
NHS Lambeth Draft Operating Plan 2012/13 Draft Lambe… · DRAFT NHS Lambeth Operating Plan 2012-13...
49
NHS Lambeth Draft Operating Plan 2012/13 Version 1 .0 27 Feb 2012
Transcript of NHS Lambeth Draft Operating Plan 2012/13 Draft Lambe… · DRAFT NHS Lambeth Operating Plan 2012-13...

NHS Lambeth
Draft Operating Plan 2012/13 Version 1 .0 27 Feb 2012

2
DRAFT NHS Lambeth Operating Plan 2012-13
NHS Lambeth
Version: 2.0 28_2_2012 MM
Key Contacts: Title Name Telephone Email
Clinical
Commissioning
Collaborative Chair:
Dr Adrian McLachlan 0203 049 4444 [email protected]
Managing
Director:
Andrew Eyres 0203 049 4444 [email protected]
Executive Lead
for operating planning:
Moira McGrath
Director of Care Pathway
Commissioning
0203 049 4481
Finance: Christine Caton
Chief Financial Officer
0203 049 4444 [email protected]
Workforce: Una Dalton
Director of HR and Corporate
Affairs
0203 049 4444 [email protected]
Performance: Emma Smith
Performance and
Information Manager
0203 049 4444 [email protected]
Engagement/ Sign off:
Supporting statement outlining process of consultation and engagement with stakeholders in development of Operating Plan for 2012-13.
Lambeth Clinical Commissioning Collaborative Board (LCCCB) is working as a sub-committee of Lambeth
Primary Care Trust with fully delegated responsibility for commissioning healthcare services for the
population of Lambeth and other patients registered with Lambeth GP practices.
The Operating Plan for 2012/13 builds on the work undertaken in the development of the NHS Lambeth
Commissioning Strategy Plan for 2012/13-2014/15: The development of clinical commissioning in
Lambeth has been a key means by which we have been able to enhance clinical involvement in the
development of our CSP refresh. While clinical design and involvement has always been part of our
strategic planning in Lambeth, through the leadership of the LCCCB we have increased the depth of
clinical involvement. As part of the development of the CSP we have undertook a series of clinical
discussions
31 August 2011
Lambeth & Southwark clinical leads meeting
3
Discussed high level priorities and possible joint QIPP
Attended by clinical commissioning board members from Lambeth & Southwark
14 October 2011
Informal LCCCB board seminar
Joint Strategic Needs Assessment (JSNA) refresh presented and discussed
Confirmed health improvement priorities and identified further areas for testing.
Attended by clinical board members.
5 October 2011
Formal LCCCB meeting
Progress update on Strategic Plan updating on areas identified for further work and agreed engagement
process.
Attended by clinical board members.
12 October 2011
Lambeth practice event
Half day workshop for practices to discuss Strategic Plan priorities and implementation. Discussions
helped shape our programmes of work.
Attended by representatives from 34 of our 52 practices.
7 Dec 2011
The LCCCB agreed the draft Commissioning Strategy Plan at its meeting in public
11 Jan 2012
LCCCB reviewed the NHS Operating Framework guidance and implications for Lambeth
31 Jan 2012
Lambeth Practice event
Half day workshop for practices to consider locality and practice development and information needs
Attended by representatives from 36 of our 52 practices.
1 Feb 2012
LCCCB reviewed the proposed content of the Operating Plan
7 March 2012
LCCCB reviewing first draft of Lambeth Operating Plan
4 April 2012
Final draft of Lambeth Operating Plan to be reviewed by LCCCB alongside SEL Plan
The development of the Strategic Plan had been informed by work within each of our 4 programmes :
Planned care, Unplanned care, Mental Health and Staying Healthy
Each of these programmes has a clinical lead from the clinical commissioning board. The memberships
include a range of clinical engagement including hospital consultants, nurses, AHPs, GPs, Practice nurses,
Pharmacists, Dentists and Optometrists, social workers, paramedics and voluntary sector providers. They
have been engaged in pathway redesign work to inform our priorities, QIPP assumptions and work
programmes.
Our programme boards include senior representatives from our local provider organisations (through

4
Lambeth & Southwark Urgent Care Network for Unplanned Care) who have been involved in developing
our plans as part of the CSP and in developing the Operating Plan. We presented our plan to Strategy
leads from Kings Health Partners in January 2012 in a joint session with NHs Southwark and ran 2
sessions to share our QIPP plans across Lambeth and Southwark to Kings and Guy’s & St Thomas in Dec
2011 and Jan 2012. The plans led by the Integrated Care Programme have been agreed by the multi
agency Programme Board representing all health and social care statutory organisations across Lambeth
and Southwark.
As part of the refresh of the CSP in 2011 we have undertaken a specific programme of engagement with
Lambeth residents, voluntary and community organisations and elected representatives involving a
discussion of ideas and principles of the Plan:
11 October 2011 partnership event with Lambeth LINk
Presentation and workshops on key aspects of the Strategic Plan. Feedback given on availability and
access to urgent care and primary care including pharmacies, staying healthy, outpatients, engagement
and communications.
20 October 2011 Health and Wellbeing Voluntary and Community Sector Forum
Question and answer session on the role of Lambeth clinical commissioning group, strategic priorities and
plans.
Feedback on older people and the Integrated Care Pilot, cancer services and screening, mental health and
diabetes. Discussion of co-creating principles across a wider range of care pathways.
16 November 2011 LINk Steering Group
Review of actions and input on the Strategic Plan
21 November 2011 Children’s Trust Board
Aligning approaches with the Children’s partnership
28 November 2011 Health & Wellbeing Partnership Workshop
Aligning the JSNA and the development of a health & wellbeing strategy across the partners working with
our communities.
7 December 2011 Lambeth Health and Adult Services Scrutiny Sub-Committee
Presentation of Strategic Plan to elected members of local authority
20 March 2012 Lambeth Health and Adult Services Scrutiny Sub-Committee
Paper on the Lambeth Operating Plan to be discussed
March 2012 (to be confirmed)
Proposed workshop with Lambeth LINk and voluntary sector on equality delivery scheme and Lambeth
plans
Patient and public participation plans for the workstreams described are in development and will be set
out in the April 2012 final version of the Operating Plan.
Dr Adrian
McLachlan, Chair of Lambeth Clinical
Commissioning Collaborative
Enter signature here

5
Section One: Strategic Overview NHS Lambeth has agreed health outcomes as p[art of ots 3 year Commissioning
Strategy Plan ‘Improving Health, Improving Quality’. These are set out on te next
page
In addition, as part of the process across South East London, Lambeth has
contributed to and agreed a series of goals:
Better for You – Our vision for 2015
More people In South East London will stay healthy, and every patient will
experience joined-up healthcare which meets their needs in the most effective
way.
South East London strategic goals – In South East London we commission physical and mental healthcare across
home, primary, community and acute settings from a variety of NHS, voluntary
and independent sector providers. In every case, our ambition is to meet the
same strategic goals, that:
1. In every contact with the NHS and local public service partners, people are
encouraged and enabled to positively manage their own health, in partnership
with health professionals and their carers.
2. Patients experience the NHS as a joined-up personalised service, rather than a
disconnected set of services they are required to navigate.
3. Patients are treated with dignity and the respect due to them at all times.
4. Clinical decision-making and healthcare delivery is in line with evidence-based
best practice and takes account of value for money.
5. The logistics of healthcare delivery, within and across different care settings,
are
designed to meet patient needs, whether long-term or acute, in the most
effective way.
More effective clinical decision-making and healthcare delivery logistics will drive
a significant increase in productivity and enable the health and social care system
in South East London to manage increasing levels of demand without an
equivalent increase in resources. We have set an ambitious target for our health
economy of productivity improvement to the value of £117m over four years.
Through monitoring execution of plan and the achievement of our strategic goals,
we will be able to ensure and demonstrate to our population that we have been
able to make savings without compromising our ambition, or patients’
expectations, for care quality.

6
NHS Lambeth Strategic Vision and Goals
Mission
Vision
Health
goals
Outcomes 2010-15 as
reviewed
To improve the health and reduce health inequalities of Lambeth people and to commission the highest quality health services on their behalf.
Health: Men will live 17 months longer and women 7 months longer; and the gap in life expectancy between most and least deprived will be reduced by 2 months Access: Comprehensive, round the clock access to integrated pathway based care, general and specialist; delivered through neighbourhood networks Affordability: A thriving, financially viable health economy delivering safe, effective, high quality care.
Cutting edge: Local services grounded in world class research, innovation and clinical education; in partnership with Kings Health Partners
Serious mental illness
Enable 1000 people with people with serious mental illness to move on from secondary care by accessing a new asset / recovery based service offer.
Cardio Vascular Disease
Improve hypertension control of 1000 more people in Lambeth
Diabetes
Help 5000 more people with diabetes bring their blood sugar under control
HIV
Halve the proportion of Lambeth residents diagnosed very late with HIV (<200 CD4 cells/mm3)
Smoking
Help over 12500 more people in Lambeth quit smoking
Childhood obesity
Help 900 more children overcome or avoid obesity; and help over 10000 children maintain a healthy weight
Life expectancy Health Inequalities Patient experience
98% users in CPA with
HONOS
76% of people with hypertension with BP <=
150/90
74.5% for
HbA1c <8
26% (2009) to
13% (by 2015)
1062 smoking quitters per
100,000
22.3% Year 6 obesity prevalence in
children
Alcohol (to be confirmed)
Increase the number of frontline staff who have received training in screening and brief intervention for alcohol misuse
90% of the identified frontline staff have received training in screening and brief intervention for alcohol
misuse

7
Overview of case for change
Lambeth is an inner London borough with a growing population. Key features include high relative
deprivation, population mobility, diversity and density. It has a breadth of ethnic and cultural traditions
which have established their presence in particular town centre areas and quarters. The census area
classifications describe Lambeth as a London Cosmopolitan area similar to Southwark, Lewisham,
Hackney, Islington, Haringey and Brent.
Population Key Facts
The resident population was estimated at 283,300 with projected growth by a further 15% to 317,000 by
2028. The General practice registered population is estimated at 370,000. There is an even split of
males / females. Lambeth has a much younger population than seen nationally with over 50% aged 20-
44. Approximately 37% of the population is from Black & Minority Ethnicity (BME) communities. About
80,000 residents are classified as Black African or Caribbean and the Black African population is projected
to increase till 2031. There are about 137 different first languages spoken by children in schools
Deprivation - Poverty and social exclusion are some of the social challenges in the borough. Lambeth is
the 9th most deprived borough in London in 2010. In England, Lambeth is the 29th most deprived.
Income deprivation is relatively worse in both older people and children compared to London and England
as a whole as shown below.
Deprivation index Lambeth London England
Income Deprivation
Affecting Older People
Index
37%
27%
21%
Income Deprivation
Affecting Children Index
38% 30% 20%
Source: IMD 2010
Health Status of Lambeth Population
Progress overall
Life expectancy – Overall NHS Lambeth is one of the few spearhead areas to have increased life
expectancy in both men and women as a result of reduced premature deaths from cardiovascular
diseases, cancers, infant deaths and other causes. Between 1995-97 and 2007-09 life expectancy at
birth increased
- for men by 4.7 years to 76.4 years
- for women by 2.7 years to 81.1 years
- Compared to England the gap in life expectancy has reduced in the same timeframe for both men (by
37%) and women (by 7%).
Infant mortality – Infant mortality (deaths of infants aged under 1 year) has reduced by 39% (from 8.8
per 1000 live births in 1995-97 to 5.4 per 1000 live births in 2007-09).
Premature deaths from circulatory diseases –A three-year average mortality rate for circulatory
diseases (< 75 years) has fallen by 49% since the baseline, from 175.3 deaths per 100,000 in 1995-97 to
90.2 in 2007-09. The absolute gap in mortality rates between England and Lambeth has reduced by 42%
from a baseline gap of 34 deaths per 100,000 in 1995-97 to 20 in 2007-09.
Premature deaths from cancer – The three year average premature mortality (< 75 years) from all
cancers has fallen by 15% from a baseline 161.8 per 100000 in 1995-97 to 137.9 per 100000 to 2007-
09. However for the latest period the overall absolute gap between Lambeth and England has worsened
by 25%.
Despite this progress in key areas the health burden and inequalities remains a challenge. The main
causes of death leading to the life expectancy gap are heart disease, stroke, cancer of the lung,
respiratory disease and peptic ulcers and liver cirrhosis. In addition to the mortality gap people in
Lambeth are living longer with one or more long term conditions. Mental illness forms the largest
component of this burden but people are also living longer with cardiovascular disease, cancers, and

8
chronic respiratory and digestive system disorders as survival improves. It is thus important to consider
early active case-detection, case management, medicine’s management and referral quality to avoid
unnecessary hospital admissions and improve quality of life. It is also important to consider end of life
care provision and support. People in Lambeth currently develop health conditions at a younger age and
live with these conditions for longer, often undetected until their condition is well advanced.
Key strategic priorities
Smoking
Lambeth has made good progress in reducing smoking prevalence with the development of a Lambeth
wide tobacco control strategy and sustained efforts to support smokers to quit. However smoking related
deaths and hospital admissions remain high and smoking remains an important priority for Lambeth.
Sexual Health
Lambeth has significant numbers of STIs diagnosed in local residents, high rates of teenage conceptions
and high rates of terminations. Therefore we have invested significantly in developing local services to
meet these needs. In the last five years we have made significant progress. Lambeth has the highest
Chlamydia screening uptake rates in England, has increased numbers of TOPs before 10 weeks gestation
and has introduced successful HIV testing pilots in primary care.
Teenage Conceptions
The under 18 conception rate is 59.5 per 1000 females aged 15-17 (267 conceptions). The under 18
conception rate has declined by 30.2% since 1998, the baseline and by 42.1% since 2003 when the rate
was at its highest. Lambeth has traditionally had one of the highest rates of under 18 conceptions.
However, data from 2009 shows that Lambeth has now the 11th highest rate in England
HIV
NHS Lambeth has identified HIV as a strategic priority. Lambeth Southwark and Lewisham have one of
the highest prevalence of HIV in the UK. Two main affected population groups are men having sex with
men (MSM), and black African heterosexuals. Late diagnosis of HIV is the most important factor
associated with HIV related morbidity and mortality and inpatient care in the UK. HIV testing is key to
reducing late diagnosis of HIV and in preventing secondary transmission. NHS Lambeth has set up an HIV
testing pilot in primary care and aims to expand this pilot to all practices.
Obesity, physical activity and healthy eating
The level of obesity in Lambeth adults (18.6%) is lower than the England average (23.6%) but is
worsening. Obesity in children aged 10-11 is high with up to 1 in 4 obese. 13.3% of children at reception
level are obese in Lambeth compared with 11% in London, and 9.9% in England.
Long Term Conditions
Diabetes
− Diabetes is a key strategic priority
− There are 13600 people with diabetes in Lambeth and the prevalence and numbers of detected cases
is increasing. Obesity is a major risk factor for type 2 diabetes.
− Key issues are the lower detection (see primary care services below) and the variation in
management of diabetes.
− NHS Lambeth is working with the Diabetes Modernisation Initiative to improve the detection and
management of diabetes.
− Early detection and reduced variation in the management and control of risk factors (secondary
prevention) remains an important challenge. Capacity to deal with the rising prevalence will also be
an important challenge.
Cardiovascular disease
− Cardiovascular disease is a key strategic priority
− There are just over 5000 detected cases of heart disease and over 3000 detected cases of stroke in
Lambeth. Other areas of importance in this condition include heart failure and heart arrhythmias
(particularly atrial fibrillation)
− Premature mortality is reducing significantly especially among men.
9
− Key issues are under detection and variation in the management and control of people with CVD.
− Early detection and reduced variation in the management and control of risk factors (secondary
prevention) remains an important challenge and in particular implementation of NHS Health checks
for early detection and management of risk.
Mental Health
Mental health is a key strategic priority in Lambeth for two reasons
- Mental ill health is the biggest cause of years of life lost to disability locally. It is also a leading
contributor to premature death in people with other long term conditions such as diabetes and
cardiovascular disease.
- The costs of disability due to mental ill health are very high, not only to the NHS and social care but
also to the wider economy and to families and individuals on a social level.
- Lambeth partners (including voluntary sector and service users and carers) are collaborating on a
substantial service redesign ‘the Lambeth Living Well Collaborative’ (LLWC) for people with severe
mental illness (SMI) which has been awarded £100k by NESTA as one of six pilot projects in their
People Powered Health Programme. The aim of the LLWC is to ‘change the rules’ about services and
use co-production to develop a culture where people receiving services are at the heart of strategic
direction and decision making as well as planning their own recovery.
Other key issues
Alcohol
Alcohol and substance misuse is an important problem in the borough. It is estimated that 23%-24% of
Lambeth’s population (~70,000) drink excessively and Lambeth has higher levels of alcohol-related
hospital admissions than both London and England.
Cancer
Cancer is a South East London wide priority and iLambeth works on this with the South London wide
Cancer Network. Cancer accounts for approximately 25% of deaths in Lambeth. Over the last decade
there has been a steady in decline in the rate of cancer death in those aged under 75 in line with the
national target with the exception of a rise in 2008. There is a focus on preventing premature death from
cancer.
The uptake of cervical, breast and colorectal screening is below the national average although improving
slowly. Initiatives to improve uptake, targeted at Primary Care, are planned.
Raising awareness of cancer and it’s early detection are priorities. Lambeth has had a number of
successful bids from the National Raising Awareness and Early Detection Initiative (NAEDI) and run a
social marketing campaign for head and neck cancer. Plans are being formulated for the national bowel
cancer campaign which will be launched in January 2012.
Priorities and Opportunities
Priority outcome
Latest performance (and date) Trajectory for 2012/13
Serious mental illness
Cardio Vascular Disease
Diabetes
HIV
Smoking
Childhood Obesity
Alcohol
To deliver against these target priorities within the resources available Lambeth has set up 4 programmes
of work:
• Integrated Care: Planned
• Integrated Care : Unplanned
10
These programmes are run jointly with NHS Southwark and are underpinned by the Integrated Care
Programme across NHS Lambeth, NHS Southwark, London Boroughs of Lambeth and Southwark and
Kings Health Partners
• Mental Health (linked to 4 borough commissioning approaches with Southwark, Lewisham and
Croydon and our partner London Boroughs)
• Staying Healthy (part of joint planning with London Borough of Lambeth)
Lambeth also works in the following commissioning partnerships:
Sexual Health (with Lewisham and Southwark)
Heart and Stroke (through the South London Cardiac and Stroke Network)
Cancer (through the South London Cancer Network)
Integrated Care: Planned Care
The Planned Care programme focuses on the development and delivery of an outpatient strategy to
reduce the risk of premature mortality and improve quality of life by:
• supporting patients to manage their own condition
• patient-centred care, with a shift in service provision along the care pathway, for identified
priorities, from treatment to prevention
• early detection of long term conditions (including HIV) to avoid preventable unplanned admissions
to hospital
• securing equity of access to services
• securing the quality and productivity in the management of elective condition and identifying the
most appropriate settings for support and treatment
• promoting appropriate referrals to specialist care
• reducing inappropriate variation in care
• reduce waiting times for patients for planned care
Our strategy will inform and be informed by work with local providers of care including Kings Health
partners. The strategy will include infrastructure planning across our three localities, including centres at
Akerman Road (due to open in July 2012) , Norwood Hall (due to open in 2013 subject to scheme
approval) and a review of Gracefield Gardens Neighbourhood Resource Centre. The programme will
oversee implementation of appropriate referral management processes. The programme is supported by
valuable resources from Guy’s & St Thomas’ Charity which funds the Diabetes Modernisation Initiative
across Lambeth and Southwark and has previously supported similar work in kidney care and sexual
health.
Key metrics for 2012/13
Outpatient referrals by source (GP/GDP/Consultant to consultant/other)
Numbers and waits for referral to treatment (RTT)
Outpatient attendances (first and follow up)
Diabetes HbA1c measures
Hypertension and cholesterol measures
Integrated care: Unplanned Care
The Unplanned Care Programme spans the organisational boundaries of acute, community, primary and
social care services to prevent avoidable hospital admission, support timely discharge and maximise
independent living by:
• Improving the quality of care and reducing the number of avoidable hospital admissions and
readmissions for frail older people
• Reducing the number of avoidable hospital admissions for conditions that can be managed in the
community by earlier identification and management of people at risk of admission
• Reduce avoidable readmissions to hospital
11
• Reduce A&E attendance by people whose conditions can be self-managed or supported by a
pharmacist, nurse or GP
• Support hospital A&E departments to reduce waiting times
• Reviewing the virtual hospital and rapid response services piloted during 2011/12 and links to
intermediate care
• Rolling out of the reablement programme
• Reducing the number of people dying in hospital who would prefer to die at home
• Improving cost effectiveness of care including continuing care and moving people into planned
care pathways and development of the 111 access point for unscheduled care
Key metrics for 1012/13:
A&E attendances
A&E waiting times
Emergency admissions and length of stay
Numbers of people dying in their place of choice
Ambulance conveyance times
Mental Health
The Mental Health Improvement Programme was formed in 2010-11 to take forward NHS Lambeth’s
strategic priorities for MH including delivery of QIPP. A multi agency programme board co-chaired by
LCCCB clinical commissioner is focused on five key priority areas as outlined below which fully support
delivery of No Health Without Mental Health (NHWMH) strategy and Operating Framework.
• Serious Mental Illness (SMI) service redesign based on co-production principles via the Lambeth
Living Well Collaborative
• Integration of talking therapy services
• Criminal justice/forensic service redesign
• Implementation of Payment by Results (PBR) and Self directed support
• Implementation of Lambeth dementia strategy.
a) SMI redesign via LLWC
The Collaborative aims to use “co-production” as the operating framework for the delivery and
commissioning of services and support provided for people with long term mental illness. It has
undertaken extensive engagement with users, carers and partners. This has resulted in broad agreement
on a much improved service offer which it is currently implementing. This includes building capacity
within primary care via the new primary care mental health support service (PASS); recovery focused
provision within the Voluntary sector via the Community Options service; a more responsive and easier to
navigate secondary care (SLaM) supported by CQUINs; extensive development of peer support networks
and the expansion of time banking across the borough. The overall aim is to support people to take
control over their lives through recovery orientated personalised care and support and reduce the
dependency on (especially) secondary care services that this a common feature of mental health systems
nationally as well as in Lambeth. The Collaborative is working toward developing integrated service
arrangements via the development of an Alliance Contract Framework across the whole system, i.e.
primary care, social care, secondary care and the Voluntary sector. Key to this will be system wide
workforce training and development to support the significant culture change required to support “co-
production” in the delivery of public services in with the ambitions set out by Lambeth’s Cooperative
Council initiative, of which the Collaborative is an early adopter project. Whilst initially focused on people
with long term mental illness the Collaborative is of the view that the approach taken is equally
applicable to all people with long term conditions and as such will be seeking to widen its scope in future.
b) Criminal justice and forensic services care pathway redesign
This project focuses on developing early intervention and diversion (where appropriate) to address the
high number of people with untreated mental illness (especially amongst the BME population) in the
criminal justice system. A new criminal justice mental health support service is due to start in January
2012 (funded by Guy’s and St Thomas’ Charity) targeting people in police custody and the courts.
Agreement has been reached with SLaM on a stepped reduction in low/med secure beds from 12-13
onwards supported through application of triage; improved case management including speedier

12
discharge and application of more flexible hospital/
c) Implementation of Payment by Results (PbR)
NHS Lambeth instigated and now facilitates the four borough/SLaM wide project group taking this work
forward. Key milestone shave been for 11/12 with implementation plans for the introductory year being
worked up. Allied to PbYR is the Self Directed Support/Personalisation workstream which will support
integrated health/social care packages . Lambeth is a Personal Health Budget pilot site for MH and is
currently processing 50 referrals with 11 people in receipt of budgets. It is expected this will be rolled out
further during 12-13.
d) Integrated talking therapies / counselling services
This project aims to improve access to, and the clinical effectiveness of, primary care talking therapies
commissioned by NHS Lambeth. An integrated talking therapy service specification has been developed
which covers the current IAPT (Improving Access to Psychological Therapy) and primary care counselling
services. As well as improving access, this will reduce fragmentation, duplication and overall cost. The
service is out to procurement and it is planned that a new contract for services will be in place from
August 2012.
e) Implementation of Dementia strategy
Service redesign aimed at supporting more effective community based services is the priority of the
Lambeth dementia strategy. It is planned to reduce the number of SLaM continuing care beds and
reinvest the savings to help more people remain in their own homes. Additional investment has been
targeted towards the expansion of the memory service, new day centre and the development of assisted
technology.
Key metrics for 2012/13:
Improving Access to Psychological Therapies (IAPT) performance
HONOS scores
Staying Healthy
People in Lambeth have relatively lower life expectancy than other areas in London and are a population
at higher risk of morbidity. The greatest contributors to premature mortality are cardiovascular disease
and cancer, which can be prevented by addressing some common risk factors through an integrated and
systematic approach.
The key objective of the Staying Healthy Programme is to improve health outcomes for Lambeth
residents through the commissioning of systematic health promotion and prevention services that have
the effect of improving mortality rates, reducing morbidity and reducing the prevalence of key risk
factors. The Programme aims are to:
• Reduce health inequalities and improve health, identifying the need for interventions that improve
population health such as environment (physical activity) nutrition, etc and linking these wider
determinants to the delivery and management of preventable Long Term Conditions
• Develop Tobacco control measures including increasing the numbers of people stopping smoking
• Promote sensible drinking including ensuring all first contact health professionals deliver brief
intervention training and support work in A&E
• Prevent infant mortality (e.g. screening, immunisation, maternal health, childhood poverty
strategy)
• Integrate approaches to addressing the needs in Early Years, including increasing capacity and
skills of Early Years workforce to ensure implementation of Healthy Child Programme
• Develop early intervention and prevention for adolescent health. To reduce risk-taking behaviour:
sexual health & teenage pregnancy, youth violence, substance misuse, emotional & mental well
being and obesity
• Wellbeing programme
Key metrics for 2012/13:
Smoking cessation
Childhood height and weight measures at reception & Y6

13
Immunisation rates
Breastfeeding rates
Vascular health checks
Sexual Health
Lambeth has some of the highest levels of sexual ill health nationally as indicated by the local HIV
prevalence and high rates of HIV late diagnosis and local teenage conception and repeat abortions rates.
Sexual Health Commissioning seeks to reduce health inequalities and barriers and increase service access
for the three main at risk target groups; Young people, BME communities and Gay Men / men who have
sex with men (MSM).
The following are Sexual Health & HIV priorities in the coming year
HIV -reduction of HIV late diagnosis
a) HIV Screening
• Ongoing expansion of HIV testing sites beyond 10 is planned although dependent on an evaluation
of the current pilot sites that have been in place since Jan 2010. An evaluation framework is in
development and will have been finalised by April 2012 with the planned completion of the
evaluation in Q1 12/13 with expansion to 10 additional sites in Q2 12/13 onwards
• Develop KPI for the core GP contract
• The ongoing development of communication and information sharing with the local population
through campaigns, publication and social networking - to be developed for 2012/13 as part of the
normalisation of HIV and to reduce HIV related stigma
• Expansion of Sexual Health in Practice (SHIP) training programme within 70% of the Lambeth
screening practices by Q3 2012/13. This programme has shown to be successful in Birmingham
and in improving HIV testing rates within the new patient registration cohorts but also for
delivering a high positive patient yield in targeted HIV screening following training. This training
would also provided a stronger foundation on which to build 'HIV shared care' models to maximise
the uptake of primary care services bp people living with HIV.
b) HIV care and support
HIV can now be managed as a long term treatable condition if diagnosed and treated early. Prevalence
rates in Lambeth are the highest nationally and this presents one of the highest risk areas in sexual
Health.The HIV care and support review completed in 2011 has provided a service model defining a long
term activity shift agenda, that will develop capacity within mainstream services and develop the
interface between HIV specialist services and primary care. The 3 month public consultation is completed
and the response drafted but the major milestones for 2012/13 are the development of a robust
implementation plan and defining of multiple projects of work that will drive re-design in care pathways
and release efficiencies to support the ongoing expansion of HIV testing. There will be a defined work
stream to focus on mental health & HIV and a phased shift activity out of the CASCAID.service into IAPT
services starting in 2012/13. Exact shift percentages are to be defined
c) Sexual Health tariff
To improve patient experience and service outcomes through the Implementation of the integrated
Sexual Health Tariff in year across Lambeth services. Work with providers to drive service re-design and
the optimal staff alignment according to tariff and to review the service landscape in year in relation to
the KHP agenda. Mitigate against service destabilisation throughout the implementation process.
d) HIV Prevention
Release savings from re-tender of the Pan London HIV prevention programme for re-tender in 2012/13
and through the re-tender of the African HIV prevention programme, ensure clearer linkages and
synergies between the regional and local provision and clearer linkages to HIV testing.
e) Strategy
Refresh of the Sexual Health & HIV Strategy in advance of transition to the London Borough of Lambeth

14
Primary Care
High quality primary care underpins the successful delivery of all of our plans for out of hospital care and
primary and community services transformation, being the foundation of each care pathway (e.g. safe
care, right care, end of life care, urgent and emergency care, long term conditions) and our vision for
integrated care networks. Our ambition is to achieve continuous improvements in quality, productivity,
patient experience and health outcomes of primary care and produce a legacy for our Pathfinders to build
upon.
Primary care contracting is led by one team across South East London working with LCCCB to improve the
quality and cost effectiveness of services.
To drive efficiency and productivity improvements we have commenced Primary Medical Services (PMS)
reviews for Lambeth with the aim of commissioning services to match the identified health needs of the
population through a core offering to be delivered by each practice.
There is a strong need for greater transparency of performance information. Using the London-wide List
Maintenance policy, we will ensure that all practices have accurate and validated registered lists. This will
enable monitoring of practices’ actual performance regarding, for example, immunisation levels,
screening coverage and prevalence levels of long term conditions. This information will feed into the pan-
London dashboard for quality outcomes and contract compliance that we will utilise to support improved
performance in 2012/13. We will continuously monitor contract performance and quality of services
delivered. The performance framework reviews on infection control, health and safety, business
continuity, child protection, employment checks and clinical governance domains. We will continue to,
proactively managing instances of poor performance in south east London, including the issue of breach
and remedial notices as required. Opportunities are being taken on retirement of practitioners to review
the current provision and to agree new arrangements such as list dispersal.
We will roll out EMIS Web (a GP practice information system) to practices across Lambeth which will allow
the delivery of the electronic transfer of patient records between GP practices, the uploading of the
summary care record and the next iteration of the electronic prescription service (EPS2). EPS2 will allow
patients to nominate their pharmacy for prescription pickup and assist practices in reducing repeat
prescription workload. Unplanned care in SEL London is provided through a complex network of services,
including primary and secondary care services. We have an opportunity to build upon existing services
and developments to ensure quality and value for money.
We aim to:
• Understand the current issues regarding the delivery of unplanned care both in and out of hours
• Understand what is driving demand
• Review how services are commissioned and develop best practice consistent approaches to support
future contractual arrangements, where appropriate
• Understand future changes and their impact, including but not exclusive to the implementation of 111
• Map potential duplication in provision of unscheduled care services within and across boroughs and
make recommendations for cost effective commissioning of services to future CCGs and the NHS National
Commissioning Board.
Milestones / Key Actions Achievement Date
See Appendix 1
15
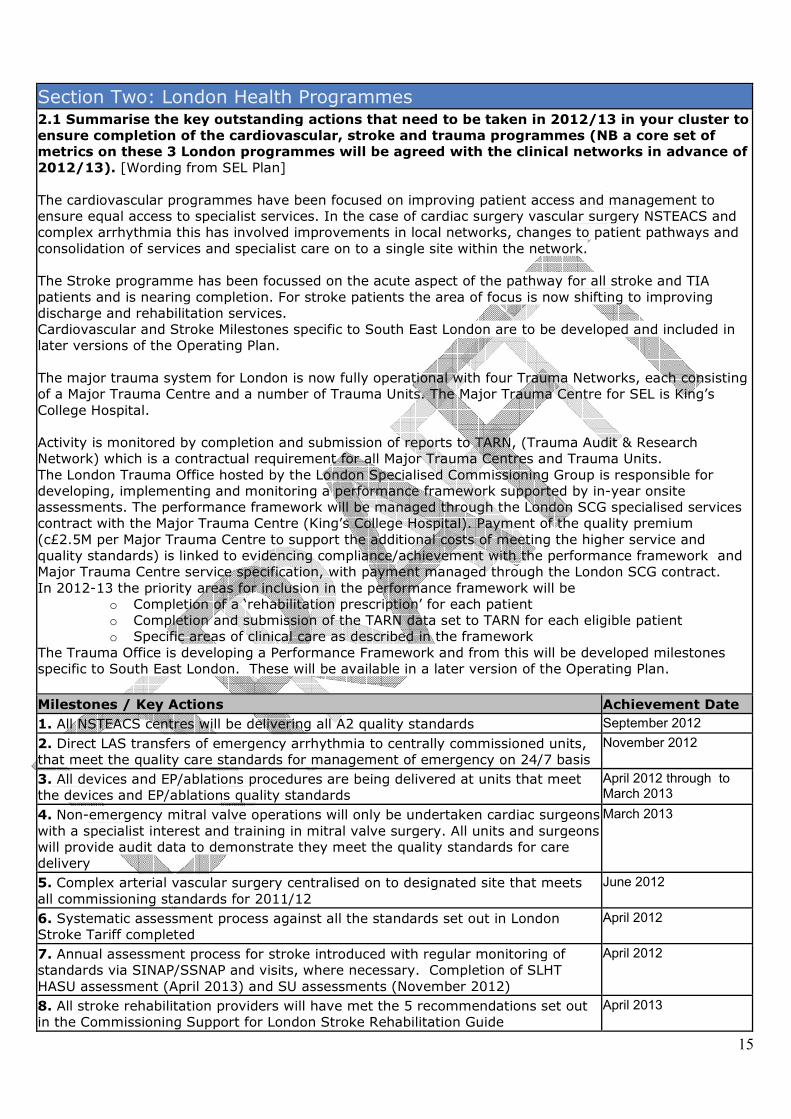
Section Two: London Health Programmes 2.1 Summarise the key outstanding actions that need to be taken in 2012/13 in your cluster to
ensure completion of the cardiovascular, stroke and trauma programmes (NB a core set of
metrics on these 3 London programmes will be agreed with the clinical networks in advance of
2012/13). [Wording from SEL Plan]
The cardiovascular programmes have been focused on improving patient access and management to
ensure equal access to specialist services. In the case of cardiac surgery vascular surgery NSTEACS and
complex arrhythmia this has involved improvements in local networks, changes to patient pathways and
consolidation of services and specialist care on to a single site within the network.
The Stroke programme has been focussed on the acute aspect of the pathway for all stroke and TIA
patients and is nearing completion. For stroke patients the area of focus is now shifting to improving
discharge and rehabilitation services.
Cardiovascular and Stroke Milestones specific to South East London are to be developed and included in
later versions of the Operating Plan.
The major trauma system for London is now fully operational with four Trauma Networks, each consisting
of a Major Trauma Centre and a number of Trauma Units. The Major Trauma Centre for SEL is King’s
College Hospital.
Activity is monitored by completion and submission of reports to TARN, (Trauma Audit & Research
Network) which is a contractual requirement for all Major Trauma Centres and Trauma Units.
The London Trauma Office hosted by the London Specialised Commissioning Group is responsible for
developing, implementing and monitoring a performance framework supported by in-year onsite
assessments. The performance framework will be managed through the London SCG specialised services
contract with the Major Trauma Centre (King’s College Hospital). Payment of the quality premium
(c£2.5M per Major Trauma Centre to support the additional costs of meeting the higher service and
quality standards) is linked to evidencing compliance/achievement with the performance framework and
Major Trauma Centre service specification, with payment managed through the London SCG contract.
In 2012-13 the priority areas for inclusion in the performance framework will be
o Completion of a ‘rehabilitation prescription’ for each patient
o Completion and submission of the TARN data set to TARN for each eligible patient
o Specific areas of clinical care as described in the framework
The Trauma Office is developing a Performance Framework and from this will be developed milestones
specific to South East London. These will be available in a later version of the Operating Plan.
Milestones / Key Actions Achievement Date
1. All NSTEACS centres will be delivering all A2 quality standards September 2012
2. Direct LAS transfers of emergency arrhythmia to centrally commissioned units,
that meet the quality care standards for management of emergency on 24/7 basis
November 2012
3. All devices and EP/ablations procedures are being delivered at units that meet
the devices and EP/ablations quality standards
April 2012 through to March 2013
4. Non-emergency mitral valve operations will only be undertaken cardiac surgeons
with a specialist interest and training in mitral valve surgery. All units and surgeons
will provide audit data to demonstrate they meet the quality standards for care
delivery
March 2013
5. Complex arterial vascular surgery centralised on to designated site that meets
all commissioning standards for 2011/12
June 2012
6. Systematic assessment process against all the standards set out in London
Stroke Tariff completed
April 2012
7. Annual assessment process for stroke introduced with regular monitoring of
standards via SINAP/SSNAP and visits, where necessary. Completion of SLHT
HASU assessment (April 2013) and SU assessments (November 2012)
April 2012
8. All stroke rehabilitation providers will have met the 5 recommendations set out
in the Commissioning Support for London Stroke Rehabilitation Guide
April 2013

16
9. ‘Life after stroke: commissioning guide’ - progress in implementing
recommendations in the Life after stroke: commissioning guide
April 2013
10. Improvements have been made to the cardiac surgery, vascular surgery,
NSTEACS and complex arrhythmia local networks, changes to patient pathways
and consolidation of services and specialist care on to a single site within the
network
April 2012
Section Three: Performance and Quality 3.1 Performance in 2011/12 against the Headline and Supporting Measures
During 2011/12 (based on April to December) where NHS Lambeth performed well against a
number of the acute performance measures, notably:
• PCT on target to meet the MRSA target
• Overall Cancer targets (2 week urgent referrals, 31 day referral to treatment, 31 day subsequent
chemotherapy, 62 day referral from screening)
• Access to stroke services
During 2011/12 (based on April to October) where NHS Lambeth performed well against a
number of the non acute performance measures, notably:
• Smoking quitters
• Breastfeeding (improvement in prevalence and coverage)
• Immunisations (improvement in update)
• NHS Health Checks (improved recording resulting in the target being exceeded)
• IAPT – Proportion of people with depression referred for and receiving psychological therapy.
• The number of new cases of psychosis served by early intervention teams.
• Access to dentistry
• Carers Breaks (plans and budgets in place to support carers)
In 2011/12 there have also been some acute areas which have performed below the expected
levels:
• A&E 4 hour waits (subject to conformation of Quarter 4 figures 2011/12)
• Referral to Treatment Times
• CDifficile (improving)
In 2011/12 there have also been some non acute areas which have performed below the
expected levels:
• Cervical screening Test results.
•
3.2 Summarise the Cluster's performance priorities and challenges for 2012/13:
Lambeth’s priorities and challenges for 2012/13 :
• Referral to Treatment – Guy’s & St Thomas’ current plan is to eliminate the admitted backlog by
quarter 2, 2012/3. The focus will be on sustaining a specialty level monthly performance. Both
trusts have made significant improvements in reducing the number of patients on incomplete
pathways and will continue to reduce these in 2012/13. They have also made significant inroads
in addressing diagnostics backlogs. The Cluster is working with trusts to establish a suitable level
of capacity to manage the increased in workload expected from the Bowel Cancer Awareness
Campaign and screening age extension.
• Emergency Access- NHS Lambeth is working through the Integrated Care Programme to develop
the following during 2012/13:
o Urgent (24/48 hour) access to holistic older people’s assessment on an outpatient basis at
St Thomas’ and Kings
o Developing registers at GP practice level of older people at risk of admission

17
o Annual holistic review of older people in primary care
o Commissioning community based urgent access provision for patients with COPD
In addition NHS Lambeth will be undertaking the following urgent care initiatives:
o Re-commissioning the urgent care centre at St Thomas’
o Commissioning the 111 unscheduled care service in partnership with other South East
London CCGs
o Commissioning diversion schemes from St Thomas’ including patient advisory and liaison
services and piloting diversion to local practices.
o Reviewing the 8am-8pm primary care service at Gracefield Gardens
o Developing further the ‘Choose Well campaign to support patients to make informed
choices about services they use
• The 2012/13 objectives for healthcare associated infection (HCAI) are challenging both at acute
trust and PCT level (hospital cases). Initial trajectories for delivering both MRSA and CDI
(clostridium difficile Infection) objectives have been set with acute trusts and BSUs. Following the
recently published guidance on CDI testing, the trajectories for CDI may be amended. The new
guidance proposes a dual testing process in acute trusts, similar to that already undertaken by
GSTT.
With the introduction of a new double testing regime for CDiff at GSTT in September 2010 more
cases are being detected than the originally set baseline. This is impacting on local targets and will
prove challenging during 2012/13. Lambeth’s CDiff target for 2012/13 is 73 and 4 for MRSA. Local
commissioners and public health leads and working together with Trusts to consider alternative
approaches to management and monitoring for 2012/13.
• 62 day urgent referrals to treatment – GST has made improvements in the urology pathway
earlier in the year and more recently in the pathway for Lower GI, particularly access to
colonoscopies through the use of the additional endoscopy capacity on the St Thomas’ site. Early
indications are that this has resulted in improved performance (Oct 2011). If this level of
performance is maintained then this performance threshold should not present an issue in
2012/13.
• Ambulance service CAT A emergency calls - key events that could impact upon performance in
2012/13 are as follows:
o Olympics – separate funding has been agreed with the DH in order to maintain business as
usual and includes funding for a expected general rise in activity.
o Other large events – Queen’s Jubilee, Public Demonstrations
o Implementation of 111 – ambulance activity could potentially rise while new providers bed
in.
o Further Industrial Action
Plans are already underway to mitigate against the risks identified above.
• Immunisation - Lambeth's priority for 12/13 is to improve performance in immunising hard to
reach children including those over the age of 5. A CQUIN is proposed in the 12/13 Provider
contract to ensure this targeted work is prioritised and supported and monitored effectively. A
new database, GPIUS will be used from March 2012 which will improve data quality and free up
health visitors to concentrate on improving performance. This includes engagement with primary
schools and early years providers to implement standardised collection of information on the
immunisation status of new entrants, exploring options for offering vaccinations to under-
vaccinated children, and identify opportunities to promote immunisation. A detailed Action plan
has been reviewed and amended for 12/13 onwards and implementation is overseen by the
Lambeth & Southwark childhood immunisation strategy group, which reports to the executive lead in each BSU. Targets remain at 90% for all childhood immunisations for 2012/13.
• Breast feeding - Although performance has improved there is still some way to go in 2012/13.
Lambeth is implementing improved ways of working including data collection by health visitors in
order to increase prevalence at 6-8 weeks, taking into account learning from colleagues in
Southwark where performance is good. Lambeth is undergoing the UNICEF Baby Friendly

18
Initiative (BFI) and is in the process of finalising the detailed action plan and community
breastfeeding policy which will be implemented in a range of community settings including
children Centres and GP practices. Lambeth is on track to receive the certificate of commitment
by April 2012 and will work towards Level 1 accreditation throughout 12/13. This will focus on
developing and implementing an effective multi-agency training strategy; reviewing all
breastfeeding policy and procedures in a range of community settings and developing and
implementing a communication strategy with parents. There is good governance for breastfeeding
with an operational group overseeing BFI implementation and a Lambeth Breastfeeding strategy
group established which is attended by the clinical commissioning lead. The target remain at 90% for breastfeeding prevalence and 95% for coverage.
• Smoking Quitters -In line with the 2012/13 Operating Framework Public Health Quality Smoking
Quitters performance measure, this area will be a priority moving forward. Lambeth made huge
progress during 2011/12 and exceeded Department of Health targets. Target performance will be
maintained during 2012/13 and a further local stretch target has been set. King's Health Partners
has developed a Stop Smoking Focus Group, which involves key stakeholders across the health
care community. The group is developing innovation that will enhance smoking cessation services
across Lambeth and Southwark. This proactive approach ensures there is the opportunity to focus
on individual cohorts of patients that historically have been difficult to engage. The 2012/13 target
for Lambeth is 1910 patients quitting at the 4 week stage.
• Cervical Screening Test Results - Lambeth performance on this target improved considerably
during 2011/12 Q3 reaching 99% in December, however performance has not always been
consistent and remains an area that requires ongoing attention. Guy's and St Thomas' Trust has
acknowledged that it has been understaffed in the laboratories and has provided a commitment to
staff up to sufficient levels to maintain the improvement in performance
• Bowel Screening - The bowel cancer national awareness which runs for 8 weeks from the end of
January will pose a risk to performance in 2012/13 as projected demand increases. The roll out of
the age extension for the Bowel Cancer Screening Programme was due to commence Q4 2011/12
however this will be delayed until Q1/2 2012/13 due to impact of national awareness programme.
Planning with the Acute Trusts to increase capacity has commenced and performance leads will
continue to work with the Cancer Screening Lead for South East London and the South East
London Cancer Network. Work streams have been identified and are currently being worked
through and the recently formed South East London Cancer Screening Board will be reviewing
performance and progress.
• Health Checks – Lambeth has exceeded targets for 2011/12 and will be embedding good practice
during 2012/13 in primary care and through targeting harder to reach people through the Lambeth
Early Intervention and Prevention services (LEIPS) Lambeth, Southwark and Lewisham have
developed a joint service specification, which will ensure more consistency of provision. A
comprehensive programme of evaluation will take place during 2012/13.
Milestones / Key Actions Achievement Date
See Appendix 2 (in development) to contain trajectories agreed for targets above:

19
Section Four: Priority areas Priority areas
To be inserted by
NHSL once Op
Framework is out
DH Requirement Delegation to
CCGs
(yes/no)?
Actions required to maintain or achieve requirement.
Please include key risks and mitigations.
Achievement
Date
Health
visitors/Family
Nurse
Partnerships
• Clusters to work towards delivering
provider-based 2012/13 trajectories due
to be issued by NHSL w/c 5th December.
This is in line with the Government
commitment of an additional 4200 by
April 2015.
• Maintain existing delivery and continue
expansion of the Family Nurse
Partnership programme in line with the
Government commitment to double
capacity to 13,000 places by April 2015.
(Section 2.13 of Operating Framework)
Based on the most recent trajectory from NHSL based on
the deprivation model, Lambeth is on course to meet the
target for number of staff in post as at April 2012 (42.2).
We are working closely with GSTT to ensure effective
recruitment & retention in subsequent years and have
identified funding to support this commissioning process for 2012/13.
Lambeth will be undergoing our FNP annual review in
Jan/Feb 2012. In line with recommendations from the
previous Southwark annual review we are establishing a
S&L Advisory Group to oversee key developments and
ensure continued delivery and expansion in line with the Government directive.
April 2013
Olympic-
Paralympic
Games-time
delivery
[SEL Plan
wording]
• Deliver business as usual performance
levels, whilst meeting any increase in
demand associated with the Games
(“Games Effect”) at Games-time.
• Meet the bid commitments by providing
LOCOG with the necessary ambulance and
paramedic resources at all LOCOG Events
and through the Designated Hospitals
(Non-designated hospitals if clinically
appropriate) providing free healthcare for
the accredited members of the Games
Family.
• Provide appropriate contingency for
health resilience at Games Time in
compliance with DH guidance as part of
A pan Cluster Olympics and Paralympics co-ordinating
group, chaired by the deputy CEO, was established in
Summer 2011. The approach is to focus on borough
working with pan-SEL co-ordination.
This group recognises that it is the Cluster’s role to co-
ordinate a system response to Games time planning across
SE London and it is working to the requirements and
timescales of the of the London wide games time delivery
group and overseeing the delivery of a comprehensive
project plan with six priority work streams :-
• Emergency planning and response
• Human resources and staffing
• Communications and engagement
• Readiness of Acute Hospital services
20
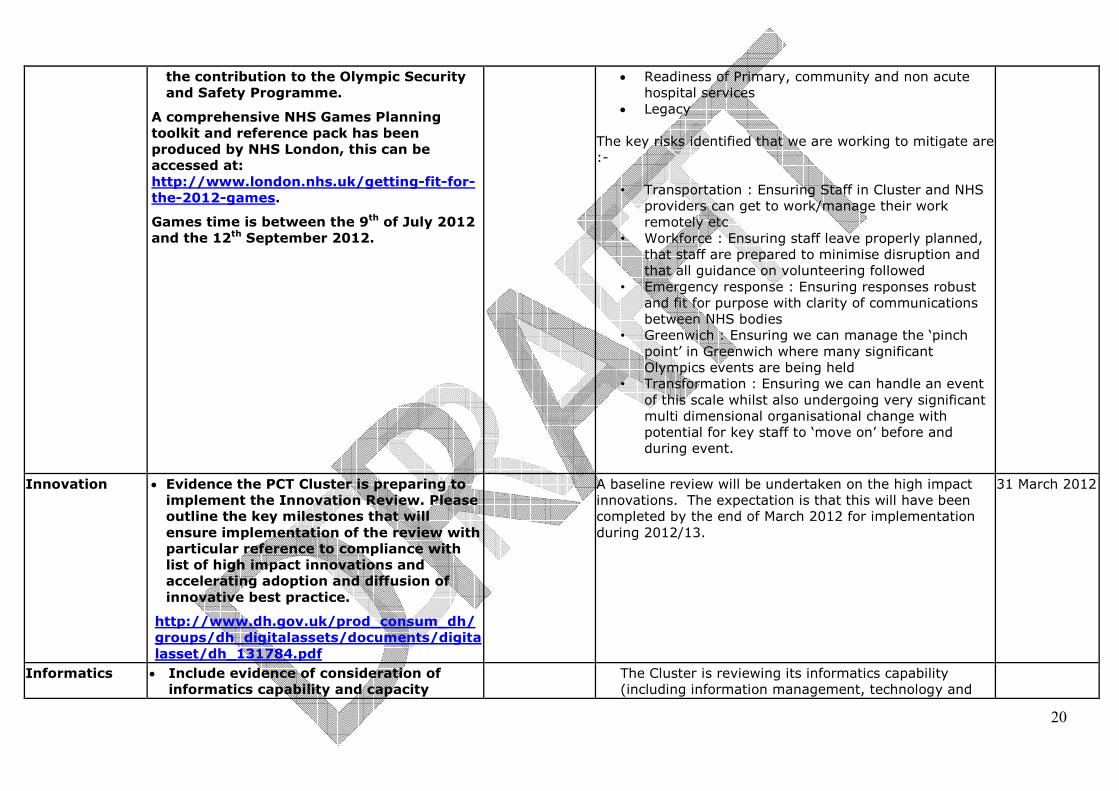
the contribution to the Olympic Security
and Safety Programme.
A comprehensive NHS Games Planning
toolkit and reference pack has been
produced by NHS London, this can be
accessed at:
http://www.london.nhs.uk/getting-fit-for-
the-2012-games.
Games time is between the 9th of July 2012
and the 12th September 2012.
• Readiness of Primary, community and non acute
hospital services
• Legacy
The key risks identified that we are working to mitigate are
:-
• Transportation : Ensuring Staff in Cluster and NHS
providers can get to work/manage their work
remotely etc
• Workforce : Ensuring staff leave properly planned,
that staff are prepared to minimise disruption and
that all guidance on volunteering followed
• Emergency response : Ensuring responses robust
and fit for purpose with clarity of communications
between NHS bodies
• Greenwich : Ensuring we can manage the ‘pinch
point’ in Greenwich where many significant
Olympics events are being held
• Transformation : Ensuring we can handle an event
of this scale whilst also undergoing very significant
multi dimensional organisational change with
potential for key staff to ‘move on’ before and
during event.
Innovation
• Evidence the PCT Cluster is preparing to
implement the Innovation Review. Please
outline the key milestones that will
ensure implementation of the review with
particular reference to compliance with
list of high impact innovations and
accelerating adoption and diffusion of
innovative best practice.
http://www.dh.gov.uk/prod_consum_dh/
groups/dh_digitalassets/documents/digita
lasset/dh_131784.pdf
A baseline review will be undertaken on the high impact
innovations. The expectation is that this will have been
completed by the end of March 2012 for implementation
during 2012/13.
31 March 2012
Informatics
• Include evidence of consideration of
informatics capability and capacity
The Cluster is reviewing its informatics capability
(including information management, technology and

21
[SEL Plan
wording]
necessary to support the transition.
• Include a credible proposal for giving
patients on-line access to their medical
records, starting with their GP records.
• Provide an achievable trajectory for
providing Summary Care Records by
March 2013 to all residents who have
been written to.
(Section 3.26 of Operating Framework)
governance) to ensure that it remains fit for purpose
for current and emerging organisations. The Cluster
Management Board is responsible for considering
informatics capacity and capability, and considering
proposals for strengthening this key service area. The
South London Commissioning Support Service
programme will oversee the specific development of a
capable informatics service to support emerging
Clinical Commissioning Groups. This programme will
also oversee the provision of ICT services to a range of
other third parties, such as the South East London
health Protection Unit, to assure service provision
through 2012/13 and beyond. The ICT service will
dovetail with Estates services to ensure collaboration
and the development of complementary strategies.
The Primary Care Directorate are working with primary
care contractors, emerging Clinical Commissioning
Groups and the LMC to ensure that giving access for
patients to their GP records, and moving forwards to
their full medical record, is considered a key priority.
The ICT function is and will continue to engage with
clinical system providers to ensure that a) the technical
capability is in place across all GP practices within
South East London, and b) that a deployment plan will
be created in partnership with GPs and patients to
ensure that access is granted in line with national,
regional and locally agreed timetables. Progress in
delivering this capability will be overseen by the
Cluster’s ICT Steering Group, supported by a Primary
Care ICT Programme Board.
There are 267 practices of which 114 practices have
uploaded SCR covering 768,000 patients (41%). SEL
has a project board set up to oversee SCR which meets
monthly to review progress against plans. Resource
has been authorised to deploy SCR to LSL-G has the
necessary required staff allocated to deliver EMIS Web
and SCR with dedicated project managers, clinical
22
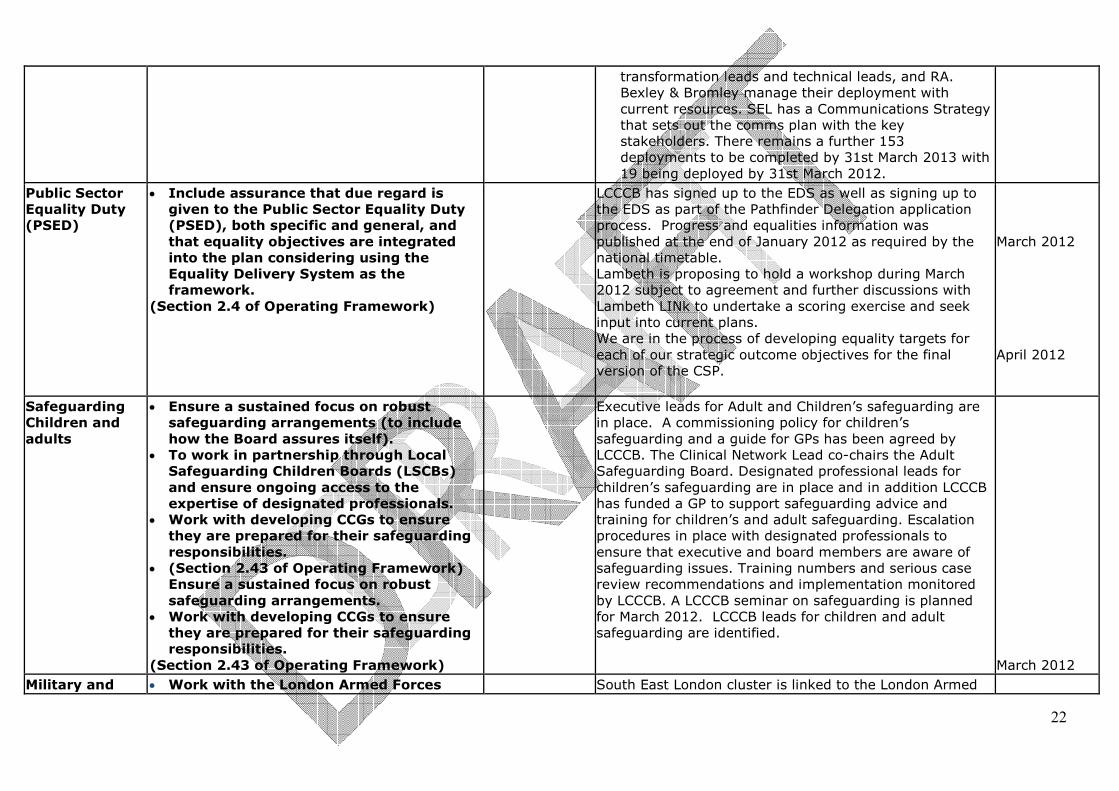
transformation leads and technical leads, and RA.
Bexley & Bromley manage their deployment with
current resources. SEL has a Communications Strategy
that sets out the comms plan with the key
stakeholders. There remains a further 153
deployments to be completed by 31st March 2013 with
19 being deployed by 31st March 2012.
Public Sector
Equality Duty
(PSED)
• Include assurance that due regard is
given to the Public Sector Equality Duty
(PSED), both specific and general, and
that equality objectives are integrated
into the plan considering using the
Equality Delivery System as the
framework.
(Section 2.4 of Operating Framework)
LCCCB has signed up to the EDS as well as signing up to
the EDS as part of the Pathfinder Delegation application
process. Progress and equalities information was
published at the end of January 2012 as required by the
national timetable.
Lambeth is proposing to hold a workshop during March
2012 subject to agreement and further discussions with
Lambeth LINk to undertake a scoring exercise and seek
input into current plans.
We are in the process of developing equality targets for
each of our strategic outcome objectives for the final
version of the CSP.
March 2012
April 2012
Safeguarding
Children and
adults
• Ensure a sustained focus on robust
safeguarding arrangements (to include
how the Board assures itself).
• To work in partnership through Local
Safeguarding Children Boards (LSCBs)
and ensure ongoing access to the
expertise of designated professionals.
• Work with developing CCGs to ensure
they are prepared for their safeguarding
responsibilities.
• (Section 2.43 of Operating Framework)
Ensure a sustained focus on robust
safeguarding arrangements.
• Work with developing CCGs to ensure
they are prepared for their safeguarding
responsibilities.
(Section 2.43 of Operating Framework)
Executive leads for Adult and Children’s safeguarding are
in place. A commissioning policy for children’s
safeguarding and a guide for GPs has been agreed by
LCCCB. The Clinical Network Lead co-chairs the Adult
Safeguarding Board. Designated professional leads for
children’s safeguarding are in place and in addition LCCCB
has funded a GP to support safeguarding advice and
training for children’s and adult safeguarding. Escalation
procedures in place with designated professionals to
ensure that executive and board members are aware of
safeguarding issues. Training numbers and serious case
review recommendations and implementation monitored
by LCCCB. A LCCCB seminar on safeguarding is planned
for March 2012. LCCCB leads for children and adult
safeguarding are identified.
March 2012
Military and • Work with the London Armed Forces South East London cluster is linked to the London Armed

23
veterans’
health
[SEL plan
wording]
Network to ensure the principles of the
Armed Forces Network Covenant are met
for the armed forces, their families and
veterans.
• Ensure that the Ministry of Defence/NHS
Transition Protocol for those who have
been seriously injured in the course of
their duty is implemented in any
commissioned service.
• PCT Clusters, and organisations they
commission from, should be supportive
towards those staff who volunteer for
reserve duties.
(Section 2.12 of Operating Framework)
Forces Network which has four key work programmes on
veterans community mental health, reservist terms &
conditions, primary care engagement and access for
veterans to NHS care.
Mental health
• Continue to meet expectations within No
Health Without Mental Health and NHS
Outcomes Framework.
• IAPT to meet 15% prevalence with
recovery rate of at least 50%.
• Focus needed on minority groups, older
people, people with serious mental
illness and long term conditions.
• Reduction of mortality from physical
illness in those with mental illness.
• Focus on joint working with National
Offender Management Service.
• Focus on mental health prevention in
looked after children and other young
people at risk.
• QIPP achievement monitored against MH
Performance Framework covering new
cases of psychosis served by EIT,
gatekeeping of acute admissions by crisis
teams, 7-day post discharge follow up for
those on CPA.
• Elimination of mixed sex accommodation
(Section 2.23 of Operating Framework)
• Minority groups – Lambeth’s various initiatives are
addressing needs of minority groups as outlined
here
• Mortality – CQUIN physical health targets are being
met by SLaM ; the improved primary care and
secondary care interface through the primary care
mental health support service will further sustain
improvements in this key target area.
• Offender health - NHS Lambeth works with NOMS
and other criminal justice agencies in a number of
ways. The re-role of HMP Brixton is being
undertaken in a planned, collaborative way with the
Prison, the providers, NHS Wandsworth (in relation
to HMP Wandsworth transfers) and NOMS to ensure
a smooth transition for patient health care. NHS
Lambeth is involved in development and operation
of the Integrated Offender Management (IOM)
programme in Lambeth. The Lambeth MHIP
Criminal Justice Pathway project (as above)
involves the entire criminal justice pathway, per the
Bradley Report, including prisons and Probation.
• Looked After Children (LAC) - range of Tier 2 and
Tier 3 community services in place for 2012/2013,
including a LAC CAMH Service (CLAMHS), YOS

24
CAMH Service and an integrated Early Intervention
Service. Implementation of CAMHS IAPT service in
Lambeth is in process, which will be integrated with
existing parenting programmes.
• QIPP Key performance targets - CPA, HONOS, EI
and HTT are being met together with MH QIPP
savings target
• SLaM continue to comply with the Mixed sex
accommodation policy with no breaches during
2011-12
Carers
• Publication by 30 September 2012 of
Local Authority and PCT Cluster joint
needs assessment with agreed plans
policies and identified budgets with Local
Authorities and voluntary groups to
support carers.
• To include identification of total budget
to support carers breaks and indicative
number of breaks available within the
budget.
(Section 2.11 of Operating Framework)
Following the publication of the Refreshed National Carers
Strategy, the Lambeth Carers Strategy was refreshed in
2011. The Refreshed Lambeth Carers Strategy which took
into consideration the needs of carers outlined agreed
plans and identified budgets to support carers till the end
of the financial year 2012/2013 including the number of
available breaks. The Carers Strategy is a joint LB
Lambeth/NHS Lambeth document.
A major piece of work is currently being carried out to
review all forms of respite provision for carers in Lambeth.
The intended outcome is to develop policy proposals
leading to new models of care, direct payment for carers
and ensuring investment equity for carers of all types.
Dementia and
care of older
people
• Ensure providers are compliant with NICE
quality standards and information
published in provider quality accounts.
• Work with GPs to ensure improvements
in general practice and community
services including improvement of
diagnostic rates.
• Ensure participation in and publication of
national clinical audits.
• Outline initiatives to reduce inappropriate
antipsychotic prescribing.
• Continued drive to eliminate Mixed Sex
Providers are required to comply with NICE quality
standards and to publish as part of Quality Accounts as
part of our contractual requirements We will continue to
monitor this through a well established process of quality
outcome review meetings and challenging providers to
improve quality and improve efficiency.
We are seeking to improve participation in national audit
and would hope to confirm a programme of participation in
national audits over the coming year.
We propose that participation in national clinical audit
should form part of contractual requirements for 2012/13.
It is part of the national Quality Accounts template.

25
Accommodation. Reporting of
inappropriate admission rates.
• Non payment for emergency
readmissions within 30 days of discharge
from elective admission.
(Section 2.08 of Operating Framework)
The Lambeth & Southwark Dementia workplan will ensure
Lambeth and Southwark participate in and publish results
of national clinical audits.
To participate in NHS London Primary Care Audit on use of
antipsychotic medication
To develop and implement an action plan following
outcome of audit working with local GPs, specialist mental
health services, voluntary and third sector providers.
To continue to raise awareness of dementia amongst
health and social care workers
To monitor the impact of the Southwark and Lambeth
Memory Service.
To analyse referral by GP practice targeting those who
refer fewer than expected numbers of patients
To improve awareness and diagnosis of dementia for
people in acute hospital setting by the implementation and
monitoring of National Dementia CQUIN across all sectors
of care
Local mental health services are compliant with privacy
and dignity requirements and elimination of mixed sex
accommodation. Any breach in same sex accommodation
requirements is received in the reporting data from
providers and monitored through the course of our
contract monitoring arrangements.
We have agreed proposals in 2011/12 contracts for non
payment for emergency readmissions within 30 days of
discharge from elective admissions and propose a similar
agreement for 2012/13 with commensurate re-investment
in schemes to prevent inappropriate readmission.
TBC
Action plan in
place by (TBC)
Implemented
by end March
2013
Ongoing
Ongoing
CQUIN to be in
place by end
March 2012
Implementatio
n 2012/13
Any Qualified
Provider
• Extend patient choice of community and
mental health services to AQP in 3
service lines per Cluster between April
Arrangements for Any Qualified Provider are being taken
forward by NHS South East London. An Implementation
Group has been established to cover the three areas which
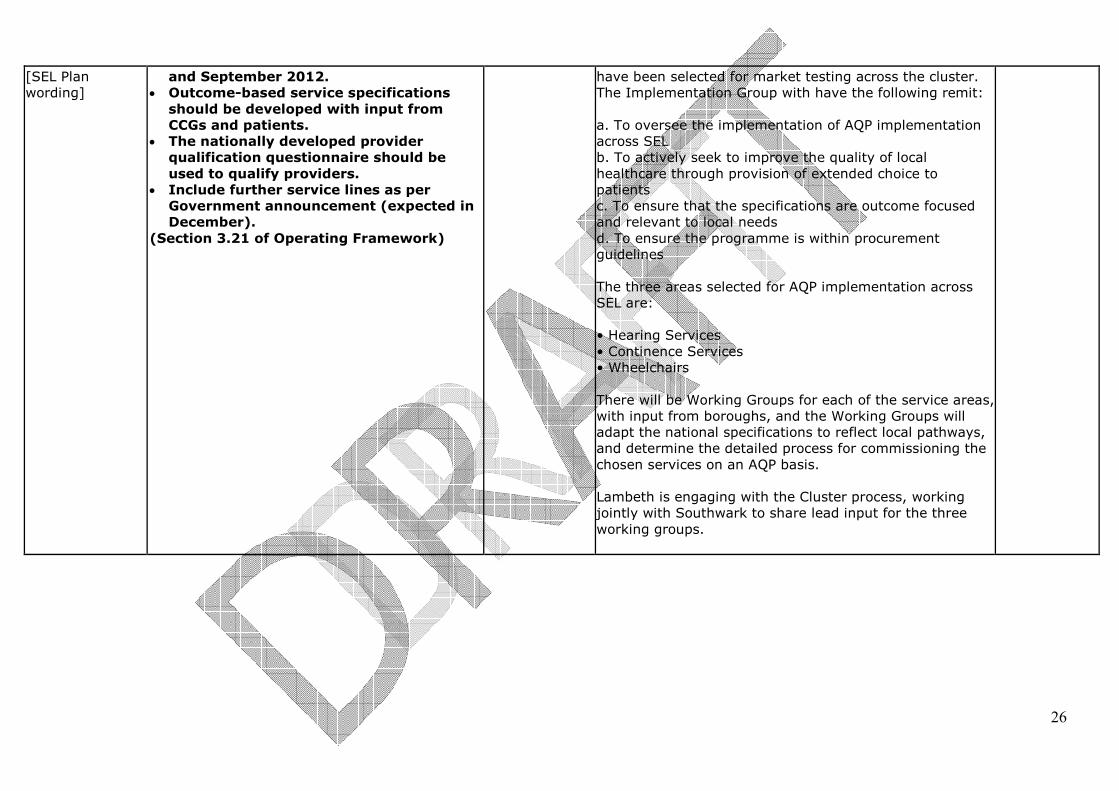
26
[SEL Plan
wording]
and September 2012.
• Outcome-based service specifications
should be developed with input from
CCGs and patients.
• The nationally developed provider
qualification questionnaire should be
used to qualify providers.
• Include further service lines as per
Government announcement (expected in
December).
(Section 3.21 of Operating Framework)
have been selected for market testing across the cluster.
The Implementation Group with have the following remit:
a. To oversee the implementation of AQP implementation
across SEL
b. To actively seek to improve the quality of local
healthcare through provision of extended choice to
patients
c. To ensure that the specifications are outcome focused
and relevant to local needs
d. To ensure the programme is within procurement
guidelines
The three areas selected for AQP implementation across
SEL are:
• Hearing Services
• Continence Services
• Wheelchairs
There will be Working Groups for each of the service areas,
with input from boroughs, and the Working Groups will
adapt the national specifications to reflect local pathways,
and determine the detailed process for commissioning the
chosen services on an AQP basis.
Lambeth is engaging with the Cluster process, working
jointly with Southwark to share lead input for the three
working groups.

27
Section Five: Commissioning Development PCT Clusters have an important role in the development of commissioning structures and
processes in their area during 2012/13. This includes:
o successful establishment of the new commissioning architecture to ensure effective clinical commissioning and handover by April 2013, comprising; commissioning support
organisations, or the transfer of commissioning responsibilities to the NHS Commissioning
Board, and nurturing clinical leadership through emerging CCGs, o and delivering full authorisation of as many CCGs as possible by April 2013 wherever emerging CCGs are ready and willing to achieve this.
The following areas are subject to change depending on the passage of the Health and Social
Care Bill and the drafting of the commissioning development section of the NHS Operating
Framework 2012/13.
5.1.
Summarise the PCT Cluster’s commissioning development priorities for 2012/13 and how
these will be implemented:
The sections below outline how Lambeth will transition to full CCG authorisation, support the development
of the South London Commissioning Support Organisation and contribute to the establishment of the
:Lambeth Health and Wellbeing Board.
We plan to work with and support the emerging NHS Commissioning Board to ensure an effective
transition of functions, along with local authorities for public health and the CCGs.
Once the timetable is known plans will be put in place for the transfer of staff and where required,
contract novation to all receiving bodies
5.2.
A. Summarise how the PCT Cluster will oversee and ensure the delivery of commissioning
responsibilities that have been delegated, during 2012/13, including; setting out the
approach to delegation including eligible commissioning budgets allocating non pay
running costs and staff: [SEL Plan wording]
- How delegated responsibilities will operate during 2012/13
- How the experience of delegated responsibilities will be captured to support
emerging CCGs in developing a track record for Authorisation, and
- Summarising plans for the transition of all commissioning responsibilities to
CCGs and others by the end of March 2013.
From April 2012 Lambeth will take on responsibility for commissioning all delegated budgets, and in
accordance with the South East London governance arrangements.
Additionally, the planning round for 2012/13 has been jointly delivered by the cluster and clinical
commissioners
A programme of work has commenced which will ensure that we successful transition to full authorisation
by April 2013, with support from the cluster team.
It is proposed that a full shadow year of running takes place from April 2012, with the central cluster
team continuing to support as required. The commissioning support offer to CCGs for south London has
been designed in order to be delivered, in shadow form, from April 2012.
Current arrangements for performance management of delegation are through the borough stocktake
meetings, and the emphasis and remit of these will change from April 2012 as the CCG has full
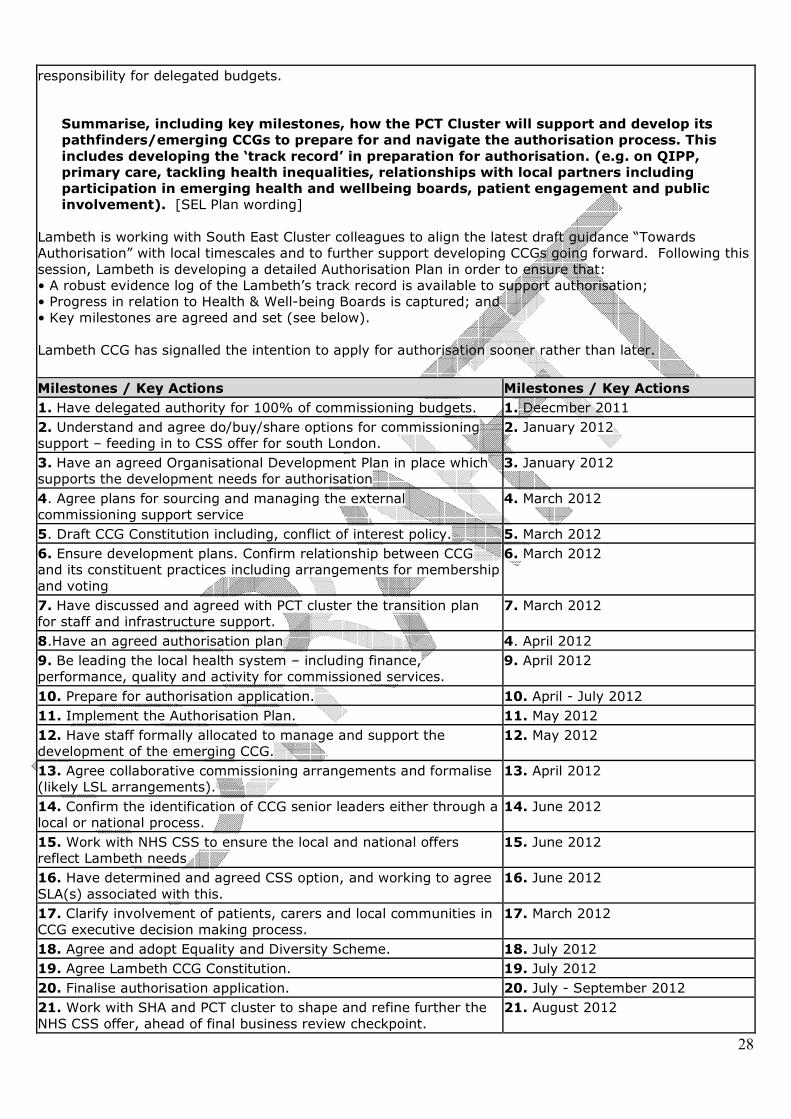
28
responsibility for delegated budgets.
Summarise, including key milestones, how the PCT Cluster will support and develop its
pathfinders/emerging CCGs to prepare for and navigate the authorisation process. This
includes developing the ‘track record’ in preparation for authorisation. (e.g. on QIPP,
primary care, tackling health inequalities, relationships with local partners including
participation in emerging health and wellbeing boards, patient engagement and public
involvement). [SEL Plan wording]
Lambeth is working with South East Cluster colleagues to align the latest draft guidance “Towards
Authorisation” with local timescales and to further support developing CCGs going forward. Following this
session, Lambeth is developing a detailed Authorisation Plan in order to ensure that:
• A robust evidence log of the Lambeth’s track record is available to support authorisation;
• Progress in relation to Health & Well-being Boards is captured; and
• Key milestones are agreed and set (see below).
Lambeth CCG has signalled the intention to apply for authorisation sooner rather than later.
Milestones / Key Actions Milestones / Key Actions
1. Have delegated authority for 100% of commissioning budgets. 1. Deecmber 2011
2. Understand and agree do/buy/share options for commissioning
support – feeding in to CSS offer for south London.
2. January 2012
3. Have an agreed Organisational Development Plan in place which
supports the development needs for authorisation
3. January 2012
4. Agree plans for sourcing and managing the external
commissioning support service
4. March 2012
5. Draft CCG Constitution including, conflict of interest policy. 5. March 2012
6. Ensure development plans. Confirm relationship between CCG
and its constituent practices including arrangements for membership
and voting
6. March 2012
7. Have discussed and agreed with PCT cluster the transition plan
for staff and infrastructure support.
7. March 2012
8.Have an agreed authorisation plan 4. April 2012
9. Be leading the local health system – including finance,
performance, quality and activity for commissioned services.
9. April 2012
10. Prepare for authorisation application. 10. April - July 2012
11. Implement the Authorisation Plan. 11. May 2012
12. Have staff formally allocated to manage and support the
development of the emerging CCG.
12. May 2012
13. Agree collaborative commissioning arrangements and formalise
(likely LSL arrangements).
13. April 2012
14. Confirm the identification of CCG senior leaders either through a
local or national process.
14. June 2012
15. Work with NHS CSS to ensure the local and national offers
reflect Lambeth needs
15. June 2012
16. Have determined and agreed CSS option, and working to agree
SLA(s) associated with this.
16. June 2012
17. Clarify involvement of patients, carers and local communities in
CCG executive decision making process.
17. March 2012
18. Agree and adopt Equality and Diversity Scheme. 18. July 2012
19. Agree Lambeth CCG Constitution. 19. July 2012
20. Finalise authorisation application. 20. July - September 2012
21. Work with SHA and PCT cluster to shape and refine further the
NHS CSS offer, ahead of final business review checkpoint.
21. August 2012

29
22. Signal intention for commissioning support for 2013/14 to
enable completion of business plans by NHS CSS.
22. August 2012
23. Agree risk sharing arrangements between practices/localities in
CCG.
23. September 2012
24. Complete formal CCG authorisation process. 24. December 2012 (at latest)
25. Have SLA in place with hosted NHS CSS ahead of taking on full
responsibilities from 1 April 2013.
25. January 2013
26. Be operating and preparing to take on full statutory
responsibilities.
26. March 2013 (at latest)
5.3.
Summarise, including key milestones, the PCT Cluster’s plan for the development of a
Commissioning Support Organisation to provide the required commissioning support for the
local market. This includes identifying local need, mapping the scope and scale of services to
be provided and developing cost models to ensure that the overarching strategic approach to
commissioning support will be affordable. [SEL Plan wording]
NHS SE and SW London have worked closely with emerging clinical commissioning groups and with local
authorities to produce an overarching plan for the development of a South London CSS.
By transforming current working practice it is believed that a SL CSS will be able to provide significant
benefits to Clinical Commissioning Groups the NHS Commissioning Board (NHS CB) and other potential
customers in delivering both improved health outcomes and value for money. It will also support CCGs in
their application for authorisation as they demonstrate access to robust and cost effective commissioning
support arrangements. Although complex and challenging to deliver, a South London solution provides
stability and opportunities for the development of commissioning support services and staff during the
transition and beyond, thus retaining NHS expertise.
Development work has been led by the directors of transition from SE and SW London supported by a
programme director and a development group of 10 service heads drawn from both clusters. Building on
this, and following the appointment of an interim managing director in December 2011, a core leadership
team is being established. Recruitment for a substantive managing director and head of acute contracting
are underway.
The service offering for the SL CSS has been guided by local CCGs. This has been achieved by CCGs and
NHS SE and SW London through their commitment to the joint development of this organisation through a
varied engagement strategy. Through this engagement, the PCT cluster has mapped the scope and scale
of all the services to be offered by the CSS. The CCG requirements can be summarised as detailed below:
• Core commissioning delivery support e.g. Contracting support , IT & Informatics
• Additional expertise e.g. Strategy development , business planning , QIPP planning and project
management
• Corporate support e.g. Governance support, Finance, and other back office functions.
The operating model for the SL CSS has been designed to reflect the expectations of CCGs. Each seeks a
strong local focus and close working relationship so that the needs of their local population remain the
priority whilst maintaining access to high levels of technical expertise. Services will also be delivered with
the help of a number of partner organisations as the benefits will allow SL CSS the:
• Ability to quickly build expertise / gain capabilities
• Scale for transactional elements of service delivery
• Flexibility to obtain right resources quickly for services with cyclical or unpredictable demand
Developing and commissioning new models of integrated care will be a priority for all CCGs across South
London. The SL CSS service offer will support existing and proposed joint commissioning arrangements
through its locally focused teams and integrated performance framework and contract support.
Discussions are currently underway with local authorities including public health to consider how a
collaborative structure with improved partnership working can develop. This will be further reflected in
Outline Business Case in March. Key to the success of the SL CSS will be the development of effective
partnerships between Primary, Secondary and the tertiary sector.

30
Work is underway to ensure the overall affordability of the CCG and CSS structures within the £25/head
target. SE and SW London clusters are leading this work of both support and challenge for CCGs and the
CSS. Running Costs
The key risks identified include; securing people with the right skills to support transformation, insufficient
buy in to the business, failure to deliver business as usual, overwhelmed by cluster activities and loss in
flexibility for deciding end state of the organisation. These risks will be mitigated through; marketing,
tendering, buying in additional expertise and developing staff within the organisation with potential;
regular communication and feedback, tight central and internal performance management, identifying
separate capacity to drive the changes – introducing an interim MD, an arms-length advisory board and a
development team as well as buying in outside consultancy support and working closely with DH and NHS
London to understand the shape of centralised services.
Prior to the submission of the Outline Business Case (OBC) in March 2012, progress will be made in the
following areas:
• Greater consensus on the level of support CCGs require from SL CSS.
• Further challenge and scrutiny of SL CSS costs to achieve profit margin and lower unit costs.
• Development of business strategy for SL CSS and consequential financing requirements.
• Complete mapping and transition from current state to future state.
To achieve a balanced position on running costs and so match the national target of £25/head, the next
phase of development will focus on the following issues:
• Further iteration on the balance between running cost provided CCG in-house versus outsourced to SL
CSS.
• Further test the ability of all services to deliver the required quality and capacity and an understanding
of how CSS core services integrate with CCG services
• Explore further opportunities for joint working with other CCGs and LAs.
• Clarify the ability of CCGs to invest in new services that are not part of the current system (e.g.
Integration of primary care data to data warehouse, risk stratification of patients).
• More detailed modelling of the transition to end state.
The service offering will continue to evolve over the next few months as discussions further shape the
CSS strategy and offer. As CCGs determine which services they will subscribe for, this will be reflected in
updated financial modelling. However, given the emerging consensus between the CCGs around the core
offering, SL CSS has been able to develop a pricing model reflecting three bundled packages. – Core,
additional, and bespoke/negotiated services (bought on a one off basis). This model provides a significant
amount of flexibility for CCGs when considering the support required to deliver their commissioning and
business priorities. A detailed pricing package for the three bundled packages of support will be developed
in more detail within the OBC in March, recognising the costs of business development, both to secure
new business and to defend existing income streams.
Developing the SL CSS will be achieved through the already established SL CSS transformational
programme. The priorities for this programme build on feedback from all pathfinders and local
authorities and include a focus on:
• Delivering a huge cultural change
• Setting a pace for the transition which will involve trade-offs e.g. long-term structure by 2012 vs. 2013
• Improving the quality of services providing the architecture, tools, products and services to deliver the
new clinical model of commissioning
• Access to new skills and capabilities (obtained either by building internally or sourcing from outside) to
secure a customer base which ensures the organisation as commercially viable
Alongside this programme of work the SL CSS will, over the next 15 months, drive forward its business
planning with the support of a number of enabling strategies including:
• Marketing & Business Development strategies
• An Organisational Development plan
• A Communications and Engagement strategy

31
• A HR strategy
• IT and Estates strategies
Milestones / Key Actions Milestones / Key Actions
1. South London CSS design, prospectus & stakeholder
support
1. September to December 2011
2. OBC, CCG sign up to prospectus and pricing, transition plan
including organisation structure
2. January to March 2012
3. FBC and staged implementation, subject to HR framework
3. April to August 2012
4. South London CSS fully operational
4. October 2012
5.4.
Summarise, including key milestones, the PCT Cluster’s provision of development support and
leadership development for pathfinders, which will be delivered during 2012/13.
This section should describe the activities in addition to that which is being provided through
NHS London’s development support offer and include what the PCT cluster will undertake to
provide development support to pathfinders during 2012/13. This should include:
• Development support provided and achievements to date
• Detail on the development plans in place.
• The plans in place for development support during 2012/13
Enter text here outlining risks and mitigations where necessary.
To be completed
Milestones / Key Actions Milestones / Key Actions
1. Enter text here
NB. ensure actions listed are not business as usual activity
NHSL will pre-populate milestones and dates where possible.
Have an updated Development Plan in place.
1. Enter text here
NB. ensure actions listed are not
business as usual activity
NHSL will pre-populate
milestones and dates where
possible.
5.5.
Summarise, including key milestones, the PCT Cluster’s role in the development of the single
operating model for the direct commissioning responsibilities the NHS Commissioning Board
will have (including primary care, dental services, armed forces etc.), and plans for handover
to ensure a safe and proper transfer of responsibilities in 2013 through an agreed process of
convergence. [SEL Plan wording]
Over the last nine months, the cluster has proactively supported the “Once For London” Pan-London
Operating Principles and chaired the development of the PMS Review Principles within this work. The
Cluster has developed through its Joint Standing Liaison Committee with the LMC, cluster wide policies
for:

32
Primary Care Performers List Management
GP Locum Reimbursement
GP Premises Cost Reimbursements & Rent Reviews- Application and Review Process
2011/12 QOF Process
GP Performance Management (incorporating Pan London GPOC)
Infection Control and Prevention Programme
GP Site Surveys
Cluster wide policies developed for other contractor groups include:
Primary Care Performers List Management Policy agreed with the LDC, LPC and LOC.
Optometry Contract Compliance Arrangements
Optometry PVV arrangements
Pharmacy Contract Performance Management Arrangements
Pharmacy Application Process
Dental Performance Management Arrangements
Initial discussions have been held with NHS South West Primary Care colleagues on joint programmes of
work and sharing best practice to the advantage of both clusters. Directorate representation at DH/SHA
events has assisted the development of policy.
The above activity is assisting in creating a single operating model within NHS South East London which
will assist in the transfer to the NCB model.
The Cluster has commenced the stocktake stage of the contracts transition PCT Implementation Plan and
will complete the sign off of the transition controls data capture tool and risk assessment for primary care
contracting by the 16th January 2012. This has been achieved with the recruitment of interim support and
it is intended to continue with this support through to the end of March 2012.
Circa 1,200 contracts have been identified during this stocktake stage and a risk assessment is being
completed to inform a development programme to provide a comprehensive and consistent contract
portfolio for transfer to the NCB. This will address the regularisation of contract documentation and
financial sign off of contract values by commissioner/provider.
The Cluster will undertake a GP premises survey to ensure statutory compliance and to assist practices to
prepare for CQC registration from April 2013. An application for improvement grant funds forms part of
the 2012/13 capital bids to address highlighted issues. The issue of leases for those practices occupying
PCT premises will be addressed and appropriate charging mechanisms put in place.
The cluster has approved capital monies to rollout EMIS web with SCR and EPS2 capability to 138
practices in LSLG with a similar programme in Bromley.
Early discussions have been had with local representative groups and cluster clinical advisors to form pilot
LPNs and to work through this grouping to develop fully functioning LPNs to assist in commissioning
decisions for the planning round 2013/14.
The cluster is developing plans based on the “Once for London” List maintenance policy to undertake a
review with practices of their registered lists. This work is aimed to set FP69 flags by the 1st October 2012
to regularise lists for the 1st April 2013.
Milestones / Key Actions Milestones / Key Actions
1. Completion of Stocktake. 1. 16/01/2012
2. Risk Assessment and development of Action Plan. 2. 31/01/2012
3. Stabilisation of contract documentation and financial
signoff within resource envelope.
3. 31/03/2012

33
4. Development of Local Professional Networks Pilots to fit
for purpose vehicles.
4. 30/09/2012
5. Regularisation of Premises Issues. 5. 30/09/2012
6. List Maintenance Exercise. 6. 30/09/2012
7. EMIS Web Rollout with SCR and EPS2 capability. 7. 31/03/2013
5.6.
Summarise, including key milestones, how the PCT Cluster will develop with emerging CCGs
and local authorities the Joint Strategic Needs Assessment, Joint Health and Well Being
Strategy, and joint/integrated commissioning arrangements during 2012/13. How will the
PCT Cluster ensure successful handover to CCGs, NHS CB, and local authorities for these
responsibilities? –
Health and Wellbeing
Lambeth has been designated as an Early Implementer Health and Wellbeing site and with local partners
we have the H&WBB has held a series of workshops, facilitated by the Kings Fund, to discuss the priority
areas for joint working. LCCCB members are taking a leading and very active role in the development of
our health and wellbeing arrangements in Lambeth. The Health & Wellbeing Board H&WBB will develop
the Joint Strategic Needs Assessment (JSNA), a borough-wide Health and Well-being Strategy and for
overseeing health improvement in our local community. All partners are committed to ensuring that the
work of the Board has practical benefits for the people who live in Lambeth. Two further areas of
importance have been identified as enhancing the involvement of our communities and the role of Public
Health. The shadow Board will be operational from April 2012.
Milestones / Key Actions Milestones / Key Actions
1. Shadow Health and Well Being Board in operation 1. April 2012
2. Refreshed JSNAs
2. July 2012
3. Health and Wellbeing strategy agreed
3. Sept 2012
4. Full Health and Well Being Boards operational
4. By March 2013
5.7.
Summarise, including key milestones, the PCT Cluster’s plan for the development of a Public
Health transition plan to ensure successful handover of responsibilities to local authorities and
Public Health England. – [SEL Plan wording]
Across South East London (SEL), each borough has identified a lead officer in relation to the transition of
the Public Health function. In each borough there are ongoing conversations about the transition between
the DPH, lead officer and a number of other relevant senior people of both the council and the BSU. The
boroughs are currently considering local design solutions for managing Public Health in the future. One
Borough is already in shadow arrangement using a section 75 agreement (Bromley). This will form the
basis of the design for the final structures in Bromley.
In addition there is work under way looking at the potential for sharing public health services across
boroughs, specifically between the four boroughs of Lambeth, Southwark, Lewisham and Greenwich.
These discussions are still in an early stage. To inform this piece of work the Directors of Public Health in
these four boroughs have undertaken a review of all services to transfer to the local authorities, analysed
where there is potential for work to be shared and put forward proposals about sharing of services. The
four councils that are considering sharing are currently discussing their approach or process for agreeing
what can be shared and how this might be designed. Bexley council has also expressed some interest in
the potential to be involved sharing of some services with these four.
The cluster has established a Public Health Transition Group with the role of coordinating all aspects of
transition of Public Health functions to local authorities, Public Health England and NHS Commissioning
Board. The Group includes all DsPH, representatives from the 6 local authorities, 2 Managing Directors of

34
BSUs, with HR, finance and communications representatives. The SEL HPU is also represented. A draft
work programme is in place and this will be refined in the light of further emerging national guidance and
financial allocations. The group will continue to meet and oversee all aspects of transition throughout the
transition period. The role of the group is not to supplant local (trans-) borough-based design and
planning but to support, inform and coordinate it, with the transition processes for other services. The
group will work to support 6 local transition plans in accordance with annex 6 of national guidance on
transition.
As part of the PH Transition Board the Cluster has established a HR working group consisting of Cluster
NHS lead on HR and a HR representative from each of the local authorities, with a public health
representative.
Information is being collected on all contracts as part of the wider cluster and national information
collection. The findings will feed into a transition workstream on transfers of contracts for all current
public health services. This will be overseen by the cluster Public Health Transition Group with local
discussions of the implications of transfer of each contract.
In recognition of the expected publication of the shadow budgets the SEL Public Health Transition group
plans to devote a considerable amount of the February agenda to the subject of finance and budgets. This
will complement local borough based work on understanding of the implications of the shadow budgets
and their relationship to the functions and contracts that will transfer from NHS to local authority.
Milestones / Key Actions Milestones / Key Actions
1. NHS SEL Public Health Transition Group established
1. Underway
2. Design processes for each borough underway
2. Underway
3. Assessment of implications of Shadow budgets
3. February 2012
4. Borough based plans for Transition of the Public Health functions
4. March 2012
5. Implementation of Transition Plans
5. Throughout 2012/13
6. Transfer of functions, staff and responsibilities
6. By end March 2013
5.8.
Summarise, including key milestones, how the PCT Cluster will develop plans for the transition
of specific responsibilities to local authorities , for example in addition to Public Health above,
the known areas of, Complaints and advocacy, information and signposting, and Independent
Mental Health Advocates (IMHA). –
This section should describe any planning to date and activities the PCT Cluster will undertake
to agree and plan jointly with Local Authorities to ensure a safe and proper transfer of
responsibilities during 2012/13.
Enter text here outlining risks and mitigations where necessary.
To be completed
Milestones / Key Actions Milestones / Key Actions
1. Enter text here
NB. ensure actions listed are not business as usual activity
NHSL will pre-populate milestones and dates where possible.
1. Enter text here
NB. ensure actions listed are
not business as usual activity

35
NHSL will pre-populate
milestones and dates where
possible.
2.
2.
3.
3.
4.
4.
5.
5.

36
Section Six: QIPP Summarise the CCG's key QIPP priorities and challenges for 2012/13 Lambeth faces continuing growth in demand and cost of secondary care services, driven by population
growth, demographic changes and the expansion of available health technologies. People are living
longer in Lambeth – in the past 10 years average life expectancy for men has increased by 4 years and
women by 2 years.There is also an increased expectation of the quality and extent of health service
delivery as a consequence of advances in medicine. At the same time the rate of increase of funding for
the NHS has considerably slowed down to just above inflation. This means that the underlying rate of
deficit will increase if no action is taken.
It is clear that the level of financial challenge facing the NHS over the next few years is unprecedented,
especially when compared to the significant levels of financial growth enjoyed by the NHS over the last
decade. A step change in how we approach the development and delivery of QIPP plans is therefore
required to address the level of financial deficit in the “do - nothing” scenario.
The financial challenge facing NHS Lambeth is therefore to secure significant QIPP delivery over the
course of the next three years to provide the financial resource to support delivery of our vision, health
goals and supporting strategies. If no action is taken then the underlying financial positions will
deteriorate, year on year resulting in a worsening in the current cumulative position. The plans to
achieve this are set out in Section 7.
Governance
Lambeth has developed a programme approach to the delivery of QIPP supported by formal contract
management arrangements. The programme structure is set out overleaf.

37
Joint Lambeth and
Southwark Clinical Leads Groups Leads
Planned care joint with Southwark
• management of long
term conditions
(including HIV)
• early detection
• secondary prevention
• management of elective
care in the most
appropriate settings
• shifting service
provision promoting
appropriate referral
• reducing inappropriate variability in care
Unplanned Care joint with Southwark
• Urgent Care • Frail Older People
Mental Health • Lambeth Living Well
Collaborative
• Forensic services
• Payment by Results
• Talking Therapies/
Counselling • Dementia
Staying Healthy • Tobacco and alcohol
• Adult and Childhood obesity
• Physical activity
• Health Checks
• Access to prevention
• Mental well-being
PCT Boards
Lambeth Clinical Commissioning Collaborative Board

38
Section Seven: Finance Planning Please complete the financial planning spreadsheets attached as Annex A.
7.1. Overview of financial position
Delivery in 2012/13, including FCOT, risks, opportunities, non-recurrent matters, etc.
Lambeth CCG has developed plans to deliver surpluses in line with the 1% surplus requirement, although
it should be noted that this is dependent on the return of 2011/12 surpluses. The underpinning plans that
enable the delivery of 2012/13 surplus requirements have been developed using robust processes,
modelling and methodologies for assessing underlying demand and service pressures, price pressures and
issues and QIPP initiatives and delivery plans. In doing so we have reviewed historic performance and
trends and also ensured lessons from 2001/12 processes and delivery have been learnt.
In addition we have focussed specifically on risks and opportunities in finalising our plans for 2011/13,
including ensuring that we have taken proactive steps to mitigate risks where feasible at this stage of the
planning process. The key risk risks and opportunities are summarised below:
• Over performance against 2012/13 start plans. Our modelling of underlying demand has been
more sophisticated for 2012/13, using an approach that moves away from a straight line outturn
projection to one that models on the basis of seasonality and working days. We consider that this
approach provides a more realistic baseline for our contracts. In addition we have worked with
providers to assess the further activity impact of meeting key targets for 2012/13, particularly
RTT, to enable these to be quantified up front for start contracts. Finally we have set aside
population and incidence reserves to fund further expected increases in demand over 2012/13.
• Pace and scale of change associated with the delivery of QIPP savings. Key mitigations have been
: learning lessons form 2011/12 QIPP delivery in terms of allowing within our plans for the phased
delivery of savings over the year, the development of plans in excess of the bottom line savings
requirements to mitigate against under delivery, collaborative work with providers over 2011/12
on 2011/12 plans, a contractual approach that makes explicit the responsible owner and risk
holder for each QIPP initiatives.
• The impact of PbR tariff in 2012/13, including for mental health providers. We have been prudent
in our assumptions and have established reserves to cover prices pressures such as Best Practice
Tariffs and to mitigate against areas of the contract where national average assumptions are not
delivered due to case mix. In addition we have worked with providers to complete as much work
as possible on expected and known tariff issues, across both PbR and local prices, to ensure prior
agreements have been reached at an early stage, thus enabling accurate assumptions to be
reflected in our 2012/13 plans.
• Return of 2012/12 surpluses, thus providing the flexibility to ensure delivery of 2012/13 surplus
requirements.
• Successful negotiation of 2012/13 contractual agreements. Our intention is to sign contracts in a
timely manner, thus providing financial certainty in relation to contractual agreements and
commitments for the start of the year. To facilitate this we have been working with providers since
the summer to enable early agreement on approaches to key issues. Agreed contract terms
represent an opportunity in terms of enabling effective risk mitigation, particularly in relation to
QIPP, as above.
• Access to 2% non-recurrent funds – providing opportunities for delivery and risks if funds are not
forthcoming to facilitate the delivery of QIPP initiatives. As this stage CCGs have been prudent in
committing 2% non-recurrent funds while we await confirmation of the proposed NHS London
approach in 2012/13. However at this stage some assumptions have been made and these are
listed in section 7.2.
7.2. Key assumptions in 2012/13
Including but not limited to:
- Service developments
- Tariff impact / changes
- Workforce
- Commissioning intentions

39
- N/R items
- Cluster access to 2% N/R funds
- Readmissions and reablement funds - Cluster risk pooling fund (CTB) - sources and applications
Lambeth CCG has been working closely together with other CCGs and with Cluster colleagues in
developing robust and consistent budgetary assumptions for 2012/13 in line with Operating Framework
guidance, building on and updating previous plans and sharing intelligence across boroughs as well as
learning the lessons from 2011/12.
Service developments - a range of service developments are planned for 2012/13 focussed specifically
on supporting the delivery of Lambeth CCG Commissioning Intentions and agreed service redesign
initiatives to support QIPP delivery. Over and above these locally-initiated service developments the SEL
Cluster will be implementing though contracts London Commissioning Intentions, new NICE guidance and
new cancer drugs. The key focus of our agreed service developments is agreement and implementation of
developments that further our strategic intention of shifting work from acute to community based settings
and delivering care pathway redesign to do so.
Tariff impact/changes - Looking back on 2011/12, it is clear that PCTs’ assumptions around the level
of underlying growth, particularly in the acute sector, were in line with expected population and incidence
growth but that price pressures had limited the ability of PCTs to ensure adequate investment in volumes
to meet underlying demand.
In developing 2012/13 budgets and in preparing for the negotiation of 2012/13 contracts, contracting
teams have agreed up front a number of assumptions relating to price changes in 2012/13 and these
assumptions are included in CSPs and Operating Plans. In terms of the impact of the 2012/13 PbR tariff,
while a national -1.8% tariff deflator was expected and this is built into budget, past experience would
suggest that such as assumption is risky and CCGs have therefore assumed a further 0.5% cost pressure
relating to the acute tariff. In addition, QIPP savings plans have not been delivered in full in 2011/12,
which has contributed to financial pressures faced by PCTs. The Cluster is mitigating against this by the
development of additional QIPPs in 2012/13, allowing the establishment of QIPP risk reserves as a
contingency should the pace of delivery be slower than planned.
Commissioning Intentions – Lambeth CCG has developed its own local commissioning intentions as
part of the SEL Cluster CSP and in addition the CSP incudes a number of Cluster wide priorities and
commissioning intentions. For the 2012/13 operating Plan we will be implementing year 1 deliverables,
focussing specifically on implementing agreed service and care pathway redesign to support QIPP and on
supporting the delivery in SEL of London and national commissioning priorities. From a financial
perspective where commissioning intentions require investment or pump priming these have been
accounted for within our plans for 2011/12 and where it is anticipated that they will deliver savings these
have been reflected in our plans, but with mitigation with respect to QIPP particularly also built in to our
plans.

40
• Recurrent Uplifts, Tariff and Generic Uplifts, Demographic & Non-Demographic Growth
and Primary Care Prescribing Uplifts
Lambeth CCG’s uplift assumptions are set out below:
Lambeth
Recurrent uplift 2.80%
Reablement 0.18%
Total Uplift 2.98%
demographic Growth 0.51%
Non-demographic growth 1.10%
Total population & incidence growth 1.60%
Prescribing growth 5.00%
Tariff/Inflation Uplift 2.03%
Tariff efficiency assumption/Price Efficiency applied -3.21%
Net Tariff/Inflation Uplift -1.19%
Further details on uplift assumptions are provided below:
° Recurrent Uplifts
The PCT Revenue Resource Limit (RRL) uplifts are as per confirmed allocation uplifts of 2.8%
plus a further 0.18% in respect of reablement.
° Tariff and Generic Uplifts
Tariff uplifts have been assumed at a net -1.8%, including a built in 4.0% efficiency
assumption. This has been applied to acute, mental health and community spend. Funds have
also been earmarked to fund the expected impact of the ending of the MFF payment cap,
applied to Guy’s & St Thomas’ in 2011/12.
° Demographic & Non-Demographic Growth
Detailed work has been undertaken to review planning assumptions related to demographic
and non demographic acute growth for the CSP. The objective has been to ensure robust and
realistic borough based planning assumptions related to population and incidence factors,
which take account of demographic growth estimates and historic acute demand trends. To do
so the following process has been undertaken :
− A review of population growth assumptions by borough (including GLA and ONS figures) for
acute services.
− A review of historic demand trends by borough for acute services, with supporting trend
analysis completed for the following key areas of acute activity – outpatients, elective, A&E
attendances, and emergency admissions, maternity and other.
− The development of proposed demographic and non demographic growth assumptions by
CCG by admission method, applied on a consistent basis across the six SEL boroughs.
− The testing of assumptions with SEL clinical commissioners, CCGs and CSP leads, to
confirm proposed planning assumptions.
This process has resulted in a consensus agreement, supported by robust analytics, on the

41
demographic and non demographic assumptions to be utilised for the CSP.
• Brought Forward Surpluses
Forecast surpluses for 2011/12 have been assumed to be carried forward into 2012/13.
• Full Year effect of 2011/12 outturn
The full year recurrent impact of 2011/12 forecast outturn expenditure has been included within
2012/13 expenditure plans, including the costs of reinstating PCT contingencies at 0.5% of
recurrent resource limits.
• Investment Proposals and Cost Pressures
Borough investments and cost pressures have been included in financial plans for 2012/13. While
detailed expenditure plans are in place for 2012/13, these remain draft pending the release of all
detailed planning guidance for 2012/13 and also further progress in the negotiation of 2012/13
contracts.
• QIPP Savings Initiatives
Lambeth CCG has reviewed its existing detailed QIPP savings plans with support from Cluster
teams. New QIPP schemes have been initiated and included in financial plans. Our total QIPP
savings schemes in 2012/13 are £22.883m. However schemes have been RAG rated to deliver
savings of £15.256m and it is this total that is assumed to be delivered within financial plans.
A summary of QIPP initiatives and their impact by expenditure area over 2012/13 are set out
below:
Lambeth
£'000
Planned QIPP Savings
Acute 7,134
Client Groups 6,542
Primary Care 7,407
Corporate 1,000
Other Budgets and Reserves 800
Total QIPP Savings Before Risk Rating 22,883
Risk Rating (7,627)
Total QIPP Savings After Risk Rating 15,256
• 2% Non-Recurrent Funds
Plans assume that 2% funds will be made available in full as an enabler for QIPP delivery and to
effectively manage the transition to the new commissioning environment. However, at this stage
CCGs have been prudent in committing 2% non-recurrent funds while we await confirmation of the
proposed NHS London approach in 2012/13. Lambeth CCG is however assuming that commitments
including the following:
o Primary and Community Care Estates enablers – specifically the non recurrent costs of the
Norwood and Akerman Road developments
o Planned Care Programme Implementation
o Mental Health Programme - including PbR Implementation
o Primary Care QIPP – project/transition costs
o Unplanned Care Programme
o Community Services transformation – enabling costs

42
• Emergency, Readmissions and reablement funds
No assumptions have been made relating to the reinvestment of 70% emergency over-performance
funds transferred to NHS London, noting that these funds are minimal across South East London,
due to the high 2008/09 emergency baseline and the fact that emergency admissions have reduced
since 2008/09 in most areas.
New reablement funds allocated to PCTs in 2012/13 have been earmarked for investment in agreed
whole system initiatives.
National guidance for emergency readmissions has recently been confirmed. We will be reflecting
the guidance in our contracts with SEL providers for 2012/13 with an agreed clinically led audit over
Q1 to agree appropriate non-funding agreements and targets with providers. However a number of
local commitments have already been made in relation to investment in admissions avoidance
schemes and where this is the case all parties have agreed that existing commitments will be
honoured.
• Risk Pooling
No new assumptions have been made in terms of pooling of risk across CCGs in 2012/13 to date but
it should be noted that CCGs agreed a policy of mutual financial assistance in 2011/12 so
understand the importance of ensuring financial balance and legacy across the local commissioners
as CCGs move towards full authority by 1st April 2013.
• Running Costs
QIPP plans assume the delivery of running costs reductions in 2012/13. The Cluster is in the process
of assessing the redundancy provisions requirement to include in 2011/12 PCT accounts.
7.3. Key bridging movements from 2011/12 FCOT to 2012/13 plan
Including changes by revenue type, cost type, QIPP, overall surplus/deficit and underlying
surplus/deficit.
Key bridging movements for Lambeth CCG are set out below:
Income and Expenditure changes 2012/13
Lambeth
£'000
Income
Recurrent Uplift 18,262
Prior Year Surplus brought forward 6,605
Total Income Changes 24,867
Expenditure
Full year effect of 2011/12 outturn 17,065
Net Generic Uplifts
Tariff and generic uplifts 12,781
Efficiency with Tariff (20,271)
Net Tariff/ Generic Uplift (7,490)

43
Demographic & Non-Demographic Growth
demographic Growth 3,150
Non-demographic growth 6,841
Total Demographic & Non-Demographic Growth 9,991
Investment Proposals and cost pressures 13,556
QIPP Savings Initiatives (15,256)
Change in Recurrent Expenditure 17,867
Surplus/ (Deficit) 7,000
Surplus as % of Recurrent RRL 1.10%
7.4. Delegation of budgets to pathfinders / CCGs
Including commentary on:
- £2/head GP development
- Budgets delegated to pathfinders / CCGs at 1st April 2012 - Timeline for delegation of budgets (if not fully delegated at 1st April 2012)
The Cluster and Lambeth CCG achieved full delegation of budgets in December 2012. The active
involvement of Lambeth Clinical Commissioners in the 2012/13 acute contracting round is part of the
process of embedding full responsibility for these budgets. This builds on our experience in 2011/12 and
2010/11 working with Practice Based Commissioning and clinical commissioning
Lambeth CCG is planning on £2/head GP development funds being available in full in 2012/13. These
funds are included within the 2012/13 Operating Plan and will be used to support the development of
Lambeth CCG. This includes meeting the cost of supporting organisational development and systems of
governance, developing a strong local clinical network and taking forward practice level information
analysis.
Planned outcomes for delegated commissioning activities are incorporated within the Operating Plan and
Business Plans. Outcome measures cover:
• Delivery of Financial balance and our QIPP plans
• Quality assurance of ongoing safety of services
• Patient reported outcomes and improved patient experience of services
• Enhanced effectiveness of services and care pathways
• Shift of care to out of hospital settings and from treatment to prevention
• Delivery of performance standards.
It should be noted that Operating Plan budgets include specialist commissioning and public health
budgets in full. Specialist commissioning budgets have been set in line with agreed LSCG budgets and
therefore the impact on other CCG held budgets has been built into assumptions.
7.6. Triangulation
Describe the triangulation activity that has taken place to ensure robustness in respect of:
- Activity

44
- SLA values - Workforce
Enter text here [this should include a specific link between the QIPP schemes, activity and
SLAs] outlining risks and mitigations where necessary.
Activity and QIPP schemes are covered in detail in Section 7.5: Activity.
Contracts for 2012-13 have not been finalised as yet and this information will be included in a later
version of the Operating Plan.
7.7. Key capital schemes
Include scheme name, values, purpose, funding source, etc.
Akerman Road – Lambeth
This £13.1m, 5200m2 LIFT funded development is under construction and will be completed in July 2012
and provides a local neighbourhood resource centre hub for 3 general practice, community health
services, dental services and a base for adult social care services. This is a key development in a highly
deprived part of Lambeth.
Norwood Hall – Lambeth
Subject to approval this £14.2m, 5402m2 LIFT development will reach financial and commercial close in
2012. This development is being carried out jointly with Lambeth Council, who will take the head lease,
and will provide a customer service centre, swimming pool and other sports facilities as well as health
services covering 2460m2 of space including general practice, community health services and a specialist
dental school. Norwood is scheduled to open in 2014/15.
7.8. Liquidity / cash flow / loan requirements
All the PCTs in the SEL Cluster are on target to achieve their 2011/12 cash target by drawing down their
cash limits in full with minimal cash balances at 31 March 2012. It is, therefore, assumed that the
availability of cash resources in 2012/13 will not be impacted by adjustments relating to 2011/12.
The Cluster PCTs’ cash assumptions in 2012/13 are based on the availability of cash resources in line with
both recurrent and non-recurrent revenue and capital resources, with the exception of carry forward
surpluses from 2011/12. Cash in 2012/13 will be managed through the movement in working balances. It
is, therefore, anticipated that the Cluster PCTs will not require additional cash support from NHS London.
7.9. Key financial risks and opportunities in 2012/13
All NHS organisations are facing ongoing financial pressures, after many years of unprecedented growth
in available funds. Further details of these risks are outlined below:
• 2011/12 Outturn
Outturn assumptions have been updated since submission of the CSP and in the Operating Plan we
have funded 2011/12 outturn based on the latest forecasts, taking into account the use of non
recurrent savings or sources of funds and the impact of this in 2012/13, as well as seasonality,
working days and Referral to Treatment requirements. The extent to which actual outturn deviates
from this may provide some financial risks, which will present itself as over-performance against
contracted levels of activity in 2012/13, which would need to be funded from contingency
reserves.
• QIPP

45
All QIPP initiatives have been risk-assessed to give increased confidence that the savings that will
be achieved in 2012/13. GP Leads and Project managers are clear that their objective is to aim for
the stretch QIPP plans in 2012/13. Implementation plans have been developed and signed-off by
individual CCGs. For those initiatives that are owned by the provider we expect our contract terms
to mitigate the risk of non-delivery from the PCT/CCG perspective and Trusts are equally
committed to ensuring full delivery of agreed targets. Each local health economy has in place
processes to ensure the effective monitoring and management of QIPP delivery in year.
• 2% Non-Recurrent Funds
Plans assume and include use of the 2% funds in full as an enabler for QIPP delivery and to
effectively manage the transition to the new commissioning environment. This represents both a
risk and opportunity in 2012/13 and the Cluster and Lambeth CCG will that ensure robust plans
are in place to ensure access to funds at an earlier stage in the financial year. The 2% Non
Recurrent Investment Fund is recognised as being important to deliver QIPP targets and ensure
the achievement of underlying financial balance over 2012/13 and the strategic period.
• Return of 2011/12 Surpluses
The remains uncertainty on the return of our planned 2011/12 surpluses in 2012-13. This is
current Treasury policy but there is the risk that this may be used to manage overall NHS cost
pressures. The Operating Plan assumes that this surplus is returned in full. If this was not the
case our QIPP plans would need to increase accordingly and/ or planned surpluses in 2012/13 are
reduced.
• The impact of PbR tariffs in 2012/13, including for mental health providers.
We are currently assessing the impact of the final acute PbR tariff – the impact of the new tariffs
will differ by provider and for each CCG and any deviation from the assumed -1.8% could present
financial risks. However our financial plans have assumed under delivery of the -1.8% and we
consider therefore that in aggregate terms the impact of 2012/13 acute PbR tariffs will be
manageable within our existing plans.
The impact and timing of the introduction of Mental Health Payment by Results (PbR) remains
unclear. Commissioners have agreed principles for rebasing contract baselines in negotiation with
SLAM associated with the introduction of PbR full implementation of responsible commissioner
guidance, to minimise risk across both commissioners and provider. Work is jointly being
undertaken during 2011/12 and in 2012/13, the introductory year to ensure that activity and
financial information is robust and forms a strong base for the implementation of PbR.
• Successful negotiation of 2012/13 contractual agreements.
For acute providers we have now received costed proposals for the majority of our key providers
and negotiations are progressing well. We expect to have achieved early signing of the contract
with LHNT (end February 2012), ad also to reach a timely agreement with GST and KCH. A
successful negotiation in terms of securing early agreement and financial certainty in relation to
SLHT however remains a risk – we are working with SLHT, with senior level Chief Executive
involvement, to try to mitigate against SLHT related risks. Good progress is being made with non-
acute provider negotiations for 2012/13 and we expect to be able to reach timely agreement
within the parameters set out in our 2012/13 plans.
• Ensuring Financial Delivery
Financial balance and the delivery of the PCTs’ planned financial positions is a core priority and a
statutory requirement for NHS SE London. Lambeth CCG, working in conjunction with the Cluster
plays a vital leadership role in this.
The financial position is reviewed regularly by Lambeth CCG, the Cluster Joint Board and the

46
Cluster Performance, Finance & QIPP Committee. Quarterly Joint Cluster and CCG QIPP Stocktake
meetings provide executive assurance of financial and service performance including QIPP delivery
and review progress against the achievement of full authorisation. Internal and external audit
review the PCTs’ financial management, reporting and controls. Further external assurance is
also put in place where this is needed.
The achievement of in-year and underlying financial balance is supported by the delivery of
Recovery Plans. These plans are kept under Board review as part of the agreed overall financial
reporting arrangements. Savings proposals are developed through a process of budget challenge
across all areas of activity.
Lambeth CCG is implementing an Organisation Development Plan that takes account of the NHS
London Roadmap recognised by the Department of Health as a means of achieving full
authorisation. The Roadmap’s eight domains include finance and governance, and development
programmes will strengthen Lambeth CCG’s skills in these areas. This work is underpinned by a
detailed Authorisation Work Plan.
Organisational change and the associated period of transition bring significant changes in the
responsibilities of individual staff members, different reporting lines and changes in key personnel
and represents an organisational risk. The Cluster and NHS Lambeth finance teams is working with
senior staff to ensure changes to the budgetary framework are quickly embedded, including:
o Revised budgetary framework
o Refreshed budgetary delegation to budget holders
o Refreshed authorised signatory lists
o Enhanced reporting arrangements
o Budget holder guidance and training
The Cluster is actively pursuing debtor management to ensure all the income due to the PCTs is
recovered. Processes are in place to ensure that creditors are paid efficiently and on time so that
the Better Payment Practice Code (BPPC) can be met and outstanding creditor balances are,
wherever possible, minimised. This involves regular reporting of outstanding invoices supported by
staff training in the use of electronic workflow systems.
The Cluster has implemented a new Sollis information system across all boroughs and is continuing to
develop opportunities to improve data validation, claims management and forecasting.
7.10. Overall contingency / reserves
All CCGs within the SEL Cluster have set aside the following reserves and contingencies in 2012/13 initial
budgets and plans:
• Contingency reserves of 0.5%, in line with NHS London guidance.
• Funds to deliver surpluses equivalent to 1.0% of recurrent resource limits. This will however be
dependent on the carry forward of surpluses from 2011/12.
• Earmarked sums for population & incidence growth. These will be released to fund activity above
2011/12 forecast outturn, as agreed with providers. These may also need to be used, in part, to
fund any unanticipated cost pressures in 2012/13, including the impact of final PbR tariffs.
• Reserves relating to the difference between 150% QIPP savings and the 100% required. These
reserves will be released to fund reductions in agreed QIPP savings, closer to the 100%, should
savings be guaranteed to CCGs.

47
Section Eight: Workforce 8.1. Workforce impact of strategic goals
Will your service vision for the cluster have a workforce impact for your
providers?
Please provide a description of the anticipated impact for workforce
within local provider Trusts and Community providers as a result of the
cluster’s strategic initiatives e.g. describing anticipated increases /
decreases for your main providers and services that may see significant
change.
Yes
To be completed
8.2. Effective communication with providers
Does your organisation have a process in place by which it can assure the
workforce strategies of its provider organisations are fully integrated
with service and financial plans; have clinical ownership and aligned with
the cluster’s vision as highlighted in its commissioning intentions communicated to its providers?
Yes / No
(delete as
appropriate)
To be completed
8.3. Quality of service / education considerations
8.3.1 Has the cluster made clear to their provider organisations that their
education and training funding should be used to transform their
workforce to support the delivery of the cluster’s service vision, and does
the cluster have mechanisms in place to assess whether provider
organisations have appropriate plans to support this objective?
No
To be completed
8.3.2 Does the cluster have processes in place to ensure that provider
organisations carry out appropriate workforce risk assessments and
address capability or capacity issues ahead of the changes that the
Cluster’s local service vision will require?
Yes / No
(delete as
appropriate)
To be completed
8.4. Statutory workforce obligations
Does the organisation have a process in place by which it can assure
statutory workforce obligations (e.g. EWTD, mandatory training, %
appraisal rates, quality of appraisals, medical revalidation) are delivered
within its provider organisations?
Yes / No
(delete as
appropriate)
To be completed

48
8.5. Monitoring and performance management
Does the cluster include workforce metrics, benchmarking, trends and
plans within its contract performance process with its providers? Are
these metrics incorporated with related quality metrics and intelligence,
and used to identify and raise concerns about future trends and
performance? Where the workforce indicators of a provider raises
concern, please describe the process that the cluster will take to resolve
the risk identified? How will the cluster ensure that CQC and Monitor
have been involved as appropriate?
Yes / No
(delete as
appropriate)
The expectation here is that Clusters monitor workforce in their providers to ensure that any
issues are highlighted in relation to workforce before patient safety is put at risk.
E.G. The Cluster has negotiated as part of its contract with its providers the provision of the
following data on a quarterly basis: 12-month rolling sickness and turnover rate, vacancy
rate, agency usage as part of its total staff pay bill, progress against training plan and
progress against its staff health and well-being plan. If any of these areas reported on are
rated red, they form part of the discussion for example in the quarterly workforce review
session which we hold with each of our providers. Please see a copy of the template which
shows this information is submitted to the Cluster as evidence.
To be completed
8.6. Managing of workforce risk
Where workforce changes have been identified, please describe the risks
that these changes may have to patient care standards during the
transition and the process by which the Cluster will mitigate these risks
with the providers?
Yes / No
(delete as
appropriate)
To be completed

49
Appendices Confirmation of upload of 2012/13 UNIFY planning templates
Please attach the operating plan 2012/13 Workforce return
Please attach the operating plan 2012/13 FIMS Operating Plan
Please attach the 2012/13 QIPP milestone tracker return


















