Mesenteric Ischemia: Silent Killer - Lieberman's...
47
Joseph M Reardon, HMS3 Gillian Lieberman, MD 3/2012 Mesenteric Ischemia: Silent Killer Joseph M Reardon, HMS3 Gillian Lieberman, MD Beth Israel Deaconess Medical Center Harvard Medical School
Transcript of Mesenteric Ischemia: Silent Killer - Lieberman's...

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Mesenteric Ischemia: Silent Killer
Joseph M Reardon, HMS3
Gillian Lieberman, MD
Beth Israel Deaconess Medical Center
Harvard Medical School

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 2

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 3

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Patient Presentation Hx: 83yo F with 4d of nausea, vomiting, diarrhea. No abdominal pain or fever/chills. Found by EMS unable to get out of bed or take POs PMH: HTN, CKD (baseline Cr 1.7-2), HLD, hypothyroidism, osteoporosis, non-Hodgkin lymphoma s/p radiation therapy in remission since 2001, Hx endometrial cancer Meds: atenolol, levothyroxine, pravastatin SH: Retired radiation researcher; lives with disabled relative for whom she is primary caretaker Exam: Hypotensive to 70s, A&Ox3, conversant, lungs CTAB, RRR, abd soft, NT/ND, no CVA tenderness Labs: WBC 14.1 with L shift, INR 1.5, BUN 26, Cr 2.0, LFTs, Trop 0.08, nl CK-MB, TSH 6.2, Lactate 5.0, ABG 65/27/7.4
4

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 5

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Clinical DDx: N/V/D, Hypotension
“V I T A M I N C D” Vascular Mesenteric ischemia Hypovolemia Embolism MI
Infection/Inflammation Sepsis Gastritis Gastroenteritis Acute Hepatitis Cholecystitis Abscess UTI Perforated ulcer Trauma Fall
Autoimmune IBD Allergy
Metabolic DKA Pancreatitis Acute Renal Failure
Iatrogenic Ventral hernia Partial obstruction / Adhesions
Neoplastic Recurrent lymphoma Gastric cancer Colon cancer Pancreatic cancer Hepatic cancer Carcinoid
Congenital Intestinal volvulus Adrenocortical insufficiency
Drugs B-blocker overdose Thyroid storm EtOH TSS, Food poisoning (Staph Toxin A)
6
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 7

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Imaging Modalities For our patient with N/V/D, BP
• CT- abdomen & pelvis with contrast to evaluate for bowel inflammation, perforation, looping, vascular supply (Rating 8)
• Ultrasound – RUQ U/S for biliary pathology (Rating 6) • MRI – T1 to assess abnormal fat distribution; T2 to
assess for edema, 1st line in pregnant patient (Rating 6) • XR – KUB to evaluate for free air or dilated loops
(Rating 5) • Nuclear Medicine – Ga-67 scan to evaluate for sites of
metabolic activity (Rating 4) • Invasive – ultrasound-guided fluid drainage, ostomy
placement via Seldinger technique Based on: “Acute Abdominal Pain and Fever or Suspected Abdominal Abscess.” ACR Appropriateness Criteria. American College of Radiology, 2008.
8

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Fu
• Use of IV Contrast in CT:
– Contraindicated in chronic renal insufficiency
– Contraindicated in acute kidney injury
– Weigh risks and benefits
• Concern for renal damage:
– Use Visipaque (iodixanol) rather than Optiray (ioversol)
– Ensure adequate pre-hydration
9
Imaging and Use of Contrast

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Balance of Benefits & Burdens
10
• Renal Damage • Radiation Risk • Cost
• Speed • Information
CT

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 11

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
12
Anatomy Review
From Gray’s Anatomy
Celiac artery
http://commons.wikimedia.org/wiki/File:Gray532.png

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Anatomy Review, continued
From Gray’s Anatomy http://en.wikibooks.org/wiki/File:Gray534.png http://en.wikibooks.org/wiki/File:Gray537.png
Superior Mesenteric Artery Inferior Mesenteric Artery Most tenuous blood supply – Marginal artery of Drummond
13

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 14

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
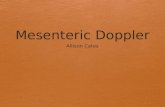
Posterior Right Portal Vein thrombosis
Fat Stranding Fluid tracking along portal vein
NG Tube
Anterior Right Portal Vein obliteration
Left hydronephrosis
Axial CT (Portal Venous Phase)
Axial C+ CT; PACS, BIDMC Note margin of liver hypoattenuation
*
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
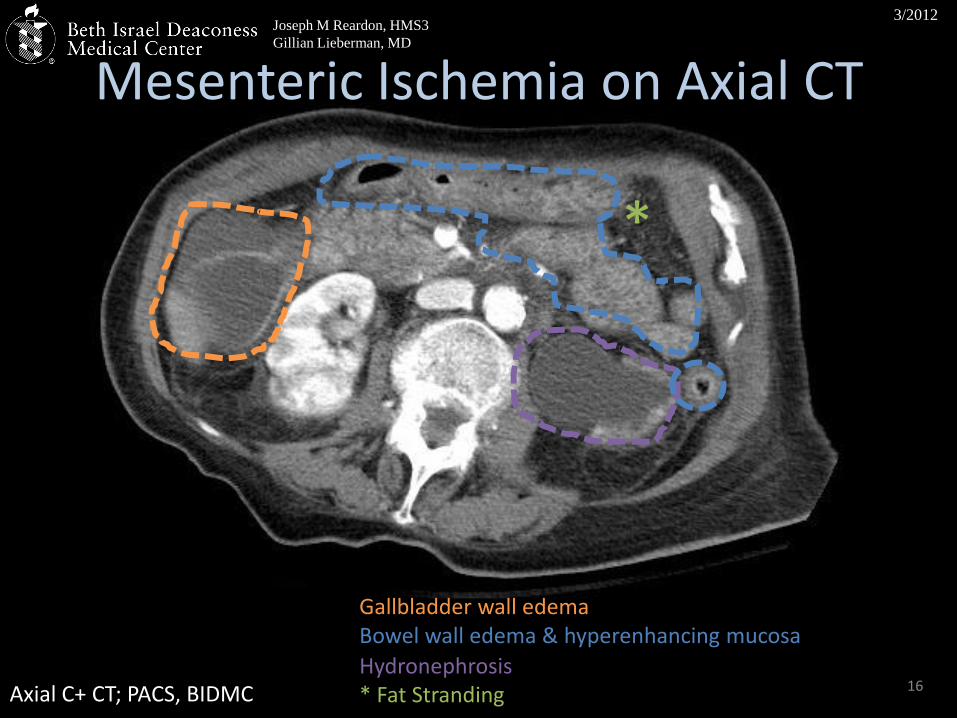
16
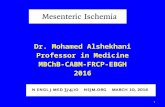
Bowel wall edema & hyperenhancing mucosa
Hydronephrosis * Fat Stranding
Gallbladder wall edema
*
CT Abdomen (3):
Mesenteric Ischemia on Axial CT
Axial C+ CT; PACS, BIDMC

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
17
Free fluid in pelvis
Bowel wall edema
Pelvic Free Fluid on Axial CT
Axial C+ CT; PACS, BIDMC
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
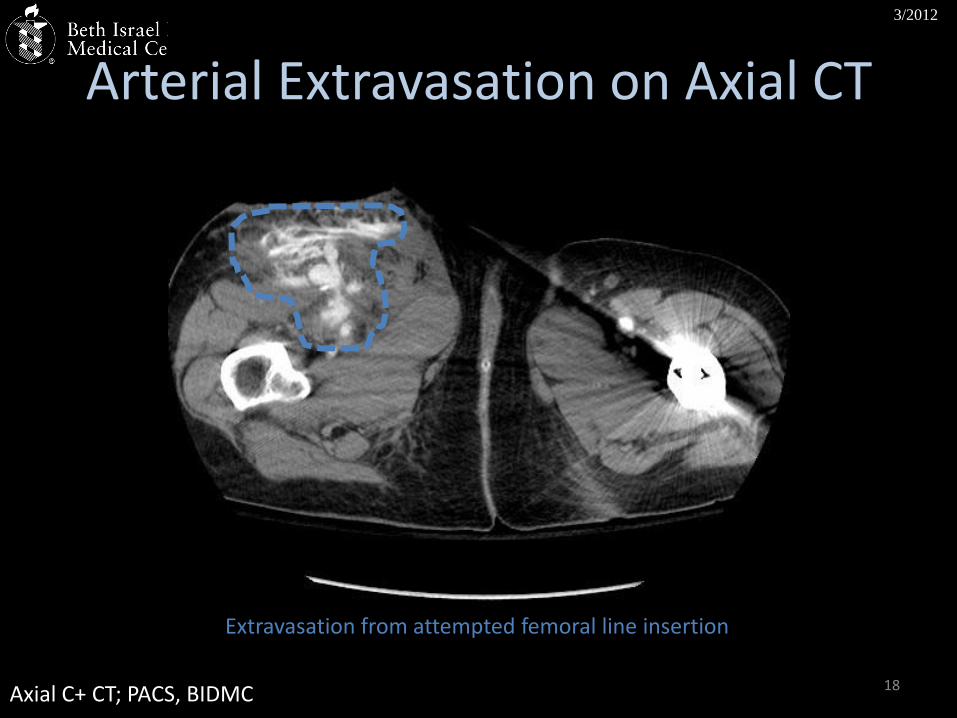
Extravasation from attempted femoral line insertion
18
Arterial Extravasation on Axial CT
Axial C+ CT; PACS, BIDMC

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
• How can
19
How can we link the patient’s presentation with disease
processes?

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Putting Together the Findings
History of Nausea, Vomiting, Diarrhea
Hypotension
Coagulopathy
Aggressive Resuscitation
20
Underlying Liver Disease
? Sepsis
Elevated Cardiac Enzymes
? MI
? UTI ? Acalculous Cholecystitis
Mesenteric Ischemia
Clinical Findings Contributing Factors

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
• How can
21
How do the disease processes manifest radiologically?
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
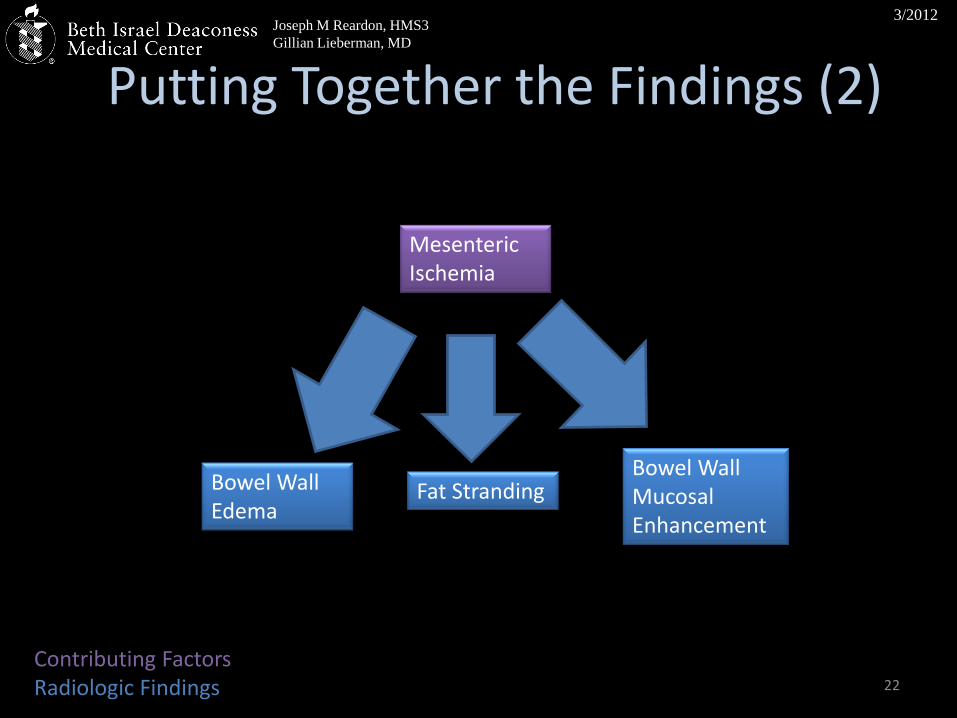
22
Putting Together the Findings (2)
Mesenteric Ischemia
Bowel Wall Edema
Bowel Wall Mucosal Enhancement
Fat Stranding
Contributing Factors Radiologic Findings
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
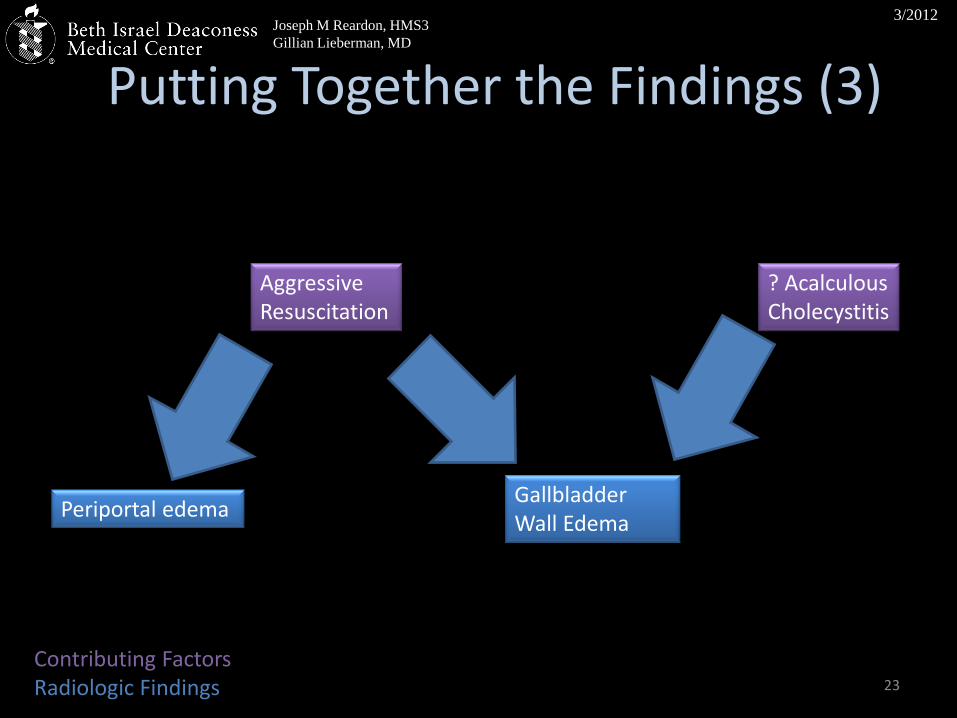
23
Putting Together the Findings (3)
Gallbladder Wall Edema
Periportal edema
Aggressive Resuscitation
? Acalculous Cholecystitis
Contributing Factors Radiologic Findings

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
24
Putting Together the Findings (4)
Arterial Extravasation
Portal Vein Thrombosis
Clinical Findings Radiologic Findings Contributing Factors
Hypotension Coagulopathy
? Underlying Liver Disease

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 25

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
What is Mesenteric Ischemia?
• Development
– Lack of perfusion to bowel mesentery
– Causes:
• Infarction – arterial or venous
• Embolism
• Low-Flow State
• Pathophysiology:
– Anoxia Buildup of metabolites (H+, K+) Cell death Necrosis
From Al-Shraim MM, Zafer MH, Rahman GA. Acute occlusive mesenteric ischemia in high altitude of southwestern region of Saudi Arabia. Ann Afr Med 2011;1:5-10.
26

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Presentation of Mesenteric Ischemia • S/Sx:
– Abdominal pain – Vomiting – Abdominal distension – Fever – Melena
• Hx: May have Afib, hypercoagulability • DDx: thromboembolic disease, digitalis toxicity,
drug reaction, small bowel obstruction, cecal volvulus, gastroenteritis, compression from tumor, complicated diverticulitis, inflammatory bowel disease, cholecystitis, appendicitis, peptic ulcer disease
27

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Why is Mesenteric Ischemia a Silent Killer? Mortality Rates of Comparable Conditions
28
Mo
rtal
ity
Rat
e (%
)

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Radiologic Diagnostic Signs
• Mucosal hyperenhancement
• Bowel wall hypoattenuation
(edema)
• Bowel wall thickening >3mm
From Macari M, Balthazar, EJ. “CT of Bowel Wall Thickening: Significance and Pitfalls of Interpretation.” Am J Roentgenology. 2001;5:1105-1116.
29

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Radiologic Diagnostic Signs, Contd
• Mesenteric vessel occlusion (+/-)
• Mesenteric fat stranding
• Ascites
From NYPEmergency.org
From meddean.luc.edu
From Johnson PT, Horton KM, Fishman EK. “Nonvascular Mesenteric Disease: Utility of Multidetector CT with 3D Volume Rendering.” RadioGraphics. 2009;29:721-740.
30

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
CT Hypotension Complex
• “Shock Bowel” – Mucosal enhancement
– Submucosal edema
– Luminal distension
• Other: – Collapsed vena cava
– Adrenal hyperenhancement
– Peripancreatic fat stranding
– Hypoenhancing spleen
31

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 32

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Comparison Patient
• 41yo F with Hx IBS, colitis, HLD, atherosclerosis who presented with LUQ/LLQ pain and leukocytosis
• History notable for smoking, obesity, & family history of heart disease
• Intermittent flare-ups of acute, diffuse abdominal pain over preceding 3 yrs, associated with loose stools and 35 lb weight loss
33

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Comparison Patient 1
34
1 month prior to presentation
Occluded Celiac Artery
Stenosed SMA
PACS Axial C+ CT; PACS, BIDMC

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
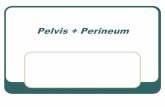
Comparison Patient 1
35
Portal venous gas Pneumatosis Coli
Axial C+ CT; PACS, BIDMC

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Comparison Patient 2
• 78yo F transferred from OSH for 2 days of NB/NB emesis, nonbloody diarrhea, and bilateral lower abdominal pain
• WBC 6.9, 77% PMNs
• VS on arrival: HR 120 BP 90/52 T99 O2 95% on 1L
• Abdominal distention with palpable loop of bowel
36

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Comparison Patient 2
37 Axial CT with PO Contrast; PACS, BIDMC
Portal venous gas Aortic calcification
Bowel wall thickening
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 38
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 39

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Management of Mesenteric Ischemia
Options:
• Emergent Surgery – Bowel Resection
• Stenting
• Thrombolysis
Prognosis:
• 50-90% mortality rate – Lactate level correlates with mortality
Julio Murra-Saca, gastrointestinalatlas.com
40

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Our Patient
• ~23:00 – Patient calls EMS; hypotensive to 70s; taken to ED
• ~23:30 – Patient arrives in ED; lactate of 5.0; central line placed; empiric antibiotics started
• 00:10 – Anterior T-wave inversions; Cards consult
• 00:30 – Bedside echo suggests decreased cardiac output and possible ischemia heparinized
41

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Our Patient, Contd • 01:30 – Patient complains of feeling “unwell”,
then becomes unresponsive, HR 40s, BP 50s, resuscitated with 1 round of CPR, atropine & Ca, intubated
• 02:05 – CT chest/abdomen with contrast shows mesenteric ischemia
• ~03:00 – Transfer to MICU
• Immediately after transfer, patient develops PEA arrest; CPR resumed
• After 10 more minutes of CPR, futility is determined and patient expires.
42

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Agenda
• Patient Presentation
• Differential Diagnosis
• Available Imaging Modalities
• Relevant Anatomy
• Radiologic Findings
• Pathophysiology
• Related Cases
• Patient Management & Disposition
• Take-Home Points 43
Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Pearls • In patients such as ours, mesenteric ischemia may be a
marker of other life-threatening conditions even if it is not the primary cause of death
• Mesenteric ischemia can be acute (from hypotension, hypovolemia, embolism) or chronic (from atherosclerosis)
• In patient with risk factors, always get abdominal CT with contrast to rule out mesenteric ischemia
• Weigh the risks and benefits of IV contrast in patients at risk for renal damage
• If mesenteric ischemia is on the differential must be excluded IMMEDIATELY no matter how remote
• Use radiologic findings to guide both prediction of outcome and amenability to therapy
• Keep VESSELS on list of organs that could cause pain when examining films.
44

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
References • “Acute Abdominal Pain and Fever or Suspected Abdominal Abscess.” ACR
Appropriateness Criteria. American College of Radiology, 2008. • Al-Shraim MM, Zafer MH, Rahman GA. Acute occlusive mesenteric ischemia in high
altitude of southwestern region of Saudi Arabia. Annals of African Medicine 2011;1:5-10.
• Ames JT, Federle, MP. “CT Hypotension Complex (Shock Bowel) is not always due to traumatic hypovolemic shock.” Am J Roentgenology. 2009:192:W230-W235.
• “Ascites.” Surgery Curriculum, Loyola University-Chicago. http://www.meddean.luc.edu/lumen/MedEd/Radio/curriculum/Surgery/Ascites.htm
• Broder, JS. “Mesenteric Ischemia.” Feature Article CME. EMedHome.com. 2011, Jan 1. • Donnan GA, Fisher M, Macleod M, Davis SM. “Stroke.” Lancet 2008;371:1612-1623. • Furukawa A, Kansaki S, Naoaki K et al. “CT Diagnosis of Acute Mesenteric Ischemia from
Various Causes.” Gastrointestinal Imaging. 2009;192:408-416. • Gray’s Anatomy of the Human Body, 20th Edition. • Helton WS, Fisichella PM. “Intestinal Obstruction” in ACS Surgery. WebMD. 2004. 4:10. • Johnson PT, Horton KM, Fishman EK. “Nonvascular Mesenteric Disease: Utility of
Multidetector CT with 3D Volume Rendering.” RadioGraphics. 2009;29:721-740. • Kaewlai R, Kurup D, Singh A. “Imaging of Abdomen and Pelvis: Uncommon Acute
Pathologies.” Seminars in Roentgenology. 2009;228-236. • Levy AD. “Mesenteric Ischemia.” Radiologic Clin N Am. 2007;593-599. • Macari M, Balthazar, EJ. “CT of Bowel Wall Thickening: Significance and Pitfalls of
Interpretation.” Am J Roentgenology. 2001;5:1105-1116. 45

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
References, contd • “Mesenteric Panniculitis.” New York – Presbyterian Emergency Medicine. Sept 2008.
http://nypemergency.org/radiology/radiology_2008/case-of-the-month-0908.html
• “Mesenteric Ischemia” in El Salvador Atlas of Gastrointestinal Video Endoscopy. http://www.gastrointestinalatlas.com/English/Jejuno_and_Ileum/Etc__Etc_/etc__etc_.html
• Mirvis SE, Shanmuganathan K, Erb R. “Diffuse Small-Bowel lschemia in Hypotensive Adults After Blunt Trauma (Shock Bowel): CT Findings and Clinical Significance.” Am J Roentgenology. 1994;163:1375-1379.
• Nishijima DK, Su M. “Mesenteric Ischemia in Emergency Medicine.” Medscape eMedicine. http://emedicine.medscape.com/article/758674-overview
• Oldenburg WA, Lau LL, Rodenberg TJ et al. “Acute Mesenteric Ischemia: A Clinical Review.” Arch Int Med. 2004;164:1054-1062
• Reeder MM. “G-69: Mesenteric Vascular Compromise.” in Reeder & Felson’s Gamuts in Radiology. Springer, 2003.
• Rha SE, H HK, Lee SH, et al. “CT and MR Imaging Findings of Bowel Ischemia from Various Causes.” RadioGraphics. 2000;20:29-42.
• “Universal differential diagnosis.” Musculoskeletal Radiology, University of Washington. http://www.rad.washington.edu/academics/academic-sections/msk/teaching-materials/online-musculoskeletal-radiology-book/general-principles
• Zafari AM. “Myocardial Infarction.” Medscape eMedicine. http://emedicine.medscape.com/article/155919-overview
46

Joseph M Reardon, HMS3
Gillian Lieberman, MD
3/2012
Acknowledgements
• Gillian Lieberman, MD
• Mark Masciocchi, MD, PGY1 reviewed the presentation and provided comparison cases
• Elizabeth Asch, MD, PGY2 reviewed the presentation and index case
• Grant Smith, HMS3; Christian Strong, HMS3; Michael Honigberg, HMS3
47