Newly Diagnosed: Ovarian Cancer 101, Gordon Mills, MD, PhD
31
DREAM TEAM DREAM NO SMALL DREAMS GOETHE TIME MAGAZINE WOMEN’S CANCER MOONSHOT
-
Upload
ovarian-cancer-research-fund-alliance -
Category
Health & Medicine
-
view
1.092 -
download
0
Transcript of Newly Diagnosed: Ovarian Cancer 101, Gordon Mills, MD, PhD

DREAM TEAM
DREAM NO SMALL DREAMS GOETHE
TIME
MAGAZINE
WOMEN’S CANCER MOONSHOT
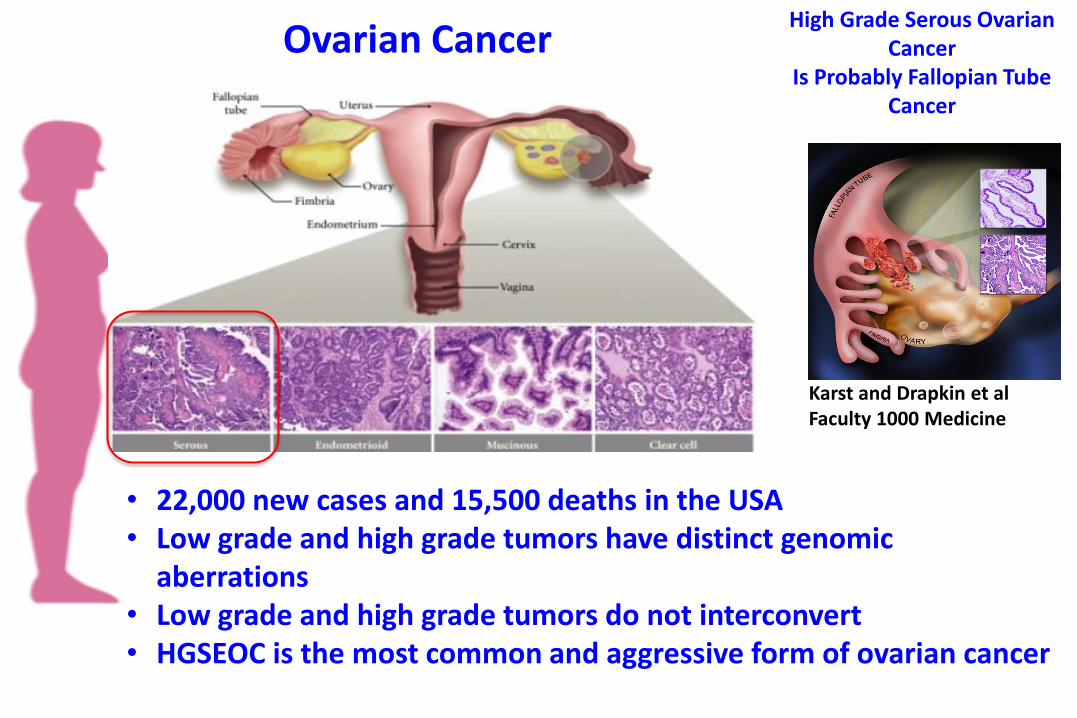
Ovarian Cancer
Karst and Drapkin et al Faculty 1000 Medicine
High Grade Serous Ovarian Cancer
Is Probably Fallopian Tube Cancer
• 22,000 new cases and 15,500 deaths in the USA • Low grade and high grade tumors have distinct genomic
aberrations • Low grade and high grade tumors do not interconvert • HGSEOC is the most common and aggressive form of ovarian cancer

DIFFERENT HISTOLOGICAL SUBTYPES OF OVARIAN CANCER INDICATE DIFFERENT THERAPEUTIC OPPORTUNITIES
Serous
Endometrioid
Mucinous
Clear cell
High grade low grade
High grade low grade
Low grade serous
KRAS
Clear Cell
PIK3CA mutations
Endometrioid
ARID1A mutation and deletion
Mucinous
Probably metastatic colon
High grade serous
p53, BRCA1/2 copy number
long tail of actionable mutations
Targeted agents
Bevaczumib
PARP inhibitors have now been
FDA approved
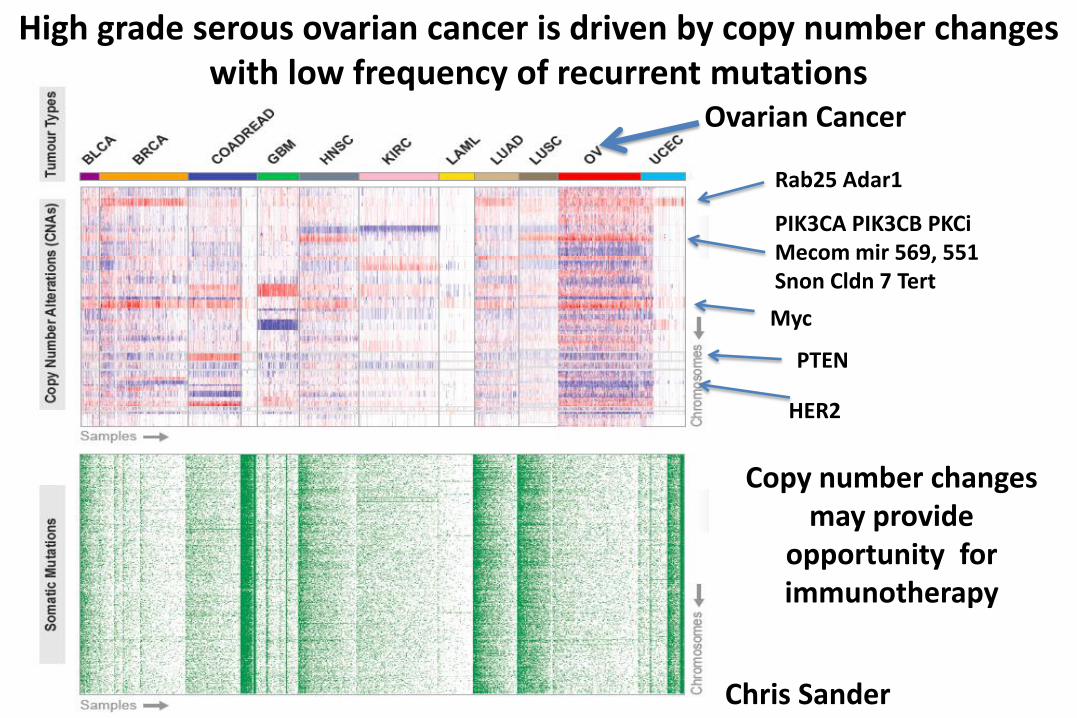
Chris Sander
Rab25 Adar1
PIK3CA PIK3CB PKCi Mecom mir 569, 551 Snon Cldn 7 Tert
HER2
PTEN
Ovarian Cancer
Myc
High grade serous ovarian cancer is driven by copy number changes with low frequency of recurrent mutations
Copy number changes may provide
opportunity for immunotherapy

HGSEOC is primarily driven by DNA copy number abnormalities with
p53 and BRCA1/2 pathway mutations
Gene % of mutations
TP53 96.4
CSMD3 4.8
FAT3 4.8
NF1 3.2
BRCA1 2.7
BRCA2 2.5
CDK12 2.2
RB1 1.5
GABRA6 1.5
Somatic Mutated Genes in HGSEOC
TCGA Ovarian Network Joe Gray
Rab25 PRKCI, MECOM Snon,PIK3CA, TERT mir551 569
MYC PVT1
Cyclin E
BRCA1/2 germline mutations and loss in 20-
25% of of ovarian cancers Improved patient outcomes

Opportunities associated with genomic aberrations in high grade serous ovarian cancer
• P53 – Wee1 inhibitors have increased activity in p53 mutated tumors
– P53 is frequently retained but unfolded and non-functional • Can be normalized by a number of compounds
– COTI2, ZMC1, Prima1
– P53 loss is common • Can result in loss of nearby genes
– POL2RA heterozygous loss can sensitize to alpha amanitin
• Homologous Recombination (HR) defects – Almost half of HGSEOC have evidence for defective HR
– A number of assays have been developed to identify patients likely to benefit from targeting HRD
– Sensitize to platinum based therapy
– PARP therapy is demonstrating activity • Rational Combinations with PARP therapy
• Almost half of all HGSEOC have a mutation in an actionable gene – Are these drivers or passengers Will targeting these genes benefit patients


The Impact Of Residual Tumor: What Is Optimal Debulking?
Progression-free survival Overall Survival
Dubois et al, Cancer, 2009: Mar 15; 115(6): 1234-44
R0 R0
R0 25%
0 < R1 <1 cm 50%
R2 > 1cm 25%

Rates of R0 resection
Nick et al., Nature Rev Clin Oncol, 2015

Opportunity For Quality Improvement: Personalized Surgical Therapy
Implementation of evidence-based patient care guidelines
Multidisciplinary approach
Improvement in the quality of surgical care
Standardized care
Improvement in rates of complete gross resection (R0) with reciprocal improvement in patient overall survival
Developing a personalized surgical approach that translates across different clinical practice settings

Women w/ suspected ovarian cancer
Primary Assessment
Laparoscopy: Validated score
Intraoperative agreement
R0 not feasible
Neo-adjuvant chemotherapy
R0 feasible
Primary tumor reductive surgery
Tissue
Immune & molecular analyses
Opportunity For Quality Improvement: Personalized Surgical Therapy

Primary cytoreduction 20% 88% (n = 87)
NACT → Interval cytoreduction 60% 76% (n = 65)
Surgical Outcomes (R0 Rates) since implementation of Flagship 2A
Pre- implementation
Post- implementation
Major effort focused on R0 resection included education, clinical retreats (consensus among all 21 gynecologic oncologists), and engaging other specialties (e.g., thoracic, GI surgery)
Compliance is over 98%
Flagship 2B: Novel Clinical Interventions
Develop integrated predictors of response to standard chemotherapy
Assess tumor heterogeneity and molecular evolution to determine adaptive responses to standard therapeutics
Novel clinical trial designs

New Moonshot Projects - FP2B HGSOC Fl
agsh
ip P
roje
ct 2
LSC
Score <8
FP2b Phase 0 “Window” trials
1-2 wks Single Agents “POSITION” Trial
Debulking
Tissue acquisition
Novel therapy vs. Std therapy
Score >8
FP2b Phase Ib-2 Treatment Trials
NACT
Pac/Carbo + novel Debulking
Adjuvant
Pac/Carbo + novel
Tissue acquisition
Tissue acquisition

Clinical Trial Standard of Care
Matched sites Ovary/Primary Omentum Diaphragm Other peritoneum
Ovarian Cancer Window of Opportunity Trial
Analysis: • HRD assessment
• DNA, RNA, Protein • Immune profile • Generation of PDX and lines

Flagship 2C: PDX Models - Transition to the clinic
Development of breast and ovarian cancer patient-derived xenograft models:
• Molecularly characterized (DNA, RNA, protein)
• Therapy naïve
• TNBC: >10 (6 genomically characterized)
• HGSOC: 10
• Post-therapy/resistant
• TNBC: 5
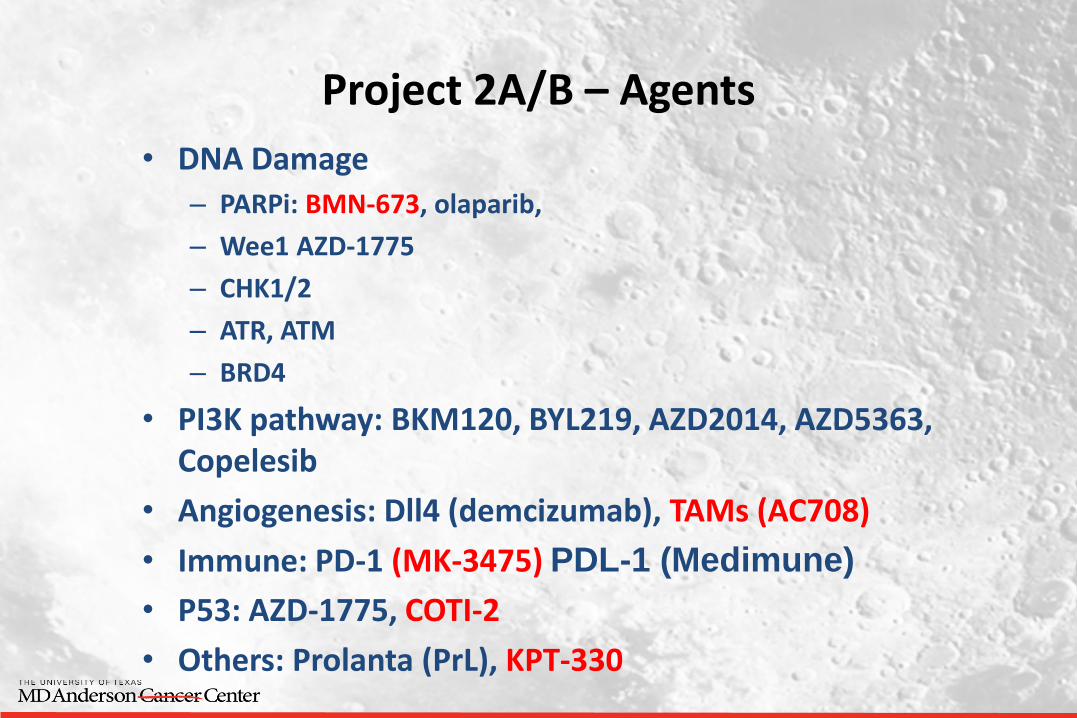
Project 2A/B – Agents
• DNA Damage
– PARPi: BMN-673, olaparib,
– Wee1 AZD-1775
– CHK1/2
– ATR, ATM
– BRD4
• PI3K pathway: BKM120, BYL219, AZD2014, AZD5363, Copelesib
• Angiogenesis: Dll4 (demcizumab), TAMs (AC708)
• Immune: PD-1 (MK-3475) PDL-1 (Medimune)
• P53: AZD-1775, COTI-2
• Others: Prolanta (PrL), KPT-330

Expanding our Program
Regional care centers in the greater Houston area • Katy, The Woodlands, Sugarland,
Bay Area and Pearland • LBJ Hospital (Houston, TX) • MDACC Cancer Network
MD Anderson Cancer Center at Banner and Cooper National and International Sister
Institutions Other national and international
centers

Building a Pipeline for Future • Translational biology
• P53 based approaches – synthetic lethality
• New animal models and imaging to prioritize the massive numbers of potential new targets and drugs
• Rational combination therapy: new combinations of kinase inhibitors; identify synergistic combinations with PARP inhibitors
• Immune modulation/inflammation as therapy targets
• Re-define “druggable” targets – co-extinction strategies
• Survivorship
• Identify and validate predictors of long-term survival
• Predictors of toxicity
• Early Detection and prevention
• New biomarkers for screening and drugs for prevention

WOMEN’S CANCER MOONSHOT
BRCA1 and BRCA2
10% of TNBC or HGSOC
Family history
TNBC or HGSOC
Predisposition to breast and
ovarian cancer
BRCA2 Male breast cancer
Prevention decreases risk by at
least 80%
New therapy (PARPi) effective
for patients

Germline BRCA-1 and -2 testing
(>10% will be positive)
FP1A Active Outreach
FP1C Screening Prevention
Offer genetic testing to all patients
with TNBC or HGSOC
NCCN Guidelines
No charge to patient or MDACC
Making Cancer History for the Family
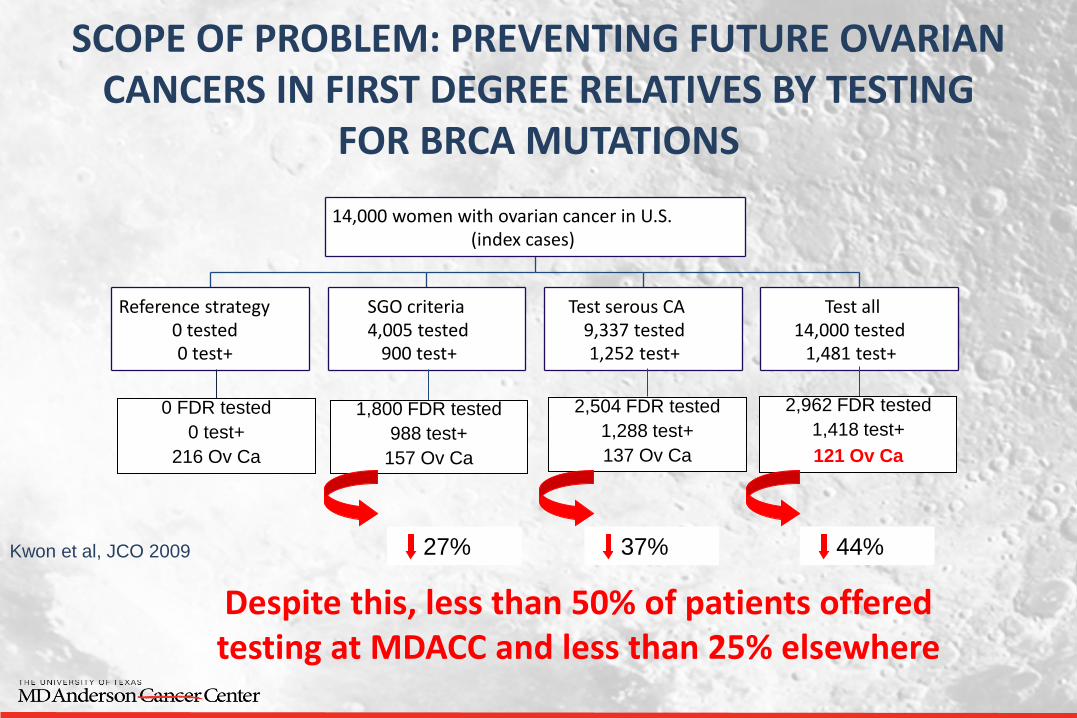
SCOPE OF PROBLEM: PREVENTING FUTURE OVARIAN CANCERS IN FIRST DEGREE RELATIVES BY TESTING
FOR BRCA MUTATIONS
Reference strategy 0 tested 0 test+
SGO criteria 4,005 tested
900 test+
Test serous CA 9,337 tested 1,252 test+
Test all 14,000 tested
1,481 test+
14,000 women with ovarian cancer in U.S. (index cases)
0 FDR tested
0 test+
216 Ov Ca
1,800 FDR tested
988 test+
157 Ov Ca
2,504 FDR tested
1,288 test+
137 Ov Ca
2,962 FDR tested
1,418 test+
121 Ov Ca
27% 37% 44% Kwon et al, JCO 2009
Despite this, less than 50% of patients offered testing at MDACC and less than 25% elsewhere

Breast Ovarian Number of patients 2458 680 Number of pts. tested at MDA 1729 389 Percentage tested 72% 57% BRCA⁺ among TNBC/HGSOC 51 73 Percent positive 14% 19%
FAMILY OUTREACH PROTOCOL (REACH) Total number of family members 121 Contacted 47 (50%)
Current Reporting Metrics for TNBC/HGSOC Patients (9/1/2012 – 3/31/15)
IMPACT: Increased testing rate from 25% to 65%!!
Making Cancer History for the Family
Previvors • Surgical Prevention • Chemoprevention • Screening
• Recently Funded-SU2C • CHECMATE Trial - CHance to End
hereditary ovarian Cancer by MAking Testing better and Easier
• WISDOM Trial - Women choosing Interval Salpingectomy with Delayed Oophorectomy to postpone Menopause

Best way to improve
outcomes is to prevent the
disease
5 years
80% decrease in deaths in
family members
12% improvement in
survival
Making Cancer History for the Family
20-50% of patients will
have a defect BRCA1 or
BRCA2 function
PARP-inhibitor based
therapy
8 fold improvement
Offer genetic testing to all
patients with TNBC or
HGSOC
HELPING THE PATIENT
Academic Industrial
Collaboration
Other moonshots
Identification of patients
likely to benefit
HELPING THE PATIENT
Rational combination therapy
with PARPi
7 new trials

Improving
outcomes
across
Houston,
Texas and the
world
PARADIGM SHIFT
Patient
Family


Current state-of-knowledge Front-line Therapy:
- Surgery
• Comprehensive staging or cytoreduction for metastatic disease
• Tumor residuum is the strongest prognostic factor
- Adjuvant therapy
• Nearly all cases
• Platinum-taxane based
Recurrence Therapy:
– Chemo-sensitive disease
• Approach like frontline therapy
• Surgery (+/-)
• Platinum based
– Chemo-resistant disease
• Emergence is cause of death
• Multiple agents of poor response
Roles of biologic and maintenance therapy are evolving
Som
e a
re c
ure
d! N
on
e are
cure
d!