
Pathophysiology of Glomerulonephritis Raj Maganti Anatomic Pathology Resident March 29, 2012.
36
Pathophysiology of Glomerulonephritis Raj Maganti Anatomic Pathology Resident March 29, 2012
-
Upload
estefania-earnest -
Category
Documents
-
view
225 -
download
1
Transcript of Pathophysiology of Glomerulonephritis Raj Maganti Anatomic Pathology Resident March 29, 2012.

Pathophysiology of Glomerulonephritis
Raj MagantiAnatomic Pathology Resident
March 29, 2012

Glomerular diseases Glomerulonephritis - Immune mediated/Infectious/Chemical induced
Clinically manifest as nephrotic syndrome
– Proteinuria (lose more than 3.5 g protein/day)
– Hypoalbuminemia and generalized edema
– Hypercholesterolemia and hyperlipoproteinemia: compensatory hepatic change to restore colloid osmotic pressure
Glomerulopathy
– lacks the cellular inflammatory component.
– Similar clinical manifestations
Glomerulitis: Bacterial (embolic) and viral
Glomerular Amyloidosis
Glomerular Vasculopathy
Glomerular Lipidosis: incidental in dogs; inherited hyperlipoproteinemia
in cats

Anatomy of the Glomerulus
Mesangial Cells
Glomerular Capillary Lumina
Urinary Space
Parietal Epithelial Cells
(Bowman’s Capsule)


2 types of mesangial cells Myofibroblastic type: structural & contractile Phagocytic/inflammatory type
Mesangial cells

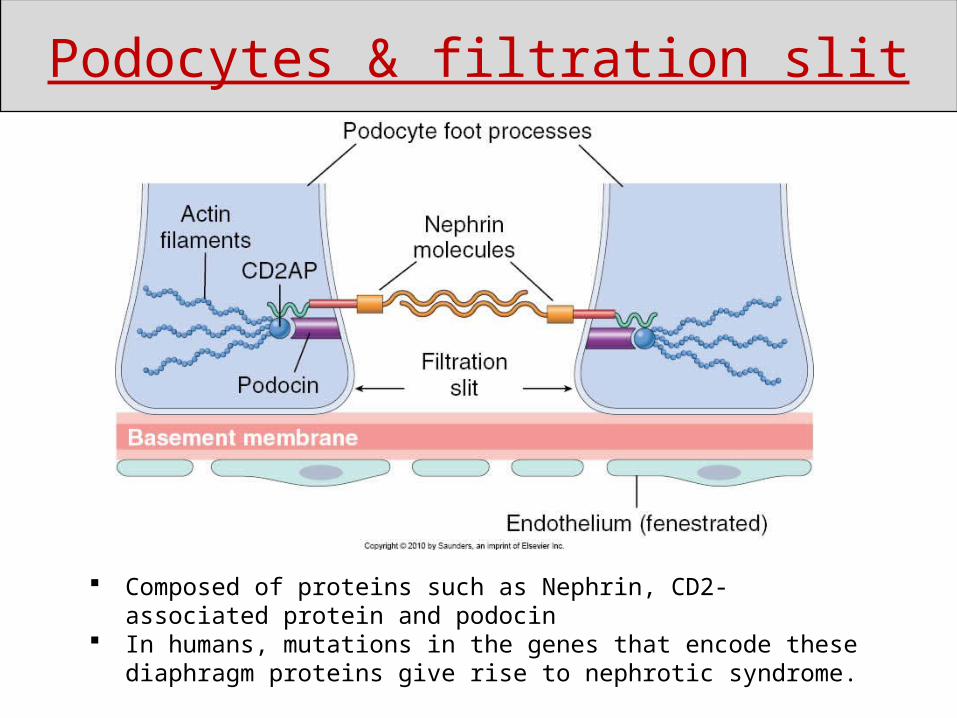
Podocytes & filtration slit
Podocytes & filtration slit
Composed of proteins such as Nephrin, CD2- associated protein and podocin
In humans, mutations in the genes that encode these diaphragm proteins give rise to nephrotic syndrome.

Type IV Collagen
Laminin(glycoprotein)
Heparin Sulfate(negative-charged polyanion)
Lamina rara externa
Lamina densa
Lamina rara interna
capillary lumen
Podocyte foot processes
Endothelial cell
urinary space
Glomerular Basement Membrane (GBM)

Glomerular and Epithelial Cell Injury
Antibodies to epithelial cell antigens, with subsequent toxins, cytokines, or other factors causing injury and detachment of epithelial cells, resulting in protein leakage

Mediators of Glomerular injury

Combination of immune complex with C3 results in solubilization and subsequent removal of the immune complex. Finnish-Landrace lambs: inherited C3 deficiency - severe glomerular disease
Excess antigens stimulate complement fixation. Leukocyte-dependent:Complement fragments (C3a, C5a, C567) - chemotactic for neutrophils.
Leukocyte-independent:C5b-9- terminal membrane attack complex of complement
Stimulate mesangial cells and glomerular epithelial cells to produce chemical mediators (proteases, oxidants, IL-1, PG).
Additional membrane damage through neutrophil release of proteinases, arachidonic metabolites (e.g. thromboxane), and oxidants (esp oxygen derived free radicals and H2O2).
Mediators of Glomerular injury
Neutrophils Infiltrate glomerulus due to immune complex activation & complement
Release C5a and Fc-mediated immune adherance
Release lysosomal enzymes: collagenases, elastases, chymotrypsin like protease, arachidonic acid metabolites, oxygen derived free rads, vasodilator peptides and chemotactic substances for macrophages
Activated macrophages Infiltrate glomerulus due to immune complex activation & complement &
chemotatic substances produced by neutrophils
Release proteases, complement components, chemotactic factors for neutrophils, reactive oxygen metabolites, IL-1, and platelet activating factor.
Monocytes produce a procoagulant factor that activates the extrinsic coagulation pathway.
Mediators of Glomerular injury
Platelets Platelets release arachidonic acid metabolites and growth factors
Interaction of platelets with complement fragments and/or damaged endothelial cells can initiate coagulation, thrombosis, and fibrinolysis.
Antiplatelet agents have beneficial effects in both human and experimental glomerulonephritis
Fibrinogen Leak into Bowman's space and in this region are relatively inaccessible to
fibrinolytic mechanisms.
Consequently fibrin in this location may stimulate epithelial cell proliferation and infiltration of macrophages.
Mediators of Glomerular injury

Immune mediated: Ab-Ag complex & Complement
Infectious: Bacteria and Viruses
Chemicals: Chemotherapeutic agents
Types of glomerulonephritis
2 mechanisms in dogs and cats:Preformed circulating Ag-Ab complexes:
Heymann’s model – anti-rat antibodies were harvested from rabbits and injected into rats
Antigen is trapped in glomerular capillary wall and circulating antibodies form complexes with them (FIP, FeLV, Dirofilaria immitis, SLE, neoplasia)
The 3rd mechanism: Formation of anti-GBM Ab Goodpasture’s syndrome (Humans and NHP) Abs against NC1 (Non-Collagen domain 1) of α3 of collagen
type 4
Immune mediated Glomerulonephritis

Lumpy-Bumpy pattern (Preformed complexes/Trapped antigen
Smooth linear pattern (Anti-GBM antibodies)
Immunflorescence microscopy
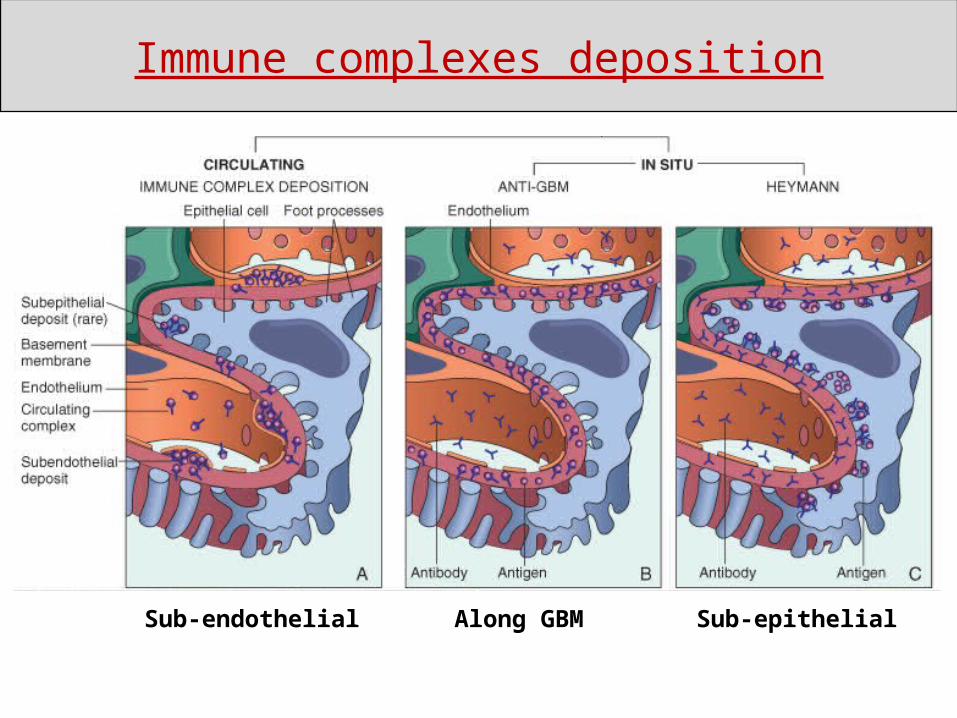
Sub-endothelial Along GBM Sub-epithelial
Immune complexes deposition

Direct injury to glomerular endothelial and epithelial cells
Altered Renal Blood Flow (e.g. cyclosporin A)
Induction of Immune complex formation and inflammation
Some examples: Puromycin aminonucleosideAdriamycinCyclosporine AHistamine receptor antagonistsd-penicillamine andProcainamide
Chemical Induced Glomerular Injury

Morphology of Glomerulonephritis

Glomerulonephritis Chronic Pyelonephritis
Chronic Renal Failure (Interstitial Fibrosis)
Common types of renal disease: gross appearance

The small, white, round foci in the cortex are enlarged glomeruli
Subacute Glomerulonephritis

Membranous GN: characterized by thickened GBM Most common form of immune-complex GN in cats Predominantly subepithelial deposits Bacterial kidney disease of salmonids: Rainbow trouts with
Renibacterium salmoninarum
Proliferative GN: characterized by hypercellularity Proliferation of mesangial cells + influx of WBCs Budgerigar fledging disease (polyomavirus)
Membranoproliferative GN: Combination of thickened GBM and proliferation of mesangial cells Most common form of immune-complex GN in dogs Predominently subendothelial deposits
Histological patterns of Glomerulonephritis

Types of Membranoproliferative Glomerulonephritis
Type I: Subendothelial deposits
type II: Intramembranous dense deposits (dense deposit disease).
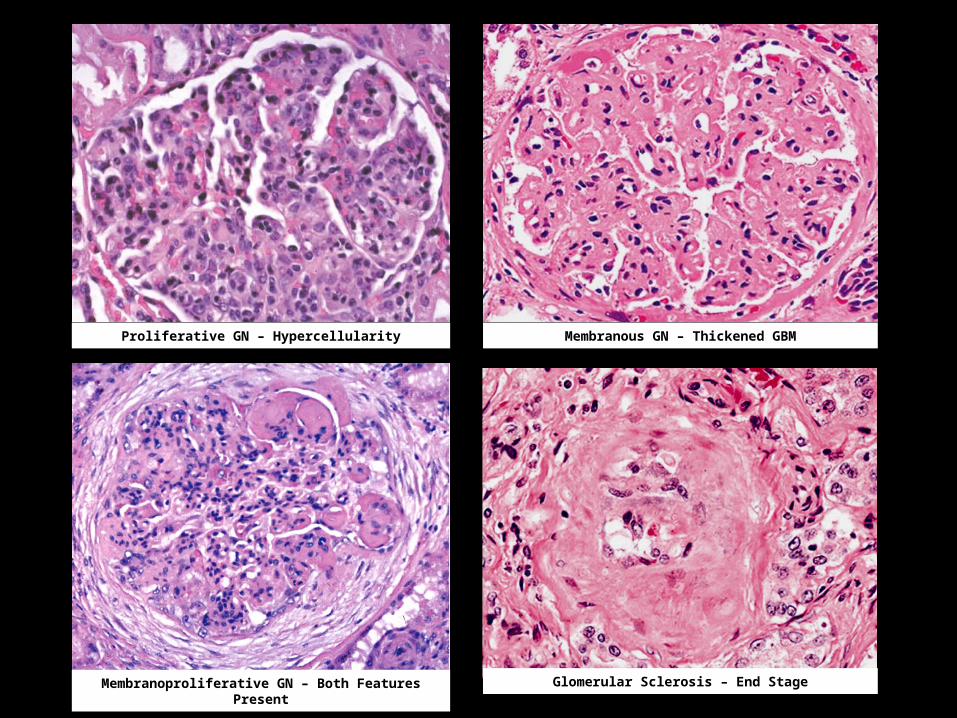
Proliferative GN – Hypercellularity Membranous GN – Thickened GBM
Membranoproliferative GN – Both Features Present Glomerular Sclerosis – End Stage

• Glomerulosclerosis: Fibrosis, hyalinization or scarring of glomeruli resulting in a shrunken, hypocellular and nonfunctional structure.
• Glomerular synechia (synechiae): Adhesion of glomerular tufts to the Bowman's capsule
• Sclerosis/Hyalinization of Bowman’s capsule
• Global GN: Lesion affects the entire glomerulus
• Segmental GN: Lesion involves only a portion of the glomerulus.
Histological changes in Glomerulonephritis
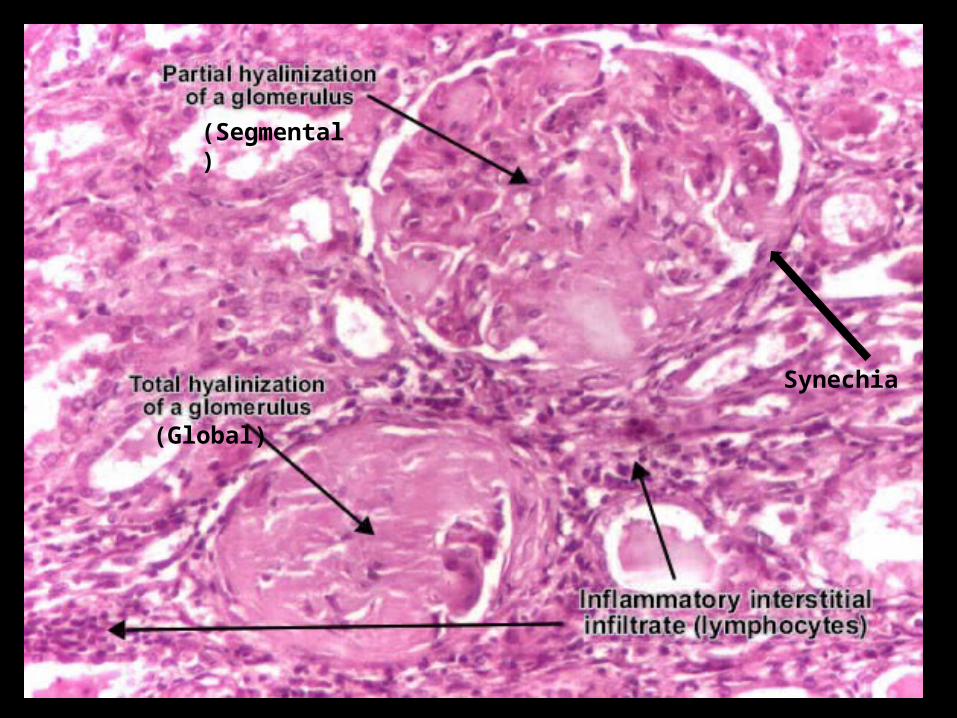
Synechia
(Segmental)
(Global)

Glomerulosclerosis Glomerular hypertrophy -> glomerular hypertension -> injury to
podocyte and endothelial cells -> glomerulosclerosis
Tubulointerstitial fibrosis Injured podocytes cannot proliferate -> gaps in GBM -> proteinuria ->
damaging to tubular epithelium -> tubulointerstitial fibrosis
Additional tubular injury from : Sclerotic glomeruli -> downstream tubular ischemia Close association with glomerular inflammation
Downstream changes of Glomerulonephritis

Embolic (bacterial) Glomerulitis
Hematogenous spread common in neonates and animals with immunosuppression Puppies: Streptococcus sp., E. coli Foals: Actinobacillus equuli Neonatal pigs: Erysipelothrix rhusiopathiae Sheep and Goat: Corynebacterium pseudotuberculosis Calves: Archanobacterium pyogenes; Mannheimia hemolytica

Dogs: Infectious Canine Hepatitis
Horses: Equine Viral Arteritis
Swine: Hog Cholera & Porcine Cytomegalovirus
Avian: Newcastle disease
Direct viral damage to glomerular endothelial cells secondary to viral replication in endothelium
ICH - Intranuclear Viral Inclusions
Viral Glomerulitis

Greyhound: Idiopathic Glomerular & Cutaneous Vasculopathy
The fine white dots in the cortex (both on the capsular and cut surfaces) are glomeruli with extensive glomerular capillary thrombosis.
Necrotic glomerular endothelial cells and glomerular capillary
thrombosis
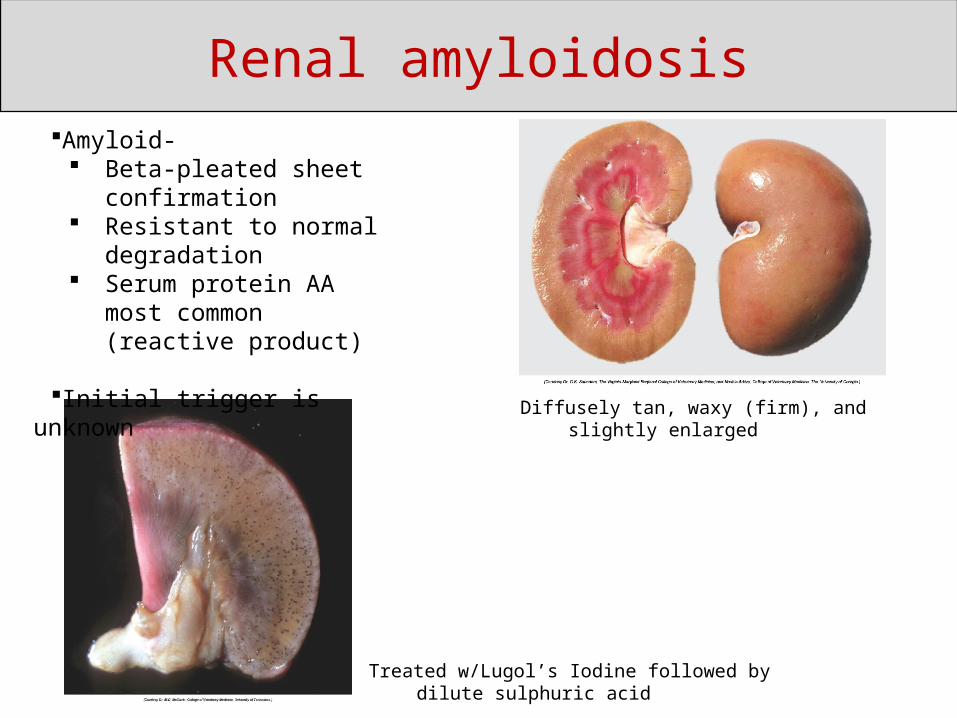
Renal amyloidosis
Diffusely tan, waxy (firm), and slightly enlarged
Amyloid- Beta-pleated sheet
confirmation Resistant to normal
degradation Serum protein AA most
common (reactive product)
Initial trigger is unknown
Treated w/Lugol’s Iodine followed by dilute sulphuric acid

Glomerular amyloidosis
Congo red

Dog - Glomerular Amyloidosis
Glomerular amyloid most common in dogs and cattle. Deposits in mesangium and subendothelial sites.
Medullary deposits in Shar-peis and cats, especially Abyssinian. Therefore, may not see proteinuria.
“The Abyssinian and Shar-pei got married at the pink amyloid wedding. Medussa attended the wedding.”
Cat – Interstitial Amyloidosis
Renal amyloidosis

• Dogs: Membranoproliferative GNSamoyed hereditary glomerulopathy – X-linked trait; mutation in COL4A5 (α5 of type 4 collagen)Other breeds: Bull Terrier (autosomal dominant); English Cocker Spaniel (autosomal recessive); Bernese Mountain; Dobermann; Norwegian ElkhoundBorrelia; dirofilaria; ICH (adenovirus)
• Cats: Membranous GN; FeLV; FIP; FIV
• Horse: Membranoproliferative GN; Equine infectious anemia; streptococcus equi; Herpes virus infections
• Pig: Membranoproliferative GN ; PCV-2
• Ruminants: Membranoproliferative GN; Finnish Landrace sheep – deficiency of complement component C3 – causes impairedComplement-mediated stabilization of immune complexes
Prevalence of Glomerulonephritis

Thanks?



















