Neonatal hyperbilirubinemia JFK pediatric core curriculum MGH Center for Global Health Pediatric...
26
Neonatal hyperbilirubinemia JFK pediatric core curriculum MGH Center for Global Health Pediatric Global Health Leadership Fellowship Credits: Brett Nelson, MD, MPH Rachel Siegel, MD Susan O’Brien, MD
-
Upload
meghan-stafford -
Category
Documents
-
view
215 -
download
0
Transcript of Neonatal hyperbilirubinemia JFK pediatric core curriculum MGH Center for Global Health Pediatric...

Neonatal hyperbilirubinemiaJFK pediatric core curriculum
MGH Center for Global HealthPediatric Global Health Leadership Fellowship
Credits:Brett Nelson, MD, MPH
Rachel Siegel, MDSusan O’Brien, MD

Discussion outline
• Bilirubin pathophysiology
• Physiologic and non-physiologic jaundice
• Causes of non-physiologic jaundice– Unconjugated hyperbilirubinemia– Conjugated hyperbilirubinemia
• Workup
• Treatment

Bilirubin pathophysiology
• Bilirubin is breakdown product of heme, from circulating RBCs
• Carried by albumin to hepatocytes, where processed for excretion
• In hepatocytes, uridine diphosphogluconurate glucuronosyltransferase (UGT) catalyzes conjugation of bilirubin with glucuronic acid
• Conjugated bilirubin is now more water soluble and can be excreted in bile (and urine)

Bilirubin pathophysiology

Epidemiology: neonatal jaundice
• Neonatal jaundice is quite common– >50% of normal newborns and– 80% of preterm infants have some degree of
jaundice
• Two types of neonatal jaundice:– Normal / physiological– Abnormal / non-physiological

Reasons for physiologic jaundice
• In term newborns, bilirubin production is 2-3 times higher than in adults– Hematocrit of 50-60%, shorter RBC life span (90
days), and increased turnover of RBCs
• Bilirubin clearance decreased in newborns, mainly due to deficiency of enzyme UGT– UGT activity in term infants at 7 days is ~1% of adult
liver and doesn’t reach adult levels until 14 weeks
• Increase enterohepatic circulation of bilirubin, further increasing bilirubin load

Greater concerns in preterm infants
• Even more RBC turnover and destruction
• Physiologically impaired conjugation and elimination of bilirubin– An even less mature liver– Reduced bowel motility due to inadequate
oral intake– Delayed elimination of meconium– Increased enterohepatic circulation

Physiologic jaundice
• Jaundice appears around 72 hrs of life• Bilirubin peaks <14 mg/dl• Direct bilirubin <10% of total bilirubin• Rate of rise <5mg/dL/day• Jaundice resolves in 1-2 weeks in term
infants, 2 weeks in preterm infants
• Otherwise the jaundice is abnormal…

Two forms of hyperbilirubinemia
• Unconjugated / indirect hyperbilirubinemia: – Pre-hepatic cause, or impairment in conjugation
VS.
• Conjugated / direct hyperbilirubinemia: – Injury at the level of the hepatocytes, or post-hepatic
obstruction– Consider diagnosis of conjugated hyperbilirubinemia if
direct bilirubin is >3mg/dL, or is >10% of total bilirubin

Non-physiologic jaundice
• Early jaundice– Starts on first day of life
• Jaundice of long duration– >14 days in term or >21 days in preterm
infants
• Deep jaundice– Palms and soles deep yellow– Objectively, high bilirubin lab levels
• Jaundice with fever

Differential diagnosis: Unconjugated hyperbilirubinemia
• Breastfeeding jaundice– Occurs at 1-3 days of age; due to dehydration and lack of stooling (treat by increasing
feeding frequency)• Breast milk jaundice
– Occurs at 4-10 days of age; substance in breast milk inhibits glucuronyl transferase (treat by temporary switch to formula)
• Hemolysis– ABO/Rh incompatibility– RBC membrane defects– Alpha thalassemia– G6PD deficiency– Cephalohematoma– Polycythemia
• Infection• Hypothyroidism• Gilbert’s
– impaired conjugation, associated with stress, no overt hemolysis• Crigler-Najjar’s
– absent (type 1) or diminished (type 2) UDP-glucoronyl transferase

Differential diagnosis: Conjugated hyperbilirubinemia
• Biliary atresia– ~60% of cases; an obliterative process of bile ducts; diagnosed by U/S
or biopsy• Infection
– Hepatitis B, TORCH• Metabolic
– Galactosemia– Alpha-1-antitrypsin deficiency: most common genetic cause– Dubin Johnson or Rotor’s syndrome: defective liver secretion of bilirubin
• Iatrogenic– Drug-mediated– TPN-related: occurs in ~2/3 of infants given TPN over 2 weeks of
duration; unknown mechanism, possibly mediated by bacterial endotoxins, oxidative stress, glutathione depletion
• Idiopathic– neonatal non-infectious hepatitis (diagnosis of exclusion)

The concern: Kernicterus
• Bilirubin exceeds albumin-binding capacity, crosses BBB, and deposits on basal ganglia and brainstem nuclei
• Risks increase with levels >20 mg/dl– Or lower levels in setting of sepsis,
meningitis, hemolysis, hypothermia, hypoglycemia, or prematurity

Signs of kernicterus
• Acute sequelae:– Poor suck, lethargy, hypotonia, seizure– Then hypertonia (opisthotonus, retrocollis),
fever, high-pitched cry
• Chronic sequelae:– Choreoathetoid CP, gaze paresis,
sensorineural hearing loss, mental retardation

Cause analysis of kernicterus
• Early discharge <48hrs without follow-up within 48hrs
• Failure to check bilirubin level when jaundice within 24hrs of life
• Failure to recognize risk factors• Underestimating severity by visual
assessment• Delay in initiating treatment• Failure to respond to parental concerns
AAP Subcommittee on Neonatal Hyperbilirubinemia. Pediatrics 2001; 108: 763-765.
Work up: assess risk factors
• Maternal:– Race or ethnic group
(Asian, Mediterranean)– ABO, Rh incompatibility– Previous jaundiced infant– Advanced maternal age– Diabetes
• Infant:– Gestation <38 weeks– Bruising, cephalohematoma– Infection– G6PD deficiency– Polycythemia– Male gender
• Nutritional:– Breastfeeding– Weight loss– Decreased feeding
frequency– Decreased stooling– Decreased urine output

Work up: laboratory studies
• Where possible, confirm clinical jaundice with bilirubin levels
• Possible additional investigations, depending on likely diagnoses and lab availability:– Hemoglobin/hematocrit (PCV) to look for hemolysis– Blood smear– Reticulocyte count– WBC to look for signs of infection (WBC <5, WBC>20, or I:T
ratio >20%)– Blood type of baby and mother, and Coombs test– Syphilis serology (e.g. VDRL)– G6PD screen, thyroid function tests, liver ultrasound

Treatment options: Unconjugated hyperbilirubinemia
• Hydration / feeding– Consider formula supplementation with temporary
interruption of breastfeeding
• Phototherapy… (see next slide)• Antibiotics if suspected infection• Antimalarials if fever and positive smear
• (Exchange transfusion)• (IVIG in immune-mediated red cell destruction)
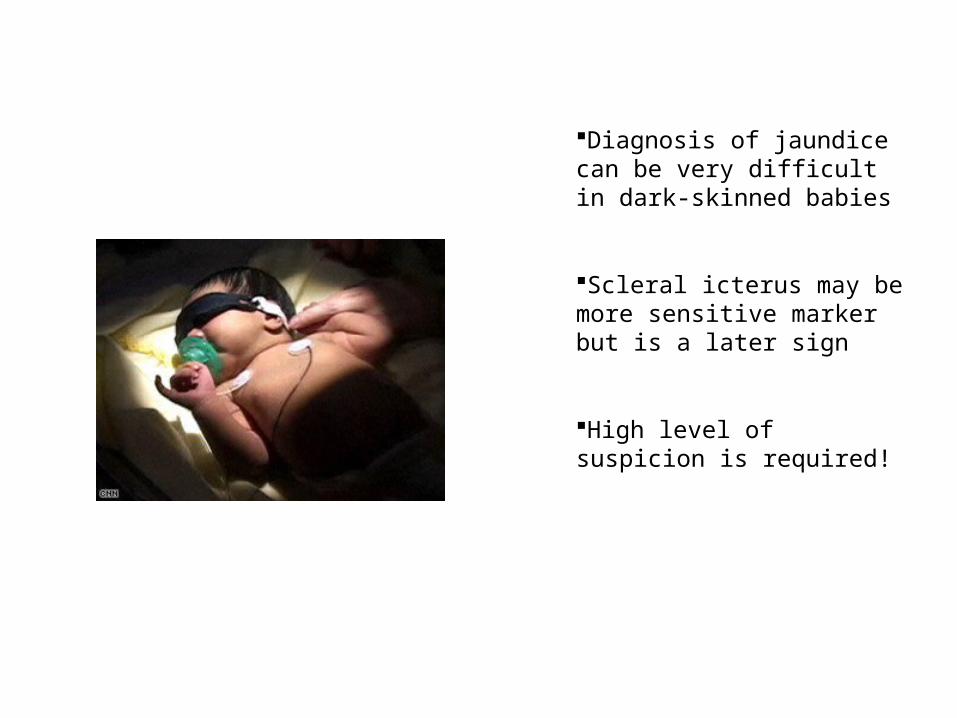
Diagnosis of jaundice can be very difficult in dark-skinned babies
Scleral icterus may be more sensitive marker but is a later sign
High level of suspicion is required!

Phototherapy
• Clinical indications1:– Jaundice on day 1– Jaundice in premature infant– Deep jaundice involving palms and soles
of the feet
• Laboratory indications:– In full-term infants, bilirubin levels per
Bhutani curves– In premature infants, when bilirubin level
≥5x weight (e.g. threshold for 3kg newborn = 3kg x 5 = 15mg/dl)
1. Pocket Book of Hospital Care for Children. WHO. 2005.

Nomogram for designation of risk in 2840 well newborns at 36 or more weeks' gestational age with birth weight of 2000 g or more or 35 or more weeks' gestational age and birth weight of 2500 g or more based on the hour-specific serum bilirubin values. (Subcommittee on Hyperbilirubinemia, Pediatrics 2004;114:297-316)
Bhutani curve: identifying risk
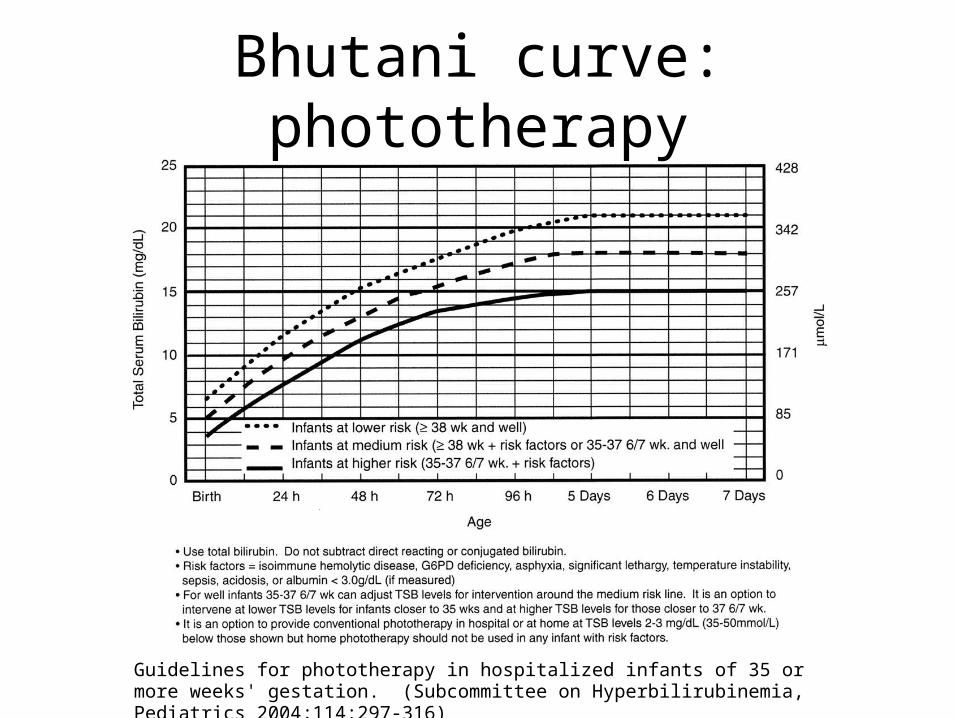
Guidelines for phototherapy in hospitalized infants of 35 or more weeks' gestation. (Subcommittee on Hyperbilirubinemia, Pediatrics 2004;114:297-316)
Bhutani curve: phototherapy

WHO guidelines: phototherapy
Pocket Book of Hospital Care for Children. WHO. 2005.

Key points regarding treatment:
• Bilirubin levels above 20 are an emergency that need to be treated emergently
• Multiple unit phototherapy, up to 6-8 lights, if they are available, can and should be used
• If bilirubin is high, need to provide multi-unit therapy, encouragement of frequent feeding and possibly IV fluids as well

Treatment: Conjugated hyperbilirubinemia
• Phototherapy is contraindicated• Treat underlying cause
• Phenobarbital– increases conjugation and excretion of bilirubin;
however, could affect cognitive development, therefore used cautiously
• Ursodiol– increases biliary flow and improves cholestatic
jaundice

Conclusion
• Neonatal jaundice is a very common condition• Important to prevent kernicterus• Pathologic jaundice is early, deep, quickly
progressing, or of long duration • Assess jaundice through identifying risk factors
and laboratory analysis• Bhutani curves guide phototherapy treatment for
unconjugated hyperbilirubinemia• Treat underlying cause of conjugated
hyperbilirubinemia