Molecular Pathology in Surgical Pathology Alan Brown, MD Resident - Pathology – UT HSC May 20,...
57
Molecular Pathology in Surgical Pathology Alan Brown, MD Resident - Pathology – UT HSC May 20, 2013
-
Upload
aldous-flynn -
Category
Documents
-
view
227 -
download
4
Transcript of Molecular Pathology in Surgical Pathology Alan Brown, MD Resident - Pathology – UT HSC May 20,...

Molecular Pathology in Surgical Pathology
Alan Brown, MDResident - Pathology – UT HSC
May 20, 2013

Disclosures• No financial disclosures • No reference bias disclosures
• I am currently a Resident in Pathology• I am not Board Certified in Molecular Genetics

Goals & Objectives1. Appreciation of scenarios requiring genetic testing
2. Realization of the potential impact of Molecular pathology results
3. Better ability to properly handle tissue and interpret results
4. Review and understand genetic testing methods
5. Understanding of major testing methods in Molecular Pathology
6. Provide clear and applicable situations requiring genetic testing
7. Improved confidence in genetic testing knowledge to allow for better management and efficiency

Chapters
1. Justification of Genetic Testing
2. Basics of genetic testing1. Cytogenetic versus Molecular Genetics
2. Uses of Genetic Testing
3. Case Scenario #1
3. “Red flag” situations when genetics should be considered
4. Challenges of molecular genetic testing1. Pre-analytical
2. Post-analytic
3. Interpreting Test Results
5. Review – Case Scenario #2 and Questions

Justification• Why is this important The ancillary tools available to surgical
pathology (immunohistochemistry, molecular pathology and cytogenetics) can allow for better diagnosis and classification of numerous pathologies that can have resounding impacts on eventual prognosis and treatment of the patient.
• Will I actually see these things? Depending on the clinical setting and size of a surgical pathology laboratory, the frequency of uncommon or nebulous neoplasms may be limited resulting in irregular secondary testing or required consultation.
• This lecture seeks to clarify situations requiring molecular genetic testing and provide straightforward procedure-based methods to ensure proper understanding, handling and interpretation of results.

Modern Pathology – Patient Centered
Patient
Surgical Patholog
y
Chemistry /
Serology
Cytogenetics
Molecular
Genetics
Immuno histoche
mical stains
Specialty
Consultants

1. Evolution of Ancillary Testing2. Cytogenetics versus Molecular genetics3. Applications of Genetic Testing4. Case Scenario #1
Basics of Genetic Testing

Key Points to Molecular Pathology (Henry’s Laboratory Methods – 22nd ed. – Unger ER, Bluth MH, Pincus MR)
• The revolution in molecular biology has had a profound impact on pathology.
• Techniques can identify very small quantities of DNA that can be useful in numerous scenarios.
• The Human Genome Project has allowed for the development of high-throughput and highly sensitive genetic methods.

Appreciation of Pathology (Evolution of Ancillary Testing)
1. Disease Stigmata
2. Gross Evaluation
3. Histology/Cytology
4. Special Stains (proteins, vacuoles, granules)
5. Immunohistochemical Stains (hybridomas)
6. Cytogenetics / Karyotyping
7. FISH Probes
8. PCR Probes
9. Genome Sequencing

Types of DNA MutationMutation Description Disease
Point Single base pair substitution Sickle Cell Anemia
Deletion / Insertion Subtraction or deletion of codon
Becker Muscular Dystrophy(less severe)
Frameshift Subtraction or deletion of amino acid resulting in reading frame shift
Duchenne Muscular Dystrophy
Amplification / Trinucleotide Repeat
Increased repeat sequences of microsatellite DNA which can block gene expression
Fragile X syndrome, Huntington’s disease
Translocation / Inversion Chromosomal exchange of large chromosomal segments resulting in a “hybrid” gene
Chronic myelogenous leukemia
*Adapted from Henry’s Laboratory Methods 22nd ed. – Steinau M, Piper MA, Unger ER - Table 65-4

Methods of Nucleic Acid Analysis
1. Electrophoresis
2. Nucleic acid hybridization (annealing a probe)1. Southern Blot (out-dated)
2. In-situ Hybridization (FISH)
3. DNA Microarray Chip (grid oligonucleotides)
3. Amplification (PCR)
4. Polymorphism Assays (SNPs)
5. Genome/Gene Sequencing 1. Sanger (Human Genome Project)
2. Direct Specific Gene Sequencying (HPV, BRCA)
3. Next-generation ($1000 genome)
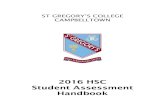
What is the difference between cytogenetics & molecular genetics?
CYTOGENETICS / FISH• Identification of chromosomal
abnormalities (translocations, deletions, inversions, duplication, triploidy)
• Focus on the numerical and structural appearance of chromosomes.
• Used in conjunction with FISH probes to identify “smaller” chromosomal anomalies.
PCR / Amplification• Uses specific “probes” to isolate
and amplify targeted genes• Extremely sensitive even with
very small amounts of available DNA.
• Quantitative and real time providing “mutation burden”

18-23 hrs 1-2 hrs
Chromosome Analysis – BasicsCell Cycle
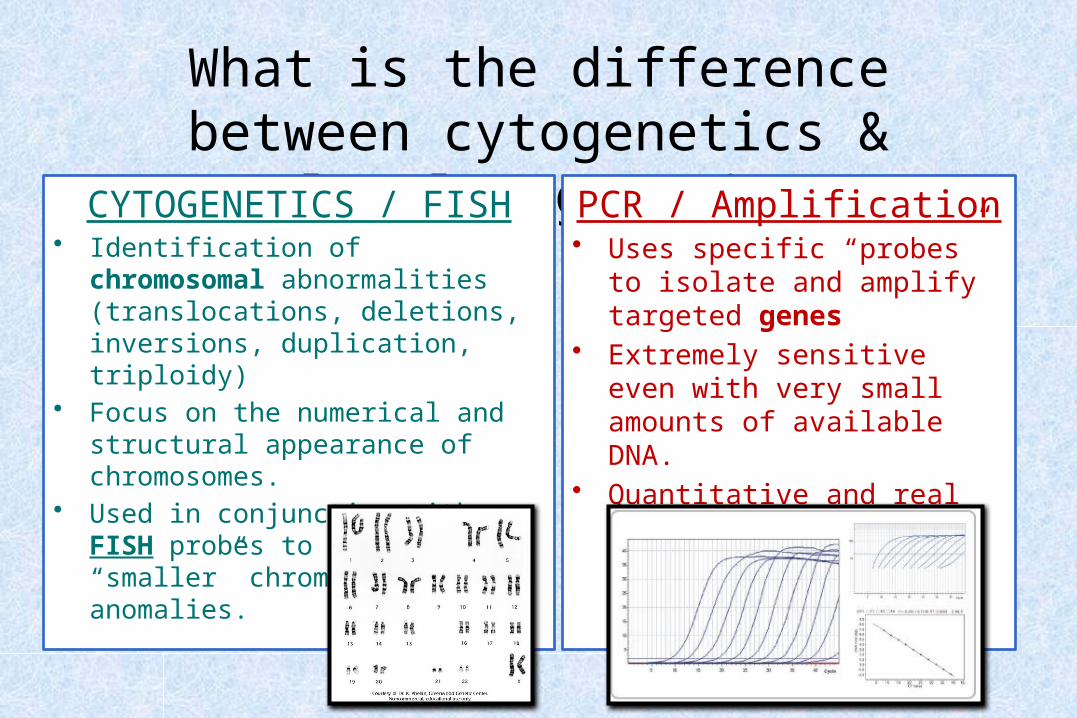
CYTOGENETICS
CYTOGENETICS

Fluorescence In Situ Hybridization (FISH)
• sensitivity of molecular techniques• specificity of cytogenetic techniques• increased resolution• exceptional tool for diagnosis
• in Cancer Cytogenetics
FISH invaluable because of interphase analysisTissue viability not an issue (fresh or formalin)
FISH

Types of FISH Probes
1. Enumeration / deletion -5q, -7q, tri8
– Usually paired with centromere marker (D00Z1)
2. Fusion BCR-ABL, PML-RARA, IGH-BCL2
3. Breakapart MLL (11q), ERG (21), EWSR1(22)
FISH

Fluorescence In Situ Hybridization (FISH) Fusion probes Fusion Negative
Fusion Positive
FISH

Fusion or Breakapart? Normal Abnormal
*Images courtesy of Dr. Velagaleti, UTHSCA Cytogenetic
FISH

Fusion or Breakapart? Normal Abnormal
*Images courtesy of Dr. Velagaleti, UTHSCA Cytogenetic
FISH

Polymerase Chain Reaction (PCR)• Simple in vitro chemical reaction that permits amplification
of essentially limitless quantities of targeted nucleic acid sequences.
• Uses a “probe” to select and isolated desired sequence• Steps:
1. Denaturation
2. Annealing
3. Extension / Amplification
• Types:– Reverse Transcriptase (RNA)– Real-time Quantitative– Multiplex
PCR

Real-time Quantitative Polymerase Chain
Reaction
(RQ-PCR)
PCR

RQ-PCR DetectionPCR
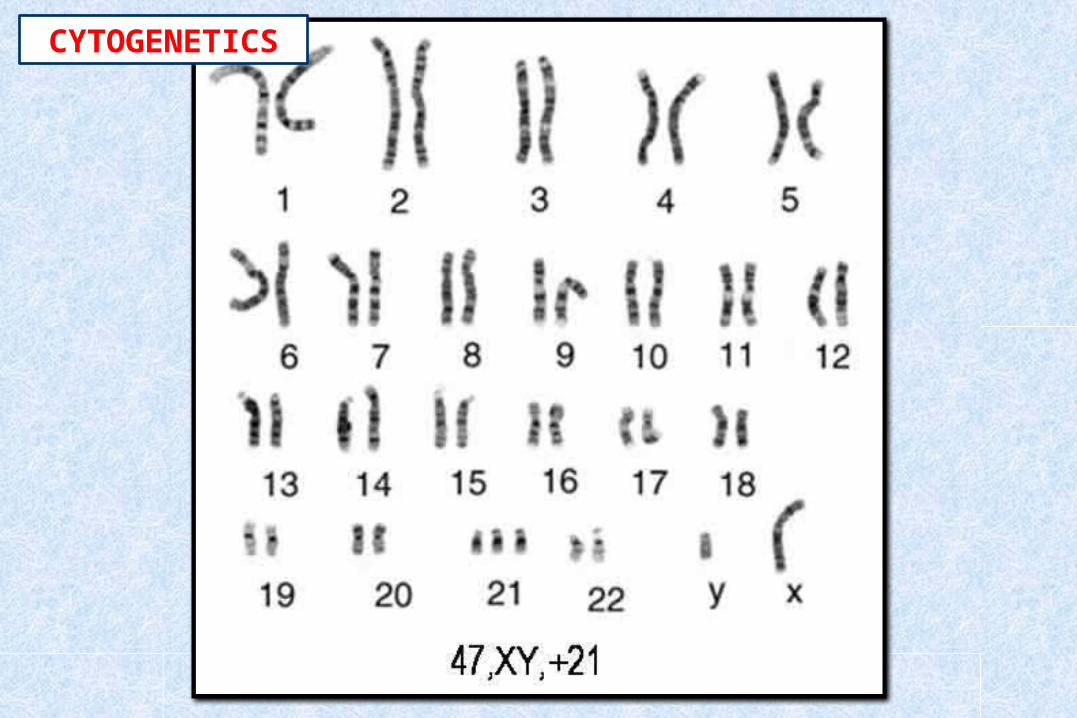
Uses of Genetic Testing
Diagnosis Prognosis Treatment
ClassificationMonitoring of
ProgressionPrediction of
response
Response to treatment
Pre-symptomatic risk assessment
Pharmacogenomics
Tier
1
2
3

Now, many situations seek elucidation by both cytogenetics and molecular genetics. This is particularly common in
Hematopathology and Bone/Soft tissue Tumors.

Scenario #1 - A Straightforward Case
• 8 year old boy with “nodular” index finger mass – at the distal phalangeal joint– no biopsy; preoperative diagnosis: benign– following trauma 4 months prior– 2 x 1.5 x 1.2 cm – white-tan irregular rubbery tissue
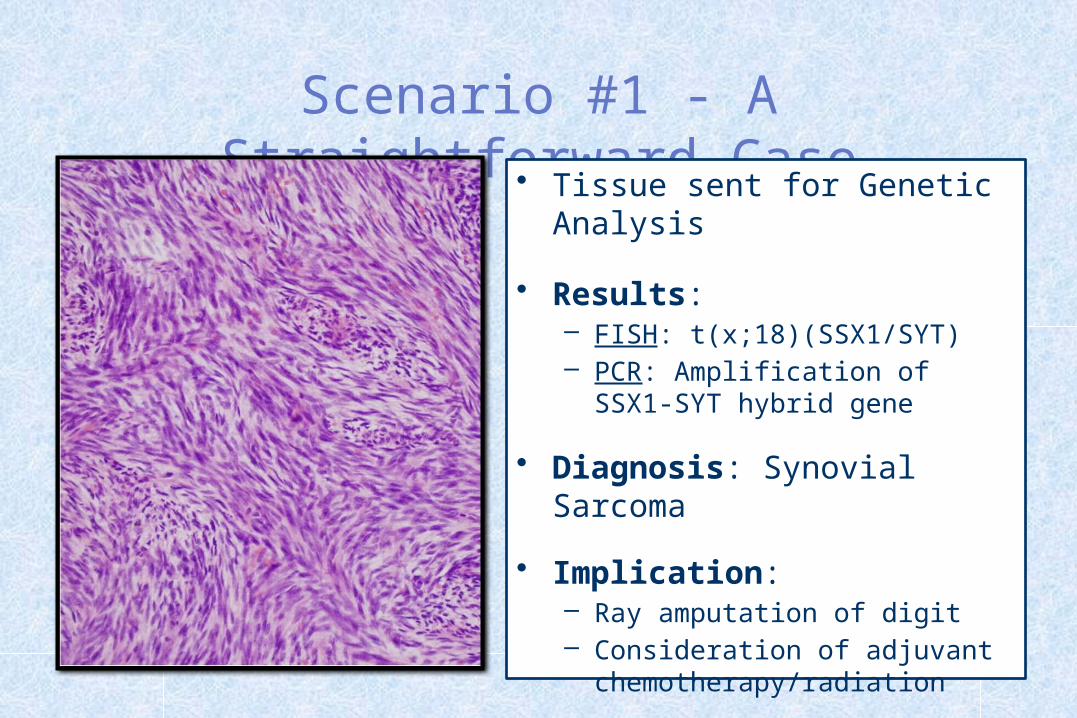
Scenario #1 - A Straightforward Case
• Tissue sent for Genetic Analysis
• Results:– FISH: t(x;18)(SSX1/SYT) – PCR: Amplification of SSX1-SYT
hybrid gene
• Diagnosis: Synovial Sarcoma
• Implication:– Ray amputation of digit – Consideration of adjuvant
chemotherapy/radiation

1. Lung – Small cell versus Non-small cell carcinomas2. Hematolymphoid – Almost all types3. Gynecologic – Breast, Ovary, Uterus Malignacy4. Fetal – Chromosomal and Inherited Conditions5. Brain & Neuroendocrine
**Molecular genetics will gradually expand into almost every surgical specimen as “personalized medicine” become more prevalent.**
“Red Flag” Situtation(When genetic testing should be considered and why it’s useful)

The usual scenario. • It’s a busy day in surgical pathology and frozen specimens have
been coming in all day. • Nearing 5PM, OR#1 unexpectedly delivers an infiltrative,
heterogeneous shoulder girdle mass • Of course, there is no biopsy and the patient has never been
seen at your hospital • The exhausted surgeon shrugs out a few possible preoperative
diagnoses, “Ummm, maybe..”:– Sarcoma– Fibromatosis / Desmoid tumor– Peripheral nerve sheath tumor
• What are we going to do?

The usual scenario. • Guess what! Genetic testing may be helpful:
– Most sarcomas have well-documented, specific genetic anomalies– Aggressive fibromatosis (APC, numerous atypical gene expressions)– Malignant peripheral nerve sheath tumor (t(X;19); genetic not very helpful)
• How should we save tissue? 1. Live culture (Cytogenetics) RPMI or Cell Culture Nutrient Preservative
2. Molecular (PCR) Snap fresh Fresh tissue
3. FISH and some Molecular Formalin-fixed paraffin embedded
**I recommend collection in all 3 formats if there is any confusion**

The usual scenario. 1.) RPMI 2.) SNAP
Freeze3.)Formalin
**ONLY IF THERE IS SUFFICIENT TISSUE – ALWAYS GET TISSUE FOR FORMALIN**

Generally Speaking…• Rules of thumb:
1. Consider saving tissue for Cytogenetics and Molecular testing when the possible diagnosis is: 1. Hematolymphoid, all types
2. Sarcoma and Stromal tumors (GISTs), all types
3. Brain / CNS, most types
4. Breast / Gyn, particularly Ashkenazi Jewish, 2+ close relative, <40 yoa
5. Suspected familial or inherited syndrome presentation
6. Carcinoma in very young, familial, very aggressive or atypical
2. Only collect tissue for ancillary testing if there is sufficient tissue available (ie – lung biopsies, testing on embedded tissue)
3. If unsure OR rushed, collect fresh tissues JUST IN CASE as it can always be fixed later.

A few examples for emphasisDO NOT MEMORIZEUseful Genetic Markers Expand Daily
Gradually Inching into Every Organ SystemAwareness is important
Knowledge of all mutations is impossible
WHO Classification of myeloid neoplasms and acute leukemia
Myeloproliferative neoplasms (MPN/MPD) Myeloid and lymphoid neoplasms associated with
eosinophilia and abnormalities of PDGFRA,PDGFRB and FGFR1
Myelodysplastic syndromes (MDS) Acute myeloid leukemia (AML) and related neoplasms B-lymphoblastic leukemia/lymphoma T-lymphoblastic leukemia/lymphoma
Vardiman et al., Blood 114: 937-951, 2009

CLL (8)6q deletion D6Z1 / MYBtrisomy 12 D12Z111q deletion D11Z1 / ATMt(14;18) IGH / BCL214q rearrange IGH17p deletion p53t(11;14) CCND1 / IGH13q deletion RB1 / CTB-163C9
Multiple Myeloma (6)11q deletion D11Z1 / ATM17p deletion p5313q deletion RB1 / CTB-163C9t(11;14) CCND1 / IGHt(4;14) FGFR3 / IGHhyperdiploidy ATM / MAF / FGFR3
AML/MDS (8)-5q del / mono 5 TAS2R1 / EGR1-7q del / mono7 RELN / TESt(8;21) ETO / AML111q rearrange MLLt(15;17) PML / RARAinv(16) MYH11 / CBFB17p del p5320q del / mono20 MYBL2 / PTPRT
8q rearrange cMYC-9p del p16 / D9Z3hyperdip – chr. 4 FIP1L1 / CHIC2 / PDGFRAhyperdip – chrs. 10 & 17 D10Z1 / D17Z1t(12;21) ETV6 / AML111q rearrange MLLt(9;22) ABL1 / BCR14q rearrange IGH
ALL (8)


Solid Tumors Fusions to Remember
• Alveolar Rhabdomyosarcoma - t(2;13) t(1;13)
• Ewing’s Sarcoma - t(11;22)(EWS – FLI1)• Synovial Sarcoma - t(X;18)(SSX1 - SYT)• Myxoid liposarcoma – t(12;16)• GIST – KIT / PDGFRA (Chrom4) – High risk
and potential response to Gleevec
• -

Inherited Breast CancersAssociated syndrome Gene Chromosome
site% of all cases Cancer risk
HBOC BRCA1 17q21 3% Ovary, fallopian tube, male breast, pancreas, prostate*, possibly cervix and uterus
HBOC BRCA2 13q12-132 Ovary, fallopian tube, male breast, pancreas,
prostate*, possibly biliary tract, stomach, and melanoma
Li-Fraumeni P53 / CHEK2 17p13.1 1 Soft tissue and bone sarcomas, leukemia, brain, adrenocortical malignancies
Cowden PTEN 10q22-231 Hamartomas (papillomas of the lips and mucous
membranes, acral skin keratoses, trichillemomas of skin), uterus, non-medullary thyroid
Hereditary Diffuse Gastric Cancer Syndrome
CDH1 16q22.1
<1
Lobular breast cancer, diffuse gastric cancer
Peutz-Jeghers STK11 19p13.3<1 Hamartomatous gastrointestinal tract polyps, small
bowel, stomach, colorectal, pancreas, lung, uterus, ovary
HNPCC / Muir-Torre
MMR (MLH1>MSH2>MSH6)
Mismatch repair genes / Microsatellite instability
<1Colon, endometrial, ovarian, breast, gastric, urothelial
Sporadic - - 90%

BRCA1/2 Genetic Testing• BRCA mutations are seen in multiple malignancies (including breast,
ovarian, pancreatic, colon, uterine, and prostate)
• BRCA-1 and 2 Overall 80% female risk of breast CA; 50% risk of ovarian CA
• Over a thousand different mutations in BRCA1 and BRCA2 have been reported.
• Complete gene sequencing to exclude most known mutations (~$3000)
• Testing includes sequencing and five large (most common) rearrangements.
• Full sequencing testing is provided in the United States by only one commercial laboratory, Myriad Genetic Laboratories®. (DISPUTED)

The Philadelphia Chromosomet(9;22)(q34;q11.2)
Gleevec (Glivec or STI-571)• Constitutively activated kinase plays a vital role in CML
• STI-571 (signal transduction inhibitor) blocks the tyrosine kinase activity of ABL
• STI-571 inhibited cell proliferation and reversed the clinical and hematological abnormalities
• Effective in both chronic phase & blast crisis
NEJM 2001: 344: 1084-1086, Editorial

Potential Imitinib Responders
1. CML– t(9;22) (ABL/BCR) – (not the same segment as ALL)
2. Hypereosinophilic syndrome – PDGFR/CHIC2/FIPIL1
– del 4q22 or t(4;var) – PDGFRA/CHIC2– del 8p11 or t(8;var) – FGFR1 – t(5;12) – PDGFRB/ETV6

Drug Therapeutic Area Biomarker Label Sections
Abacavir3 Antivirals HLA-B*5701 Boxed Warning, Contraindications, Warnings and Precautions, Patient Counseling Information
Ado-Trastuzumab Emtansine4 Oncology ERBB2 (HER2) Indications and Usage, Warnings and Precautions, Adverse Reactions, Clinical Pharmacology, Clinical Studies
Aripiprazole5 Psychiatry CYP2D6 Clinical Pharmacology, Dosage and Administration
Arsenic Trioxide6 Oncology PML/RARα Boxed Warning, Clinical Pharmacology, Indications and Usage, Warnings
Atomoxetine7 Psychiatry CYP2D6 Dosage and Administration, Warnings and Precautions, Drug Interactions, Clinical Pharmacology
Atorvastatin8 Metabolic and Endocrinology LDL receptor Indications and Usage, Dosage and Administration, Warnings and Precautions, Clinical Pharmacology, Clinical Studies
Azathioprine9 Rheumatology TPMT Dosage and Administration, Warnings and Precautions, Drug Interactions, Adverse Reactions, Clinical Pharmacology
Boceprevir10 Antivirals IL28B Clinical Pharmacology
Brentuximab Vedotin11 Oncology CD30 Indications and Usage, Description, Clinical Pharmacology
Busulfan12 Oncology Ph Chromosome Clinical Studies
Capecitabine13 Oncology DPD Contraindications, Precautions, Patient Information
Carbamazepine14 Neurology HLA-B*1502 Boxed Warning, Warnings and Precautions
Carisoprodol15 Musculoskeletal CYP2C19 Clinical Pharmacology, Special Populations
Carvedilol16 Cardiovascular CYP2D6 Drug Interactions, Clinical Pharmacology
Celecoxib17 Analgesics CYP2C9 Dosage and Administration, Drug Interactions, Use in Specific Populations, Clinical Pharmacology
Cetuximab (1)18 Oncology EGFR Indications and Usage, Warnings and Precautions, Description, Clinical Pharmacology, Clinical Studies
Cetuximab (2)19 Oncology KRAS Indications and Usage, Dosage and Administration, Warnings and Precautions, Adverse Reactions, Clinical Pharmacology, Clinical Studies
Cevimeline20 Dermatology and Dental CYP2D6 Drug Interactions
Chlordiazepoxide and Amitriptyline21 Psychiatry CYP2D6 Precautions
Chloroquine22 Antiinfectives G6PD Precautions
Cisplatin23 Oncology TPMT Clinical Pharmacology, Warnings, Precautions
Citalopram (1)24 Psychiatry CYP2C19 Drug Interactions, Warnings
Citalopram (2)25 Psychiatry CYP2D6 Drug Interactions
Clobazam26 Neurology CYP2C19 Clinical Pharmacology, Dosage and Administration, Use in Specific Populations
Clomipramine27 Psychiatry CYP2D6 Drug Interactions
Clopidogrel28 Cardiovascular CYP2C19 Boxed Warning, Dosage and Administration, Warnings and Precautions, Drug Interactions, Clinical Pharmacology
Pharmacogenomic Biomarkers in Drug Labels

1.) Pre-Analytical2.) Post-Analytical 3.) Interpretation of results
Challenges of Molecular Genetic Testing

Pre-Analytical Challenges1. Failure to recognize need for testing (dumped in formalin)
2. Unfamiliarity with collection procedure (tumor, non-tumor)
3. Improper fixation or processing (in fridge over the weekend)
4. Transportation and reference laboratory (who can you trust)
5. Reimbursement (who’s paying)
Working experience is invaluable but a practice run or workshop can help things
run smoother.
Post-Analytical Challenges1. Positive and Negative results
2. Equivocal or Degraded
3. Delivering genetic information 1. Presymptomatic testing
2. Informed consent
3. Pregnancy termination
4. Potential stigmatization or discrimination
5. Poor prognosis
**Genetic tests should NEVER be ordered
without prior INFORMED consent**

Other Challenges - Promiscuous Genes
Atlas Genet Cytogenet Oncol Hematol, Jan,98

Oncotype DX© The clinician ordering the testing will likely interpret and disclose the results

Genetic Counseling• Genetic testing for hereditary breast cancer should only be
performed after thorough genetic counseling and after signing an informed consent statement. The meaning of positive or negative results should be clearly explained.
• In the United States, most insurance companies will cover 90 percent or more of the costs of commercial BRCA testing in appropriate candidates.
• Even following negative study results, a deleterious mutation could be present in BRCA1 or BRCA2 which cannot detected by available methods.

1. Summary points2. Case Scenario #2 3. Questions
Review of Molecular Genetics

Summary• Molecular pathology will continue to impact the practice of pathology
“Get on the bus before your in the dust!”• Improved diagnostics with growing prognostic and therapeutic applications• Potential source of increased patient involvement and revenue• Gradual paradigm shift from histology-only diagnosis• Increasing burden of testing modalities and results informatics mandates the need
for proactive, knowledgeable laboratory management
• Recall “currently” useful application• Collect tissue if unsure and sufficiently available• Accept the challenges and applications of genetic testing• Stay grounded – It’s only another test.

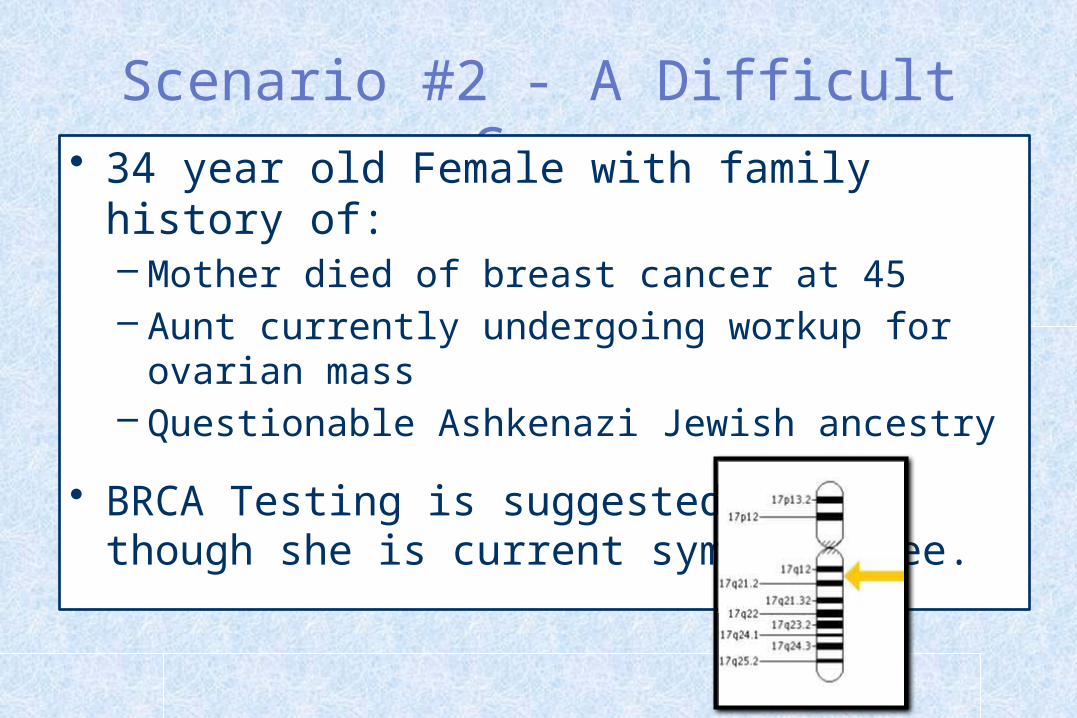
Scenario #2 - A Difficult Case• 34 year old Female with family history of:
– Mother died of breast cancer at 45– Aunt currently undergoing workup for ovarian mass– Questionable Ashkenazi Jewish ancestry
• BRCA Testing is suggested even though she is current symptom free.

Inherited Breast CancersAssociated syndrome Gene Chromosome
site% of all cases Cancer risk
HBOC BRCA1 17q21 3% Ovary, fallopian tube, male breast, pancreas, prostate*, possibly cervix and uterus
HBOC BRCA2 13q12-132 Ovary, fallopian tube, male breast, pancreas,
prostate*, possibly biliary tract, stomach, and melanoma
Li-Fraumeni P53 / CHEK2 17p13.1 1 Soft tissue and bone sarcomas, leukemia, brain, adrenocortical malignancies
Cowden PTEN 10q22-231 Hamartomas (papillomas of the lips and mucous
membranes, acral skin keratoses, trichillemomas of skin), uterus, non-medullary thyroid
Hereditary Diffuse Gastric Cancer Syndrome
CDH1 16q22.1
<1
Lobular breast cancer, diffuse gastric cancer
Peutz-Jeghers STK11 19p13.3<1 Hamartomatous gastrointestinal tract polyps, small
bowel, stomach, colorectal, pancreas, lung, uterus, ovary
HNPCC / Muir-Torre
MMR (MLH1>MSH2>MSH6)
Mismatch repair genes / Microsatellite instability
<1Colon, endometrial, ovarian, breast, gastric, urothelial
Sporadic - - 90%

For non-Ashkenazi Jewish women:
• Two first-degree relatives with breast cancer, one of whom was diagnosed at age 50 or younger
• A combination of three or more first or second-degree relatives with breast cancer regardless of age at diagnosis
• A combination of both breast and ovarian cancer among first and second-degree relatives
• A first-degree relative with bilateral breast cancer
• A combination of two or more first or second degree relatives with ovarian cancer, regardless of age at diagnosis
• A first or second-degree relative with both breast and ovarian cancer at any age
• History of breast cancer in a male relative
For women of Ashkenazi Jewish descent:
• Any first-degree relative (or two second degree relatives on the same side of the family) with breast or ovarian cancer
Recommendations from the United States Preventive Services Task Force on who should be offered genetic
testing for BRCA mutations*
U.S. Preventive Services Task Force. Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: recommendation statement. Ann Intern Med 2005; 143:355.

Scenario #2 - A Difficult Case• She consents to biopsy with BRCA testing• A $3000 complete workup by Myriad, Inc. is
negative. • Due to family history, she remains under close
monitoring and develops
breast cancer 4 years
later that is histologically
BRCA-like.

Scenario #2 - A Difficult Case• Unfortunately, her inherited mutation was most likely
outside of the 5 major sequencing domains reviewed in complete tests
• This will likely become a more common issue as molecular links to neoplasia continue to expand
• Molecular testing cannot replace good patient follow up and traditional gross and histologic evaluation.

References1. Special Thanks to Drs. Fan and Velagaletti, Department of Pathology, UT HSC, San Antonio, TX.
2. McPherson RA, Pincus MR. Henry’s Clinical Diagnosis and Management by Laboratory Methods. 22e. Saunders-Elsevier. Philadelphia, 2011: 1255-1290.
3. Morrissette J, Bagg A. Acute myeloid leukemia: Conventional cytogenetics, FISH, moleculocentric methodologies. Clin Lab Med, 2011; 31: 659-686.
4. Grimwade D, Hills RK, Moorman AV, et al.National Cancer Research Institute Adult Leukaemia Working Group. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010;116:354–65.
5. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58: 71–96.
6. Volpi EV, Bridger JM. FISH glossary: an overview of the fluorescence in situ hybridization technique. Biotechniques 2008;45:385–6.
7. Mertens F, Fletcher CDM, Antonescu CR et al. Clinicopathologic and molecular genetic characterization of low grade fibromyxoid sarcoma and cloning of a novel FUS/CREB3LI fusion gene. Lab Invest 2005; 85:408-415.
8. Wang W L, Evans H L, Meis J M et al. FUS rearrangements are rare in 'pure' sclerosing epithelioid fibrosarcoma. Mod Pathol 2012; 25:846-853.
9. Feero WG, Green ED. Genomics education for health care professionals in the 21st century. JAMA, 2011; 306: 989.
10. Ashley EA, et al. Clinical assessment incorporating a personal genome. Lancet, 2010; 375: 1525.
11. Jones SJ, et al. Evolution of an adenocarcinoma in response to selection by targeted kinase inhibitors. Genome Biol, 2010; 11: R82.
12. National Human Genome Research Institute. The human genome project completion: Frequently asked questions. http://www.genome.gov/11006943; accessed 2/10/13.
13. Roychowdhoury S, et al. A model for pathology and genomics. Sci Transl Med 2011; 3: 111-121.
14. Salari K. The Dawing Era of Personalized Medicine Exposes a Gap in Medical Education. PLoS Medicine 2009; 6: e1000138.

QUESTIONS?