
McHenry Western Lake County EMS System Mandatory CE for ... · McHenry Western Lake County EMS...
31
McHenry Western Lake County EMS System Mandatory CE for Paramedics, EMT-B and PHRN’s SOP Rollout - Medications Online CE 2017 With the roll out of the 2017 MWLC Region IX SOP, there is going to be some changes in medications, dosages of medications and responsibilities of who can administer these medications. This CE is going to cover some basic aspects of these medications including; the different names, some basic functions and how to administer them. This will be a review for some and new information for others. This will be a good way for all of us to make sure we are all on the same page. General Aspects of Medications All medications have four names: Brand Name, Generic Name, Official Name and Chemical Description. The Chemical Description is used to help identify what a specific medication does. The Official Name is how the medication is listed in the United States Pharmacopeia (USP). The Brand Name is how the manufacturer sells their product. (This is usually what promotes loyalty to the brand. Think about people that ask for Tylenol or Motrin when they have a headache. Both of them do very different things, but most people just know the name of the medication that usually works for them.) The Generic Name is made by the manufacturer and once the rights are given up, is a way for the drug to be sold without the Brand name. The following is an example of the four names for Valium: 1 Brand Name: Valium Generic Name: diazepam Official Name: diazepam, USP Chemical Name: 7-chloro-1,3-dihydro-1-methyl-5-phenyl-2H-1,4-benzodiazepin-2-one There are four sources for medications: Plant, Animal, Mineral and Synthetic. A lot of the medications that are made in a lab (or are manufactured) have their origins in plants and animals. With advances in chemistry, we were able to isolate and reproduce the effect certain plants have on the body and turn it into a pill. Generally, medications do not add anything to the body. What they do is modify or exploit existing functions of the body. Medications aren’t able to limit their effect on only one area of the body, so they can affect multiple systems, this is a side effect. A contraindication means that the medication will cause a worse problem or create a situation that the patient may not recover from. Nitroglycerin is a good medication to consider. There are side effects and contraindications that need to be understood. The patient’s blood pressure can fall once the Nitroglycerin has been given (side effect). Nitroglycerin is stopped if the
Transcript of McHenry Western Lake County EMS System Mandatory CE for ... · McHenry Western Lake County EMS...
McHenry Western Lake County EMS System Mandatory CE for Paramedics, EMT-B and PHRN’s
SOP Rollout - Medications Online CE 2017
With the roll out of the 2017 MWLC Region IX SOP, there is going to be some changes in medications, dosages of medications and responsibilities of who can administer these medications. This CE is going to cover some basic aspects of these medications including; the different names, some basic functions and how to administer them. This will be a review for some and new information for others. This will be a good way for all of us to make sure we are all on the same page. General Aspects of Medications All medications have four names: Brand Name, Generic Name, Official Name and Chemical Description. The Chemical Description is used to help identify what a specific medication does. The Official Name is how the medication is listed in the United States Pharmacopeia (USP). The Brand Name is how the manufacturer sells their product. (This is usually what promotes loyalty to the brand. Think about people that ask for Tylenol or Motrin when they have a headache. Both of them do very different things, but most people just know the name of the medication that usually works for them.) The Generic Name is made by the manufacturer and once the rights are given up, is a way for the drug to be sold without the Brand name. The following is an example of the four names for Valium: 1 Brand Name: Valium Generic Name: diazepam Official Name: diazepam, USP Chemical Name: 7-chloro-1,3-dihydro-1-methyl-5-phenyl-2H-1,4-benzodiazepin-2-one There are four sources for medications: Plant, Animal, Mineral and Synthetic. A lot of the medications that are made in a lab (or are manufactured) have their origins in plants and animals. With advances in chemistry, we were able to isolate and reproduce the effect certain plants have on the body and turn it into a pill. Generally, medications do not add anything to the body. What they do is modify or exploit existing functions of the body. Medications aren’t able to limit their effect on only one area of the body, so they can affect multiple systems, this is a side effect. A contraindication means that the medication will cause a worse problem or create a situation that the patient may not recover from. Nitroglycerin is a good medication to consider. There are side effects and contraindications that need to be understood. The patient’s blood pressure can fall once the Nitroglycerin has been given (side effect). Nitroglycerin is stopped if the
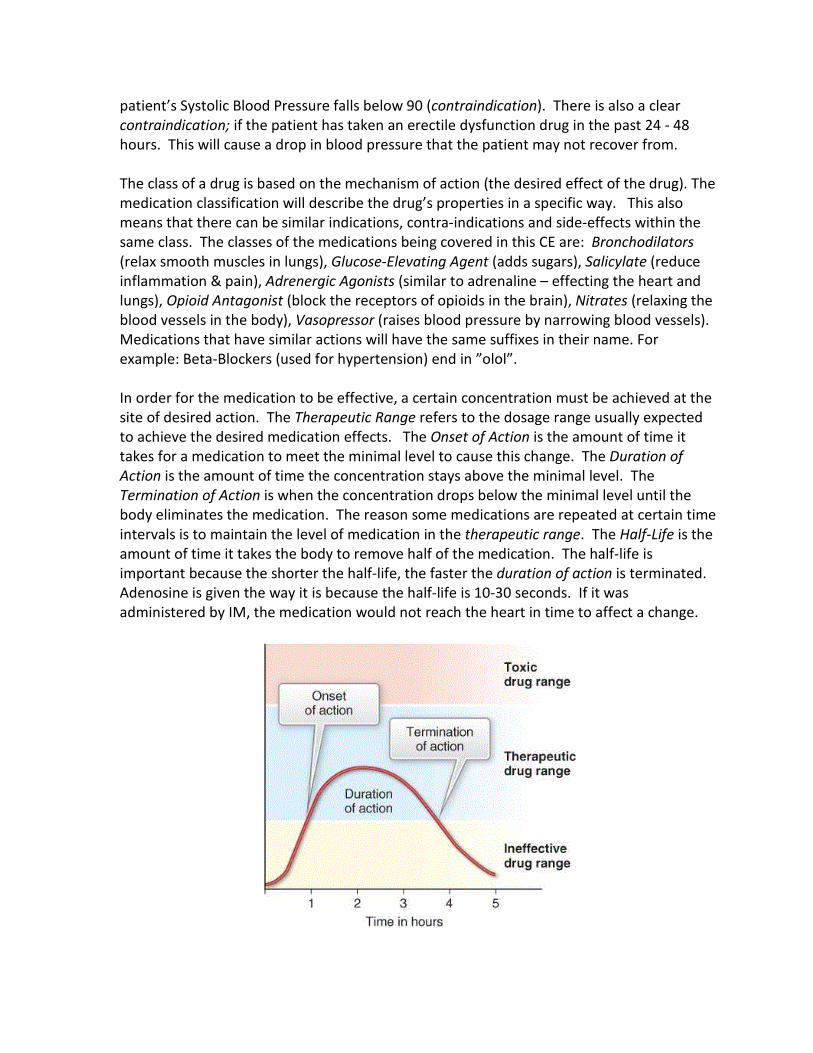
patient’s Systolic Blood Pressure falls below 90 (contraindication). There is also a clear contraindication; if the patient has taken an erectile dysfunction drug in the past 24 - 48 hours. This will cause a drop in blood pressure that the patient may not recover from. The class of a drug is based on the mechanism of action (the desired effect of the drug). The medication classification will describe the drug’s properties in a specific way. This also means that there can be similar indications, contra-indications and side-effects within the same class. The classes of the medications being covered in this CE are: Bronchodilators (relax smooth muscles in lungs), Glucose-Elevating Agent (adds sugars), Salicylate (reduce inflammation & pain), Adrenergic Agonists (similar to adrenaline – effecting the heart and lungs), Opioid Antagonist (block the receptors of opioids in the brain), Nitrates (relaxing the blood vessels in the body), Vasopressor (raises blood pressure by narrowing blood vessels). Medications that have similar actions will have the same suffixes in their name. For example: Beta-Blockers (used for hypertension) end in ”olol”. In order for the medication to be effective, a certain concentration must be achieved at the site of desired action. The Therapeutic Range refers to the dosage range usually expected to achieve the desired medication effects. The Onset of Action is the amount of time it takes for a medication to meet the minimal level to cause this change. The Duration of Action is the amount of time the concentration stays above the minimal level. The Termination of Action is when the concentration drops below the minimal level until the body eliminates the medication. The reason some medications are repeated at certain time intervals is to maintain the level of medication in the therapeutic range. The Half-Life is the amount of time it takes the body to remove half of the medication. The half-life is important because the shorter the half-life, the faster the duration of action is terminated. Adenosine is given the way it is because the half-life is 10-30 seconds. If it was administered by IM, the medication would not reach the heart in time to affect a change.

The body also has a limited amount of ways to remove the medication once the effect is done. It can be eliminated as waste by the bowels or kidneys, exhaled, sweated off through the skin, by saliva or through breast milk. Though not a big consideration in the pre-hospital setting, depending on how healthy the patient is, they may have the medication in their systems for a long time. This is why drug screens can be given after the effect of the medication is below the Duration of Action. Pre-hospital Medication Basics There are numerous ways to administer a medication. Not all of them are used in the pre-hospital setting. Pre-hospital medications that are administered need to affect a relatively quick change. The quickest way for a medication to be administered is directly into the patient. This can be achieved by insertion of a needle, the patient inhaling the medication or the patient swallowing the medication. How quickly the medication needs to cause a change will determine the best way for the medication to be introduced. Medications that are given directly into the blood can cause the quickest change. This is done through an IV (Intravenous) or IO (Intraosseus). Another route can be in the muscle (IM), in the fat below the skin (SQ) or in the nostrils (IN). Lastly, the medications can be absorbed through digestion (SL or PO). SL is sublingual (or absorbed under the tongue) and PO is per os (by mouth) and is swallowed. Medications that need to affect the lungs are better absorbed through the use of a Nebulizer (HHN). Medications have can have different concentrations based on if they are given by IV/IO or IM. The specific route of administration helps determine how much of the medication will get to the targeted system. A good example of this is Epinephrine. When given IM, the concentration is 1mg/1ml (a higher concentration). When given IV/IO, it is given 1mg/10ml (a more diluted concentration). If the wrong concentration is given by the wrong route, you can give the patient a lot more medication even though the fluid amount is still the same. The 6 Rights of Medications To prevent the wrong administration of a medication, the 6 Rights of Medications are taught. They are: Right Medication: Are you holding the medication you are supposed to be. You should look at the medication 3 times; when you first grab it, when you set it up for administration (IV/IO/IM/SL/PO) and right before you administer the medication to the patient. Right Dose: Medications can be given as an amp (all of the vial) or based on patient’s weight. Verify the amount that should be given. If you calculate that you need to open 4 packages of a medication, refigure the dose. Right Time: Medications need to be given at appropriate times or in certain orders to enhance their affect. Also giving a medication when it is contraindicated can have a fatal outcome.

Right Route: Verify that the medication is being administered by the proper route. Giving Epinephrine (1mg/1ml) by IV will put a large amount of strain on the patient. For an 80 y/o patient, it could be fatal. Right Patient: In a multiple patient situation, you have to make sure the right patient is receiving what they are supposed to. This could also be a time to verify you are following the right SOP for what the patient’s symptoms are. Right Documentation: Everything we do needs to be documented. If it is not documented, it wasn’t done. The care of the patient will also continue after the patient is dropped off at the hospital. Treatment can be based off of what was done in the pre-hospital setting. If the medication is not documented, it may be duplicated or react with a treatment that is given later. With the release of the SOP it is important that we understand who can administer the medications, how they can be administered and the proper SOPs to follow. Pay close attention to the SOPs. Some medications can be given by EMT-Bs, but only to specific patients. Skills like IN (Intranasal) application can be used by EMT-Bs, but not for all medications. Pay close attention to your Indications and Contraindications. There is a quiz at the end that will have questions marked for EMT-Bs and Paramedics. The EMT-Bs will only need to answer the questions marked for them. The Paramedics will need to answer all the questions.
Reference:
1 Bledsoe, Bryan E., Porter, Robert S., Cherry, Richard A., (2013). Paramedicine Fundamentals, Paramedic Care, Principles & Practice Vol. 2 (pp. 140). Bledsoe, Bryan E., Porter, Robert S., Cherry, Richard A., (2013). Paramedicine Fundamentals, Paramedic Care, Principles & Practice Vol. 2 (Chapter 3 – Emergency Pharmacology).

The following pages are a list of the medications that have been added, had dosages changed or have a scope of practice change. They are taken for the MNLC Reg. IX SOP – 2017. They are laid out in the following format:
General Name
(Brand Names)
Scope of Who can administer the medication? Practice:
Class: What is the action of the medication? Indications: What is the applicable use for the medication? Contraindicated: When the medication would cause harm. Precaution: Considerations for the administration of the medication Dose: Expected dosages for the medication: Can be SOP specific Side Expected changes that can occur in other systems Effects: Time: Expected time for the medication to react the Onset of Action SOP: Specific SOP where medication can be administered. Pay attention to Scope of practice on the SOP page.

Albuterol
(Proventil, Ventolin, ProAir, AccuNeb)
Scope of EMT-B, Paramedic
Practice: Class: Bronchodilators Indications: Bronchospasm associated w/asthma, COPD, allergic
reaction, croup, or cystic fibrosis
Precaution: Cardiac stimulant. Use w/caution in pts w/ACS, dysrhythmias, symptomatic tachycardia, diabetes, HTN, seizures; or active labor.
Hypoxia may ↑ incidence of CV SE
Dose: 2.5 mg / 3 mL added to albuterol dose/HHN/in-line neb (Same for Peds and Adults)
Side CNS: Tremors, nervousness, anxiety, dizziness, HA Effects: CV: ↑ HR; ↑ or ↓ BP, palpitations, dysrhythmias, chest pain, angina
GI: nausea/vomiting Resp: Paradoxical bronchospasm, hypoxia d/t ventilation/perfusion mismatch Metabolic: hypokalemia
Time: Onset: 5-15 min Peak: 30-90 min
SOP: Allergic Reaction (Pg. 13), Asthma/COPD (Pg. 14), Acute Abdominal/Flank Pain (Pg. 24), Muscular/Skeletal Trauma (Pg. 49), PEDS Allergic Reaction (Pg. 74), Peds Asthma (Pg. 75),

ASPIRIN (Acetylsalicylic acid, "ASA")
Scope of EMT-B, Paramedic
Practice:
Class: Salicylate
Indications: Suspected ACS, angina equivalents, & AMI regardless of pain unless contraindicated or an adequate dose of immediate-release ASA can be verified as taken.
Precaution: Children ≤ 18; AMS
Chest pain/STEMI following recent trauma (esp. head) prior to CT Possible stroke or ICH Currently vomiting; surgery within 2 wks., bleeding disorders; ≥ 6 mos. pregnant; active peptic ulcer/severe liver disease
Dose: 324 mg chewable tabs (4 tabs 81 mg) chewed and swallowed while prepping for 12L EKG
Sips of water help dissolve tabs and move drug out of mouth & esophagus where it can irritate lining.
Side - GI: Nausea/vomiting; irritation/bleeding Effects: - Prolonged bleeding time
- Asthma pts may have ASA sensitivity; cause bronchospasm
Time: Onset: 5-30 min Peak: 15 min – 2 hrs
SOP: Acute Coronary Syndromes (Pg. 16), Wide Complex Tachycardia with a PULSE (Pg. 19), Heart Failure/Pulmonary Edema (Pg.22)

DEXTROSE 10% (25 g/250 mL) IVPB
Scope of Paramedic Practice: Class: Glucose-Elevating Agent Indications: Hypoglycemia: bG <70 and/or S&S hypoglycemia and bG reading unavailable
If HF or Hx of HF & lungs clear: dose as usual, slow infusion rate to 50 mL increments followed by reassessment If HF & crackles or wheezes: Call OLMC for orders
Precaution: bG normal or high
Do not give sub-q or IM IV patency before infusing Giving too forcefully can result in loss of IV line and damage to surrounding tissues. If IV infiltrates / IVF extravasates, stop infusion & inform OLMC If transport refused after dextrose, assure pt. eats
Dose: See glucose emergencies SOP for dosing instructions.
Adult: bG 60-70: 12.5 grams (125 mL or ½ IV bag) Adult: bG < 60 (no pulmonary edema: 25 gms (250 mL) run IV WO PEDS: 0.5 g/kg (5 mL/kg) (0.1 g/1 mL in solution) Max initial dose: 25 g See dose chart p. 101
Side Hyperglycemia Effects: SE not as likely with D10% as D50%:
Hyperosmolarity, hypervolemia, phlebitis pulmonary edema, cerebral hemorrhage, cerebral ischemia
Time: Onset: Rapid Peak: Rapid
SOP: Alcohol Intoxication/Withdrawal (Pg. 25), Altered Mental Status (AMS)/Syncope (Pg. 26), Glucose/Diabetic Emergencies (Pg.32), Stroke (Pg. 36), Seizures (Pg. 38), PEDS Bradycardia with a Pulse (Pg. 77), PEDS Glucose/Diabetic Emergencies (Pg. 83), PEDS Drug Overdose/Poisoning (Pg. 84), PEDS Seizures (Pg. 86)

Diazepam (Valium, Diastat)
Scope of Paramedic Practice: Class: Benzodiazepine Indications: Procedural sedation prior Cardioversion - Generalized tonic/clonic seizure activity - Severe anxiety/agitation - Muscle relaxant for long bone fractures - Stimulant-induced excited delirium, ACS, tachycardia, HTN crisis; (cocaine, amphetamines ephedrine, PCP)
Precaution: -Allergy - Glaucoma - Shock (SBP <90) - Pregnancy unless seizing Dose: Adults: 2mg increments to 10mg slow IVP/IO or 4-20mg IR Peds: 0.3mg/kg IVP/IO (max 10mg) or 0.5mg/kg IR (max 20 mg) Side CNS: Drowsiness, sedation, confusion, amnesia, ataxia Effects: Resp: Respiratory depression, arrest CV: Hypotension, bradycardia/tachycardia
Time: Onset: Rapid - (up to 15 minutes) Peak: 1 to 1.5 hours Duration: Up to 48 hours SOP: This is an alternative medication to be used in place of Fentanyl and Morphine. Reference Fentanyl information for SOPs

DIPHENHYDRAMINE (Benadryl)
Scope of EMT-B, Paramedic Practice: Class: Antihistamine Indications: - Allergic reactions/ anaphylaxis
- Per OLMC: Dystonic reactions due to phenothiazines (Thorazine, Compazine, Stelazine, Prolixin)
Contraindicated: Acute asthma attack - Hx asthma w/current allergic reaction – OK to use
Precaution: - Do not give sub-q
- Peds likely to have CNS stimulation (vs. sedation) - Angle closure glaucoma - Prostatic hypertrophy
Dose: Lower acuity: 1 mg/kg (max 50 mg) PO/IM [BLS] Emergent: 50 mg IM [BLS] Critical Rx: 50 mg IM [BLS] Peds: 1 mg/kg (max 50 mg) PO/IM [BLS]
Side CNS: Drowsiness, blurred vision, dilated pupils, Effects: hallucinations, vertigo, weakness, ataxia
Resp: thickened bronchial secretions CV: ↑ HR; ↓ BP GI: Dry mouth, N / V
Time: Onset: 20 – 30 min Peak: 2 – 4 hrs
SOP: Allergic Reaction (Pg. 13), PEDS Allergic Reaction (Pg. 74)

DOPAMINE
(Intropin)
Scope of Paramedic Practice: Class: Endogenous catecholamine; SNS agonist Indications: ß dose: Inotrope: Cardiogenic shock; bradycardia and/or ROSC w/ hypotension
Contraindicated: - Tachydysrhythmias (↓ BP due to rate problem)
- Adrenal tumor Precaution: Occlusive vascular disease - Hypovolemic shock: Pressors not a substitute for hemostasis & IVF replacement Dose: Beta (ß) dose: 5 mcg/kg/min; May titrate up to 20 mcg/kg/min to maintain SBP ≥ 90 (MAP ≥ 65). Calculation tip: Beta dose: Take 1st 2 # of wt. in lbs; subtract 2 = mcgtts/min. Ex: 150 lbs = 13 mcgtts/min Use lowest dose to minimize Side Effects Use large vein and IV patency before infusing Side CNS: H/A, dizziness Effects: CV: ↑ HR; palpitations, ectopy, ↑ O2 demand; risk of ACS, dysrhythmias, vasoconstriction Resp: SOB Eyes: dilated pupils Skin: may cause tissue necrosis if infiltrates; notify OLMC ASAP Time: Onset: within 5 min
Peak: 5-10 minutes
SOP: This is an alternative medication to be used in place of Norepinephrine. Reference Norepinephrine information for SOPs
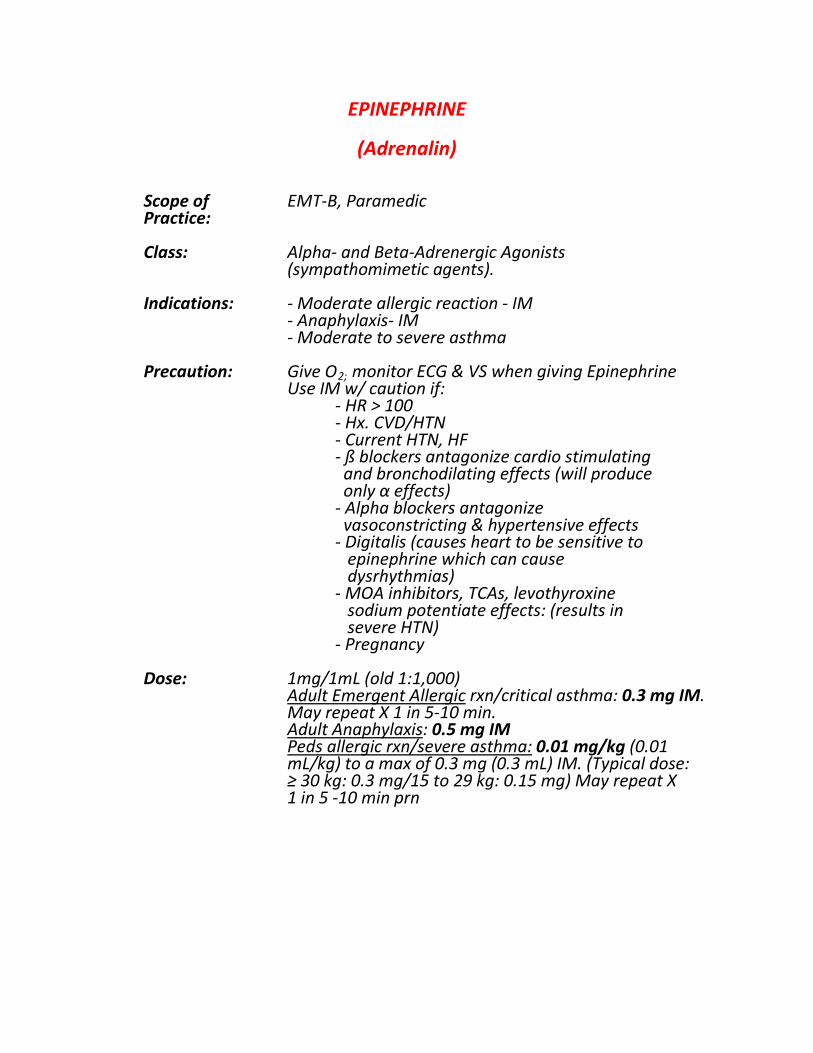
EPINEPHRINE
(Adrenalin)
Scope of EMT-B, Paramedic Practice: Class: Alpha- and Beta-Adrenergic Agonists (sympathomimetic agents).
Indications: - Moderate allergic reaction - IM
- Anaphylaxis- IM - Moderate to severe asthma
Precaution: Give O2; monitor ECG & VS when giving Epinephrine Use IM w/ caution if: - HR > 100 - Hx. CVD/HTN - Current HTN, HF - ß blockers antagonize cardio stimulating and bronchodilating effects (will produce only α effects) - Alpha blockers antagonize vasoconstricting & hypertensive effects - Digitalis (causes heart to be sensitive to epinephrine which can cause dysrhythmias) - MOA inhibitors, TCAs, levothyroxine sodium potentiate effects: (results in severe HTN) - Pregnancy
Dose: 1mg/1mL (old 1:1,000) Adult Emergent Allergic rxn/critical asthma: 0.3 mg IM. May repeat X 1 in 5-10 min. Adult Anaphylaxis: 0.5 mg IM Peds allergic rxn/severe asthma: 0.01 mg/kg (0.01 mL/kg) to a max of 0.3 mg (0.3 mL) IM. (Typical dose: ≥ 30 kg: 0.3 mg/15 to 29 kg: 0.15 mg) May repeat X 1 in 5 -10 min prn

Side Elderly at higher risk for Side Effects Effects: CNS: HA, anxiety, restlessness, dizziness, tremors, excitability, lightheadedness
CV: ↑ HR, palpitations, tachydysrhythmias, ventricular ectopy, high dose may produce vasoconstriction, may compromise perfusion; HTN, angina, ↑ myocardial O2 consumption; can cause worsened ischemia GI: N/V Skin: Pallor; necrosis at injection site
Time: Onset: Variable Peak: Unknown
SOP: Allergic Reaction (Pg. 13), Asthma/COPD (Pg. 14), Ventricular Fibrillation (VF) (Pg. 20), Asystole; PEA (Pg. 21), Newborn Resuscitation (Pg. 64), PEDS Allergic Reaction (Pg. 74), Peds Asthma (Pg. 75), Croup/
Epiglottitis/RSV/Bronchiolitis (Pg. 76), PEDS Bradycardia (Pg.77), PEDS Ventricular Fibrillation (Pg. 80), PEDS Asystole/PEA (Pg. 81)

FENTANYL Citrate Scope of Paramedic Practice:
Class: Synthetic opiate - Short acting narcotic
Indications: Treatment of pain
Contraindicated: - Intolerance to opiates - AMS (GCS <15) or mentation not appropriate for age/usual state - Respiratory depression - Hypotension - Acute/severe asthma - Myasthenia Gravis - Intermittent pain - Patients on depressant drugs Precaution: - Avoid over sedation of COPD - resp depression Concurrent use of alcohol, benzos, drugs of abuse - Cardiac Hx: bradydysrhythmias or those given Amiodarone or Verapamil - Liver or kidney Dx: ↓ hepatic metabolism & renal excretion. - Pregnant women (Cat C) - Uncontrolled hypothyroidism Dose: 1 mcg/kg (round to nearest 5 mcg) up to 100 mcg
- May repeat once in 5 min: 0.5 mcg/kg (max 50 mcg) to a total of 1.5 mcg/kg /SOP.
Elderly (>65), debilitated or SCI: 0.5 mcg/kg (max 50 mcg). Additional doses require OLMC. May repeat 0.5 mcg/kg q. 5 min to total of 3 mcg/kg (300 mcg) prn & if available. The safety of FENTANYL in children younger than two years of age has not been established. Contact OLMC.

Side Resp: hypoventilation; SpO2 < 90% on 15 L O2 Effects: CV: Bradycardia (reverse w/ atropine), hypotension CNS: GCS < 15; sedation, confusion, dizziness, euphoria, seizures Uncommon: GI: N/V (give Ondansetron) MS: Muscle rigidity, myoclonic movements - Hives, itching, abd pain, flushing - Blurred vision, small pupils - Laryngospasm, diaphoresis, spasm of the sphincter of Oddi Anaphylaxis Time: Onset: minutes (sl. delayed w/ IN vs. IV route) Peak: 3-5 min (sl. lower peak with IN vs. IV) Duration: 30-60 min SOP: General Patient Assessment/Initial Medical Care (IMC) (Pg. 4), Elderly Patients (65 and older) (Pg. 9), Acute Coronary Syndromes (ACS) (Pg. 16), Bradycardia with a Pulse (Pg. 17), Narrow QRS Complex Tachycardia (Pg. 18), Wide Complex Tachycardia with a Pulse (Pg. 19), Acute ABDOMINAL/FLANK PAIN (Pg. 24), Drug Overdose/Poisoning (Pg. 27), Environmental: Cold Emergencies (Pg. 29), Hypertension (Pg. 33), Initial Trauma Care (ITC) (Pg. 40), Burns (Adult & Peds) (Pg. 44), Eye Emergencies /Facial Trauma (Pg. 47), Musculo- Skeletal Trauma (Pg. 49), Trauma in Pregnancy (Pg. 60), PEDS Initial Medical Care (Pg. 68), PEDS Bradycardia with a Pulse (Pg. 77), PEDS Initial Trauma Care (Pg. 85), Peds ITC: Secondary Assessment (Pg. 88),
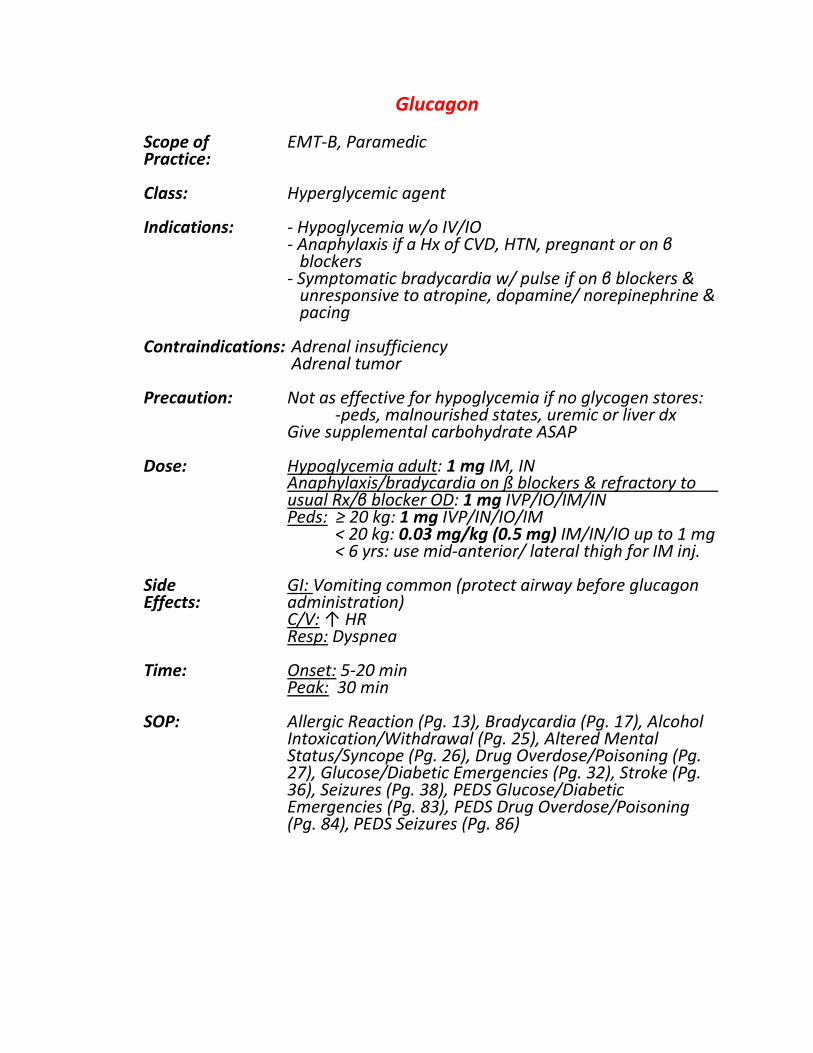
Glucagon Scope of EMT-B, Paramedic
Practice: Class: Hyperglycemic agent Indications: - Hypoglycemia w/o IV/IO
- Anaphylaxis if a Hx of CVD, HTN, pregnant or on β blockers - Symptomatic bradycardia w/ pulse if on β blockers & unresponsive to atropine, dopamine/ norepinephrine & pacing
Contraindications: Adrenal insufficiency Adrenal tumor
Precaution: Not as effective for hypoglycemia if no glycogen stores: -peds, malnourished states, uremic or liver dx
Give supplemental carbohydrate ASAP
Dose: Hypoglycemia adult: 1 mg IM, IN Anaphylaxis/bradycardia on ß blockers & refractory to usual Rx/β blocker OD: 1 mg IVP/IO/IM/IN Peds: ≥ 20 kg: 1 mg IVP/IN/IO/IM < 20 kg: 0.03 mg/kg (0.5 mg) IM/IN/IO up to 1 mg < 6 yrs: use mid-anterior/ lateral thigh for IM inj.
Side GI: Vomiting common (protect airway before glucagon Effects: administration)
C/V: ↑ HR Resp: Dyspnea
Time: Onset: 5-20 min Peak: 30 min
SOP: Allergic Reaction (Pg. 13), Bradycardia (Pg. 17), Alcohol Intoxication/Withdrawal (Pg. 25), Altered Mental Status/Syncope (Pg. 26), Drug Overdose/Poisoning (Pg. 27), Glucose/Diabetic Emergencies (Pg. 32), Stroke (Pg. 36), Seizures (Pg. 38), PEDS Glucose/Diabetic Emergencies (Pg. 83), PEDS Drug Overdose/Poisoning (Pg. 84), PEDS Seizures (Pg. 86)

IPRATROPIUM BROMIDE INHALATION SOLUTION, 0.02%
(Atrovent)
Scope of EMT-B, Paramedic Practice: Class: Bronchodilators
Indications: Bronchospasm assoc. w/
- Mod/severe allergic reaction - COPD/Asthma Considered relatively safe to use in pregnant women
Precaution: - Pts allergic to MDI formulation (peanut allergy) may safely use neb solution: contact OLMC
- Bladder neck obstruction - Prostate hypertrophy - Narrow-angle glaucoma
Dose: Adult: 0.5 mg added to albuterol dose/HHN/in-line neb
Peds (off label): 0.25-0.5 mg added to albuterol
Side GI: Dry mouth, bitter taste in mouth, nausea Effects: Eyes: Blurred vision, dilated pupil (mist leak exposing eyes). Neb mouthpiece preferred over mask to avoid contact w/eyes if glaucoma.
Time: Onset: 15-30 min
Peak: 1-2 hours Duration: 4-8 hours
SOP: Allergic Reaction (Pg. 13), Asthma/COPD (Pg. 14), SHOCK Differential / Hypovolemic - Septic (Pg. 39),
PEDS Allergic Reaction (Pg. 74), Peds Asthma (Pg. 75)
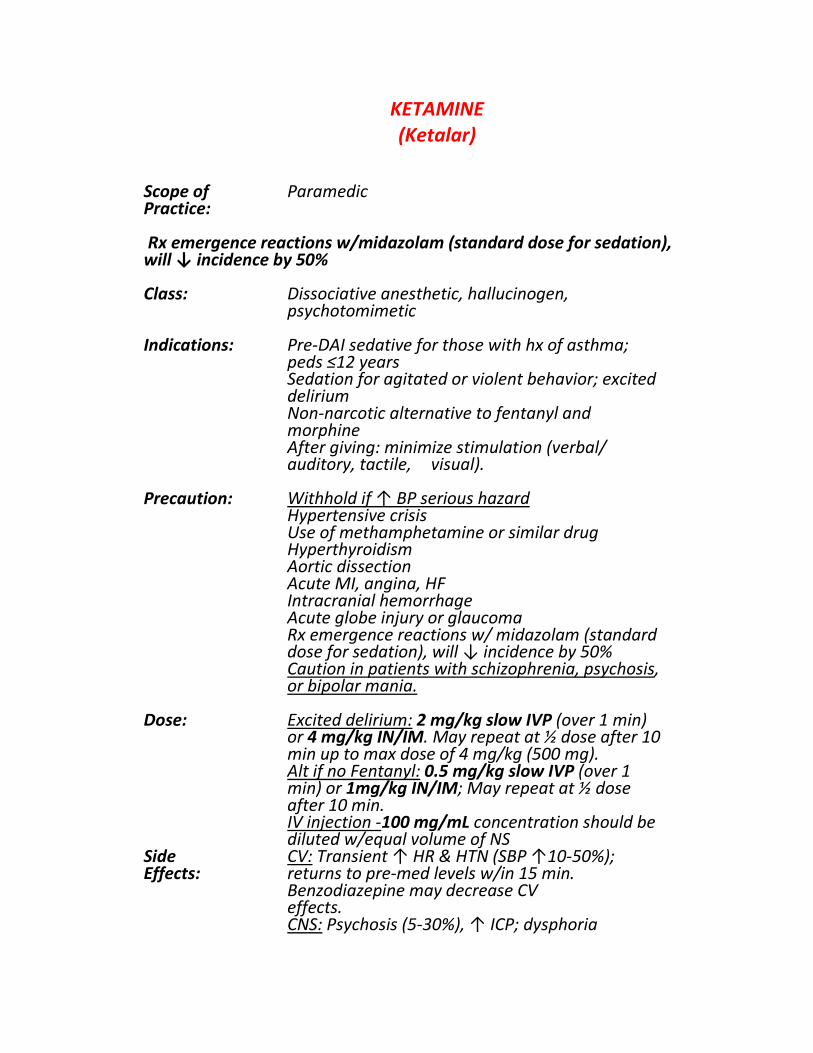
KETAMINE (Ketalar)
Scope of Paramedic Practice:
Rx emergence reactions w/midazolam (standard dose for sedation), will ↓ incidence by 50% Class: Dissociative anesthetic, hallucinogen, psychotomimetic Indications: Pre-DAI sedative for those with hx of asthma; peds ≤12 years
Sedation for agitated or violent behavior; excited delirium Non-narcotic alternative to fentanyl and morphine After giving: minimize stimulation (verbal/ auditory, tactile, visual).
Precaution: Withhold if ↑ BP serious hazard Hypertensive crisis Use of methamphetamine or similar drug Hyperthyroidism Aortic dissection Acute MI, angina, HF Intracranial hemorrhage Acute globe injury or glaucoma Rx emergence reactions w/ midazolam (standard dose for sedation), will ↓ incidence by 50% Caution in patients with schizophrenia, psychosis, or bipolar mania.
Dose: Excited delirium: 2 mg/kg slow IVP (over 1 min) or 4 mg/kg IN/IM. May repeat at ½ dose after 10 min up to max dose of 4 mg/kg (500 mg).
Alt if no Fentanyl: 0.5 mg/kg slow IVP (over 1 min) or 1mg/kg IN/IM; May repeat at ½ dose after 10 min. IV injection -100 mg/mL concentration should be diluted w/equal volume of NS
Side CV: Transient ↑ HR & HTN (SBP ↑10-50%); Effects: returns to pre-med levels w/in 15 min. Benzodiazepine may decrease CV effects.
CNS: Psychosis (5-30%), ↑ ICP; dysphoria

MSK: Rigidity, dystonic reaction, depressed reflexes Psych: Emergence reactions: anxiety, restlessness, confusion; disorientation, auditory & visual hallucinations, delirium, irrational behavior; lasting 2-24 hrs. Resp: Beta-adrenergic and vagolytic properties produce Bronchodilation
Time: Onset: Rapid Peak: 5-10 min
SOP: This is an alternative medication to be used in place of Fentanyl and Morphine. Reference Fentanyl information for SOPs

MORPHINE
Scope of Paramedic Practice: Class: Narcotic analgesic
- ↓ pain and apprehension Indications: Treatment of pain
Precaution: - Multiple trauma - ↓ BP, volume depletion; shock - Use w/ caution in pts who may be preload dependent (RV infarct). - AMS; head injury - Hypoventilations/resp. depression - Known allergy to narcs. - Pts on depressant drugs - Caution in COPD - Relative contraindication: severe abdominal pain w/ peritonitis Dose: Adults: 2 mg increments up to 10 mg slow IVP or 10 mg IM if no IV in MS trauma. Peds: 0.1 mg/kg slow IVP/IM Max single dose: 2 mg Less likely to cause respiratory depression if given slowly. Reverse with Naloxone Side CNS: Sedation, H/A Effects: CV: ↓ SVR, ↓ BP, ↓ P Resp: Depression Eyes: Dry eyes, blurred vision GI: N/V Skin: rashes, itching Interactions: Depressive effects enhanced if used w/ other sedatives, hypnotics, antihistamines, antiemetics, barbs, ETOH. Time: Onset: Rapid
Peak: 20 minutes Half-life: Up to 20 hours
SOP: This is an alternative medication to be used in place of Fentanyl. Reference Fentanyl information for SOPs

NALOXONE (Narcan)
Scope of EMT-B, Paramedic Practice:
Class: Opioid Antagonist
Indications: - Narcotic/synthetic narcotic OD w/ AMS & respiratory depression
- Coma of unknown etiology with respiratory depression (may or may not have constricted pupils)
Precaution: Rapid reversal may result in opiate withdrawal syndrome – agitated, combative, uncooperative, rapid HR.
Give O2 while prepping med to prevent reversal tachycardia. Use with caution in infants of addicted moms or pts dependent on opiates w/ CV disease (contact OLMC)
Dose: Adult: If breathing: 0.4 mg; repeat q. 30 sec until ventilations increase up to 4 mg
If apneic: 1 mg. Repeat q. 30 sec until breathing resumes up to 4 mg. All additional doses require OLMC. PEDS: 0.1 mg/kg (max single dose 0.4 mg) IVP/IN/IO/IM w/repeat doses q/ 30 sec until ventilations increase up to 4 mg.
Side CNS: Tremor, agitation, combativeness, seizure Effects: (opioid antagonists stimulate the sympathetic NS)
CV: ↑ HR, ↑ BP, dysrhythmias Resp: Hyperventilation GI: N / V Rare anaphylactic reactions & flash pulmonary edema reported after naloxone use.
Time: Onset IV/IN: 1-2 min Onset IM: 2-10 min Half- life: 30-81 min Half-life of naloxone often shorter than the half-life of narcotic taken; repeat doses is often required.

SOP: Ventricular Fibrillation (VF) (Pg. 20), Asystole; PEA (Pg. 21), Altered Mental Status/Syncope (Pg. 26), Drug Overdose/Poisoning (Pg. 27-28), PEDS Respiratory Arrest (Pg. 73), PEDS Ventricular Fibrillation (Pg.80), PEDS Asystole/PEA (Pg. 81), Altered Mental Status (Pg. 82), PEDS Glucose/Diabetic Emergencies (Pg. 83), PEDS Drug Overdose/Poisoning (Pg. 84-85)
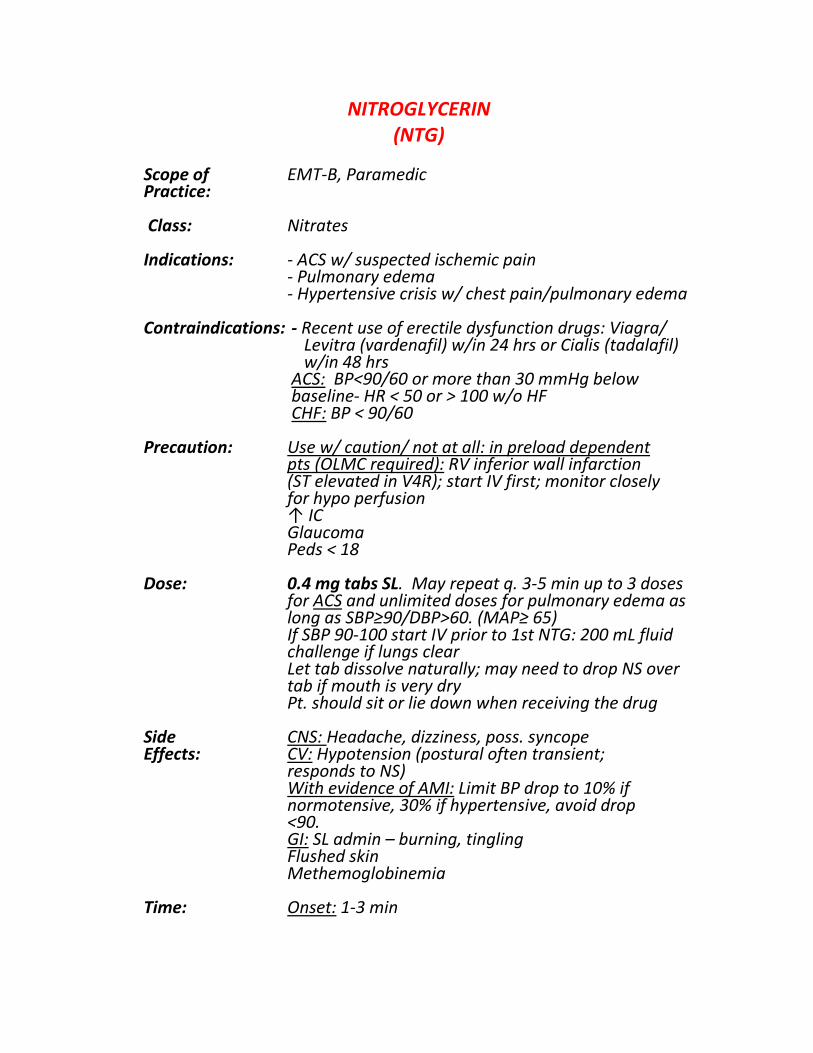
NITROGLYCERIN (NTG)
Scope of EMT-B, Paramedic Practice: Class: Nitrates Indications: - ACS w/ suspected ischemic pain
- Pulmonary edema - Hypertensive crisis w/ chest pain/pulmonary edema
Contraindications: - Recent use of erectile dysfunction drugs: Viagra/ Levitra (vardenafil) w/in 24 hrs or Cialis (tadalafil) w/in 48 hrs ACS: BP<90/60 or more than 30 mmHg below baseline- HR < 50 or > 100 w/o HF
CHF: BP < 90/60
Precaution: Use w/ caution/ not at all: in preload dependent pts (OLMC required): RV inferior wall infarction (ST elevated in V4R); start IV first; monitor closely for hypo perfusion
↑ IC Glaucoma Peds < 18
Dose: 0.4 mg tabs SL. May repeat q. 3-5 min up to 3 doses for ACS and unlimited doses for pulmonary edema as long as SBP≥90/DBP>60. (MAP≥ 65)
If SBP 90-100 start IV prior to 1st NTG: 200 mL fluid challenge if lungs clear Let tab dissolve naturally; may need to drop NS over tab if mouth is very dry Pt. should sit or lie down when receiving the drug
Side CNS: Headache, dizziness, poss. syncope Effects: CV: Hypotension (postural often transient; responds to NS)
With evidence of AMI: Limit BP drop to 10% if normotensive, 30% if hypertensive, avoid drop <90. GI: SL admin – burning, tingling Flushed skin Methemoglobinemia
Time: Onset: 1-3 min

SOP: Acute Coronary Syndrome (Pg. 16), Heart Failure/ Pulmonary Edema (Pg. 22), Hypertension (Pg. 33)

NOREPINEPHRINE bitartrate (Levophed)
Scope of Paramedic Practice:
Class: Vasopressor
Indications: Patients with severe hypotension (MAP < 60). Pressor agent used mainly to treat patients in vasodilatory shock states such as septic and neurogenic shock, while showing fewer adverse side-effects compared to dopamine.
Pregnancy: May have adverse effects on fetus, call OLMC
Precaution: Hypovolemic shock: Do not give NaHCO3 (Sodium Bicarb) in IV line containing norepinephrine
- Pts receiving monoamine oxidase inhibitors (MAOI) or antidepressants of the triptyline or imipramine types - severe, prolonged HTN may result. - Asthma; - Bisulfite sensitivity - At high doses, and especially when combined with other vasopressors, it can lead to limb ischemia and limb death
Dose: Given IVPB into a large vein (antecubital) Adult (18 and Older): 0.03 mg IVP with caution Retake BP every 2 min from time drug is started until desired BP reached, then every 5 min infusion site frequently for patency. Avoid extravasation – inform OLMC ASAP if it occurs.
Side CV: Severe HTN; tachycardia. arrhythmias; severe Effects: peripheral and visceral vasoconstriction, ↓ renal perfusion and urine output, poor systemic blood flow despite “normal” BP, tissue hypoxia, and lactic acidosis
CNS: Anxiety, confusion, HA (if HTN results), tremor Resp: Dyspnea with or w/o respiratory difficulty Skin: Sweating, extravasation
Time: Onset: 30-60 seconds Peak: Rapid

SOP: Bradycardia W/Pulse (Pg17), V-Fib/Pulseless V- Tach (Pg. 20), Asystole/PEA (Pg. 21), Heart Failure/Pulmonary Edema (Pg. 22), Shock (Pg. 39), Spine Trauma (Pg. 51)

ONDANSETRON (Zofran)
Scope of EMT-B, Paramedic Practice:
Class: Antiemetic
Indications: Nausea/vomiting
Precaution: Phenylketonuria (PKU): ODT contains aspartame that forms phenylalanine.
Don’t push ODT through blister foil package; tabs are fragile
Dose: Adults: 4 mg oral dissolve tablet. May repeat in 10 minutes to a total of 8 mg PO.
Peds: 0.15mg/kg up to a total of 4 mg IVP or ODT
Side Rare: Transient blurred vision after rapid IV Effects: infusion,
Headache, lightheadedness Sedation Nausea/vomiting Diarrhea in children
Time: Onset: Rapid Peak: 2 hours PO
SOP: General Pt. Assessment (Pg. 4), Environmental: Heat Emergencies (Pg. 31), Initial Trauma Care (ITC) (Pg. 40), Burns (Adult & Peds) (Pg. 44), Facial Trauma (Pg. 47), Head Trauma/Traumatic Brain Injury (Pg. 48), Spine Trauma: Adult & peds (Pg. 50), PEDS Initial Medical Care (Pg. 68), PEDS Initial Trauma Care (Pg. 87)

McHenry Western Lake County EMS System Mandatory CE for Paramedics, EMT-B and PHRN’s
SOP Rollout - Medications Online CE 2017
NAME: _________________________ DEPT. ______________________ DATE: __________
Provider Level: EMT-B Paramedic
1) Which medication cannot be given IM by an EMT-B? [BLS] a. Fentanyl b. Narcan c. Glucagon d. Diphenhydramine
2) Which medication can be given IN by an EMT-B? [BLS]
a. Fentanyl b. Midazolam c. Glucagon d. Diphenhydramine
3) You are called for a 45 y/o diabetic patient. Upon contact, the Pt is lethargic and has shallow respirations. Coworkers state that the patient has not been eating because they have had a cold. Unknown if the patient has eaten at all today. You check a Blood Glucose level and it is 45. What could you do for this patient? [BLS]
a. Administer Epi (1mg/1ml) 0.3 mg IM/IN b. Administer Glucagon 1 mg IM/IN c. Administer Glucagon 0.03 mg/kg IM/IN d. Administer D50% 25 gm IVP
4) When giving Albuterol and Ipratropium in the HHN, what are the doses? [BLS] a. We don’t give Albuterol and Ipratropium together. b. Albuterol 6 mg/Ipratropium 0.5 mg c. Albuterol2.5 mg/Ipratropium 6mg d. Albuterol 2.5 mg/Ipratropium 0.5 mg
5) You have an 11 y/o patient that was stung by a bee. The pt is coughing and stating they are having difficulty taking a deep breath. You hear wheezing in both lungs. Vitals: B/P 110/80, P 100, Resp 24, SPO2 96%, EtCO2 is 35. The patient’s weight is around 75 lbs. What medication can be given to this patient? [BLS]
a. Epinephrine (1mg/1mL) 0.15 mg IM b. Epinephrine (1mg/1mL) 0.30 mg IM c. Epinephrine (1mg/10mL) 0.15 mg IM d. Epinephrine (1mg/10mL) 0.03 mg IM
6) Zofran is given to which patient? [BLS] a. A patient that is having a seizure b. A patient that is nauseous c. A patient with a bee sting d. A patient that is dizzy
7) Before giving a Nitroglycerin Tab, we need to know what? [BLS]
a. Last menstrual cycle for female patients b. Use of any erectile dysfunction medications in the last 24 - 48 hrs c. How many baby aspirin were taken prior to EMS arrival d. If the patient’s Systolic Blood Pressure is greater than 120
8) Which is not one of the 6 Rights of Medications? [BLS] a. Time b. Date c. Dose d. Documentation
9) The ___________ refers to the dosage range usually expected to achieve the desired medication effects. The ___________is the amount of time the concentration stays above that minimal level. [BLS]
a. Therapeutic Range, Duration of Action b. Duration of Action, Therapeutic Range c. Sedation Concentration, Half-life d. Contraindication, Side Effect
10) A ________ is an expected action that affects other body systems; a ________ can cause an irreversible problem. [BLS]
a. Reaction, Effect b. Acrocyanosis, Decompression c. Side Effect, Contraindication d. Contraindication, Side Effect
11) The dosage for Norepinephrine administration is? [ALS]
a. 3.0 mg IVBP b. 0.003 ml IVBP c. 0.03 ml IVSP d. 0.03 mg IVSP
12) For a 20 y/o patient with altered mentation and a blood Glucose of 59, what medication
(and dose) would be given? [ALS] a. D50 150 gms, IVP b. D10 12.5 gms, IVBP c. D10 25 gms, IVBP d. D50 10gms, IVP
13) Fentanyl is given for pain management. Which of the following is true? [ALS]
a. The only alternative medication is Ketamine b. Naloxone cannot be used as a reversal agent c. Cannot be used in patients under 2 y/o without contacting OLMC d. Maximum single dose is 75 mcg with a maximum total dose of 150 mcg
14) What is the minimum age for a patient to receive Norepinephrine? [ALS]
a. 12 b. Signs of Puberty c. 18 d. 21

15) You are transporting a CHF Pt for difficulty breathing. You have the patient on CPAP at 10 PEEP. They also have chest pain. Pain is 5 out of 10. Vitals: B/P 100/90 (on CPAP), P 110, RR 16. 12 lead shows ST segment elevation in V1 and V2. Aspirin (324 mg) has been given with no relief. What is the next medication to be given? [ALS]
a. Repeat Aspirin at 162 mg b. Norepinephrine 0.03mg IVP c. Midazolam 2 mg IVP q. 2 min up to 10 mg IVP/IN d. Nitroglycerin 0.4 mg SL - no maximum as long as SBP is above 90.
THIS QUIZ IS MANDATORY FOR ALL EMT-P, EMT-B, AND PHRN’S WITHIN THE MCHENRY WESTERN LAKE COUNTY EMS SYSTEM. IT IS DUE IN THE EMS OFFICE NO LATER THAN 3/31/17 TO REMAIN IN GOOD STANDING.
PLEASE FAX THIS QUIZ TO 815/206-3455, THEN CALL CINDY TABERT AT 815/334-3174 TO CONFIRM THAT SHE RECEIVED IT.
THANK YOU.


















