Navigating the 2017 MIPS Roadmap - Nephrology...
5
Navigating the 2017 MIPS Roadmap FALCON PHYSICIAN DISCLAIMER: This material is provided for informaonal purposes only and should not be regarded as legal or compliance advice. If legal advice or other expert assistance is required, the services of a competent professional person should be sought.
Transcript of Navigating the 2017 MIPS Roadmap - Nephrology...

Navigating the 2017 MIPS RoadmapFALCON PHYSICIAN
DISCLAIMER: This material is provided for informational purposes only and should not be regarded as legal or compliance advice. If legal advice or other expert assistance is required, the services of a competent professional person should be sought.
SubmitSome Data
Submit Partial Year
Submit Full yr.
0
+%
+%
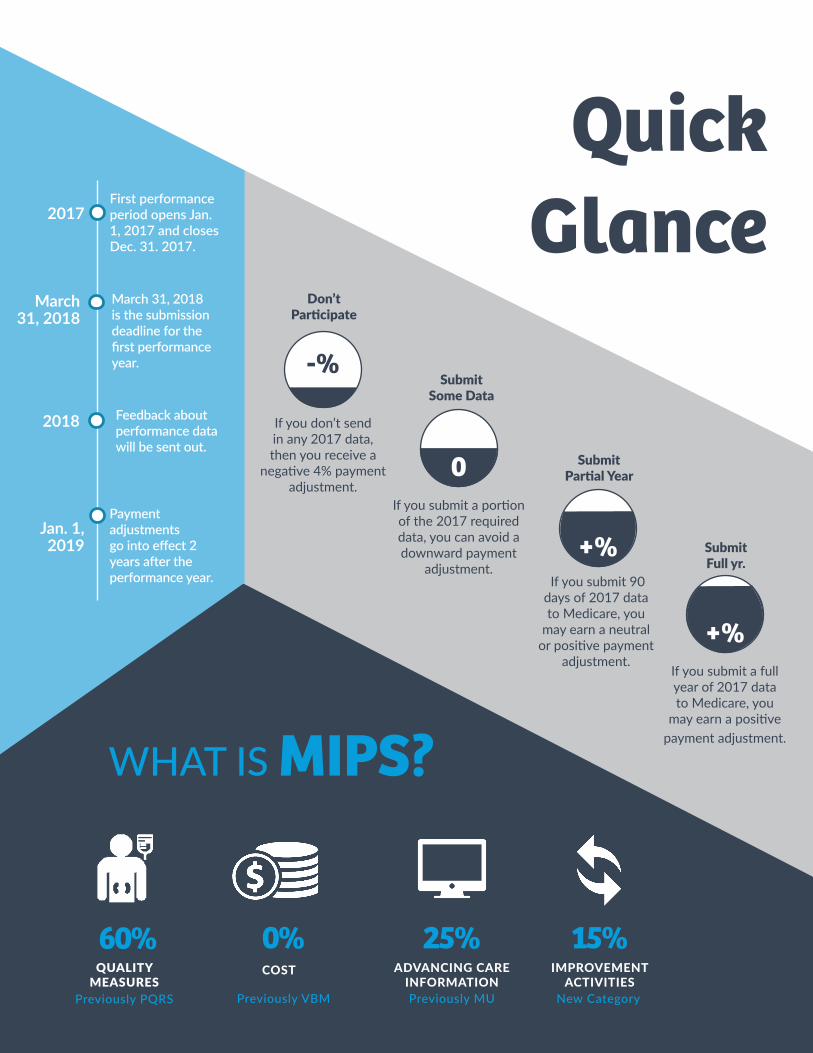
Don’t Participate
-%
If you don’t send in any 2017 data, then you receive a
negative 4% payment adjustment.
If you submit a portion of the 2017 required data, you can avoid a downward payment
adjustment. If you submit 90
days of 2017 data to Medicare, you
may earn a neutral or positive payment
adjustment.If you submit a full year of 2017 data to Medicare, you
may earn a positive payment adjustment.
WHAT IS MIPS?
60%COST IMPROVEMENT
ACTIVITIESADVANCING CARE
INFORMATION
0% 15%25%QUALITY
MEASURESPreviously PQRS Previously VBM Previously MU New Category
Quick Glance2017
2018
First performance period opens Jan. 1, 2017 and closes Dec. 31. 2017.
March 31, 2018 is the submission deadline for the first performance year.
Feedback about performance data will be sent out.
Payment adjustments go into effect 2 years after the performance year.
March 31, 2018
Jan. 1, 2019

1 2 3
QualityThe Quality Performance Category is very similar to the legacy
Physician Quality Reporting System (PQRS). In 2017, the Quality category is worth 60% of the Merit-based Incentive
Payment System (MIPS) Composite Score and requires the submission of quality measure information to CMS.
Test Option – report 1 Quality Measure to avoid the MIPS downward adjustment
Partial or Full Option – report data from a 90 day period or a full year
• Report at least 6 Quality Measures
• Include at least one Outcome measure, and if no Outcome measure is applicable, report at least 1 High Priority measure
• Select additional measures to report
- Bonus points awarded for selecting Outcome or High Priority measures- 6 highest scoring measures will be used to calculate your score
• Your 2017 reporting period must be at least 90 consecutive days between Jan. 1, 2017 and Dec. 31, 2017
• October 2, 2017 is the deadline to begin collecting data for a 90-day reporting period
• Clinicians receive 3 to 10 points for each quality measure based on performance against benchmarks
• If a measure cannot be reliably scored against a benchmark, only 3 points will be awarded
• If a measure can be reliably scored against a benchmark 3 to 10 points will be awarded
Reliable scores means: • Benchmarks exist• Sufficient case volume (>=20 cases
for most measures; >=200 cases for readmissions)
• Data completeness is met (at least 50 % of possible data is submitted)
Benchmarks:• There are separate benchmarks for
the quality measures based on the data submission method
• All reporters, individuals and groups, regardless of specialty or practice size are combined into one benchmark
• If no benchmark exists then only 3 points will be awarded
DETERMINE YOUR LEVEL OF PARTICIPATION & SELECT WHICH MEASURES TO SUBMIT
DETERMINE REPORTING PERIOD AND RECORD QUALITY MEASURE DATA REVIEW DATA
60%
Reporting Quality
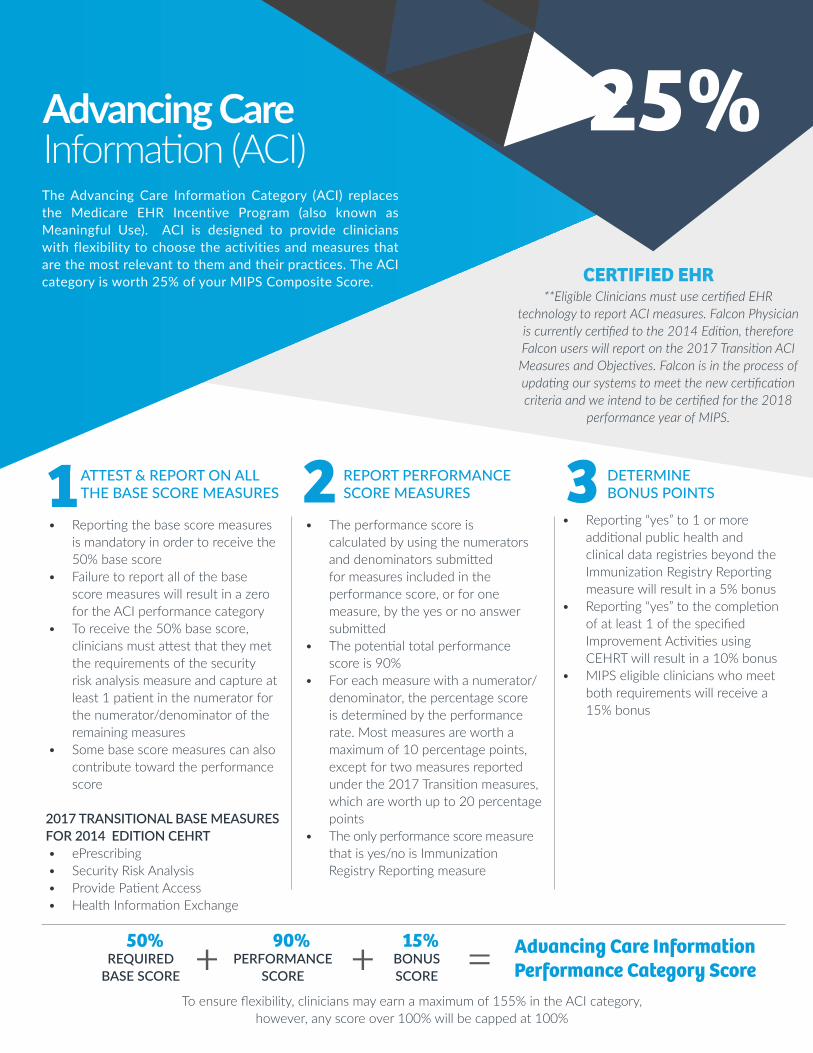
2 3• Reporting the base score measures
is mandatory in order to receive the 50% base score
• Failure to report all of the base score measures will result in a zero for the ACI performance category
• To receive the 50% base score, clinicians must attest that they met the requirements of the security risk analysis measure and capture at least 1 patient in the numerator for the numerator/denominator of the remaining measures
• Some base score measures can also contribute toward the performance score
2017 TRANSITIONAL BASE MEASURES FOR 2014 EDITION CEHRT• ePrescribing• Security Risk Analysis• Provide Patient Access• Health Information Exchange
• The performance score is calculated by using the numerators and denominators submitted for measures included in the performance score, or for one measure, by the yes or no answer submitted
• The potential total performance score is 90%
• For each measure with a numerator/denominator, the percentage score is determined by the performance rate. Most measures are worth a maximum of 10 percentage points, except for two measures reported under the 2017 Transition measures, which are worth up to 20 percentage points
• The only performance score measure that is yes/no is Immunization Registry Reporting measure
• Reporting “yes” to 1 or more additional public health and clinical data registries beyond the Immunization Registry Reporting measure will result in a 5% bonus
• Reporting “yes” to the completion of at least 1 of the specified Improvement Activities using CEHRT will result in a 10% bonus
• MIPS eligible clinicians who meet both requirements will receive a 15% bonus
ATTEST & REPORT ON ALL THE BASE SCORE MEASURES
REPORT PERFORMANCE SCORE MEASURES
DETERMINE BONUS POINTS1
50%REQUIRED
BASE SCORE
90%PERFORMANCE
SCORE
15%BONUS SCORE
+ + = Advancing Care Information Performance Category Score
Advancing Care Information (ACI)The Advancing Care Information Category (ACI) replaces the Medicare EHR Incentive Program (also known as Meaningful Use). ACI is designed to provide clinicians with flexibility to choose the activities and measures that are the most relevant to them and their practices. The ACI category is worth 25% of your MIPS Composite Score.
25%
CERTIFIED EHR
To ensure flexibility, clinicians may earn a maximum of 155% in the ACI category, however, any score over 100% will be capped at 100%
**Eligible Clinicians must use certified EHR technology to report ACI measures. Falcon Physician is currently certified to the 2014 Edition, therefore Falcon users will report on the 2017 Transition ACI Measures and Objectives. Falcon is in the process of updating our systems to meet the new certification criteria and we intend to be certified for the 2018
performance year of MIPS.

2 3Groups with 15 or fewer clinicians, non-patient facing clinicians and/or clinicians located in a rural area or HPSA
• Each activity is weighted either medium or high. To achieve the maximum 40 points for the Improvement Activity score, you may select either of these combinations:
• 1 high-weighted activity• 2 medium-weighted activities
• High-weighted activities are worth 40 points
• Medium-weighted activities are work 20 points
Groups with more than 15 clinicians• Each activity is weighted either
medium or high. To get the maximum score of 40 points for the Improvement Activity score, you may select any of these combinations:
• 2 high-weighted activities• 1 high-weighted activity and 2
medium-weighted activities• Up to 4 medium-weighted
activities• High-weighted activities are worth
20 points• Medium-weighted activities are
worth 10 points
Select from a list of 90+ activities listed on the Quality Payment Program website
For each activity that meets the 90-day requirement (activities that you performed for at least 90 consecutive days during the 2017 performance period) attest that you met the measure by indicating “yes”
UNDERSTAND SCORE CHOOSE ACTIVITIES ATTEST TO ACTIVITIES1
Improvement ActivitiesThe Improvement Activities Performance Category is
new for 2017, and assesses how much you participate in activities that improve clinical practice. Examples include
ongoing care coordination, patient safety practices, and expanding practice access. The Improvement Activities
Performance Category is worth 15% of the MIPS Composite Score in 2017.
15%