Multi-vessel Disease Patient with Coronary Artery Disease...
39
V. Voudris MD PhD FESC FACC Director 2nd Interventional Cardiology Division Chairman Cardiology Department Onassis Cardiac Surgery Center Multi-vessel Disease Patient with Coronary Artery Disease: Is There any Difference in Treatment After SYNTAX Study
Transcript of Multi-vessel Disease Patient with Coronary Artery Disease...

V. Voudris MD PhD FESC FACCDirector 2nd InterventionalCardiology DivisionChairman Cardiology DepartmentOnassis Cardiac Surgery Center
Multi-vessel Disease Patient with Coronary ArteryDisease: Is There any Difference in Treatment After
SYNTAX Study

Conflict of Interest
Advisory Board : Medtronic

© Cordis Corporation 2007© Cordis Corporation 2007 3
770,000810,000
850,000920,000
980,0001,030,000
1,092,0001,037,000
305,000 289,000296,000299,500395,000
485,000
542,000
514,000
200,000
500,000
800,000
1,100,000
PCI Vs CABG: New Vs Old Technology
Sources: Cordis Database, Morgan Stanley
2000 2001 2002 2004 2005 2006 20072003
Angioplasty
Bypass Surgery


The Patient with LM / 3 VD CAD
Interventionalist
Surgeon
Patient
Interventionalist

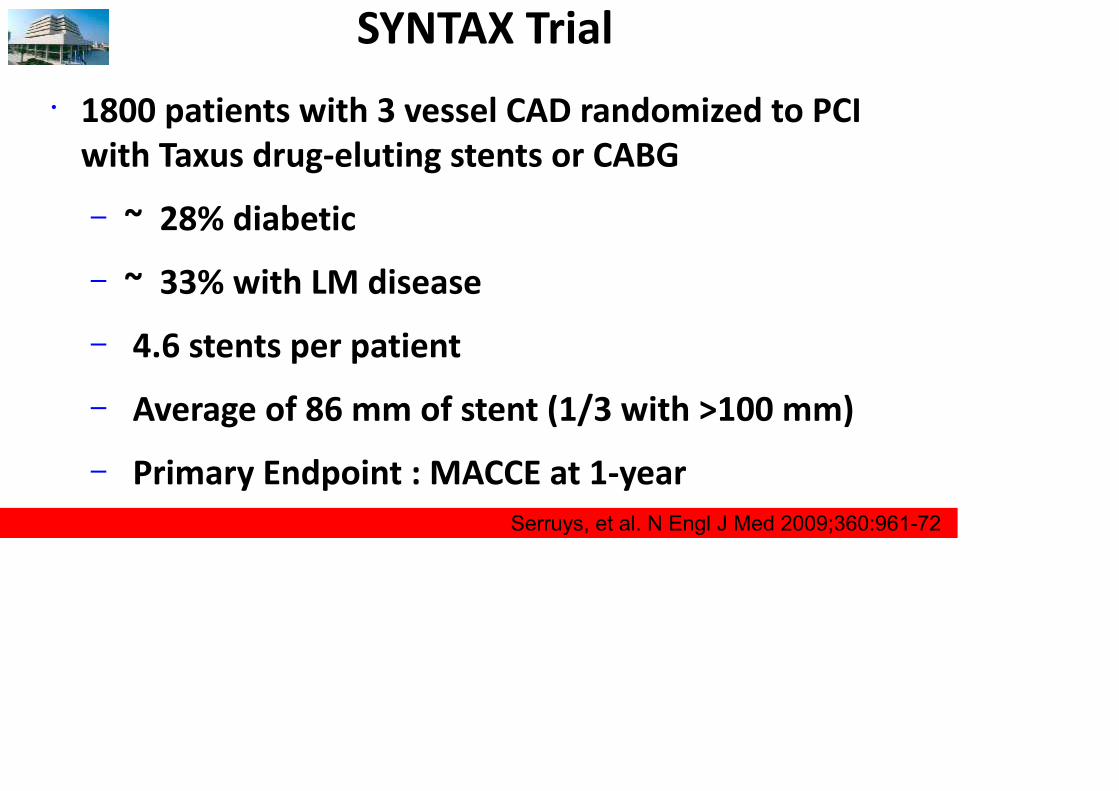
SYNTAX Trial• 1800 patients with 3 vessel CAD randomized to PCI
with Taxus drug-eluting stents or CABG– ~ 28% diabetic– ~ 33% with LM disease– 4.6 stents per patient– Average of 86 mm of stent (1/3 with >100 mm)– Primary Endpoint : MACCE at 1-year
• Yearly F/U thereafter (up to 5 years)Serruys, et al. N Engl J Med 2009;360:961-72

SYNTAX Trial - 5 Year
Mohr, et al. Lancet 2013;381:629-38
All Cause Mortality
Stroke

SYNTAX -
Mohr, et al. Lancet 2013;381:629-38
5 Year Rates of Death, Stroke, or MI

SYNTAX - 5 Year MACCE
Mohr, et al. Lancet 2013;381:629-38

SJ Head et al. European Heart Journal (2014) 35, 2821–2830
CABG vs. PCI for patients with 3 vessel disease:5 - year FU of the SYNTAX trial

SJ Head et al. European Heart Journal (2014) 35, 2821–2830
CABG vs. PCI for patients with 3 vessel disease:5 - year FU of the SYNTAX trial

SJ Head et al. European Heart Journal (2014) 35, 2821–2830
SYNTAXTrial :5 YearsResults
3 VesselDiseasePatients

Syntax Trial – 3 Vessel Disease PatientsThe 5-year analysis of patients with 3VD randomized in theSYNTAX trial demonstrated that treatment with PCI resulted insignificantly higher rates of MACCE, which were driven notonly by increased rates of repeat revascularization but also bysignificantly higher all-cause death and MI
Stroke rates were comparable between CABG and PCI
Treatment with PCI was found to be an independent predictor,not only of 5-year MACCE but also of all-cause death andcomposite safety endpoint of death/stroke/MI

SJ Head et al. European Heart Journal (2014) 35, 2821–2830
CABG vs. PCI for patients with 3 vessel disease:5 - year FU of the SYNTAX trial

Syntax Trial – IncompleteRevascularizationIncomplete revascularization occurs more frequently in
patients with chronic total occlusions undergoing PCIresulting in large areas of non-revascularized/ischaemic
myocardium that could potentially increase the risk ofdeath during follow-up
Incomplete revascularization in CABG usually encompassessmall vessels with less ischaemic myocardium at riskdiffusely diseased vessels which are often well
collateralized

Five-year incidence of cardiac events in left maincoronary artery (LM) patients
MC Morice et al. Circulation. 2014;129:2388-2394
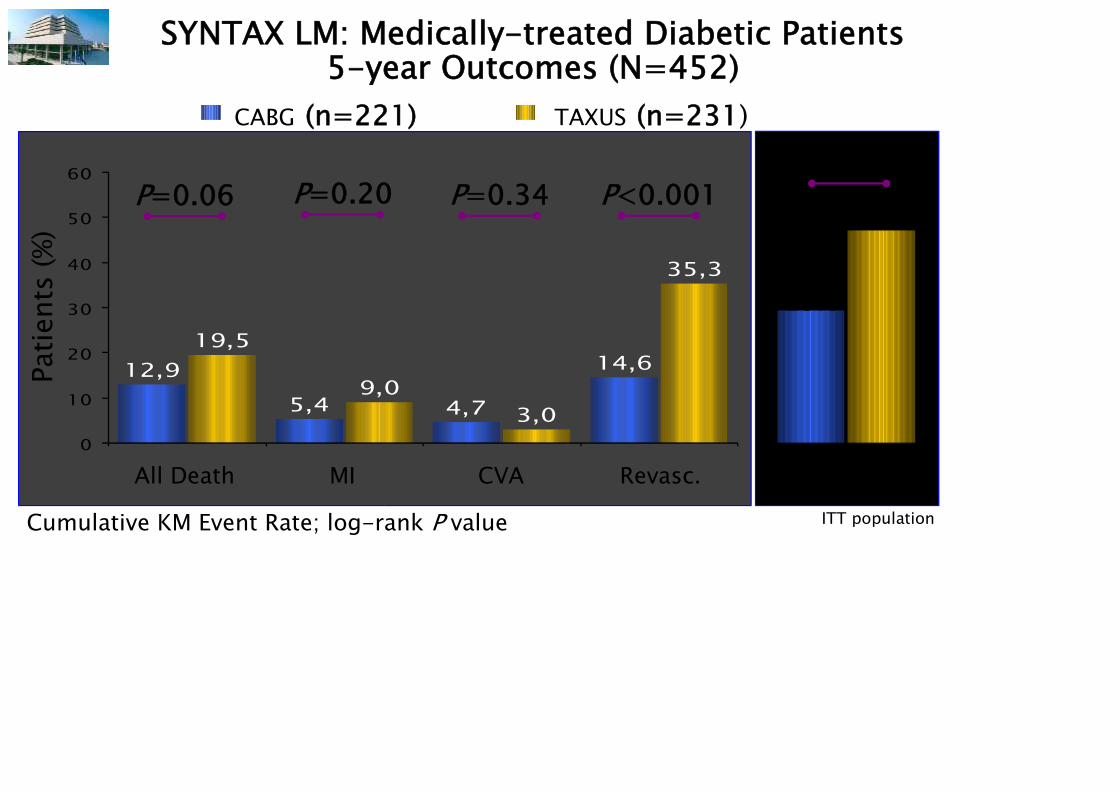
SYNTAX LM: Medically-treated Diabetic Patients5-year Outcomes (N=452)
12,95,4 4,7
14,619,5
9,03,0
35,3
0
10
20
30
40
50
60
TAXUS (n=231)CABG (n=221)
All Death MI CVA Revasc.
P=0.06
Patie
nts
(%)
P=0.20 P=0.34 P<0.001P<0.001
29.0
46.5
MACCEITT populationCumulative KM Event Rate; log-rank P value

Site-reported data
Heterogeneity in the Left Main Group

0102030405060
P=0.12 P=0.30 P=0.67 P=0.24 P=0.04
MACCE to 5 Years Left Main SubsetsPa
tient
s (%
)
TAXUSCABG

Dominance
SYNTAXscore
Diseased
Segment
#
Tota
lOc
clusio
n
Trifurcation
Bifurcation
Aorta OstialSevere
Tortuosity
Leng
thHeavy
Calcific
atio
nThrombus
DiffuseSmall
WWW.SYNTAXSCORE.COM

SYNTAX Score - 5 Year MACCELowest SYNTAX Tertile (0-22)
All Patients
Mohr, et al. Lancet 2013;381:629-38
All Patients
Middle SYNTAX Tertile (23-32)
All Patients
Highest SYNTAX Tertile (33+)

Five-year Incidence of Cardiac Events in Left Main(LM) Coronary Artery Patients
MC Morice et al. Circulation. 2014;129:2388-2394

HIGHER SYNTAX SCOREFAVOURS CABG
LOWER SYNTAX SCOREFAVOURS PCI
PCI
CABG

SYNTAX: Definite/Probable ARC Stent Thrombosis to 5 Years (Per Patient)
0
6
12
(3/896) (23/893) (15/874) (11/850) (12/830)
Days Post-procedure
Acute≤1 d
Subacute2-30 d
Late31-365 d
Very Late(10/803) (7/768)
366-730 d
731-1095 d
1096-1460 d
1461-1825 d
0.3
2.61.7 1.3 1.4 1.2 0.9
~3% ST rate within 30 days, and then~1-2%/yr thereafter
Serruys PW. TCT2012

SYNTAX: Short- and Long-term Clinical Impact of StentThrombosis and Graft Occlusion at 5 Years
Conclusion: Rates of stent thrombosis, graft occlusion at 5 years aresimilar, but stent thrombosis has greater effect on mortality
Analysis of patients with left main or 3-vessel disease undergoing PCI with Taxus(n = 871) or CABG (n = 805), using per protocol and ARC or ARC-like definitions
5-Year Follow-upARC Definite Stent
Thrombosis(n = 47)
ARC-like DefiniteGraft Occlusion
(n = 32)P Value
0-30 Days 3.0% 1.0% 0.03
31 Days-5 Years 4.2% 4.5% 0.68
Cardiac mortality was 35.4% in patients with stent thrombosis comparedwith 0% in patients with graft occlusion
Farooq V, et al. J Am Coll Cardiol.2013

• Higher initial cost of PCI vs CABG (due to the cost of stents, repeatrevascularization, medications) narrowed over 5 years
• Projected beyond 5 years, CABG provides gains in both life expectancyand quality-adjusted life-years, meeting the threshold for society’swillingness to pay
• In subgroup analyses, PCI was cost-effective for patients with a lowSYNTAX score (≤ 22) or left main disease
Five-year data from SYNTAX (n = 1,800) used to extrapolate costs, lifeexpectancy, and quality-adjusted life expectancy over a lifetime
Cost-Effectiveness of PCI with DES vs Bypass Surgeryfor Patients with 3-Vessel or Left Main CAD
Implications: For most patients with 3-vessel or left main disease, CABGis preferred for both clinical and economic reasons, but PCI is cost-effective for less complex anatomy
Cohen DJ, et al. Circulation. 2014;Epub ahead of print.

Syntax Trial MessagesThe treatment effect of PCI vs. CABG differed significantlybetween patients with LM and 3 vessel disease
left main PCI has become more common since theresults from the SYNTAX trial established similarsafety and efficacy in comparison with CABG
for multivessel disease this study for the first timeprovides robust evidence that CABG is superior to PCIusing first-generation DES in reducing long-term hardclinical endpoints of death and MI

Syntax Trial MessagesCABG should remain the standard of care for patientswith complex lesions (high or intermediate SYNTAX scores)
For patients with less complex disease (low SYNTAX scores)or left main coronary disease (low or intermediate SYNTAXscores), PCI is an acceptable alternative
All patients with complex multivessel coronary arterydisease should be reviewed and discussed by botha cardiac surgeon and interventional cardiologist to reachconsensus on optimum treatment

Implementation of the SYNTAX results in recent ESCguidelines on myocardial revascularization
.
European Heart Journal (2014) 35, 2541-2619

Limitations of the Syntax Trial
The non-inferiority end point of 12-monthMACCEs was not met in the overall population
Thus, the analysis of LM or 3 vessel diseasepatients should be considered observationaland hypothesis generating
• The conventional SYNTAX Score is advocated inthe US & European revascularisation guidelinesas a tool to aid the Heart Team
• These guidelines also state that clinical variablesshould be taken into account
• Recent attempts have been made to merge theSYNTAX Score with cardiac based surgical riskscores to overcome this limitation
Limitations of the SYNTAX Score

SYNTAX Score IIDesigned to Objectively to Balance Patient Risk To Guide
Decision Making Between CABG and PCI
25
Tables
Table 1
Title: Development (SYNTAX Trial) (a) and validation (DELTA Registry) (b) data
for the SYNTAX Score II.
Legend: Hazard ratios (HR) in a multivariable Cox Proportional Hazards Model for
the SYNTAX Score II are shown for the CABG and PCI arms, followed by the
interaction effects (HRPCI/HRCABG) in influencing long term mortality between CABG
and PCI.
CABG 4-Year DeathMultivariable adjustedHR and 95% CI
PCI 4-Year DeathMultivariable adjustedHR and 95% CI
Interaction EffectHRPCI/HRCABG
(95% CI and p-value)a) Development PopulationSYNTAX Trial (n=1800)SYNTAX Score (per 10 point increase)Age (per 10 year increase)Creatinine Clearance† (per 10 ml/min increase)LV Ejection Fraction (per 10% increase)Peripheral Vascular Disease†ULMCA DiseaseFemaleCOPD
0.97 (0.79, 1.18)1.88 (1.34, 2.64)0.91 (0.77, 1.07)0.84 (0.61, 1.16)2.79 (1.66, 4.71)1.47 (0.93, 2.34)0.59 (0.32, 1.10)2.84 (1.64, 4.90)
1.27 (1.08, 1.50)1.29 (0.97, 1.71)0.82 (0.72, 0.93)0.56 (0.43, 0.73)2.79 (1.72, 4.53)0.82 (0.54, 1.23)1.70 (1.11, 2.60)1.35 (0.74, 2.47)
1.32 (1.01, 1.71; p=0.039)0.69 (0.44, 1.07; p=0.095)0.89 (0.73, 1.10; p=0.30)0.67 (0.44, 1.00; p=0.053)1.00 (0.49, 2.04; p=1.00)0.56 (0.30, 1.03; p=0.062)2.87 (1.35, 6.07; p=0.0059)0.48 (0.21, 1.08; p=0.074)
b) External Validation PopulationDELTA Registry (n=2891)SYNTAX Score (per 10 point increase)Age (per 10 year increase)Creatinine Clearance (per 10 ml/min increase)LV Ejection Fraction (per 10% increase)Peripheral Vascular Disease*ULMCA DiseaseFemaleCOPD*
1.12 (0.95, 1.32)1.46 (1.15, 1.85)0.91 (0.78, 1.06)0.59 (0.47, 0.75)1.37 (0.68, 2.79)
-0.52 (0.31, 0.87)
3.63 (1.31, 10.04)
1.32 (1.20, 1.46)1.34 (1.19, 1.52)0.93 (0.86, 1.00)0.57 (0.50, 0.65)1.77 (1.01, 3.09)
-1.09 (0.82, 1.46)1.97 (0.88, 4.42)
1.18 (0.98, 1.42; p=0.083)0.92 (0.70, 1.21; p=0.56)1.02 (0.86, 1.21; p=0.82)0.96 (0.72, 1.27; p=0.75)1.29 (0.51, 3.22; p=0.59)
-2.09 (1.16, 3.76; p=0.014)0.54 (0.20, 1.47; p=0.23)
† Retained in SYNTAX Score II to improve the predictive accuracy of 4-year mortality in the CABG
and PCI arms (weak [CrCl] or negligible [PVD] interaction effects between CABG and PCI for 4-year
mortality)
* Data reported by the study sites in 1363/2891 (47.1%) patients for PVD and 1061/2891 (36.7%)
patients for COPD.
Abbreviations: CABG coronary artery bypass graft, PCI percutaneous coronary intervention, HR
hazard ratio, SD standard deviation, ULMCA unprotected left main coronary artery, LV left
ventricular, COPD chronic obstructive pulmonary disease

Age
HIGHER AGEFAVOURS PCI
YOUNGER AGE FAVOURSCABG
PCI
CABG
SYNTAX Score II Left VentricularEjection Fraction
LOWER LVEFFAVOURS CABG
HIGHER LVEFFAVOURS PCI
CABG
PCI

COPDFAVOURS PCI
PCI
CABG
SYNTAX Score IICOPD
ULMCA DISEASEFAVOURS PCI
PCI
CABG
Unprotected LMCAD

Female Gender
FEMALE GENDERFAVOURS CABG
PCI
CABG
Findings recently shown (In Press) on multivariable analyses of theSYNTAX Trial, demonstrating female gender to be an independentcorrelate of long term mortality after PCI

Syntax Trial Limitations – FuturePerspectives
Newer-generation DES have been developed since theuse of the paclitaxel-eluting stent in the SYNTAX trial andhave replaced the latter in current clinical practice dueto significant reductions in MI, ST, and repeat revascularization
We are waiting the EXCEL trial, which evaluates theperformance of the everolimus eluting stent vs.revascularization surgery in patients with lesions of leftmain coronary artery

“In your case, Dave, there’s a choice: elective surgery,outpatient medical therapy, or whatever’sin the box that our lovely Carol is holding.”

Thank You
CABG
PCI
LM and 1 or 2 VD and 3 VDwith Low Syntax Score
patients
CABG
PCI
LM and 3 VD with highSyntax Score patients