
Nevus Emedicine
21
Melanocytic Nevi • Author: Timothy McCalmont, MD; Chief Editor: Dirk M Elston, MD more... Updated: Jun , !"# $ack%round Melanocytic nevi are benign neoplasms or hamartomas composed of melanocytes, the pigment-producing cells that constitutively colonize the epidermis. Melanocytes are derived from the neural crest and migrate during embryogenesis to selected ectodermal sites (primarily the skin and the CNS, but also to the eyes and the ears. !ctopic melanocytes have been id entified at autopsy in the gastrointestinal and genitourinary tracts. Congenital melanocytic nevi are thought to represent an anomaly in embryogenesis and, as such, could be considered, at least in a sense, malformations or hamartomas. "#$ %n contrast, most ac&uired melanocytic nevi are co nsidered benign neoplasms. Compare the images belo'. Melanocytic nevi occur in all mammalian species and are especially common in humans, dogs, and horses. This lar %e con%enital ne&us de&eloped papular ar eas of pi%mentation 'ithin it. Microscopic e(amination pro&ed that the )ne') areas represented small nodular collections of *eni%n melanocytes, 'ith no e&idence of e&ol&in% melanoma. he malignant analogue of a melanocytic nevus is melanoma, a topic discussed independently in Malignant Melanoma. )dditionally , the Medscape Skin Cancer *esource Center may be helpful. +athophysiolo%y Melanocytes are present in the basal layer o f the epidermis and e+hibit a certain degree of territoriality. Non-neoplastic melanocytes typically e+hibit contact inhibition to each other, and thus pigment cells are usually not found as contiguous cells. it h certain forms of stimulation, such as the e+ogenous administration of ultraviolet irradiation, the density of melanocytes in normal epithelium may increase. Normal melanocytes may also involve adne+al epithelium, most notably the bulbs of follicular papillae.
-
Upload
tutisuzaroh -
Category
Documents
-
view
25 -
download
0
description
nnn
Transcript of Nevus Emedicine

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 1/21
Melanocytic Nevi
•
Author: Timothy McCalmont, MD; Chief Editor: Dirk M Elston, MDmore...
Updated: Jun , !"#
$ack%round
Melanocytic nevi are benign neoplasms or hamartomas composed of melanocytes, the
pigment-producing cells that constitutively colonize the epidermis. Melanocytes are
derived from the neural crest and migrate during embryogenesis to selected
ectodermal sites (primarily the skin and the CNS, but also to the eyes and the ears.!ctopic melanocytes have been identified at autopsy in the gastrointestinal and
genitourinary tracts. Congenital melanocytic nevi are thought to represent an anomaly
in embryogenesis and, as such, could be considered, at least in a sense, malformations
or hamartomas."#$ %n contrast, most ac&uired melanocytic nevi are considered benign
neoplasms. Compare the images belo'. Melanocytic nevi occur in all mammalian
species and are especially common in humans, dogs, and horses.
This lar%e con%enital ne&us de&eloped papular areas of
pi%mentation 'ithin it. Microscopic e(amination pro&ed that the )ne')areas represented small nodular collections of *eni%n melanocytes, 'ith
no e&idence of e&ol&in% melanoma.
he malignant analogue of a melanocytic nevus is melanoma, a topic discussed
independently in Malignant Melanoma. )dditionally, the Medscape Skin Cancer
*esource Center may be helpful.
+athophysiolo%y
Melanocytes are present in the basal layer of the epidermis and e+hibit a certain
degree of territoriality. Non-neoplastic melanocytes typically e+hibit contact
inhibition to each other, and thus pigment cells are usually not found as contiguous
cells. ith certain forms of stimulation, such as the e+ogenous administration of
ultraviolet irradiation, the density of melanocytes in normal epithelium may increase.
Normal melanocytes may also involve adne+al epithelium, most notably the bulbs of
follicular papillae.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 2/21
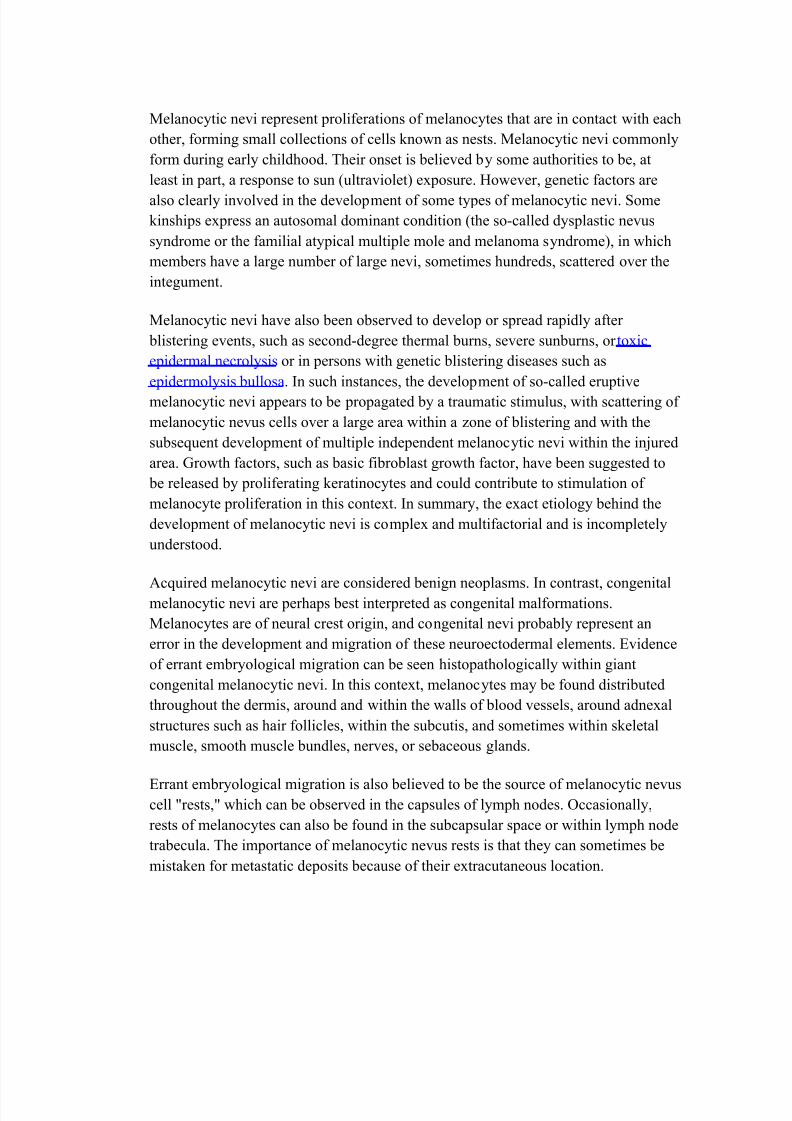
Melanocytic nevi represent proliferations of melanocytes that are in contact 'ith each
other, forming small collections of cells kno'n as nests. Melanocytic nevi commonly
form during early childhood. heir onset is believed by some authorities to be, at
least in part, a response to sun (ultraviolet e+posure. o'ever, genetic factors are
also clearly involved in the development of some types of melanocytic nevi. Some
kinships e+press an autosomal dominant condition (the so-called dysplastic nevus
syndrome or the familial atypical multiple mole and melanoma syndrome, in 'hich
members have a large number of large nevi, sometimes hundreds, scattered over the
integument.
Melanocytic nevi have also been observed to develop or spread rapidly after
blistering events, such as second-degree thermal burns, severe sunburns, or to+ic
epidermal necrolysis or in persons 'ith genetic blistering diseases such as
epidermolysis bullosa. %n such instances, the development of so-called eruptive
melanocytic nevi appears to be propagated by a traumatic stimulus, 'ith scattering of
melanocytic nevus cells over a large area 'ithin a zone of blistering and 'ith the
subse&uent development of multiple independent melanocytic nevi 'ithin the inured
area. /ro'th factors, such as basic fibroblast gro'th factor, have been suggested to
be released by proliferating keratinocytes and could contribute to stimulation of
melanocyte proliferation in this conte+t. %n summary, the e+act etiology behind the
development of melanocytic nevi is comple+ and multifactorial and is incompletely
understood.
)c&uired melanocytic nevi are considered benign neoplasms. %n contrast, congenitalmelanocytic nevi are perhaps best interpreted as congenital malformations.
Melanocytes are of neural crest origin, and congenital nevi probably represent an
error in the development and migration of these neuroectodermal elements. !vidence
of errant embryological migration can be seen histopathologically 'ithin giant
congenital melanocytic nevi. %n this conte+t, melanocytes may be found distributed
throughout the dermis, around and 'ithin the 'alls of blood vessels, around adne+al
structures such as hair follicles, 'ithin the subcutis, and sometimes 'ithin skeletal
muscle, smooth muscle bundles, nerves, or sebaceous glands.
!rrant embryological migration is also believed to be the source of melanocytic nevuscell 0rests,0 'hich can be observed in the capsules of lymph nodes. 1ccasionally,
rests of melanocytes can also be found in the subcapsular space or 'ithin lymph node
trabecula. he importance of melanocytic nevus rests is that they can sometimes be
mistaken for metastatic deposits because of their e+tracutaneous location.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 3/21
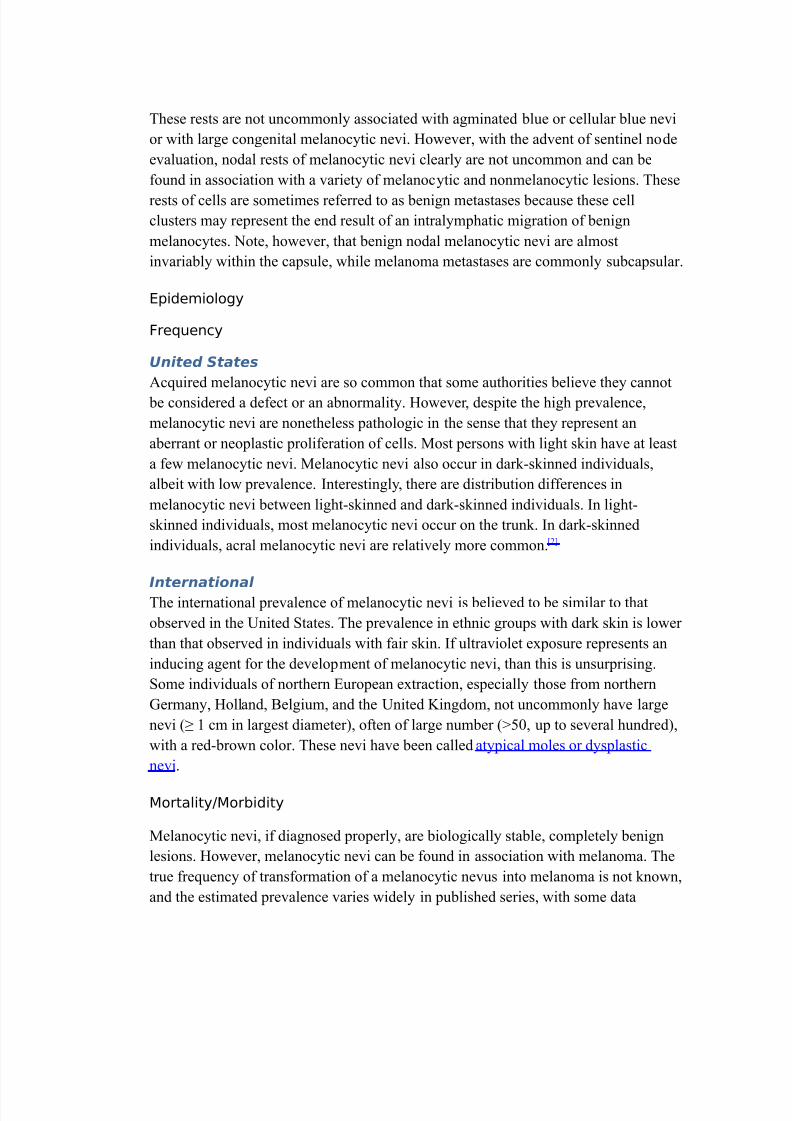
hese rests are not uncommonly associated 'ith agminated blue or cellular blue nevi
or 'ith large congenital melanocytic nevi. o'ever, 'ith the advent of sentinel node
evaluation, nodal rests of melanocytic nevi clearly are not uncommon and can be
found in association 'ith a variety of melanocytic and nonmelanocytic lesions. hese
rests of cells are sometimes referred to as benign metastases because these cell
clusters may represent the end result of an intralymphatic migration of benign
melanocytes. Note, ho'ever, that benign nodal melanocytic nevi are almost
invariably 'ithin the capsule, 'hile melanoma metastases are commonly subcapsular.
Epidemiolo%y
re-uency
United States
)c&uired melanocytic nevi are so common that some authorities believe they cannot
be considered a defect or an abnormality. o'ever, despite the high prevalence,
melanocytic nevi are nonetheless pathologic in the sense that they represent an
aberrant or neoplastic proliferation of cells. Most persons 'ith light skin have at least
a fe' melanocytic nevi. Melanocytic nevi also occur in dark-skinned individuals,
albeit 'ith lo' prevalence. %nterestingly, there are distribution differences in
melanocytic nevi bet'een light-skinned and dark-skinned individuals. %n light-
skinned individuals, most melanocytic nevi occur on the trunk. %n dark-skinned
individuals, acral melanocytic nevi are relatively more common. "2$
International
he international prevalence of melanocytic nevi is believed to be similar to that
observed in the 3nited States. he prevalence in ethnic groups 'ith dark skin is lo'er
than that observed in individuals 'ith fair skin. %f ultraviolet e+posure represents an
inducing agent for the development of melanocytic nevi, than this is unsurprising.
Some individuals of northern !uropean e+traction, especially those from northern
/ermany, olland, 4elgium, and the 3nited 5ingdom, not uncommonly have large
nevi (6 # cm in largest diameter, often of large number (789, up to several hundred,
'ith a red-bro'n color. hese nevi have been called atypical moles or dysplastic
nevi.
MortalityMor*idity
Melanocytic nevi, if diagnosed properly, are biologically stable, completely benign
lesions. o'ever, melanocytic nevi can be found in association 'ith melanoma. he
true fre&uency of transformation of a melanocytic nevus into melanoma is not kno'n,
and the estimated prevalence varies 'idely in published series, 'ith some data

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 4/21
suggesting that up to :9; of melanomas are associated 'ith a precursor melanocytic
nevus.
4oth ac&uired and congenital melanocytic nevi hold some risk for the development of
melanoma. Congenital melanocytic nevi hold the greater risk, and this is especiallytrue of giant congenital melanocytic nevi. his is believed to be a conse&uence of the
fact that the number of lesional melanocytes 'ithin large lesions is greater, and thus
the chances of a transformative event are proportionately greater. <arge and giant
congenital melanocytic nevi often have both biological and cosmetic implications.
<arge congenital nevi have a lo' but real risk for secondary malignant transformation
and the development of melanoma. Some data suggest that melanoma can develop
'ithin a giant congenital melanocytic nevus in up to 8; of cases.
/ace
Melanocytic nevi are common lesions in patients 'ith light or fair skin and are less
common lesions in dark-skinned individuals. his difference in prevalence is in part
attributable to the fact that identifying moles in dark-skinned patients is often
difficult, especially if the lesions are macular (flat.
• 0ome authorities ha&e su%%ested that melanocytic ne&i are in partstimulated *y e(posure to sunli%ht.1, 23 4f so, then indi&iduals 'ithdark skin mi%ht ha&e fe'er ne&i *ecause of the protecti&eproperties of melanin.
• E&idence indicates that *road5spectrum sunscreens attenuate thede&elopmente&olution of melanocytic ne&i 'hen used in children163
; therefore, dark5skinned indi&iduals pro*a*ly ha&e inherentprotection a%ainst the de&elopment of moles *ecause of theircutaneous melani7ation.
0e(
No clear se+ predilection is reported for the development of melanocytic nevi.
o'ever, melanocytes have been postulated to e+hibit some degree of se+ hormone
responsiveness. he findings associated 'ith melanocytic nevi during pregnancy
support this conclusion. Melanocytic nevi commonly darken and=or enlarge during pregnancy. Melanocytes have been sho'n to have cytosolic receptors for estrogens
and androgens, and melanogenesis is responsive to these steroid hormones. Some
melanomas seem to respond to hormones, an observation that might be e+plained by
these cytosolic receptors.

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 5/21
• 0u*tle di8erences may e(ist in the pre&alence of melanocytic ne&i*et'een 'omen and men. Jud%in% the incidence and pre&alence*ased on a&aila*le *iopsy data is di9cult *ecause 'omen may *emore likely to seek medical attention. 4f se(5specic &ariations inincidence do e(ist, the di8erences may *e site specic. or
e(ample, specic histopatholo%ical features are commonlyo*ser&ed in melanocytic ne&i that occur 'ithin %enital skin. Thesefeatures are noted almost e(clusi&ely 'ithin *iopsy specimens from'omen, althou%h similar alterations can occasionally *e o*ser&edin melanocytic ne&i from males.
• rom the authors data*ase <at the Uni&ersity of California, 0anrancisco=, data clearly sho' that *iopsies of %enital melanocyticne&i are much more commonly performed in 'omen than in men.
These data do not une-ui&ocally conrm that the pre&alence of%enital melanocytic ne&i is truly increased in 'omen, althou%h thisseems likely.
A%e
4y definition, congenital melanocytic nevi are present at birth or soon thereafter,
although some small congenital nevi are clearly tardive in their clinical presentation.
Current opinion holds that some elements of such nevi are present at birth but remain
inconspicuous until some later date.
• $y denition, ac-uired melanocytic ne&i are not present at *irth,and the incidence of melanocytic ne&i increases throu%hout the rst
decades of life.
• The peak incidence of melanocytic ne&i is in the fourth to fthdecades of life, and the incidence 'ith each successi&e decadedecreases, 'ith a lo' incidence in elderly persons.
• Ac-uired melanocytic ne&i ha&e *een stated to *e a*sent at *irthand at death. Althou%h not entirely true, this concept re>ects thefact that ac-uired ne&i de&elop in increasin% num*ers throu%houtchildhood and early adulthood and then slo'ly in&olute; therefore,melanocytic ne&i are inconspicuous durin% the ad&anced elderyears.
• ?e&us su*type incidence may also &ary 'ith a%es. Accordin% to astudy *y @alaudek et al, melanocytic ne&i of mi(ed pattern 'ith aperipheral rim of dark %lo*ules are su9ciently rare in persons olderthan 6" years that they should *e considered suspicious. 13
Bistory

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 6/21
Melanocytic nevi are common lesions that can be found on the integument of almost
all individuals. Some patients present 'ith fe' lesions, 'hile others have hundreds.
he number on a given individual increases in rough proportion to the degree of skin
pigmentation.
Melanocytic nevi can be broadly divided into congenital and ac&uired types.
>etermining if a lesion is congenital or ac&uired is generally easily accomplished by
direct &uery of the patient, although, as noted above, some small congenital
melanocytic nevi are tardive and may be perceived by the patient as ac&uired.
• hen e&aluatin% the nature of a melanocytic lesion, a num*er ofattri*utes must *e assessed. urther commentary descri*in%physical attri*utes can *e found in +hysical.
o hether a lesion has *ecome symptomatic <e%, itchy,painful, irritated, or *leedin%= is considered an importantindicator of potential mali%nant chan%e.
o ?ot all melanocytic ne&i that chan%e are mali%nant,especially if chan%e is noted in a person youn%er than 2"years. Bo'e&er, chan%e that is percepti*le o&er a short timeis an indicator of potential mali%nancy and desi%nates alesion deser&in% of *iopsy. An Australian study found that# of *eni%n lesions chan%ed <as measured *y se-uentialdi%ital dermoscopic ima%in%= o&er an inter&al of !.652.6months. The proportion of *eni%n lesions that chan%ed 'as
hi%her in persons a%ed "56 years than in those a%ed 56years *ut rose a%ain in the elderly <a%e 6 y=.1F3
• Ac-uired melanocytic ne&i are typically less than a centimeter indiameter and e&enly colored.
• Melanocytic ne&i most commonly are tan to *ro'n, *ut colorationcan *e &aria*le, ran%in% from skin5colored <nonpi%mented= to Get*lack. The deep pi%mentation associated 'ith dark melanocyticne&i often stems from associated intracorneal pi%mentation. Thespectrum of )hypermelanotic) melanocytic ne&us includes lesions'ith hea&y epidermal pi%mentation.
• Dysplastic melanocytic ne&i ha&e also *een referred to as Clarkne&i. The desi%nation )dysplastic) 'as applied to such lesions*ecause of an early *elief that such lesions mi%ht *e *iolo%icallyunsta*le and represent common precursors of melanoma. urtherstudy has not deniti&ely conrmed that this is the case. Dysplasticne&i present clinically as >attish, pi%mented macules or thin
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 7/21
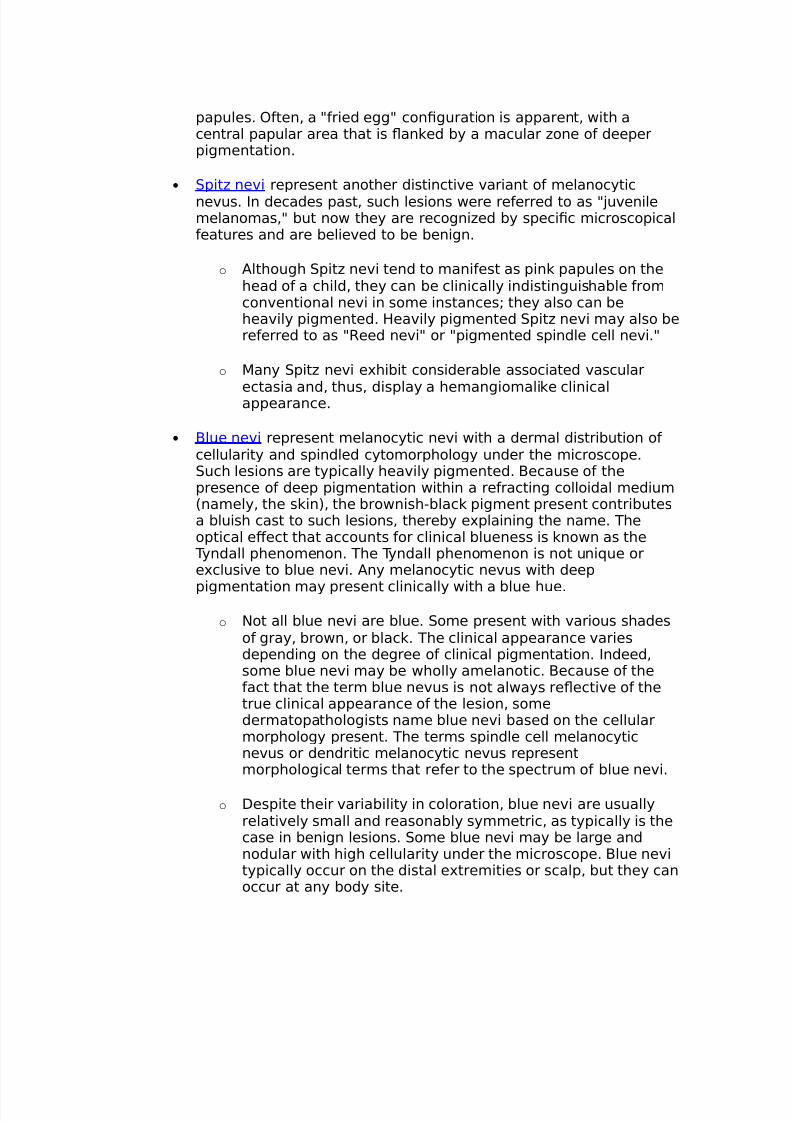
papules. Hften, a )fried e%%) con%uration is apparent, 'ith acentral papular area that is >anked *y a macular 7one of deeperpi%mentation.
• 0pit7 ne&i represent another distincti&e &ariant of melanocytic
ne&us. 4n decades past, such lesions 'ere referred to as )Gu&enilemelanomas,) *ut no' they are reco%ni7ed *y specic microscopicalfeatures and are *elie&ed to *e *eni%n.
o Althou%h 0pit7 ne&i tend to manifest as pink papules on thehead of a child, they can *e clinically indistin%uisha*le fromcon&entional ne&i in some instances; they also can *ehea&ily pi%mented. Bea&ily pi%mented 0pit7 ne&i may also *ereferred to as )/eed ne&i) or )pi%mented spindle cell ne&i.)
o Many 0pit7 ne&i e(hi*it considera*le associated &ascular
ectasia and, thus, display a heman%iomalike clinicalappearance.
• $lue ne&i represent melanocytic ne&i 'ith a dermal distri*ution ofcellularity and spindled cytomorpholo%y under the microscope.0uch lesions are typically hea&ily pi%mented. $ecause of thepresence of deep pi%mentation 'ithin a refractin% colloidal medium<namely, the skin=, the *ro'nish5*lack pi%ment present contri*utesa *luish cast to such lesions, there*y e(plainin% the name. Theoptical e8ect that accounts for clinical *lueness is kno'n as the
Tyndall phenomenon. The Tyndall phenomenon is not uni-ue ore(clusi&e to *lue ne&i. Any melanocytic ne&us 'ith deep
pi%mentation may present clinically 'ith a *lue hue.
o ?ot all *lue ne&i are *lue. 0ome present 'ith &arious shadesof %ray, *ro'n, or *lack. The clinical appearance &ariesdependin% on the de%ree of clinical pi%mentation. 4ndeed,some *lue ne&i may *e 'holly amelanotic. $ecause of thefact that the term *lue ne&us is not al'ays re>ecti&e of thetrue clinical appearance of the lesion, somedermatopatholo%ists name *lue ne&i *ased on the cellularmorpholo%y present. The terms spindle cell melanocyticne&us or dendritic melanocytic ne&us representmorpholo%ical terms that refer to the spectrum of *lue ne&i.
o Despite their &aria*ility in coloration, *lue ne&i are usuallyrelati&ely small and reasona*ly symmetric, as typically is thecase in *eni%n lesions. 0ome *lue ne&i may *e lar%e andnodular 'ith hi%h cellularity under the microscope. $lue ne&itypically occur on the distal e(tremities or scalp, *ut they canoccur at any *ody site.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 8/21
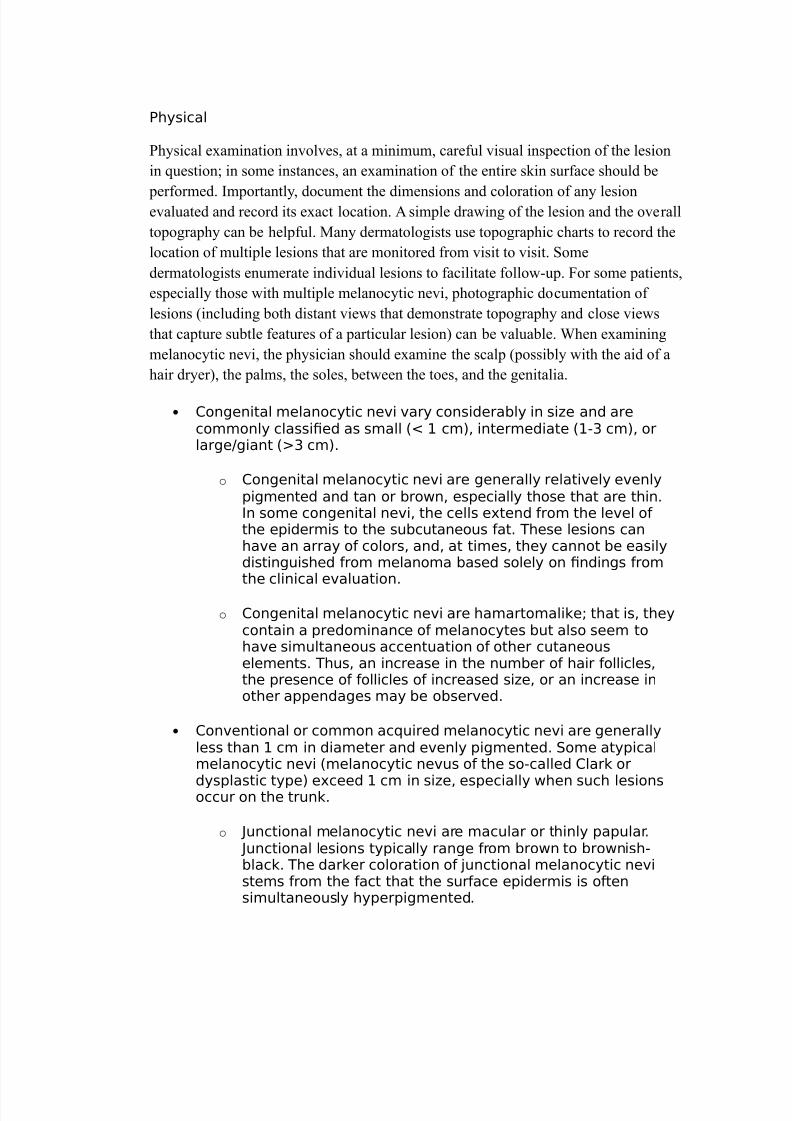
+hysical
?hysical e+amination involves, at a minimum, careful visual inspection of the lesion
in &uestion@ in some instances, an e+amination of the entire skin surface should be
performed. %mportantly, document the dimensions and coloration of any lesionevaluated and record its e+act location. ) simple dra'ing of the lesion and the overall
topography can be helpful. Many dermatologists use topographic charts to record the
location of multiple lesions that are monitored from visit to visit. Some
dermatologists enumerate individual lesions to facilitate follo'-up. Aor some patients,
especially those 'ith multiple melanocytic nevi, photographic documentation of
lesions (including both distant vie's that demonstrate topography and close vie's
that capture subtle features of a particular lesion can be valuable. hen e+amining
melanocytic nevi, the physician should e+amine the scalp (possibly 'ith the aid of a
hair dryer, the palms, the soles, bet'een the toes, and the genitalia.
• Con%enital melanocytic ne&i &ary considera*ly in si7e and arecommonly classied as small <I # cm=, intermediate <#5 cm=, orlar%e%iant < cm=.
o Con%enital melanocytic ne&i are %enerally relati&ely e&enlypi%mented and tan or *ro'n, especially those that are thin.4n some con%enital ne&i, the cells e(tend from the le&el ofthe epidermis to the su*cutaneous fat. These lesions canha&e an array of colors, and, at times, they cannot *e easilydistin%uished from melanoma *ased solely on ndin%s fromthe clinical e&aluation.
o Con%enital melanocytic ne&i are hamartomalike; that is, theycontain a predominance of melanocytes *ut also seem toha&e simultaneous accentuation of other cutaneouselements. Thus, an increase in the num*er of hair follicles,the presence of follicles of increased si7e, or an increase inother appenda%es may *e o*ser&ed.
• Con&entional or common ac-uired melanocytic ne&i are %enerallyless than # cm in diameter and e&enly pi%mented. 0ome atypicalmelanocytic ne&i <melanocytic ne&us of the so5called Clark or
dysplastic type= e(ceed # cm in si7e, especially 'hen such lesionsoccur on the trunk.
o Junctional melanocytic ne&i are macular or thinly papular. Junctional lesions typically ran%e from *ro'n to *ro'nish5*lack. The darker coloration of Gunctional melanocytic ne&istems from the fact that the surface epidermis is oftensimultaneously hyperpi%mented.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 9/21
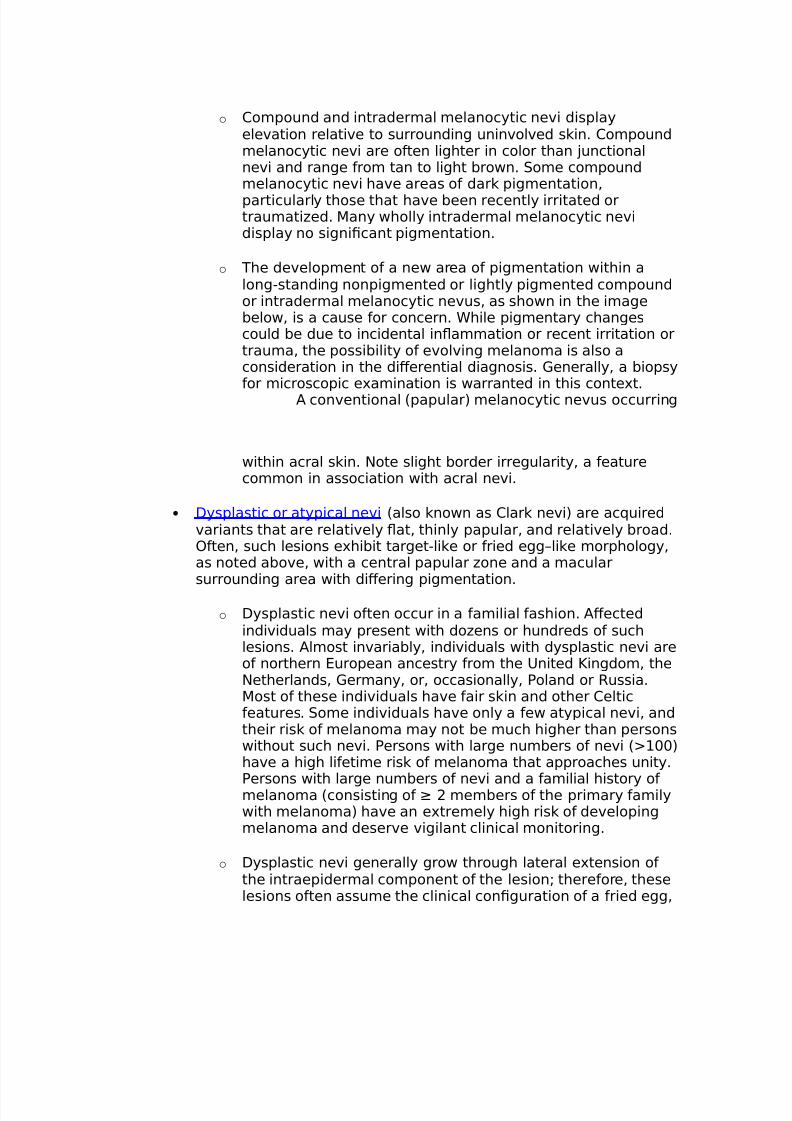
o Compound and intradermal melanocytic ne&i displayele&ation relati&e to surroundin% unin&ol&ed skin. Compoundmelanocytic ne&i are often li%hter in color than Gunctionalne&i and ran%e from tan to li%ht *ro'n. 0ome compoundmelanocytic ne&i ha&e areas of dark pi%mentation,
particularly those that ha&e *een recently irritated ortraumati7ed. Many 'holly intradermal melanocytic ne&idisplay no si%nicant pi%mentation.
o The de&elopment of a ne' area of pi%mentation 'ithin alon%5standin% nonpi%mented or li%htly pi%mented compoundor intradermal melanocytic ne&us, as sho'n in the ima%e*elo', is a cause for concern. hile pi%mentary chan%escould *e due to incidental in>ammation or recent irritation ortrauma, the possi*ility of e&ol&in% melanoma is also aconsideration in the di8erential dia%nosis. enerally, a *iopsyfor microscopic e(amination is 'arranted in this conte(t.
A con&entional <papular= melanocytic ne&us occurrin%
'ithin acral skin. ?ote sli%ht *order irre%ularity, a featurecommon in association 'ith acral ne&i.
• Dysplastic or atypical ne&i <also kno'n as Clark ne&i= are ac-uired&ariants that are relati&ely >at, thinly papular, and relati&ely *road.Hften, such lesions e(hi*it tar%et5like or fried e%%Klike morpholo%y,as noted a*o&e, 'ith a central papular 7one and a macularsurroundin% area 'ith di8erin% pi%mentation.
o Dysplastic ne&i often occur in a familial fashion. A8ectedindi&iduals may present 'ith do7ens or hundreds of suchlesions. Almost in&aria*ly, indi&iduals 'ith dysplastic ne&i areof northern European ancestry from the United Lin%dom, the?etherlands, ermany, or, occasionally, +oland or /ussia.Most of these indi&iduals ha&e fair skin and other Celticfeatures. 0ome indi&iduals ha&e only a fe' atypical ne&i, andtheir risk of melanoma may not *e much hi%her than persons'ithout such ne&i. +ersons 'ith lar%e num*ers of ne&i <#""=ha&e a hi%h lifetime risk of melanoma that approaches unity.
+ersons 'ith lar%e num*ers of ne&i and a familial history ofmelanoma <consistin% of ! mem*ers of the primary family'ith melanoma= ha&e an e(tremely hi%h risk of de&elopin%melanoma and deser&e &i%ilant clinical monitorin%.
o Dysplastic ne&i %enerally %ro' throu%h lateral e(tension ofthe intraepidermal component of the lesion; therefore, theselesions often assume the clinical con%uration of a fried e%%,
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 10/21
'ith a central papular 7one and a surroundin% macular areaof di8erin% pi%mentation. The peripheral *order is oftenpercei&ed as *lurred or fu77y *ecause of this laterale(tension of supercial melanocytes.
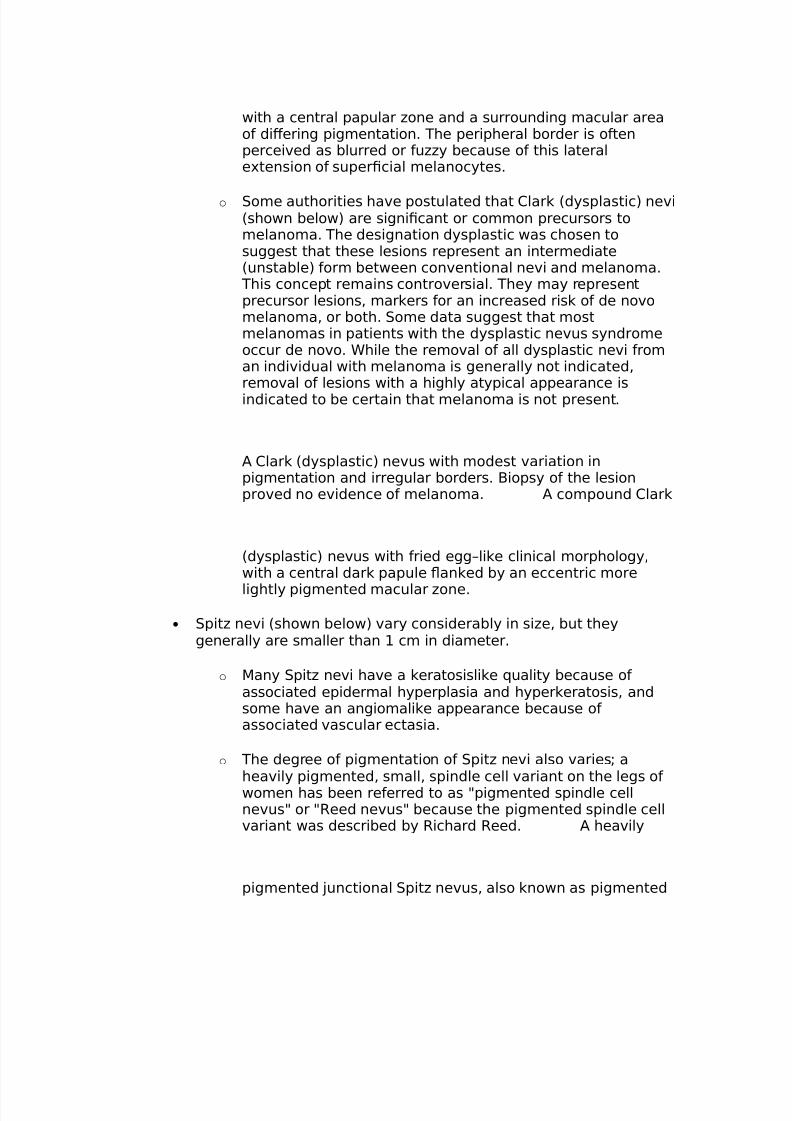
o 0ome authorities ha&e postulated that Clark <dysplastic= ne&i<sho'n *elo'= are si%nicant or common precursors tomelanoma. The desi%nation dysplastic 'as chosen tosu%%est that these lesions represent an intermediate<unsta*le= form *et'een con&entional ne&i and melanoma.
This concept remains contro&ersial. They may representprecursor lesions, markers for an increased risk of de no&omelanoma, or *oth. 0ome data su%%est that mostmelanomas in patients 'ith the dysplastic ne&us syndromeoccur de no&o. hile the remo&al of all dysplastic ne&i froman indi&idual 'ith melanoma is %enerally not indicated,remo&al of lesions 'ith a hi%hly atypical appearance isindicated to *e certain that melanoma is not present.
A Clark <dysplastic= ne&us 'ith modest &ariation inpi%mentation and irre%ular *orders. $iopsy of the lesionpro&ed no e&idence of melanoma. A compound Clark
<dysplastic= ne&us 'ith fried e%%Klike clinical morpholo%y,'ith a central dark papule >anked *y an eccentric more
li%htly pi%mented macular 7one.
• 0pit7 ne&i <sho'n *elo'= &ary considera*ly in si7e, *ut they%enerally are smaller than # cm in diameter.
o Many 0pit7 ne&i ha&e a keratosislike -uality *ecause ofassociated epidermal hyperplasia and hyperkeratosis, andsome ha&e an an%iomalike appearance *ecause ofassociated &ascular ectasia.
o The de%ree of pi%mentation of 0pit7 ne&i also &aries; ahea&ily pi%mented, small, spindle cell &ariant on the le%s of'omen has *een referred to as )pi%mented spindle cellne&us) or )/eed ne&us) *ecause the pi%mented spindle cell&ariant 'as descri*ed *y /ichard /eed. A hea&ily
pi%mented Gunctional 0pit7 ne&us, also kno'n as pi%mented
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 11/21
spindle cell ne&us. ?ote that many 0pit7 ne&i arenonpi%mented and may ha&e an an%iomalike clinicalappearance.
• $lue ne&i are not al'ays *lue, and they are not e&en al'ays
pi%mented. The desi%nation *lue ne&us, althou%h >a'ed, has *eenpreser&ed for historical reasons.
o $lue ne&i are sometimes lar%er than other melanocytic ne&i,occasionally measurin% ! cm or %reater in diameter. This isparticularly true of cellular lesions <cellular *lue ne&i= thatoccur at sun5protected sites, such as the *uttocks.
o $lue ne&i are often rm *ecause of associated stromalsclerosis, and they often ha&e a nodular -uality, a re>ectionof their deeper position 'ithin the skin.
o Bea&ily pi%mented *lue ne&i manifest clinically as *lue,*lack, or %ray lesions, 'hereas *lue ne&i 'ith lesser de%reesof pi%mentation may *e tan or *ro'n or strictly the color ofsurroundin% healthy skin.
o Bypocellular *lue ne&i that co&er an e(tensi&e clinicaldistri*ution ha&e *een referred to as )dermal melanocytichamartomas) *y some authors. This spectrum includes theentities ne&us of 4to, ne&us of Hta, and ne&us of 0un.
Causes
he etiology of melanocytic nevi remains unkno'n. No established genetic or
environmental influences are kno'n to contribute to the development of congenital
nevi. o'ever, after studying #:: children in Naples, researchers concluded that
development of melanocytic nevi early in life is the result of complicated
relationships among nevus evolution, anatomic location, and environmental and
constitutional factors."B$ he specific genetic factors that contribute to the
development of ac&uired melanocytic nevi also remain unkno'n. o'ever, data
suggest that the propensity for developing large numbers of nevi, such as multiple
dysplastic nevi, might be inherited as an autosomal dominant trait.
• +atients 'ith the familial atypical multiple mole and melanomasyndrome <also kno'n as the dysplastic ne&us syndrome= de&elopdo7ens to hundreds of melanocytic ne&i and ha&e an ele&atedlifetime risk for the de&elopment of melanoma. As the nameimplies, this disorder is *elie&ed to ha&e an inherited *asis.

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 12/21
• As noted pre&iously, population5*ased e&idence su%%ests thatultra&iolet irradiation may tri%%er the de&elopment of ac-uiredmelanocytic ne&i. The num*er of melanocytic ne&i in childhood isin&ersely related to the de%ree of skin pi%mentation and is hi%h inchildren 'ith poor sun tolerance. The mechanism of this induction
has not *een ade-uately in&esti%ated, *ut such induction couldrepresent an e(ample of tumor promotion *y ultra&iolet li%ht.
Di8erential Dia%noses
• Atypical Mole <Dysplastic ?e&us=
• Mali%nant Melanoma
• ?e&i of Hta and 4t
Na*oratory 0tudies
• ?o la*oratory studies are indicated in the e&aluation of commonac-uired melanocytic ne&i.
• As a rule, patients 'ith con%enital melanocytic ne&i also do notre-uire la*oratory e&aluation.
4ma%in% 0tudies
• 4ma%in% is not 'arranted in the e&aluation of most patients 'ith
ac-uired melanocytic ne&i; ho'e&er, the possi*ility ofneurocutaneous melanosis should *e considered in patients<children= 'ith multiple con%enital melanocytic ne&i in&ol&in% theskin o&erlyin% the spine and the posterior part of the scalp.
o 0ome patients 'ith multiple con%enital ne&i o&erlyin% theC?0 'arrant radiolo%ic ima%in%. 0uch indi&iduals are at riskfor leptomenin%eal melanosis.
o 0ome patients 'ith neurocutaneous melanosis ha&e nests ofmelanocytes 'ithin the C?0 at specic sites. These nests ofcells can *e detected usin% M/4 <especially 'ith T#5'ei%hted
ima%es=.1O3
o Althou%h the nests of melanocytes are *eni%n, these cellspose a risk for transformation to C?0 melanoma, and follo'5up care is indicated.
+rocedures

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 13/21
• 0imple e(cisional *iopsy is the procedure of choice for remo&al anddia%nosis of a melanocytic ne&us. All remo&ed melanocytic ne&ishould *e su*mitted for microscopic e&aluation. $ecause theinterpretation of pi%mented lesions may *e challen%in%, manydermatolo%ists prefer to ha&e their specimens read *y a -ualied
dermatopatholo%ist.1#"3
• Either sha&e *iopsy or punch *iopsy is typically used for cosmeticremo&al of *anal melanocytic ne&i.
• 4t is optimal to stri&e for complete e(cision of a %i&en lesion, if at allpossi*le, 'hen melanoma is considered in the di8erential dia%nosis.
• A complete e(cisional *iopsy permits all a&aila*le histopatholo%icalcriteria to *e applied to a lesion and thus ena*les a more precisedia%nosis.
• hen a partial punch or sha&e *iopsy sample is taken from a lesion,the interpretin% patholo%ist cannot apply important criteria, such assymmetry and circumscription <lateral demarcation=, to theassessment of the lesion. 4f a partial *iopsy specimen of a lar%erlesion is o*tained *ecause of clinical necessity, the fact that thespecimen is partial should *e clearly indicated on the re-uisitionform.
• +artial *iopsy samples can sometimes lead to misdia%nosis *ecauseof samplin% error.
• +artial *iopsy samples can in>ate the num*er of proceduresre-uired for dia%nosis *ecause a partial *iopsy sample that doesnot ena*le a deniti&e dia%nosis to *e made necessarily leads tosu*se-uent ree(cision of the lesion in -uestion.
Bistolo%ic indin%s
he chief histopathological differential diagnosis involves the distinction of
melanoma from various forms of melanocytic nevi, including Spitz nevi.
!+amination via conventional microscopy remains the criterion standard for making
this distinction. /enomic analysis via comparative genomic hybridization (C/ or
fluorescence in situ hybridization (A%S is being used on a limited basis to
supplement conventional histopathological interpretation. /enomic analysis permits
screening of fi+ed tumor tissue for cytogenetic aberrations. o date, studies indicate
that multiple cytogenetic fla's are typical of melanoma, 'hereas most melanocytic
nevi are cytostructurally normal.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 14/21

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 15/21
Conventional (ordinary or common ac&uired melanocytic nevi develop as a
proliferation of single melanocytes along the dermoepidermal unction. )s the
melanocytes proliferate, small nests of cells develop in the lo'er-most part of the
epidermis, and the resultant lesion is termed a unctional melanocytic nevus. ith
continued proliferation, nests persevere along the unction, but they can also be found
'ithin the superficial dermis, a configuration termed compound melanocytic nevus.
)s a nevus ages, the unctional component often diminishes or entirely involutes. he
resultant nevus is termed an intradermal melanocytic nevus, depicted belo'.
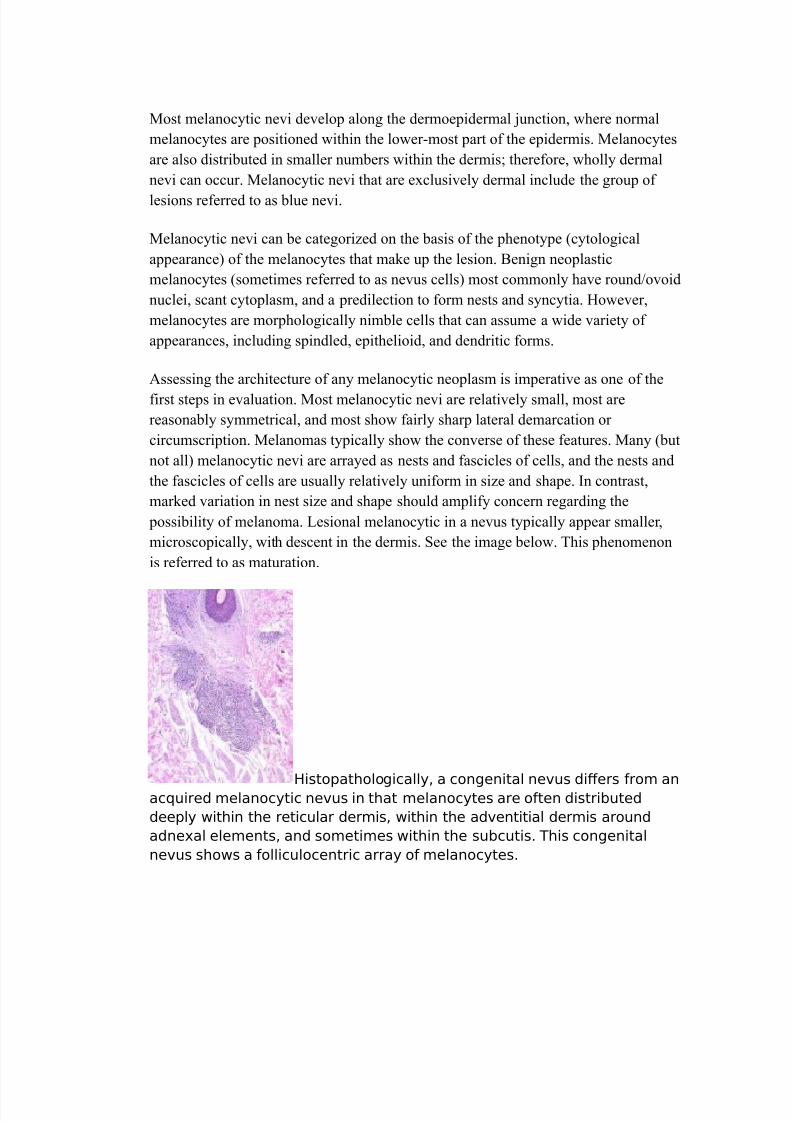
A con&entional compound melanocytic ne&us.
?ote the presence of melanocytes 'ith small nuclei in nests alon% the
dermoepidermal Gunction and the presence of similar melanocytes in nests
and syncytia in the su*Gacent dermis.
Congenital melanocytic nevi are similar to their ac&uired counterparts in that
unctional, compound, and intradermal patterns can be seen. Most congenital nevi
e+tend 'ell into the dermis, 'ith melanocytes positioned in the interstitial dermis
bet'een collagen bundles. he depth of e+tension into the dermis is variable. Some
large congenital nevi e+hibit cells that e+tend into subcutaneous septa. Congenital
melanocytic nevi 'ith melanocytes confined to the upper half of the reticular dermis
have been termed superficial congenital nevi. <esions of this type are typically
smaller than 2 cm in overall diameter.
Spitz nevi, sho'n belo', are virtually al'ays ac&uired melanocytic nevi, and they
can e+hibit a microscopic pattern that is unctional, compound, or 'holly intradermal.
<ike all benign nevi, Spitz nevi tend to be relatively small and symmetrical and
laterally demarcated, but Spitz nevi differ from conventional nevi in that
nucleomegalic cells are common and predominate in some lesions. Suchnucleomegalic Spitz nevus cells may be aneuploid, tetraploid, or octoploid. he
e+planation as to 'hy Spitz nevi are commonly nondiploid 'hile lacking other
attributes of malignancy has not yet been forthcoming. Clearly, anomalies in ploidy
alone are not sufficient for full malignant transformation.
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 16/21
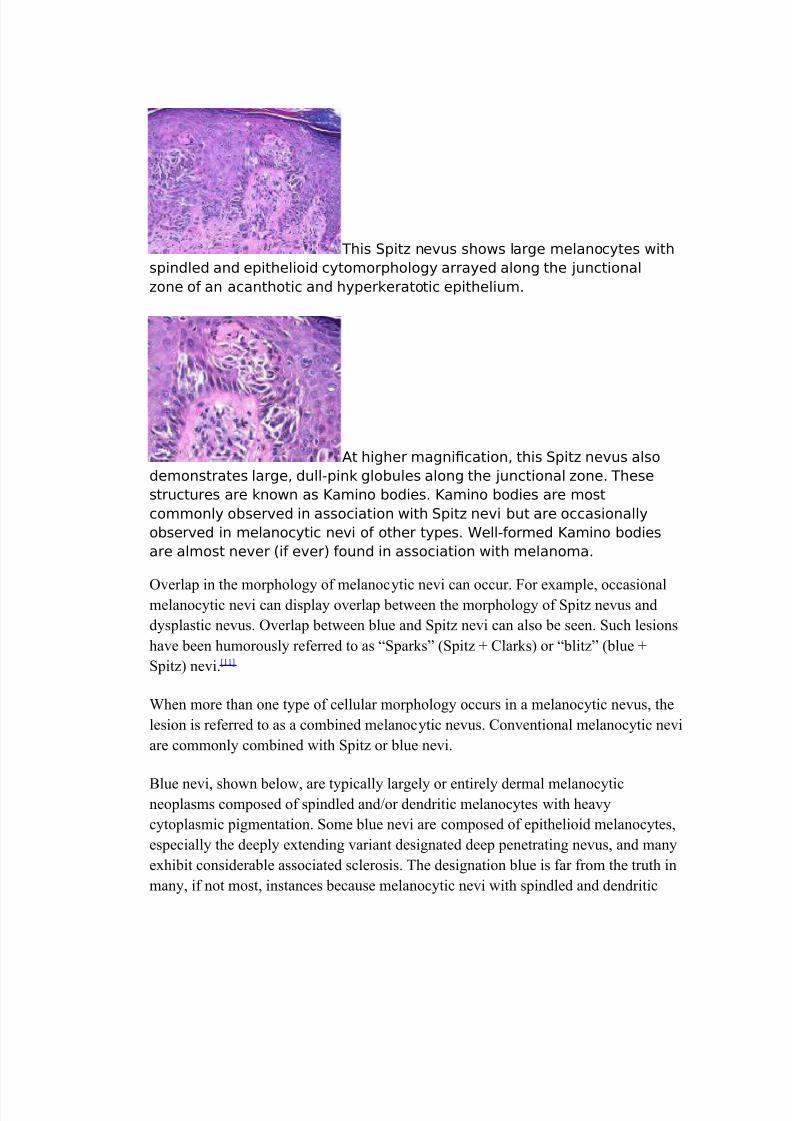
This 0pit7 ne&us sho's lar%e melanocytes 'ith
spindled and epithelioid cytomorpholo%y arrayed alon% the Gunctional
7one of an acanthotic and hyperkeratotic epithelium.
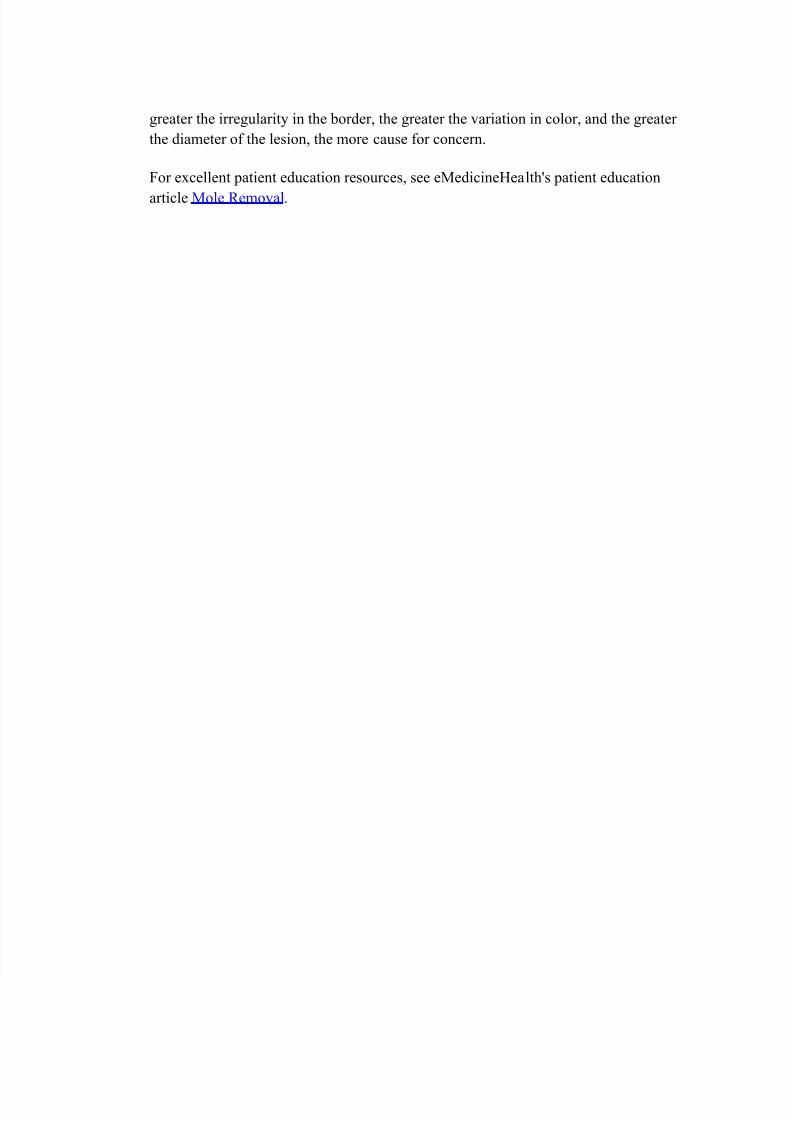
At hi%her ma%nication, this 0pit7 ne&us also
demonstrates lar%e, dull5pink %lo*ules alon% the Gunctional 7one. These
structures are kno'n as Lamino *odies. Lamino *odies are most
commonly o*ser&ed in association 'ith 0pit7 ne&i *ut are occasionally
o*ser&ed in melanocytic ne&i of other types. ell5formed Lamino *odies
are almost ne&er <if e&er= found in association 'ith melanoma.
1verlap in the morphology of melanocytic nevi can occur. Aor e+ample, occasionalmelanocytic nevi can display overlap bet'een the morphology of Spitz nevus and
dysplastic nevus. 1verlap bet'een blue and Spitz nevi can also be seen. Such lesions
have been humorously referred to as SparksD (Spitz E Clarks or blitzD (blue E
Spitz nevi."##$
hen more than one type of cellular morphology occurs in a melanocytic nevus, the
lesion is referred to as a combined melanocytic nevus. Conventional melanocytic nevi
are commonly combined 'ith Spitz or blue nevi.
4lue nevi, sho'n belo', are typically largely or entirely dermal melanocyticneoplasms composed of spindled and=or dendritic melanocytes 'ith heavy
cytoplasmic pigmentation. Some blue nevi are composed of epithelioid melanocytes,
especially the deeply e+tending variant designated deep penetrating nevus, and many
e+hibit considerable associated sclerosis. he designation blue is far from the truth in
many, if not most, instances because melanocytic nevi 'ith spindled and dendritic

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 17/21
melanocytes can be tan, bro'n, black, gray, or even skin-colored@ ho'ever, despite its
inaccuracy, the designation blue nevus remains the universal standard for this
category of lesions.
This *lue ne&us is composed of small dendritic
melanocytes. This type of cytomorpholo%y can *e seen in so5called
common *lue ne&i and in topo%raphically restricted lesions such as ne&us
of 4to or ne&us of Hta.
Some authorities have promoted the use an eponymic approach to the classification of
melanocytic nevi. he merit of this proposal derives from the fact that eponymic
naming avoids the semantic misdeeds of the past. Aor e+ample, the benign entity
formerly (and incorrectly kno'n as uvenile melanoma becomes a Spitz nevus in the
eponymic system. >ysplastic nevi are eponymically kno'n as Clark nevi, in memory
of allace Clark. he designation Miescher nevus can be used to designate dome-
shaped, superficial congenital nevi that are commonly e+pressed on the face and the
upper part of the trunk, 'hereas the designation 3nna nevus can be used to refer to
acrochordonlike lesions that commonly develop near skin folds."#2, #F$
>espite the enthusiasm for eponymic naming in some areas, the usage of such
designations can impede communication 'ith the uninitiated. he author sees no
difficulty in the usage of eponyms (and uses eponyms sporadically in his o'n
practice, as long as the e+act nature of the lesion in &uestion is clearly stated in the
language of the pathology report.
0ta%in%
Melanocytic nevi are benign lesions. No staging is re&uired, 'ith the possible
e+ception of atypical benign lesions for 'hich uncertainty e+ists regarding the
diagnosis and melanoma cannot be entirely eliminated from the differential diagnosis.
Medical Care

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 18/21
Medical treatment is typically ineffective and inappropriate for the management of a
benign neoplasm such as a melanocytic nevus.
0ur%ical Care
Melanocytic nevi can be surgically removed for cosmetic considerations or because
of concern regarding the biological potential of a lesion.
• Melanocytic ne&i remo&ed for cosmesis are often remo&ed *ytan%ential or sha&e e(cision.
• +unch e(cision can *e used for relati&ely small lesions.
• Nar%e lesions may re-uire complete e(cision 'ith sutured closure,e&en if kno'n to *e *eni%n, *ecause lesions e(ceedin% # cm in
diameter often are not amena*le to the sha&e techni-ue.
• A simple conser&ati&e e(cisional *iopsy 'ith a sutured closure isusually the most e(peditious means to dia%nosis if concern e(istsre%ardin% the possi*ility of melanoma. 4f the lesion is found to *e*eni%n, then, ordinarily, no further treatment is re-uired.
• +ro&idin% the patholo%ist 'ith a complete e(cisional specimena8ords him or her the *est opportunity to make an accuratedia%nosis *ecause all a&aila*le criteria <includin% lo'5ma%nicationattri*utes such as si7e, circumscription, and symmetry= can *eapplied to the lesion.
• 4f a partial *iopsy is o*tained, information re%ardin% the si7e andappearance of the lesion that under'ent *iopsy should *efor'arded to the interpretin% patholo%ist or dermatopatholo%ist.
• 4nterpretin% partial *iopsy samples of melanoma is not prudent,especially for patholo%ists 'ith limited e(perience in themicroscopic e&aluation of melanocytic neoplasms; notuncommonly, it can lead to a false dia%nosis of ne&us. 4f a *iopsyspecimen represents a partial sample of a lar%er lesion, the clinicianshould clearly indicate this to the dermatopatholo%ist or patholo%iston the re-uisition form. 4f any atypical feature is present, a second
opinion from an e(pert dermatopatholo%ist should *e pursued.
Consultations
Studies have clearly demonstrated that e+perience is an important factor in the
clinical diagnosis of cutaneous pigmented lesions, including both melanocytic nevi
and melanoma.

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 19/21
• Any %eneralist or primary care physician should ha&e a lo'threshold for referral to a dermatolo%ist 'hen -uestions e(istre%ardin% the clinical dia%nosis and mana%ement of a pi%mentedlesion. 4f a dermatolo%ist is not locally a&aila*le, a %eneralist 'ith adi%ital camera can nd teledermatolo%y resources readily a&aila*le
&ia the 4nternet.
• Hnce a *iopsy has *een performed on a lesion and ahistopatholo%ical dia%nosis has *een made, stron% considerationshould *e %i&en to the possi*ility of consultation 'ith a *oard5certied dermatopatholo%ist if the primary dia%nosis has *eenissued *y a %eneral patholo%ist. This is especially true if thedia%nosis of melanoma has *een for'arded or if thehistopatholo%ical dia%nosis is discordant 'ith the ori%inal clinicaldia%nosis.
• Consultation 'ith an e(perienced physician, typically adermatolo%ist, is indicated if any concern e(ists re%ardin% api%mented lesion.
• Clinical %uideline summaries are as follo's:
o The Cancer Council Australia, Australian Cancer ?et'ork,0ydney and ?e' @ealand uidelines roup 5 Con%enitalmelanocytic nae&i. Clinical practice %uidelines for themana%ement of melanoma in Australia and ?e' @ealand 1#23
o innish Medical 0ociety Duodecim 50kin cancer1#63
o 0cottish 4ntercolle%iate uidelines ?et'ork 5 Cutaneousmelanoma. A national clinical %uideline1#3
Diet
>iet is not kno'n to be related to the development of melanocytic nevi.
Acti&ity
)ctivity level is unrelated to the development or occurrence of melanocytic nevi.
Medication Summary
%n current practice, medications have no role in the diagnosis or management of
melanocytic nevi.
urther 4npatient Care

7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 20/21
%npatient care is not re&uired in the diagnosis or evaluation of patients 'ith
melanocytic nevi.
Deterrence+re&ention
?reliminary evidence suggests that childhood ultraviolet radiation e+posure is
correlated 'ith the number of melanocytic nevi that develop in subse&uent years."#G$ %f
this is presumed to be true, then measures to limit ultraviolet light e+posure (eg,
'earing sunscreen, providing sun education might yield reductions in the incidence
of melanocytic nevi and melanoma over time."#B, #H$
Complications
No kno'n complications are directly related to the presence of melanocytic nevi@
ho'ever, minor surgical intervention during the biopsy or the removal of such lesions
can lead to common complications (eg, infection, hemorrhage.
+ro%nosis
he prognosis associated 'ith any single melanocytic nevus is favorable because
these lesions are benign neoplasms 'ith no potential for malignant behavior, unless
evolution of melanoma occurs.
?atients 'ith multiple melanocytic nevi or sizable melanocytic nevi appear to have an
increased lifetime risk of melanoma, 'ith the risk increasing in rough proportion to
the size and=or number of lesions.
+atient Education
?atients should be educated regarding self-e+amination of melanocytic nevi. each
patients to use an )4C>! approach, in 'hich the patient assesses the asymmetry,
border irregularity, color, diameter (size, and evolution of any given lesion. Some
authorities add an A for 0funny looking,0 suggesting that 0ugly duckling0 lesions that
differ from the patientIs other nevi should be evaluated. )n e+planation of any
changes and observations for changes are important. Nevi can change in diameter,
outline, and=or color, and they can ac&uire an itch or begin to bleed. hese changesre&uire evaluation by a trained observer to determine the malignant potential of a
lesion.
?atient handouts that illustrate these changes and their significance are available from
the )merican )cademy of >ermatology. he greater the degree of asymmetry, the
7/21/2019 Nevus Emedicine
http://slidepdf.com/reader/full/nevus-emedicine 21/21
greater the irregularity in the border, the greater the variation in color, and the greater
the diameter of the lesion, the more cause for concern.
Aor e+cellent patient education resources, see eMedicineealthIs patient education
article Mole *emoval.









![Pemphigus Vulgaris [Print] - eMedicine Dermatology Vulgaris .pdf · emedicine.medscape.com eMedicine Specialties > Dermatology > Bullous Diseases Pemphigus Vulgaris Bassam Zeina,](https://static.fdocuments.net/doc/165x107/5c984ab609d3f21c3a8b874e/pemphigus-vulgaris-print-emedicine-vulgaris-pdf-emedicinemedscapecom.jpg)





![ptosis [emedicine]](https://static.fdocuments.net/doc/165x107/577cdd4a1a28ab9e78acb3ee/ptosis-emedicine.jpg)
