MPNP Handbook 2011
34
Sponsored as a service to the medical profession by Pfizer. Editorial development by UBM Medica. The opinions expressed in this publication are not necessarily those of the publisher or sponsor. Any liability or obligation for loss or damage howsoever arising is hereby disclaimed. © 2011 UBM Medica. All rights reserved. No part of this publication may be reproduced by any process in any language without the written permission of the publisher. A Summary of Recommendations Issued by the Multidisciplinary Panel on Neuropathic Pain (MPNP) www.neuropainhk.org UBM Medica 27th Floor, OTB Building 160 Gloucester Road, Wan Chai, Hong Kong Tel: (852) 2559 5888 Fax: (852) 2559 6910 E-mail: [email protected] http://www.ubmmedica.com Handbook of Neuropathic Pain Management Guidelines 2nd Edition Endorsed by 2nd Edition
-
Upload
made-supadma -
Category
Documents
-
view
56 -
download
3
Transcript of MPNP Handbook 2011
Sponsored as a service to the medical profession by Pfizer. Editorial development by UBM Medica. The opinions expressed in
this publication are not necessarily those of the publisher or sponsor. Any liability or obligation for loss or damage howsoever arising is hereby disclaimed.
© 2011 UBM Medica. All rights reserved.No part of this publication may be reproduced by any process in any language
without the written permission of the publisher.
A Summary of Recommendations Issued by the Multidisciplinary Panel on Neuropathic Pain (MPNP)
www.neuropainhk.org
UBM Medica 27th Floor, OTB Building160 Gloucester Road, Wan Chai, Hong KongTel: (852) 2559 5888 Fax: (852) 2559 6910E-mail: [email protected] http://www.ubmmedica.com
Handbook of Neuropathic Pain M
anagement Guidelines 2nd Edition
Endorsed by
2nd Edition

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 1
Introduction to neuropathic pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Introduction to the Multidisciplinary Panel on Neuropathic Pain (MPNP) . . . . . . . . . . . . . 4
MPNP members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Overview of contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Diagnosis and assessment of pain severity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Drugs used in the treatment of neuropathic pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Drug options and dosages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Side effect profiles and management tips . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Recommendations for postherpetic neuralgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Recommendations for idiopathic trigeminal neuralgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Recommendations for painful diabetic peripheral neuropathy . . . . . . . . . . . . . . . . . . . . . . . . 18
Recommendations for neuropathic pain associated with peripheral nerve entrapment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Recommendations for central post-stroke pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Recommendations for neuropathic cancer pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Recommendations for neuropathic pain due to spinal cord pathologies . . . . . . . . . . . . . . . . . 26
Recommendations for complex regional pain syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Table of Contents

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition2
Introduction to neuropathic pain
Neuropathic pain covers a diverse group of pain conditions characterized by a primary lesion or dysfunction of the sensory nervous system. It is particularly challenging for clinicians to manage because of its chronicity and severity, poor responsiveness to
traditional pain therapies, and wide individual variations in pain responsiveness.1,2 Unfortu-nately, neuropathic pain conditions are likely to increase as populations age and age-related disorders, such as herpes zoster, diabetes mellitus, cerebrovascular accidents, Parkinson’s disease and cancer, rise in prevalence.3 Medical treatment of neuropathic pain remains unsatisfactory for a substantial proportion of patients, and with the rising rates of disorders known to incite neuropathic pain syndromes, it is vital to improve patient outcomes with existing treatment options and continue to pursue new therapeutic strategies.
What is the difference between neuropathic pain and nociceptive pain?There are two types of pain: nociceptive pain and neuropathic pain. Nociceptive pain serves as a warning of ongoing tissue damage due to injury or disease (eg, a wound, thermal insult or inflammation).3 It comprises somatic pain (in skin, muscles, joints, bone) and visceral pain (in an organ or its covering), and is an acute, self-limiting symptom.
In contrast, neuropathic pain is initiated by injury or dysfunction of the peripheral or central nervous system, resulting in a delayed chronic response to damage that is no longer acute, but which continues to evoke pain.3
What causes neuropathic pain?This disorder can be caused by injury to neuronal cell bodies in the peripheral or cen-tral nervous system via compression, transection, infiltration, ischaemia or metabolic injury, or any combination of these effects. Examples of peripheral neuropathic pain conditions include diabetic peripheral neuropathy, postherpetic neuralgia, tumour infiltration neuropa-thy, phantom limb pain, complex regional pain syndrome and trigeminal neuralgia. Central neuropathic pain conditions include multiple sclerosis, spinal cord injury, central post-stroke pain and Parkinson’s disease.
Although the underlying neuronal mechanisms of neuropathic pain are not completely understood, various distinct pathophysiological mechanisms appear to be involved, resulting in both peripheral and central sensitization.4 Nerve lesions can trigger molecular changes in nociceptive neurons, making them abnormally sensitive and evoking pathological spontaneous activity. Inflammation in the damaged nerve trunk can induce ectopic no-ciceptor activity, causing spontaneous pain. This hyperactivity in nociceptors can induce
Neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 3
secondary changes in processing neurons in the spinal cord and brain, so that input from mechanoreceptive A fibres is perceived as pain. In addition, neuroplastic changes in the central pain modulatory systems can lead to further hyperexcitability.4
What are the symptoms of neuropathic pain?Neuropathic pain is commonly described as burning, electric, tingling and shooting in nature. The pain may be continuous or paroxysmal in presentation. Other common symptoms include3:• Allodynia – Pain due to nonnoxious stimuli (clothing, light touch) when applied to the
affected area. May be mechanical, dynamic or thermal• Anaesthesia – Loss of normal sensation to the affected region• Dysaesthesia – Spontaneous or evoked unpleasant abnormal sensations• Hyperalgesia – Exaggerated response to a mildly noxious stimulus applied to the af-
fected region• Hyperpathia – Delayed and explosive response to a noxious stimulus applied to the
affected region• Hypoaesthesia – Reduction of normal sensation to the affected region• Paraesthesias – Nonpainful spontaneous abnormal sensations• Phantom pain – Pain from a specific site that no longer exists (eg, amputated limb) or
where there is no current injury• Referred pain – Occurs in a region remote from the source
How to assess a patient for neuropathic pain Neuropathic pain should be suspected in patients who present with pain that they describe in any of the following terms: burning, searing or scalding, cold, numbness, tingling, shoot-ing, electric shock-like, stabbing, crushing, or vise-like.
Clinical evaluation should include a history to assess pain intensity, sensory descriptions of the pain quality, temporal variations in pain intensity and functional impact. A physical examination of gross motor function, deep tendon reflexes, and the somatosensory system should be performed. The sensory examination should include assessment of responses to touch, pinprick, pressure, cold, heat, vibration and temporal summation in the area of maximal pain.2
Patient-completed neuropathic pain screening tools can assist primary care physicians in differentiating between nociceptive and neuropathic pain. Examples of screening tools include ID Pain and painDETECT.
Neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition4
Introduction to the Multidisciplinary Panel on Neuropathic Pain (MPNP)
The Multidisciplinary Panel on Neuropathic Pain (MPNP) comprises local thought lead-ers dedicated to improving the awareness and understanding of neuropathic pain in Hong Kong. The panel includes specialists from a range of disciplines involved in
treating neuropathic pain: neurology, neurosurgery, geriatric medicine, anaesthesiology and orthopaedics. For some time, Hong Kong physicians lacked local guidelines for managing neuropathic pain, and were potentially unaware of the most appropriate referral pathways and treat-ments. Therefore, the MPNP has endeavoured to improve the understanding and general awareness of neuropathic pain syndromes, and to contribute to better diagnosis, manage-ment and treatment of these conditions in Hong Kong. It aims to act as an information source for medical professionals on the treatment and management of neuropathic pain and provide evidence-based resources on neuropathic pain.
The
MPN
P

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 5
MPNP members
Dr Phoon Ping ChenMBBS, FHKAM(Ana), FANZCA, FFPMANZCA, DipPainMgt(HKCA), MHAConsultant and Chief of Service, Department of Anaesthesiology and Operating Services, Alice Ho Miu Ling Nethersole Hospital and North District Hospital, and Adjunct Associate Professor, The Chinese University of Hong Kong, Hong Kong SAR
Dr Josephine WY IP MBBS, MS, FRCS(Edin), FHKAM(Ortho), DipHandSurg (FESSH)Associate Professor and Chief, Division of Hand and Foot Surgery, Department of Orthopaedic Surgery, The University of Hong Kong, Queen Mary Hospital, Hong Kong SAR
Dr Joseph MK LaM MBChB, FRCS(Edin), FCSHK, FHKAM(Surg)Honorary Consultant and Honorary Clinical Associate Professor, Division of Neurosurgery, Department of Surgery, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong SAR
Dr Vincent MoK MBBS, FHKAM(Med), FRCP(Edin), MD(CUHK)Associate Professor and Honorary Associate Consultant, Division of Neurology, Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong SAR
Dr Tak hong TsoIMBBS, MRCP, FRCP(Edin), FRCP(Glas), FRCP(Lond), FHKCP,
FHKAM(Med)Neurologist and Consultant Physician, Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Hong Kong SAR
Dr Chun Por WongMBBS, FRCP(Lond), FRCP(Glas), FRCP(Edin), FHKAM(Med), FHKCPChief of Service, Integrated Medical Services, Consultant and Head, Department of Geriatrics, Ruttonjee and Tang Shiu Kin Hospitals, Hong Kong SAR
Dr steven ho shan WongMBBS, FHKAM(Ana), FANZCA, DipPainMgt(HKCA)Consultant Anaesthesiologist and Head of Pain Management Team, Department of Anaesthesiology and Operating Theatre Services, Queen Elizabeth Hospital, Hong Kong SAR
L-R (standing): Steven Ho Shan Wong,
Joseph MK LaM, Tak Hong TSoi and Vincent MoK;
L-R (seated): Chun Por Wong,
Josephine WY iP and Phoon Ping CHen
The
MPN
P
Dr Tsun Woon LeeMBBS, FANZCA, FFPMANZCA, FHKCA, FHKAM (Ana), DipPainMgtHospital Chief Executive, Pok Oi Hospital, Hong Kong SAR
Professor Lawrence Ks WongMBBS, MD, MRCP, FHKAM (Med), FRCPProfessor and Head, Division of Neurology, Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong SAR
Current members
Past members

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition6
Overview of contents
Since its inception in 2001, the MPNP has published recommendations on a variety of neuropathic pain conditions. This booklet summarizes these recommendations, which are endorsed by the Hong Kong Pain Society and are updated regularly.
Particular emphasis is paid to details of appropriate treatment options.
The contents include simple tools to assist in the diagnosis and evaluation of neuropathic pain, summary tables of dosage and administration details of many of the drugs used for neuropathic pain, and notes on the most common side effects associated with neuropathic pain medications. The largest section of the handbook is devoted to reproducing the treatment algorithms recommended by the MPNP for the management of neuropathic pain conditions.
The booklet is provided as a convenient summary of the medical management options in neuropathic pain conditions, and is not meant as a comprehensive guide to the complete multidisciplinary management of patients with these conditions. For full details, physicians are encouraged to consult the original versions of the MPNP recommendations, which are available on the MPNP Web site (www.neuropainhk.org). It is important to note that not all drugs mentioned are licensed for use in neuropathic pain conditions. Full prescribing infor-mation should always be consulted before initiating therapy.
It is hoped that this concise guide will assist Hong Kong physicians in their daily manage-ment of patients suffering from neuropathic pain conditions, thus ultimately helping to improve the quality of life of patients with these disabling conditions.
Over
view
DisclaimerEvery effort has been made to ensure that the information contained in this handbook is accurate at the time of publication. As new research and clinical experience broadens medical knowledge, the diagnosis and management of neuropathic pain will undoubtedly change. The MPNP cannot be held liable for any consequence arising from inappropriate application of the information provided in this handbook.

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 7
Diagnosis and assessment of pain severity
The following patient-completed screening questionnaire, called ID Pain, can assist primary care physicians in differentiating nociceptive from neuropathic pain, and facilitate earlier and more appropriate treatment. The Chinese version has recently
been validated. The two other items can help patients describe the extent and severity of pain, and can be used to monitor the effectiveness of therapy.
Screening Questionnaire5,6
Asse
ssm
ent o
f neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition8
Asse
ssm
ent o
f neu
ropa
thic
pai
n
Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 9
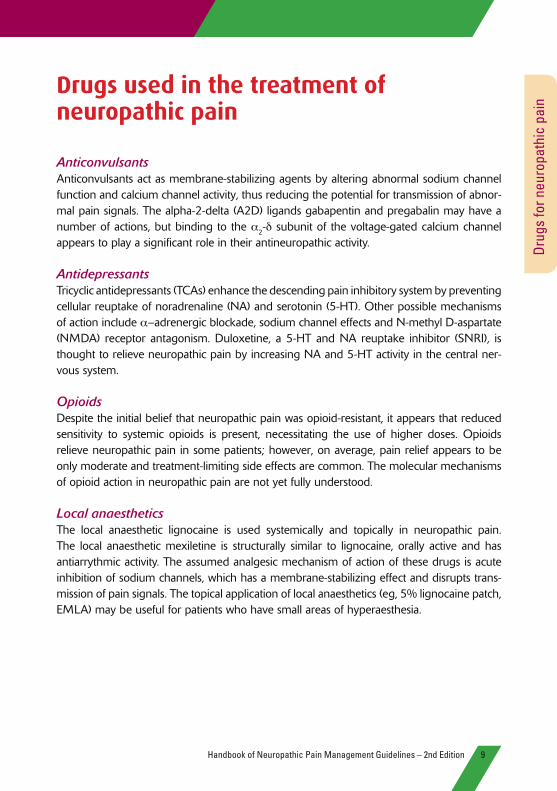
Drugs used in the treatment of neuropathic pain
AnticonvulsantsAnticonvulsants act as membrane-stabilizing agents by altering abnormal sodium channel function and calcium channel activity, thus reducing the potential for transmission of abnor-mal pain signals. The alpha-2-delta (A2D) ligands gabapentin and pregabalin may have a number of actions, but binding to the α2-d subunit of the voltage-gated calcium channel appears to play a significant role in their antineuropathic activity.
AntidepressantsTricyclic antidepressants (TCAs) enhance the descending pain inhibitory system by preventing cellular reuptake of noradrenaline (NA) and serotonin (5-HT). Other possible mechanisms of action include α–adrenergic blockade, sodium channel effects and N-methyl D-aspartate (NMDA) receptor antagonism. Duloxetine, a 5-HT and NA reuptake inhibitor (SNRI), is thought to relieve neuropathic pain by increasing NA and 5-HT activity in the central ner-vous system.
OpioidsDespite the initial belief that neuropathic pain was opioid-resistant, it appears that reduced sensitivity to systemic opioids is present, necessitating the use of higher doses. Opioids relieve neuropathic pain in some patients; however, on average, pain relief appears to be only moderate and treatment-limiting side effects are common. The molecular mechanisms of opioid action in neuropathic pain are not yet fully understood.
Local anaestheticsThe local anaesthetic lignocaine is used systemically and topically in neuropathic pain. The local anaesthetic mexiletine is structurally similar to lignocaine, orally active and has antiarrythmic activity. The assumed analgesic mechanism of action of these drugs is acute inhibition of sodium channels, which has a membrane-stabilizing effect and disrupts trans-mission of pain signals. The topical application of local anaesthetics (eg, 5% lignocaine patch, EMLA) may be useful for patients who have small areas of hyperaesthesia.
Drug
s fo
r neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition10
Drug options and dosagesThis table covers most of the first- and second-line drugs mentioned in the treatment al-gorithms included in this booklet, but does not represent an exhaustive list of treatment options. Full prescribing information should be consulted before initiating therapy.
Drug Recommended for starting dosage Dose titration (if necessary) Maximum dosage Duration of adequate trial
anticonvulsants
Pregabalin* PHN (1st line)DPN (1st line)TN (2nd line)
150 mg/day as 75 mg bid Increase to 300 mg daily after 3–7 days, then by 150 mg/d every 3–7 days as tolerated
600 mg daily (200 mg tid or 300 mg bid) 4 wks
Gabapentin* PHN (1st line)DPN (1st line)TN (2nd line)
300 mg at bedtime on Day 1; 300 mg bid on Day 2; 300 mg tid on Day 3
Increase by 300 mg tid every 1–7 days as tolerated
3,600 mg daily (1,200 mg tid) 3–8 wks for titration plus 2 wks at maximum tolerated dosage
Carbamazepine† TN (1st line)PHN (2nd line)
100 mg bid 100 mg every 3–7 days 1,600 mg/day 8-12 wks
Lamotrigine TN (2nd line) 25 mg/day for 2 weeks Increase to 50 mg/day for 2 wks, then increase by 50–100 mg every wk
200–400 mg/day 12 wks (including titration period)
antidepressants
Amitriptyline PHN (1st line)DPN (1st line)TN (2nd line)
10–25 mg daily at bedtime Increase by 10 to 25 mg weekly Up to 75 mg daily 3 months at maximum tolerated dosage
Nortriptyline, desipramine
PHN (1st line)DPN (1st line)TN (2nd line)
10–25 mg at bedtime Increase by 25 mg daily every 3–7 days as tolerated
150 mg daily 6–8 wks with at least 2 wks at maximum tolerated dosage
Duloxetine DPN (1st line) 60 mg/day – 60 mg/day –
opioids
Morphine, oxycodone, methadone, levorphanol
PHN (2nd line) 10–15 mg morphine q4h or as needed (equianalgesic dosages should be used for other opioid analgesics)
After 1–2 wks, convert total daily dosage to long-acting opioid analgesic and continue short-acting medication as needed
No maximum dosage with careful titration
4–6 wks
Tramadol DPN (2nd line) 50 mg daily or bid Increase by 50–100 mg daily in divided doses every 3–7 days as tolerated
400 mg daily (100 mg qid); 300 mg daily in patients >75 years
4 wks
Local anaesthetics
IV lignocaine 5 mg/kg over 30–60 min Titrated based on symptoms of cyclic antidepressant toxicity, eg, perioral numbness, slurring of speech, tinnitus, dizziness, diplopia, convulsions
–
Mexiletine 150 mg daily to 200 mg bid Increase by 50 mg every 2 to 3 days prn 1,200 mg/day –
5% lignocaine patch PHN (1st line) Apply patch for a maximum of 12 h
None needed 3 patches daily for no more than 12 h in 24 h
2–4 wks
EMLA® PHN (1st line) tid, under occlusive dressing if possible
– – –
Drug
s fo
r neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 11
Drug Recommended for starting dosage Dose titration (if necessary) Maximum dosage Duration of adequate trial
anticonvulsants
Pregabalin* PHN (1st line)DPN (1st line)TN (2nd line)
150 mg/day as 75 mg bid Increase to 300 mg daily after 3–7 days, then by 150 mg/d every 3–7 days as tolerated
600 mg daily (200 mg tid or 300 mg bid) 4 wks
Gabapentin* PHN (1st line)DPN (1st line)TN (2nd line)
300 mg at bedtime on Day 1; 300 mg bid on Day 2; 300 mg tid on Day 3
Increase by 300 mg tid every 1–7 days as tolerated
3,600 mg daily (1,200 mg tid) 3–8 wks for titration plus 2 wks at maximum tolerated dosage
Carbamazepine† TN (1st line)PHN (2nd line)
100 mg bid 100 mg every 3–7 days 1,600 mg/day 8-12 wks
Lamotrigine TN (2nd line) 25 mg/day for 2 weeks Increase to 50 mg/day for 2 wks, then increase by 50–100 mg every wk
200–400 mg/day 12 wks (including titration period)
antidepressants
Amitriptyline PHN (1st line)DPN (1st line)TN (2nd line)
10–25 mg daily at bedtime Increase by 10 to 25 mg weekly Up to 75 mg daily 3 months at maximum tolerated dosage
Nortriptyline, desipramine
PHN (1st line)DPN (1st line)TN (2nd line)
10–25 mg at bedtime Increase by 25 mg daily every 3–7 days as tolerated
150 mg daily 6–8 wks with at least 2 wks at maximum tolerated dosage
Duloxetine DPN (1st line) 60 mg/day – 60 mg/day –
opioids
Morphine, oxycodone, methadone, levorphanol
PHN (2nd line) 10–15 mg morphine q4h or as needed (equianalgesic dosages should be used for other opioid analgesics)
After 1–2 wks, convert total daily dosage to long-acting opioid analgesic and continue short-acting medication as needed
No maximum dosage with careful titration
4–6 wks
Tramadol DPN (2nd line) 50 mg daily or bid Increase by 50–100 mg daily in divided doses every 3–7 days as tolerated
400 mg daily (100 mg qid); 300 mg daily in patients >75 years
4 wks
Local anaesthetics
IV lignocaine 5 mg/kg over 30–60 min Titrated based on symptoms of cyclic antidepressant toxicity, eg, perioral numbness, slurring of speech, tinnitus, dizziness, diplopia, convulsions
–
Mexiletine 150 mg daily to 200 mg bid Increase by 50 mg every 2 to 3 days prn 1,200 mg/day –
5% lignocaine patch PHN (1st line) Apply patch for a maximum of 12 h
None needed 3 patches daily for no more than 12 h in 24 h
2–4 wks
EMLA® PHN (1st line) tid, under occlusive dressing if possible
– – –
wks, weeks; IV, intravenous; EMLA, eutectic mixture of local anesthetics; –, information unavailable/incomplete; DPN, diabetic poly-neuropathy; PHN, postherpetic neuralgia; TN, trigeminal neuralgia
N.B. There is no evidence that paracetamol and NSAIDs are effective for the treatment of neuropathic pain.
* Pregabalin and gabapentin are licensed in Hong Kong for the treatment of neuropathic pain.
† Carbamazepine is licensed in Hong Kong for the treatment of trigeminal neuralgia and diabetic polyneuropathy.
Sources: American Medical Association. Assessing and Treating Neuropathic Pain. Module 9. September 2007. Available at: http://www.amacmeonline.com/pain_mgmt/printver-sion/ama_painmgmt_m9.pdf. Accessed April 18; 2008; Gilron I, Watson CPN, Ca-hill CM, Moulin DE. Neuropathic pain: a practical guide for the clinician. CMaJ 2006;175:265-275; Leicestershire Medi-cines Strategy Group. Guideline for treat-ing patients with neuropathic pain. May 2007. Available at: http://www.lmsg.nhs.uk/Guidelines/pdfdocs/NeuropathicPainGuide-line200711.pdf. Accessed April 18, 2008; The Merck Manual for Healthcare Profession-als. Neurological Disorders. Pain. Available at: http://www.merck.com/mmpe/sec16/ch209/ch209a.html#CACIDGIH. Accessed April 18, 2008.
Drug
s fo
r neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition12
Side effect profiles and management tipsThis table summarizes some of the more commonly encountered adverse effects associated with neuropathic pain treatments. The list is not exhaustive and full prescribing information should be consulted before initiating any therapy.
Drug Potential adverse effects Comments
anticonvulsants
Pregabalin Dizziness, somnolence, weight gain, blurred vision, dry mouth, constipation, peripheral oedema, euphoric mood, disturbed attention, increased appetite, balance disorder
Dose adjustment needed in renal dysfunction
Gabapentin Dose adjustment needed in renal dysfunction
Carbamazepine Sedation, dizziness, gait abnormalities, nausea & vomiting; serious AEs: hyponatraemia, agranulocytosis, aplastic anaemia, Stevens-Johnson syndrome*
Monitor CBC, liver enzymes and sodium levels for 1 year; contraindicated in porphyria, AV block or with concomitant MAO inhibitors; patients should seek immediate medical assistance if fever, sore throat, rash or mouth ulcers, bruising/bleeding develop
Lamotrigine Skin rash (potentially severe), irritability, headache, drowsiness, insomnia, dizziness, tremor, nystagmus, ataxia, diplopia, blurred vision, nausea, vomiting, diarrhoea, constipation, tiredness, arthralgia, painful menses, back pain
Very slow dose titration minimizes risk of rash; most cases of rash occur within first 8 weeks
antidepressants
Amitriptyline
Dry mouth, sweating, sedation, disturbed vision, cardiotoxicity, palpitations, postural hypotension, urinary retention, constipation, drowsiness
Give dose at bedtime to minimize effect of sedation; titrate dose slowly; may be poorly tolerated by the elderly; CI in patients with glaucoma and those taking MAO inhibitors
Nortriptyline, desipramine Nortriptyline causes less sedation and anticholinergic effects than amitriptyline; CI in patients with glaucoma and those taking MAO inhibitors
Duloxetine Nausea, dry mouth, constipation, GI distress, nausea/vomiting, decreased appetite, insomnia, dizziness, somnolence, blurred vision, increased sweating, fatigue
–
opioids
Morphine, oxycodone, methadone, levorphanol
Constipation, sedation, nausea, dizziness, vomiting, respiratory depression Coadminister pre-emptive stool softeners and antiemetics
Tramadol Dizziness, dry mouth, nausea, constipation, somnolence; risk of seizures/ epilepsy; risk of serotonergic syndrome if combined with SSRIs
Initiate therapy at low dose and titrate as tolerated; use with caution in epileptic patients
Local anaesthetics
IV lignocaine Tremor, insomnia or drowsiness, lightheadedness, slurred speech, ataxia, depression, agitation, change in sensorium, a change in personality, nystagmus, hallucinations, memory impairment, emotional lability
Decrease the infusion rate or discontinue treatment if signs of toxicity
Mexiletine Lightheadedness, dizziness, nervousness, inco-ordination, GI distress, nausea/vomiting, trembling, unsteady gait, tremor, ataxia; proarrhythmia, impaired haemodynamics
Consider cardiac evaluation before initiating therapy in patients with a significant heart disorder; monitor blood pressure; monitor and adjust dose to prevent QTc prolongation; administer with food or prescribe antacids to reduce GI AEs; has a narrow therapeutic index
5% lignocaine patch Mild localized skin reactions around application site Only apply to healed intact skin; apply to affected area
EMLA® Pale skin, redness or swelling at the application site, burning, change in hot or cold sensation
–
Drug
s fo
r neu
ropa
thic
pai
n

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 13
Drug Potential adverse effects Comments
anticonvulsants
Pregabalin Dizziness, somnolence, weight gain, blurred vision, dry mouth, constipation, peripheral oedema, euphoric mood, disturbed attention, increased appetite, balance disorder
Dose adjustment needed in renal dysfunction
Gabapentin Dose adjustment needed in renal dysfunction
Carbamazepine Sedation, dizziness, gait abnormalities, nausea & vomiting; serious AEs: hyponatraemia, agranulocytosis, aplastic anaemia, Stevens-Johnson syndrome*
Monitor CBC, liver enzymes and sodium levels for 1 year; contraindicated in porphyria, AV block or with concomitant MAO inhibitors; patients should seek immediate medical assistance if fever, sore throat, rash or mouth ulcers, bruising/bleeding develop
Lamotrigine Skin rash (potentially severe), irritability, headache, drowsiness, insomnia, dizziness, tremor, nystagmus, ataxia, diplopia, blurred vision, nausea, vomiting, diarrhoea, constipation, tiredness, arthralgia, painful menses, back pain
Very slow dose titration minimizes risk of rash; most cases of rash occur within first 8 weeks
antidepressants
Amitriptyline
Dry mouth, sweating, sedation, disturbed vision, cardiotoxicity, palpitations, postural hypotension, urinary retention, constipation, drowsiness
Give dose at bedtime to minimize effect of sedation; titrate dose slowly; may be poorly tolerated by the elderly; CI in patients with glaucoma and those taking MAO inhibitors
Nortriptyline, desipramine Nortriptyline causes less sedation and anticholinergic effects than amitriptyline; CI in patients with glaucoma and those taking MAO inhibitors
Duloxetine Nausea, dry mouth, constipation, GI distress, nausea/vomiting, decreased appetite, insomnia, dizziness, somnolence, blurred vision, increased sweating, fatigue
–
opioids
Morphine, oxycodone, methadone, levorphanol
Constipation, sedation, nausea, dizziness, vomiting, respiratory depression Coadminister pre-emptive stool softeners and antiemetics
Tramadol Dizziness, dry mouth, nausea, constipation, somnolence; risk of seizures/ epilepsy; risk of serotonergic syndrome if combined with SSRIs
Initiate therapy at low dose and titrate as tolerated; use with caution in epileptic patients
Local anaesthetics
IV lignocaine Tremor, insomnia or drowsiness, lightheadedness, slurred speech, ataxia, depression, agitation, change in sensorium, a change in personality, nystagmus, hallucinations, memory impairment, emotional lability
Decrease the infusion rate or discontinue treatment if signs of toxicity
Mexiletine Lightheadedness, dizziness, nervousness, inco-ordination, GI distress, nausea/vomiting, trembling, unsteady gait, tremor, ataxia; proarrhythmia, impaired haemodynamics
Consider cardiac evaluation before initiating therapy in patients with a significant heart disorder; monitor blood pressure; monitor and adjust dose to prevent QTc prolongation; administer with food or prescribe antacids to reduce GI AEs; has a narrow therapeutic index
5% lignocaine patch Mild localized skin reactions around application site Only apply to healed intact skin; apply to affected area
EMLA® Pale skin, redness or swelling at the application site, burning, change in hot or cold sensation
–
CI, contraindicated; MAO, monoamine oxidase; AEs, adverse effects; CBC, complete blood count; AV, atrioventricular; SSRI, selective serotonin reuptake inhibitor; EMLA, eutectic mixture of local anesthetics; IV, intravenous; GI, gastrointestinal; –, information unavailable/incomplete
* Genetic susceptibility for Stevens-Johnson syndrome (HLA-B1502) should be assessed in Asian patients before commencing treatment with carbamazepine.
Sources:American Medical Association. Assessing and Treating Neuropathic Pain. Module 9. September 2007. Available at: http://www.amacmeonline.com/pain_mgmt/printversion/ama_painmgmt_m9.pdf. Accessed April 18; 2008; Dworkin RH, O’Connor AB, Backonja M, et al. Pharmacologic management of neuropathic pain. Evidence-based recommenda-tions. Pain 2007;132:237-251; Gilron I, Watson CPN, Cahill CM, Moulin DE. Neuropathic pain: a practi-cal guide for the clinician. CMaJ 2006;175:265-275; Leicestershire Medicines Strategy Group. Guideline for treating patients with neuropathic pain. May 2007. Available at: http://www.lmsg.nhs.uk/Guide-lines/pdfdocs/NeuropathicPainGuideline200711.pdf. Accessed April 18, 2008; The Merck Manual for Healthcare Professionals. Neurological Disorders. Pain. Available at: http://www.merck.com/mmpe/sec16/ch209/ch209a.html#CACIDGIH. Accessed April 18, 2008.
Drug
s fo
r neu
ropa
thic
pai
n

Postherpetic neuralgia14
Recommendations for postherpetic neuralgia7
TCA, tricyclic antidepressant; A2D, alpha-2-delta; EMLA, eutectic mixture of local anaesthetics; TENS, transcutaneous electrical nerve stimulation; NMDA, N-methyl D-aspartateThe A2D ligands are pregabalin and gabapentin
* Genetic susceptibility for Stevens-Johnson syndrome (HLA-B1502) should be assessed in Asian patients before commencing treatment with carbamazepine.
Post
herp
etic
neu
ralg
ia
Postherpetic neuralgia is a neuropathic pain syndrome
that occurs following acute herpes zoster infection
or shingles.

Postherpetic neuralgia 15
• Start low-dose amitriptyline or nortriptyline therapy (10 to 25 mg at night) and titrate weekly up to the maximum tolerated dose or a maximum of 150 mg.
• For patients older than 60 years, or in cases where TCAs are not tolerated or are contra-indicated, the A2D ligands pregabalin or gabapentin may be used.8-13 In some practices, pregabalin and gabapentin are considered first-line therapy.
• Add a topical local anaesthetic, such as a lignocaine patch14-16 or EMLA cream.17,18 This can be first-line treatment if antidepressants and anticonvulsants are contraindicated.
• Carbamazepine is commonly used, but there is little evidence to support its use.
• Consider tramadol19 or opioids20 if antidepressants and anticonvulsants are ineffective or are contraindicated.
• Consider transcutaneous electrical nerve stimulation (TENS) as adjunctive therapy.
• If adequate pain control is not achieved after 8 weeks, consider referring the patient to a pain medicine specialist for alternative therapies, such as NMDA receptor antagonists,21 intrathecal steroids,22 intravenous adenosine 5’-triphosphate (ATP),23,24 or combination therapy.25,26 A multidisciplinary approach to managing these difficult-to-treat patients may be necessary.
Post
herp
etic
neu
ralg
ia

Painful diabetic peripheral neuropathy16
Diab
etic
neu
ropa
thy
Recommendations for idiopathic trigeminal neuralgia27
A2D, alpha-2-delta; PRFR, percutaneous radiofrequency rhizotomy; BCR, balloon compression rhizotomy; PRGR, percutaneous retro-Gasserian glycerol rhizotomyThe A2D ligands are pregabalin and gabapentin
* Genetic susceptibility for Stevens-Johnson syndrome (HLA-B1502) should be assessed in Asian patients before commencing treatment with carbamazepine.
The second or third division of the trigeminal nerve is
affected in most trigeminal neuralgia patients.

Painful diabetic peripheral neuropathy 17
Diab
etic
neu
ropa
thy
• The primary care physician should try carbamazepine first.28
• If the response is not satisfactory or the patient cannot tolerate treatment, one or two second-line drugs may be tried. The second-line drugs include pregabalin,11-13,29-31 gabapentin,32 phenytoin,33 sodium valproate,33 clonazepam,34,35 baclofen,36 lamotrigine33 and antidepressant agents.37
• For chronic, intractable pain, a patient should be referred to a multidisciplinary pain management centre.
• Peripheral trigeminal nerve block is a useful adjunctive therapy, and may be used while pharmacotherapy is being optimized.38-40
• If treatment is not successful following a trial of two or three medications for an adequate period (3 to 6 months), an operation or interventional treatment should be considered.
• Selecting a procedure is both difficult and controversial. Patients should be allowed to consider all of the available options.
– In general, for patients younger than 70 years who have a low surgical risk and prefer to preserve trigeminal nerve function, microvascular decompression should be recommended.41
– Percutaneous radiofrequency rhizotomy (PRFR) can be considered for patients who have failed medical treatment and suffer from intractable TN.42
– In cases involving the ophthalmic division or all three divisions, balloon compression rhizotomy (BCR) should be considered over PRFR.43
– Gamma knife radiosurgery (GKR) should be reserved for patients who have failed both surgical and percutaneous procedures.44,45

Idiopathic trigeminal neuralgia18
Trig
emin
al n
eura
lgia
Recommendations for painful diabetic peripheral neuropathy46
TCA, tricyclic antidepressant; A2D, alpha-2-delta; NMDA, N-methyl-D-aspartate; PENS, percutaneous electrical nerve stimulation; TENS, transcutaneous electrical nerve stimulation; SNRI, serotonin–norepinephrine reuptake inhibitorThe A2D ligands are pregabalin and gabapentin
Approximately 20 to 40% of diabetic patients develop some
sort of neuropathy. Diabetic neuropathy may lead to foot
ulceration and even the need for amputation.

Idiopathic trigeminal neuralgia 19
Trig
emin
al n
eura
lgia
• A2D ligands (eg, pregabalin and gabapentin) should be considered as first-line treatment options due to their efficacy and safety.28-31,47 In addition, A2D ligands are generally associ-ated with fewer side effects compared with TCAs, carbamazepine or phenytoin. Also, the side effects can be further minimized by slow dosage titration.
• For chronic pain, TCAs (eg, amitriptyline, nortriptyline, desipramine) should be considered first-line therapies.28 Pain relief may not be apparent for up to 3 weeks. TCAs are contra-indicated in patients with cardiac and hepatic disease. Some patients cannot tolerate the side effects of TCAs, but these can be minimized by starting with a low dose at night and increasing gradually. Nortriptyline, imipramine and desipramine are less sedating than amitriptyline.
• For acute pain, start with simple analgesics and progress to TCAs or other adjuvant analgesics, if necessary.
• If TCAs are contraindicated , ineffective and/or not well tolerated, SNRIs should also be considered as an alternate first-line choice, or as an add-on therapy to A2D ligands.48-50
• Tramadol may be an effective alternative for some patients.51
• Patients remaining refractory to a reasonable trial of pharmacotherapy (eg, 2 to 3 months with two to three different agents) should be referred to a multidisciplinary pain clinic for further therapeutic initiatives.
• Physical stimulation, such as TENS52 and acupuncture, may counteract painful sensations. However, acupuncture and topical treatments should be used with caution in the lower leg in patients with diabetes, as these may aggravate the skin and lead to infection. More invasive stimulatory interventions, such as spinal cord stimulation, may be considered as a last option.53
• Pain management programmes and behavioural therapy can also be used with pharma-cological approaches to teach patients how to live with pain. Regular walking, warm baths or elastic stockings may also help to relieve leg pain.

Neuropathic pain associated with peripheral nerve entrapment20
Cervical radiculopathy
Lumbar radiculopathy
Carpal tunnel syndrome
Cubital tunnel syndrome
Conservative treatment
• Cervical collar• Oral NSAIDs• Physiotherapy/neck
care exercises• Anticonvulsants or
antidepressants• Epidural
corticosteroid injection
• Lumbar corset • Oral NSAIDs• Physiotherapy• PENS/TENS• Anticonvulsants
or antidepressants• Epidural
corticosteroid injection
• Chemonucleolysis
• Physiotherapy• Wrist splinting• Oral steroids
and local steroid injections
• Diuretics
• Educate patient on how to avoid provoking symptoms
• Conservative treatment does not have a great role in management
surgical interventions
• Anterior discectomy with spinal fusion
• Microforaminotomy• Cervical arthroplasty
• Discectomy• Microdiscectomy• Percutaneous
discectomy• Lumbar
foraminotomy• Lumbar spinal
fusion
• Carpal tunnel release (open or endoscopic)
• Simple neurolysis• Anterior transposition
of ulnar nerve• Medial
epicondylectomy of distal humerus
• Cubital tunnel release (open or endoscopic)
Recommendations for neuropathic pain associated with peripheral nerve entrapment54
NSAIDS, nonsteroidal anti-inflammatory drugs; PENS, percutaneous electrical nerve stimulation; TENS, transcutaneous electrical nerve stimulation
Perip
hera
l ner
ve e
ntra
pmen
t
Carpal tunnel syndrome results from compression of the median nerve at the carpal tunnel.

Neuropathic pain associated with peripheral nerve entrapment 21
Cervical radiculopathy• Mild cases may improve without treatment, or may benefit from short-term use of a cer-
vical collar, nonsteroidal anti-inflammatory drugs (NSAIDs), neck-care exercises, postural training and activity modification, and intermittent cervical traction. Pregabalin has dem-onstrated some benefit in cervical radiculopathy.55
• Surgery (eg, decompression via an anterior cervical approach with spinal fusion or a posterior approach with laminectomy) is indicated for more severe cases or when other treatments have failed.
Lumbar radiculopathy• Bed rest is not recommended; mobility must be maintained.56
• Oral NSAIDs57 and physiotherapy may be beneficial. Epidural corticosteroids and percu-taneous or transcutaneous electrical nerve stimulation may give short-term relief.58-60
• Gabapentin was effective in patients with chronic radiculopathy (L4-5 and/or L5-S1 bulg-ing and/or protrusion).61 Pregabalin as monotherapy or add-on therapy improved patient-reported clinical outcomes in painful lumbar or cervical radiculopathy.55
Carpal tunnel syndrome• Conservative strategies that may be of benefit include good ergonomics, splinting of the
wrist in a neutral position, rest at intervals and minimizing hand or wrist movements. Acupuncture and ultrasound may also reduce pain.62
• NSAIDs, diuretics and oral corticosteroids are options for mild-to-moderate carpal tunnel syndrome. Local steroid injection may be superior to oral corticosteroids.63,64
• Carpal tunnel release surgery (open or endoscopic) is indicated when conservative thera-py has failed, or motor involvement or severe numbness is present.
Cubital tunnel syndrome• Frequently requires a release operation, such as simple neurolysis, anterior transposition
of the ulnar nerve or medial epicondylectomy of the distal humerus.
Perip
hera
l ner
ve e
ntra
pmen
t

Central post-stroke pain
Recommendations for central post-stroke pain65
A2D, alpha-2-delta; TCA, tricyclic antidepressant; CPSP, central post-stroke painThe A2D ligands are pregabalin and gabapentin
Cent
ral p
ost-s
troke
pai
n
CPSP is characterized by constant or intermittent pain
following a stroke. Around 8% of stroke patients will develop CPSP.

Central post-stroke pain 23
• TCAs such as amitriptyline or nortriptyline should be considered as first-line therapy for central post-stroke pain (CPSP). To minimize side effects, commence at a low dose and titrate to a higher maintenance dose.
• The A2D ligand pregabalin is a first-line treatment option as it has been shown to significantly reduce pain and improve health status in patients with central pain, including CPSP.66
• Lamotrigine may be used as a second-line agent or an alternative first-line treatment to TCAs.67
• Gabapentin, another A2D ligand, is approved for the treatment of neuropathic pain and may be effective in treating CPSP.68
• Central pain appears to be poorly responsive, but not totally unresponsive, to opioids.69
• Intravenous lignocaine may provide pain relief in some patients with CPSP.70,71
• Mexiletine may be used as an adjunct to TCAs when patients do not respond to TCAs alone.72
• Patients remaining refractory to a reasonable trial of pharmacotherapy should be referred to a multidisciplinary pain clinic for further therapeutic initiatives.
• Intrathecal baclofen may be effective in some patients with CPSP,73,74 but should only be considered after the failure of other pharmacologic therapies.
• Surgical interventions can be considered for patients unresponsive to pharmacological therapy, but may be associated with morbidity and mortality. Motor cortex stimulation, spinal cord stimulation and stereotactic mesencephalic tractotomy may be beneficial.75,76
Cent
ral p
ost-s
troke
pai
n

Neuropathic cancer pain24
Recommendations for neuropathic cancer pain77
Neu
ropa
thic
can
cer p
ain
A2D, alpha-2-delta; TCA, tricyclic antidepressant; CPSP, central post-stroke painThe A2D ligands are pregabalin and gabapentin

Neuropathic cancer pain 25
• For neuropathic pain caused by direct tumour involvement, first-line management is oncologic treatment and may include surgery, radiation therapy or chemotherapy.78 For example, radiotherapy can relieve neuropathic pain due to tumour-induced neural compression or irritation.79
• Correctable causes of neuropathic pain (eg, spinal cord compression) should be managed appropriately.
• Anticonvulsants should be considered if neuropathic pain is unresponsive to conventional analgesics. Neuropathic pain specifically due to cancer treatment may be treated with gabapentin.80 Pregabalin after epidural anaesthesia significantly improved visual analogue scale (VAS) and quality-of-life scores in chronic cancer patients.81 Anticonvulsants should be initiated at a low dose and slowly titrated until the patient achieves adequate pain relief or side effects develop.82
• Antidepressants such as TCAs or selective serotonin reuptake inhibitors are alternative options for management of neuropathic pain.83,84 Antidepressants may be given together with anticonvulsants when there is unsatisfactory response to either medication.85
• Systemic ketamine may be effective, but because of its adverse effects should be limited to experienced teams.86,87
• Other adjunctive therapies include systemic lignocaine.82
• Interventional therapy may also be effective for neuropathic cancer pain.88 However, certain interventional techniques for neuropathic pain should only be considered when pharmacologic interventions have failed, are poorly tolerated or inappropriate.87
• Patients with postsurgical neuropathic pain may also benefit from topical capsaicin cream when appropriate.89
Neu
ropa
thic
can
cer p
ain

Neuropathic pain due to spinal cord pathologies26
Recommendations for neuropathic pain due to spinal cord pathologies90
A2D, alpha-2-delta; TCA, tricyclic antidepressantThe A2D ligands are pregabalin and gabapentin
Spin
al c
ord
path
olog
y Pain develops in around 60 to 70% of patients with spinal cord injury, and about one third will report severe pain.

Neuropathic pain due to spinal cord pathologies 27
• Treatment of neuropathic pain due to spinal cord lesions includes primary treatment of the underlying cause (eg, surgery for certain structural abnormalities) and other neuro-logical sequelae (eg, motor deficits, incontinence).
• Spinal cord injury (SCI) causing compression should be treated within 8 hours of com-pression, if possible.91 Methylprednisolone may be given as a 30 mg/kg-bolus dose, then maintained at a dose of 5.4 mg/kg/h. If initiated within 3 hours, treatment should be maintained for 24 hours; maintain treatment for 48 hours if initiated between 3 and 8 hours after injury. If neuropathic pain is due to direct compression by tumour, anti-neoplastic treatment may reduce tumour size and provide pain relief.92
• There is very little evidence that NSAIDs have benefit for pain due to spinal cord lesions.93,94
• A2D ligands (eg, pregabalin, gabapentin) may be used in conjunction with physical and psychological therapy as first-line treatments for neuropathic pain due to spinal cord le-sions.95,96 Alternatively, TCAs may also be considered as a first-line management option despite limited evidence.28 Patients may also be given other anticonvulsants or opioids to improve pain control.93,96-100
• Intravenous ketamine may be used as third-line therapy, but requires meticulous monitoring for side effects.100,102,103
• Patients who respond poorly to oral, transdermal or intravenous analgesics may be considered for invasive procedures, such as intrathecal drug administration, neurostimula-tion (eg, spinal cord stimulation, electroacupuncture) and dorsal root entry zone lesioning (DREZotomy).104-114
• A multidisciplinary approach should be taken to rehabilitation.91 Many patients achieve significant pain relief from physical therapy.94
Spin
al c
ord
path
olog
y

Complex regional pain syndrome28
Recommendations for complex regional pain syndrome115
*Primarily diagnostic and/or to facilitate physical rehabilitation. The efficacy of sympathetic blocks in the treatment of CRPS is still poorly defined. CRPS, complex regional pain syndrome; NSAID, nonsteroidal anti-inflammatory drug; TCA, tricyclic antidepressant; TENS, transcutaneous electrical nerve stimulationAdapted from treatment algorithm proposed by the International Coalition on Neuropathic Pain.116
Com
plex
regi
onal
pai
n sy
ndro
me

Complex regional pain syndrome 29
• Patient outcomes are improved if treatment is started at an early stage: patients should be referred as soon as possible to pain specialists or physicians with experience in managing complex regional pain syndrome (CRPS).117
• An early programme of physical and occupational therapy, especially for at-risk patients, is essential to treat the secondary complications of CRPS, such as decreased joint and tendon movement. This will improve pain control and mobility.117
• Psychological support and cognitive behavioural management programmes can help patients manage their pain, and reduce depression and dependence on health care.
• For patients with sympathetic maintained pain (SMP), sympathetic blocks provide effec-tive pain relief to facilitate physical rehabilitation.
• Whenever appropriate, anti-inflammatory medications are useful in the acute phase following injury to minimize pain and swelling.118,119
• Primary pain management should include tricyclic antidepressants ([TCAs] eg, amitripty-line)120,121 or anticonvulsants (eg, gabapentin, pregabalin).66,122,123 Slow dosage titration (up to 8 weeks) is necessary to minimize side effects of both TCAs and anticonvulsants; pain relief may not be apparent for 3 weeks at the maximum tolerated dosage.
• When the response to TCAs and anticonvulsants is unsatisfactory, a trial of combined TCA and anticonvulsant may be effective.116
• Rescue therapy with opioids may be necessary, but this should only be used for short-term treatment.124
• For patients remaining refractory to trials of pharmacotherapy and physiotherapy, invasive procedures can be considered. Neurostimulation of the spinal cord or peripheral nerves may be effective,125,126 but may not improve long-term prognosis. Destructive or ablative surgery is not recommended127 and only has a limited role in providing relief for patients with a short life expectancy.
Com
plex
regi
onal
pai
n sy
ndro
me

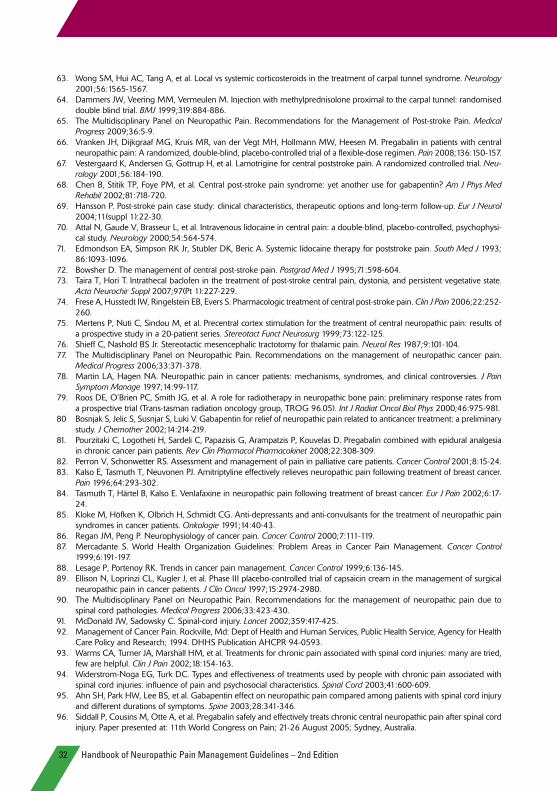
Handbook of Neuropathic Pain Management Guidelines – 2nd Edition30
References1. De Andrés J, Garcia-Ribas G. Neuropathic pain treatment: the challenge. Pain Practice 2003;3:1-7.2. Gilron I, Watson CPN, Cahill CM, Moulin DE. Neuropathic pain: a practical guide for the clinician. CMAJ 2006;175:265-
275. 3. Galluzzi KE. Managing neuropathic pain. J Am Osteopath Assoc 2007;107(suppl 6):ES39-ES48. 4. Baron R. Mechanisms of disease: neuropathic pain – a clinical perspective. Nat Clin Pract Neurol 2006;2:95-106.5. Portenoy R. Development and testing of a neuropathic pain screening questionnaire: ID Pain. Curr Med Res Opin
2006;22:1555-1565.6. Chan A, Wong S, Chen PP, et al. Validation study of the Chinese ID Pain questionnaire for neuropathic pain. Hong Kong
Med J In Press.7. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the Management of Postherpetic Neuralgia.
Medical Progress 2006;33:475-482.8. Rice AS, Maton S, Postherpetic Neuralgia Study Group. Gabapentin in postherpetic neuralgia: a randomized, double
blind, placebo-controlled study. Pain 2001;94:215-224.9. Rowbotham M, Harden N, Stacey B, et al. Gabapentin for the treatment of postherpetic neuralgia: a randomized con-
trolled trial. JAMA 1998;280:1837-1842.10. Serpell MG, Neuropathic Pain Study Group. Gabapentin in neuropathic pain syndromes: a randomised, double-blind,
placebo-controlled trial. Pain 2002;99:557-566. 11. Freynhagen R, Strojek K, Griesing T, et al. Efficacy of pregabalin in neuropathic pain evaluated in a 12-week, randomised,
double-blind, multicentre, placebo-controlled trial of flexible- and fixed-dose regimens. Pain 2005;115:254-263. 12. Dworkin RH, Corbin AE, Young JP Jr, et al. Pregabalin for the treatment of postherpetic neuralgia: a randomized, placebo-
controlled trial. Neurology 2003;60:1274-1283.13. Sabatowski R, Galvez R, Cherry DA, et al. Pregabalin reduces pain and improves sleep and mood disturbances in patients
with post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial. Pain 2004;109:26-35. 14. Rowbotham MC, Davies PS, Fields HL. Topical lidocaine gel relieves postherpetic neuralgia. Ann Neurol 1995;37:246-
253.15. Rowbotham MC, Davies PS, Verkempinck C, Galer BS. Lidocaine patch: double-blind controlled study of a new treatment
method for post-herpetic neuralgia. Pain 1996;65:39-44.16. Galer BS, Rowbotham MC, Perander J, Friedman E. Topical lidocaine patch relieves postherpetic neuralgia more effectively
than a vehicle topical patch: results of an enriched enrollment study. Pain 1999;80:533-538.17. Litman SJ, Vitkun SA, Poppers PJ. Use of EMLA cream in the treatment of post-herpetic neuralgia. J Clin Anesth 1996;8:54-
57.18. Attal N, Brasseur L, Chauvin M, Bouhassira D. Effects of single and repeated applications of a eutectic mixture of local
anaesthetics (EMLA) cream on spontaneous and evoked pain in post-herpetic neuralgia. Pain 1999;81:203-209.19. Boureau F, Legallicier P, Kabir-Ahmadi M. Tramadol in post-herpetic neuralgia: a randomized, double-blind, placebo-
controlled trial. Pain 2003;104:323-331. 20. Watson CP, Babul N. Efficacy of oxycodone in neuropathic pain: a randomized trial in postherpetic neuralgia. Neurology
1998;50:1837-1841.21. Kanazi GE, Johnson RW, Dworkin RH. Treatment of postherpetic neuralgia: an update. Drugs 2000;59:1113-1126.22. Kotani N, Kushikata T, Hashimoto H, et al. Intrathecal methylprednisolone for intractable postherpetic neuralgia. N Engl J
Med 2000;343:1514-1519.23. Hayashida M, Fukuda K, Fukunaga A, et al. Analgesic effect of intravenous ATP on postherpetic neuralgia in comparison
with responses to intravenous ketamine and lidocaine. J Anesth 2005;19:31-35.24. Moriyama M, Kitamura A, Ikezaki H, et al. Systemic ATP infusion improves spontaneous pain and tactile allodynia, but not
tactile hypesthesia, in patients with postherpetic neuralgia. J Anesth 2004;18:177-180. 25. Gilron I, Bailey JM, Tu D, et al. Morphine, gabapentin, or their combination for neuropathic pain. N Engl J Med
2005;352:1324-1334. 26. White WT, Patel N, Drass M, Nalamachu S. Lidocaine patch 5% with systemic analgesics such as gabapentin: a rational
polypharmacy approach for the treatment of chronic pain. Pain Med 2003;4:321-330. 27. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the Management of Idiopathic Trigeminal Neu-
ralgia. Medical Progress 2006;33:527-534.28. Attal N, Cruccu G, Baron R, et al. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision.
Eur J Neurol 2010;17:1113-e88.29. Rosenstock J, Tuchman M, LaMoreaux L, Sharma U. Pregabalin for the treatment of painful diabetic peripheral neuropa-
thy: a double-blind, placebo-controlled trial. Pain 2004;110:628-638. 30. Lesser H, Sharma U, LaMoreaux L, Poole RM. Pregabalin relieves symptoms of painful diabetic neuropathy: a randomized
controlled trial. Neurology 2004;63:2104-2110. 31. Richter RW, Portenoy R, Sharma U, et al. Relief of painful diabetic peripheral neuropathy with pregabalin: a randomized,
placebo-controlled trial. J Pain 2005;6:253-260.

Handbook of Neuropathic Pain Management Guidelines – 2nd Edition 31
32. Wiffen P, Collins S, McQuay H, et al. Anticonvulsant drugs for acute and chronic pain. Cochrane Database Syst Rev 2000;(3):CD001133.
33. Spina E, Perugi G. Antiepileptic drugs: indications other than epilepsy. Epileptic Disord 2004;6:57-75.34. Caccia MR. Clonazepam in facial neuralgia and cluster headache. Clinical and electrophysiological study. Eur Neurol
1975;13:560-563.35. Chandra B. The use of clonazepam in the treatment of tic douloureux (a preliminary report). Proc Aust Assoc Neurol
1976;13:119-122.36. Fromm GH, Terrence CF, Chattha AS. Baclofen in the treatment of trigeminal neuralgia: double-blind study and long-term
follow-up. Ann Neurol 1984;15:240-244.37. Dworkin RH, Backonja M, Rowbotham MC, et al. Advances in neuropathic pain: Diagnosis, mechanisms, and treatment
recommendations. Arch Neurol 2003;60:1524-1534.38. Stajcic Z, Juniper RP, Todorovic L. Peripheral streptomycin/lidocaine injections versus lidocaine alone in the treatment of
idiopathic trigeminal neuralgia. A double blind controlled trial. J Craniomaxillofac Surg 1990;18:243-246.39. Bittar GT, Graff-Radford SB. The effects of streptomycin/lidocaine block on trigeminal neuralgia: a double-blind crossover
placebo controlled study. Headache 1993;33:155-160.40. Hyodo M, Akutagawa T, Shirofuji T, Morimoto M, Morimoto E. Peripheral branch block treatment with high concentration
bupivacaine for primary trigeminal neuralgia. Pain Clin 1993;6:187-19141. Toda K. Operative treatment of trigeminal neuralgia: review of current techniques. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2008;106:788-805.42. Cruccu G, Gronseth G, Alksne J, et al. AAN-EFNS guidelines on trigeminal neuralgia management. Eur J Neurol
2008;15:1013-1028.43. Brown JA. Percutaneous balloon compression for trigeminal neuralgia. Clin Neurosurg 2009;56:73-78.44. Kondziolka D, Zorro O, Lobato-Polo J, et al. Gamma Knife sterotactic radiosurgery for idiopathic trigeminal neuralgia.
J Neurosurg 2010;112:758-765.45. Dhopple AA, Adams JR, Maggio WW, et al. Long-term outcomes of Gamma Knife radiosurgery for classic trigeminal
neuralgia: implications of treatment and critical review of the literature. J Neurosurg 2009;111:351-358.46. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the Management of Painful Diabetic Peripheral
Neuropathy. Medical Progress 2006;33:579-585. 47. Backonja M, Beydoun A, Edwards KR, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients
with diabetes mellitus: a randomized controlled trial. JAMA 1998;280:1831-1836.48. Wernicke JF, Wang F, Pritchett YL, et al. An open-label 52-week clinical extension comparing duloxetine with routine care
in patients with diabetic peripheral neuropathic pain. Pain Med 2007;8:503-513.49. Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy or chronic pain. Cochrane Database Syst Rev
2009;(4):CD007115.50. Simpson DA. Gabapentin and venlafaxine for the treatment of painful diabetic neuropathy. J Clin Neuromuscul Dis
2001;3:53-62.51. Harati Y, Gooch C, Swenson M, et al. Double-blind randomized trial of tramadol for the treatment of the pain of diabetic
neuropathy. Neurology 1998;50:1842-1846.52. Kumar D, Alvaro MS, Julka IS, Marshall HJ. Diabetic peripheral neuropathy. Effectiveness of electrotherapy and amitripty-
line for symptomatic relief. Diabetes Care 1998;21:1322-1325.53. Daousi C, Benbow SJ, MacFarlane IA. Electrical spinal cord stimulation in the long-term treatment of chronic painful
diabetic neuropathy. Diabet Med 2005;22:393-398.54. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for neuropathic pain associated with peripheral nerve
entrapment. Medical Progress 2010;37:369-375.55. Saldaña MT, Navarro A, Pérez C, Masramón X, Rejas J. Patient-reported-outcomes in subjects with painful lumbar or
cervical radiculopathy treated with pregabalin: evidence from medical practice in primary care settings. Rheumatol Int 2010;30:1005-1015.
56. Vroomen PC, de Krom MC, Wilmink JT, Kester AD, Knottnerus JA. Lack of effectiveness of bed rest for sciatica. N Engl J Med 1999;340:418-423.
57. Dreiser RL, Le Parc JM, Vélicitat P, Lleu PL. Oral meloxicam is effective in acute sciatica: two randomised, double-blind trials versus placebo or diclofenac. Inflamm Res 2001:50(Suppl 1):S17-S23.
58. Carette S, Leclaire R, Marcoux S, et al. Epidural corticosteroid injections for sciatica due to herniated nucleus pulposus. N Engl J Med 1997;336:1634-1640.
59. Samanta A, Beardsley J. Sciatica: which intervention? BMJ 1999;319:302-303. 60. Ghoname EA, White PF, Ahmed HE, Hamza MA, Craig WF, Noe CE. Percutaneous electrical nerve stimulation: an alterna-
tive to TENS in the management of sciatica. Pain 1999;83:193-199. 61. Yildirim K, Sisecioglu M, Karatay, et al. The effectiveness of gabapentin in patients with chronic radiculopathy. Pain Clinic
2003;15:213-218. 62. Ebenbichler GR, Resch KL, Nicolakis P, et al. Ultrasound treatment for treating the carpal tunnel syndrome: randomised
“sham” controlled trial. BMJ 1998;316:731-735.
Handbook of Neuropathic Pain Management Guidelines – 2nd Edition32
63. Wong SM, Hui AC, Tang A, et al. Local vs systemic corticosteroids in the treatment of carpal tunnel syndrome. Neurology 2001;56:1565-1567.
64. Dammers JW, Veering MM, Vermeulen M. Injection with methylprednisolone proximal to the carpal tunnel: randomised double blind trial. BMJ 1999;319:884-886.
65. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the Management of Post-stroke Pain. Medical Progress 2009;36:5-9.
66. Vranken JH, Dijkgraaf MG, Kruis MR, van der Vegt MH, Hollmann MW, Heesen M. Pregabalin in patients with central neuropathic pain: A randomized, double-blind, placebo-controlled trial of a flexible-dose regimen. Pain 2008;136:150-157.
67. Vestergaard K, Andersen G, Gottrup H, et al. Lamotrigine for central poststroke pain. A randomized controlled trial. Neu-rology 2001;56:184-190.
68. Chen B, Stitik TP, Foye PM, et al. Central post-stroke pain syndrome: yet another use for gabapentin? Am J Phys Med Rehabil 2002;81:718-720.
69. Hansson P. Post-stroke pain case study: clinical characteristics, therapeutic options and long-term follow-up. Eur J Neurol 2004;11(suppl 1):22-30.
70. Attal N, Gaude V, Brasseur L, et al. Intravenous lidocaine in central pain: a double-blind, placebo-controlled, psychophysi-cal study. Neurology 2000;54:564-574.
71. Edmondson EA, Simpson RK Jr, Stubler DK, Beric A. Systemic lidocaine therapy for poststroke pain. South Med J 1993; 86:1093-1096.
72. Bowsher D. The management of central post-stroke pain. Postgrad Med J 1995;71:598-604.73. Taira T, Hori T. Intrathecal baclofen in the treatment of post-stroke central pain, dystonia, and persistent vegetative state.
Acta Neurochir Suppl 2007;97(Pt 1):227-229.74. Frese A, Husstedt IW, Ringelstein EB, Evers S. Pharmacologic treatment of central post-stroke pain. Clin J Pain 2006;22:252-
260.75. Mertens P, Nuti C, Sindou M, et al. Precentral cortex stimulation for the treatment of central neuropathic pain: results of
a prospective study in a 20-patient series. Stereotact Funct Neurosurg 1999;73:122-125.76. Shieff C, Nashold BS Jr. Stereotactic mesencephalic tractotomy for thalamic pain. Neurol Res 1987;9:101-104.77. The Multidisciplinary Panel on Neuropathic Pain. Recommendations on the management of neuropathic cancer pain.
Medical Progress 2006;33:371-378.78. Martin LA, Hagen NA. Neuropathic pain in cancer patients: mechanisms, syndromes, and clinical controversies. J Pain
Symptom Manage 1997;14:99-117. 79. Roos DE, O’Brien PC, Smith JG, et al. A role for radiotherapy in neuropathic bone pain: preliminary response rates from
a prospective trial (Trans-tasman radiation oncology group, TROG 96.05). Int J Radiat Oncol Biol Phys 2000;46:975-981. 80 Bosnjak S, Jelic S, Susnjar S, Luki V. Gabapentin for relief of neuropathic pain related to anticancer treatment: a preliminary
study. J Chemother 2002;14:214-219. 81. Pourzitaki C, Logotheti H, Sardeli C, Papazisis G, Arampatzis P, Kouvelas D. Pregabalin combined with epidural analgesia
in chronic cancer pain patients. Rev Clin Pharmacol Pharmacokinet 2008;22:308-309.82. Perron V, Schonwetter RS. Assessment and management of pain in palliative care patients. Cancer Control 2001;8:15-24. 83. Kalso E, Tasmuth T, Neuvonen PJ. Amitriptyline effectively relieves neuropathic pain following treatment of breast cancer.
Pain 1996;64:293-302. 84. Tasmuth T, Härtel B, Kalso E. Venlafaxine in neuropathic pain following treatment of breast cancer. Eur J Pain 2002;6:17-
24. 85. Kloke M, Höfken K, Olbrich H, Schmidt CG. Anti-depressants and anti-convulsants for the treatment of neuropathic pain
syndromes in cancer patients. Onkologie 1991;14:40-43. 86. Regan JM, Peng P. Neurophysiology of cancer pain. Cancer Control 2000;7:111-119. 87. Mercadante S. World Health Organization Guidelines: Problem Areas in Cancer Pain Management. Cancer Control
1999;6:191-197. 88. Lesage P, Portenoy RK. Trends in cancer pain management. Cancer Control 1999;6:136-145. 89. Ellison N, Loprinzi CL, Kugler J, et al. Phase III placebo-controlled trial of capsaicin cream in the management of surgical
neuropathic pain in cancer patients. J Clin Oncol 1997;15:2974-2980.90. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the management of neuropathic pain due to
spinal cord pathologies. Medical Progress 2006;33:423-430.91. McDonald JW, Sadowsky C. Spinal-cord injury. Lancet 2002;359:417-425.92. Management of Cancer Pain. Rockville, Md: Dept of Health and Human Services, Public Health Service, Agency for Health
Care Policy and Research; 1994. DHHS Publication AHCPR 94-0593.93. Warms CA, Turner JA, Marshall HM, et al. Treatments for chronic pain associated with spinal cord injuries: many are tried,
few are helpful. Clin J Pain 2002;18:154-163.94. Widerstrom-Noga EG, Turk DC. Types and effectiveness of treatments used by people with chronic pain associated with
spinal cord injuries: influence of pain and psychosocial characteristics. Spinal Cord 2003;41:600-609.95. Ahn SH, Park HW, Lee BS, et al. Gabapentin effect on neuropathic pain compared among patients with spinal cord injury
and different durations of symptoms. Spine 2003;28:341-346.96. Siddall P, Cousins M, Otte A, et al. Pregabalin safely and effectively treats chronic central neuropathic pain after spinal cord
injury. Paper presented at: 11th World Congress on Pain; 21-26 August 2005; Sydney, Australia.
32

97. To TP, Lim TC, Hill ST, et al. Gabapentin for neuropathic pain following spinal cord injury. Spinal Cord 2002;40:282-285.98. Tai Q, Kirshblum S, Chen B, et al. Gabapentin in the treatment of neuropathic pain after spinal cord injury: a prospective,
randomized, double-blind, crossover trial. J Spinal Cord Med 2002;25:100-105.99. Levendoglu F, Ogun CO, Ozerbil O, et al. Gabapentin is a first line drug for the treatment of neuropathic pain in spinal
cord injury. Spine 2004;29:743-751.100. Eide PK, Stubhaug A, Stenehjem AE. Central dysesthesia pain after traumatic spinal cord injury is dependent on N-methyl-
D-aspartate receptor activation. Neurosurgery 1995;37:1080-1087.101. Attal N, Guirimand F, Brasseur L, et al. Effects of IV morphine in central pain: a randomized placebo-controlled study.
Neurology 2002;58:554-563.102. Kvarnstrom A, Karlsten R, Quiding H, et al. The analgesic effect of intravenous ketamine and lidocaine on pain after spinal
cord injury. Acta Anaesthesiol Scand 2004;48:498-506.103. Klepstad P, Borchgrevink P, Hval B, et al. Longterm treatment with ketamine in a 12-year-old girl with severe neuropathic
pain caused by a cervical spinal tumor. J Pediatr Hematol Oncol 2001;23:616-619.104. Siddall PJ, Taylor DA, Cousins MJ. Classification of pain following spinal cord injury. Spinal Cord 1997;35:69-75.105. Devulder J, Crombez E, Mortier E. Central pain: an overview. Acta Neurol Belg 2002;102:97-103.106. Fenollosa P, Pallares J, Cervera J, et al. Chronic pain in the spinal cord injured: statistical approach and pharmacological
treatment. Paraplegia 1993;31:722-729.107. Siddall PJ, Molloy AR, Walker S, et al. The efficacy of intrathecal morphine and clonidine in the treatment of pain after
spinal cord injury. Anesth Analg 2000;91:1493-1498.108. Herman RM, D’Luzansky SC, Ippolito R. Intrathecal baclofen suppresses central pain in patients with spinal lesions. A pilot
study. Clin J Pain 1992;8:338-345.109. Loubser PG, Donovan WH. Diagnostic spinal anaesthesia in chronic spinal cord injury pain. Paraplegia 1991;29:25-36.110. Laffey JG, Murphy D, Regan J, et al. Efficacy of spinal cord stimulation for neuropathic pain following idiopathic acute
transverse myelitis: a case report. Clin Neurol Neurosurg 1999;101:125-127.111. Mekhail NA, Aeschbach A, Stanton-Hicks M. Cost benefit analysis of neurostimulation for chronic pain. Clin J Pain
2004;20:462-468.112. Rapson LM, Wells N, Pepper J, et al. Acupuncture as a promising treatment for below-level central neuropathic pain: a
retrospective study. J Spinal Cord Med 2003;26:21-26.113. Sindou M, Mertens P, Wael M. Microsurgical DREZotomy for pain due to spinal cord and/or cauda equina injuries: long-
term results in a series of 44 patients. Pain 2001;92:159-171.114. Falci S, Best L, Bayles R, et al. Dorsal root entry zone microcoagulation for spinal cord injury-related central pain: operative
intramedullary electrophysiological guidance and clinical outcome. J Neurosurg Spine 2002;97:193-200.115. The Multidisciplinary Panel on Neuropathic Pain. Recommendations for the Management of Complex Regional Pain
Syndrome. Medical Progress 2009;36:421-427.116. International Coalition on Neuropathic Pain. Changing the Course of Neuropathic Pain Management: An ICNeP Program.
ICNeP; 2003.117. Albazaz R, Wong YT, Homer-Vanniasinkam S. Complex regional pain syndrome: A review. Ann Vasc Surg 2008;22:297-
306.118. Harden RN. Complex regional pain syndrome. Br J Anaesth 2001;87:99-106. 119. Yung Chung O, Bruehl SP. Complex regional pain syndrome. Curr Treat Options Neurol 2003;5:499-511.120. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-227.121. Max MB. Thirteen consecutive well-designed randomised trials show that antidepressants reduce pain in diabetic neu-
ropathy and postherpetic neuralgia. Pain Forum 1995;4:248-253. 122. Van de Vusse AC, Stomp-van den Berg SG, Kessels AH, et al. Randomised controlled trial of gabapentin in Complex
Regional Pain Syndrome type 1. BMC Neurol 2004;4:13.123. Gilron I, Flatters SJ. Gabapentin and pregabalin for the treatment of neuropathic pain: a review of laboratory and clinical
evidence. Pain Res Manag 2006;11:16A-29A.124. Rho RH, Brewer RP, Lamer TJ, et al. Complex regional pain syndrome. Mayo Clin Proc 2002;77:174-180.125. Taylor RS, Van Buyten JP, Buchser E. Spinal cord stimulation for complex regional pain syndrome: a systematic review of
the clinical and cost-effectiveness literature and assessment of prognostic factors. Eur J Pain 2006;10:91-101.126. Kemler MA, Barendse GA, van Kleef M, et al. Spinal cord stimulation in patients with chronic reflex sympathetic dystrophy.
N Engl J Med 2000;343:618-624.127. Mailis A, Furlan A. Sympathectomy for neuropathic pain. Cochrane Database Syst Rev 2003;(2):CD002918.


















