
Meeting Agenda Presentations on endpoints –Regulatory issues –Scientific issues Pros and cons of...
38
Meeting Agenda • Presentations on endpoints – Regulatory issues – Scientific issues • Pros and cons of end points – Classical end points – Non-classical end points • End points and trial designs according to lung cancer stage
-
Upload
suzanna-parrish -
Category
Documents
-
view
217 -
download
0
Transcript of Meeting Agenda Presentations on endpoints –Regulatory issues –Scientific issues Pros and cons of...

Meeting Agenda
• Presentations on endpoints– Regulatory issues– Scientific issues
• Pros and cons of end points– Classical end points– Non-classical end points
• End points and trial designs according to lung cancer stage

Presentations
• Regulatory background– General regulatory requirements– US lung cancer approvals – International lung cancer approvals
• Classical lung cancer end points
• Non-classical lung cancer end points

Outline of Presentation
• FDA requirements for new drug approval
• Regular approval of cancer drugs: end points used
• Accelerated approval
• Endpoints and issues

Requirements for Drug Approval
• Safety (FDAC, 1933)• Efficacy demonstrated in adequate and well
controlled studies (1962)• Basis for efficacy:
– Regular approval• Clinical benefit, or
• Established surrogate for clinical benefit
– Accelerated approval• Surrogate (reasonably likely to predict CB)

How many trials?• 505(d) of the Act:
Substantial evidence: “Adequate and well-controlled investigations”
• Single trial1:“generally only in cases in which a single multicenter
study of excellent design provided highly reliable and statistically strong evidence of an important clinical benefit… and a confirmatory study would have been difficult to conduct on ethical grounds.”
– 1Efficacy Guidance, May 1998

Oncology Efficacy Supplements
Only one additional trial may be needed for closely related indications:– Advanced cancer and earlier cancer– Different dosing regimens– New combinations of drugs
1Draft Guidance on New Cancer Treatment Uses, 1997.

Regular Approval Endpoints in Oncology

Clinical Benefit Endpoints Supporting Oncology Drug Approval
• Survival
• Improvement in tumor-related symptoms
• Disease-free survival (selected settings)

Established Surrogates Supporting Approval
• Complete response rates in some settings (e.g., acute leukemia)
• Partial response rate in some settings (e.g., hormonal treatment of breast cancer)

DODP: Endpoints for Approval (1/1/90 - 11/1/02)
Approvals not based on Survival: – 73% (48/66) of all approvals
– 67% (37/55) excluding accelerated approvals

Summary of Endpoints for DODP RegularApprovals (1/1/90 - 11/1/02) *
Total 55Survival 18RR 26 -RRalone -10 -RR+ Tumor Specific Symptoms -9 -RR+ TTP -7 Tumor Specific Symptoms 4DFS 2TTP 1Recurrence Malignant PleuralEffusion
2
Occurrence Breast Cancer 2* Derived from Johnson et al., JCO 21: 1404, 2003

Examples of endpoints in oncology
• Idarubicin -Prolonged remission in leukemia
• Zinecard -Protection from cardiac toxicity
• Photofrin -Dysphagia scale
• Aredia -Skeletal morbidity scale
• Daunozome -Visible lesions of KS
• Novantrone -Pain

Accelerated approval • Serious or life-threatening disease• Drug must provide benefit over available
therapy• Surrogate endpoint may be used• Surrogate endpoint must be reasonably
likely to predict clinical benefit• Post marketing studies must verify clinical
benefit

• Regular approval: clinical benefit or established surrogate
• Accelerated approval (AA): surrogate endpoint reasonably likely to predict clinical benefit.– AA used only when new treatment represents
benefit over available therapy– Sponsor must do phase 4 trial showing clinical
benefit
New Drug Approval Efficacy Requirement

Evidence for Accelerated Approval
• Substantial evidence from well controlled clinical trials regarding a surrogate endpoint
• NOT: Borderline evidence regarding a clinical benefit endpoint

ODAC Meeting on: Accelerated Approvals
(March 2003)
• 19 NDAs or BLAs for new treatment indications (involving 16 drugs)

DODP Accelerated Approvals
Drug IndicationSurrogateEndpoint
Liposomaldoxorubicin
Kaposi sarcoma Response
Docetaxel Breast cancer ResponseIrinotecan Colon cancer ResponseCapecitabine Breast cancer ResponseLiposomalcytarabine
Lymphomatismeningitis
Cytologic response
Temozolomide Anaplastticastrocytoma
Response
Liposomaldoxorubicin
Ovarian cancer Response
Gemtuzumabozogamicin
AML CR and CRp
Imatinib mesylate CML Response (Heme&Cyt)Imatinib mesylate GI stromal tumor
(GIST)Response
Oxaliplatin Colon cancer Response and TTPAnastrozole Breast cancer
(Adjuvant)Disease-free survival

ODAC Meeting on: Accelerated Approvals
(March 2003)
• Confirmatory studies should be part of drug development plan
• Early discussion of confirmatory studies with Agency
• ODAC wanted to be consulted on confirmatory study plans

Single Arm Trials (SAT) and Accelerated approval (AA)
• SAT require few patients
• SAT for AA limit study to refractory disease
• SAT have limited ability to evaluate valuable endpoints such as TTP, QOL, and Survival

Randomized Trials (RT) and Accelerated approval (AA)
• More patients and time• Allows AA at any disease stage
(surrogate beats available therapy)
• Allows “add-on” design (A vs A + B)
• Allows a variety of endpoints– Time to event (TTP, survival)– Endpoints requiring blinding (symptoms, QOL)
• Defines individual drug contribution– (oxaliplatin vs 5FU/LCV versus oxaliplatin + 5FU/LCV)

Endpoints and Issues

Survival
• Gold standard
• Superiority design: beat anything
• The crossover problem
• Non-inferiority design: problematic with current regimens

Superior A/Pla
Hazard Ratio = 1
No sign. diff. A/C
Non inferior A/C
AB (placebo)
Established effect of A
Non-inferiority trials
.5 .8

Tumor Response Rate
• Can be assessed in single-arm study
• Documents activity in a subset of patients
• When can it be considered an established surrogate?– Suggested as such by ODAC for topotecan
treatment of refractory small cell lung cancer
• When can it be considered a “reasonably likely surrogate”?– ODAC, lung cancer discussion 2002

• Does it measure clinical benefit?
• Is it reliable?
TTP: Critical Regulatory Questions

• Measured in all patients
• Measures cytostatic activity
• Progression is often the basis for change in therapy
• Assessed before crossover
• Requires smaller studies
• ?Face validity
TTP: Advantages

• Indirect measure of patient benefit.
• Unclear clinical meaning of small TTP difference
• Expensive to measure carefully
• Reliability in unblinded setting?
• Unknown reliability of small TTP difference with usual trial monitoring
TTP: Problems
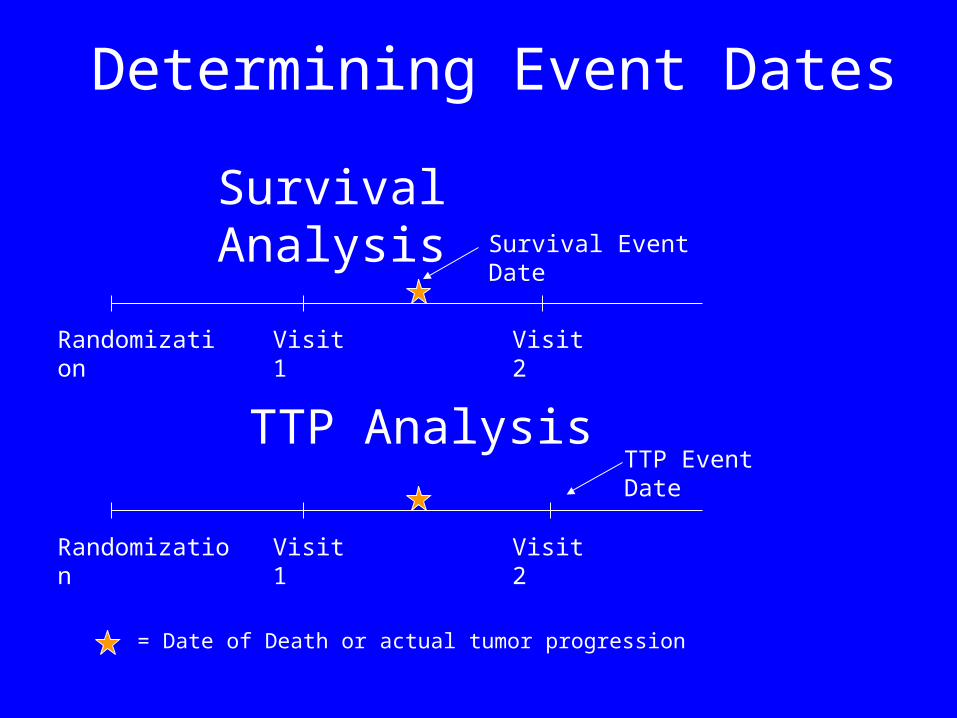
Visit 1 Visit 2Randomization
= Date of Death or actual tumor progression
Survival Event Date
Visit 1 Visit 2Randomization
TTP Event Date
Survival Analysis
TTP Analysis
Determining Event Dates

Tumor-Related Symptoms
• Evaluation of patient morbidity has supported many NDA approvals
• Major impediments– Lack of blinding– Missing data
• Time to symptomatic progression– Frequently discussed, not yet successful

Review of Presentation
• FDA requirements for new drug approval
• Regular approval of cancer drugs: end points used
• Accelerated approval
• Endpoints and issues


Endpoints Discussion
• Classical end points (pros and cons)
• Non-classical end points (pros and cons)
• Discussion according to stage
(End points and trial designs)

1. What are the Pros and Cons of each end point:
• As a regular approval endpoint?(A measure of clinical benefit or a reliable
surrogate)
• As an accelerated approval endpoint?(A surrogate reasonably likely to predict
clinical benefit)
• As a secondary end point for labeling?

2. For each endpoint, what are the important trial design issues?

Classical Endpoints
• Survival
• Response Rate
• Time to progression
• Disease-free Survival

Non-classical endpoints
• Specific quality of life instruments
• Assessment of tumor-specific symptoms

Treatment settings
• Neoadjuvant
• Adjuvant
• First-line therapy
• Second-line and subsequent therapy

Trial designs
• Superiority design (A beats B)
• Add-on design (A+B beats A)
• Non-inferiority design (e.g., A + B is non-inferior to A + C)


















