Neonatal resuscitation 2015 aha guidelines update for cpr
24
Neonatal Resuscitation 2015 AHA Guidelines Update for CPR www.pediatrics.org/cgi/doi/10.1542/peds.2015-3373G doi:10.1542/peds.2015-3373G What's new?
-
Upload
chandan-gowda -
Category
Health & Medicine
-
view
587 -
download
2
Transcript of Neonatal resuscitation 2015 aha guidelines update for cpr

Neonatal Resuscitation 2015 AHA Guidelines Update for CPR
www.pediatrics.org/cgi/doi/10.1542/peds.2015-3373Gdoi:10.1542/peds.2015-3373G
What's new?


Steps of resuscitation:
1. Initial steps in stabilization.
2. Ventilate and oxygenate-O2 administration and
monitoring,PPV,PEEP,advanced airways.
3. Initiate chest compressions.
4. Administer epinephrine and/or volume.
5. Witholding and discontinuation of resuscitation.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Positivepressure ventilation
•No mention about SIP
•PEEP admisnitered in resuscitation of prterm.
•Routine application of sustained infaltionpressure>5 sec not recommended.
•PPV whenadministered to Preterm,use of PEEP-5cm is suggested.
Class 2b
Class 2b
•3 RCT, 2 cohort studies demonstrateda benefit of SIP for reducing need for mechanical ventilation,no benefit was found for reduction of mortality, BPD, or air leak.
•PPV delivered with flow infalting,selfinfalting bag or T piece resucitator.•Needs addititionof PEEP valve to self infalting bag• 2 RCT suggestedthat addition of PEEP during deliveryroom resuscitation of pretermnewborns resulted in no improvementin mortality.
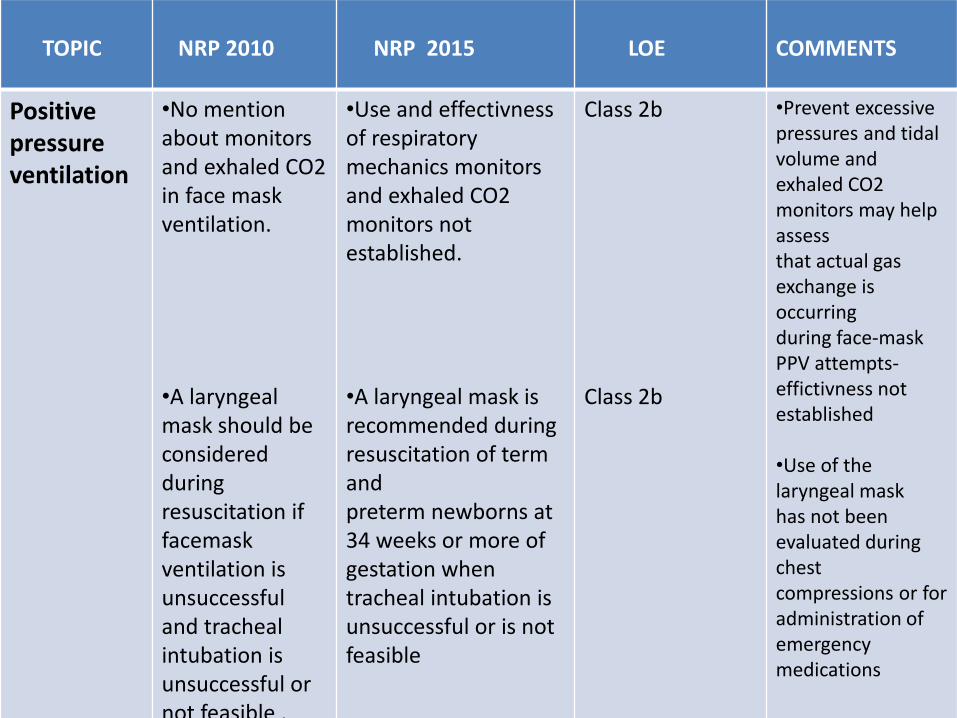
TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Positivepressure ventilation
•No mention about monitors and exhaled CO2 in face mask ventilation.
•A laryngeal mask should be considered during resuscitation if facemask ventilation is unsuccessful and tracheal intubation is unsuccessful or not feasible .
•Use and effectivnessof respiratory mechanics monitors and exhaled CO2 monitors not established.
•A laryngeal mask is recommended during resuscitation of term andpreterm newborns at 34 weeks or more of gestation whentracheal intubation is unsuccessful or is not feasible
Class 2b
Class 2b
•Prevent excessivepressures and tidal volume andexhaled CO2 monitors may help assessthat actual gas exchange is occurringduring face-mask PPV attempts-effictivness not established
•Use of the laryngeal maskhas not been evaluated during chestcompressions or for administration ofemergency medications

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Positivepressure ventilation
Spontaneously breathing preterm infants who have respiratory distress may be supported with CPAP or with intubation and mechanical ventilation.
CPAP: Spontaneously breathing preterm infantswith respiratory distress may be supported with CPAP initially ratherthan routine intubation for administering PPV .
Class 2b 3 RCT enrolling 2548 preterms-Starting CPAP resulted indecreased rate of intubation in thedelivery room, decreased duration of ventilation with reduction of death and BPD, and nosignificant increase in air leak or severeIVH.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
O2 in Preterm infants
•Recommended that whether born at term or preterm, should be an oxygen saturation value in the interquartilerange of preductalsaturations.
•<35 wks GA begin resuscitation with low O2{21%-30%}
•Titrate according to preductal SpO2.
•Initiating resuscitationof preterm newborns with high oxygen (65% or greater) is not recommended
Class 1,LOE B-R
Class III
Meta-analysis of 7 RCT-initiation with high oxygen(65% or greater) and low oxygen (21- 30%) showed no improvement insurvival to hospital discharge with the use of high oxygen.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
O2 in term infants
Initiating resuscitation with air or a blended oxygen and titrating the oxygen concentration to achieve an SpO2 in the target range as described above using pulse oximetry .
Initiate resuscitationwith air (21% ) Supplementaryoxygen may be administeredand titrated to achieve a preductaloxygen saturation approximating the interquartilerange measured in healthyterm infants after vaginal birth at sealeve

• PPV-Flow infalting,self infalting or T piece resuscitator.
• When administeringPPV for preterm provide PEEP of 5cm .
• Initiate PPV in room air for Term and Fio2 21-30% for preterm infants.
• LMA can be used >34 wk GA infant when intubation is not successful.
• CPAP rather than routine intubation for spontaneously breathing preterm infants with respiratory distress

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Chestcompression
Indicated for a heart rate that is <60 per minute despite adequate ventilation with supplementary oxygen for 30 seconds.
Compressions should be delivered on the lower third of the sternum to a depth of approximately one third of the A-P diameter of the chest .
If the heart rate is less than 60/min despite adequate ventilation (via endotrachealtube if possible), chest compressions are indicated
Compressions are delivered on the lower third of the sternum to a depth of approximately one third of the anterior-posterior diameter of the chest.
Class 2b No change in recommendation

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Chestcompression
•The 2 thumb–encircling handstechnique is recommended for performing chest compressions in newly born infants .
• The 2-finger technique may be preferable when access to the umbilicus is required during insertion of an umbilical catheter.
2-thumb technique generates higher blood pressuresand coronary perfusion pressure with less rescuer fatigue, the 2thumb–encircling hands technique is suggested as the preferredMethod
2-thumb technique can be continued from the head of the bed while the umbilicus is accessed for insertion of an umbilical catheter, the 2-finger technique is no longer needed.
Class 2b

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Chestcompression
Same 3:1 where gas exchange is nearlyalways the primary cause of cardiovascular collapse, butrescuers may consider using higher ratios (eg, 15:2) if the arrestis believed to be of cardiac origin
Class 2b

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Chestcompression
If the baby is bradycardic (HR <60 per minute) after 90 seconds of resuscitation with a lower concentration of oxygen, O2concentration should be increased to 100% until recovery of a normal heart rate .
•Endorses increasing the oxygen concentration to 100% whenever chest compressions are Provided
•Supplementary oxygen concentration should be weaned as soon as the heart rate recovers
Class 2b
Class 1
Animal evidence show no advantage to 100% oxygen during CPR.By the time resuscitationof a newborn infant has reached the stage of chest compressions,efforts to achieve return ofspontaneous circulation using effective ventilation with lowconcentrationoxygen should have been attempted

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Chestcompression
•HR used for assesment of ROSC.
•Current measure for determining successful progress inneonatal resuscitation is to assess the heart rate response.
Class 2b • ET CO2 monitoring and pulse oximetry,useful techniques to
determine return ofspontaneous circulation occurs.
•In asystolic/bradycardic neonates, routine use of anydevice such as ETCO2
monitors or pulseoximeters for detection of ROSC, is not recommended astheir usefulness for this purpose in neonates has not been wellEstablished.

• Chest compression if HR<60 despite adequate ventilation.
• Compression delivered over lower third of sternum.
• Compression to ventilation ratio of 3:1.
• 2 thumb and 2 finger technique.
• 2 finger technique no longer recommended.
• Use 100% O2 whenever compressions are administered.
• Assesment of HR is best measure to assess progress, use of ET CO2 and oximetry not routinely recommended.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Induced Therapeutic HypothermiaResource-Limited Areas
Should be administered under clearly defined protocols similar to those used in published clinical trials and in facilities with the capabilities for multidisciplinary care and longitudinal follow-up
Use of therapeutic hypothermia in resource limitedsettings may be considered and offered under clearly definedprotocols .
Class 2b

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Guidelines for Withholding andDiscontinuing
•Not indicated-almost certain death and unaccepatablehigh morbidity.
•Nearly always indicated-High rate of survival and acceptable morbidity.
•Borderline-survival borderline and morbidity is relatively high,parentaldesires shouldbe supported.
•For GA<25 wks,consideraccuracy of GA, the presence or absenceof chorioamnionitis, and the level of care available .
•Decision to be influenced by region-specific guidelines.
No new data have Been published that would justify a change to these guidelines as published in 2010.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Guidelines for Withholding andDiscontinuing
In a newly born baby with no detectable heart rate, it is appropriate to consider stopping resuscitation if the heart rate remains undetectable for 10 minutes .
Infants with an Apgarscore of 0 after 10 minutes ofresuscitation, if the heart rate remain undetectable, it may be reasonableto stop assisted ventilations.
Class 2b Decision to continue ordiscontinue resuscitative efforts must be individualized-etiology,GA,associated complications,role of hypothermia .

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Provider training:
2010 Guidelines suggested that simulation should become a standard component in neonatal resuscitation training
Suggested that neonatal resuscitation task training occurmore frequently than the current 2-year interval.

TOPIC NRP 2010 NRP 2015 LOE COMMENTS
Instructor training:
None Instructors be trained usingtimely,objective
structured, and individuallytargeted verbal and/orwritten feedback .

Unchanged Recommendations:
TOPIC RECOMMENDATION
Temperature control Resuscitation should be performed with temperature-controlling interventions.
Clearing the airway when amniotic fluid is clear
Routine suctioning is not recommended
Assessment of need of oxygen therapyand monitoring of oxygen therapy
Oximetry should be used to monitor if any neonate needs PPV, with persistent central cyanosis persists and with the use of supplementary oxygen.
Initial breaths and assisted ventilation An initial inflation pressure of 20 cm water is adequate; some term babies mayrequire up to ≥30 to 40 cm water. Rate of giving PPV- 40 to 60 per minute.

Unchanged Recommendations:
TOPIC RECOMMENDATIONS
Endotracheal tube placement Exhaled CO2 detection is most reliable.
Chest compressions Coordinated chest compressions and PPV should be done if heart rate<60 perminute after establishing effective ventilation
Epinephrine IV dose - 0.01 to 0.03 mg/kg of 1:10 000 epinephrine. For an endotracheal route- 0.05 to 0.1 mg/kg
Volume Expansion Volume expansion when blood loss is known/suspected.Dose - 10 mL/kg ofisotonic crystalloid solution or blood, may be repeated.

Thank you