McGarvey- EEG and Doppler Ultrasound Monitoring (H)
15
1/22/2015 1 Intraoperative EEG and Transcranial Doppler Ultrasound Monitoring Michael McGarvey MD Associate Professor of Neurology Department of Neurology Hospital of the University of Pennsylvania EEG and TCD Two separate techniques Clearly distinct methods of monitoring Both used to monitor vascular procedures that place brain at risk for ischemia Potentially complementary Why is this Monitoring Important? Cardiac surgery Neurologic complications occur in up to 15% of cases Behavioral complications in up to 70% Economic impact of stroke after Cardiac surgery is estimated to be 2-4 billion dollars world-wide Aortic surgery: Ischemic stroke Arch repairs: up to 5% (DHCA) Aortic Dissections: up to 11% TAAA surgery: up to 10% TEVAR: 5-10% TaVi: ?
Transcript of McGarvey- EEG and Doppler Ultrasound Monitoring (H)

1/22/2015
1
Intraoperative EEG and Transcranial
Doppler Ultrasound Monitoring
Michael McGarvey MD
Associate Professor of Neurology
Department of Neurology
Hospital of the University of Pennsylvania
EEG and TCD
� Two separate techniques
� Clearly distinct methods of monitoring
� Both used to monitor vascular procedures that place brain at risk for ischemia
� Potentially complementary
Why is this Monitoring Important?� Cardiac surgery
� Neurologic complications occur in up to 15% of cases
� Behavioral complications in up to 70%
� Economic impact of stroke after Cardiac surgery is estimated to be 2-4 billion dollars world-wide
� Aortic surgery: Ischemic stroke� Arch repairs: up to 5% (DHCA)
� Aortic Dissections: up to 11%
� TAAA surgery: up to 10%
� TEVAR: 5-10%
� TaVi: ?
1/22/2015
2
Why is this Monitoring Important?
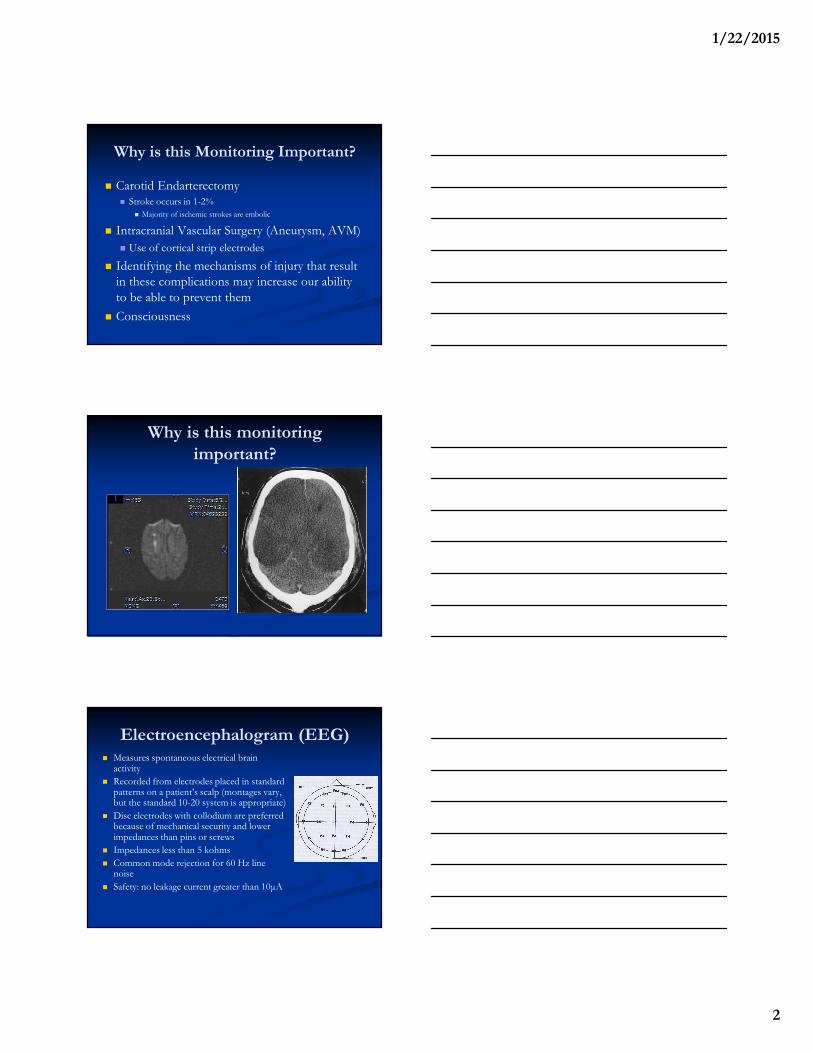
� Carotid Endarterectomy� Stroke occurs in 1-2%
� Majority of ischemic strokes are embolic
� Intracranial Vascular Surgery (Aneurysm, AVM)
� Use of cortical strip electrodes
� Identifying the mechanisms of injury that result in these complications may increase our ability
to be able to prevent them
� Consciousness
Why is this monitoring
important?
Electroencephalogram (EEG)� Measures spontaneous electrical brain
activity
� Recorded from electrodes placed in standard patterns on a patient’s scalp (montages vary, but the standard 10-20 system is appropriate)
� Disc electrodes with collodium are preferred because of mechanical security and lower impedances than pins or screws
� Impedances less than 5 kohms
� Common mode rejection for 60 Hz line noise
� Safety: no leakage current greater than 10µA
1/22/2015
3
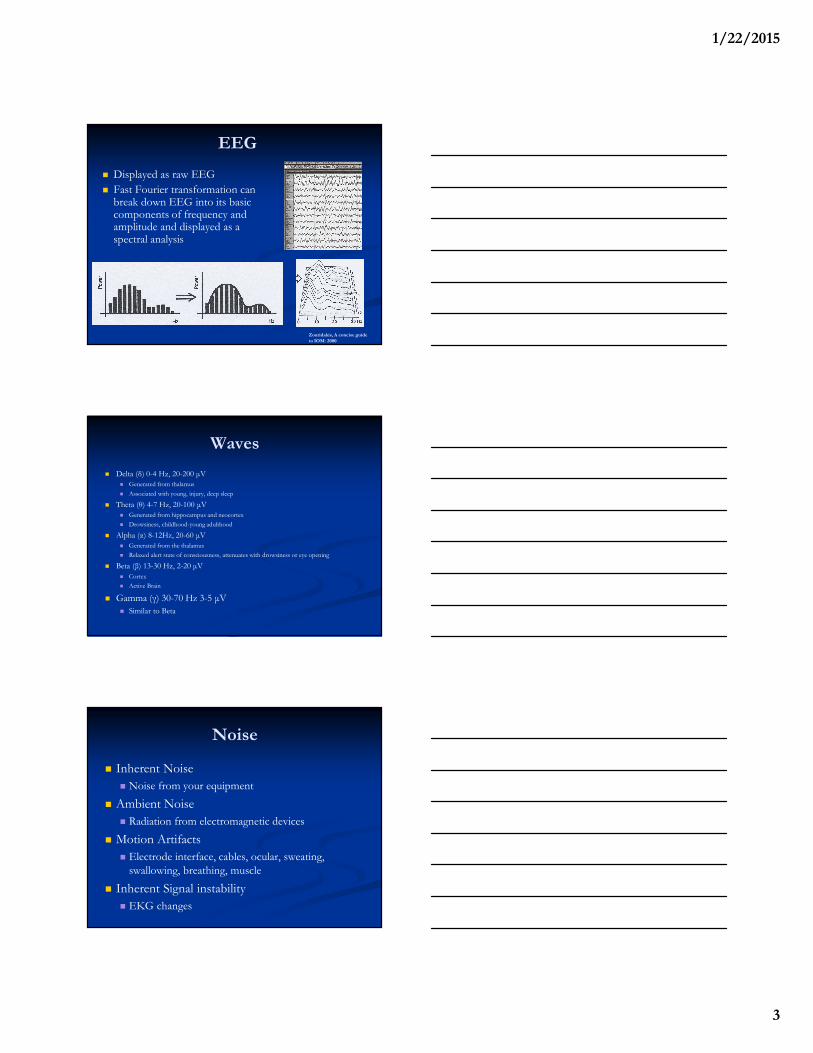
EEG
� Displayed as raw EEG
� Fast Fourier transformation can break down EEG into its basic components of frequency and amplitude and displayed as a spectral analysis
Zouridakis, A concise guide
to IOM: 2000
Waves
� Delta (δ) 0-4 Hz, 20-200 µV
� Generated from thalamus
� Associated with young, injury, deep sleep
� Theta (θ) 4-7 Hz, 20-100 µV
� Generated from hippocampus and neocortex
� Drowsiness, childhood-young adulthood
� Alpha (α) 8-12Hz, 20-60 µV
� Generated from the thalamus
� Relaxed alert state of consciousness, attenuates with drowsiness or eye opening
� Beta (β) 13-30 Hz, 2-20 µV
� Cortex
� Active Brain
� Gamma (γ) 30-70 Hz 3-5 µV
� Similar to Beta
Noise
� Inherent Noise
� Noise from your equipment
� Ambient Noise
� Radiation from electromagnetic devices
� Motion Artifacts
� Electrode interface, cables, ocular, sweating, swallowing, breathing, muscle
� Inherent Signal instability
� EKG changes

1/22/2015
4
Spectral Analysis
� Caution
� Difficult to distinguish artifact from real EEG changes
� EKG, muscles, or the other operating room electrical contaminates
� Anesthetic adjustments
� Recommend its use as adjunctive or for research purposes
EEG
� About 40% of the brain’s metabolic demand is used to keep cellular activity, the remainder is for neurophysiologic function.
� Function is lost prior to structural injury
� This is how EEG serves as a warning of impeding injury
� Generally cells can survive approximately 3 minutes without oxygen
� Ischemic changes begin when flow drops below 20ml per 100 g per min
EEG
� A change in a patient’s background EEG activity from baseline during a procedure may indicate ischemia
� Decrease in fast activity, slow waves( delta activity increase greater than 1 Hz), loss of amplitude
� A 50 % decrease in EEG amplitude has been considered a significant change by most authors.

1/22/2015
5
Limitations of EEG in IOM� Reflects only cortical
activity
� Does not reflect subcortical structures
� SSEPS
� Complicated by anesthetic agents
� Goal is steady state
� Burst suppression?
� High sensitivity, but
low specificity
� Small emboli?Zouridakis, A concise guide to IOM: 2000
Utility of EEG in Surgery
� Identifying injury
� Depth of Anesthesia
� Consciousness
� Increase complications
� Awake, moderate, general anesthesia, isoelectric
� General anesthesia vs. ischemia
Carotid Endarterectomy� One of the most common uses for EEG
� A small proportion of strokes are due to hypoperfusion
� Both animal and human blood flow studies that loss of EEG activity reflects reduction of blood flow
� A critical point during CEA is clamping of the carotid artery to perform the endarterectomy� Adequacy of collateral flow of the circle of Willis
� Hypertension or a carotid shunt may be used to alleviate the ischemia
� Severe contralateral stenosis or occlusion increases risk
� Vertebral stenosis
� Mild ipsilateral stenosis increase risk
� The risk of patients with bilateral disease and global ischemia

1/22/2015
6
Carotid Clamping
Case
� 70 year old woman with history of hyperlipidemia, TIA with right hemiparesis and
aphasia, and left 90% carotid stenosis
� Scheduled for Left carotid endarterectomy
� The surgery begins
Carotid Endarterectomy
1/22/2015
7
What is happening?
� Anesthesia?
Clamping
Shunt Removal and Unclamping
1/22/2015
8
Carotid Shunting
� Surgeons approach shunting differently
� Selective vs. non-selective shunters
� Shunting itself carries risk
� May increase restenosis
� EEG reduces the use of
shunts
Efficacy of EEG Monitoring in CEA� Significant EEG changes can occur in up to 25% of cases
� despite this, strokes do not occur in a majority of these cases without shunting
� In series of 469 patients undergoing CEAs without carotid shunting but with EEG monitoring, � 44 patients suffered significant EEG changes� 6 of these suffered intraoperative strokes� It is also possible that if selective shunting had been used here based on
EEG, 6 strokes may have been averted in these cohorts.
� The use of selective shunting based on EEG is further supported by a series of 369 patients � 73 patients were shunted based on significant EEG changes
and no intraoperative strokes occurred in the cohort
� May improve outcomes (Sundt)
Blume et al. 1986; Redekop and Ferguson 1992; Zampella et al. 1991; Ballotta et al. 1997
Techniques in CEA
� Meta-analysis of 4664 measurements taken form 29 studies (Cochrane style review)
� Trials of 20 or more patients
� Cerebral monitoring compared to clinical monitoring
during regional anesthesia
� TCD (739), cerebral saturation(320),stump pressure
(2549), EEG (742), EP (187), JVP (79), jugular venous lactate (48)
� Stump pressure with EEG or TCD superior
� Number of EEG channels Can J Anesthsth, 2013 60:266-279

1/22/2015
9
EEG, Aortic Arch Surgery and Deep
Hypothermic Circulatory Arrest (DHCA)� These repairs require discontinuation of
CPB to complete the repair (DHCA)
� Deep hypothermia is used as neuroprotection to allow the repair
� EEG is used as a criteria for initiating DHCA following cooling
� There is a typical pattern that occurs with cooling
� Isoelectric EEG occurs around 12-180C
� Time of recovery of EEG with rewarming may be predictive of injury
� Identification of focal stroke
Stecker, M. Deep hypothermic circulatory arrest I: 2001
Aortic Dissection�Risk
�Malperfusion
�Hypotension
�Ischemic Stroke
The Distal Aorta
� We are advancing?
� Subclavian-Carotid Bypass
� Open Distal Aortic Repairs involving the left subclavian artery with and without stenting (Hybreds or Zone 2 repairs) or TEVAR
� Aortic dissections
� The left vertebral artery is at risk
� Particularly if this is the dominant vertebral artery
� Need a peripheral response
� Posterior circulation strokes
� These cases need both upper and lower SSEP monitoring

1/22/2015
10
EEG during Aneurysm Surgery
� Monitoring for brain retraction, anesthetic depth, burst suppression, temporary arterial occlusion,
permanent clip, vasospasm, thrombosis
� Limitations of scalp EEG
� ECoG (cortical EEG) silicon strip electrodes
� MCA aneurysms
� Limitations deep structures
� Combined with evoked potentials
� Doppler
Transcranial Doppler Ultrasound
� Uses high-energy bidirectional pulsed Doppler sound wave
� Doppler principle is the frequency shift of an echo returning from a moving object which is proportional to its velocity� Piezoelectric crystal makes
high frequency vibrations
� Typically low frequency (2 MHz)� Can penetrate the thin areas
human skullMohr, Stroke: 2004
TCD
� Sound wave is reflected at higher or lower frequency depending on the velocity of the reflector
� Blood has multiple reflectors
� The equipment detects reflections over a linear range at a given depth
� A waveform is created based on Fourier transformation of the Doppler signal and reflects the blood velocity at particular depths
� Real color flow imaging is available
1/22/2015
11
TCD
� Probes have both transmitters and receivers
� Flow towards the probe is a positive velocity while flow away from the probe is negative
� Insonation depth is controlled by gating that is
the time interval which pulsed echos are
recorded
� Multigating is now possible allows the visualization of velocity signals over a wide
depth range
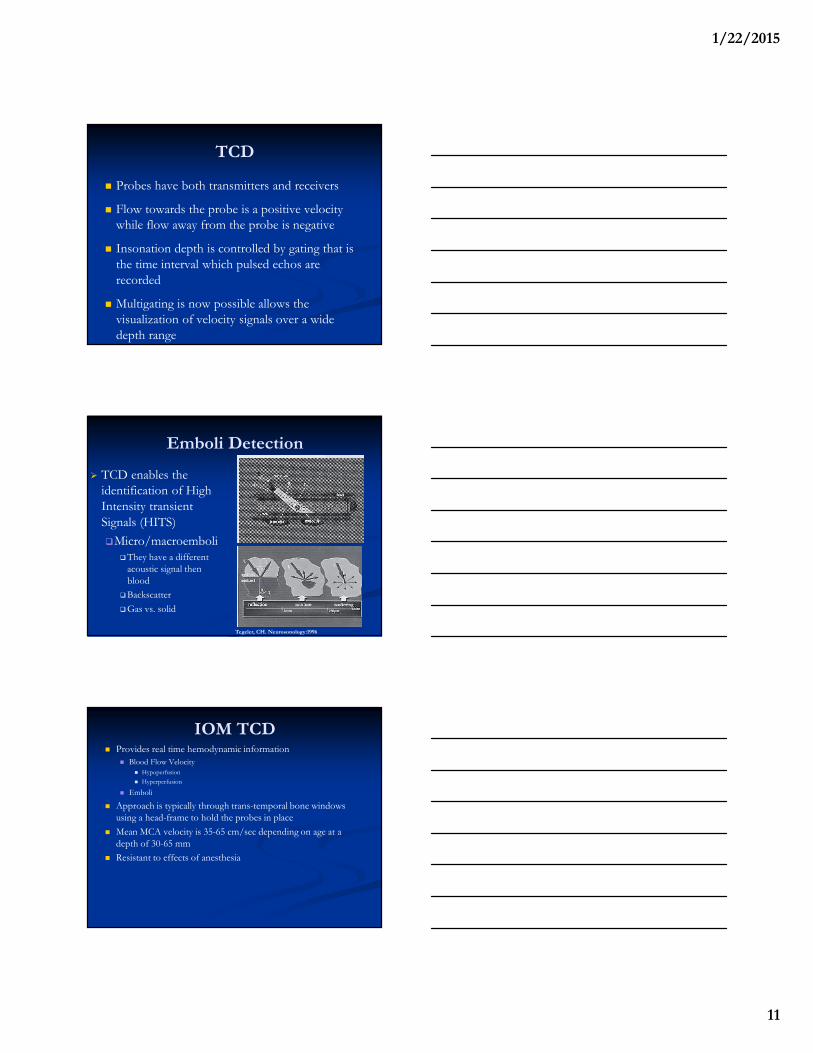
Emboli Detection
� TCD enables the identification of High
Intensity transient
Signals (HITS)
�Micro/macroemboli�They have a different
acoustic signal then blood
�Backscatter
�Gas vs. solid
Tegeler, CH. Neurosonology:1996
IOM TCD� Provides real time hemodynamic information
� Blood Flow Velocity
� Hypoperfusion
� Hyperperfusion
� Emboli
� Approach is typically through trans-temporal bone windows using a head-frame to hold the probes in place
� Mean MCA velocity is 35-65 cm/sec depending on age at a depth of 30-65 mm
� Resistant to effects of anesthesia

1/22/2015
12
Power M-mode TCD� Allows for measurements of flow velocity and direction of all major cerebral
vessels through a depth of approximately 5 cm.
Limitations of TCD
� Threshold questions
� Reductions in flow of more than 50%
� 10% of people have no window
� Differentiating the type and size of emboli
� Gas vs. solid
� Whether they are important?
� Number?
� Equipment can be cumbersome
� Changes in temperature and CO2 can effect flow
TCD in Carotid Surgery
� Detection of intraoperative emboli� May alter technique
� Criteria for shunting or increasing blood pressure to prevent ischemia during cross-clamping � decreases in the velocity greater than 60% result involved flow
less than 20 mL/100 g/minute and EEG suppression
� Impending stroke or occlusion based on emboli after the endarterectomy
� >1/minute HIT may be predictive impending stroke
� Dextran 50, re-exploration
� May identify those at risk for Post-operative hyperperfusion syndrome

1/22/2015
13
TCD, Cardiac Surgery and CPB
� Embolism
� Gas vs. Solid
� Pump or open chamber Procedures
� TCD can be used to detect problems in the bypass
pump (air leaks) or improper de-airing
� Whether microemboli are responsible for
neurocognitive injury is questionable
� Teaching the surgeon (biofeedback)
� De-airing, cannulation, cross-clamping
� TAVI experience
TCD in Aortic Arch Surgery and Deep
Hypothermic Circulatory Arrest
� Ensures adequate retrograde and antegrade cerebral perfusion
� Shown to decrease the rate of Neuro-cognitive deficits following DHCA
� 25 % patients may have inadequate circle of Willis to handle single carotid antegrade flow
� Allows for monitoring in cases where EEG and evoked potentials may be attenuated or absent due to temperature
� Embolic events are registered as High Intensity Transient Signals (HITS) on PMD-TCD, which can be automatically detected by a proprietary algorithm available on the PMD-TCD system
� HITS can also be inspected visually by observation of the PMD-TCD display.
� Autoregulation during rewarming

1/22/2015
14
� Balloon inflated too high on left carotid, resulting in a technical cannula malpositioning- flow decreases bilaterally. Flow begins to return 30 seconds after surgeon begins adjustments to cannula. Flow fully and permanently returns at 90 secs after cannula adjustments begin. EEG was flat due to
anesthesia and cooling, and thus unable to detect this change.
Multimodality Monitoring
� Combining the techniques may be beneficial
� TCD and EEG (SSEPS)
� They examine different mechanisms
� Flow and emboli vs. electrical activity
1/22/2015
15
Potential Therapies in Cardiac and
Vascular Surgery Based on IOM� Intraoperative stroke detected by neurophysiologic monitoring
� Current options limited
� Ischemic or Hemorrhagic stroke
� Supportive Care
� Increase intravascular volume (transfusion, albumen)
� Treat hyperglycemia
� Avoid hyperthermia
� Thrombolytic Therapy
� Intra-arterial Thrombolysis (6 hour time window)
� Clot Retrieval Devices
� Retrograde flow (YEH et al, 2003)
edu