New injectable and radiopaque antibiotic loaded acrylic bone cements
9
New Injectable and Radiopaque Antibiotic Loaded Acrylic Bone Cements Lidia Hernandez, M. Eugenia Mun ˜ oz, Isabel Gon ˜ i, Marilo ´ Gurruchaga Universidad del Paı´s Vasco 20009-San Sebastia ´ n, Spain Received 26 December 2006; revised 22 January 2008; accepted 25 January 2008 Published online 7 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.b.31105 Abstract: The use of antibiotic loaded bone cements (ALBCs) has become a common clinical practice in the prevention and treatment of prosthesis-related infections. However, due to antibiotic resistance, there is a general interest in broadening the antibacterial spectrum of currently used drugs. The aim of this work is to formulate ALBCs for specific use in vertebroplasty and kyphoplasty, and to study the effect of the addition of ciprofloxacin alone and in combination with vancomycin on some properties of the cement. The cements were formulated using bismuth salicylate as the radiopacifier. The setting properties, residual monomer content, release of antibiotics, rheological behavior, injectability, and mechanical properties of these formulations were studied. They showed long setting times and low curing temperatures. From the release studies, antibacterial properties are assumed because the concentration of released antibiotic was higher than the minimum effective. Although the experimental cements had slightly reduced mechanical properties, the other alterations shown were negligible. ' 2008 Wiley Periodicals, Inc. J Biomed Mater Res Part B: Appl Biomater 87B: 312–320, 2008 Keywords: bone cement-PMMA; antimicrobial; vertebral; viscosity, mechanical properties INTRODUCTION One of the first modifications of acrylic bone cements con- cerns one of the more serious complications of orthopedic surgery: bacterial bone infections (osteomyelitis). 1 In the early 70s, Buchholtz and Engelbrecht 2 already included gentamicin sulphate (GS) in a standard formulation to treat an infection in a total hip arthroplasty. 2 Thanks to their success, the use of antibiotic loaded bone cements (ALBCs) has become common clinical practice in the pre- vention and the treatment of prosthesis-related infections 3 with the aim of attaining high local drug levels, while maintaining low systemic levels. 4 Apart from GS, other antibiotics such as erythromycin, clindamycin or tobramy- cin 5 are also being used as additives for bone cements. However, due to antibiotic resistance, there is a growing in- terest in the addition of other antibiotics or mixtures of antibiotics to bone cements, which broadens the antibacte- rial spectrum of currently used drugs. 3 In recent years, new surgical techniques have emerged, such as vertebroplasty (VP) or kyphoplasty (KP), which mainly consist of the percutaneous injection of acrylic bone cement into a damaged vertebra to reduce the pain by sta- bilizing the vertebral body. 6 KP, moreover, entails the inflation of a balloon tamp prior to the injection in an attempt to restore vertebral body height and reduce the kyphotic deformity. 7 Up to now, physicians have adapted classical acrylic formulations to these techniques, 8 on the one hand by increasing radiological visibility by means of adding high atomic number metals in powder form, such as barium, tantalum or tungsten. 9,10,11 In our case to prevent the need for this intervention by the physician, our group has worked on this by adding bismuth salicylate (BS) as a radiopacifier to a cement formulation and have obtained good results. 12,13 On the other hand, in an attempt to inject the cement through the needle easily and also to increase the working time, some physicians reduce the viscosity by adding more monomer to the cement mixture 14 or by chill- ing the constituents of the cement prior to the mixing. 15 In a previous study, we found that the use of polymethyl methacrylate (PMMA) beads of bigger size and low molec- ular weight is a better way to decrease maximum curing temperature and increase the working time. 16 Moreover, de- spite the low incidence of infection in these procedures, 17 apart from preoperative intravenous antibiotics, 18 inciden- ces of the addition of powdered antibiotics to the cement formulation have been reported in the operating theater. 11 In light of the reality described above, the aim of this work is to formulate ALBCs for specific use in VP and KP, and to study the effect of the addition of two antibiot- Correspondence to: M. Gurruchaga (e-mail: [email protected]) ' 2008 Wiley Periodicals, Inc. 312
-
Upload
lidia-hernandez -
Category
Documents
-
view
214 -
download
1
Transcript of New injectable and radiopaque antibiotic loaded acrylic bone cements

New Injectable and Radiopaque Antibiotic Loaded AcrylicBone Cements
Lidia Hernandez, M. Eugenia Munoz, Isabel Goni, Marilo Gurruchaga
Universidad del Paıs Vasco 20009-San Sebastian, Spain
Received 26 December 2006; revised 22 January 2008; accepted 25 January 2008Published online 7 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.b.31105
Abstract: The use of antibiotic loaded bone cements (ALBCs) has become a common clinical
practice in the prevention and treatment of prosthesis-related infections. However, due to
antibiotic resistance, there is a general interest in broadening the antibacterial spectrum of
currently used drugs. The aim of this work is to formulate ALBCs for specific use in
vertebroplasty and kyphoplasty, and to study the effect of the addition of ciprofloxacin alone
and in combination with vancomycin on some properties of the cement. The cements were
formulated using bismuth salicylate as the radiopacifier. The setting properties, residual
monomer content, release of antibiotics, rheological behavior, injectability, and mechanical
properties of these formulations were studied. They showed long setting times and low curing
temperatures. From the release studies, antibacterial properties are assumed because the
concentration of released antibiotic was higher than the minimum effective. Although the
experimental cements had slightly reduced mechanical properties, the other alterations shown
were negligible. ' 2008 Wiley Periodicals, Inc. J Biomed Mater Res Part B: Appl Biomater 87B: 312–320,
2008
Keywords: bone cement-PMMA; antimicrobial; vertebral; viscosity, mechanical properties
INTRODUCTION
One of the first modifications of acrylic bone cements con-
cerns one of the more serious complications of orthopedic
surgery: bacterial bone infections (osteomyelitis).1 In the
early 70s, Buchholtz and Engelbrecht2 already included
gentamicin sulphate (GS) in a standard formulation to treat
an infection in a total hip arthroplasty.2 Thanks to their
success, the use of antibiotic loaded bone cements
(ALBCs) has become common clinical practice in the pre-
vention and the treatment of prosthesis-related infections3
with the aim of attaining high local drug levels, while
maintaining low systemic levels.4 Apart from GS, other
antibiotics such as erythromycin, clindamycin or tobramy-
cin5 are also being used as additives for bone cements.
However, due to antibiotic resistance, there is a growing in-
terest in the addition of other antibiotics or mixtures of
antibiotics to bone cements, which broadens the antibacte-
rial spectrum of currently used drugs.3
In recent years, new surgical techniques have emerged,
such as vertebroplasty (VP) or kyphoplasty (KP), which
mainly consist of the percutaneous injection of acrylic bone
cement into a damaged vertebra to reduce the pain by sta-
bilizing the vertebral body.6 KP, moreover, entails the
inflation of a balloon tamp prior to the injection in an
attempt to restore vertebral body height and reduce the
kyphotic deformity.7 Up to now, physicians have adapted
classical acrylic formulations to these techniques,8 on the
one hand by increasing radiological visibility by means of
adding high atomic number metals in powder form, such as
barium, tantalum or tungsten.9,10,11 In our case to prevent
the need for this intervention by the physician, our group
has worked on this by adding bismuth salicylate (BS) as a
radiopacifier to a cement formulation and have obtained
good results.12,13 On the other hand, in an attempt to inject
the cement through the needle easily and also to increase
the working time, some physicians reduce the viscosity by
adding more monomer to the cement mixture14 or by chill-
ing the constituents of the cement prior to the mixing.15 In
a previous study, we found that the use of polymethyl
methacrylate (PMMA) beads of bigger size and low molec-
ular weight is a better way to decrease maximum curing
temperature and increase the working time.16 Moreover, de-
spite the low incidence of infection in these procedures,17
apart from preoperative intravenous antibiotics,18 inciden-
ces of the addition of powdered antibiotics to the cement
formulation have been reported in the operating theater.11
In light of the reality described above, the aim of this
work is to formulate ALBCs for specific use in VP and
KP, and to study the effect of the addition of two antibiot-
Correspondence to: M. Gurruchaga (e-mail: [email protected])
' 2008 Wiley Periodicals, Inc.
312

ics on some properties of the cement, such as setting prop-
erties, residual monomer content, release of antibiotics,
rheological behavior, injectability and mechanical proper-
ties. Ciprofloxacin (CFX) alone and in combination with
vancomycin (VM) were chosen for this study. The high
penetration depth of CFX into bone and the success of the
combined therapy for the elimination or prevention of
implants infection in hip surgery were the reasons for
including these antibiotics in the new cements.19
MATERIALS AND METHODS
Materials and Specimen Preparation
Table I summarizes the formulations studied: two commer-
cially available (I and II) and three experimental (III to V)
loaded with BS as the radiopacifier and CFX and VM, as
antibiotics.
The experimental formulations were prepared using a
solid: liquid ratio of 2:1. The liquid component consisted
of methylmethacrylate (MMA, Merck) monomer and N,N-
dimethyl-p-toluidine (Merck, 1 wt % with respect to the
liquid phase), in all cases. The solid component consisted
of benzoyl peroxide (Merck, 1.25 wt % with respect to the
solid phase), 10% of BS (Fluka), the corresponding antibi-
otic (pure CFX was purchased from Fluka and the VM
hydrochloride from Normon. The PMMA beads employed
in the solid phase were a mixture of Colacryl DP300
(Lucite) and Plexigum (Rohm and Haas) in a ratio of
80/2016 (wt).
The preparation of commercial cement samples was car-
ried out according to the manufacturer’s instructions. The
components of bone cement were hand-mixed and before
the dough state was reached the mass was placed in the
corresponding Teflon mould and allowed to cure for 1 h at
378C.Either for the experimental formulation specimen’s prep-
aration or their characterization, the methods described in
the ISO 5833 standard for bone cements used in arthro-
plasty20 were followed. However, we must take into
account that there are not specific rules for VP cements.
Curing Parameters
Exotherms of the polymerisation were registered in compli-
ance with ISO 5833.20 The mixture was introduced in a
Teflon mould connected to a high sensitivity thermotester
and the changes in temperature were recorded as a function
of the time from the moment of mixing. The maximum
temperature (Tmax) attained by the bulk was recorded and
the setting time (tset) was determined as the time taken to
reach a temperature midway between room temperature
and Tmax. The given values are the mean of at least two
determinations, as required by the ISO standard.
Residual Monomer Content
Proton nuclear magnetic resonance (1H NMR) spectroscopy
was selected to determine the percentage of residual mono-
mer. 20 mg of cement cured for 1 h at 378C were dissolved
in deuterated chloroform containing tetramethylsilane as
the internal standard to obtain the 1H NMR spectra using a
FT-NMR Bruker spectrophotometer operating at 300 MHz.
To assign the peaks and estimate the residual MMA con-
tent we took into account the references given by other
authors.21 Measurements were performed in triplicate.
Mechanical Properties
Compressive properties were determined according to the
ISO 5833 standard.20 Specimens testing was carried out af-
ter 24 h of storage in air at room temperature. At least six
12-mm high and 6-mm wide cylinders were tested for each
formulation on the 4301 INSTRON testing machine
equipped with a cell load of 100 kN, with a cross-head dis-
placement of 22 mm/min. Additional tests were performed
on the specimens after 1 month of immersion in saline so-
lution at 378C.The bending tests were performed in three-point bending
mode, and following the ISO 5833 standard specifica-
tions.20 At least six specimens (75 3 10 3 3.3 mm3) were
tested on a 4301 INSTRON machine after conditioning
the samples in water at 378C for 50 h. The displacement
rate for the bending tests was 5 mm/min. After tests, frac-
ture surfaces were examined by scanning electron micros-
copy (SEM) in a Hitachi S-2700 with an accelerating
voltage of 15 kV. Previously, samples were gold coated
(Fine Coat Ion Sputter JFC-1100).
Izod impact testing was carried out according to the
ASTM D256 standard.22 The specimens measured 63.5 312.7 3 6.35 mm3 and were machined to obtain a notch of
458, with a radius of 0.25 mm and a depth under the notch
of 10.16 mm. No fewer than 10 specimens were tested in a
CEAST 6548/000 pendulum equipped with a 1 J hammer.
Rheological Behavior and Injectability
Rheological oscillatory measurements were selected to
characterize the viscoelastic phase of the cement between
TABLE I. Brief Description of the Acrylic BoneCements Studied
Formulation Main Characteristics
I (Simplex P) Radiopaque Cement (10% BaSO4)
II (Osteopal G) Radiopaque Cement (10% ZrO2), loaded
with antibiotic (GS)
III Radiopaque Cement (10% BS)
IV Radiopaque cement (10% BS), loaded with
antibiotic (5% CFX)
V Radiopaque Cement (10% BS), loaded with
a mixture of antibiotics (3% CFX 13%VM)
313INJECTABLE RADIOPAQUE ANTIBIOTIC LOADED CEMENT
Journal of Biomedical Materials Research Part B: Applied Biomaterials

the mixing and the complete setting by means of complex
(or true) viscosity (g*), since this parameter contain both
the real (elastic) and loss (viscous) components.23 Evolu-
tion of g* as a function of time was measured in a Rheo-
metric Ares rheometer in dynamic oscillation mode using
plate-plate configuration, at a frequency of 1 Hz. The ra-
dius of the plates was 25 mm and the gap between the
plates was 2 mm. The rheometer was used in a constant
strain mode with strain amplitude of 1% and measurements
were conducted at room temperature (258C). A significant
benefit of this technique is the ability to extract viscoelastic
parameters such as the storage (G0) and loss moduli (G00)and their ratio, called loss tangent (tan d 5 G00/G0).24
For the Injectability tests, we followed the method pro-
posed by other authors.25 Injectability (I%) was defined as
the weight percent of cement injected into a Teflon recipient,
expressed as a percentage of the total amount of cement
charged into the syringe. Time of mixing was considered as
the time needed to reach a homogeneous mass ready to be
injected. In order to ascertain the time during which the
cement had the appropriate consistency and fluidity to be
injected (the injection time), tests were performed slowly until
the solidity of the mass impeded the injection.
Water Uptake Capacity
Taking into account the high presence of water in the
human body, water absorption of any polymeric material is
of importance for surgical applications since it influences
the mechanical properties of the cement and monomer
release. Moreover, in this case in which the salicylic salt is
used as radiopacifier, water absorption can to the hydrolysis
of the salt and the subsequent release of salicylic acid.12,13
Thus, specimens were immersed in phosphate buffered sa-
line (PBS, pH 5 7.4) at 378C for 1 month. Water absorp-
tion (%A) and the percentage of elution (%E) of the
cements were calculated using the following expressions
[Eqs. (1) and (2)]26:
%A ¼ Mw �Mf
M0
3 100 ð1Þ
%E ¼ M0 �Mf
M0
3 100 ð2Þ
where M0 is the dry sample weight, Mf the dry weight after
testing and Mw the weight at the equilibrium absorption
point.
Release of Antibiotics
The release experiments were performed using cement
sheets measuring 10 3 25 3 1 mm3, by two different
methods: In the first experiment, the determination of the
GS released from Osteopal G was performed by immersing
the cement sheet in 100 mL of PBS. The measurements
were taken from an aliquot of 10 mL, which was immedi-
ately replaced with fresh PBS. In the second case, the
quantities of GS released were measured at 332 nm by
means of the UV-spectrophotometry (UV CECIL CE2041)
following the derivatizing method described by Zhang
et al.27 The relationship between UV absorption and con-
centration was determined by means of solutions of differ-
ent known concentrations, giving a linear plot (C 561.91A, r 5 0.9971).
Because of the simultaneous release of salicylic acid,
CFX and VM from formulations IV and V, high perform-
ance liquid chromatography (HPLC) was employed to sepa-
rate the substances released before their quantification.
Specimens’ sheets were immersed onto 15 mL of PBS and
incubated without stirring. Samples of 0.500 mL were
taken at different times, and immediately replaced with
fresh solution. The HPLC equipment consisted of a Perking
Elmer LC-250 pump, a UV-VIS detector Perking Elmer
LC-95, and a Waters lBoundapack 3.9 3 300 mm C-18
column. The wavelengths used were 272 nm for CFX and
211 nm for VM. The separation of CFX required the addi-
tion of a counterion (PIC A, Waters), so the mobile phase
for the determination of CFX was a methanol/ aqueous so-
lution of PIC-A (60:40). For the determination of VM a
methanol/water (80:20) solution was used as the mobile
phase at the same flow rate, which was 1 mL/min. The reten-
tion time of the CFX and VM peaks relative to the standard
were 5.7 and 6.8 min. The calibration curves were obtained
for the complete set of measurements, displaying correlation
coefficients of 0.999 for CFX and 0.994 for VM. Samples
were assayed in duplicate.
Radiopacity
The X-ray photograph of the cement specimens was taken
using a standard clinical General Electric X-ray instrument
(set at 25 KV and 11 MAS). The specimens were rectangu-
lar sheets measuring 25 3 10 3 1 mm3.
Statistical Analysis
Results were evaluated using the one-way Anova statistical
analysis with respect to the reference formulations. The
error protection method used in this research was the Fisher
PLSD method and the confidence interval used was 95%.
Because of the obvious differences between the com-
mercial cements and experimental formulations, the statisti-
cal analysis was focused on the radiopaque cement with
10% of BS (Formulation III). Taking this cement as a ref-
erence, comparisons were made between commercial
cements and the new formulations.
RESULTS
Setting Parameters
As we can see from the setting diagrams (Figure 1), experi-
mental formulations (III to V) exhibit significantly higher
314 HERNANDEZ ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials

setting times than commercial cements, and significantly
lower maximum temperatures. As we have demonstrated in
a previous study, this is due to a careful selection of the
PMMA beads employed in the solid phase of the experi-
mental formulations.16 The characteristics of these beads
(particle size overall) make possible to obtain optimum
cement setting at long polymerization times and not very
high polymerization temperatures. In this case, it is also
important to point out that the addition of these quantities
of powdered CFX and VM did not affect the polymeriza-
tion kinetics, since no significant differences were found
between the curing parameters (Tmax and tset) of experimen-
tal cements.
Residual Monomer Content
Results of the determination of the residual monomer con-
tent are shown on Table II. The differences observed ini-
tially in the setting kinetics did not significantly affect the
residual monomer content, which remained at similar val-
ues for all cement samples after 1 h of setting at 378C.
Mechanical Properties
Compressive Properties. The results of the compres-
sion tests are given in Table III and indicate that, in dry
specimens, the addition of antibiotics does not significantly
affect the compressive strength (rc) or Young’s modulus
(Ec) of the experimental formulations. Immersion in saline
solution for 1 month decreases both parameters due to the
plastizicing effect of the absorbed water and the porosity
induced by the release of antibiotics and salicylic acid.
This is more noticeable in formulation V due to its higher
weight loss and release, giving a significant decrease of the
compression parameters with respect to Formulation III.
The compressive parameters of experimental cements are
comparable with commercial ones and all specimens
showed a higher rc than the minimum value required by
the ISO 5833 standard (70 MPa). On the other hand, it has
to be clearly stated that Table III shows results at two dif-
ferent time points and two different test conditions and,
consequently, the presented values are not comparable.
Bending Tests. The bending strength (B) and modulus
(E) of all formulations are also presented on Table III. All
experimental formulations show significantly lower values
of B than commercial bone cements, and the values are
below the minimum value required by the ISO standard
(50 MPa). This is probably due to the poorer dispersion of
the ingredients in these cements compared with that of the
commercial ones, as can be seen in the fracture surfaces
examined by SEM (Figure 2). Since there are no significant
differences between experimental formulations, we can
deduce that the addition of antibiotics does not further
deteriorate the bending strength of the experimental
cements. Regarding the modulus, except for the significant
increase found in Simplex P, the rest of the formulations
do not show differences in this parameter, which complied
with the ISO standard (E[ 1800 MPa).
Impact Strength. Determining the impact strength is im-
portant for acrylic implants since a strong positive relation
was found between this parameter and fracture toughness.28
Regarding impact strength results (Table III), once again
Simplex P showed significant superiority, whereas Osteopal
G and Formulation III did not show statistical differences.
In this test, the addition of antibiotics weakened the
cements, since a significant decrease impact resistance was
observed in Formulations IV and V with respect to Formu-
lation III.
Figure 1. Exotherms of polymerization of all formulations studied.
TABLE II. Residual Monomer Content After 1 h of Curing at 378C (% Mr), Results of the InjectabilityTests and Water Uptake Behavior of the Various Formulations
Formulation % Mr (mol)
Injectability Tests Water Uptake
Time of Mixing (min) Injection Time (min) I (%) A (%) E (%)
I (Simplex P) 2.60 (0.25) – – – 1.29a (0.01) 0.00a (0.00)
II (Osteopal G) 2.03 (0.38) 1a 2.0 45.94a (5.73) 2.89a (0.09) 0.50a (0.13)
III 2.34 (0.45) 3 5.8 80.11 (4.68) 2.16 (0.10) 0.72 (0.10)
IV 1.92 (0.11) 3 6.4 74.55a (3.05) 2.01 (0.09) 0.74 (0.14)
V 2.50 (0.23) 3 6.2 75.19a (5.56) 2.62a (0.04) 1.22a (0.10)
Results are given as mean and standard deviation (SD) in parentheses.a Values with significant differences with respect to Formulation III (p\ 0.05).
315INJECTABLE RADIOPAQUE ANTIBIOTIC LOADED CEMENT
Journal of Biomedical Materials Research Part B: Applied Biomaterials

Rheological Behavior and Injectability
Figure 3 (upper) shows performance during the curing of
complex viscosity (g*) versus elapsed time from mixing
for all formulations, which reflects the different characteris-
tics of each type of cement and the different ways in which
they are intended to be used.24 Simplex P is a hand-dough
usage cement, which quickly reaches quite high values of
g* that remain stable during working time. After this, due
to its early curing, its g* increases very quickly. Osteopal
G is sold as ‘‘low viscosity cement.’’ We can see that it
really does exhibit low values of g*. However, we can
observe that due to the early setting of this cement there is
a very rapid increase of g* at about 5–6 min after the mix-
ing. The three experimental cements, which are formulated
for injectable use, at the very outset of the experiment,
showed initial values of g* similar to Osteopal G, but due
to their delayed setting, the g* remain almost constant at
these low values for longer times.
Figure 4 shows the plots of G0, G00 (upper), and tan d(G00/G0) (down) for all the cements. Although initially G00
tends to be greater than G0, from the moment that we can
see in the figure, G0 is greater than G00 and both compo-
nents increase over time. However, G0 increases more rap-
idly since the material changes from being predominantly
viscous to being predominantly elastic. This becomes evi-
dent when we observe the decrease of tan d over time. As
in the previous tests, the addition of antibiotics did not
affect, for a long period, the behavior of the experimental
formulations.
Results of the injectability tests are shown in Table II
except for formulation I, which is formulated for hand-
dough usage. These values corroborate the rheological
behavior observed before, since all experimental formula-
tions show similar results, that is, higher injectability val-
ues and longer injection times than Osteopal G, due to
their longer setting times. Differences between injectability
parameters of the experimental formulations did not reach
statistical significance (p[ 0.05) and the addition of antibi-
otics did not change the injection behavior of the cement
formulations, as expected from rheological results.
Water Uptake Capacity
Results for absorption (A) and elution (E) are also shown
in Table II. Simplex P has a moderate water uptake and a
negligible weight loss after 1 month of immersion in saline
solution. The rest of the formulations showed a significant
increase in these parameters due to the higher polarity of
the ingredients of these formulations. Regarding the elution
results, which give us an idea of the total release of sub-
stances from the cements, all experimental formulations
experienced a lost of weight due to the release of salicylic
acid. Formulations III and IV did not show statistical differen-
ces between them despite the incorporation of CFX to the for-
mulation, which could be attributable to the low solubility of
CFX or even to the affinity for the polymer.29 However, the
addition of a more soluble antibiotic as in the case of VM
obviously enhanced the weight loss of the cement.
Antibiotic Release
Release kinetic plots obtained for all the antibiotic-loaded
formulations are shown in Figure 5. In many cases, release
was fast at the beginning of the experiment due to the dis-
solution of the particles located at or near the surface of
the specimen, which is called ‘‘burst effect.’’ In fact, we
have observed this ‘‘burst effect’’ for GS in Osteopal G
cement and for VM in formulation V. However, for CFX,
we did not observe the burst effect. After 1 month, we can
consider that release is almost finished. If we observe the
kinetics, CFX is released at significantly lower percentages
than GS and VM. There is a trend showing more gradual
release of CFX in formulation V due to the incorporation
of VM. However, the difference did not reach statistical
significance.
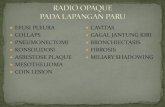
Radiopacity
Minimally invasive techniques for spinal surgery, such as
VP or KP, require injectable materials with high radiopac-
ity to accurately follow the evolution of the cement within
the vertebral body. Figure 6 shows the X-Ray image of the
TABLE III. Mechanical Properties of the Cements Studied: Compressive Strength (rc) and Modulus (Ec),Bending Strength (B) and Modulus (E), and the Impact Resistance (IR)
Formulation
Compression Tests
Bending Tests Impact TestsDry Specimens Wet Specimens
rc (MPa) Ec (MPa) rc (MPa) Ec (MPa) B (MPa) E (MPa) I R (KJ/m2)
I (Simplex P) 112a (3) 1590a (60) 105a (4) 1545a (60) 81a (5) 2600a (80) 1.06a (0.03)
II (Osteopal G) a104 (4) a1740 (40) 1a93 (1) a1340 (80) a67 (3) a2310 (220) a0.91 (0.07)
III a104 (2) a1780 (70) 1a94 (3) a1695 (50) a41 (3) a2500 (70) a0.85 (0.06)
IV a105 (4) a1825 (65) 1a93 (2) a1680 (20) a39 (1) a2480 (90) 0.75a (0.05)
V a101 (4) a1840 (60) 185a (4) a1740 (60) a41 (1) a2470 (70) 0.71a (0.06)
For the compression tests, results of dry and wet specimens (soaked in saline solution at 378C for 1 month) are presented. Results are given as mean and standard deviation
(SD) in parentheses.a Values with significant differences with respect to Formulation III (p\ 0.05).
316 HERNANDEZ ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials
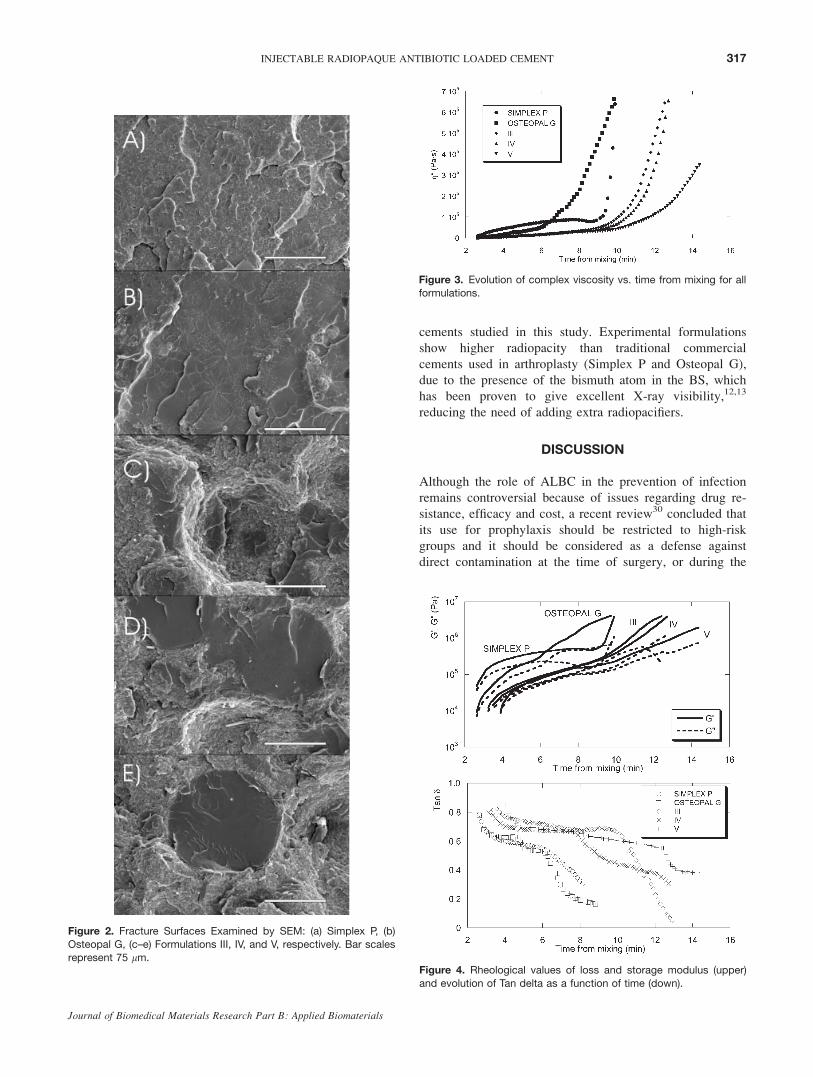
cements studied in this study. Experimental formulations
show higher radiopacity than traditional commercial
cements used in arthroplasty (Simplex P and Osteopal G),
due to the presence of the bismuth atom in the BS, which
has been proven to give excellent X-ray visibility,12,13
reducing the need of adding extra radiopacifiers.
DISCUSSION
Although the role of ALBC in the prevention of infection
remains controversial because of issues regarding drug re-
sistance, efficacy and cost, a recent review30 concluded that
its use for prophylaxis should be restricted to high-risk
groups and it should be considered as a defense against
direct contamination at the time of surgery, or during the
Figure 2. Fracture Surfaces Examined by SEM: (a) Simplex P, (b)
Osteopal G, (c–e) Formulations III, IV, and V, respectively. Bar scales
represent 75 lm.
Figure 3. Evolution of complex viscosity vs. time from mixing for all
formulations.
Figure 4. Rheological values of loss and storage modulus (upper)
and evolution of Tan delta as a function of time (down).
317INJECTABLE RADIOPAQUE ANTIBIOTIC LOADED CEMENT
Journal of Biomedical Materials Research Part B: Applied Biomaterials

postoperative period as the wound seals. Thus the research
of new formulation of ALBC must go on.
The new highly radiopaque and injectable cements
loaded with antibiotics formulated in this research for spe-
cific use in the field of vertebroplasty or kyphoplasty,
showed long setting times, which is positive when consid-
ering their injectablility, as their viscosities remained at
low values for longer times than conventional cements.
Moreover, their low curing temperatures minimize the ther-
mal damage to the surrounding tissues. In the cases in
which low polymerization temperature are attained, the
measurement of monomer presence is particularly impor-
tant to demonstrate the high polymerization yield. This pa-
rameter remained at similar values for all cement samples
after 1 h of curing at body temperature.
Because of the variety of methods reported in bibliogra-
phy, it is difficult to establish proper comparisons between
the different studies realized about the effect of the addi-
tion of antibiotic on the mechanical performance of the
cements.31 In general, a weakening effect is observed as a
result of the presence of differentiated particles,5 since anti-
biotic particles act as voids or defects. The greater the anti-
biotic concentration the bigger the antibiotic domains from
which rupture initiates.32–35 In general, the compression
strength is not affected by small additions of antibiot-
ics.31,32,35,36 However, at higher percentages, this parameter
can decrease below the minimum required by the ISO
standard (70 MPa).35,36 The effect is more noticeable in
flexural tests34,36 and, above all, in fatigue tests, since in
these assays there is a significant decrease of the fatigue
life with the addition of small quantities of antibiotics to
the cement formulation.32,33,37 With the aim of minimizing
the detrimental effects of the addition of antibiotics, some
authors recommend the use of commercial formulations
with antibiotics included. These formulations are more con-
sistent and homogeneous than hand-mixed ones, which can
show lower strengths.2 Other options to improve the
cements properties are the vacuum mixing or the centrifu-
gation of the formulation, two processes which result in a
lower porosity and in an enhancement of the fatigue life.
However, the lower porosity will hinder the release of anti-
biotics.
In our study, as expected from the studies reported
above, the addition of antibiotics did not affect the com-
pression performance of the new cements, which complied
with the standard even after 1 month of immersion in
saline medium. However, the flexural test for experimental
cements showed low values and impact strength, which has
been correlated previously with the fatigue performance of
the cements, decreased with the addition of antibiotics. It
has been shown from fracture surfaces (Figure 2) that
whereas commercial cements showed smooth surfaces
where any of the ingredients could be distinguished, the ex-
perimental cements show differentiated particles, which
corresponds to BS, CFX, or VM. So, either dissolution of
the radiopacifier12 or the mechanical mixing of the constit-
uents is considered to be able to produce a more consistent
and reproducible mixture, thus enhancing the mechanical
properties of these formulations.28 This affirmation is based
on the studies of other authors.31,32 In one of them,32 they
found that bone cements in which tobramycin had been
hand-blended was weaker than their prepackaged counter-
part.
The results from the rheological study and the injectabil-
ity tests emphasize again the differences between the com-
mercial and our new formulations specifically designed to
maintain low viscosity for use as cements in vertebroplasty.
As we have demonstrated in the previous studies,12,16 the
slower the decrease of tan d, the easier the cement is to
inject. Thus, the fast increase of the viscosity and the ear-
lier decrease of tan d showed by the commercial cements
indicate the lack of suitability for use as formulations in
VP and KP. These observations are in accordance with the
results of the injectability tests, that is, higher injectability
values and longer injection times for the experimental
cements compared with the commercial cements.
The release of active substances from the cement matrix
is affected by a number of factors, from which we can
highlight: (a) the kind and number of antibiotics38; (b) their
concentration—higher concentrations give as a result an
increase of the total amount of antibiotic released. This is
due to the fact that the ‘‘extra’’ antibiotic acts as a soluble
additive that leaves a network of void or holes, thus pro-
moting a higher release. Taking this into account, the addi-
Figure 6. X-Ray Photograph of the bone cements studied.
Figure 5. Release of GS from Osteopal G, CFX from formulations
IV and V, and VM from formulation V.
318 HERNANDEZ ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials

tion of soluble additives, such as lactose39 or polivinilpirro-
lidone40 has been reported in a bid to increase the total
amount of antibiotic released; (c) the cement itself: its po-
rosity, chemical composition, its surface characteristics (to-
pography, surface area), the technique of mixing the
ingredients of the formulation (vacuum mixing decreases
porosity), or the addition of antibiotic with or without a
mixer; (d) the characteristics of the release medium (stir-
ring, temperature, volume, or composition) also affect to
the results of the release experiment. All these factors and
the lack of standardized release experiments give as a con-
sequence conflicting results in no end of reported studies.
Moreover, In vivo new factors can be considered, for
instance, the composition of the surrounding medium,
which is obviously different from the physiological
mediums used in the release studies.
Nevertheless, most studies are in keeping with the
releasing mechanism. The antibiotics release in two steps:
first, there is a rapid dissolution of the antibiotic located at
or near the surface, which is essentially a surface phenom-
enon. Usually, an immediate dissolution of antibiotic can
be measured; this is called ‘‘burst effect.’’ After this, there
is a long and gradual release of the antibiotic located at
inner zones of the specimen, which can continue during
some days or months. It has been proven41 that at this
stage of the experiment, the drug is released as the water
absorption process is completed and the release pathways
are created.
In our experiments, we can consider that release is
almost finished after 1 month. If we observe the kinetics,
we can affirm that solubility of the drug is essential for the
release process, since CFX (low solubility, pure) is released
at significantly lower percentages than GS and VM. There
is a trend showing more gradual release of CFX in formu-
lation V due to the incorporation of VM. This leads us to
believe that the porosity induced by the release of VM
would enhance the release of CFX. However, the difference
did not reach statistical significance. It seems that low solu-
bility and the influence of the PMMA are of greater impor-
tance than the diffusion. We must add that even if the
release of CFX was very slow, the quantities released are
far greater than the minimum inhibitory concentration,
which has been reported to be 0.125 lg/l42.The greater X-ray visibility showed by experimental
cements makes them very suitable for use in vertebroplasty
and kyphoplasty. We are confident that the use of powder
mixing techniques or the dissolution of the radiopaci-
fier12,13 would improve the homogeneity and the visibility
even more.
CONCLUSIONS
The new highly radiopaque and injectable cements loaded
with antibiotics formulated for specific use in the field of
VP or KP showed long setting times, which is positive
when considering their injectability, as their viscosities
remained at low values for longer times than conventional
cements. Moreover, their low curing temperatures minimize
the thermal damage to the surrounding tissues.
The release of the antibiotics tested in this research
seem to offer antibacterial properties to the cements since
the concentration attained was higher than the effective
minimum.
In spite of experimental cements did not show better me-
chanical properties than standard cement, we observed that
the addition of antibiotics did not affect the compression per-
formance of the new cements, which complied with the stand-
ard even after 1 month of immersion in saline medium.
Moreover, we are confident about the improvement of the
flexural and impact tests results by using industrial mixing
methods or using the salicylic salt dissolved in the monomer.
REFERENCES
1. Torrado S, Frutos P, Frutos G. Gentamycin bone cements:Characterization and release (in vitro and in vivo assays). IntJ Pharm 2001;217:57–69.
2. Buchholtz HW, Engelbrecht H. Uber die Depotwirkungciniger Antibiotica bei Vermischung mitdem Kunstharz Pala-cos. Chirurg 1970;41:511–515.
3. Hendriks JGE, van Horn JR, van der Mei HC, Busscher HJ.Backgrounds of antibiotic-loaded bone cement and prosthesis-related infection. Biomaterials 2004;25:545–556.
4. Dıez-Pena E, Frutos G, Frutos P, Barrales-Rienda JM. Genta-micin sulphate release from a modified commercial acrylicsurgical radiopaque bone cement. I. Influence of the gentami-cin concentration on the release process mechanism. ChemPharm Bull 2002;50:1201–1208.
5. Kuhn K-D. Bone cements: Up-to-date comparison of physicaland chemical properties of commercial materials. Heidelberg:Springer Verlag; 2000. 149p.
6. Garfin SR, Reilley MA. Minimally invasive treatment ofosteoporotic vertebral body compression fractures. Spine J 2002;2:76–80.
7. Ortiz AO, Zoarski GH, Beckerman M. Kyphoplasty. TechVasc Interv Radiol 2002;5:239–249.
8. Jasper lE, Deramond H, Mathis JM, Belkoff SM. Materialproperties of various cements for use with vertebroplasty.J Mat Sci: Mat Med 2002;13:1–5.
9. Moreland DB, Landi MK, Grand W. Vertebroplasty: Techni-ques to avoid complications. Spine J 2001;1:66–71.
10. Martin JB, Jean B, Sugiu K, San Millan Ruiz D, Piotin M,Murphy K, Rufenacht B, Muster M, Rufenacht A. Vertebro-plasty. Clinical experience and follow-up results. Bone 1999;25 (Suppl):11S–15S.
11. Theodorou DJ, Theodorou SJ, Duncan TD, Garfin SR, WongWH. Percutaneous balloon kyphoplasty for the correction ofspinal deformity in painful vertebral body compression frac-tures. Clin Imag 2002;26:1–5.
12. Hernandez L, Fernandez M, Collıa F, Gurruchaga M, Goni I.Preparation of acrylic bone cements for vertebroplasty withbismuth salicylate as radiopaque agent. Biomaterials 2006;27:100–107.
13. Hernandez L, Vazquez B, Lopez-Bravo A, Parra J, Goni I,Gurruchaga M. Acrylic bone cements with bismuth salicylate:Behaviour in simulated physiological conditions. J BiomedMater Res A 2007;80:321–332.
14. Belkoff SM, Sanders JC, Jasper LE. The effect of the mono-mer-to-powder ratio on the material properties of acrylic bonecement. J Biomed Mater Res B 2002;63:396–399.
319INJECTABLE RADIOPAQUE ANTIBIOTIC LOADED CEMENT
Journal of Biomedical Materials Research Part B: Applied Biomaterials

15. Hide IG, Gangi A. Percutaneous vertebroplasty: History,technique and current perspectives. Clin Radiol 2004;59:461–467.
16. Hernandez L, Gurruchaga M, Goni I. Influence of powderparticle size distribution on complex viscosity and other prop-erties of acrylic bone cement for vertebroplasty and kypho-plasty. J Biomed Mat Res Part B Appl Biomater 2006;77:98–103.
17. Walker DH, Mummaneni P, Rodts GE Jr. Infected vertebro-plasty. Report of two cases and review of the literature.Neorosurg Focus 2004;17:E6.
18. Mathis JM, Wong W. Percutaneous vertebroplasty: Technicalconsiderations. J Vasc Interv Radiol 2003;14:953–960.
19. Tunney MM, Ramage G, Patrick S, Nixon JR, Murphy PG,Gorman SP. Antimicrobial susceptibility of bacteria isolatedfrom orthopedic implants following revision hip surgery.Antimicrob Ag Chemother 1998;42:3002–3005.
20. International Standard ISO 5833. Implants for bone surgery—Acrylic resin cements; 2002.
21. Pascual B, Vazquez B, Gurruchaga M, Goni I, Ginebra P, GilJ, Planell JA, Levenfeld B, San Roman J. New aspects of theeffect of size and size distribution on the setting parametersand mechanical properties of acrylic bone cements. Biomateri-als 1996;17:509–516.
22. ASTM D256-00. Standard test methods for determining theIzod pendulum impact resistance of plastics.
23. Lewis G, Carroll M. Rheological properties of acrylic bonecement during curing and the role of the size of the powderparticles. J Biomed Mater Res B 2002;63:191–199.
24. Farrar DF, Rose J. Rheological properties of PMMA duringcuring. Biomaterials 2001;22:3005–3013.
25. Mendez JA, Fernandez M, Gonzalez-Corchon A, Salvado M,Collıa F, de Pedro JA, Levenfeld BL, Lopez-Bravo A, Vaz-quez B, San Roman J. Injectable self-curing bioactive acrylic-glass composites charged with specific anti-inflammatory/anal-gesic agent. Biomaterials 2004;25:2381–2392.
26. Domingo C, Arcıs RW, Lopez-Macipe A, Osorio R, Rodrı-guez-Clemente R, Murtra J, Fanovich MA, Toledano M. Den-tal composites reinforced with hydroxyapatite: Mechanicalbehaviour and absorption/elution characteristics. J BiomedMater Res A 2001;56:297–305.
27. Zhang X, Wyss UP, Pichora D, Goosen MFA. A mechanisticstudy of antibiotic release from biodegradable poly(d,1-lac-tide) cylinders. J Controlled Release 1994;31:129–144.
28. Lewis G, Mladsi S. Relationship between fracture toughnessand impact strength of acrylic bone cement. Crit Rev BiomedEng 2000;28:451–455.
29. DiCicco M, Duong T, Chu A, Jansen SA. Tobramycin andgentamycin elution analysis between two in situ polymeriz-able orthopedic composites. J Biomed Mat Res Part B ApplBiomat 2003;65B:137–149.
30. Jiranek WA, Hanssen AD, Greenwald AS. Antibiotic-loadedbone cement for infection prophylaxis in total joint replace-ment. J Bone Joint Surg 2006;88:2487–2500.
31. Chohfi M, Langlais F, Fourastier J, Minet J, Thomazeau H,Cormier M. Pharmacokinetics, uses, and limitations of vanco-mycin-loaded bone cement. Int Orthop 1998;22:171–177.
32. Klekamp J, Dawson J, Haas D, DeBoer D, Christie M. Theuse of vancomycin and tobramycin in acrylic bone cement.Biomechanical effects and elution kinetics for use in jointarthroplasty. J Arthroplasty 1999;14:339–346.
33. Weisman DL, Olmstead ML, Kowalski JJ. In vitro evaluationof antibiotic elution from polymethylmethacrylate (PMMA)and mechanical assessment of antibiotic-PMMA composites.Vet Surg 2000;29:245–251.
34. Davies JP, Harris WH. Effect of hand mixing tobramycin onthe fatigue strength of Simplex P. J Biomed Mat Res 1991;25:1409–1414.
35. Armstrong MS, Spencer RF, Cunningham JL, Gheduzzi S,Miles AW, Learmonth ID. Mechanical characteristics of anti-biotic-laden bone cement. Acta Orthop Scand 2002;73:688–690.
36. Lautenschlager EP, Jacobs JJ, Marshall GW, Meyer PR Jr.Mechanical properties of bone cements containing large dosesof antibiotic powders. J Biomed Mater Res 1976;10:929–938.
37. Schurman D, Swenson L, Piziali R. Bone cement with andwithout antibiotics: A study of the mechanical properties. In:Proceedings of 6th Open Scientific Meeting of Hip Society;1978. pp 87–96.
38. Cerretani D, Giorgi G, Fornara P, Bocchi L, Neri L, Ceffa R,Ghisellini F, Ritter MA. The in vitro elution characteristics ofvancomycin combined with imipenem-cilastatin in acrylicbone-cements. A pharmacokinetic study. J Arthroplasty 2002;17:619–626.
39. Virto MR, Frutos P, Torrado S, Frutos G. Gentamicin releasefrom modified acrylic bone cements with lactose and hydrox-ypropylmethylcellulose. Biomaterials 2003;24:79–87.
40. Frutos P, Diez-Pena E, Frutos G, Barrales-Rienda JM. Releaseof gentamicin sulphate from a modified commercial bonecement. Effect of (2-hydroxyethyl methacrylate) comonomerand poly(N-vinyl-2-pyrrolidone) additive on release mecha-nism and kinetics. Biomaterials 2002;23:3787–3797.
41. van de Belt H, Neut D, Uges DRA, Schenk W, van Horn JR,van der Mei HC, Busscher HJ. Surface roughness, porosityand wettability of gentamicin-loaded bone cements and theirantibiotic release. Biomaterials 2000;21:1981–1987.
42. Niemela SM, Ikaheimo I, Koskela M, Veiranto M, Suokas E,Tormala P, Waris T, Ashammakhi N, Syrjala H. Ciprofloxa-cin-releasing bioabsorbable polymer is superior to titanium inpreventing Staphylococcus epidermidis attachment and biofilmformation in vitro. J Biomed Mat Res B Appl Biomater2006;76:8–14.
320 HERNANDEZ ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials