
2015 AHA GUIDELINES UPDATE FOR CPR AND ECC - … in 2015 AHA CPR... · 2015 aha guidelines update...
36
2015 AHA GUIDELINES UPDATE FOR CPR AND ECC - HIGHLIGHTS Steve Lin, MD, MSc, FRCPC Emergency Physician, Trauma Team Leader, St. Michael's Hospital Scientist, Rescu, Li Ka Shing Knowledge Institute Assistant Professor, Department of Medicine, University of Toronto
Transcript of 2015 AHA GUIDELINES UPDATE FOR CPR AND ECC - … in 2015 AHA CPR... · 2015 aha guidelines update...

2015 AHA GUIDELINES UPDATE FOR CPR AND ECC - HIGHLIGHTS
Steve Lin, MD, MSc, FRCPC Emergency Physician, Trauma Team Leader, St. Michael's Hospital
Scientist, Rescu, Li Ka Shing Knowledge Institute Assistant Professor, Department of Medicine, University of Toronto
SPEAKER DISCLOSURES
• No financial conflicts
• Evidence Reviewer for ILCOR • Chapter Author for 2015 AHA Guidelines for CPR and ECC

INTERNATIONAL EVIDENCE EVALUATION AND COUNCIL
GUIDELINES

ACHIEVING CONSENSUS REGARDING RESUSCITATION SCIENCE The American Heart Association and other member councils of International Liaison Committee on Resuscitation (ILCOR) complete a review of resuscitation science every five years.
Australian Resuscitation
Council
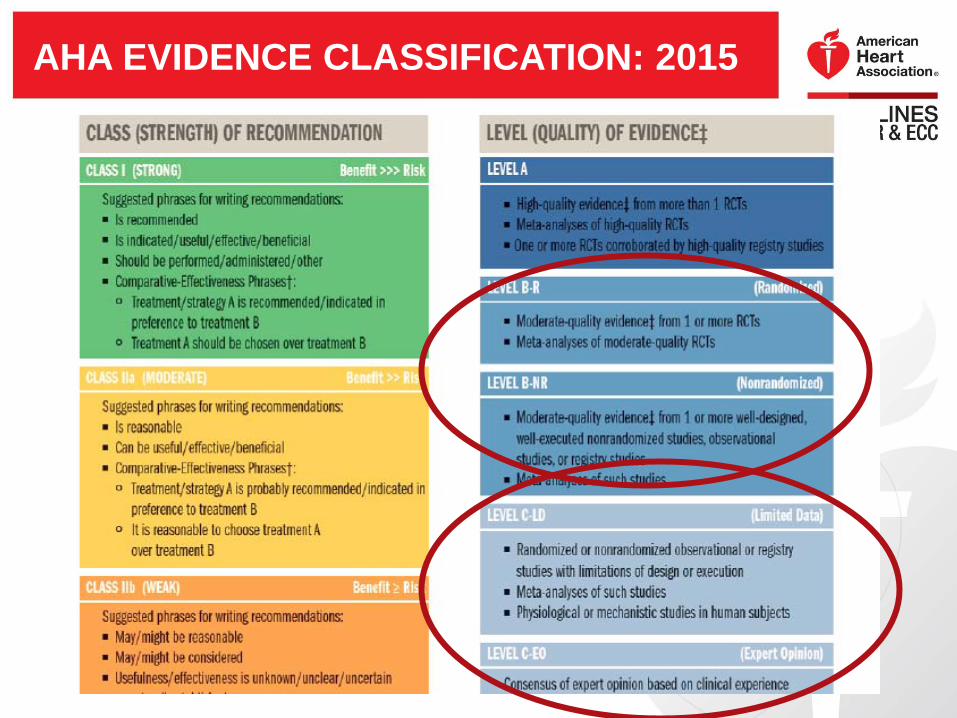
AHA EVIDENCE CLASSIFICATION: 2015

AHA RECOMMENDATION CLASSIFICATION: NEW CLASS III

KEY NEW AND UPDATED RECOMMENDATIONS:
SYSTEMS OF CARE

UNIVERSAL TAXONOMY FOR SYSTEMS OF CARE: NEW

NEW AHA ADULT CHAINS OF SURVIVAL
IN-HOSPITAL (note new Surveillance and Prevention link)
OUT-OF-HOSPITAL, Including EMS

SOCIAL MEDIA TO SUMMON RESCUERS?
Recommendation: • It may be reasonable to
incorporate social media technologies to summon rescuers in close proximity to a victim.
Why? • Low evidence, but low
harm and potential benefit, municipalities could consider incorporating into their system.
Screen shot from San Ramon Fire Department website: http://mobile.firedepartment.org/?rev=0?reload
EARLY WARNING/RAPID RESPONSE SYSTEMS
• May reduce incidence of cardiac arrest, particularly on general care wards

KEY NEW AND UPDATED RECOMMENDATIONS:
ADULT BLS

DISPATCHER IDENTIFICATION OF AGONAL GASPS: UPDATED
Recommendation: • Dispatchers should be trained to identify agonal gasps and other presentations of cardiac arrest
• Allows for immediate dispatcher-guided CPR
Why? • Dispatchers should be trained to
recognize agonal gasping

CHEST COMPRESSION RATE: UPDATED
Recommendation: • Compression rate: 100-120/minute.
–2010 recommendation: Compression rate at least 100/min.
Why? • Absolute number of compressions
delivered per minute linked with survival.
• Actual compression rate is often well below 100/minute.
• Rates below 100/min or above 120/min adversely affect outcomes.

ADULT CHEST COMPRESSION DEPTH: UPDATED Recommendation: •Compress at least 2 inches (5cm) for average adult • Avoiding excessive compression depth (greater than 2.4 inches [6cm])
–2010 recommendation was at least 2 inches
Why? • In one study of 170 patients
(Hellevuo et al, Resuscitation, 2013) injuries occurred with depths greater than 2.4 inches (6cm).
Note: • Difficult to judge depth without CPR feedback
devices • Rescuers often do not “push hard” enough

CHEST COMPRESSIONS ARE CRITICAL
Without effective chest compressions: • Oxygen flow to brain stops. • Oxygen flow to heart stops. • Drugs go nowhere.

BYSTANDER NALOXONE FOR OPIOID OVERDOSE: NEW
Recommendation: • In additional to
standard BLS care, trained lay rescuers and BLS providers may use IM or IN Naloxone for life-threatening emergency with suspected opioid overdose.

BLS SEQUENCES FOR CPR
• Allow for ubiquitous mobile phones (rescuers can remain with victim and activate emergency response system)
• Mobile phone should be placed beside victim on “speaker” so dispatcher can guide rescuer in CPR
• Enable Health Care Provider to tailor activation to clinical setting (but no later than when cardiac arrest identified)

HEALTHCARE PROVIDER ADULT BLS SEQUENCE: UPDATED
•Verify scene safety •Recognize unresponsive adult •Simultaneously check no breathing /no normal breathing (ie, agonal gasps) and check for pulse (10 sec or less)
•Activate emergency response, retrieve AED (or send someone to do this)
• If no breathing and no pulse, begin sets of 30 chest compressions: 2 breaths
•Use AED as soon as available

G2015 BLS ALGORITHM—PART 1 OF 2

G2015 BLS ALGORITHM—PART 2 OF 2

SUMMARY OF HIGH-QUALITY CPR COMPONENTS FOR BLS PROVIDERS

SUMMARY OF HIGH-QUALITY CPR COMPONENTS FOR BLS PROVIDERS—PART 2

DELAYED VENTILATION BY SOME EMS PROVIDERS Recommendation: • For witnessed OHCA with a shockable rhythm, EMS
systems with priority-based multi-tiered response may use a strategy of up to 3 cycles of 200 continuous compressions with passive oxygen insufflation and airway adjuncts.
Why? • Delaying PPV for victims with witnessed arrest and
shockable shown to be effective in these systems.
• In studies cited, providers received additional training with emphasis on high-quality compressions.

VENTILATION DURING CPR WITH AN ADVANCED AIRWAY: UPDATED
Recommendation: • May be reasonable to deliver 1
breath every 6 seconds (10 breaths/min) while continuous chest compressions are being performed (adult and peds).
Why? • Simplified from range of 1
breath every 6-8 seconds (8-10 breaths/min).
• Should be easier to learn, remember, and perform.
TEAM RESUSCITATION: BASIC PRINCIPLES: NEW
Recommendation: • Increased flexibility for
modifications in BLS algorithm when appropriate.
Why: • Algorithms have been
presented as a sequence to prioritize actions; certain factors may require localized modifications.

KEY NEW AND UPDATED RECOMMENDATIONS:
ACLS

VASOPRESSORS IN CARDIAC ARREST
Recommendations: • Vasopressin + epinephrine offers no advantage over standard
dose epinephrine—vasopressin deleted from ACLS Cardiac Arrest algorithm.
• It may be reasonable to administer epinephrine as soon as feasible after the onset of cardiac arrest with initial nonshockable rhythm
Why? • No benefit from addition of vasopressin vs epinephrine alone. • Very large observational study found association of better
outcome (increased ROSC, survival to hospital discharge, and neurologically intact survival) with early vs later epinephrine administration.

LOW ETCO2 ONE ELEMENT PREDICTING FAILED RESUCITATION? Recommendation: • In intubated patients, failure to achieve an ETCO2
greater than 10 mm Hg by waveform capnography after 20 minutes of CPR may be considered one component of a multimodal approach to decide when to end resuscitative efforts but should not be used in isolation
• Efforts should be made to optimize CPR quality
Why? • Failure to achieve an ETCO2 greater than 10 mm
Hg after 20 minutes associated with poor outcome
• Low ETCO2 likely indicates very low cardiac output and pulmonary blood flow during CPR

POST-CARDIAC ARREST DRUG THERAPY: NEW
Lidocaine • Inadequate evidence to support the
routine use of lidocaine after cardiac arrest. It may be considered immediately after ROSC from cardiac arrest due to VF/pVT.
β-Blockers • Inadequate evidence to support the
routine use of a β-blocker after cardiac arrest. However, the initiation or continuation of an oral or IV β-blocker may be considered early after hospitalization from cardiac arrest dueto VF/pVT.

KEY NEW AND UPDATED RECOMMENDATIONS:
POST-CARDIAC ARREST CARE

POST-CARDIAC ARREST ELEMENTS OF CARE: UPDATED • Emergent coronary angiography:
• Should be performed for OHCA patients with suspected cardiac etiology and ST elevation on ECG.
• May be reasonable for patients who are comatose after OHCA with a cardiac etiology and no ST elevation.
• Reasonable post-arrest where indicated, whether comatose or awake.
• Targeted temperature management
• Avoid and correct hypotension

TARGETED TEMPERATURE MANAGEMENT
• Targeted Temperature Management (TTM) between 32°C and 36°C
• Continue TTM beyond 24 hours by actively preventing fever if patient still comatose.
• Routine prehospital cooling of patients with rapid infusion of cold IV fluids is not recommended (no benefit, possible complications)
PROGNOSTICATION FOR POOR OUTCOME USING CLINICAL EXAM
• Patients not treated with TTM –72 hours or later after cardiac arrest –Longer interval after cardiac arrest (ie, beyond 72 hours) needed if residual effect of sedation or paralysis is suspected to confound clinical exam.
• Patients treated with TTM –Reasonable to wait 72 hours after return to normothermia if sedation or paralysis could confound clinical examination
POTENTIAL ORGAN DONORS POST-CARDIAC ARREST
• All patients resuscitated from cardiac arrest who progress to death or brain death should be evaluated as potential organ donors.
• Patients who do not achieve ROSC and would otherwise have resuscitation terminated may be considered as potential kidney or liver donors in settings where rapid organ recovery programs exist.

QUESTIONS?


















