MOBILITY/MOBILIZATIO PROCESS - ANG MSC …angmscsociety.org/wp-content/uploads/2014/09/Med...MISSIO...
26
MISSIO READIESS MODULE MSC READIESS SUSTAIMET VERIFICATIO PROGRAM MOBILITY/MOBILIZATIO PROCESS OBJECTIVE Provide an overview of the mobility/mobilization process as it relates to medical personnel. ITRODUCTIO AFI 10-402 provides the primary guidance for mobility planning. AFI 10-403 governs deployment planning. MSC officers must know how to plan for and carry out all degrees of volunteerism, call up, and mobilization. The President of the United States may augment the military with up to 200,000 reservists for up to 270 days, when needed, to meet the requirements of an operational mission. OVERVIEW Mobility Process Mobilization Activation or Recall Process Deactivation REFERECES AFH 10-416 Personnel Readiness and Mobilization AFI 10-402 Mobilization Planning AFI 10-403 Deployment Planning AFI 36-507 Mobilization of the Civilian Workforce AFMAN 10-401 Operation Plan and Concept Plan Development and Implementation AFRCI 10-404 Air Force Reserve Command (AFRC) Unit Notification and Assembly Procedures PRESETATIO A. Mobility Process Mobility refers to meeting deployment requirements. Requirements for mobilization include both personal and mission-specific details that must be prepared for in advance. Examples of mission requirements include having an adequate amount of personnel trained for handling hazardous cargo, operating unit deployment software, and cargo prep/pallet buildup. Examples of personal items include the following: immunizations, prescription medications, spectacle inserts, ID tags, ID cards, DD Form 93, wills, powers of attorney, dependent care plans, personal and financial matters. The Unit Deployment Manager maintains most of these items in a Personnel Readiness Folder (PRF). Once activated, individuals may be required to process through a mobility line to ensure compliance with the above stated requirements. B. Mobilization Process
-
Upload
doankhuong -
Category
Documents
-
view
216 -
download
0
Transcript of MOBILITY/MOBILIZATIO PROCESS - ANG MSC …angmscsociety.org/wp-content/uploads/2014/09/Med...MISSIO...

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
MOBILITY/MOBILIZATIO� PROCESS OBJECTIVE
Provide an overview of the mobility/mobilization process as it relates to medical personnel. I�TRODUCTIO�
AFI 10-402 provides the primary guidance for mobility planning. AFI 10-403 governs deployment planning. MSC officers must know how to plan for and carry out all degrees of volunteerism, call up, and mobilization. The President of the United States may augment the military with up to 200,000 reservists for up to 270 days, when needed, to meet the requirements of an operational mission. OVERVIEW
• Mobility Process • Mobilization • Activation or Recall Process • Deactivation
REFERE�CES
AFH 10-416 Personnel Readiness and Mobilization AFI 10-402 Mobilization Planning AFI 10-403 Deployment Planning AFI 36-507 Mobilization of the Civilian Workforce AFMAN 10-401 Operation Plan and Concept Plan Development and Implementation AFRCI 10-404 Air Force Reserve Command (AFRC) Unit Notification and Assembly
Procedures PRESE�TATIO�
A. Mobility Process Mobility refers to meeting deployment requirements. Requirements for mobilization include both personal and mission-specific details that must be prepared for in advance. Examples of mission requirements include having an adequate amount of personnel trained for handling hazardous cargo, operating unit deployment software, and cargo prep/pallet buildup. Examples of personal items include the following: immunizations, prescription medications, spectacle inserts, ID tags, ID cards, DD Form 93, wills, powers of attorney, dependent care plans, personal and financial matters. The Unit Deployment Manager maintains most of these items in a Personnel Readiness Folder (PRF). Once activated, individuals may be required to process through a mobility line to ensure compliance with the above stated requirements. B. Mobilization Process

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
Mobilization is the actual process of deploying. With appropriate authority and call up, units may be mobilized within time-frame annotated on the Unit DOC Statement. Mobilization encompasses all activities necessary for the orderly transition of active and Air Reserve Component (ARC) forces from a peacetime to a wartime posture. The War and Mobilization Plan, Volume 6 (WMP-Vol 6), covers this transition. There are four basic phases in the mobilization process: Deployment, Employment, Re-deployment, and Demobilization. The WMP drives the process from the Air Staff level to the unit level. The WMP is a multi-volume Air Force (AF) document that provides Air Staff and Air Force commanders with current policies, forces, and planning factors for conducting and supporting wartime operations. The basic plan portion of WMP-1 addresses the general situation, mission, concept of operations, and execution tasks for Air Forces in regional conflicts. C. Activation or Recall Generally, the nature and imminence of an emergency governs the level of response. There are seven types of activation: Retired Members, Volunteerism, Selective Mobilization, Presidential Selected Reserve Callup, Partial Mobilization, Full Mobilization, and Total Mobilization. Another type of mobilization is called “Push-Pull” Mobilization. It is a method of accelerating the mobilization of selected members of the Pre-trained Individual Manpower (PIM) which includes the Indefinite Ready Reserve, Standby Reserve, and retirees in anticipation of their need to fill wartime requirements. The Push-Pull process is intended to supplement the normal requirements based on the mobilization process and will be employed only when deemed appropriate by the Secretary of the Air Force. Initially, a warning order will be issued from higher HQ staff (could be Air Staff or COCOM) to the Major Command (MAJCOM). The warning order is a “heads-up” that prudent pre-deployment processes, planning and preparation should begin and an actual order is possible in the near future. It is not authority to conduct any movement of personnel or equipment. The authority to deploy is provided in an execution or deployment order, which is based on a tasking list. The tasking list is based upon the the supported COCOM requirement and articulated in a Time-Phased Force and Deployment Document (TPFDD). Unit Recall is the reassembling of a unit personnel. The ability of a commander to recall his or her entire unit members is one of the basic premises for a unit to mobilize and meet its wartime commitments. To accomplish this, a plan must be in place that ensures all assigned personnel will be able to be contacted within the required response time as designated in the mobilization order. The response time could be as early as the time stipulated in the Designed Operational Capability (DOC) Statement for the unit. The wing commander designates the office of primary responsibility for managing and monitoring the recall program. Use a pyramid notification system and include both home and business telephone numbers in the notification roster. It is extremely important to ensure unit members promptly report any changes of their home address or telephone number to the orderly room. Include cellular phone numbers or pager numbers when applicable.

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
D. Deactivation Process When the Secretary of the AF authorizes deactivation of the ARC forces, he/she may delegate that authority to the MAJCOM commanders and agencies. Deactivation processing for ARC assigned unit personnel will be accomplished by the ARC Military Personnel Flight (MPF). Deactivation processing for Individual Mobilization Augmentees (IMA) and PIM members will be accomplished by the Active Duty (AD) MPFs. When ARC personnel are released to their home station and the deactivation date is established, operational control reverts to the ARC MAJCOM and the member's unit commander. Exceptions are if the member has applied for retention on AD for medical hold, personal hardship, or if court martial/UCMJ action is pending. The key to a smooth and successful deactivation is coordination between the following: AD and AFRC MAJCOMs, AF Military Personnel Center (AFMPC), and Air Reserve Personnel Center (ARPC). SUMMARY
The mobility/mobilization process involves four critical processes: (1) Mobility (2) Mobilization (3) Activation/Recall and (4) Deactivation. Each process has been generally defined and more detailed information is available in the above-mentioned references. FORMS
DD Form 93 Identification Tag ACRO�YMS
AF Air Force AD Active Duty AFMPC Air Force Military Personnel Center ARC Air Reserve Component (Air National Guard & Air Force Reserve) ARPC Air Reserve Personnel Center COCOM Combatant Command DOC Designed Operational Capability IMA Individual Mobilization Augmentee MAJCOM Major Command MPF Military Personnel Flight PIM Pre-trained Individual Manpower PRF Personnel Readiness Folder TPFDD Time-Phased Force and Deployment Document UTC Unit Type Code WMP War Mobilization Plan

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
TRAI�I�G
OBJECTIVE
Provide an overview of training requirements for deployment preparation. Also a short discussion of training requirements that may be obtained during deployment as part of expeditionary base requirements.
I�TRODUCTIO�
Air Force Medical Service (AFMS) personnel require highly specialized initial, sustainment, and theater-specific training to respond to varied missions and environments. The following block discusses the training requirements each Air Force (AF) member must have in preparation for expeditionary taskings.
OVERVIEW
• Tier 1 • Tier 2A • Tier 2B • Tier 3 • Tier 4 • Additional Training During Deployment
REFERE�CES
AFI 10-2501 AF Emergency Management Program Planning and Operations AFI 41-106 Medical Readiness Program Management
PRESE�TATIO�
A. Pre-deployment Training Requirements
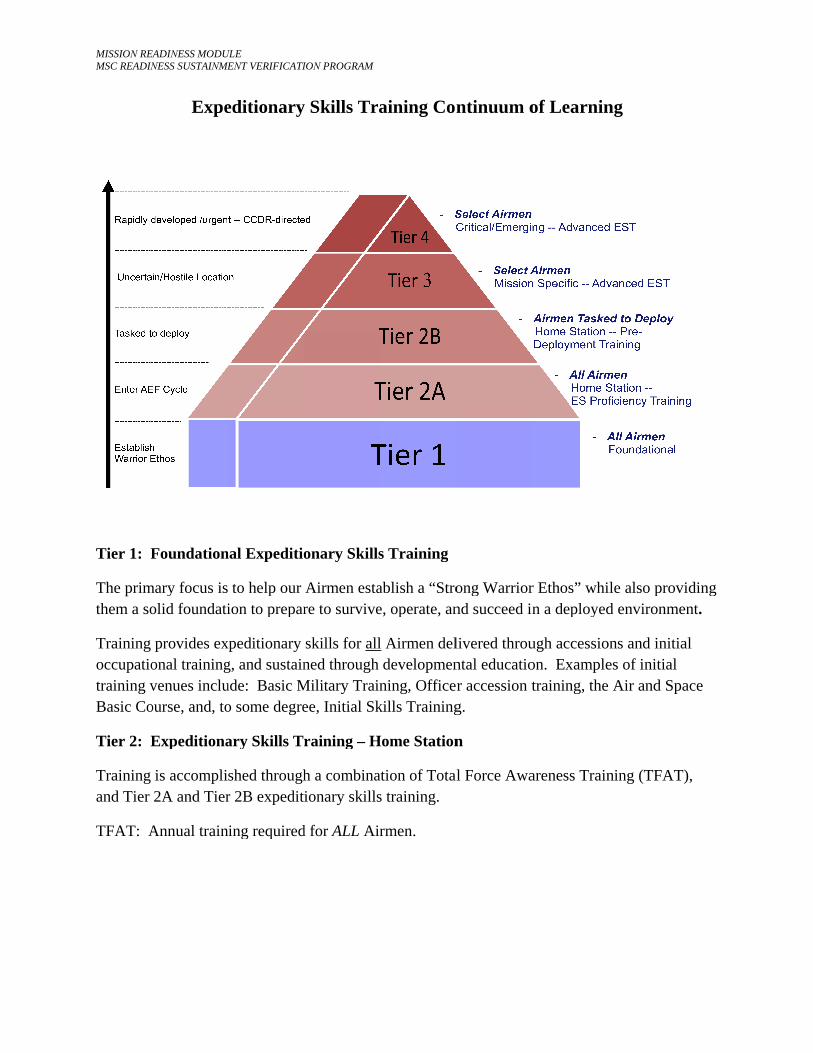
The AFMS has established a Continuum of Learning that describes the tiered approach used to ensure individual members receive and maintain the training they need to succeed and operate in an expeditionary environment. The following diagram depicts this tiered approach:
MISSIO� READI�MSC READI�
Tier 1: Foundational Expeditionary Skills Training
The primary focus is to help our Airmen establish a them a solid foundation to prepare to survive, operate, and succeed in a deployed environment
Training provides eoccupational training,training venues include: Basic Course, and, to some
Tier 2: Expeditionary Skills
Training is accomplished through a combination of Total Force Awareness Training (TFAT), and Tier 2A and Tier 2B expeditionary skills training.
TFAT: Annual training required for
EADI�ESS MODULE�ESS SUSTAI�ME�
Expeditionary Skills Training Continuum of Learning
Foundational Expeditionary Skills Training
mary focus is to help our Airmen establish a olid foundation to prepare to survive, operate, and succeed in a deployed environment
provides exonal training,venues include: ourse, and, to some
Expeditionary Skills
is accomplished through a combination of Total Force Awareness Training (TFAT), 2A and Tier 2B expeditionary skills training.
Annual training required for
ULEE�T VERIFICATIO�
editionary Skills Training Continuum of Learning
nal Expeditionary Skills Training
to help our Airmen establish a ion to prepare to survive, operate, and succeed in a deployed environment
xpeditionary skillsg, and sustained through developmental educationude: Basic Military Training, Officer accession trainingo some degree, Initial Skills Training.
ary Skills Training
shed through a combination of Total Force Awareness Training (TFAT), r 2B expeditionary skills training.
ning required for
IO� PROGRAM
y Skills Training Continuum of Learning
onary Skills Training
Airmen establish a re to survive, operate, and succeed in a deployed environment
skills for allned through developmental education
Military Training, Officer accession trainingee, Initial Skills Training.
raining – H
h a combination of Total Force Awareness Training (TFAT), ionary skills training.
d for ALL Airmen.
aining Continuum of Learning
s Training
ablish a “Strong Warrior Ethos” while also providing e, operate, and succeed in a deployed environment
l Airmen delivered through accessions and initial developmental educationning, Officer accession training
kills Training.
Home Station
ation of Total Force Awareness Training (TFAT), s training.
rmen.
ntinuum of Learning
ong Warrior Ethos” while also providing nd succeed in a deployed environment
livered through accessions and initial ntal educationr accession trainingg.
n
l Force Awareness Training (TFAT),
of Learning
r Ethos” while also providing n a deployed environment
ugh accessions and initial on. Examples of initial training, the Air and Space
areness Training (TFAT),
ng
ile also providing d environment
ons and initial es of initial Air and Space
ning (TFAT),
iding ent.
al
ace
),

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
Tier 2A: Expeditionary Skills (ES) Proficiency Training
All Airmen will maintain ES proficiency by completing AF expeditionary training computer based training (CBTs) when entering their postured AEF vulnerability period
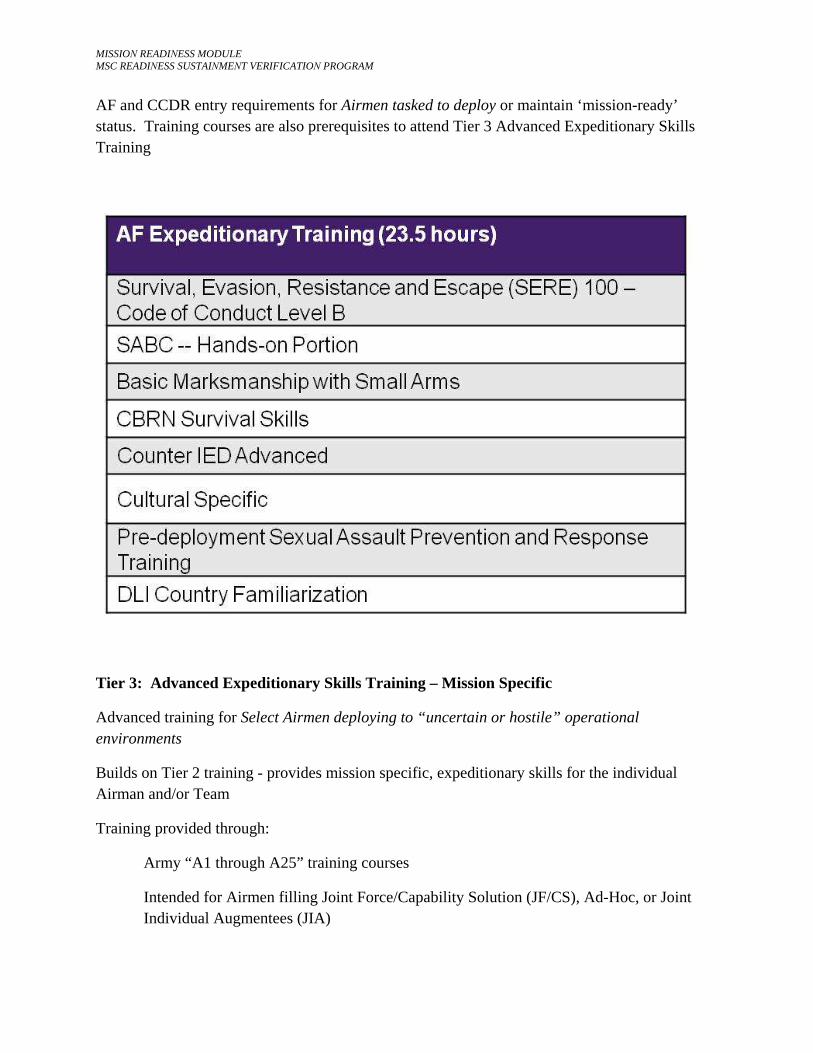
Tier 2B: Home-Station Pre-Deployment Training
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
AF and CCDR entry requirements for Airmen tasked to deploy or maintain ‘mission-ready’ status. Training courses are also prerequisites to attend Tier 3 Advanced Expeditionary Skills Training
Tier 3: Advanced Expeditionary Skills Training – Mission Specific
Advanced training for Select Airmen deploying to “uncertain or hostile” operational environments
Builds on Tier 2 training - provides mission specific, expeditionary skills for the individual Airman and/or Team
Training provided through:
Army “A1 through A25” training courses
Intended for Airmen filling Joint Force/Capability Solution (JF/CS), Ad-Hoc, or Joint Individual Augmentees (JIA)

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
AF Functional-directed training
Currently: Security Forces Regional Training Centers
AF Combat Airman Skills Training (CAST)
Creates an Airman capable of accomplishing his/her AF mission in a ground combat environment
For select deployers -- attendance is dictated by mission and threat/location
Taught at Camp Bullis, Camp Guernsey, and Fort Dix
AETC standardizing CAST curriculum at all 3 locations
B. Training Requirements during Deployment

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
During a deployment, individuals that are assigned to work as the Medical Readiness Officer (MRO) either as a primary responsibility or as an additional duty may be required to supplement their training by completing additional training requirements, particularly if they are assigned as the team chief, or as a member, of the Medical Control Center (MCC) disaster team, or as a member of the Incident Command staff for the base. Additional training CBTs that may be required include:
• Unit Control Center • AF Emergency Response Operations, Introduction • AF Emergency Response Operations, Command and Control
These training courses are all available on the ADLS training system.
SUMMARY
The AFMS has established a Continuum of Learning that describes the tiered approach used to ensure individual members receive and maintain the training they need to succeed and operate in an expeditionary environment. This tiered approach includes: Tier 1: Foundational Expeditionary Skills Training, Tier 2: Expeditionary Skills Training – Home Station which includes proficiency and pre-deployment training, Tier 3: Advanced Expeditionary Skills Training, and for certain Airmen, Tier 4: Combatant Commander Directed training for specific developing missions. Airmen may also be required to complete additional training while deployed to supplement their training skills.
ACRO�YMS
ADLS Advanced Distributed Learning System AEF Air Expeditionary Forces AF Air Force AFMS Air Force Medical Service CAST Combat Airman Skills Training CBRN Chemical, Biological, Radiological, Nuclear CBT Computer Based Training CCDR Combatant Commander C-IED Counter Improvised Explosive Device DLI Defense Language Institute ES Expeditionary Skills EST Expeditionary Skills Training FTX Field Training Exercise GPS Global Positioning System HEAT HMMWV Egress Trainer HRI High Risk of Isolation IED Improvised Explosive Device

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
JF/CS Joint Force/Capability Solution JLI Joint Individual Augmentee LOAC Law of Armed Conflict MCC Medical Control Center MRO Medical Readiness Officer OPSEC Operational Security SABC Self Aid and Buddy Care SERE Survival, Evasion, Resistance, and Escape TFAT Total Force Awareness Training TTP Tactics, Techniques, and Procedures
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
EXPEDITIO�ARY BASE MEDICAL READI�ESS PROGRAM
OBJECTIVE
Provide an overview of Medical Readiness responsibilities in an expeditionary environment.
I�TRODUCTIO�
The Air Force Medical Service (AFMS) provides seamless health service support to AF and combatant commanders and assists in sustaining the performance, health and fitness of every Airman in-garrison and while deployed within the Continental United States (CONUS) or overseas (OCONUS) in support of global operations. This capability is summarized by the phrase ―global medical readiness which includes the full spectrum of medical operations (expeditionary deployment operations, humanitarian assistance, disaster response, and global health engagement to support building partnerships and stability operations). It also includes the necessary planning, training, and readiness support functions (reports, disaster management, and others) associated with these operations.
As with many home station in-garrison medical readiness responsibilities, a Medical Service Corps (MSC) officer in a deployed environment may be assigned the role of Medical Readiness Officer (MRO), either as a primary duty, or as an additional duty, and will have the role of ensuring many of the same tasks and responsibilities as home station are completed in an expeditionary medical treatment facility (MTF).
OVERVIEW
• Deployed Mission • Medical Control Center (MCC) • Emergency Management • Plans • Reports • Exercises, Training, and Recalls • Relationships
REFERE�CES
AFI 10-206 Operational Reporting AFI 10-2501 Air Force Emergency Management (EM) Program Planning and
Operations AFI 10-2604 Disease Containment Planning Guidance AFI 41-106 Medical Readiness Program Management
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
AFMAN 10-2502 Air Force Incident Management System (AFIMS) AFPD 10-25 Emergency Management AFTTP 3-42.32 Home Station Medical Response to Chemical, Biological, Radiological
and Nuclear (CBRN) Events AFTTP 3-42.5 Air Evac (AE) AFTTP 3-42.53 Contingency Air Staging Facility (CASF) AFTTP 3-42.71 Expeditionary Medical Support (EMEDS) PRESE�TATIO�
A. Deployed Mission
The primary mission for medical personnel assigned to a deployed MTF is to provide medical care for the sick and wounded. AF medical personnel spend many hours at home station perfecting their skills in a primary duty responsibility and training to ensure they are ready for any contingency.
AF MTFs worldwide are required to plan for conducting their home station and expeditionary missions simultaneously. This is no different in a deployed environment because the expeditionary base is considered a member’s home station while deployed, but members must also be prepared to forward deploy to other expeditionary locations if ordered by their deployed commander.
Deployment missions may include facility expansion, which can increase the bed capacity of many MTFs to receive and care for large numbers of casualties; patient decontamination; and medical response/support to contingencies confined to the installation or involving Host Nation governments, including Medical Counter-Chemical, Biological, Radiological, Nuclear (MC-CBRN) events. Because of this diverse set of circumstances, the Medical Readiness office can be the hub of mission activities at a deployed MTF, particularly if the Medical Control Center (MCC) is activated on a full-time basis. Inpatient facilities or MTFs with AE or CASF missions will usually maintain MCCs or Medical Readiness Offices that are activated on a full-time basis.
B. Medical Control Center
The MRO is tasked by the Group Commander to establish the MCC. In this capacity the MRO needs to ensure sufficient space, equipment, and checklists/plans are provided to conduct operations. In addition, the MRO will often be tasked to provide the MTF staff with access to classified materials if required.
In a deployed environment communication is key to conducting successful operations; therefore, the MRO should work closely with the local communications squadron (Comm Sq) to ensure guidance is strictly adhered to and equipment items including telephones, at least one secure terminal equipment (STE), computer systems (secure/non-secure), and land mobile radios
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
(LMRs) are available and operational in the MCC. Note: All authorized communications items should be physically in the MCC when feasible. Additionally, LMRs may be used for daily operations but must be identified for MCC use when needed.
As the communication hub for the MTF, the MRO needs to establish, evaluate and maintain the capability to provide and/or arrange for emergency care and transport of casualties resulting from local medical contingencies. An understanding of base resources, Host Nation capabilities and the MTFs treatment and casualty care limits are essential to making this happen. Circumstances can change very quickly in a deployed environment making this information essential to MTF operations.
An important component of the provision of care is the development of installation medical emergency management Memorandum of Understanding/Memorandum of Agreement/Mutual Aid Agreements (MOU/MOA/MAAs) with Joint Service partners and Host Nation agencies to ensure all medical capabilities necessary to fully execute all installation plans are included. The MRO has a major role in the development of these agreements and should ensure thorough coordination of agreements through the Base Legal Office and other specified base units.
C. Emergency Management
With the uncertainties that encompass the deployed environment, EM is an important component in expeditionary MTF operations. A comprehensive EM program will ensure the MRO and the MTF staff in general are prepared to respond to any contingency that might occur. To maintain the capability to respond to all emergencies and/or contingencies, the deployed MTF commander relies on highly-trained medics and state-of-the-art, light, ruggedized medical equipment to ensure the MTF response is swift and provides the correct capabilities for each situation. As at home station, comprehensive planning and realistic exercises ensure personnel are prepared to support expeditionary, humanitarian assistance, and disaster relief (HA/DR) operations. In the deployed environment, monthly exercises typically occur, many of which are the same types of exercises medics experience at home station prescribed by Wing Plans, and the Medical Readiness Training and Exercise Schedule (MRTES).
To ensure a coordinated response, Wing leadership in many deployed locations rely on the principles and programs codified in the National Incident Management System (NIMS). This will include adherence to the command and control structure of the Incident Command System (ICS) in order to direct EM assets during all phases of emergency response operations. Overarching governance for AF emergency management is contained in AFPD 10-25, Emergency Management, and AFI 10-2501, Air Force Emergency Management (EM) Program Planning and Operations. Deployed units should be flexible and responsive to the Host Nation Emergency Management system if deployed in a Disaster Response or Humanitarian Assistance role.

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
Deployed medical units are trained to respond to any contingency that may occur, but the MRO should ensure the MTF establishes and maintains the capabilities to respond to MC-CBRN events, to include patient decontamination prior to patient entry into the MTF, and patient triage, stabilization, treatment, and transportation and tracking for all types of medical scenarios involving multiple types and degrees of injured or wounded casualties. The importance of training, exercises, and properly equipping the facility and staff to perform operations cannot be over-emphasized. The MRO maintains an important role in ensuring the staff is properly prepared. MC-CBRN capabilities are specifically explained in AFTTP 3-42.32. Other references that can be helpful to the deployed MRO include AFI 41-106, Medical Readiness Program Management, AFTTP 3-42.71, Expeditionary Medical Support (EMEDS). AFTTP 3-42.5, AE, and AFTTP 3-42.53, CASF.
D. Plans
Unit level planning is critical to ensuring the unit is capable of meeting its expeditionary and emergency management missions. It includes developing unit plans and providing input to wing and local community plans by assessing the medical unit’s capabilities to support expeditionary and installation response requirements. Plans utilized and supported include but are not limited to:
Medical Contingency Response Plan (MCRP). The MCRP details responsibilities and actions required to accomplish the unit’s contingency response mission.
Comprehensive Emergency Management Plan (CEMP) 10-2. The Installation CEMP 10-2 is a base-level plan that aligns AF planning with the National Response Framework. Details are provided in AFI 10-2501.
Disease Containment Plan (DCP). The DCP addresses roles and procedures for responding to a disease outbreak. Details are provided in AFI 10-2604, Disease Containment Planning Guidance. An important piece of the DCP is the Mass Prophylaxis Plan. In recent years this was a separate plan for most units, but written guidance has changed requiring units to incorporate the Mass Prophylaxis Plan into the DCP and in many cases the CEMP. The Mass Prophylaxis Plan provides methods for wide dissemination of vaccinations, medications, and other medical supplies in a short period of time plans and based on credible threats or events. A second plan that has now also been incorporated into the DCP is the Pandemic Influenza (PI) Plan. The PI Plan provided the original thinking regarding mass prophylaxis which is now the foundation of the Mass Prophylaxis Plan.
Host Nation Response Plan (if developed). For installations outside the United States, support during emergency operations is provided through established host nation support agreements, by direction of the Combatant Command, or upon direction of the installation commander to save lives, prevent human suffering, or mitigate great property damage. Requests for US military

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
support of stability operations and disaster response outside the United States are typically submitted by the host nation through the Department of State (DOS).
DOD teams work cooperatively with the host nation to identify temporary military-specific support capabilities and resources necessary to minimize human suffering. The provision of direct medical services to host nation members will be focused on short-term objectives, transitioning to non-governmental or international organizations as soon as practical.
The MCRP is the medical unit commander’s plan, establishing procedures for the unit’s expeditionary missions identified in the Designed Operational Capability (DOC) statement and emergency response missions identified in the CEMP 10-2. The MRO will manage the preparation, coordination, publication, and distribution of the MCRP if required by local Wing and/or MTF leadership. As the core document for MTF readiness operations, the MCRP is one of the most important documents a deployed MTF can have at its disposal, particularly in the event the CEMP is activated.
Per AFI 41-106, deployed MTFs are not required to have an MCRP, but if MTF or Wing leadership require and MCRP as part of base contingency planning, then the MRO should develop an MCRP. AFI 41-106 describes how to write and develop and MCRP and what should be included in this document. Although not required, deployed units will conduct a realistic assessment of their contingency response capabilities (including MC-CBRN) and incorporate them into the installation’s CEMP 10-2, or sister service equivalent. MROs will use the MCRP team annex guidance in AFI 41-106, Attachment 2 as the framework for preparing CEMP 10-2 inputs, utilizing the established MCRP team names.
MROs should clearly identify MTF capabilities, roles and responsibilities in support of a collaborative installation response, including support provided via MOUs/MOAs/MAAs, as appropriate. Additionally, disaster teams may be developed and utilized as at home station. If disaster teams are utilized, ensure personnel are assigned and trained utilizing existing MCRP team names and training requirements outlined in this AFI 41-106 and in the Minimum MCRP Team Training matrix provided on the AF Medical Readiness Community of Practice (CoP).
Units should develop and maintain current medical response checklists in support of installation plans, addressing unit control center activation, major accident response, natural disaster response, MC-CBRN response, and casualty management, at a minimum. All plans and checklists will be reviewed at the beginning of each rotation to ensure continuity across the staff. Deployed MTF commanders will review response checklists upon assignment and validate procedures at least once each AEF rotation.
The deployed MFT staff must review the MCRP each rotation and team chiefs should review and update their respective annexes and checklists annually. Finally, a smaller version of the MRTES could be developed in coordination with the Wing Plans Office to appropriately plan for

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
training and exercises, particularly if incorporating disaster team training into the Wing’s exercise schedule.
E. Reports
The MRO is responsible for collecting unit mission preparedness data and preparing the unit’s operational readiness reports. AFI 10-206, Operational Reporting, provides guidance as to reports for which the MRO is responsible.
F. Training, Exercises, and Recalls
Training is an important aspect of the deployed environment to keep staff members sharp and to ensure people are ready for any contingency that might occur. As discussed in the section on Plans, MROs have the responsibility to ensure disaster teams are developed with members assigned if the MTF Commander requires team formation as part of MTF operations. As at home station, MROs should provide oversight, guidance, and support to disaster team chiefs. Additionally, they should also facilitate disaster team training at the discretion of the commander.
Ensure team chiefs know their responsibilities, which include, but are not limited to: maintaining contact information for their team members; developing and maintaining team training lesson plans; ensuring their team members are trained; obtaining, maintaining and inventorying team supplies and/or equipment; reviewing and updating the team’s annex in the MCRP as well as supporting operational checklists.
In coordination with the Wing Plans Office, the MRO has the responsibility to incorporate training events, courses, and exercises into a schedule that meets the training needs of all assigned personnel, while considering the unit’s mission, resource availability and limiting factors.
Coordinate with the Wing and MTF Exercise Evaluation Team (EET) Chiefs. Provide exercise requirements to assist with exercise scenario development to ensure medical capabilities are adequately tested. Coordinate with the Medical EET representative to facilitate the integration of medical exercise requirements with planned wing exercises to the greatest extent possible.
If required, develop the MRTES, incorporating unit developed readiness training programs under and Wing training schedules as available. A sample MRTES format is provided on the AF Medical Readiness CoP.
Finally, develop and maintain recall rosters throughout the deployment duration. Combatant commands often require recalls at the beginning of new Air Expeditionary Forces (AEF) rotations and then as required by local commanders as requirements dictate. Maintaining correct, current contact information for all staff members is one of the most important duties of an MRO in an expeditionary environment.

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
G. Relationships
In an expeditionary setting, MROs need to develop close relationships with expeditionary wing leadership, Sister Service units that may be in the area, and Host Nation partners to ensure fluid operations for both the MTF and the Wing. MROs should develop close partnerships with the Wing Plans Office usually designated as AEW/XP, the Command Post (AEW/CP), the Civil Engineer (CE) and more specifically CE Readiness and/or EM, the Logistics Readiness Squadron (LRS) as the transportation function, and individual equipment issue to include Mission Oriented Protective Postures (MOPP) gear, body armor, and weapons are often maintained and issued through this squadron, the Fire Department which is a CE flight, Security Forces, Comm Sq, and Wing Exercise Evaluation Team (EET) members. Higher headquarters (HHQ) units the MRO should also know on a familiar basis include the MAJCOM Surgeon General (SG) staff, the combatant command SG staff, C-NAF SG staff, and the combatant command forward SG staff. Not only can members of these offices, squadrons, and HHQ staff assist the MRO and the MTF staff with answers to questions, it is imperative that close relationships are developed in order to allow the MTF mission to function on a daily basis. Close relationships with other Wing agencies and Host Nation partners are integral to smooth running operations. Because of the uncertain environment in a deployed setting, the old adage “cooperate and graduate” is an apt description to use. All members of an expeditionary wing are in the “same boat” when it comes to the deployed environment and it makes the job of mission accomplishment that much smoother if everyone works together with the same goals in mind.
SUMMARY
The AFMS provides seamless health service support to AF and combatant commanders and assists in sustaining the performance, health and fitness of every Airman in-garrison and while deployed within CONUS or overseas in support of global operations. This capability includes the full spectrum of medical operations (expeditionary deployment operations, humanitarian assistance, disaster response, and global health engagement to support building partnerships and stability operations) and the necessary planning, training, and readiness support functions (reports, disaster management, and others) associated with these operations. This module has addressed the roles and responsibilities an MSC who is assigned as the MRO may perform in an expeditionary environment.
ACRO�YMS
AE Air Evacuation AEF Air Expeditionary Forces AEW Air Expeditionary Wing AF Air Force AFI Air Force Instruction AFIMS Air Force Incident Management System AFMAN Air Force Manual
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
AFMS Air Force Medical Service AFPD Air Force Policy Directive AFTTP Air Force Tactics, Techniques, and Procedures CASF Contingency Air Staging Facility CBRN Chemical, Biological, Radiological, Nuclear CE Civil Engineer CEMP Consolidated Emergency Management Plan C-NAF Component Numbered Air Force CONUS Continental United States CoP Community of Practice CP Command Post DCP Disease Containment Plan DOC Designed Operational Capability DoD Department of Defense DoS Department of State DR Disaster Relief EET Exercise Evaluation Team EM Emergency Management EMEDS Expeditionary Medical Support ESF Emergency Support Functions HA Humanitarian Assistance HHQ Higher Headquarters ICS Incident Command System LMR Land Mobile Radio LRS Logistics Readiness Squadron MAA Mutual Aid Agreements MOA Memorandum of Agreement MOU Memorandum of Understanding MCC Medical Control Center MCRP Medical Contingency Response Plan MOPP Mission Oriented Protective Postures MRO Medical Readiness Officer MRTES Medical Readiness Training and Exercise Schedule MSC Medical Service Corps MTF Medical Treatment Facility NDMS National Disaster Management System NIMS National Incident Management System OCONUS Overseas Continental United States OCR Office of Coordinating Responsibility OPR Office of Primary Responsibility PI Pandemic Influenza SG Surgeon General STE Secure Terminal Equipment USAF United States Air Force XP Wing Plans
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
CO�CEPT OF OPERATIO�S
OBJECTIVE
Describe the wartime Air Force Medical Service Mission and Concept of Operations (CONOPS). Provide an understanding of the Designed Operational Capability (DOC) Statement and identify four key components outlined in the DOC statement. Provide a description of the Medical Unit Type Code (UTC) and explain their respective responsibilities. I�TRODUCTIO�
The term Concept of Operations or CONOPS is often referred to as the “commander’s concept.” It details the assumptions and intent of the operation and is designed to give an overall picture of the operation. The CONOPS for medical mission readiness is contained in several documents. It requires meeting the Air Force Medical Service's mission and objectives through planning for deployment and operations in a deployed location. Units are mobilized and deployed based on their assigned Unit Type Codes (UTC), which are identified in the DOC statements. OVERVIEW
• AF Medical Service Mission • DOC Statements • UTCs REFERE�CES
AFI 41-106 Medical Readiness Planning and Training AFDIR 41-317 Compendium of Aeromedical Evacuation Terminology PRESE�TATIO�
A. AF Medical Service Mission The Air Force Medical Service (AFMS) supports the mission of the Air Force in times of peace, national emergency, or war. The AFMS provides medical care for patients, including members of the total force and all beneficiaries, and advances the overall health of the Air Force Community through preventive and public health measures. The AFMS promotes education, research, and policy to assure a healthy population. B. DOC Statements 1. The DOC statement is prepared by the parent Major Command (MAJCOM) for each measured unit. It summarizes the DOC of the unit and contains unit identification, mission tasking narrative, mission specifics, and resources to be measured. It provides unit commanders a clear definition of their unit’s wartime capability, based upon the authorized manpower and materiel strength of the unit. The primary purpose of the DOC
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
statement is to serve as the baseline for the Status of Resources and Training System (SORTS) reporting. It is also utilized as a commander’s reference and reflects Operation Plan (OPLAN) tasking or functional manager tasking. 2. The four key essential elements referenced in a DOC statement include: - Command and Control for assigned worldwide locations - Direct communication with the military customer originating patients - Patient movement to destination hospitals - Deployment of personnel and equipment to support the AFMS mission 3. Unit Type Codes Unit type codes are used in the DOC statement to identify the tasks being supported. UTCs are an alphanumeric code assigned to personnel or equipment packages and are considered “building blocks” for accomplishing mission tasks. All alphanumeric codes begin with “FF” which signifies an Air Force Medical UTC and are designed to fulfill a specific mission. a. Aeromedical Evacuation (AE)
• ADVON (FFQAC) – arranges support requirements and initializes operational command, control, coordination and communication for deployed AE activities.
• AE Squadron HQ (FFQAD) – Establishes operational command, control, coordination and communication for deployed AE activities.
• AE Group HQ (FFQAE) – Establishes operational command, control,
coordination and communication for deployed AE activities.
• Aeromedical Staging Treatment Facility (ASTF) (FFLBD, FFLCA, FFLEA) – Demonstrates ability to receive, assess, triage, stabilize, sustain and transfer patients.
• CCATT (FFCCT) – The Critical Care Air Transport Team is able to receive,
assess, triage, stabilize and provide critical care to sustain patients on the ground and enroute to destination facility.
• AE Control Center (AECC) (FFQCU) – Accomplishes theater planning, coordinating, monitoring and execution of AE mission operations.
• AE Support Cell (FFQCT) – Demonstrates ability to sustain theater AE elements
as applicable (logistics, AGE, vehicle operations and communication equipment).
• AE Operations Team (AEOT) (FFQCY) – Accomplishes day-to-day planning,coordinating, monitoring and execution of AE mission operations.

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
• AE Crew Management Cell (FFQCX) – Exercises operational control/crew management over tasked AE crews.
• AE Crews (FFQCE) – AE Crew members (AECM) receive, assess, triage,
stabilize, sustain and transfer patients during ground and inflight operations.
• Mobile Aeromedical Staging Facility (MASF) (FFLAB) – Demonstrates ability to receive, assess, triage, stabilize, sustain and transfer patients.
• AE Liaison Team (AELT) (FFQCV) – Establishes and maintains communication
and coordination with AE elements and user services to provide optimum aeromedical evacuation of casualties.
b. Ground Medical Units
• Air Transportable Clinic (ATC) (FFDAB) – Primarily patient treatment; determines availability of, or helps arrange hospital and AE support. Expeditionary Medical Support (EMEDS)/Air Force Theater Hospital (AFTH) (FFGL2, FFMFS, FFGL3) – EMEDS Basic provides 24hr sick call and emergency medical care; provides only limited holding capability of less than 24hrs; may be rapidly augmented with additional medical capability. The 2nd increment (EMEDS +10 Bed AFTH) provides 10 inpatient beds resulting in increased capacity and diagnostic capability while maintaining a similar scope of care. The 3rd increment (EMEDS +25 Bed AFTH) increases inpatient capacity to 25 beds and increases the scope of care.
• There are numerous other UTCs including the Blood program and specialty sets (Opthamology, Primary care, Urology, etc.). Reference AFI41-106, Attachment 5, for more detailed information.
SUMMARY
The Concept of Operations, or CONOPS, is an important aspect of mission readiness and mobilization planning. Understanding how your medical unit will be utilized in the event of a contingency is paramount to the success of the operation. Knowing the basic assumptions and intent of the commander’s vision will enable the MSC to perform the necessary planning and execution of the mission. FORMS
N/A ACRO�YMS
ADVON Advanced Management Team AE Aeromedical Evacuation
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
AECC Aeromedical Evacuation Control Center AELT Aeromedical Evacuation Liaison Team AEOT Aeromedical Evacuation Operations Team AFMS Air Force Medical Service ASTF Aeromedical Staging Treatment Facility ATC Air Transportable Clinic CCATT Critical Care Air Transport Team CONOPS Concept of Operations DOC Designed Operational Capability EMEDS Expeditionary Medical Support MAJCOM Major Command MASF Mobile Aeromedical Staging Facility MSC Medical Service Corps OPLAN Operation Plan SORTS Status of Resources and Training System UTC Unit Type Code
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
POST EVALUATIO�
1. The warning order initiates the mobilization process and must be acted upon immediately.
TRUE OR FALSE 2. ________________ encompasses all activities necessary for the orderly transition of active and ARC forces from a peacetime to a wartime posture.
a. Deployment b. Employment c. Mobilization
3. Requirements for mobilization include both personal and mission-specific details that must be prepared for in advance. __________________ is an example of a mission-specific requirement.
a. Ensuring that unit members have current DD Fm 93s b. Ensuring adequate numbers of personnel are trained in handling hazardous cargo
4. The Air Force Medical Service Mission refers to peacetime health care only.
TRUE OR FALSE 5. There are ________ types of activation within the mobilization process.
a. Three b. Four c. Five d. Seven 6. Everyone must complete TFAT training on an annual basis.
TRUE OR FALSE 7. LOAC is considered _________ training.
a. Tier 1 b. Tier 2A c. Tier 2B d. Tier 3 e. None of the above 8. Combat Airman Skills Training (CAST) is for ____________________________________.
a. Expeditionary skills proficiency training
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
b. Home station pre-deployment training c. AF and CCDR entry requirements for Airmen tasked to deploy d. Select deployers whose attendance is dictated by mission and threat/location 9. Tier 1 training is foundational expeditionary skills training with a primary focus to help Airmen establish a “strong warrior ethos.”
TRUE OR FALSE 10. Training is accomplished through a combination of _______________________________ _____, and _______ and ________ expeditionary skills training.
a. CAST, TFAT, and 2A b. TFAT, 2A, 2B c. Tier 1, 2A, 2B d. Tier 1, CAST, 2B e. All of the above f. None of the above 11. Wing leadership in many deployed locations adhere to the command and control structure of the Incident Command System (ICS) in order to direct EM assets during all phases of emergency response operations.
TRUE OR FALSE 12. Plans utilized and supported in a deployed environment include but are not limited to:
a. MCRP, CEMP, and DCP b. National Military Strategy, and COCOM Plans c. TTPs, and the Deployed Medical Commanders Handbook d. AFIs and Wing and MDG OIs 13. The medical readiness report format is found in ____________.
a. DOC Statement b. AFI 41-106 c. AFI 10-206 d. AFI 10-2 14. Recalls and the use of Recall Rosters is only a home station emergency notification procedure that is not utilized in a deployed environment.
TRUE OR FALSE 15. In an expeditionary setting, MROs need to develop close relationships with expeditionary wing leadership, Sister Service units that may be in the area, and Host Nation partners to

MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
ensure fluid operations for both the MTF and the Wing.
TRUE OR FALSE 16. The _____________ gives the overall “big picture” of how the AFMS meets its mission and objectives through planning for deployment and operating in a deployed location.
a. CONOPS b. DOC statement c. OPLAN
17. Key elements referenced in a DOC statement include:
a. Command and control for assigned worldwide locations b. Direct communication with the military customer originating patients c. Patient movement to destination hospitals d. Deployment of personnel and equipment to support the AFMS mission e. A and C f. All of the above
18. Used in the DOC statement to identify the tasks being supported , ______ are alpha-numeric designations assigned to personnel or equipment packages.
a. CCATTs b. UTCs c. EMEDs
19. The __________ is able to receive, assess, triage, stabilize and provide critical care to Sustain patients on the ground and enroute to destination facility.
a. EMEDS b. CASF c. CCATT d. 46Ns 20. The EMEDS Basic provides 24hr sick call and emergency medical care.
TRUE OR FALSE
MISSIO� READI�ESS MODULE MSC READI�ESS SUSTAI�ME�T VERIFICATIO� PROGRAM
A�SWER KEY
1. FALSE 2. C 3. B 4. FALSE 5. D 6. TRUE 7. B 8. D 9. TRUE 10. B11. TRUE 12. A13. C14. FALSE 15. TRUE 16. A17. F18. B19. C20. TRUE