Neonatal Assisted Ventilation - WSRC Assisted Ventilation - NRRCC 2007.… · History of Assisted...
35
Neonatal Neonatal Assisted Assisted Ventilation Ventilation Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI.
Transcript of Neonatal Assisted Ventilation - WSRC Assisted Ventilation - NRRCC 2007.… · History of Assisted...

Neonatal Neonatal Assisted Assisted VentilationVentilation
Haresh Modi, M.D.Aspirus Wausau Hospital, Wausau, WI.

History of Assisted VentilationHistory of Assisted Ventilation
Spirophoredeveloped in 1876 with manual device to create negative pressure chamber
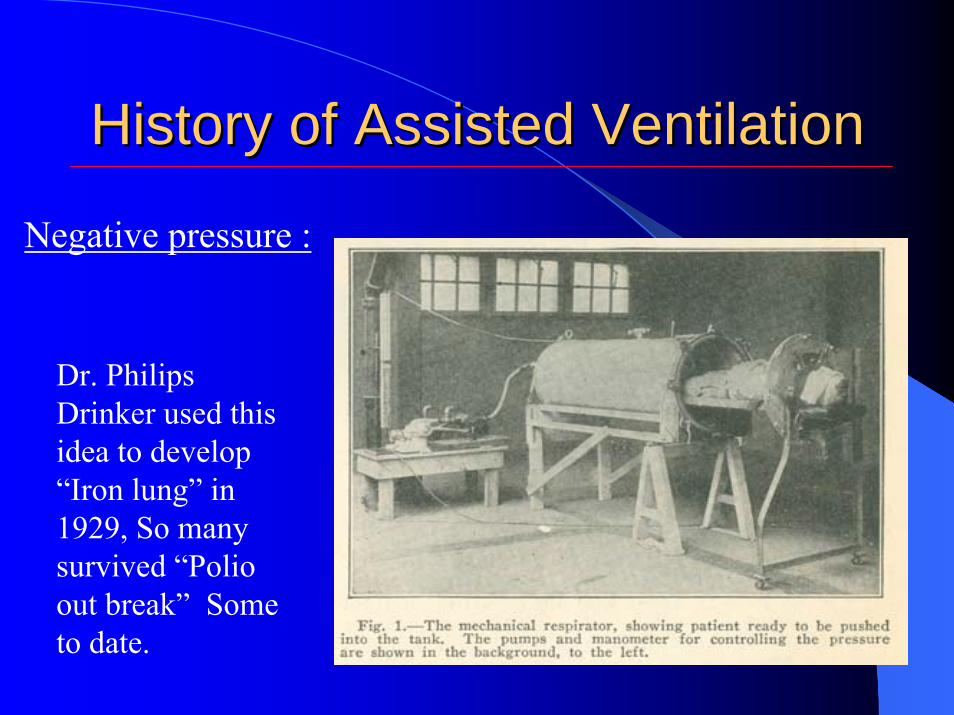
Negative pressure :
History of Assisted VentilationHistory of Assisted Ventilation
Dr. Philips Drinker used this idea to develop “Iron lung” in 1929, So many survived “Polio out break” Some to date.
Negative pressure :

Woman in iron lung celebrates 60th birthdayAfter contracting polio, Dianne Odell has spent
most of her life in machine
Updated: 3:37 p.m. CT Feb 21, 2007Associated Press Report
JACKSON, Tenn. - A Jackson woman who contracted polio 57 years ago and continues to rely on an iron lung to breathe recently celebrated her 60th birthday, defying doctors' expectations that she could live so long and so fully. Dianne Odell, who turned 60 last week, is among only 30 to 40 people in the U.S. who depend on the devices.

History of Assisted VentilationHistory of Assisted Ventilation
“Respirator Kit”used to revive apparently dead by blowing air into the lungs or rectum in 1770s in London
Positive Pressure :

History of Assisted VentilationHistory of Assisted Ventilation
The Aerophore pulmonaire :-developed by French Obstetrician for short term ventilation of newborns in 1879
Positive pressure :

History of Assisted VentilationHistory of Assisted Ventilation
The Fell-O’Dwyreapparatus developed in New York for intermittent positive pressure ventilation, 1896
Positive pressure :

Neonatal Assisted VentilationNeonatal Assisted Ventilation
1. Applied Pulmonary Mechanics2. Gas Exchange During Assisted Ventilation3. Ventilator Management4. Practical Hints For Assisted ventilation
Applied Pulmonary MechanicsApplied Pulmonary MechanicsPressure Gradient is Required to Overcome
1.Elastic Properties of Lungs and Chest Wall(Compliance)
2. Resistance to Airflow by Airway and Lung Tissue (Resistance)

Applied Pulmonary MechanicsApplied Pulmonary Mechanics
Δ Volume (L)Δ Pressure (cm H2O)
Compliance =
In neonate chest wall is very distensible so does not contribute substantial elastic load when compared to lungs.
Total compliance ∞ Lung compliance
In RDS most striking abnormality is
DECREASED LUNG COMPLIANCE

Applied Pulmonary MechanicsApplied Pulmonary MechanicsPressure Gradient is Required to Overcome
1.Elastic Properties of Lungs and Chest Wall(Compliance)
2. Resistance to Airflow by Airway and Lung Tissue (Resistance)

Applied Pulmonary MechanicsApplied Pulmonary Mechanics
Δ Pressure(cm H2O)Δ Flow (L/Sec)
Airway resistance ∞ length of airway∞ 1/radius of airway
Viscous resistance ∞ lung tissue
RDS does not contribute to resistance but ET tube does
Resistance =
Resistance is inherent property of lungs to resist airflow

Relationship of Compliance and Resistance :
Time Constant (sec)= Resistance × Compliance
Applied Pulmonary MechanicsApplied Pulmonary Mechanics
Time Constant(sec)
= Resistance(30cm H2O/L/sec)
× Compliance(0.004L/cm H2O)
= 0.12sec × 5
= 0.6 seconds

Gas Exchange During Gas Exchange During Assisted VentilationAssisted Ventilation
1. Carbon Dioxide (CO2) Elimination
2. Oxygen (O2) Uptake

Gas Exchange During Gas Exchange During Assisted Ventilation Assisted Ventilation
CO2 Elimination :
Alveolar Ventilation =(Tidal volume – Dead space)(Frequency)
With a pressure ventilator TV determined by(PIP – PEEP)

Gas Exchange During Gas Exchange During Assisted VentilationAssisted Ventilation
O2 Uptake : Mean Airway Pressure(Paw)linear direct relations
↑Paw = ↑ PaO2
Regardless of change in FiO2
Paw optimizes lung volume and ventilation-perfusion matching

Gas Exchange During Gas Exchange During Assisted VentilationAssisted Ventilation
Paw is augmented by : 1. Inspiratory flow (K)2. Peak Inspiratory Pressure (PIP)3. I:E Ratio(TI, TE)4. Positive End Expiratory Pressure
(PEEP)
1 2 3 4
Paw=K(PIP-PEEP)[TI/(TI+TE)]+PEEP

Ventilator ManagementVentilator Management1. Flow :
Increase in flow will give square wave ventilation, will Increase Paw and therefore oxygenation.
Higher flow is crucial, when TI is shorter

Ventilator ManagementVentilator Management2. Peak Inspiratory Pressure (PIP) :
Δ PIP(Press.Vent.) = Δ TV (Volu.Vent.)Advantages : Disadvantages :1. O2 Uptake 1. Barotrauma Air leaks2. CO2 Elimination 2. BPD
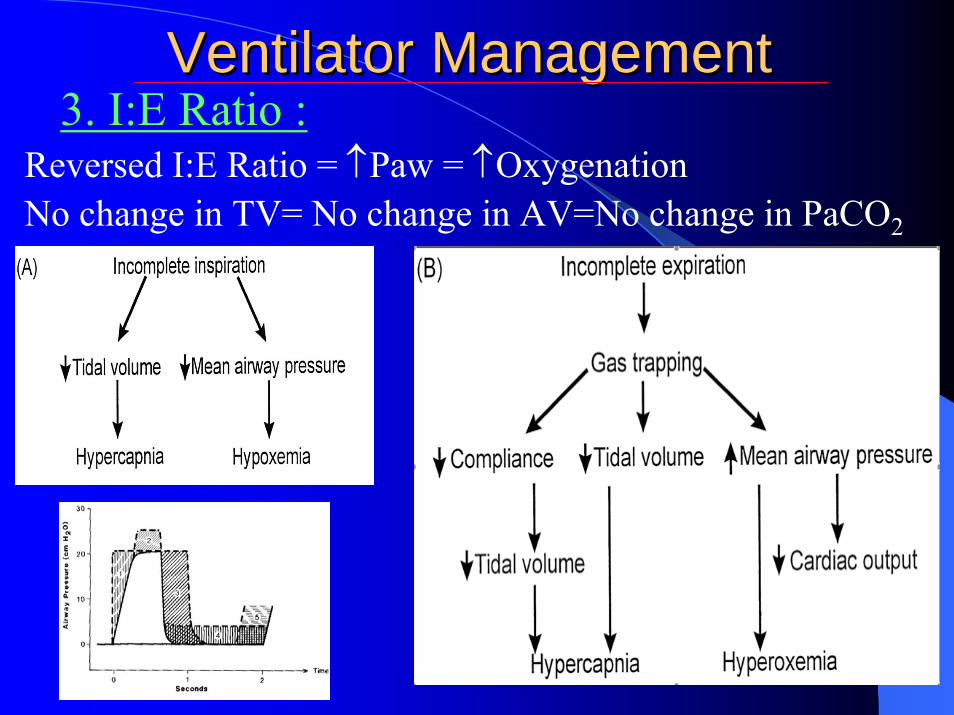
Ventilator ManagementVentilator Management3. I:E Ratio :
Reversed I:E Ratio = ↑Paw = ↑Oxygenation No change in TV= No change in AV=No change in PaCO2

Ventilator ManagementVentilator ManagementFrequency (Rate) :
Rate= AV= CO2 elimination= PaCO2
Short TI= TV= MVShort TE=gas trapping= FRC= compliance with over
distention= inadverant PEEP=Pneumothorax

Ventilator ManagementVentilator Management4. PEEP :
↑ PEEP(at lower range)= Better recruitment of lungs = ↑ PaO2
↑ PEEP(at higher range)=Over distention=↓Cardiac Output=↓PaO2, ↑PaCO2
PEEP just above Critical closing Pressure prevents atelectesis

Gas Exchange During Gas Exchange During Assisted VentilationAssisted Ventilation
Relative effectiveness of Paw on Pao2 :1.↑ PIP &PEEP more than ↑ I:E ratio2.↑ PEEP at higher range is ineffective3.↑Paw=↑Over distention=↑RL Shunt 4.↑ Paw = ↓Cardiac output
Ventilator ManagementVentilator Management
Inspired Oxygen Concentration (FIO2) :
When increasing vent. support first increase FIO2 to .60 to .70 before increasing pressure which may prevent BPD
When weaning vent. support first decrease FIO2 to .40 to.50 before decreasing pressure. Pressure should be weaned before weaning FIO2 further to prevent PTX.

Gas Exchange During Gas Exchange During Assisted VentilationAssisted Ventilation
Summary :-

Ventilator ManagementVentilator ManagementHFOV :
Ventilation above critical closing pressure at ↑PEEP &↑Paw =↑PaO2↓∆P at alveolar level=↑ alveolar ventilation = ↓PaCO2

Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation
Indications for Assisted Ventilation :
1. Respiratory acidosis with pH < 7.20 to 7.252. Severe hypoxemia, PaO2 < 50 torr. With FIO2 > 0.703. Apnea complicating RDS4. Persistent Fetal Circulation

Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation
Initial Ventilator Settings :
Normal RDSPIP 12-18 cm H2O 20-25 cmH2OPEEP 2-3 cmH2O 4-5 cmH2ORate 10-20 per minute 20-40 per minuteI:E Ratio 1:2 to 1:10 1:1 to 1:3

Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation
Acceptable Blood Gas Values :
pH 7.25 – 7.45PaO2 50 – 80 torrPaCO2 35 – 50 torr
With more maturity even higher PaCO2 are tolerated as long as pH is maintained above 7.25

Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation
Weaning Strategy :
1. First decrease pressure <182. FIO2 <0.403.Rate <154. CPAP of 3 to 4 to overcome ET resistance
Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation
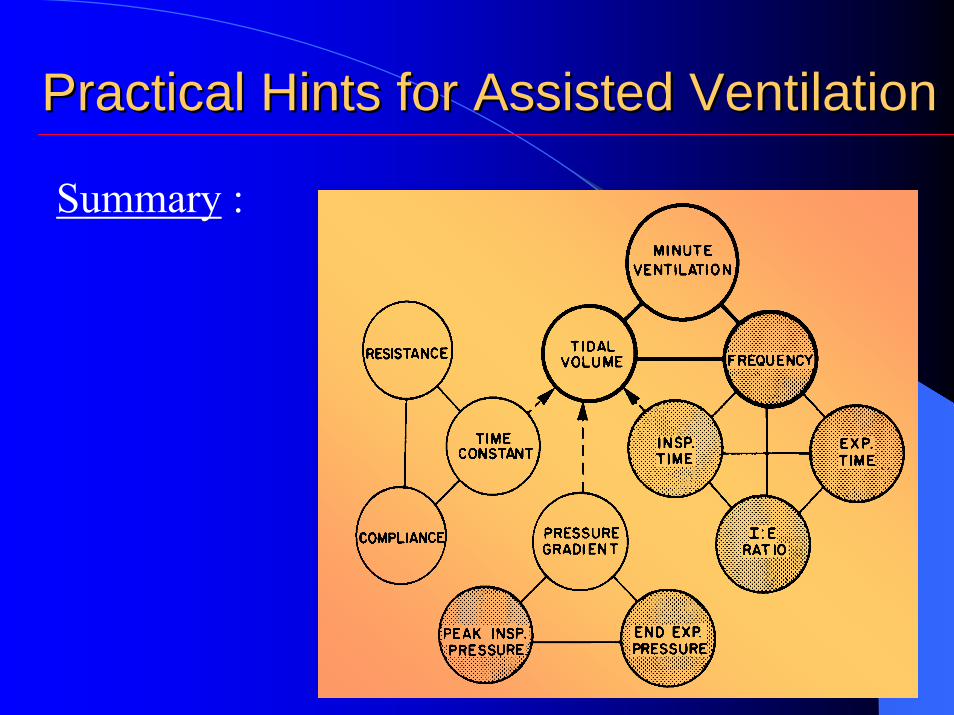
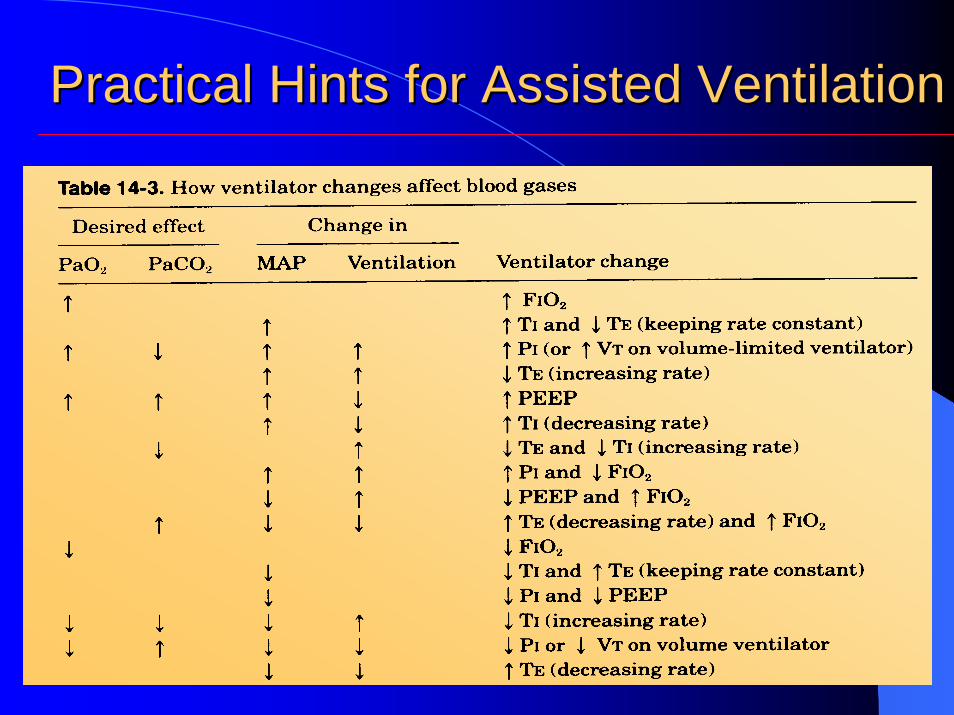
Summary :
Practical Hints for Assisted VentilationPractical Hints for Assisted Ventilation

Lung DevelopmentLung DevelopmentSignificant Milestones :
1. At 3-4 wks. Lung bud from esophagus.2. At 15-16 wks. Segmentation of bronchi complete.3.At 23-25 wks. Type II pneumatocyte develops.4.At 24 wks. Onwards surfactant production.5.At 34 wks onwards PG production.
Note : Lung maturity lags behind by 2-4 wks in maternal diabetes.

Composition of SurfactantComposition of Surfactant

Role of L/S Ratio and PGRole of L/S Ratio and PG