela Setola,1 Lucilla D. Monti,1 Elena Galluccio,2 Sabrina Costa,2 Emilia P. Sandoli,2 Isabella Fermo,3
Giovanni Rabaiotti,4 Roberto Gatti,4 and PierMarco Piatti1
1Diabetology, Endocrinology and Metabolic Disease Unit, 2Core Laboratory, Diabetology, Endocrinology and Metabolic
Disease Unit, 3Separative Technics Laboratory, and 4Rehabilitation and Functional Reeducation Division, Fondazione Centro
San Raffaele del Monte Tabor, Milan, Italy
ABSTRACT
Because chronic L-arginine supplementation improves insulin sensitivity and endothelial function in nonobese type 2 diabetic
patients, the aim of this study was to evaluate the effects of a long-term oral L-arginine therapy on adipose fat mass (FM) and
muscle free-fat mass (FFM) distribution, daily glucose levels, insulin sensitivity, endothelial function, oxidative stress, and
adipokine release in obese type 2 diabetic patients with insulin resistance who were treated with a combined period of
hypocaloric diet and exercise training. Thirty-three type 2 diabetic patients participated in a hypocaloric diet plus an exercise
training program for 21 days. Furthermore, they were divided into two groups in randomized order: the first group was also
treated with L-arginine (8.3 g/day), and the second group was treated with placebo. Although in the placebo group body
weight, waist circumference, daily glucose profiles, fructosamine, insulin, and homeostasis model assessment index
significantly decreased, L-arginine supplementation further decreased FM (P < 0.05) and waist circumference (P < 0.0001),
preserving FFM (P < 0.03), and improved mean daily glucose profiles (P < 0.0001) and fructosamine (P < 0.03). Moreover,
change in area under the curve of cGMP (second messenger of nitric oxide; P < 0.001), superoxide dismutase (index of
antioxidant capacity; P < 0.01), and adiponectin levels (P < 0.02) increased, whereas basal endothelin-1 levels (P < 0.01)
and leptin-to-adiponectin ratio (P < 0.05) decreased in the L-arginine group.
Long-term oral L-arginine treatment resulted in an additive effect compared with a diet and exercise training program alone
on glucose metabolism and insulin sensitivity. Furthermore, it improved endothelial function, oxidative stress,
and adipokine release in obese type 2 diabetic patients with insulin resistance.
American Journal of Physiology, Endocrinology and Metabolism AJP - Endo
November 2006 vol. 291 no. 5 E906-E912

L-ARGININE
Fig. 3. Relationship between mean systolic blood pressure and incremental areas for cGMP (A), ec-
SOD (B), and endothelin-1 (C) at the end of 21-day period with hypocaloric diet plus exercise
program (○) or associated with L-arginine supplementation ( ) in obese, insulin-resistant type 2
diabetic patients.
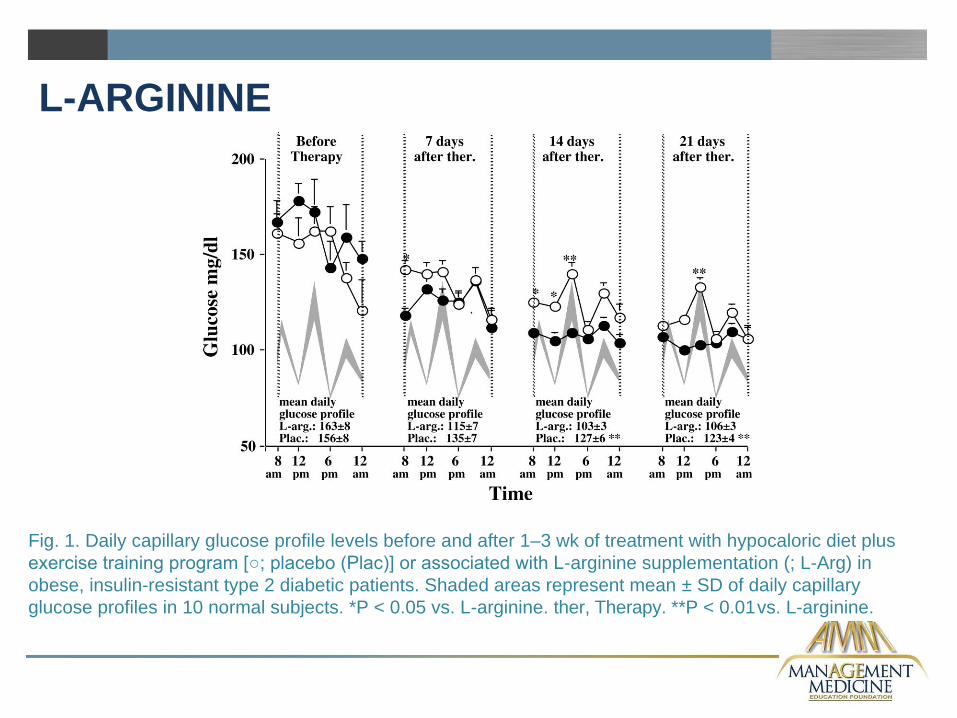
L-ARGININE
Fig. 1. Daily capillary glucose profile levels before and after 1–3 wk of treatment with hypocaloric diet plus
exercise training program [○; placebo (Plac)] or associated with L-arginine supplementation (; L-Arg) in
obese, insulin-resistant type 2 diabetic patients. Shaded areas represent mean ± SD of daily capillary
glucose profiles in 10 normal subjects. *P < 0.05 vs. L-arginine. ther, Therapy. **P < 0.01 vs. L-arginine.