
Med Student Paed Cardiol Infant
52
Congenital Heart Disease Abbreviations VSD ventricular septal defect ASD atrial septal defect PS pulmonary stenosis AS aortic stenosis HLHS hypoplastic left heart syndrome TAPVC/D totally anomalous pulmonary venous connection/drainage TGA transposed great arteries PFO patent foramen ovale PDA patent ductus arteriosus CAVC- complete Atrioventricular canal defect (PAPVC- partial= ostium primum ASD) AV valve- atrioventricular valve (usually mitral or tricuspid)
-
Upload
jennifer-dixon -
Category
Documents
-
view
12 -
download
2
description
PEDS CARDIOL
Transcript of Med Student Paed Cardiol Infant
Congenital Heart Disease Abbreviations
VSD ventricular septal defect ASD atrial septal defect PS pulmonary stenosis AS aortic stenosis HLHS hypoplastic left heart syndrome TAPVC/D totally anomalous pulmonary venous connection/drainage TGA transposed great arteries PFO patent foramen ovale PDA patent ductus arteriosus CAVC- complete Atrioventricular canal defect (PAPVC- partial=
ostium primum ASD) AV valve- atrioventricular valve (usually mitral or tricuspid)
Congenital Heart Disease
Commonest group of life threatening anomalies
8/1000 live births» VSD 30-50%, PDA 10%, ASD 7%.» PS 7%» Coarctation 6%, AS 5%» Tetralogy 5%, TGA 5%» AV canal defects 3%
Fetal Physiology
Right-to-left shunting at atrial level (PFO) and at arterial level (ductus arteriosus)
High pulmonary vascular resistance Little pulmonary blood flow Ventricles work in parallel
Presentation During Fetal Life
Valve regurgitation (especially TR, also CAVC, Truncus)
Arrhythmia- Slow (complete heart block)- Fast (usually atrial arrhythmias)
May cause fetal loss or hydrops
Transition From the Fetal Circulation
Pulmonary vascular resistance falls Ductus venosus and ductus arteriosus close Right-to-left shunting through foramen ovale
ceases
Timing of these events determines the timing of presentation of congenital heart
defects
How will this baby look at 12 hours of
age?
Presentation First 24 Hours
Critically ill” - like asphyxia
Cyanosis (may be mild) Pure heart failure is
uncommon Murmur
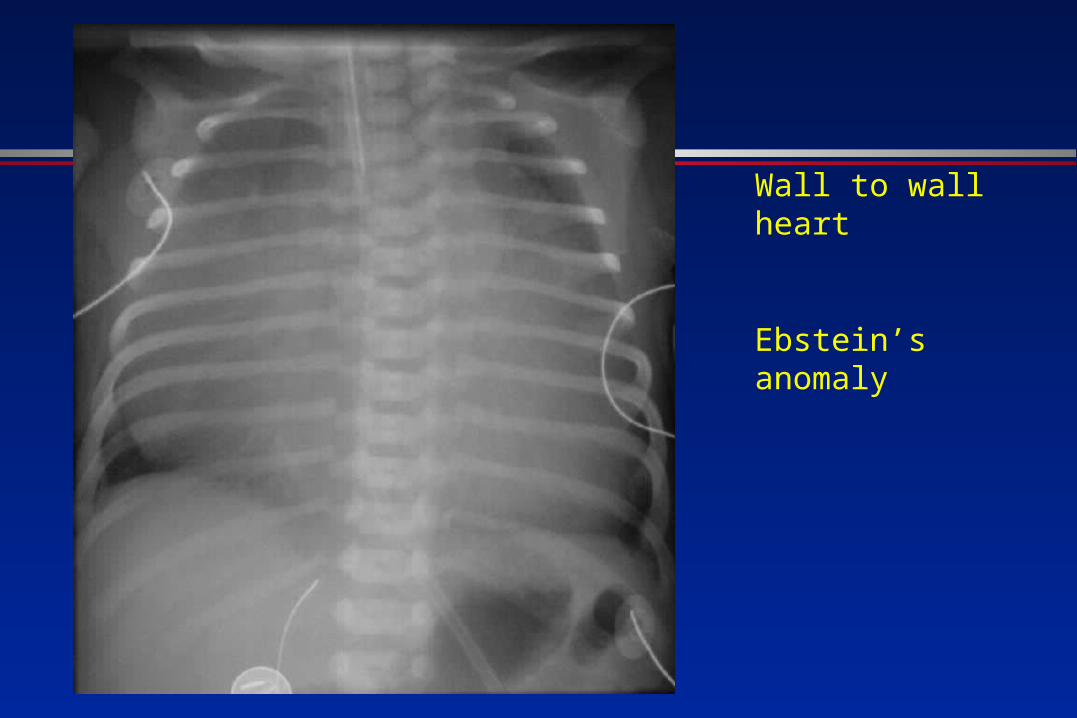
Wall to wall heart
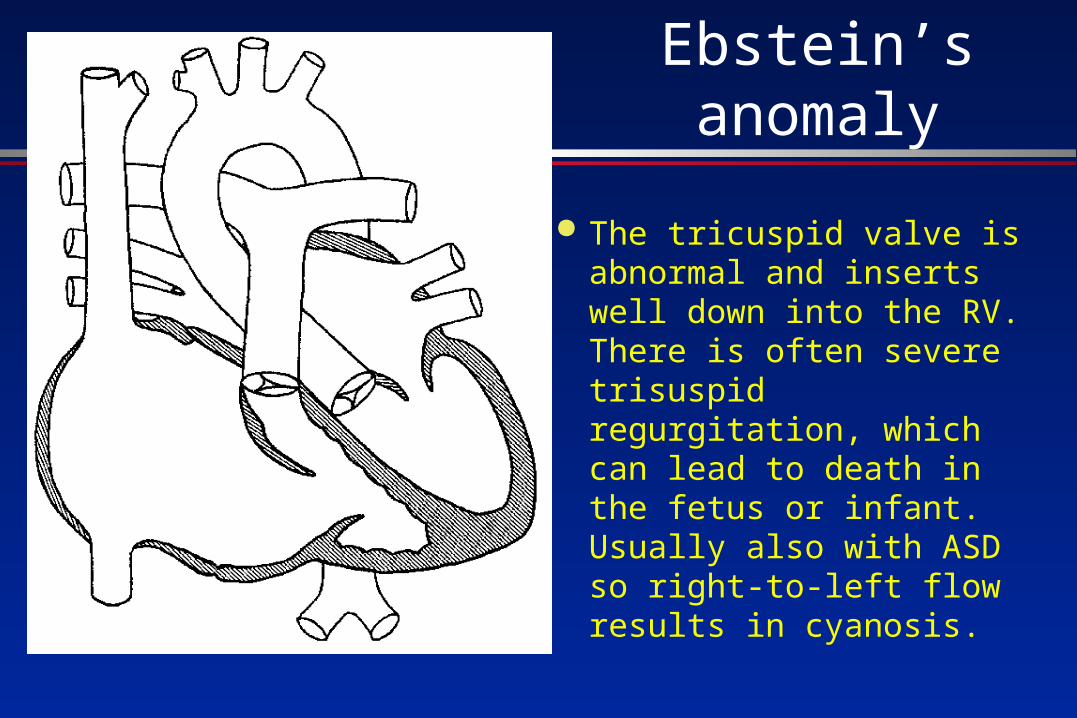
Ebstein’s anomaly
Ebstein’s anomaly
The tricuspid valve is abnormal and inserts well down into the RV. There is often severe trisuspid regurgitation, which can lead to death in the fetus or infant. Usually also with ASD so right-to-left flow results in cyanosis.
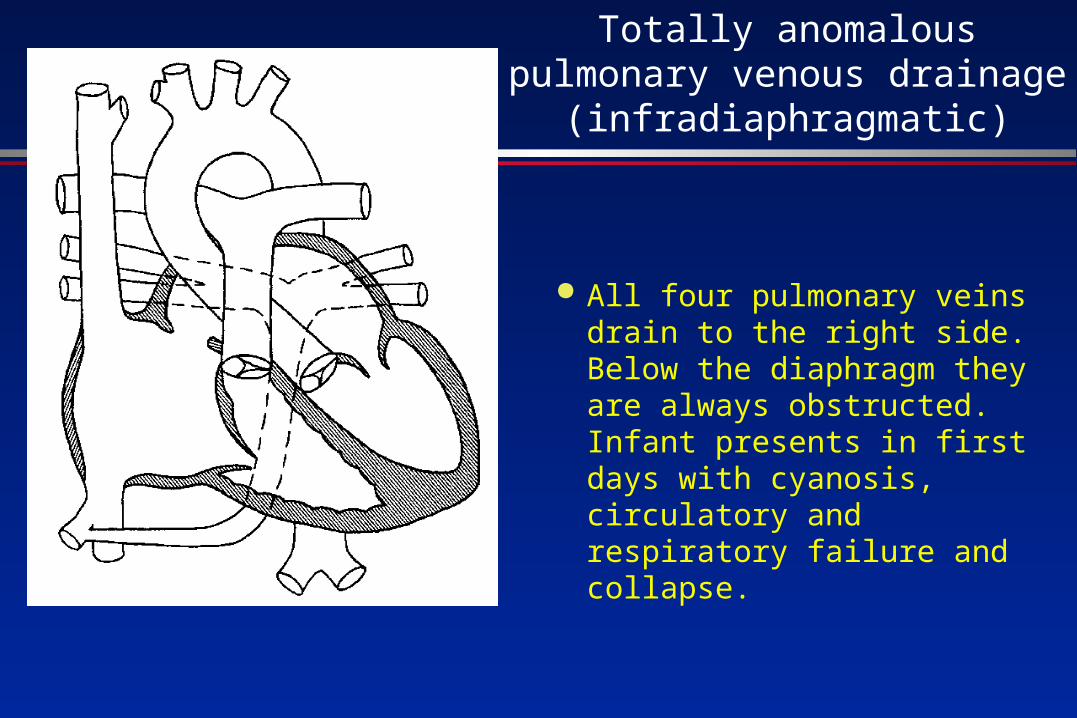
Totally anomalous pulmonary venous drainage
(infradiaphragmatic)
All four pulmonary veins drain to the right side. Below the diaphragm they are always obstructed. Infant presents in first days with cyanosis, circulatory and respiratory failure and collapse.
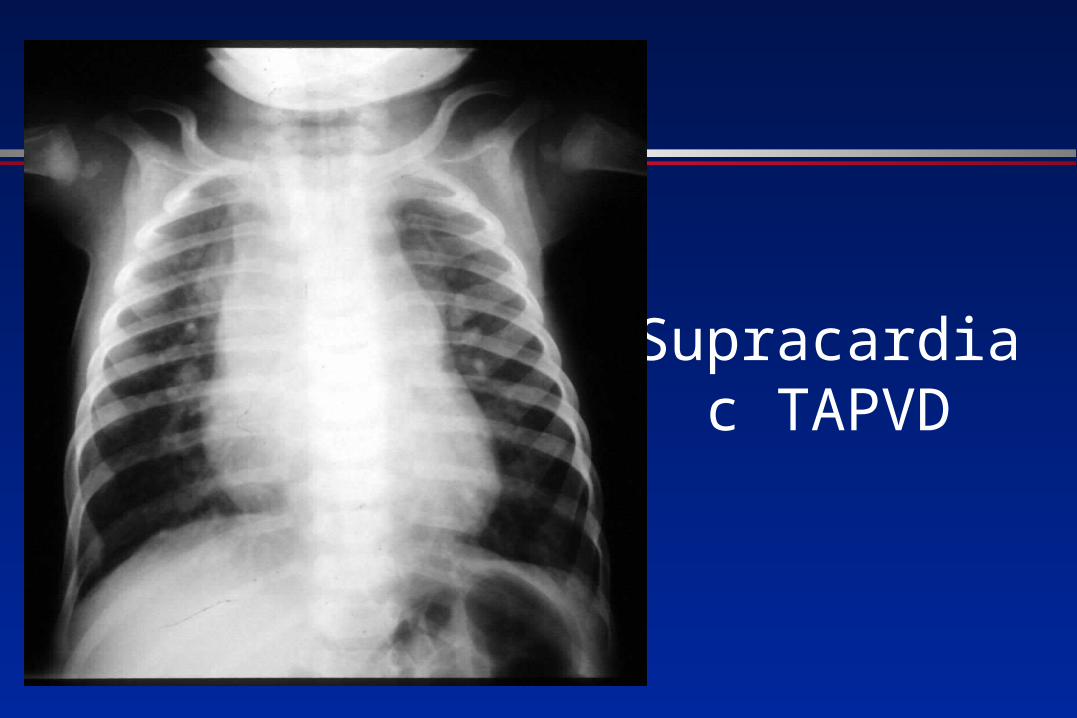
Supracardiac TAPVD
Presentation First 24 Hours
Critically ill: Valve regurgitation especially Ebstein's,
absent pulmonary valve syndrome Obstructed TAPVD “Early” duct dependent presentation Respiratory distress is usually not of
cardiac cause at this age
24 Hours to 2 weeks = 3 types of “Ductal Dependent” Lesions
Depend on patent duct for either» pulmonary blood flow,» systemic blood flow, or» mixing of systemic and pulmonary blood
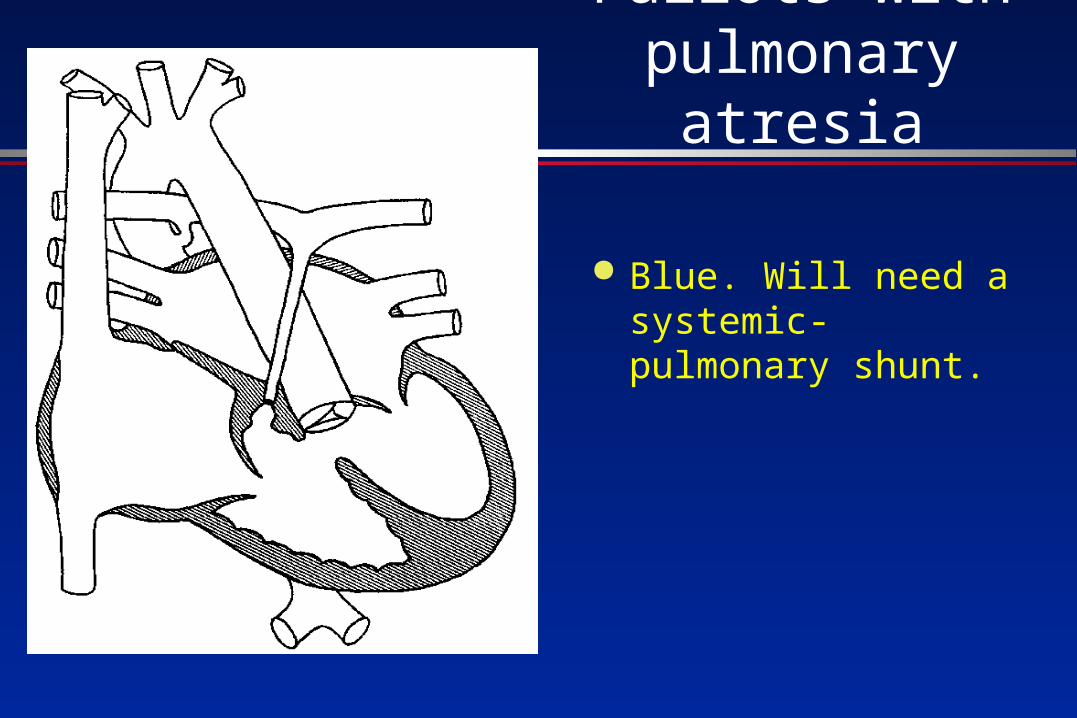
Fallots with pulmonary atresia
Blue. Will need a systemic- pulmonary shunt.
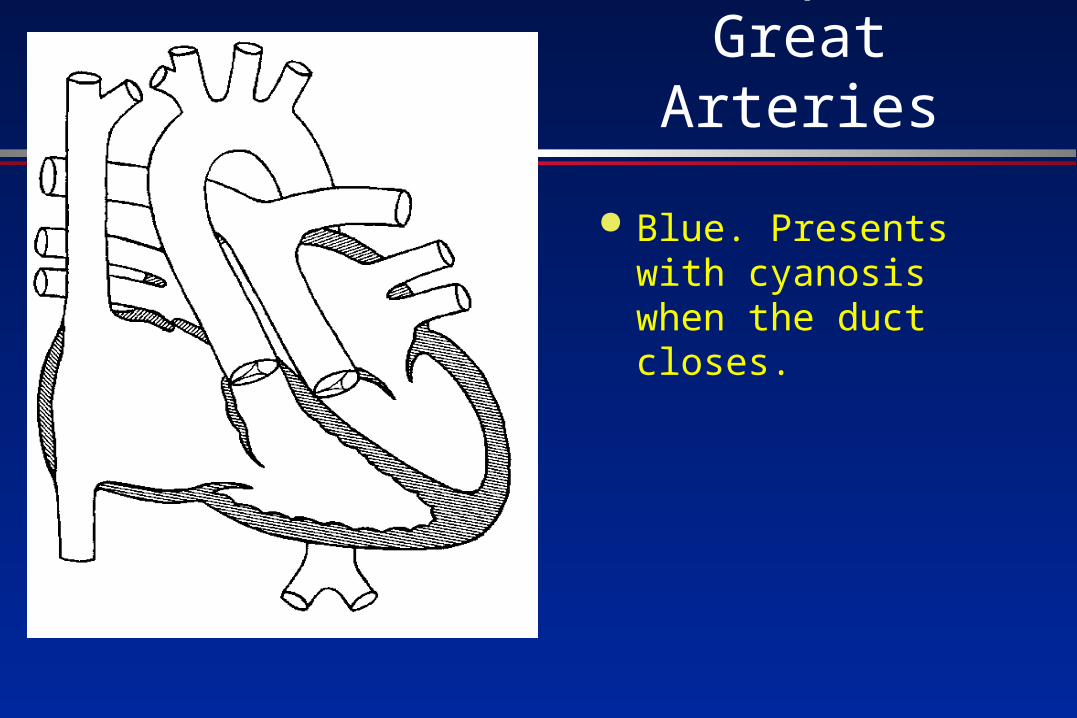
Transposed Great Arteries
Blue. Presents with cyanosis when the duct closes.
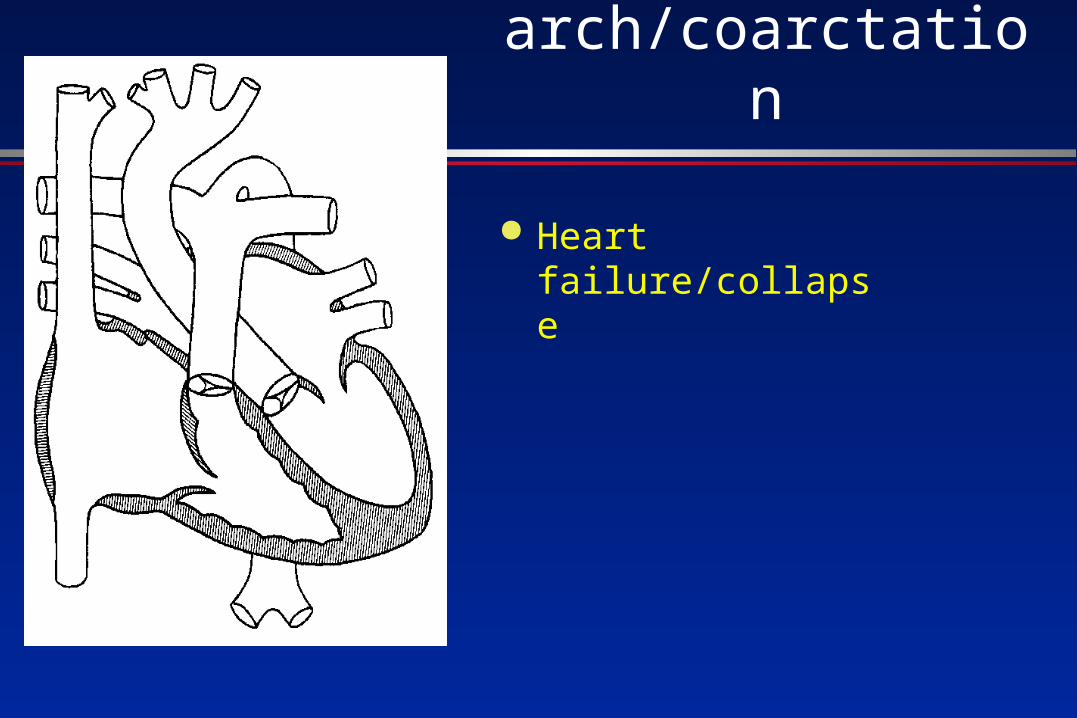
Interrupted aortic arch/coarctation
Heart failure/collapse
24 Hours to 2 Weeks Cyanotic “Ductal-Dependent” Lesions
CXR helps in diagnosis- oligaemic lungfields
PS, pulmonary atresia etc- plethoric lungfields
TGA- congestion
TAPVD- massive cardiomegaly
Ebstein’s
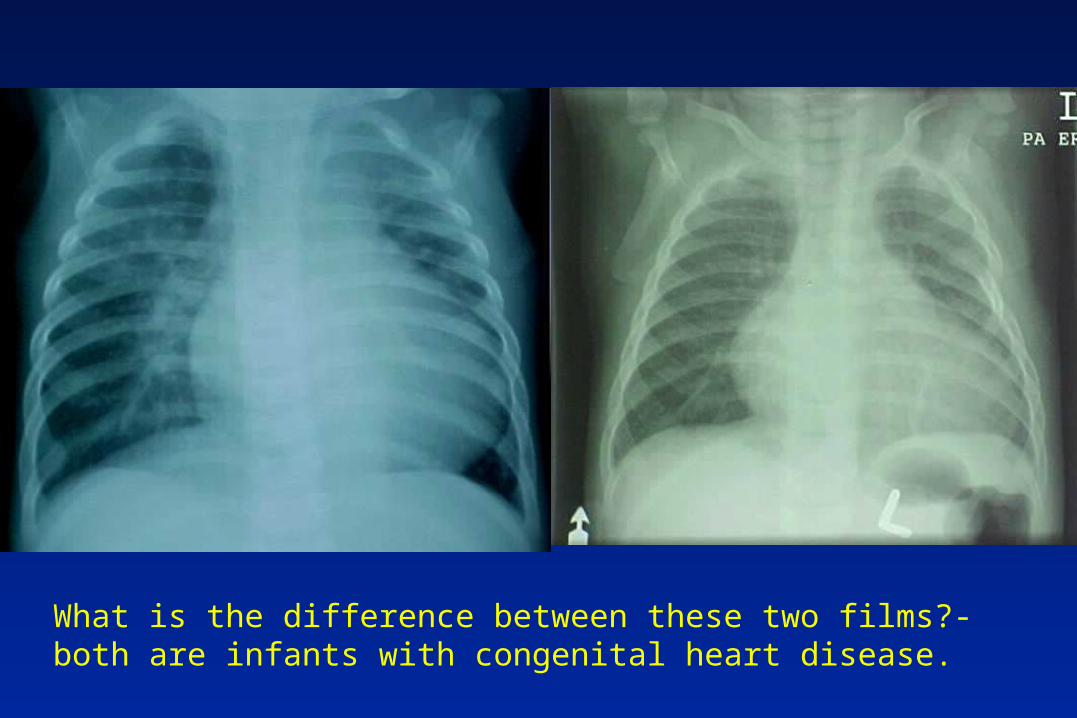
What is the difference between these two films?-both are infants with congenital heart disease.
Cyanotic infant- a lung problem or a heart problem?
Investigations- suggests heart if:- CXR- clear lung fields and- ECG- normal and- Hyperoxia test normal ( breathing 100%
oxygen, if pO2 >150mmHg very unlikely to be cyanotic heart disease)
- (Echocardiogram is the definitive test)
24 Hours to 2 Weeks Heart failure “Ductal-Dependent” Lesions
Heart failure is due to left heart obstruction NOT L-R shunts at this age! eg.» Coarctation» Critical Aortic stenosis» Hypoplastic left heart» Mitral stenosis (rare)
Symptoms of cardiac failure in the infant
Poor feedingFailure to thriveFatigue
Signs of cardiac failure in the infant
TachypnoeaTachycardiaHepatomegallySweating
2 - 6 WeeksDecreasing Pulmonary Vascular Resistance
Congestive heart failure due to L-R shunt: eg.» Large VSD, PDA, CAVC» Truncus, single ventricle with no PS» Earlier presentation if combined with
left heart obstruction eg coarctation
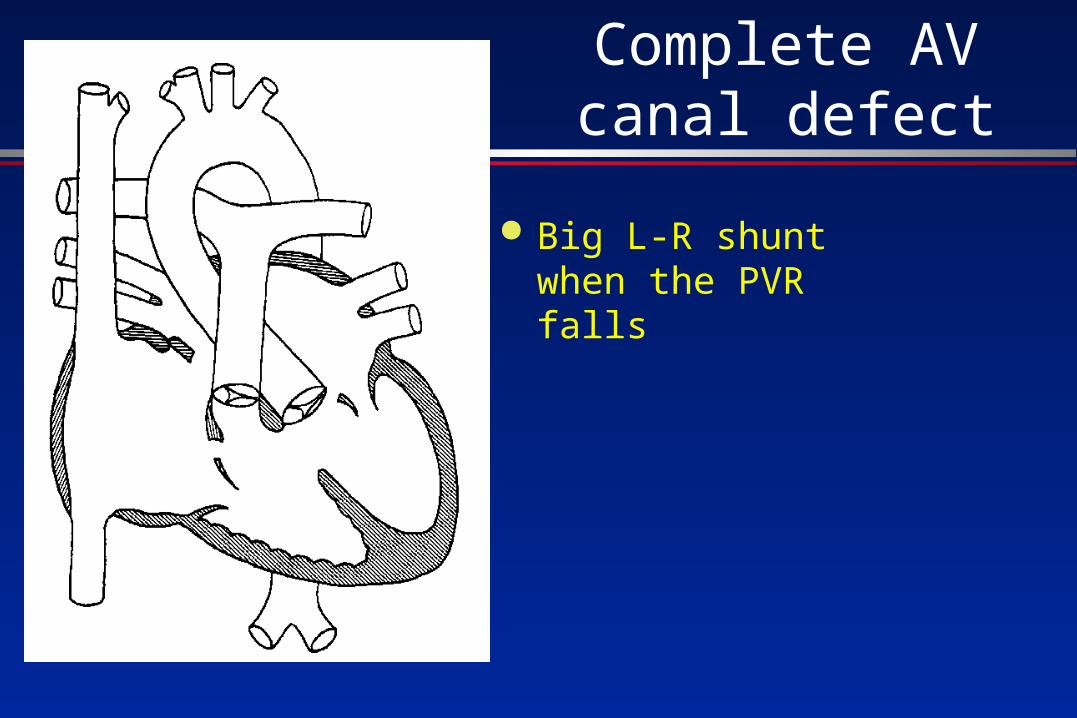
Complete AV canal defect
Big L-R shunt when the PVR falls
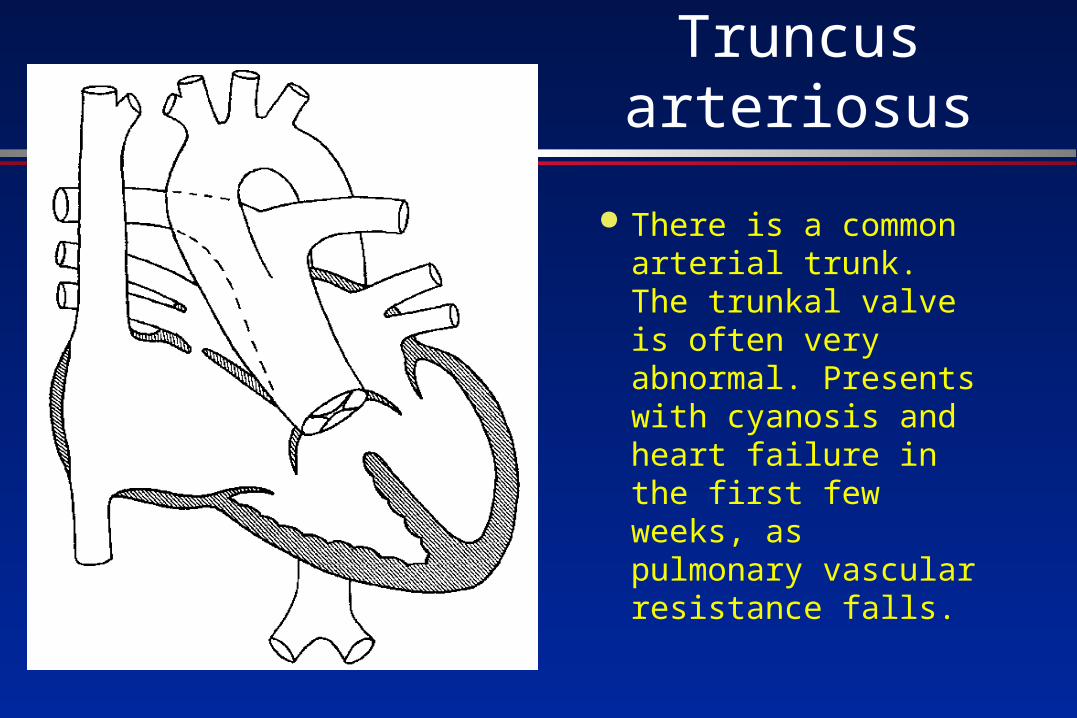
Truncus arteriosus
There is a common arterial trunk. The trunkal valve is often very abnormal. Presents with cyanosis and heart failure in the first few weeks, as pulmonary vascular resistance falls.
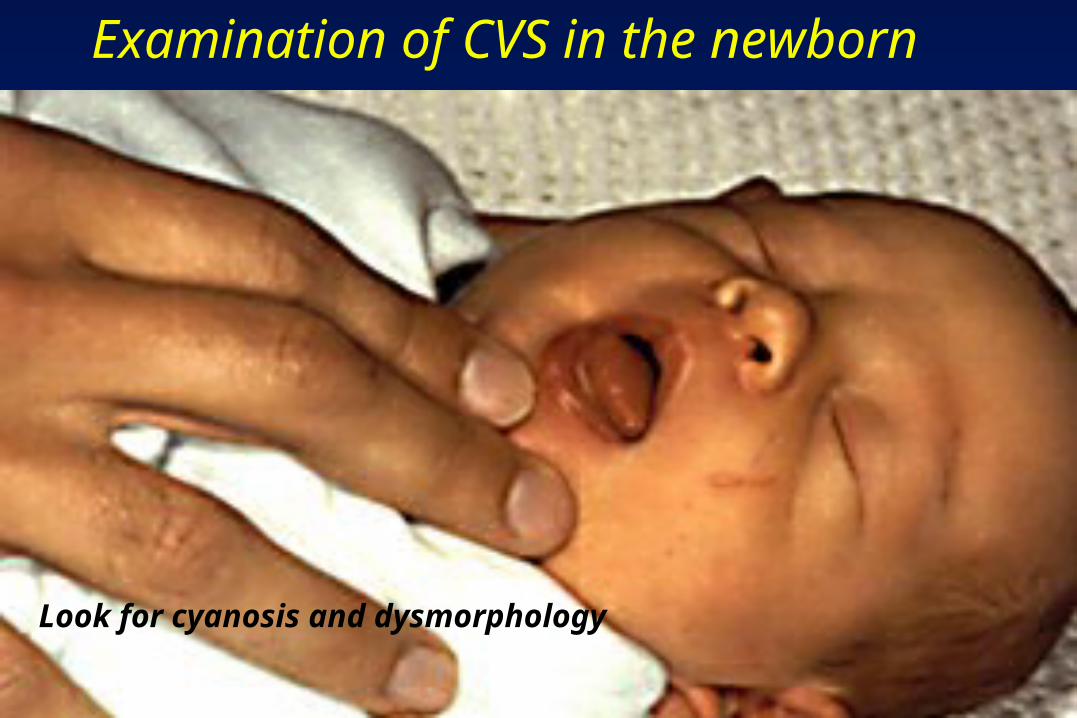
Look for cyanosis and dysmorphology
Examination of CVS in the newborn

Diagnosis?
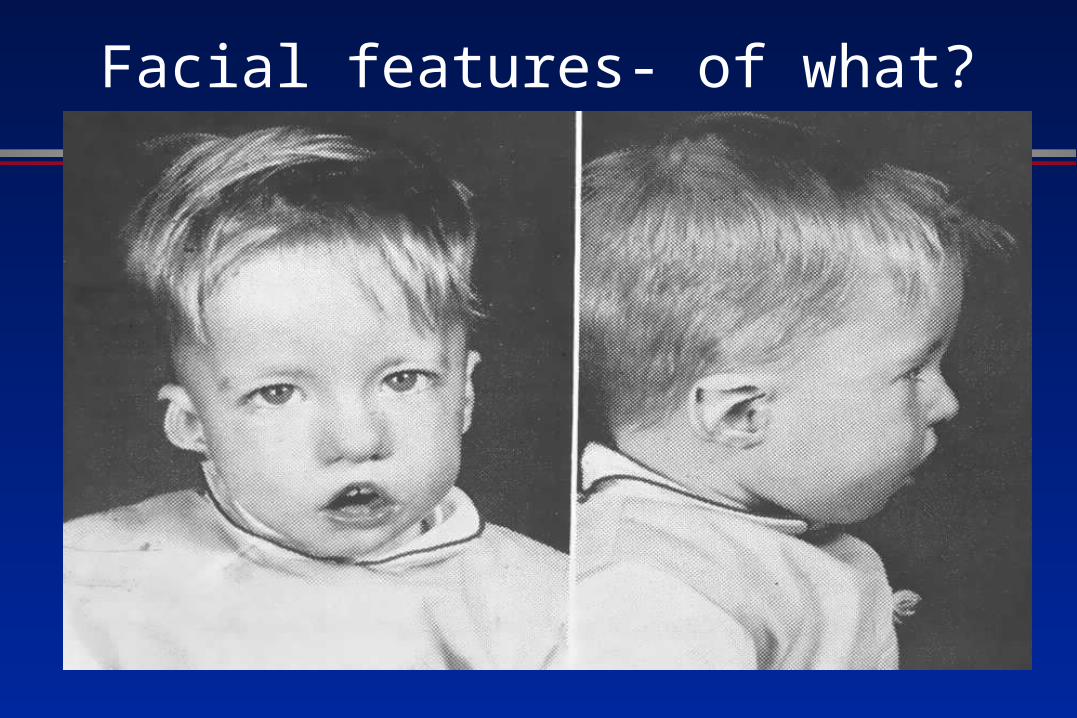
Facial features- of what?
What syndrome is associated with Truncus arteriosus/
tetralogy/interrupted aortic arch?
DiGeorge syndrome
Thymic aplasia (T-cell, immune problems) Hypocalcaemia (hypothyroid gland aplasia,
seizures) Dysmorphism (unusual facial appearance) Outflow tract abnormalities in the heart
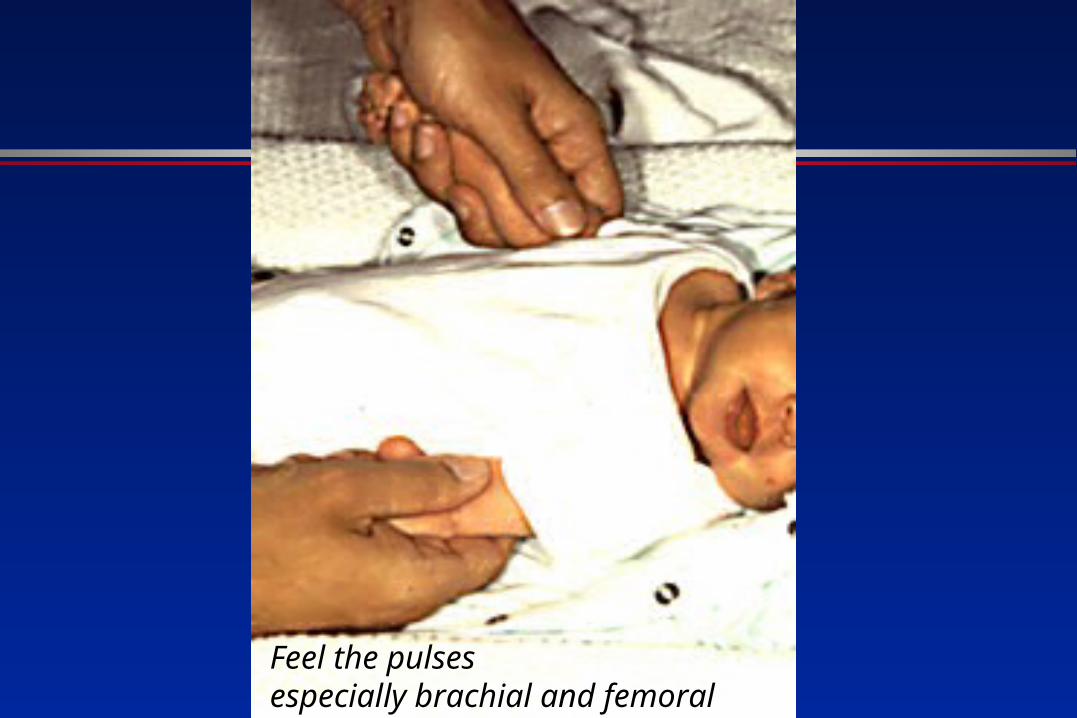
Feel the pulsesespecially brachial and femoral
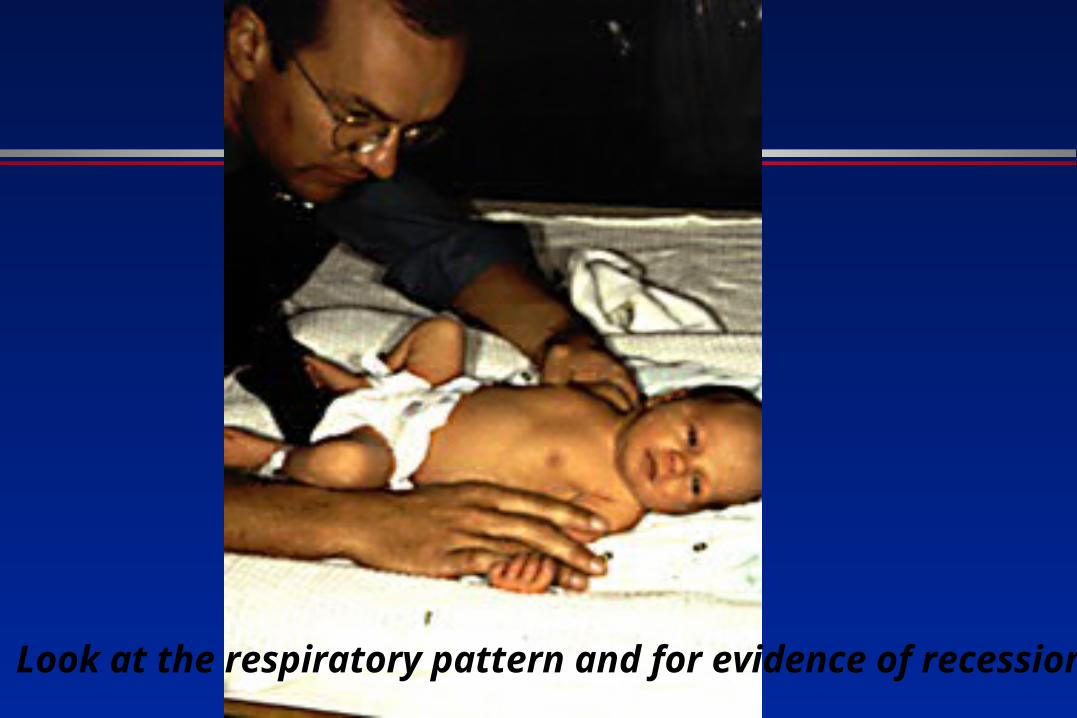
Look at the respiratory pattern and for evidence of recession
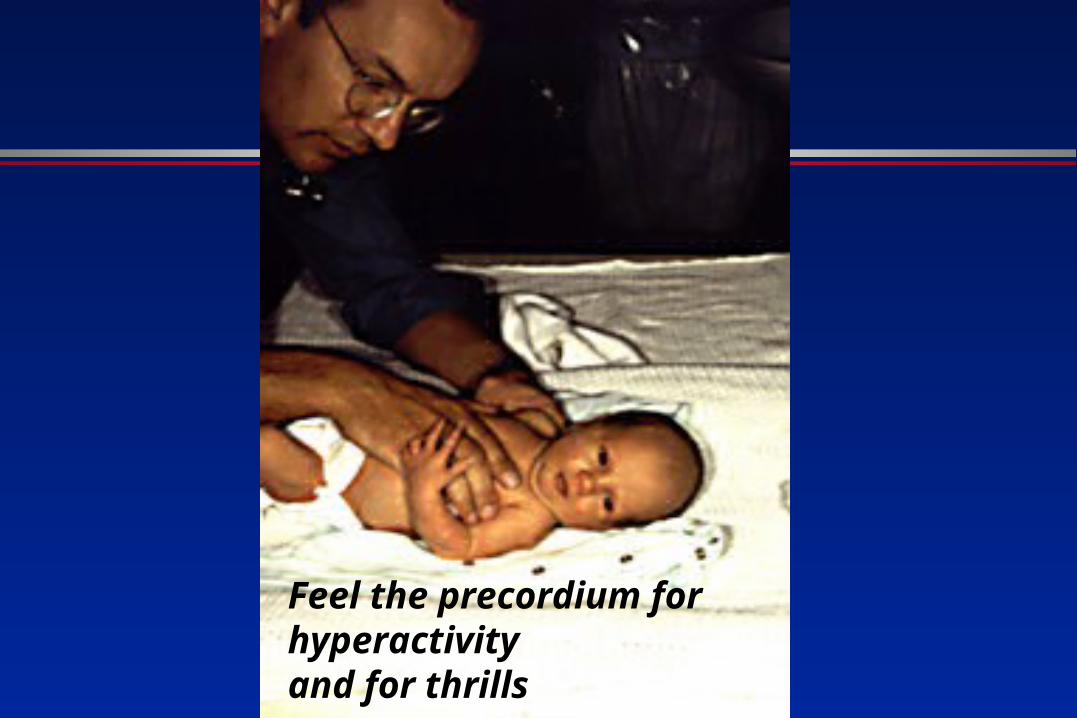
Feel the precordium for hyperactivityand for thrills

Locate the apex beat

Feel for hepatomegally

Listen carefully
Do what is necessary to calm the baby down!

Listen at the back for radiation of murmurs

3 months old- severe failure to thrive
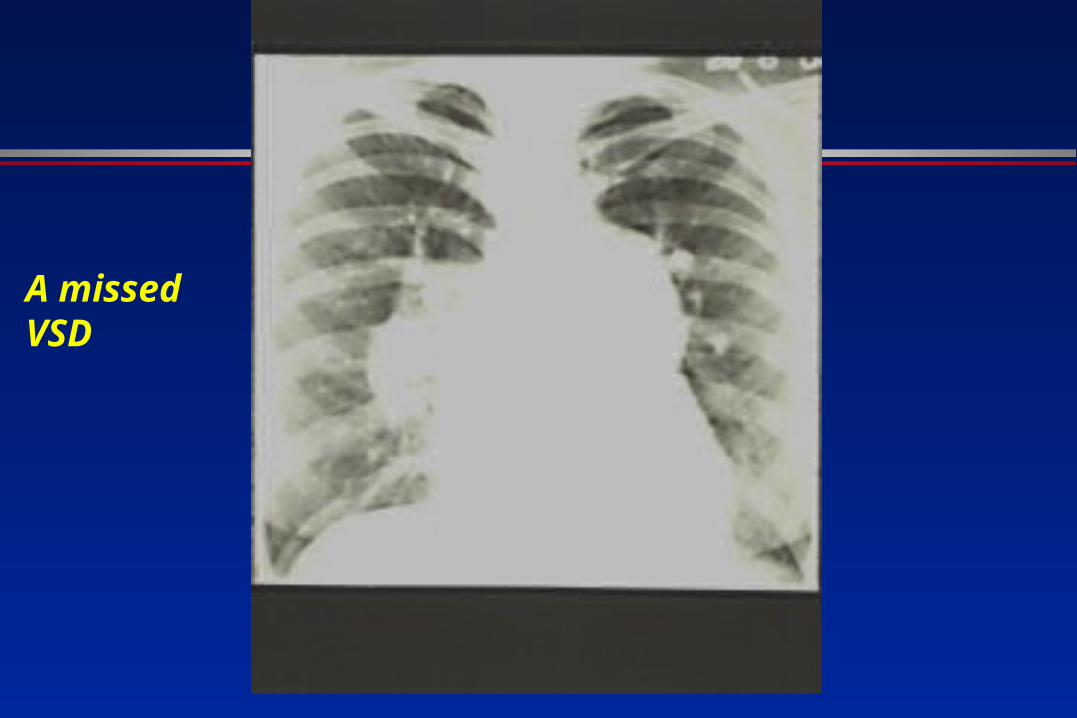
A missed VSD
Special tests- echocardiography
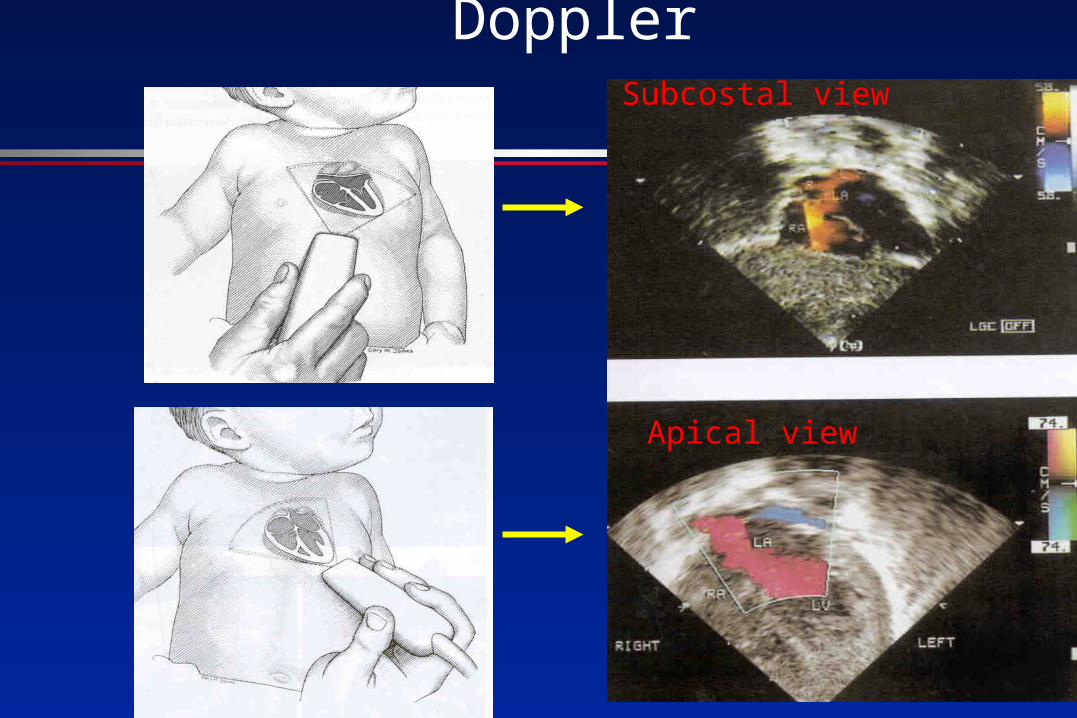
Pulmonary veins - colour DopplerSubcostal view
Apical view
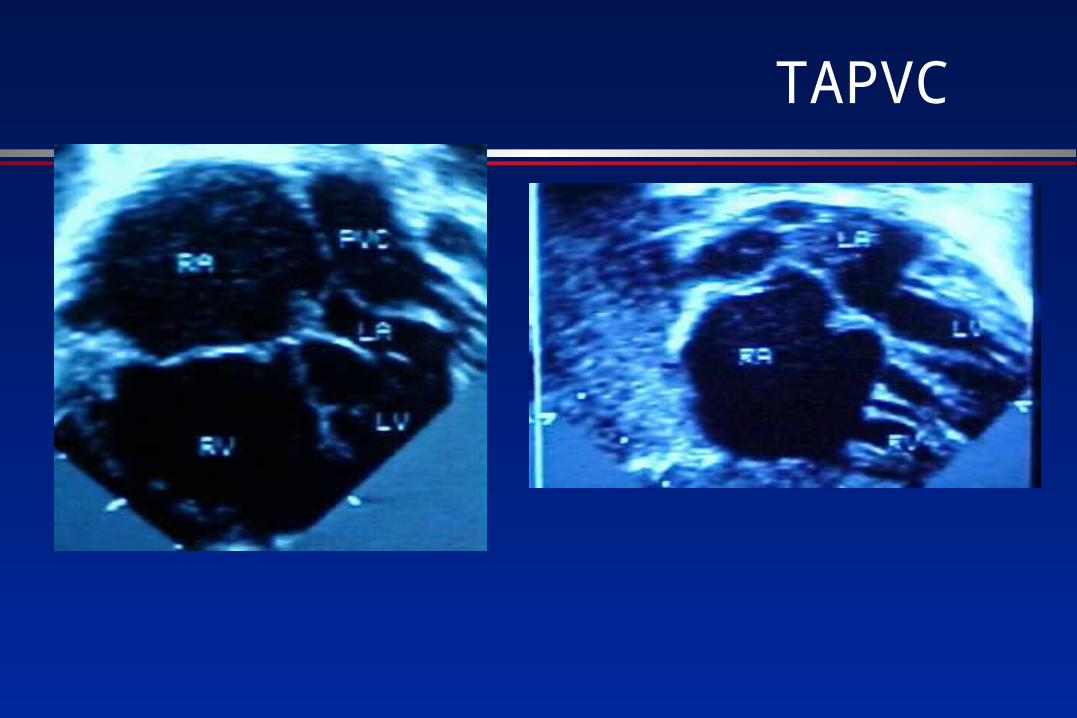
TAPVC
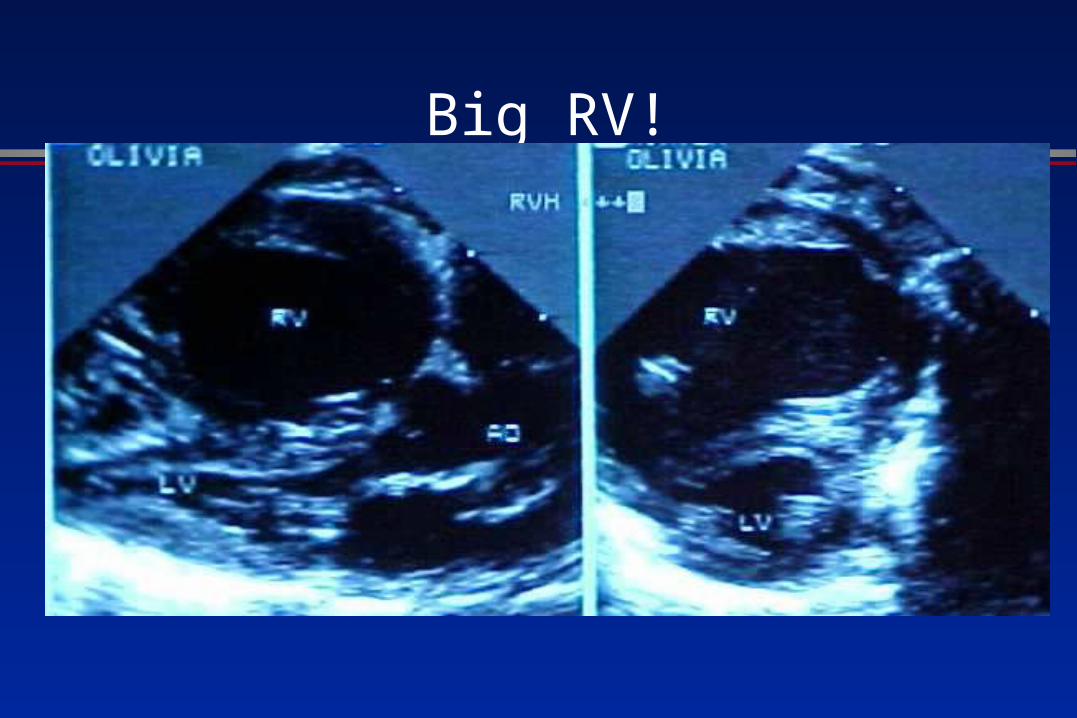
Big RV!
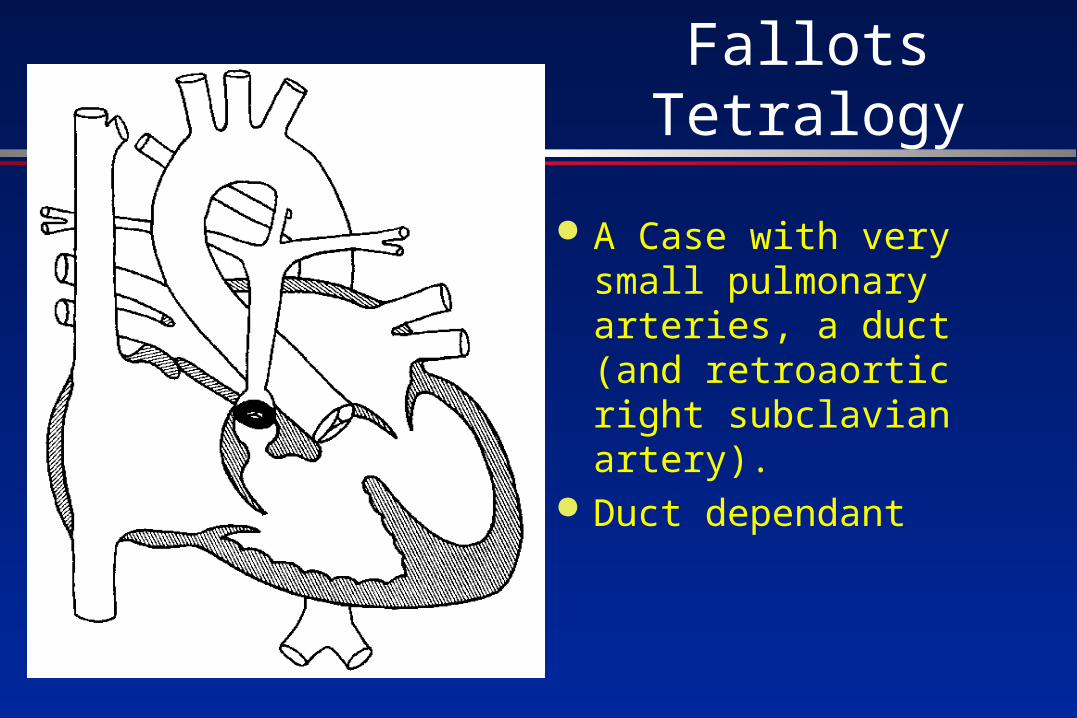
Fallots Tetralogy
A Case with very small pulmonary arteries, a duct (and retroaortic right subclavian artery).
Duct dependant
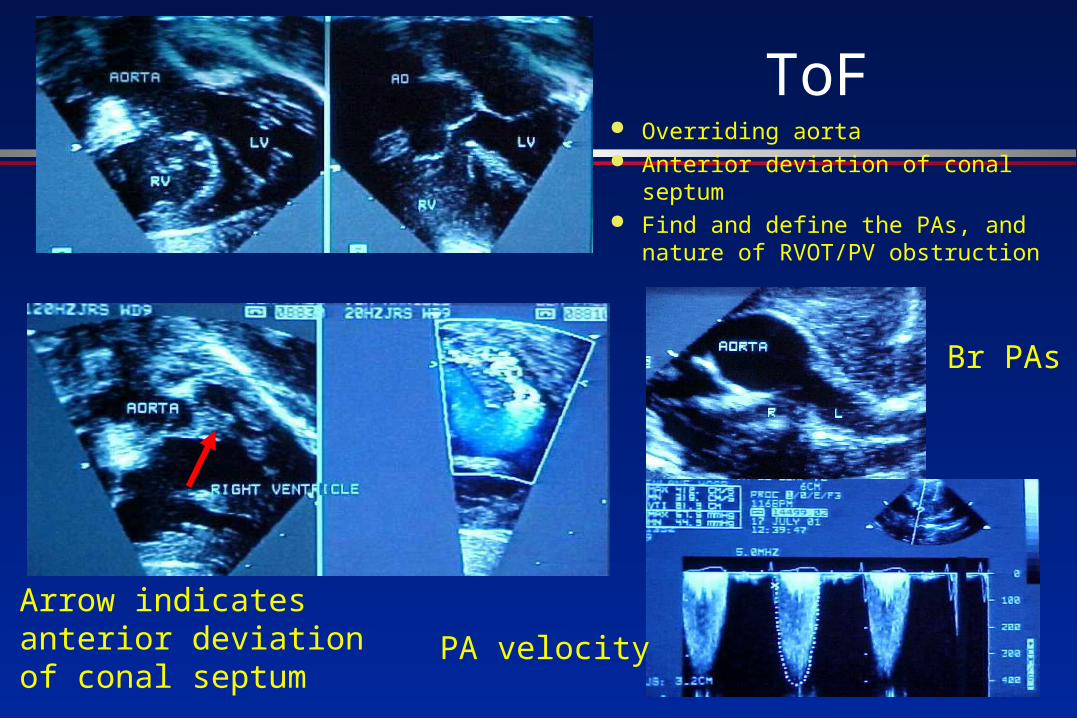
ToF Overriding aorta Anterior deviation of conal septum Find and define the PAs, and
nature of RVOT/PV obstruction
Arrow indicatesanterior deviationof conal septum
Br PAs
PA velocity
Newborn with heart failure-heart rate <200bpm- miles
from help- do what m?
Blue newborn- no respiratory distress- miles from help- do
what?
Learn your ABC!
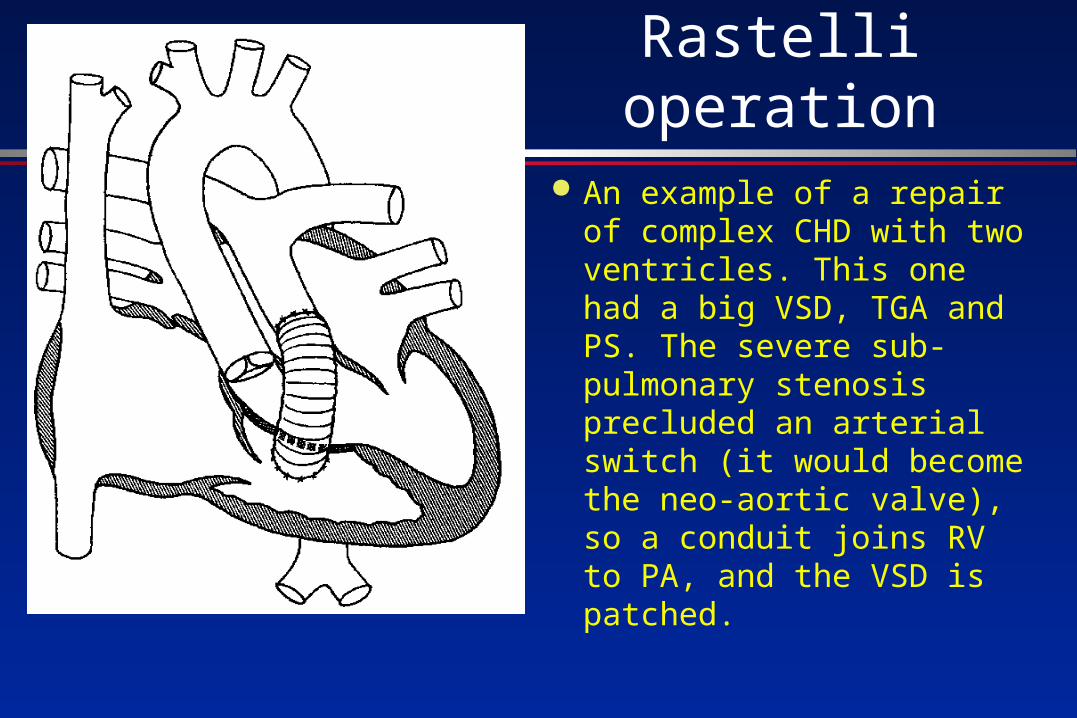
Rastelli operation An example of a repair of
complex CHD with two ventricles. This one had a big VSD, TGA and PS. The severe sub-pulmonary stenosis precluded an arterial switch (it would become the neo-aortic valve), so a conduit joins RV to PA, and the VSD is patched.
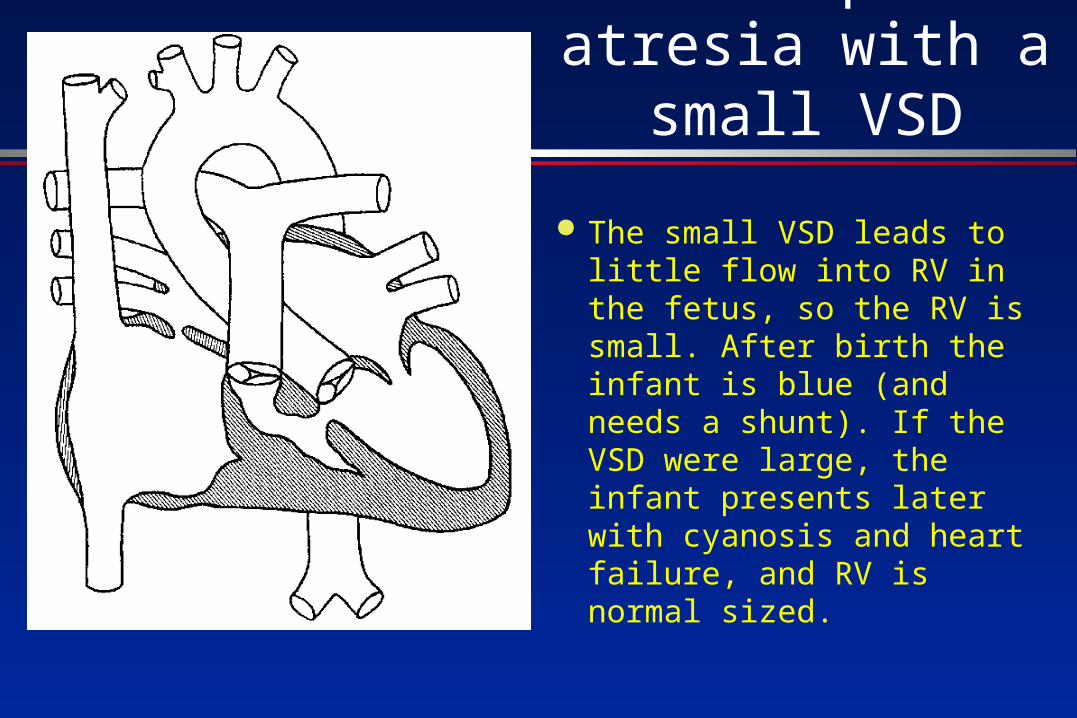
Trisupid atresia with a small VSD
The small VSD leads to little flow into RV in the fetus, so the RV is small. After birth the infant is blue (and needs a shunt). If the VSD were large, the infant presents later with cyanosis and heart failure, and RV is normal sized.
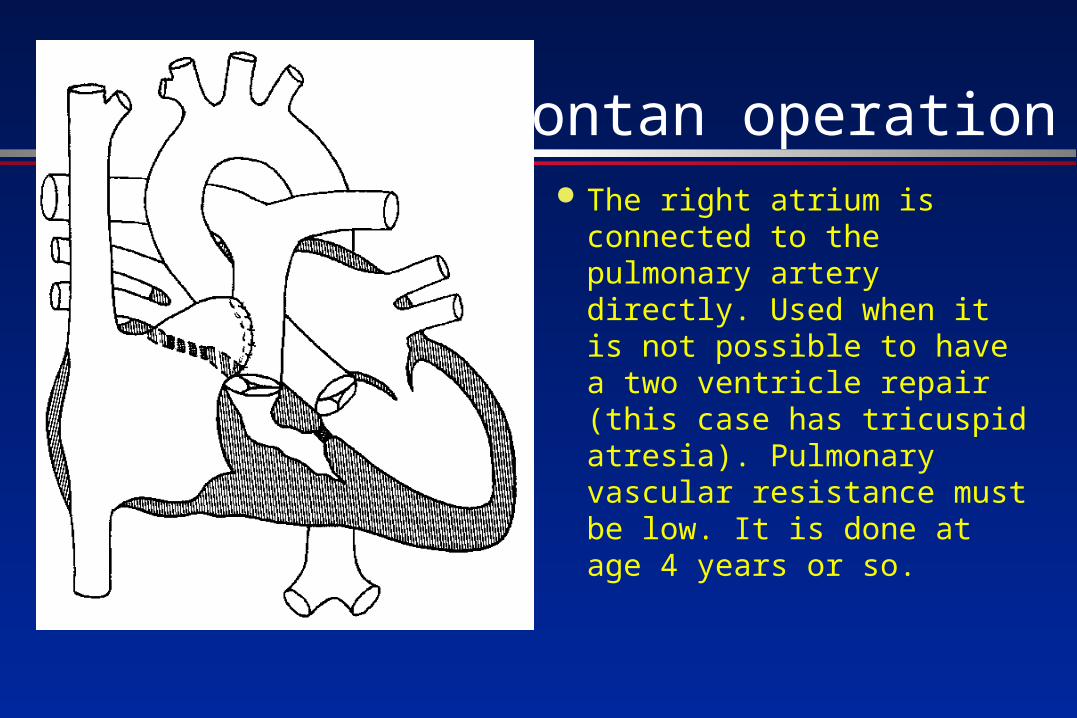
Fontan operation The right atrium is
connected to the pulmonary artery directly. Used when it is not possible to have a two ventricle repair (this case has tricuspid atresia). Pulmonary vascular resistance must be low. It is done at age 4 years or so.


















