Manual&Therapy&and&the&Canine&Thoracic&Spine&Therapy&and&the&Canine&Thoracic&Spine& ...
41
Manual Therapy and the Canine Thoracic Spine Copyright Laurie EdgeHughes, 2013 1 Manual Therapy and the Canine Thoracic Spine Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT The Canine Fitness Centre Ltd www.CanineFitness.com Four Leg Rehab Inc www.FourLeg.com The Canine Spine: Advanced Assessment & Treatment Techniques MANUAL THERAPY LITERATURE REVIEW Laurie EdgeHughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT IntroducNon • FuncNon = Mobility with Stability • The Integrated Approach – Form Closure – Force Closure – Motor Control & Timing • Manual Therapies – MobilizaNon & TracNon... Disturbed Harmony by Giorgio Vaselli MobilizaNon Form Closure: MobilizaNon or manipulaNon aimed at restoring mobility and/or correcNon of osseous alignment. “If exercise is prescribed first, without firstly restoring joint mobility, the paNent’s pain and dysfuncNon o\en gets worse.” (Lee & Lee 2004) MobilizaNon The gentle coaxing of movement by passive rhythmical oscillaNons ▪ To treat sNffness ▪ To treat pain (rather than sNffness) Maitland et al 2005
-
Upload
hoangkhanh -
Category
Documents
-
view
219 -
download
0
Transcript of Manual&Therapy&and&the&Canine&Thoracic&Spine&Therapy&and&the&Canine&Thoracic&Spine& ...

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
1
Manual Therapy and the
Canine Thoracic Spine
Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT
The Canine Fitness Centre Ltd www.CanineFitness.com
Four Leg Rehab Inc www.FourLeg.com
The Canine Spine: Advanced Assessment & Treatment
Techniques
MANUAL THERAPY LITERATURE REVIEW
Laurie Edge-‐Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT
IntroducNon
• FuncNon = Mobility with Stability
• The Integrated Approach – Form Closure – Force Closure – Motor Control & Timing
• Manual Therapies – MobilizaNon & TracNon...
Disturbed Harmony by Giorgio Vaselli
MobilizaNon
Form Closure: MobilizaNon or manipulaNon aimed at restoring mobility and/or correcNon of osseous alignment.
“If exercise is prescribed first, without firstly restoring joint mobility, the paNent’s pain and dysfuncNon o\en gets worse.” (Lee & Lee 2004)
MobilizaNon The gentle coaxing of movement by passive rhythmical oscillaNons ▪ To treat sNffness ▪ To treat pain (rather than sNffness)
Maitland et al 2005
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
2
MobilizaNon
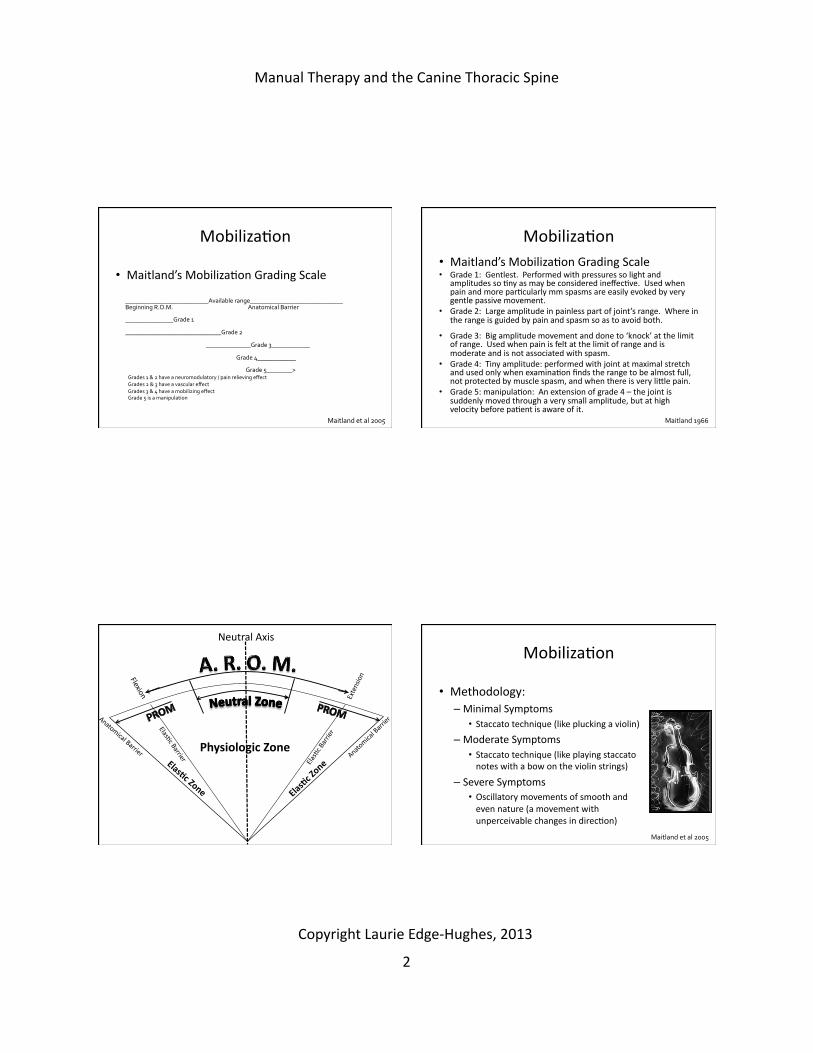
• Maitland’s MobilizaNon Grading Scale
__________________________Available range_____________________________ Beginning R.O.M. Anatomical Barrier
_______________Grade 1
______________________________Grade 2
______________Grade 3____________
Grade 4____________
Grade 5________>
Maitland et al 2005
Grades 1 & 2 have a neuromodulatory / pain relieving effect Grades 2 & 3 have a vascular effect Grades 3 & 4 have a mobilizing effect Grade 5 is a manipulation
MobilizaNon • Maitland’s MobilizaNon Grading Scale • Grade 1: Gentlest. Performed with pressures so light and
amplitudes so Nny as may be considered ineffecNve. Used when pain and more parNcularly mm spasms are easily evoked by very gentle passive movement.
• Grade 2: Large amplitude in painless part of joint’s range. Where in the range is guided by pain and spasm so as to avoid both.
• Grade 3: Big amplitude movement and done to ‘knock’ at the limit of range. Used when pain is felt at the limit of range and is moderate and is not associated with spasm.
• Grade 4: Tiny amplitude: performed with joint at maximal stretch and used only when examinaNon finds the range to be almost full, not protected by muscle spasm, and when there is very lidle pain.
• Grade 5: manipulaNon: An extension of grade 4 – the joint is suddenly moved through a very small amplitude, but at high velocity before paNent is aware of it.
Maitland 1966
Physiologic Zone Elas0c Zone Ela
s0c Zone
Flexion Extension
Anatomical Barrier Anatomical Barrier
Neutral Axis
ElasNc Barrier
ElasNc Barrier
MobilizaNon
• Methodology: – Minimal Symptoms
• Staccato technique (like plucking a violin) – Moderate Symptoms
• Staccato technique (like playing staccato notes with a bow on the violin strings)
– Severe Symptoms • Oscillatory movements of smooth and even nature (a movement with unperceivable changes in direcNon)
Maitland et al 2005

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
3
MobilizaNon
• Passive & AcNve Movements – PreservaNon of full ROM – PreservaNon of strength and flexibility of periarNcular Nssue
• Physiological Movements – AcNve or passive FUNCTIONAL movements
• Accessory Movements – Conjunct movements
• Both are used to mobilize joints Maitland et al 2005; Björnsdóttir & Kumar 1997
MobilizaNon
• Passive Accessory vs. Passive Physiological Mov’ts
Maitland et al 2005
PAIVMs (Passive Accessory Intervertebral Movements)
PPIVMS (Passive Physiological Intervertebral Movements)
Usually the first choice for manual treatment
Use if irritable to touch, or if worsened a\er palpaNon, or if neurologic signs
ParNcularly useful when loss of moNon in extension (? Canine applicaNon or not?)
ParNcularly useful when loss of moNon in flexion (? Canine applicaNon or not?)
Eg: Dorso-‐ventral (PA) pressures, TracNon, Transverse pressures.
Eg: Large movements – flexion, extension, side bending, rotaNon.
MobilizaNon
• SelecNon of techniques – To OPEN a facet joint
• Rotate or Side bend AWAY from the side of pain • Dorso-‐Ventral Pressures ON the side of pain • Transverse Pressures TOWARDS the side of pain
– To CLOSE a facet joint • Opposite of above • And if using a D-‐V pressure – direct the pressure medially
• Rule of thumb… – Try OPENING first!
Maitland et al 2005
MobilizaNon
• SelecNon of techniques based on PATHOLOGY – Acute pain or Nerve root symptoms
• StaNc tracNon – gentle – Chronic Nerve root symptoms
• Central D-‐V pressure, rotaNons, tracNon – Discogenic signs
• Generalized rotaNon – Facet joint signs
• Localized rotaNon – OsteoarthriNs
• Large movements throughout range (accessory & physiologic) Maitland et al 2005

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
4
MobilizaNon
• How bloody long do I do the technique(s) for? – TIME – If Irritable: then 20 – 30 seconds, repeated 1 or 2 Nmes
– If Non-‐Irritable: then 1 minute, repeated 4 – 6 Nmes
– TECHNIQUES PER SESSION – Add them in, but reassess before and a\er each new technique
– Perform the most effecNve technique (again) last
Maitland et al 2005
MobilizaNon
• Mechanical – RestoraNon of voluntary movement
– Aids in carNlage nutriNon – Aids in intervertebral disc nutriNon – Aids in metabolism of so\ Nssue structures
– Improved rate and quality of tendon repair
Zusman 1986; Björnsdóttir & Kumar 1997
MobilizaNon
• Requirements for a Mechanical Effect – RepeNNve passive joint movements (oscillaNons) need to be carried out at the limit of the joint’s available range in order to achieve a mechanical effect • i.e. Tissues need to be stretched
Zusman 1986
MobilizaNon
• Neurological Effects – ReducNon in acute pain – InhibiNon of reflex muscle contracNons
Zusman 1986; Katavich 1998; Björnsdóttir & Kumar 1997; Zelle et al 2005

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
5
MobilizaNon
• Neurological Effects: – RepeNNve (oscillatory) or sustained manual sNmulaNon results in a hysteresis effect: • Inhibitory effect on low threshold mechanoreceptors (group I & II)
• Inhibitory effect on high threshold nociceptors (group III & IV)
• THUS reducing intra-‐arNcular pressure and peripheral afferent discharge
Zusman 1986; Katavich 1998; Conroy & Hayes 1998; Sterling et al 2001
MobilizaNon
• Neurological effects – “cheat sheet”
MobilizaNon
Postulated Cellular Level Effects Mechanical / ConnecNve Nssue remodelling ▪ Cellular modulaNon ▪ Release of enzymes to breakdown cross links ▪ SimulaNon of fibroblast synthesis of collagen proteoglycans ▪ Realignment of old fibres ▪ Increase interfibre distance ▪ Increase interfibre lubricaNon ▪ Alignment of new fibres ▪ Stretching arNcular capsule / segmental muscles ▪ Breaking intra-‐arNcular adhesions ▪ Vertebral movement
Maffey LL 2007
MobilizaNon
• Postulated Cellular Level Effects – ArNcular CarNlage Changes
• Alter joint lubricaNon • Enhance carNlage nutriNon • Movement of joint inclusions (meniscoids) or loose bodies (carNlage fibrillaNon)
• Shi\ hard fragment of intervertebral disc
Maffey LL 2007

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
6
MobilizaNon
• Postulated Cellular Level Effects – Neurological effects *
• SNmulaNon of Type I and type II mechanoreceptors • Inhibit transmission of nocicepNve impulses
• Decrease pain percepNon • Relieve mechanical irritaNon of nervous system
• AcNvaNon of arNcular mechanoreceptors
• SNmulaNon of sympatheNc nervous system
* Validated effects Maffey LL 2007
MobilizaNon
• Postulated Cellular Level Effects – Neuromuscular response *
• Alter afferent input to effect efferent output – relax muscle
• SNmulaNon of muscle spindle and golgi tendon organ – reflex inhibiNon of segmental muscles
• Alter segmental (and more distal) muscle acNvity
• Reflex muscle response locally and at a distance
• Decrease spinal segmental facilitaNon
* Validated effects Maffey LL 2007
MobilizaNon
• Postulated Cellular Level Effects – Alter CirculaNon
• Increase supply of materials required for healing • Remove chemical irritant (hence decreasing nociceptor sNmulaNon)
Maffey LL 2007
MobilizaNon
• Postulated Cellular Level Effects – Physiological *
• Increase beta-‐endorphin levels • Immune system effects
* Validated effects Maffey LL 2007

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
7
MobilizaNon
• Postulated Cellular Level Effects – Joint Tissue Response
• Increase capsule elasNcity • Improve arNcular carNlage nutriNon
• Improve circulaNon • RestoraNon of joint play / accessory glides • RestoraNon of passive / acNve movement
• Decreased pain percepNon
Maffey LL 2007
MobilizaNon
• Research Examples -‐ Effects of MobilizaNon – Improved pressure pain threshold in pts with rheumatoid arthriNs (12 minute P-‐A pressures) (Dhondt et al 1999)
– Improved pain (VAS) & immediate neck ROM in pts with mechanical neck pain (Kanlayanaphotoporn et al 2010)
– A rapid onset analgesic response following joint mobs has been proven in rodent models (Grayson et al 2012)
MobilizaNon
• Research Examples -‐ Effects of MobilizaNon – Unilateral neck mobs facilitated acNvaNon of deep neck flexor muscle firing & reducNon in superficial neck flexor acNvity. (Sterling et al 2001)
– Improves ROM in the human hip & ankle joints and canine carpus (Hoeksma et al 2004; Collins et al 2004; Olson 1987)
– Does Not Change vertebral sNffness or have permanent effect on passive cervical ROM (Nilsson et al 1996; Goodsell et al 2000; Lee et al 1993; Allison et al 2001)
MobilizaNon
• Research Examples -‐ Effects of MobilizaNon – DOES NOT Alter sacrum-‐iIium joint posiNon (on roentgen stereophotgrammetric analysis)
– ManipulaNon might influence so\ Nssue structures, such as joint capsules, muscles, ligaments, tendons and postures Tullberg et al 1998

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
8
MobilizaNon
• Research Examples -‐ Effects of MobilizaNon – Pain is improved & FUNCTIONAL disability is reduced for 6 months following 8 sessions of mobilizaNons & non-‐specific back exercises (Balthazard et al 2012)
– MulNfidus recruitment is enhanced and sustained a\er lumbar manipulaNon which posiNvely impacted FUNCTION (Fritz et al 2012)
MobilizaNon
• THOUGHT:
IF, in fact, mobilizaNons do NOT alter joint posiNon, biomechanics, mobility or long-‐term sNffness, then perhaps we can choose ANY mobilizaNon technique (within reason…) to result in pain relief, reducNon of muscle spasm, improve muscle firing, and enhanced funcNon… followed by neuromuscular retraining.
MobilizaNon
Technical Summary of MobilizaNon Treatment ApplicaNon: PaNent consent received (informed of nature and purpose of mobs, alternate forms of assessment/Rx, associated risks & benefits)
Select starNng posiNon (relaxed and comfortable) Select starNng posiNon of the clinician Select treatment grade Select a sustained oscillatory technique Select duraNon and speed of oscillatory technique (shorter for acute condiNons)
Increase the intensity and duraNon of treatment only when evidence exists that increased dose will not exacerbate pain
Select reassessment technique to use before, during and a\er treatment
Select home program to maintain treatment effects
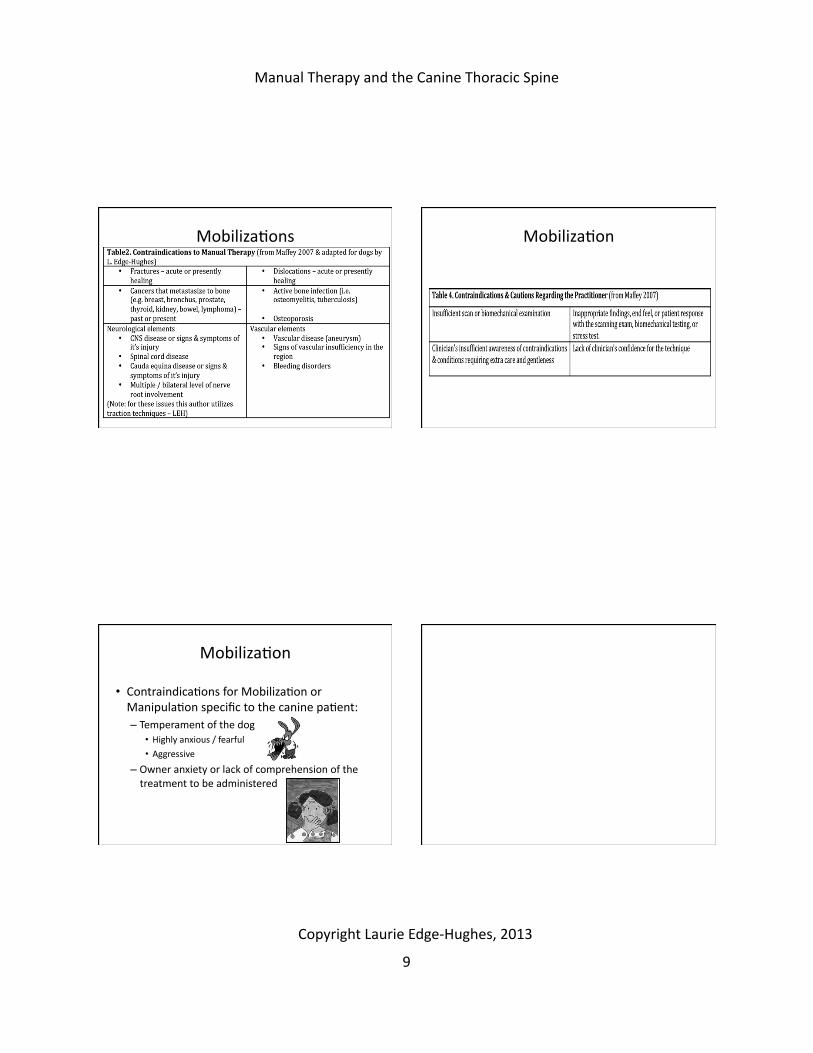
MobilizaNons
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
9
MobilizaNons MobilizaNon
MobilizaNon
• ContraindicaNons for MobilizaNon or ManipulaNon specific to the canine paNent: – Temperament of the dog
• Highly anxious / fearful • Aggressive
– Owner anxiety or lack of comprehension of the treatment to be administered

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
10
TracNon TracNon
• TracNon may break the “cycle of pain” in radiculopathy caused by herniated discs: – Disc herniaNon – Nerve root entrapment in vertebral foramina – Nerve root irritaNon
– Reflexive response to contract adjacent muscles – Further narrowing of foramina – Increased pain.
Jam 2005
TracNon: • reduce inflammaNon • improving circulaNon • reducing swelling
TracNon
• Intermident tracNon – Improves circulaNon & reduces swelling of surrounding Nssues and epidural space • Relieves the inflammatory reacNon of nerve roots
• Contributes to resorpNon and regression of the herniated disc material
– Large extruded discs tend to respond more rapidly
– Creates an alternaNng stretching and relaxaNon of adjacent so\ Nssue structures • Prevents adhesions of the dural sleeve
Constantoyannis et al 2002; Maher 2004; Ozturk et al 2005
TracNon
• Findings: – Human paNents with cervical radiculopathy < 12 weeks show less favourable improvement. • Early intervenNon is more successful
– The response to early therapeuNc intervenNon in large extruded discs is even more favourable.
– Benefits to lumbar tracNon with acute radicular pain of less than 6 weeks and concomitant neurological deficits.
Krause et al 2000
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
11
TracNon
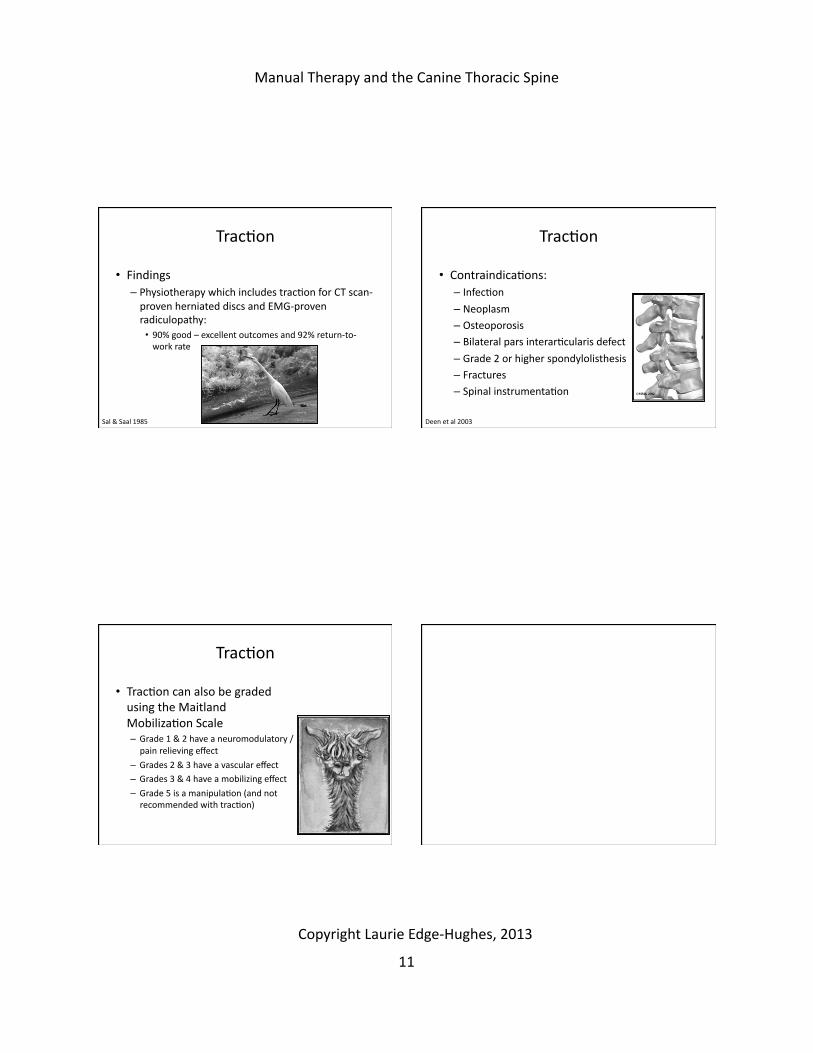
• Findings – Physiotherapy which includes tracNon for CT scan-‐proven herniated discs and EMG-‐proven radiculopathy: • 90% good – excellent outcomes and 92% return-‐to-‐work rate
Sal & Saal 1985
TracNon
• ContraindicaNons: – InfecNon – Neoplasm – Osteoporosis – Bilateral pars interarNcularis defect – Grade 2 or higher spondylolisthesis – Fractures – Spinal instrumentaNon
Deen et al 2003
TracNon
• TracNon can also be graded using the Maitland MobilizaNon Scale – Grade 1 & 2 have a neuromodulatory / pain relieving effect
– Grades 2 & 3 have a vascular effect – Grades 3 & 4 have a mobilizing effect
– Grade 5 is a manipulaNon (and not recommended with tracNon)

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
12
The Myofascial System
• THE MYOFASCIAL SYSTEM – There is a variance of myofascial states that may accompany a vertebral dysfuncNon
– Treatment of the muscle state tends to occur a\er treatment of the vertebral dysfuncNon.
The Myofascial System
• THE MYOFASCIAL SYSTEM Muscle Tone Descrip0on Treatment Hypertonicity Involuntary splinNng
Muscle response is triggered by nocicepNon in an effort to splint the back from further stress and injury.
Ignore the muscle reacNon and treat the cause
Chemical splinNng
Also involuntary (as above), it results in the retenNon of waste products which give rise to back pain. Overuse can also cause chemical splinNng. Muscle retaining waste metabolites will appear to have an elevated resNng tone and are tender and doughy to touch.
Treatments can include heat, manual muscle therapies, stretching and treatment of the underlying cause.
Voluntary splinNng
Voluntary splinNng occurs if nocicepNon reaches the threshold for pain, and the paNent voluntarily splints the affected part.
Treatment involves the prescripNon of movement and moNon needs to be encouraged.
Adapted from Paris & ViN 2007
The Myofascial System
• THE MYOFASCIAL SYSTEM
Muscle Tone Descrip0on Treatment Hypotonicity Disuse atrophy The presence of pain or sNffness has
resulted in a loss of normal mobility. The muscles may feel to have lost bulk, lack normal none and feel somewhat fibrous.
Treatment is to restore moNon, heat, and treatments to encourage circulaNon, followed by specific exercises.
WasNng & fibrosis
The result of neurological or surgical interference with normal nerve conducNon.
Treatment is to promote circulaNon and exercises to train the remaining muscles.
Adapted from Paris & ViN 2007
The Myofascial System
• THE MYOFASCIAL SYSTEM
Muscle Tone Descrip0on Treatment Normal tone / Shortened Nssues
AdapNve shortening results from muscles being held in a shortened posiNon.
Treatment includes muscle elongaNon by stretching or massage.
Compartment syndrome
Hypertrophy can result in muscle restricNon within their fascial compartments, resulNng in chronic unilateral or bilateral paravertebral back pain.
Treatment includes mobilizaNons to vertebral structures and stretching out of the connecNve Nssue envelope.
Adapted from Paris & ViN 2007
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
13
Conclusion
• Manual therapies such as mobilizaNons / manipulaNon and tracNon: – Have a proven track record clinically
• Both in pracNce and in research – Have a limited amount research to validate their cellular effects
– SNll need further research to elucidate the full potenNal of manual therapy and/or dispel any falsely propagated myths.
– The Myofascial system should also be addressed but likely secondarily to the skeletal system
On with the show!

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
14
The Canine Spine: Advanced Assessment & Treatment
Techniques
THE CANINE THORAX
Laurie Edge-‐Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT Laurie Edge-‐Hughes, BScPT, MAnimSt (Animal Physio), CAFCI, CCRT
The Thorax
• Thorax = thoracic vertebra, ribs, and sternum + adaching muscles – A biomechanical approach to treatment
• Requires and understanding of normal funcNon
• Integrates joint mobility and stability
– The dog is a good research model for the human thoracic vertebra.... • Hence allowing a transfer of assessment/treatment strategies
Lee 2003; Oda et al 1996; Takeuchi et al 1999
T/S: Anatomy & Biomechanics
• Bodies of the thoracic vertebra are shorter than those of the lumbar or cervical spines
• T1 – T7/8 spinous processes are massive
• The spinous processes decline in length from T1 to T9/10 and are caudally inclined.
• T11 is the anNclinal vertebra and the transiNon segment to the thoracolumbar region
Evans 1993
T/S: Anatomy and Biomechanics
• The spinous Nps of T6 – T9 overlie the bodies of the vertebra caudal to them.
• T12/ 13 are directly cranial to the bodies. • The Transverse processes are short, blunt, and irregular
Evans 1993
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
15
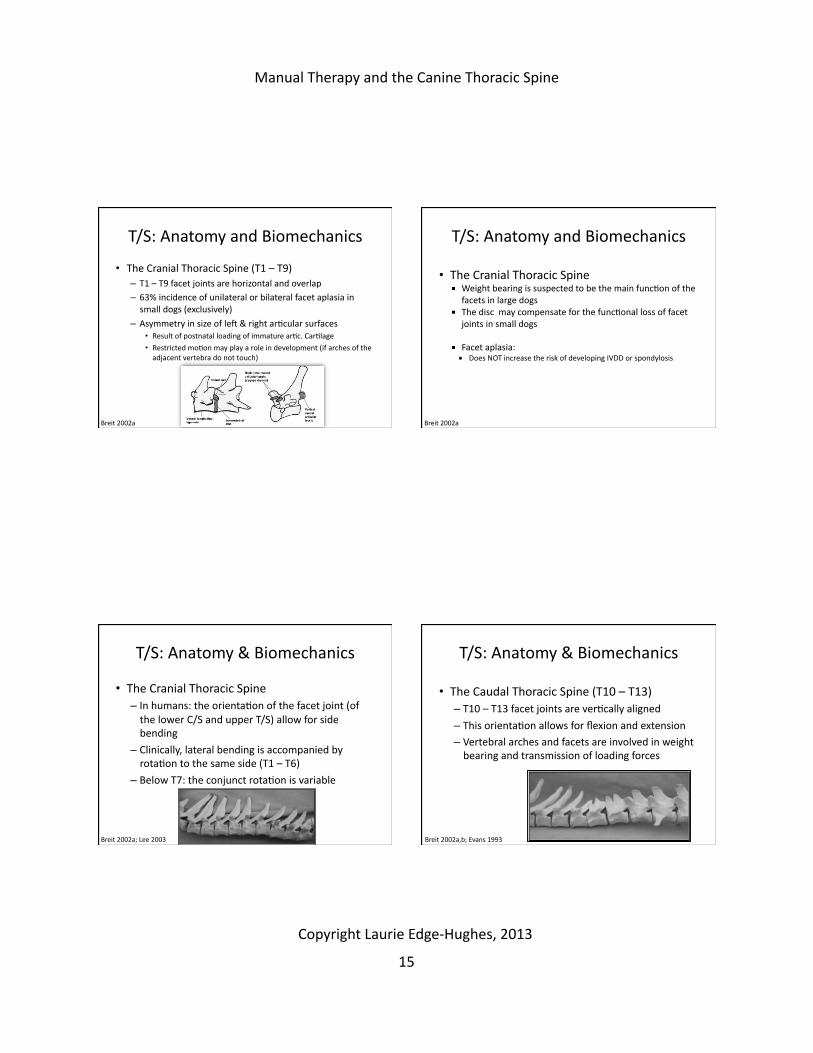
T/S: Anatomy and Biomechanics
• The Cranial Thoracic Spine (T1 – T9) – T1 – T9 facet joints are horizontal and overlap – 63% incidence of unilateral or bilateral facet aplasia in small dogs (exclusively)
– Asymmetry in size of le\ & right arNcular surfaces • Result of postnatal loading of immature arNc. CarNlage
• Restricted moNon may play a role in development (if arches of the adjacent vertebra do not touch)
Breit 2002a
T/S: Anatomy and Biomechanics
• The Cranial Thoracic Spine Weight bearing is suspected to be the main funcNon of the
facets in large dogs The disc may compensate for the funcNonal loss of facet
joints in small dogs
Facet aplasia: Does NOT increase the risk of developing IVDD or spondylosis
Breit 2002a
T/S: Anatomy & Biomechanics
• The Cranial Thoracic Spine – In humans: the orientaNon of the facet joint (of the lower C/S and upper T/S) allow for side bending
– Clinically, lateral bending is accompanied by rotaNon to the same side (T1 – T6)
– Below T7: the conjunct rotaNon is variable
Breit 2002a; Lee 2003
T/S: Anatomy & Biomechanics
• The Caudal Thoracic Spine (T10 – T13) – T10 – T13 facet joints are verNcally aligned – This orientaNon allows for flexion and extension – Vertebral arches and facets are involved in weight bearing and transmission of loading forces
Breit 2002a,b; Evans 1993

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
16
T/S: Anatomy & Biomechanics
• The Caudal Thoracic Spine (T10 – T13) – In Normally posiNoned vertebra (parallel):
• The caudal Nps of the caudal arNcular process do not come into contact with the adjoining cranial arNcular surfaces
• Lateral bending is restricted by accessory processes • RotaNon is accomplished only in flexion in this region
Breit 2002b
T/S: Anatomy & Biomechanics
• The Caudal Thoracic Spine (T10 – T13) – T10 – L7 is normal kyphoNc
– Lordosis can occur with the loss of elasNcity of the bowstring construct • The caudal arNcular surfaces adapt to higher body-‐weight by the presence of LARGER arNcular surfaces
• Thus creaNng arNcular surfaces not only laterally but also caudally and/or ventrally
Breit 2002b
T/S: Anatomy & Biomechanics
• The Caudal Thoracic Spine (T10 – T13) – Ventrally directed shears cause ventral facets
• Allows for an increase of loading capacity – Excessive extension causes caudal facets
• Due to loss of elasNc stability – Ventral and caudal facets (together) create a ball and socket joint • Reduces spinal stability & NOTHING resists axial rotaNon
Breit 2002b
T/S: Anatomy & Biomechanics
• The Caudal Thoracic Spine (T10 – T13) – In humans, arNcular asymmetry is highly prevalent
• Typically 41% – The thoracic spine looks like and responds like the lumbar spine • An abrupt decrease in the range of axial rotaNon
Singer 2004
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
17
T/S: Anatomy & Biomechanics
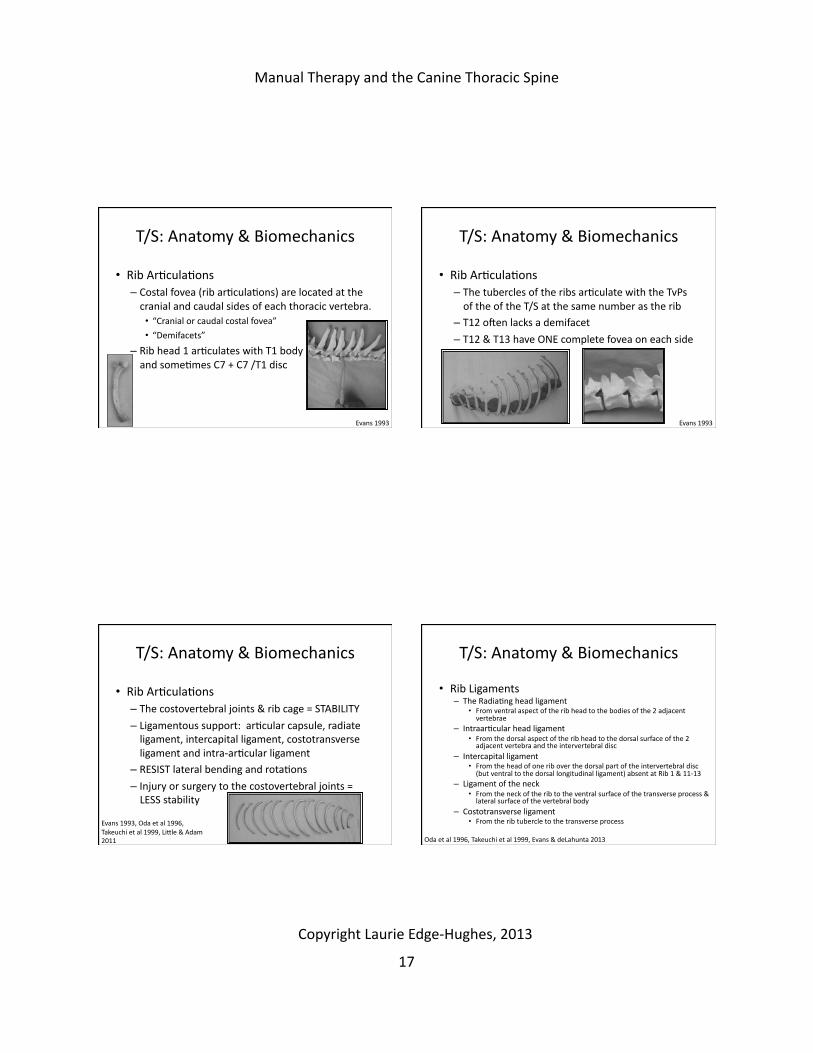
• Rib ArNculaNons – Costal fovea (rib arNculaNons) are located at the cranial and caudal sides of each thoracic vertebra. • “Cranial or caudal costal fovea” • “Demifacets”
– Rib head 1 arNculates with T1 body and someNmes C7 + C7 /T1 disc
Evans 1993
T/S: Anatomy & Biomechanics
• Rib ArNculaNons – The tubercles of the ribs arNculate with the TvPs of the of the T/S at the same number as the rib
– T12 o\en lacks a demifacet
– T12 & T13 have ONE complete fovea on each side
Evans 1993
T/S: Anatomy & Biomechanics
• Rib ArNculaNons – The costovertebral joints & rib cage = STABILITY – Ligamentous support: arNcular capsule, radiate ligament, intercapital ligament, costotransverse ligament and intra-‐arNcular ligament
– RESIST lateral bending and rotaNons – Injury or surgery to the costovertebral joints = LESS stability
Evans 1993, Oda et al 1996, Takeuchi et al 1999, Lidle & Adam 2011
T/S: Anatomy & Biomechanics
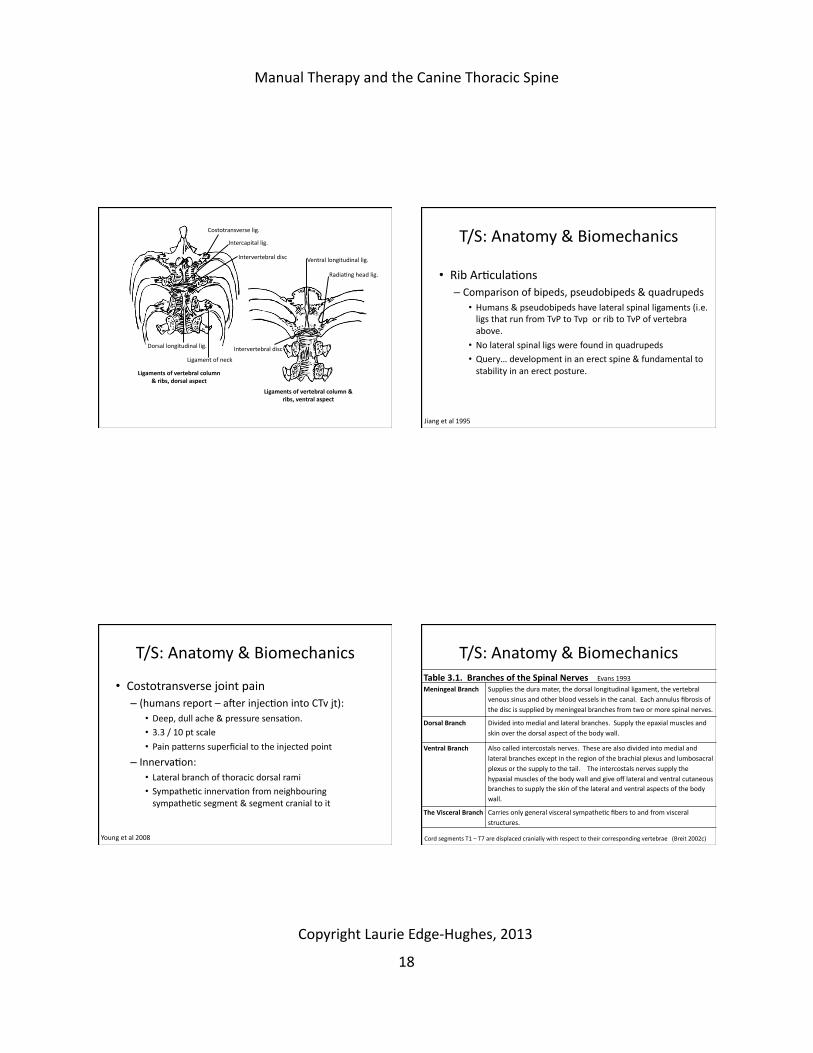
• Rib Ligaments – The RadiaNng head ligament
• From ventral aspect of the rib head to the bodies of the 2 adjacent vertebrae
– IntraarNcular head ligament • From the dorsal aspect of the rib head to the dorsal surface of the 2 adjacent vertebra and the intervertebral disc
– Intercapital ligament • From the head of one rib over the dorsal part of the intervertebral disc (but ventral to the dorsal longitudinal ligament) absent at Rib 1 & 11-‐13
– Ligament of the neck • From the neck of the rib to the ventral surface of the transverse process & lateral surface of the vertebral body
– Costotransverse ligament • From the rib tubercle to the transverse process
Oda et al 1996, Takeuchi et al 1999, Evans & deLahunta 2013
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
18
Dorsal longitudinal lig.
Ligament of neck
Intervertebral disc
Intercapital lig.
Costotransverse lig.
Intervertebral disc
Ventral longitudinal lig.
RadiaNng head lig.
Ligaments of vertebral column & ribs, dorsal aspect
Ligaments of vertebral column & ribs, ventral aspect
T/S: Anatomy & Biomechanics
• Rib ArNculaNons – Comparison of bipeds, pseudobipeds & quadrupeds
• Humans & pseudobipeds have lateral spinal ligaments (i.e. ligs that run from TvP to Tvp or rib to TvP of vertebra above.
• No lateral spinal ligs were found in quadrupeds • Query… development in an erect spine & fundamental to stability in an erect posture.
Jiang et al 1995
T/S: Anatomy & Biomechanics
• Costotransverse joint pain – (humans report – a\er injecNon into CTv jt):
• Deep, dull ache & pressure sensaNon. • 3.3 / 10 pt scale • Pain paderns superficial to the injected point
– InnervaNon: • Lateral branch of thoracic dorsal rami • SympatheNc innervaNon from neighbouring sympatheNc segment & segment cranial to it
Young et al 2008
T/S: Anatomy & Biomechanics Table 3.1. Branches of the Spinal Nerves Evans 1993 Meningeal Branch Supplies the dura mater, the dorsal longitudinal ligament, the vertebral
venous sinus and other blood vessels in the canal. Each annulus fibrosis of the disc is supplied by meningeal branches from two or more spinal nerves.
Dorsal Branch Divided into medial and lateral branches. Supply the epaxial muscles and skin over the dorsal aspect of the body wall.
Ventral Branch Also called intercostals nerves. These are also divided into medial and lateral branches except in the region of the brachial plexus and lumbosacral plexus or the supply to the tail. The intercostals nerves supply the hypaxial muscles of the body wall and give off lateral and ventral cutaneous branches to supply the skin of the lateral and ventral aspects of the body wall.
The Visceral Branch Carries only general visceral sympatheNc fibers to and from visceral structures.
Cord segments T1 – T7 are displaced cranially with respect to their corresponding vertebrae (Breit 2002c)
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
19
T/S: Anatomy & Biomechanics
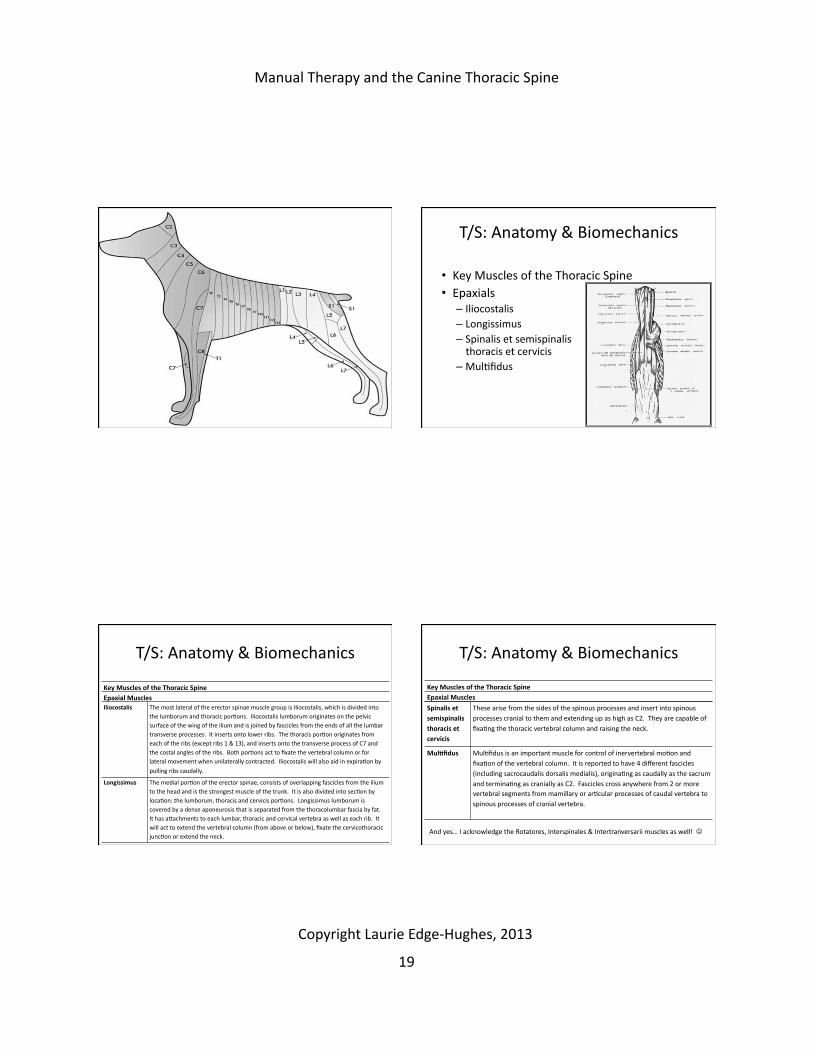
• Key Muscles of the Thoracic Spine • Epaxials
– Iliocostalis – Longissimus – Spinalis et semispinalis thoracis et cervicis
– MulNfidus
T/S: Anatomy & Biomechanics
Key Muscles of the Thoracic Spine Epaxial Muscles Iliocostalis The most lateral of the erector spinae muscle group is Iliocostalis, which is divided into
the lumborum and thoracic porNons. Iliocostalis lumborum originates on the pelvic surface of the wing of the ilium and is joined by fascicles from the ends of all the lumbar transverse processes. It inserts onto lower ribs. The thoracis porNon originates from each of the ribs (except ribs 1 & 13), and inserts onto the transverse process of C7 and the costal angles of the ribs. Both porNons act to fixate the vertebral column or for lateral movement when unilaterally contracted. Iliocostalis will also aid in expiraNon by
pulling ribs caudally.
Longissimus The medial porNon of the erector spinae, consists of overlapping fascicles from the ilium to the head and is the strongest muscle of the trunk. It is also divided into secNon by locaNon: the lumborum, thoracis and cervicis porNons. Longissimus lumborum is covered by a dense aponeurosis that is separated from the thoracolumbar fascia by fat. It has adachments to each lumbar, thoracic and cervical vertebra as well as each rib. It will act to extend the vertebral column (from above or below), fixate the cervicothoracic juncNon or extend the neck.
T/S: Anatomy & Biomechanics
Key Muscles of the Thoracic Spine Epaxial Muscles
Spinalis et semispinalis thoracis et cervicis
These arise from the sides of the spinous processes and insert into spinous processes cranial to them and extending up as high as C2. They are capable of fixaNng the thoracic vertebral column and raising the neck.
Mul0fidus MulNfidus is an important muscle for control of inervertebral moNon and fixaNon of the vertebral column. It is reported to have 4 different fascicles (including sacrocaudalis dorsalis medialis), originaNng as caudally as the sacrum and terminaNng as cranially as C2. Fascicles cross anywhere from 2 or more vertebral segments from mamillary or arNcular processes of caudal vertebra to spinous processes of cranial vertebra.
And yes… I acknowledge the Rotatores, Interspinales & Intertranversarii muscles as well!
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
20
T/S: Anatomy & Biomechanics
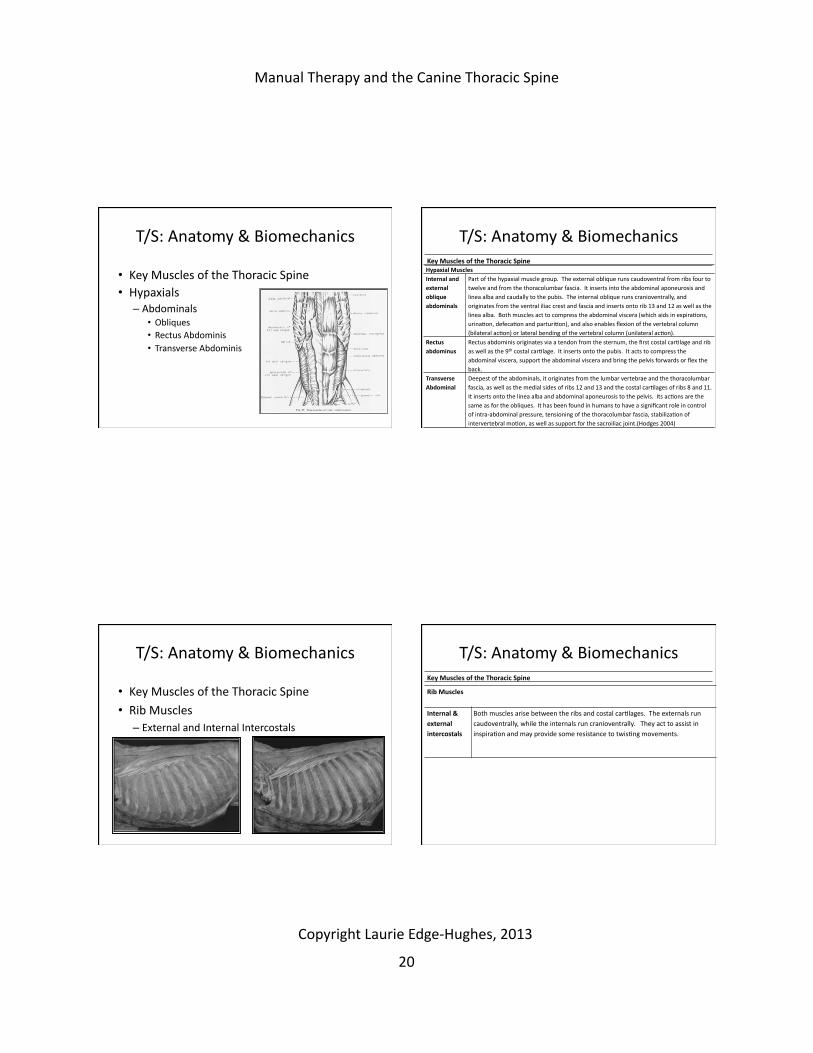
• Key Muscles of the Thoracic Spine • Hypaxials
– Abdominals • Obliques • Rectus Abdominis • Transverse Abdominis
T/S: Anatomy & Biomechanics Key Muscles of the Thoracic Spine Hypaxial Muscles Internal and external oblique abdominals
Part of the hypaxial muscle group. The external oblique runs caudoventral from ribs four to twelve and from the thoracolumbar fascia. It inserts into the abdominal aponeurosis and linea alba and caudally to the pubis. The internal oblique runs cranioventrally, and originates from the ventral iliac crest and fascia and inserts onto rib 13 and 12 as well as the linea alba. Both muscles act to compress the abdominal viscera (which aids in expiraNons, urinaNon, defecaNon and parturiNon), and also enables flexion of the vertebral column (bilateral acNon) or lateral bending of the vertebral column (unilateral acNon).
Rectus abdominus
Rectus abdominis originates via a tendon from the sternum, the first costal carNlage and rib as well as the 9th costal carNlage. It inserts onto the pubis. It acts to compress the abdominal viscera, support the abdominal viscera and bring the pelvis forwards or flex the back.
Transverse Abdominal
Deepest of the abdominals, it originates from the lumbar vertebrae and the thoracolumbar fascia, as well as the medial sides of ribs 12 and 13 and the costal carNlages of ribs 8 and 11. It inserts onto the linea alba and abdominal aponeurosis to the pelvis. Its acNons are the same as for the obliques. It has been found in humans to have a significant role in control of intra-‐abdominal pressure, tensioning of the thoracolumbar fascia, stabilizaNon of intervertebral moNon, as well as support for the sacroiliac joint.(Hodges 2004)
T/S: Anatomy & Biomechanics
• Key Muscles of the Thoracic Spine • Rib Muscles
– External and Internal Intercostals
T/S: Anatomy & Biomechanics Key Muscles of the Thoracic Spine
Rib Muscles
Internal & external intercostals
Both muscles arise between the ribs and costal carNlages. The externals run caudoventrally, while the internals run cranioventrally. They act to assist in inspiraNon and may provide some resistance to twisNng movements.
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
21
S/S of Thoracic Spine DysfuncNons
• Human Symptomology: – Pressure headaches, – Aching at the back of the shoulders, over the pelvis, in the axilla or medial side of the elbow,
– Heaviness and Nredness of the arms or legs, – A glove distribuNon of symptoms, – TraumaNc girdle pain, – Scapular / abdominal / kidney pains / chest pain or indigesNon,
– Upper limb/shoulder mobility restricNon, – Shoulder impingement-‐type pain.
Maitland et al 2005; Hengeveld and Banks 2005
S/S of Thoracic Spine DysfuncNons
Canine Symptomology: Exaggerated kyphosis or lordosis of the thoracic region,
Discomfort to pezng over the thoracic region, Expression of pain with jumping or moving while in a recumbent posiNon, wrestling with other dogs,
Forelimb lameness or limb favouring, Head-‐down posturing, A reducNon in athleNcism, Excessive stretching (‘down-‐dog’).
LEH clinical observaNons
PalpaNon Concepts
Postural analysis Reveal nothing OR show a segmental rotaNon
MulNsegmental sNffness alters thoracic curve exaggerated kyphosis, reduced lordosis, or scoliosis
Acute zygapophysial joint sprain produces localized pain over the involved joint
Chronic restricNon of either the zygapophysial or costovertebral joint produces symptoms removed from the source ▪ (contralateral side of the thorax or at levels above or below).
Maitland et al 2005; Hengeveld and Banks 2005
PalpaNon Concepts
• Posture – Kyphosis, lordosis, scoliosis, body condiNon
• Temperature – Non-‐inflammatory Increase of temp.
• Thickening – Chronic lesions may be thicker in the interspinous space
• Abnormal muscle tone – Hypertonic (acute) or hypotonic (chronic) – Atrophy
Maitland et al 2005; Hengeveld and Banks 2005
Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
22
General MoNon TesNng Concepts
• Movement awareness – Assess the quality (i.e. sensaNon throughout moNon plus the endfeel)
– Assess the quanNty (i.e. ROM)
– Assess for symptoms (i.e. pain responses)
General MoNon TesNng Concepts
• AcNve MoNon TesNng – Cookie stretches
• Willingness and/or ability • Movement compensaNons
• Generally, facet joint movement restricNons may be too subtle for the examiner to noNce in this manner
General MoNon TesNng Concepts
• Joint Play – The general sense of the moNon within a joint.
– Used to narrow the examiners search for the lesion
– Tested in the joint’s neutral posiNon – Light pressure & gentle hands
Limited amount of joint play Moderate amount of joint play
General MoNon TesNng Concepts
• ARTHOKINEMATICS • ArEcular funcEon (aka “form closure”)
– HYPOMOBILITIES
– An increase in sNffness in the neutral zone and a harder end feel in the elasNc zone are noted on passive tests for arthokinemaNc funcNon.
– The sNffness has a solid stop.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
23
General MoNon TesNng Concepts
• Adjunc7ve tests – X-‐rays may be useful to reveal serious bone disease and significant mechanic defects, but rarely provide guidance for manual therapy.
Clinical DiagnosNc Tests & Treatment Techniques
Let’s get to the dogs!
Manual testing (Adapted for the canine by L. Edge-Hughes from D. Lee 2003)
T/S PalpaNon
Review: Speak now or forever hold your peace.... Can you:
• Direct palpaNon of the spinous processes T1 – T13 • PalpaNon of the ribs 1 – 13 • PalpaNon of the sternum (including the manubrium and xiphoid process)
• T10 & T11 are found in the ‘dip’ in the middle of the dogs back
– What techniques have you been pracNcing?
– Do we need to review anything?

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
24
T/S Review – localize the lesion
• Bilateral Transverse Process Posterior – Anterior (Dorso-‐Ventral) Pressures: – Use a thumb and index knuckle to do a P-‐A on the transverse processes / arNcular pillars simultaneously.
• This may give you informaNon as to where along the thoracic spine there is sNffness (hypomobility).
• Be sure to support under the belly or chest. • Assess for quality and quanNty of movement, end feel and pain.
– Angle slightly cranially above T9/10 and straight up and down for T10/11 and below.
– However, to isolate which facet is problemaNc, you will need to do a unilateral P-‐A/(D-‐V).
Assessment or treatment
T/S Review – localize the lesion
• Bilateral Transverse Process Posterior – Anterior (Dorso-‐Ventral) Pressures:
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier
T/S Review – localize the lesion
• Unilateral Transverse Process Posterior – Anterior (Dorso-‐Ventral) Pressures: – Pressing down directly on one transverse process / arNcular pillar will examine the rotaNonal or side bending mobility of the vertebra.
– Angle slightly cranially above T9/10 and straight up and down for T10/11 and below. • Be sure to support under the belly or chest. • Assess for quality and quanNty of movement, endfeel and pain.
Assessment or treatment
T/S Review – localize the lesion
• Unilateral Transverse Process Posterior – Anterior (Dorso-‐Ventral) Pressures:
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
25
T/S Review – localize the lesion
• Individual side bend / rotaNons: – Using the side of the spinous processes and a) Push the spine away from one side, while
pulling the hips or shoulders in the opposite direcNon, with the dog in standing or lying
b) Push the spinous process towards the floor with the dog in side lie (Note: This test is most appropriate for the thoracic spine – above the level of T9/T10 usually)
Assessment or treatment
T/S Review
• Individual side bend / rotaNons:
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier
• ARTHOKINEMATICS – Ventral transla0on glide (spinal):
• Fix one vertebra via the spinous process (pinch it and hold it caudally) and the push the superior vertebrae with a dorsoventral pressure
Assessment or treatment
Passive Physiologic Intervertebral Movements (PPIVMS) & Treatment Techniques
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier
• ARTHOKINEMATICS – Dorsal transla0on glide (spinal):
• Fix the vertebra below (pinch it and hold it caudally) and then push through the thorax/chest and feel the translaNon and end feel.
Assessment or treatment
Passive Physiologic Intervertebral Movements (PPIVMS) & Treatment Techniques
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
26
• ARTHOKINEMATICS – Transverse rota0on glide (spinal):
• Fix the spinous process (pinch it and hold it caudally) of one vertebra and push laterally on the spinous process of the vertebra above. Repeat in both direcNons:
Assessment or treatment
Passive Physiologic Intervertebral Movements (PPIVMS) & Treatment Techniques
Feel for stiffness in the neutral zone and the end feel at the anatomical barrier
• ARTHOKINEMATICS – Lateral Transla0on Glide:
• For segments T3/4 to T10/11 and associated ribs. Compress one rib (i.e. le\ rib 6) (from the lateral side or dorsolateral side) and shear the contralateral rib just above (right rib 5) PURELY & medially in the transverse plane.
• NORMALLY, there should be lidle/if any movement or pain.
• The primary structure being tested is the disc! Lateral translaNons (stress test
for the disc) Assessment typically… but I use it to treat too!
Passive Physiologic Intervertebral Movements (PPIVMS) – Assessment only...
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding Dorsoventral Pressures • To Stabilize above or below? (T1/2 – T9/10)
– When performing the D-‐V pressure you can be more specific as to whether you are ‘opening’ the facet(s) or ‘closing’ the facet(s). • If you stabilize the spinous process caudal to the ‘moving’ spinous process, and glide cranially, then you are opening (flexion of) the facet(s) – i.e. Hold T7 caudally while gliding T6 cranially
• If you stabilize the spinous process cranial to the ‘moving’ spinous process, and glide cranially, then you are closing (extension of) the facet(s) – i.e. Hold T6 caudally while gliding T7 cranially
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding Dorsoventral Pressures • To Stabilize above or below? (T9/10 – L6/7)
– When performing the D-‐V pressure you can be more specific as to whether you are ‘opening’ the facet(s) or ‘closing’ the facet(s). • If you stabilize the spinous process caudal to the ‘moving’ spinous process, and glide ventrally, then you are closing (extension of) the facet(s) – i.e. Hold T13 caudally while gliding T12 ventrally
• If you stabilize the spinous process cranial to the ‘moving’ spinous process, and glide ventrally, then you are opening (flexion of) the facet(s) – i.e. Hold T12 cranially while gliding T13 ventrally

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
27
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding Unilateral Facet Joint Restric0ons.
• To Block or Assist Side bend/Rota0on techniques? – When side bending the dog you can either:
• Push the spinous process of the segment to be treated AWAY from the side bend moNon (ASSISTING movement)
• BLOCK the spinous process from moving away from the side bend moNon (thus stopping further moNon down the spine and making the end of moNon occur at that specific segment)
This is what you have been taught already
This is a new concept
TRY BLOCKING – compare to assis0ng
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding Unilateral Facet Joint Restric0ons.
• To Block or Assist Side bend/Rota0on techniques?
Blocking AssisNng
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding Unilateral Facet Joint Restric0ons.
• For Flexion or Extension lesion? – If you think the restricNon is of the facet joint that would be opening, then do the side bend/rotaNon in FLEXION of the spine
– If you think the restricNon is of the facet joint closing, then do the side bend/rotaNon in EXTENSION of the spine
TRY in Flexion & Extension
T/S: Spinal Treatment Techniques
• CONCEPT – Regarding ANY Facet Joint Restric0on in the Dog. – The problem is usually poor opening of a facet joint. (You can default to flexion techniques if you are unsure of the lesion)
– If a dog has an increase in pain or exhibits a pain response (i.e. Yelping &/or root signature stance when tesNng the Cervico-‐thoracic region or Lumbar region), when you are doing an EXTENSION technique or a BLOCKING technique – you may be dealing with an osteophyte encroaching on the nerve root foramen.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
28
T/S: Spinal Treatment Techniques
• Any zygapophysial restric7on – PosiNon the animal standing or sizng. – At the site of the lesion (localized with assessment for tenderness), press on the side of the spinous process, one direcNon at a Nme. Note the degree of discomfort and mobility of each direcNon.
– Work with the direcNon that is most sNff (and o\en most uncomfortable)
• Firstly apply a pressure in the opposite direcNon to the spinous process of the vertebra cranial and then to the one caudal.
• One of which will exaggerate the discomfort and one of which will relieve it / be less reacNve.
• Chose to mobilize whichever of these two direcNonal forces that relieves the symptoms / is less reacNve. NEW...
Try it!
T/S: Spinal Treatment Techniques
T/S: Spinal Treatment Techniques
• Trac7on: – This technique restores a bilateral restricNon of flexion.
– Cervical tracNon with the head and neck posiNoned in flexion should address the upper thoracic spine
– Lumbar tracNon (i.e. a standing tracNon) will target the mid thoracic spine and all vertebral segments caudally.
T/S: TracNon
• TracNon:
Neck tracNon in sternal recumbency
With the dog in sternal recumbency, kneel beside the dog or straddle over it (facing the same direcNon as the dog).
Now with your thumbs push away on the back of the dog’s skull (on either side of the occiput).
Go very slowly and the dog should lower its head to rest its chin on the floor.
Maintain a slow and steady pressure.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
29
T/S: TracNon • TracNon:
Neck tracNon in side lying
With the dog laying on his/her side and the head flat on the floor.
Use one hand just under the dog’s muzzle to prevent the head from being pushed into flexion and the other hand on the back of the skull to create the tracNon.
T/S: TracNon • TracNon:
Neck tracNon over the examiner’s thigh
PosiNon the animal (and yourself) so that the dog’s neck can be supported over your thigh (standing or lying depending upon size of the dog).
With a wide pinscher grip, grasp behind the skull and slowly push it away.
The other hand braces the animal’s shoulders or withers.
T/S: TracNon
• Trac7on: – Tail pulls: Grasp the base of the tail and gently pull back on it, in an arch that matches the arch of the dog’s rump. Hold the animal’s pelvis so as to maintain it in posiNon.
T/S: TracNon
• Trac7on: – One-‐man standing trac0on: Straddle the dog, facing backwards. Have your legs posiNoned just behind the shoulder blades and allow your own heels to touch each other under the torso of the dog. Bend over and place your hands in front of the dog’s pelvis (hands wide spread – using the web space border again. Be careful not to dig into the groin of the animal). Straighten your legs (to squeeze the animal) and push the pelvis away from you.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
30
T/S: TracNon
• Trac7on: – Small dog hanging trac0on: Slowly and gently pick up the dog so that its spine is against your chest. Hold it in a ‘bear hug’ with two arms if necessary (i.e. heavier dog) or with one arm to hold and the other arm to support under the bud or under the legs depending on the comfort of the animal). Straighten up or stand up, so that the animal’s feet come off of the ground and the weight of the lower body is tracNoning the spine. You can allow wiggly dogs to touch the ground with their toes or if you want to add extension into your tracNon.
T/S: TracNon
• Trac7on: – Specific trac0on: Grab one spinous above the site to tracNon and one spinous process below (if the area is too tender, then raise and/or lower the vertebra used to tracNon through so as to be further away from the painful area) and pull apart (distract).
T/S: Rib Techniques -‐ Review
• Assessing the posiNon of the ribs: Palpate both dorsally and ventrally and compare the posiNon from side to side and also in comparison to the ribs adjacent cranially and caudally. Palpate for tenderness also. (Best done in standing)
• Assess ‘general’ mobility of the ribs. Push downward from the top at the costovertebral juncNon. Pull up from below at the sternocostal juncNon or costochondral juncNon
• Mobilize: Dorsal glide & Ventral glide
T/S: Rib Techniques -‐ Review
• Ribs Dorsal glide Ventral glide

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
31
T/S: Rib Techniques – New Concept
• Ventral transla0on glide (with improved specificity):
• Stabilize the two associated spinous processes (i.e. T4 + T5) away from the rib to be mobilized • With your other hand push ventrally on the rib to be treated (i.e. Rib 5).
T/S: Rib Techniques – New Concept
• Dorsal transla0on (with specificity for the sternocostal juncNon):
NOTE posiNon of the ribs (ventral surface) looking for a step deformity, or a gap in the joint line at the sternocostal juncNon.
• Stabilize the sternum and push on the ventral aspect of the costocarNlage/rib and push dorsally (upwards).
Stabilizing hand
Mobilizing hand
T/S: Rib Techniques – New Concept
• Cranial – caudal rib glides: – Fix the corresponding spinous process (pushing it to the contralateral side) and push cranially or caudally on the corresponding rib to assess the glide at the costotransverse joint.
T/S: Rib Techniques -‐ Review
• Ribs 1 -‐ 4 localiza0on – NOTE: – RIB ONE can be accessed adjacent to the sternum and working one’s way inwards towards the cervical spine.(Midpoint between the manubrium and the
greater tuberosity of the humerus)
– RIBS 1 -‐ 3 (and someNmes 4) are located under the scapula but can be accessed (at the rib angle) by maneuvering a finger or thumb under the caudal aspect of the scapula with the shoulder joint in a slight degree of flexion.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
32
T/S: Rib Techniques -‐ Review T/S: Rib Techniques -‐ Review
• Assessing Rib one: – With the dog in sizng: Simultaneously assess both first ribs with either fingers or thumbs lying overtop of these ribs, located by moving dorso-‐caudo-‐medially from either side of the manubrium (towards C7).
– Feel for posiNon and/or push ‘downward’ (caudal) individually on the top of these ribs to assess for discomfort and sNffness.
T/S: Rib Techniques -‐ Review
Caudal glide of rib 1
• Yipe!
MOBILIZE: Push down on the one that is ‘high’ (caudal glide)
T/S: Rib Techniques – New Concept
• Rib One • – Caudal glide with improved specificity
– Glide rib one caudally (first fixate the T1 spinous process by pushing it to the contralateral side). Feel for end feel and sNffness.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
33
T/S: Rib Techniques – New Concept
• Rib One (for a rib in a cranial posi0on) In humans – with elevated rib one issues, the Scalenes are o\en Nght or shortened and can ‘hold’ rib one in a cranial posiNon.
Stretch Scalenes by pressing caudally (downwards) on rib one while turning the dogs head to the contralateral side.
You may also want to massage in the same region to release the tension in the Scalenes.
T/S: Rib Techniques – New Concept
• Rib One • Cranial glide (for a caudally displaced ‘rib one’ that is tender on palpaNon)
• From under the axilla place your thumb against the caudal border of rib 1, and then glide the spinous process of T1 caudally. • Feel for end feel and sNffness.
T/S: Rib Techniques – New Concept
• Ribs – Generic Treatment Technique • A distrac0on mobiliza0on or manipula0on
– Localize the angle of the rib and posiNoning your thumb at this spot.
– Your other thumb is placed across the ipsilateral side of the spinous processes of the two corresponding vertebra to stabilize.
– The mobilizaNon / manipulaNon occurs by creaNng a lateroventral pressure with the thumb on the corresponding rib at the ‘rib angle’.
T/S: Rib Techniques – New Concept

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
34
T/S – Force Closure
• Neuromyofascial func7on (force closure) – In humans, this test would be a prone arm lii, watching for the paNent’s method of thorax stabilizaNon.
– A similar construct could be created in the dog, with a standing unilateral front leg li\ (watching for stabilizaNon and control of balance), or a diagonal leg stand.
– The thorax should not rotate, side bend, flex, extend or translate, and the scapula should not move on the weight bearing side.
T/S – Force Closure
T/S – Force Closure
• Neuromyofascial func7on (force closure) – The deep small stabilizer muscles of the thorax (such as mulNfidus and the intercostals) can atrophy subsequent to injury to the thorax. • Firmly palpate the ‘guker’ between the spinous process and the transverse process (mulNfidus) and feel for firmness and size of the muscles (comparing side to side and above and below),
• Then palpate between each palpable rib (intercostals) and compare with adjacent and contralateral sites.
T/S – Force Closure
PalpaNon of mulNfidus between the spinous process and transverse process
PalpaNon of the intercostals between the ribs
• Neuromyofascial func7on (force closure)

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
35
T/S: Neural ConducNon & Mobility
• Neural conduc7on and mobility – The adjacent muscles (the epaxials, hypaxials, and intercostals) can be palpated for appropriate muscle bulk and tone. Segmental facilitaNon leads to hypertonicity (iniNally) and reduced motor funcNon which causes atrophy (secondarily).
– Hyperaesthesia can be one of the first signs of a neurological interference and tend to occur long before sensaNon becomes reduced.
T/S: Neural ConducNon & Mobility
• Neural conduc7on and mobility – In the human, a dural slump test might reveal thoracic pain, which is relieved by head and neck extension.
– It has been determined that vertebral column flexion in the dog can create a very small gliding distance at the T13 – L1spinal levels. (Gruenenfleder et al 2006)
– Other thoracic segments have not been tested, but it is reasonable to hypothesize that the dura at other thoracic levels could be put into tension in a full flexion posiNon
T/S: Neural ConducNon & Mobility
Dural tension test: vertebral column flexion
T/S: Force Closure and Motor Control
• Force Closure and Motor Control: – The four muscles of interest for the stabilizaNon of the lumbopelvic region are the diaphragm, transverses abdominis, deep fibres of mulNfidus and the pelvic floor.
– Based on the anatomy of the thoracic region, it is hypothesized that the deep segmental muscles (i.e. mulNfidus) will have a similar funcNon in the thoracic region.(Lee LJ 2003)

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
36
T/S: Force Closure and Motor Control
• Force Closure and Motor Control: – Restoring tonic funcNon of these muscles is essenNal for regaining segmental stability.
– Stretching, elongaNng and/or relaxing larger more dominant global muscles that could be over-‐acNvely adempNng to stabilize the thorax may need to be addressed for normalizaNon of movement and funcNon.
– AddiNonally, the most common component lost in human paNents with thoracic dysfuncNon is lateral costal expansion.(Lee LJ 2003)
T/S: Force Closure and Motor Control
• Stabiliza7on training – 3-‐leg standing, li\ing one front leg off the ground, while cueing the segmental muscles (mulNfidus) by palpaNng & rubbing just adjacent to the spinous process in the ‘guder’ between the spinous process and the erector spinae muscles OR by cueing the abdominals. This exercise can be progressed by having the animal perform it on an uneven surface such as a wobble board or balance disc.
T/S: Force Closure and Motor Control
• Stabiliza7on training – 3-‐leg standing...
3-‐leg standing sNmulaNon of mulNfidus
3-‐leg standing sNmulaNon of abdominals
T/S: Force Closure and Motor Control
• Rota7ons in standing: – In a stable standing posiNon, impart a rotaNon (twist) to the thorax with your hands spread out wide over the torso (one moves ventrally and the other moves dorsally).
– The animal must stand and acNvely resist this force. This can be done as an isometric hold technique in order to acNvate mulNfidus and/or the intercostals.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
37
T/S: Force Closure and Motor Control
Torso rotaNons in standing
T/S: Force Closure and Motor Control
• Stretches: – Stretching out of the dominant global muscles in the thoracic spine can help to normalize an over acNve stabilizing mechanism.
– Key muscles to evaluate for over-‐acNve resNng tone or adapNve shortening are the erector spinae, rhomboids, the laNssimus dorsi, the rectus and both oblique abdominal muscles.
T/S: Force Closure and Motor Control
Stretch of the thoracic fibres of rhomboids
Stretch of the cervical fibres of rhomboids
Stretching Examples
T/S: Force Closure and Motor Control
• Lateral costal expansion: – UNlizing a cardiopulmonary therapy technique, posiNon the paNent in sizng or standing, and as the paNent exhales, gently compress the lateral ribs a bit further.
– The technique occurs either in one compression movement or a succession of two or three compressions that build in compression force.
– Then quickly release your hands, sNmulaNng a greater inhale and lateral costal expansion.
– The pracNNoner should try to Nme the technique with the normal breathing padern.

Manual Therapy and the Canine Thoracic Spine
Copyright Laurie Edge-‐Hughes, 2013
38
T/S: Force Closure and Motor Control
Lateral costal expansion
The Thoracic Spine
• Key Points to Return to Ac7vity and Strengthening – Focus first on low loads and control of movement – Avoid fast ballisNc movements in early stages – Progress from stable to unstable surfaces
– For upper and middle thoracic control, incorporate greater arm movements
– Work on high load and high speed acNviNes at the end stages.
Want to conNnue to learn more? Check out:
www.FourLeg.com

REFERENCES
MANUAL THERAPY References 1. Allison G, Edmonston S, Kivinieme K et al. (2001) ‘Influence of the standardized mobilization on the
posteroanterior stiffness of the lumbar spine in asymptomatic subjects. Physiother Res Int 6 (3): pp 145 – 156. 2. Balthazard P et al. Manual therapy followed by specific active exercises vs a placebo followed by specific
active exercises on the improvement of functional disability in patients with chronic non specific low back pain: a randomized controlled trial. BMC Musculoskel Disord 13(1): 162. Epub ahead of print, 2012.
3. Björnsdóttir SV, Kumar S. (1997) ‘Posteroanterior spinal mobilization: state of the art review and discussion.’ Dis Rehab. 19 (2): pp 39 – 46.
4. Cibulka MT, Delitto A. (1993) ‘A comparison of two different methods to treat hip pain in runners.’ JOSPT. 17 (4): pp 172 – 176.
5. Cibulka MT, Delitto A, Koldehoff RM. (1998) ‘Changes in innominate tilt after manipulation of the sacroiliac joint in patients with low back pain.’ Physical Therapy. 68 (9): pp 1359 – 1363.
6. Collins N, Teys P, Vincezino B. (2004) ‘The initial effects of a Mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains. Man Ther. 9 (2): pp 77 – 82.
7. Conroy DE, Hayes KW. (1998) ‘The effect of joint mobilization as a component of comprehensive treatment for primary shoulder impingement syndrome.’ JOSPT. 28 (1): pp 3 – 14.
8. Constantoyannis C, Konstantinou D, Kourtopoulos H et al: Intermittent cervical traction for cervical radiculopathy caused by large-‐volume herniated disks. J Manipulative Physiol Ther. 25: pp 188 – 192, 2002.
9. Deen Jr, HG, Rizzo TD, & Fenton DS: sudden progression of lumbar disk protrusion during vertebral axial decompression traction therapy. Mayo Clin Proc. 78: pp 1554 – 1556, 2003.
10. Dhondt W et al. Pain threshold in patients with rheumatoid arthritis and effect of manual oscillations. Scan J Rheumatol. 28: 88 – 93, 1999.
11. Erhard RE, Welch WC, Liu B et al: Far-‐lateral disk herniations: Case report, review of the literature, and a description of nonsurgical management. J Manipulative Physiol Ther. 27: pp 27: e3, 2004.
12. Fritz JM et al. Preliminary investigation of the mechanisms underlying the effects of manipulation: exploration of a multi-‐variate model including spinal stiffness, multifidus recruitment, and clinical findings. Spine 2012. Epub ahead of print.
13. Goodsell M, Lee M, Latimer J. (2000) ‘Short-‐term effects of lumbar posteroanterior mobilization in individual with low-‐back pain.’ J Manipul Physiol Ther. 23 (5): pp 332 – 342.
14. Grayson JE et al. Spinal manual therapy produces rapid onset analgesia in a rodent model. Man Ther 17(4) 292-‐297, 2012.
15. Grieve E. (2001) ‘Diagnostic tests for mechanical dysfunction of the sacroiliac joints.’ J Manual Manip Ther. 9 (4): pp 198 – 206.
16. Herzog W, Scheele D, Conway PJ. (1999) ‘Electomyographic responses of back and limb muscles associated with spinal manipulative therapy.’ Spine. 24 (2): pp 146 – 152.
17. Hoeksma H, Dekker J, Ronday H et al. (2004) ‘Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: A randomized clinical trial.’ Arthritis Care and Research. 51: pp 722 – 729.
18. Jam B: Is there evidence to support other common interventions? In When a Back Goes Out…Where Does it Really Go? Answers for Clinicians Committed to Evidence-‐based Management of acute Low Back Pain for the
Prevention of Chronic Disability. Advanced Physical Therapy Education Institute, Thornhill, ON, Canada, 2005. 19. Kanlayanaphotoporn R et al. Immediate effects of the central PA mobilixation technique on pain and range of
motin in patients with mechanical neck pain. Disabil Rehabil 32 (8): 622 – 628, 2010. 20. Katavich L. (1998) ‘Differential effects of spinal manipulative therapy on acute and chronic muscle spasm: a
proposal for mechanism and efficacy.’ Manual Therapy. 3 (3): pp 132 – 139. 21. Krause M, Refshauge KM, Dessen et al: Lumbar spine traction: evaluation of effects and recommended
application for treatment. Man Ther. 5 (2): pp 72 – 81, 2000.
22. Lee D, Lee LJ. (2004) ‘Treating the lumbopelvic-‐hip dysfunction.’ In An approach to the examination and treatment of the lumbopelvic-‐hip region. Lee D editor. pp 163 – 248. (Churchill Livingstone: Toronto, ON, Canada).
23. Lee M, Latimer J & Maher C. (1993) ‘Manipulation: investigation of a proposed mechanism.’ Clin Biomech. 8: pp 302 – 306.
24. Maffey LL. Arthrokinematics and mobilization of musculoskeletal tissue: The principles. In Scientific
Foundation sand Principles of Practice in Musculoskeletal Rehabilitation. Magee, Zachazewski, Quillen eds. Saunders Elsevier, St Louis, pp 487 – 526, 2007
25. Maitland GD. (1966) ‘Manipulation – Mobilisation.’ Physiotherapy. 52 (11): pp 382 – 385. 26. Maitland G, Hengeveld E, Banks K, English K. (2005) Maitland’s Vertebral Manipulation. (Elsevier Butterworth
Heinmann: Toronto). 27. Malanga GA & Nadler SF: Nonoperative treatment of low back pain. Mayo Clin Proc. 74: pp 1135 – 1148,
1999. 28. Marshall P, Murphy B. (2006) ‘The effect of sacroiliac joint manipulation on feed-‐forward activation times of
the deep abdominal musculature.’ J Manipulative Physiol Ther. 29: pp 196 – 202. 29. Murphy BA, Dawson NJ, Slack JR. (1995) ‘Sacroiliac joint manipulation decreases the H-‐reflex.’ Electromyogr.
Clin. Neurophysiol. 35: pp 87 – 94. 30. Nilsson N, Wulff Christensen H, Hartvigsen J. (1996) ‘Lasting changes in passive range of motion after spinal
manipulation: A randomized, blind, controlled trial. Spine. 19 (3): pp 165 – 168. 31. Olson VL. (1987) ‘Evaluation of joint mobilization treatment. A method.’ Phys Ther. 63 (9): pp 1439 – 1444. 32. Paris SV, Viti J. Differential diagnosis of low back pain. In Movement, Stability & Lumbopelvic Pain, 2nd Ed,
Integration of Research and Therapy, Vleeming, Mooney, Stoeckart eds. Churchill Livingstone Elsevier, Toronto, 381 – 389, 2007.
33. Sal JA & Saal JS: Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Spine. 14 (4): pp 431 – 437, 1989.
34. Sasso RC, Ahmad RI, Butler JE, Reimers DL. (2001) ‘Sacroiliac joint dysfunction: A long-‐term follow-‐up study.’ Orthopedics. 24 (5): pp 457 – 460.
35. Sterling M, Jull G, Wright A. (2001) ‘Cervical mobilization: concurrent effects on pain, sympathetic nervous system activity and motor activity. Man Ther. 6 (2): pp 72 – 81.
36. Symons BP, Herzog W, Leonard T, Hguyen H. (2000) ‘Reflex responses associated with activator treatment.’ J Manipul Physiol Ther. 23 (3): pp 155 – 159.
37. Tullberg T, Blomberg S, Branth B, Johnsson R. (1998) ‘Manipulation does not alter the position of he sacroiliac joint: A roentgen stereophotgrammetric analysis.’ Spine. 23 (10): pp 1124 – 1128.
38. Zelle BA, Gruen GS, Brown S, George S. (2005) ‘Sacroiliac joint dysfunction evaluation and management. Clin J Pain. 21 (5): pp 446 – 455.
39. Zusman M. (1986) ‘Spinal manipulative therapy: review of some proposed mechanisms, and a new hypothesis.’ Aust J Phyty. 32 (2): pp 89 – 99.
THORACIC SPINE References 1. Breit S. Osteological and morphometric observations on intervertebral joints in the canine pre-‐diaphragmatic
thoracic spines (Th1 – Th9). Vet J 164: 216 – 223, 2002. 2. Breit S. Functional adaptations of facet geometry in the canine thoracolumbar and lumbar spine (Th10 – L6).
Ann Anat 184: 379 – 385, 2002. 3. Breit S. Osteological features in pure-‐bred dogs predisposing to thoracic or lumbar spinal cord compression.
Res Vet Sci 73: 87 – 92, 2002. 4. Evans HE: Millers’ Anatomy of the Dog, 3rd ed. WB Saunders Co: Philadelphia PA, 1993.
5. Gruenenfelder FI, Boos A, Mouwen M, et al. Evaluation of the anatomical effect of physical therapy exercises for mobilization of lumbar spinal nerves and the dura mater in dogs. AM J Vet Res 67(10): pp 1773 – 1779,
2006. 6. Hengeveld E & Banks K. Maitland’s Peripheral Manipulation. 4th Edition. Elsevier Butterworth Heinemann,
Toronto, 2005. 7. Hodges PW. Motor control of the trunk. In Grieve’s Modern Manual Therapy The Vertebral Column, 3rd Ed.
Boyling JD & Jull GA eds. Elsevier Churchill Livingstone, Toronto, 2004, pp 119 -‐ 139. 8. Jiang H, Moreau M, Raso VJ et al. A comparison of spinal ligaments – differences between biped and
quadrupeds. J Anat 187: 85 – 89, 1995. 9. Lee D, Walsh M. A Workbook of Manual Therapy Techniques for the Vertebral Column and Pelvic Girdle.
Nacent Publishing, Delta, BC, Canada, 1985. 10. Lee D. The Thorax, An Integrated Approach. Diane G Lee Physiotherapist Corporation, White Rock, BC,
Canada, 2003. 11. Lee LJ. Restoring force closure / motor control or the thorax. In The Thorax, An Integrated Approach. Lee D
ed., Diane G Lee Physiotherapist Corporation, White Rock, BC, Canada, 2003. 12. Little JP & Adam CJ. Effects of surgical joint destabilization on load sharing between ligamentous structures in
the thoracic spine: A finite element investigation. Clin Biomech 26: 895 – 903, 2011. 13. Maitland G, Hengeveld E, Banks K & English K. Maitland’s Vertebral Manipulation. 7th Edition. Elsevier
Butterworth, Heinemann, Toronto, 2005. 14. Oda I, Abumi K, Lu D et al. Biomechanical role of the posterior elements, costovertebral joints, and rib cage in
the stability of the thoracic spine. Spine 21 (12): 1423 – 1429, 1996. 15. Singer KP, Boyle JJW, Fazey P. Comparative anatomy of the zygapophysial joints. In Grieve’s Modern Manual
Therapy The Vertebral Column, 3rd Ed. Boyling JD & Jull GA eds. Elsevier Churchill Livingstone, Toronto, 2004, pp 17 – 53.
16. Takeuchi T, Abumi K, Shono Y et al. Biomechanical role of the intervertebral disc and costovertebral joint in stability of the thoracic spine. Spine 24 (14): 1414 – 1420, 1999.
17. Young BA, Gill HE, Wainner RS, et al. Thoracic costotransverse joint pain patterns: a study I normal volunteers. BMC Musculoskel Disorders 9: 140, 2008.