Minimal treatments and problem gamblers: A preliminary investigation
16
Minimal Treatments and Problem Gamblers: A Preliminary Investigation 1 Mark Dickerson, John Hinchy and Stephanie Legg England Department of Psychology, Australian National University In view of the increasing popularity of minimal intervention treatments for problem drinking, a self-help manual for people who wish to reduce or stop gambling was prepared. Twenty-nine (ACT residents) who responded to advertisements for help with problem gambling were allocated to either of two minimal treatments, "Manual (only)" and "Manual&Interview." On average, clients from both groups reduced the frequency of their gambling sessions, frequency of overspending, and amount spent per week in the first three months and next three months after first contact, but expenditure per session increased from three to six months, after an initial improve- ment. There was no evidence that a single in-depth interview added to the effectiveness of the manual. In an excellent review of minimal interventions for alcohol related problems, Heather (1986) noted that treatment was considered "mini- maP' if it involved smaller amounts of professional time and/or re- sources than are typical of the traditional face-to-face interaction be- tween therapist and individual clients or groups. Such a definition includes a whole range of brief interventions as well as the method of 1This project was funded by a grant from the Australian National University Faculties Research Fund. Reprint requests to Mark Dickerson, Department of Psychology, Australian National Uni- versity, PO Box 4, ACT 2601. Australia. Journal of Gambling Studies Vol. 6(1), Spring 1990 1990 Human Sciences Press 87
-
Upload
mark-dickerson -
Category
Documents
-
view
212 -
download
0
Transcript of Minimal treatments and problem gamblers: A preliminary investigation

Minimal Treatments and Problem Gamblers: A Preliminary Investigation 1
Mark Dickerson, John Hinchy and Stephanie Legg England Department of Psychology, Australian National University
In view of the increasing populari ty of minimal intervent ion t reatments for problem drinking, a self-help manua l for people who wish to reduce or stop gambl ing was prepared. Twenty-nine ( A C T residents) who responded to advert isements for help with problem gambling were allocated to ei ther of two minimal t reatments, "Manua l (only)" and "Manual&Interview." O n average, clients from both groups reduced the frequency of their gambl ing sessions, frequency of overspending, and amount spent per week in the first three months and next three months after first contact, but expendi ture per session increased from three to six months , after an initial improve- ment . There was no evidence that a single in-depth interview added to the effectiveness of the manual .
In an excellent review of min imal in tervent ions for alcohol related problems, H e a t h e r (1986) noted that t r ea tment was considered "mini- maP' if it involved smaller amoun t s of professional t ime and /o r re- sources than are typical of the tradi t ional face-to-face interact ion be- tween therapist and individual clients or groups. Such a definit ion includes a whole range of br ie f in tervent ions as well as the me thod of
1This project was funded by a grant from the Australian National University Faculties Research Fund.
Reprint requests to Mark Dickerson, Department of Psychology, Australian National Uni- versity, PO Box 4, ACT 2601. Australia.
Journal of Gambling Studies Vol. 6(1), Spring 1990 �9 1990 Human Sciences Press 87

88 JOURNAL OF GAMBLING STUDIES
interest in the present study, written self-help materials, with or with- out therapist contact.
In examining the development of minimal intervention, Heather (1986) identifies five factors that have contributed to its growth; (i) the ever increasing cost of health services, (ii) the emergence of an ideology of self-help, (iii) an ethos and theoretical base in psychology supportive to such an ideology, (iv) the erosion of illness models in areas of personal problems such as alcoholism and (v) evidence that some intensive traditional treatments are ineffective. As far as psychologists are concerned, the most influential event was the presidential address of George Miller in 1969 to the American Psychological Association in which he advocated "giving psychology away." Certainly in the 1970s the self-control behaviour therapy literature rapidly developed (Rach- m an & Wilson, 1980) and provided the theoretical and methodological base for most self-help behaviour therapy manuals.
The use of such manuals has been evaluated in a variety of problem areas from smoking to agoraphobia but their application to problem drinking did not occur until relatively late (Glasgow & Rosen, 1978). This was primarily because of the belief that no alcoholic could ever return to a controlled level of drinking and that therefore it was unethical to entertain any treatment goal other than abstinence. De- spite the continuing destructive polemics that surround this issue (Heather & Robertson, 1983), it has now been established that the use of behavioural self-help manuals results in a significant proportion of excessive drinkers controlling and reducing their alcohol intake (Heather, Whit ton & Robertson, 1986; Miller, Gribskov & Mortell, 1981; Miller & Taylor, 1980).
It has been argued (Dickerson, 1987) that research in gambling may benefit from developments in alcoholism and this may be true of minimal treatments. Although no research has yet been published on this topic there are grounds for believing that such an approach to t reatment may be particularly relevant to people who gamble exces- sively. Firstly, in most countries the availability of help for gamblers is very limited (Blaszczynski, 1985; Cornish, 1978; Dickerson, 1984). It follows that where treatment centres exist the majority of the potential clients will be geographically remote. The most important factor under- mining the development of costly traditional treatments is the absence of reliable and valid estimates of prevalence rates (Dickerson & Hinchy, 1988; Nadler, 1985; Orford, 1985; Volberg & Steadman, 1988).

MARK DICKERSON, ET AL. 89
This situation was typical of the research team's own geographical base in the Australian Capital Terri tory (ACT). With a population of approximately a quarter of a million and two legalised and popular forms of continuous gambling (off-course betting and poker machines), the only two gambling treatment centres were 400 kilometres away in Sydney. Local resources amounted to one small Gamblers Anonymous group and limited expertise of local psychologists and counsellors who had attended our training workshops. Previous attempts to obtain federal funds to provide and evaluate a traditional treatment service had not met with success. This was the context in which a self-help manual for problem gamblers was prepared (Dickerson, 1986) and evaluated.
The manual was modelled on the most recent and successful one from the alcohol literature (Robertson & Heather, 1983) now pub- lished as "Let's Drink To Your Health" (1987). In the present study the manual was titled, "Problem Gambling: a self-help manual for controlling or stopping the amount you spend on gambling," and contained the following sections: 1) definition of the potential user or problem gam- bler, 2) an examination of why people gamble, 3) how to self-monitor, 4) functional analysis of gambling behaviour, 5) goal/limit setting, 6) self-reinforcement, 7) alternative incompatible behaviours and 8) how to maintain gains in the longer term. The manual targetted an initial twelve weeks in which the desired reduction or abstinence goal would be achieved and provided recording sheets for that period. Also in- cluded was a list of all Australian G.A. meetings and contact phone numbers and a short reference list of further reading. Although not printed, the photocopy of a laser-printed original was of good quality and was spiroform bound with card covers cut to display the title.
In designing the methodology we were aware that the most appro- priate control would be a twelve week waiting list or no treatment group. In the context of alcoholism treatment research such a study might be defended, (a) because subjects most likely to benefit could be selected, e.g. those in the "hazardous" rather than "harmful" drinking categories, (Pols & Hawks, 1987) and (b) because the existing treat- ment services consist of a series of levels of problem recognition as well as a range of types of intervention. In the absence of these treatment characteristics we made a conservative choice to offer two forms of treatment both of which we had grounds for believing would be of assistance to problem gamblers; (i) the manual and a single in-depth

90 JOURNAL OF GAMBLING STUDIES
initial interview (Manual&Interview group), and (ii) the manual and telephone/postal contact only (Manual (only) group). The self-control behavioural procedures which comprised the main recommended prac- tices in the manual have been used effectively in case studies of gamblers (Dickerson & Weeks, 1979; Rankin, I982), and the question of whether personal therapist contact, however limited, enhances the use of self-help materials remains an unresolved issue in the alcohol domain. Orford & Edwards (1977) and Heather, Whitton & Robertson (1986) lead us to predict that the Manual/Interview group would show greater improvements than the Manual group.
M E T H O D
Twenty-one men and eight women, all adults, who made personal contact in writing or by phone during the course of the project were accepted provided they had a permanent address within the ACT or Queanbeyan. People who sought help from outside this area were routinely sent the Manual (only) group questionnaires and a copy of the manual but they were not included in the study.
Measures
The main dependent variable of level of involvement in gambling (frequency, time and money spent per week and per session) was assessed at baseline and follow-up by questionnaires specific to each form of gambling. For those clients interviewed, the questionnaire items formed a structured section within the assessment session. As in similar work in alcohol problems (Heather, Whitton and Robertson, 1986) the follow-up questions focussed on a limited window of the last week only. The measure of gambling involvement and a short list of demographic variables were the only questionnaires completed by the manual group.
In addition the Manual&Interview group completed visual ana- logue rating scales (Aitken, 1969) assessing the level of positive and negative impact of gambling on different aspects of their life; this same

MARK DICKERSON, ET AL. 91
form was completed independently by the interviewer. Clients also filled in measures of individual differences for use in the comparison of personality with high and low frequency non-problem gamblers (Dick- erson, Legg England & Hinchy, 1989). The interview lasted between 90 and 120 minutes and followed the sequence of: 1) reasons for seeking help, 2) description of treatment offered, 3) completion of demographic and gambling involvement items, 4) detailed unstruc- tured behavioural analysis of the gambling behaviours and their inter- relationship with all areas of the person's life, 5) completion of ratings, 6) coffee break while subject completed personality questionnaires and interviewer collated assessment and prepared opinion, 7) review and feedback to client including specific recommendations regarding action both using aspects of the manual and other community resources, and 8) letter summarising review and recommendations sent within 5 days.
Treatments
Manual (only) clients were mailed questionnaires and the man- ual; follow-up questionnaires were mailed. Manual&Interview clients were given the manual during a single in-depth assessment interview; follow-up questionnaires were mailed.
Procedure
The programme was first advertised in April 1986; a newspaper ad asked, "Gambling too much?" and gave details of the free help, the confidentiality, the free mail system and phone number. A simul- taneous press release generated local radio and TV interviews and stories. All local helping agenciefi and medical centres were sent display leaflets (later the off-course betting facilities permitted the circulation of similar leaflets). Advertising continued periodically until the end of the year, and the last subject was accepted to the project in February, 1987 (the funding for the study was limited to 2 years and 6-month follow-up and data analysis was to be completed by December, 1987). Subjects who continued to present for help at a low frequency through- out 1987 were sent postal questionnaires and the manual but not included in the data analysis.
Subjects were allocated to treatment at random; similarly to one of two psychologists within the Manual&Interview treatment.

92 JOURNAL OF GAMBLING STUDIES
[Copies of the questionnaires, the interview format, and the man- ual are available from the authors on request.]
RESULTS
Sixty-five people from the Canberra/Queanbeyan region con- tacted the program during its operation, and twenty-nine of these completed the initial stage of the program. Of the other thirty-six little is known. They contacted the project by 'phone or mail in roughly equal proportions stating they were gambling more than they would prefer, were allocated at random to one of the treatments, sent a manual and initial questionnaire or a specific time for an appointment was agreed upon. Nothing further was heard from these clients.
Participants were twenty-one males and eight females, with ages ranging from 23 to 59 years (X = 40.97). They included nineteen poker machine players, four off-course bettors, one on-course bettor, and five people whose main form of gambling was not known. The level of education completed by subjects ranged from primary school to a degree, with 84% having completed at least secondary school (me- dian education 11 years). About half of the subjects were currently married, and another 40% had been married previously.
During the preceding month, three clients had gambling sessions once a week, six gambled twice a week, sixteen gambled three to five times a week, and four gambled every day. All clients took over half an hour for a session, 61% stayed for more than two hours, and 21% for more than four hours. On average, clients spent 9 hours 17 minutes gambling per week (Range: 45 minutes to 31 hrs. 30 minutes).
In a usual session clients spent an average of $A73.35 (Range: $A10 to $A500), implying a mean weekly expenditure of $A318.55 (Range: $A30 to $A3,500), with poker machine playing being the least expensive. Participants reported being down by $A5,464, on average, over the last year (Range $A0 to $A20,000). Half the sample never planned or budgetted what they would spend in a session, but one quarter always planned their expenditure. In the last five sessions some gamblers had overspent on every occasion, while some had overspent on none (X = 3.75 times). Nevertheless, the majority of clients had taken money from leisure funds (83 %), savings (76 %), housekeeping funds (69 %), and/or a loan (62 %) during the last year to finance their gambling.

MARK DICKERSON, ET AL. 93
On a scale from 0 to 100, with 100 indicating many effects, participants rated the bad effects of gambling on their family at 71.37 (Range: 5 to 99), on their friends at 56.24 (Range: 0 to 100), financial problems at 71.97 (Range 2 to 100), and work problems at 30.45 (range: 0 to 96). Good effects on family and friends were fewer (Means: 13.56 and 28.64 respectively).
Only three clients reported that they mostly or always gambled in company. Almost 330,4 of the sample always gambled alone. This was despite the fact that 40 % have friends who gamble, 29% have work- mates who gamble, and 45% have parents who gamble (having spouses or siblings who gamble was rare). On an open-ended check list of items clients endorsed a variety of reasons for gambling: to forget troubles (79%), to win a major payout (76%), to win any money (69%), for something to do (62%), for excitement (62%), for enter- tainment (55%), for a challenge (55%), to have something to look forward to (52%), and to be sociable (14%).
Although a few clients had relatively mild problems of control and reported low levels of indirect problems at work and in relationships, as a group they seemed typical of first-time attenders at meetings of Gamblers Anonymous.
Two questions tapped expectations concerning the likely success of the programme for people generally and with respect to their own particular preferred goal. Approximately half of each treatment group for both questions indicated that they thought the treatment would be "mostly" or "totally" successful. The two treatment groups differed in the distribution of responses to the question concerning treatment objectives. The Manual&Interview group were significantly more likely to prefer "to give up entirely" compared with the Manual (only) group who preferred "to reduce your level of gambling" (X 2 = 6.63; d/2, p < .05). All but four clients had tried giving up or reducing previously and, of those who had tried, 84% had found it hard or very hard.
Allocation of gamblers to treatment groups resulted in a Manual (only) group of thirteen clients and a Manual&Interview group of sixteen subjects. Although there were no marked differences between the two groups in demographic variables, the Manual&Interview cli- ents fared worse than Manual (only) subjects on all indices of problem- atic gambling. On average the Manual&Interview clients were bigger spenders prior to joining the program, spending $443 and 11 hours 21 minutes gambling per week, compared with $165 and 6 hours 43 minutes per week for the Manual group.

94 JOURNAL OF GAMBLING STUDIES
Outcome
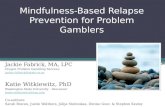
Twenty-one clients returned three month follow-up question- naires and twenty-one subjects returned six month follow-up question- naires. Their responses showed a reduction in frequency of sessions, length of sessions, and in weekly gambling expenditure in the six months following participation in the program, although the expendi- ture per session remained largely unchanged after six months. The amount of time and money spent gambling per week at first contact, three months and six months are shown in figures la and lb. Clients also reported a reduction in the frequency of spending more than planned after three months and again after six months. For each of these variables, the Manual&Interview Clients appeared to have expe- rienced more rapid improvement than the Manual (only) group in the first three months, but this progress was not sustained into the next three months. Meanwhile, the Manual (only) group continued to improve from three months to six months on most variables.
After three months all clients who had aimed initially for absten- tion were abstaining, while eight out of ten clients who had aimed to reduce had reduced or were abstaining. Two clients had increased their gambling involvement since initial contact. After six months only half of those who had initially planned to abstain were still abstaining. Strategies reported by gamblers to reach their goals included reading the self-help manual (sixteen clients), budgetting by making promises to oneself (six clients) or by behaviors like leaving money in the care (three clients) or by involving other people (two clients), and seeking help from partners (six clients), friends (three clients), family (two clients), and/or community help agencies (five clients). (These strate- gies were assessed by a questionnaire checklist of the above items plus one open-ended question).
After the first three months respondents were also asked to rate the effect of changing their level of gambling on partners, friends and workmates, finances and work. Effects on partners were unchanged for 44% of the group, with the remainder equally divided between im- proved and worsened effects. Effects on friends or workmates were unchanged for 67 % of the group, with the remainder equally divided between improved and worsened effects. Effects on finances were unchanged for 37%, with the remainder equally divided between improved and worsened. Effects on work were unchanged for 65 %,

Figure 1 Treatment outcome for Maunal&Interview ( A ) and Manual
(only) (11) Iroups at baseline, 3 and 4 month foUow-up 5 0 O
4 0 0
v Q~
~. 3 0 0
(a) m
~oo
o Q
1 0 0
_ I I I
0 3 6
~onths a f t e r i n i t i a l contact
(b)
(c)
4 v
L 3 @J
o 2i @J
i
0
120
iO0 t- o
~ ao al
c_ m 6 0
w L ,-, 4 0
121
2 0
} ! i
0 3 6 Months a f t e r i n i t i a l contact
I I I 0 3 6
Months a f t e r i n i t i a l contact
a) Expenditure per week b) Frequency of gambling sessions per week c) Expenditure per session.

96 JOURNAL OF GAMBLING STUDIES
with twice as many people reporting improved work effects as report- ing worsened work effects.
DISCUSSION
With the exception of the data derived from the initial interview of the Manual&Interview group, all measures of baseline and outcome were by" means of written answers to self-report questionnaires. In considering the reliability and validity of these data, given the random allocation of subject to treatment, it seems likely that the pretreatment reports of lower levels of financial and time involvement in gambling of the Manual (only) group may indicate a response bias to underreport. It is established that nearly all people attending Gamblers Anonymous recall frequently lying to obscure and deny the true nature of their gambling involvement (Dickerson, 1984). It therefore seems probable that the Manual (only) group were preferring to present a more socially acceptable level of gambling not only by reporting lower levels of cash and time spent gambling and lower estimates of the negative impact of gambling, but also higher estimates of the positive impact of gambling.
In addition they were less likely to nominate abstinence as their objective, preferring to reduce their gambling or failing to indicate any goal. In the supportive atmosphere of the clinical interview Man- ual&Interview clients may have been enabled to describe the realities of their situation, were more likely to prefer abstinence and were more likely to indicate that they would seek additional help. Whether these Manual&Interview clients continued to give accurate and reliable reports at follow-up cannot be determined. It is also important to note that random allocation not withstanding the baseline differences be- tween groups may have been real. As far as this study is concerned the results must be considered as tentative and requiring validation. The implication for other research, for example prevalence surveys, may be that reliable measures of pathology or excess require the use of an interview with the gambler and a significant other (Dickerson & Hinchy, 1988).
A second important aspect of the validity of the present study is whether those recruited were genuine problem gamblers. With one exception all Manual&Interview clients satisfied the revised DSM-I I I criteria of pathological gambling (Lesieur, 1988). Average weekly

MARK DICKERSON, ET AL. 97
losses of all clients were typical of those reported elsewhere in Australia (Blaszczynski, 1985). However, as reported annual losses were some- what lower and the percentage of women rather higher, it is probable that media recruitment results in a more heterogeneous population than those referred to hospital programmes. This is compatible with the telephone survey results of Volberg & Steadman (1988) and would be predicted from similar treatment research in alcoholism (Heather, 1986).
Only 45% of those who made personal contact with the pro- gramme attended for interview or returned their baseline question- naires. Similar attrition rates were found by Heather, Whitton & Robertson (1986) in their study of problem drinkers but the retention rate at 3 and 6 month follow-up was very much better with twenty-one of the original twenty-nine (74%) completing questionnaires. Mea- sures of frequency of gambling sessions and expenditure per week show a significant decrease from pretreatment to follow-up (Figures l a & lb). As shown above, these decreases were representative of the groups as a whole and not just a function of some people abstaining. In other words some subjects continued gambling but at a reduced level of involvement and reported less frequent loss of control.
The failure of ratings of change in other areas of subjects' lives to show improvement might be said to enhance the face validity of the reported reductions in involvement in gambling or to be interpreted as a sign that clients were not telling the truth about changes in gambling. Given the extent to which relationships with spouse, family and friends may be undermined by excessive gambling (Custer, 1982; Dickerson, 1984), improvement in these domains is unlikely to occur rapidly. Indeed, as reported by some clients, presenting for help and subse- quent attempts to stop or reduce gambling may have resulted in a deterioration in relationships, e.g. a spouse may for the first time learn the true extent of the problem or friendships may be disrupted by cessation of the shared leisure activity of gambling. The use of a social desirability measure such as the Marlowe-Crowne (Crowne & Mar- lowe, 1964) would have assisted in evaluating this result.
Thus, despite the probable response bias of the Manual (only) group, the validity of the data permits the tentative conclusion that the present minimal interventions were associated with a reduction in levels of involvement in gambling. Given the research design, this does not, however, confirm that either treatment was the necessary and

98 JOURNAL OF GAMBLING STUDIES
sufficient condition to bring about this change in gambling behavior. In the absence of a no-treatment control group it can be argued that all those who had reached the stage of seeking help and attending inter- view or completing assessment forms would have shown similar im- provements regardless of the form of intervention offered. For exam- ple, within the framework of Prochaska and Di Clemente's (1986) comprehensive model of change, those who "responded" to the present intervention may have been at the "contemplation" stage and moving to "action" as they made contact with the treatment programme, i.e. they were already involved in a process of change to a lower level of involvement in gambling.
A better methodology, would have been to design the interview along the lines of "Motivational Interviewing" used with problem drinkers (Miller, 1983) thereby enhancing clients' presenting motiva- tion.
The failure to find differences between the two groups may also be a function of this "readiness" of subjects to change but was none-the- less unexpected given the findings in relation to alcohol (Orford & Edwards, 1977; Heather, Whitton & Robertson, 1986).
However, the present study has a very small population followed up only for a six month period. It remains possible that the Man- ual&Interview group, because of their more frequent use of other helpers, may have shown greater long-term improvement in their relationships, finances and work and also may have maintained their reductions in gambling involvement.
One of the most interesting aspects of the present results was the apparent return to pretreatment baseline levels of the reported expen- diture per session of gambling (Figure 1 c). This was a function not just of some abstinent subjects returning to gambling but also of increases in expenditure by clients who had reported continued gambling at a reduced level at 3 month follow-up. It may be that this return to pre- treatment levels marks the beginning of a relapse process in which longer term follow-up, say at 12 or 24 months, would have revealed similar increases in frequency of sessions and weekly losses. This suggests that it may be theoretically important to distinguish between the determinants of impaired control within a session of continuous gambling (i.e. the decision to continue an ongoing session) and those factors that influence the decision to start a session. This distinction has been proposed for alcohol problems (Cameron, 1985) and has been

MARK DICKERSON, ET AL. 99
shown to have validity in assessing impaired control in poker-machine players (Corless, 1987). It is useful to speculate that in the present study those people who chose to reduce their involvement in gambling typically decided to have a single session per week and to limit their expenditure in that session. The present results suggest that it is the session budget that is hard to sustain even for 6 months. This has good face validity and fits well with the common assertion that it is the continuous, repetitive aspects of stake, play and determination that comprise one process essential to the production of excessive or patho- logical levels of gambling (Cornish, 1978; Dickerson, 1984; Orford, 1985). The present results raise the possibility that when such levels are reached it is particularly difficult to return to a lower, controlled level of gambling, despite the limited case-study evidence to the contrary (Blaszczynski, 1985; Dickerson, 1984). Not all clients who attempted reduction at three months necessarily relapsed as two-thirds became abstinent at six months. In fact, there was a trend for the initial choice of reduction to be positively associated with more successful outcomes at six months. It is possible that these subjects, on finding it too difficult to sustain their control of session length and expenditure, responded by stopping altogether.
The results indicate a trend that more successful outcomes were also associated with both the expressed initial intention to, and subse- quent reports of having used other "helpers," whether spouse, friends or counsellors. This relationship indicates the complex nature of the process of change experienced by subjects, the nature of which can only be sketched by the present preliminary study. As many subjects re- ported having previously experienced lower levels of gambling or periods of abstinence, it seems likely, as in alcoholism (Heather & Robertson, 1983) that some people may move into and out of problem- atic levels of gambling (i.e. including pathological gambling) without recourse to treatment, but typically in response to significant life events such as marriage or change of employment (Saunders & Kershaw, 1979; Tuchfield, 1976). Similarly, the maintenance of successful re- ductions in gambling may be determined more by social support and frequency of stressors than by the type of treatment experienced (Bill- ings and Moos, 1983).
If these parallels with the alcoholism literature can be sustained with empirical data confirming that the process of changing from a problematic involvement in gambling is complex and multicausal, it

100 J O U R N A L OF G A M B L I N G STUDIES
will come as no surprise that in the present study there was no homoge- neous response to the minimal intervention. The follow-up reports indicated a variety of reactions; those who reported not reading the manual and becoming abstinent, those for whom "treatment" served to confirm their intention to instigate a programme of change and those who may have actually put into practice the behavioural prescriptions detailed in the manual. The study of these very different responses requires a more sophisticated methodology and a much larger sample of clients. Future studies would benefit from the selection of a more homogenous group, the separation of the purely information-giving aspects of a manual from the assumed "active" ingredients of behav- ioural prescriptions and a more detailed follow-up using diaries and interviews.
On the basis of the present results, it can only be concluded that a minimal intervention approach to problem gambling may be accept- able to some clients and may be associated with short-term reductions in gambling involvement. However, it seems probable that some per- sonal contact, at least by way of an initial interview, may be essential in establishing valid assessments of pretreatment levels of gambling and related personal problems.
None-the-less, it seems likely that some form of self-help manual may well have a useful part to play in the provision of services for gamblers who seek help. Given the general paucity of such services and the lack of adequate prevalence data (Dickerson & Hinchy, 1988; Nadler, 1985; Volberg & Steadman, 1988) on which to base plans for more traditional treatments, a self-help manual represents a relatively cheap method of providing help particularly to clients geographically remote from the few existing in-patient facilities. It must, however, be stressed that the possible future use of minimal intervention be seen as but one component in the development of a range of types of help for problem gamblers and that self-help manuals of the kind used in the present study continue to be subjected to rigorous evaluation (Rosen, 1987).
REFERENCES
Aitken, R. (1969). Measurement of feeling using Visual Analogue Scales. Royal Society of Medicine Proceedings, 62, 909-996.
Billings, A.G & Moos, R.H. (1983). Psychosocial processes of recovery among alcoholics and their families: implications for clinicians and program evaluators. Addictive Behaviors, 8, 205-218.

M A R K D I C K E R S O N , ET AL. 101
Blaszczynski, A. (1985). Treatment approaches for the control of pathological gambling. In G. Caldwell, M.G. Dickerson, B. Haig, & L. Sylvan (Eds.) Gambling in Australia, (pp. 172-182) Sydney: Croom Helm.
Cameron, D. (1985). Why alcohol dependence-and why now? In N. Heather, I. Robertson & P. Davies, (Eds.) The Misuse of Alcohol, (pp. 59-71). London & Sydney: Croom Helm.
Corless, T. (1987). An investigation of impaired control in gambling behaviour: with specific reference to impaired control as a diagnostic criterion in DSM I l l "Pathological Gambling." Unpublished Masters thesis, Department of Psychology, Australian National University.
Cornish, D.B. (1978). Gambling." a review of the literature and its implications for policy & research. London: HMSO.
Crowne, D.P. & Marlowe, D. (1964). The Approval Motive: Studies in Evaluative Dependence. New York: Wiley.
Custer, R.L. (1982). An overview of compulsive gambling. In P.A. Carone, S.F. Yolles, S.N. Kieffer & L.W. Krinsky (Eds.) Addictive Disorders Update. New York: Human Sciences Press.
Dickerson, M.G. (1984). Compulsive Gamblers, London: Longman. Dickerson, M.G. (1986). Problem gambling: A self-help manual for controlling or stopping the
amount you spend on gambling, unpublished manuscript. In C. Allock & M.G. Dickerson, The Guide to Good Gambling, (pp. 160-193). Wentworth Falls, Australia: Social Science Press.
Dickerson, M.G. (1987). The future of gambling research-learning from the lessons of alcohol- ism. Journal of Gambling Behavior, 3, 248-256.
Dickerson, M.G. & Hinchy, J. (1988). The prevalence of excessive and pathological gambling in Australia. Journal of Gambling Behavior, 3, 135-151.
Diekerson, M.G., Legg England, S. & Hinchey, J. (1989). Pathological and social poker machine players; some empirical data on individual differences. (in preparation).
Dickerson, M.G. & Weeks, D. (1979). Controlled gambling as a therapeutic technique for compulsive gamblers. Journal of Behavior Therapy and Experimental Psychiaoy, 10, 139-145.
Glasgow, R.E. & Rosen, G.M. (1978). Behavioral bibliotherapy: A review of self-help behavior therapy manuals. Psychological Bulletin, 85, 1-23.
Heather, N. (1986). Minimal treatment interventions for problem drinkers. In G. Edwards & D. Gill (Eds.) Current Issues in Clinical Psychology (pp. 120-156) (Vo14). London: Plenum.
Heather, N. & Robertson, I. (1983). Controlled Drinking, London: Methuen. Heather, N., Whitton, B. & Robertson, I. (1986). Evaluation of a self-help manual for media
recruited problem drinkers: Six-month follow-up results, British Journal of Clinical Psychology, 25, 19-34.
Lesieur, H.R. (1988). Altering the DSM-III criteria for pathological gambling. Journal of Gam- bling Behavior, 4, 38-47.
Miller, W.R. (1983). Motivational interviewing with problem drinkers. Behavioural Psychotherapy, 11, 147-172.
Miller, W.R., Gribskov, C. & Mortell, R. (1981). The effectiveness of a self-control manual for problem drinkers with and without therapist contact. International Journal of Addictions, 16, 829-39.
Miller, W.R., & Taylor, C.A. (1980). Relative effectiveness of bibliotherapy, individual and group self-control training in the treatment of problem drinkers. Addictive Behaviours, 5, 13-24.
Nadler, L.B. (1985). The epidemiology of pathological gambling: Critique of existing research and alternative strategies. Journal of Gambling Behavior, 1, 35-50.
Orford, J. (1985). Excessive appetites: A psychological view of the addictions. Chichester: Wiley. Orford, J. & Edwards, G. (1977). Alcoholism: A comparison of treatment and advice, with a study of the
influence of marriage. Oxford: Oxford University Press. Pols, R.G. & Hawks, D.V. (1987). Is there a safe levd of daily consumption of alcohol for men and women?
Canberra: Australian Government Publishing Service. Prochaska, J.O. & Di Clemente, C.C. (1986). Toward a comprehensive model of change. In
W.R. Miller & N. Heather (Eds.) Treating Addictive Behaviours, (pp. 5-27). New York and London: Plenum.
Rankin, H. (1982). Control rather than abstinence as a goal in the treatment of excessive gambling. Behaviour Research and Therapy, 20, 185-187.
Rachman, SJ . & Wilson, G.T. (1980). The effects of psychological therapy. Oxford: Pergamon.

102 J O U R N A L OF G A M B L I N G STUDIES
Robertson, I. & Heather, N. (1987). Lets drink toyour health!-a guide to safe and sensible drinking (adapted for Australia and New Zealand by D. Watts). Sydney: Angus & Roberston.
Rosen, G.M. (1987). Self-help treatment books and the commercialisation of psychotherapy. American Psychologist, 42, 1, 46-51.
Saunders, W. & Kershaw, P. (1979). Spontaneous remission for alcoholism: Results from a community survey. British Journal of Addiction, 74, 251-265.
Tuchfield, B. (1976). Changes in the patterns of alcohal use without the aid of formal treatment, North Carolina Center for Health Studies, Research Triangle Institute, North Carolina.
Volberg, R.A. & Steadman, H.J. (1988). Refining prevalence estimates of pathological gam- bling. American Journal of Psychiaoy, 145, 502-505.