Manometry of the Normal Upper Esophageal · 1036 INTRODUCTION Upper esophageal sphincter pressure...
6
Manometry of the Normal Upper Esophageal Sphincter and its Alterations in Laryngectomy RICHARD W. WELCH, KENNETH LUCKMANN, PHILLIP NM. RICKS, SAMUEL T. DRAKE, and GEORGE A. GATEs, Division of Gastroenterology and Division oj Otorhinolarytngology, The Uniiversity of Texas Healthi Science Ceniter at San Anton1io, San Antotnio, Texas 78284 A B S T R A C T Rapid pull-through pressure profiles of the normal human upper esophageal sphincter (UES) were simultaneously studied with a conventional three-orifice Honeywell solid-state probe, an eight lumen radially perfused (RP) probe, and a circum- ferentially sensitive (CS) probe designed to measure UES pressure (UESP) without regard to probe orienta- tion. Pressure curves were digitized and analyzed by computer. The Honeywell probe recorded significantly lower peak pressures than the other two methods, and had wide intrasubject pressure variations (average co- efficient of variation, 53%). In contrast, UESP meas- ured with the CS probe was constant for each subject (mean peak UESP, 121 mm Hg; average coefficient of variation, 15%). Anteroposterior RP probe UESP were identical to CS probe pressures. Thus, peak perfused anteroposterior UESP correlates with circumferentially measured sphincter squeeze. Computer programs were written that allowed RP probe pressures to be mapped in three dimensions. Normal three-dimensional maps were characterized by anteroposterior accentuation of peak pressures and also by consistent axial asymmetry with anterior peak pres- sures occurring 0.8±0.2 cm closer to the pharynx. After defining the normal two- and three-dimensional UESP configuration, patients who had undergone lar- yngectomy were studied. Peak pressures measured with the RP probe decreased to -50 mm Hg and radial pressure asymmetry vanished. Like normals, CS probe pressures corresponded to peak RP probe pressures. UES length did not change significantly. Three-dimen- sional mapping showed that axial asymmetry also vanished. It therefore appears that the anatomic alter- ations produced by laryngectomy abolishes UESP asymmetry. Receivedfor publication 11 September 1.978 and in revised form 15Janutary 1979. 1036 INTRODUCTION Upper esophageal sphincter pressure (UESP)l is ra- dially asymmetric (1). This asymmetry makes it difficult to define the normal range of pressures and confounds attempts to detect differences in disease states. It is not known whether this radial array of pressures actually reflects circumferentially variable sphincteral squeeze or whether some of the high pressures recorded with perfused systems are just measurement artifacts. To more precisely define UESP asymmetry and to relate it to conventional methods of measuring UESP, we as- sessed UESP profiles with two conventional mano- metric probes and compared these results to a device designed to be circumferentially sensitive to sphinc- teral squeeze. Data collection and analyses were done by computer, allowing three-dimensional display of pressures and precise definition of the asymmetric features of the normal UESP. We then studied patients with laryngectomy to assess the effect of cricoid carti- lage removal on the UESP configuration. METHODS Presstsre measurintg devices. First, we used a 5.5-mm Diam Honevyell (HW) probe, Honeyvwell, Inc., Test Instruments Div., Denver, Colo. This probe is the highest fidelity con- ventional three-orifice probe available. It samples point pres- sure with three miniature strain gauges mounted in the wall of the probe. These miniature transducers are separated 1200 radially and are mounted 5 cm apart axially. This arrangement has been traditional for sampling esophageal pressures. Second, we used a 6-mm Diam, eight lumen radially per- fused (RP) polyvinyl probe whose side holes were all at the same level, thus samplinig circumferential pressures at 45° intervals. Fig. 1 is a cross-section of our RP probe at the level IAbbreviatiotns used in this pa per: CS, circumferentially sensitive; CV, coefficient of variation, CV, mean CV; RP, radially perfused; UES, upper esophageal sphincter; UESP, UES presstire. J. Clin. Intvest. (© The Americani Society for Clinical In-vestigationi, Inc., 0021 -9738179105/1036/06 $1.00 Volume 63 Mamy 1979 1036-1041
Transcript of Manometry of the Normal Upper Esophageal · 1036 INTRODUCTION Upper esophageal sphincter pressure...
Manometry of the Normal Upper Esophageal Sphincterand its Alterations in Laryngectomy
RICHARDW. WELCH,KENNETHLUCKMANN,PHILLIP NM. RICKS, SAMUELT. DRAKE, andGEORGEA. GATEs, Division of Gastroenterology and Division ojOtorhinolarytngology, The Uniiversity of Texas Healthi Science Ceniterat San Anton1io, San Antotnio, Texas 78284
A B S T RA C T Rapid pull-through pressure profiles ofthe normal human upper esophageal sphincter (UES)were simultaneously studied with a conventionalthree-orifice Honeywell solid-state probe, an eightlumen radially perfused (RP) probe, and a circum-ferentially sensitive (CS) probe designed to measureUESpressure (UESP) without regard to probe orienta-tion. Pressure curves were digitized and analyzed bycomputer. The Honeywell probe recorded significantlylower peak pressures than the other two methods, andhad wide intrasubject pressure variations (average co-efficient of variation, 53%). In contrast, UESP meas-ured with the CS probe was constant for each subject(mean peak UESP, 121 mmHg; average coefficient ofvariation, 15%). Anteroposterior RP probe UESPwereidentical to CS probe pressures. Thus, peak perfusedanteroposterior UESPcorrelates with circumferentiallymeasured sphincter squeeze.
Computer programs were written that allowed RPprobe pressures to be mapped in three dimensions.Normal three-dimensional maps were characterized byanteroposterior accentuation of peak pressures and alsoby consistent axial asymmetry with anterior peak pres-sures occurring 0.8±0.2 cm closer to the pharynx.
After defining the normal two- and three-dimensionalUESPconfiguration, patients who had undergone lar-yngectomy were studied. Peak pressures measuredwith the RP probe decreased to -50 mmHg and radialpressure asymmetry vanished. Like normals, CS probepressures corresponded to peak RP probe pressures.UES length did not change significantly. Three-dimen-sional mapping showed that axial asymmetry alsovanished. It therefore appears that the anatomic alter-ations produced by laryngectomy abolishes UESPasymmetry.
Receivedfor publication 11 September 1.978 and in revisedform 15Janutary 1979.
1036
INTRODUCTION
Upper esophageal sphincter pressure (UESP)l is ra-dially asymmetric (1). This asymmetry makes it difficultto define the normal range of pressures and confoundsattempts to detect differences in disease states. It is notknown whether this radial array of pressures actuallyreflects circumferentially variable sphincteral squeezeor whether some of the high pressures recorded withperfused systems are just measurement artifacts. Tomore precisely define UESPasymmetry and to relate itto conventional methods of measuring UESP, we as-sessed UESP profiles with two conventional mano-metric probes and compared these results to a devicedesigned to be circumferentially sensitive to sphinc-teral squeeze. Data collection and analyses were doneby computer, allowing three-dimensional display ofpressures and precise definition of the asymmetricfeatures of the normal UESP. Wethen studied patientswith laryngectomy to assess the effect of cricoid carti-lage removal on the UESPconfiguration.
METHODS
Presstsre measurintg devices. First, we used a 5.5-mm DiamHonevyell (HW) probe, Honeyvwell, Inc., Test InstrumentsDiv., Denver, Colo. This probe is the highest fidelity con-ventional three-orifice probe available. It samples point pres-sure with three miniature strain gauges mounted in the wallof the probe. These miniature transducers are separated 1200radially and are mounted 5 cm apart axially. This arrangementhas been traditional for sampling esophageal pressures.
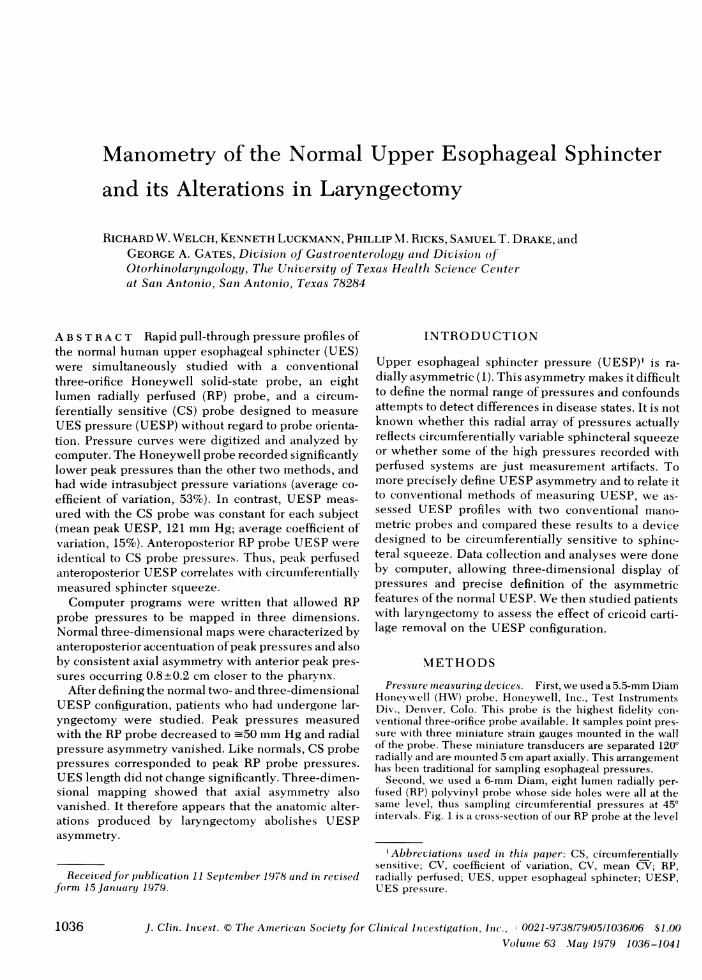
Second, we used a 6-mm Diam, eight lumen radially per-fused (RP) polyvinyl probe whose side holes were all at thesame level, thus samplinig circumferential pressures at 45°intervals. Fig. 1 is a cross-section of our RP probe at the level
IAbbreviatiotns used in this pa per: CS, circumferentiallysensitive; CV, coefficient of variation, CV, mean CV; RP,radially perfused; UES, upper esophageal sphincter; UESP,UES presstire.
J. Clin. Intvest. (© The Americani Society for Clinical In-vestigationi, Inc., 0021 -9738179105/1036/06 $1.00Volume 63 Mamy 1979 1036-1041
ANTERIORT l00
LEFT50 ~ 50
.50
6mm
* PRES100
POSTERIOR
SSURES IN mmHg
FIGURE 1 Cross-section of the RP probe at the level of theeight side holes. Superimposed is the circular coordinatesystem we used to map RP pressures.
of the eight orifices and is superimposed on the polar coordi-nate graphing system we used to map UESP. Orientation ofthis probe in the UES was confirmed by coloring one of theeight catheters and observing its position as it exited the mouthduring pull-through. Fluoroscopic monitoring of a series ofpull-throughs done in one volunteer with metallic markingson the catheter confirmed that the probe was sufficiently rigidso that twisting did not occur between the UESand the mouth.The eight lumen catheter was perfused with an Armdorferhydraulic-pneumatic perfusion device at 1 ml/min perchannel. Before the experiment, cross-clamping each channelproduced a rate of rise >300 mmHg/s.
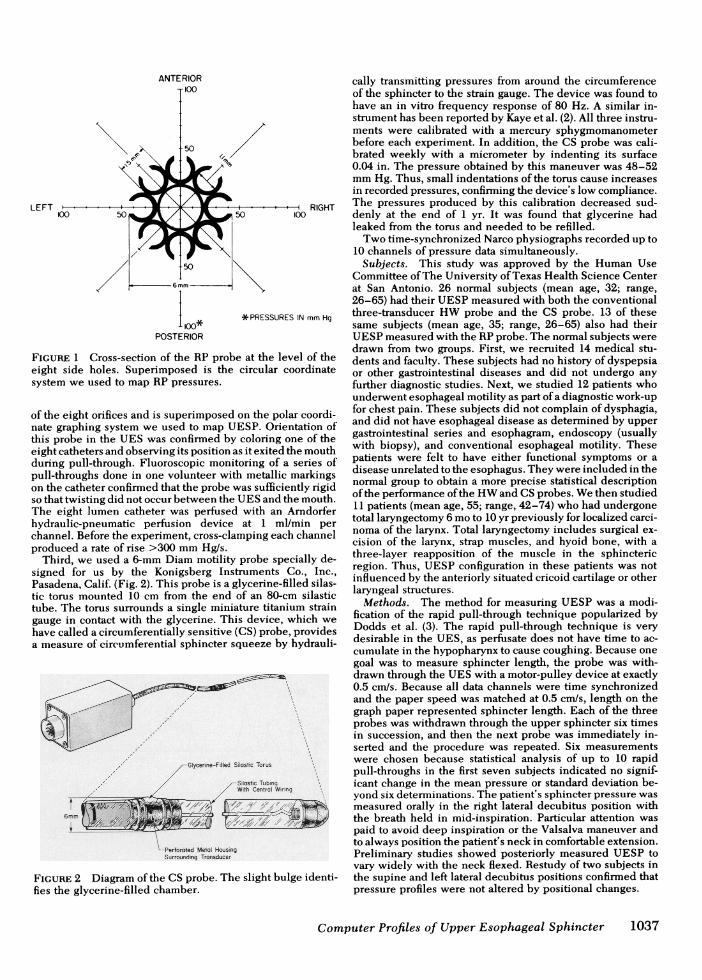
Third, we used a 6-mm Diam motility probe specially de-signed for us by the Konigsberg Instruments Co., Inc.,Pasadena, Calif. (Fig. 2). This probe is a glycerine-filled silas-tic torus mounted 10 cm from the end of an 80-cm silastictube. The torus surrounds a single miniature titanium straingauge in contact with the glycerine. This device, which wehave called a circumferentially sensitive (CS) probe, providesa measure of circumferential sphincter squeeze by hydrauli-
Glycefine-Filled Silostic Torus
,/Slastic TubingWith Centrol Woring
6mm ={ == ,
-Perforated Metal HousingSurrounding Tronsducer
FIGURE 2 Diagram of the CS probe. The slight bulge identi-fies the glycerine-filled chamber.
cally transmitting pressures from around the circumferenceof the sphincter to the strain gauge. The device was found tohave an in vitro frequency response of 80 Hz. A similar in-strument has been reported by Kaye et al. (2). All three instru-ments were calibrated with a mercury sphygmomanometerbefore each experiment. In addition, the CS probe was cali-brated weekly with a micrometer by indenting its surface0.04 in. The pressure obtained by this maneuver was 48-52mmHg. Thus, small indentations of the torus cause increasesin recorded pressures, confirming the device's low compliance.The pressures produced by this calibration decreased sud-denly at the end of 1 yr. It was found that glycerine hadleaked from the torus and needed to be refilled.
Two time-synchronized Narco physiographs recorded up to10 channels of pressure data simultaneously.
Subjects. This study was approved by the Human UseCommittee of The University of Texas Health Science Centerat San Antonio. 26 normal subjects (mean age, 32; range,26-65) had their UESPmeasured with both the conventionalthree-transducer HWprobe and the CS probe. 13 of thesesame subjects (mean age, 35; range, 26-65) also had theirUESPmeasured with the RPprobe. The normal subjects weredrawn from two groups. First, we recruited 14 medical stu-dents and faculty. These subjects had no history of dyspepsiaor other gastrointestinal diseases and did not undergo anyfurther diagnostic studies. Next, we studied 12 patients whounderwent esophageal motility as part of a diagnostic work-upfor chest pain. These subjects did not complain of dysphagia,and did not have esophageal disease as determined by uppergastrointestinal series and esophagram, endoscopy (usuallywith biopsy), and conventional esophageal motility. Thesepatients were felt to have either functional symptoms or adisease unrelated to the esophagus. They were included in thenormal group to obtain a more precise statistical descriptionof the performance of the HWand CSprobes. Wethen studied11 patients (mean age, 55; range, 42-74) who had undergonetotal laryngectomy 6 moto 10 yr previously for localized carci-noma of the larynx. Total laryngectomy includes surgical ex-cision of the larynx, strap muscles, and hyoid bone, with athree-layer reapposition of the muscle in the sphinctericregion. Thus, UESPconfiguration in these patients was notinfluenced by the anteriorly situated cricoid cartilage or otherlaryngeal structures.
Methods. The method for measuring UESPwas a modi-fication of the rapid pull-through technique popularized byDodds et al. (3). The rapid pull-through technique is verydesirable in the UES, as perfusate does not have time to ac-cumulate in the hypopharynx to cause coughing. Because onegoal was to measure sphincter length, the probe was with-drawn through the UESwith a motor-pulley device at exactly0.5 cm/s. Because all data channels were time synchronizedand the paper speed was matched at 0.5 cm/s, length on thegraph paper represented sphincter length. Each of the threeprobes was withdrawn through the upper sphincter six timesin succession, and then the next probe was immediately in-serted and the procedure was repeated. Six measurementswere chosen because statistical analysis of up to 10 rapidpull-throughs in the first seven subjects indicated no signif-icant change in the mean pressure or standard deviation be-yond six determinations. The patient's sphincter pressure wasmeasured orally in the right lateral decubitus position withthe breath held in mid-inspiration. Particular attention waspaid to avoid deep inspiration or the Valsalva maneuver andto always position the patient's neck in comfortable extension.Preliminary studies showed posteriorly measured UESP tovary widely with the neck flexed. Restudy of two subjects inthe supine and left lateral decubitus positions confirmed thatpressure profiles were not altered by positional changes.
Computer Profiles of Upper Esophageal Sphincter 1037
Data analysis. Sphincter pressures were recorded as milli-meters of mercury above esophageal base-line pressure. Be-cause esophageal pressure is less than atmospheric, a precisedefinition of the oral end of the upper esophageal high pres-sure zone has to take this pressure difference into accouint.At 50% vital capacity (mid-inspiration), Milic-Emili et al. (4)have shown this pressure difference to average 10 mmHg. Wetherefore defined 10 mmHg above esophageal base-line asthe oral end of the UES. UESPgenerated with the CS and RPprobes were analyzed by computer to obtain precise, un-biased measurements of peak UESP, length, and area underCSpressure profile. UESPmeasurements with the HWprobewere so variable that further computer analysis of the datawas not done. Our computer technique involved tracing thewithdrawal profile of the UES with a Tektronix 4010-1 digi-tizer (Tektronix, Inc., Beaverton, Oreg.). This device, whichis coupled to a PDP11/50 computer (Digital Equipment Corp.,Marlboro, Mass.), is an electromagnetic stylus that ismoved over a grid containing 106 contact points. Thepressure curve is therebv transformed into a series ofclosely spaced but discrete points that are analyzed by com-puter to provide an unbiased measure of peak pressure, length,and area under the sphincteric pressure curve. The techniquefor three-dimensional mapping also involves digitizing thesphincter profiles. The eight curves obtained with the RPmethod are digitized and pressure is sampled at 0. 1-cm inter-vals. The computer is then programmed to arrange thesepoints in three-dimensional space and connect the time-syn-chronous pressures with a smooth curve. This curve-fittinginvolved mathematical modeling with spline function analysis(5). The "hidden line" software program allowing three-di-mensional graphic display was developed by the ComputerCenter at The University of Texas Health Science Center atSan Antonio. This method allows simultaneous visual displayof the radial and axial shape of the UES. Subsequent to thisstudy, we have begun entering data directly into the computerfrom the pressure transducers by means of analog to digitalconverters, thus bypassing the recorder and the need fordigitization.
Statistical analysis was incorporated into the final computerprogram. The standard error of the mean was used to de-scribe the distribution of all values around the mean. Becauseall UESmeasurements were done the same number of timeswith each device, a paired Student's t test was used todescribe statistical differences between the HW, CS, and RPprobes. An unpaired Student's t test was used to compareUESP, length, and area in the laryngectomy patients with thenormals. The coefficient of variation was used to describethe measurement precision of each device. A mean coefficientof variation was used to describe average overall variationswith the HWand CS probes and each port of the RP probe.The statistical significance of differences between the instru-ments' variabilities were assessed by a two-way analysis ofvariance.
RESULTS
Normal subjects. Peak upper sphincter pressurewas first measured with the HWand CS probes in the26 normal subjects. The six successive pull-throughswith the HWprobe showed large variations in peakpressure. The coefficient of variation (CV) for each sub-ject ranged from 22 to 89% with a mean coefficientof variation (CV) for all 26 subjects of 53%. Lengthmeasurements with HWwere also unreliable (averagelength, 2.6 cm; CV, 64%). This marked HWprobe vari-
ability precluded meaningful computer assessment.UESPmeasured by the CS probe was far more precisewith only a 15% CV measured for all subjects. Thevariability with the CSprobe was significantly less thanwith the HWprobe (P < 0.01). Mean peak UESP forall subjects was also significantly higher with the CSdevice (121 mmHg) than with the HWprobe (76 mmHG, P < 0.05).
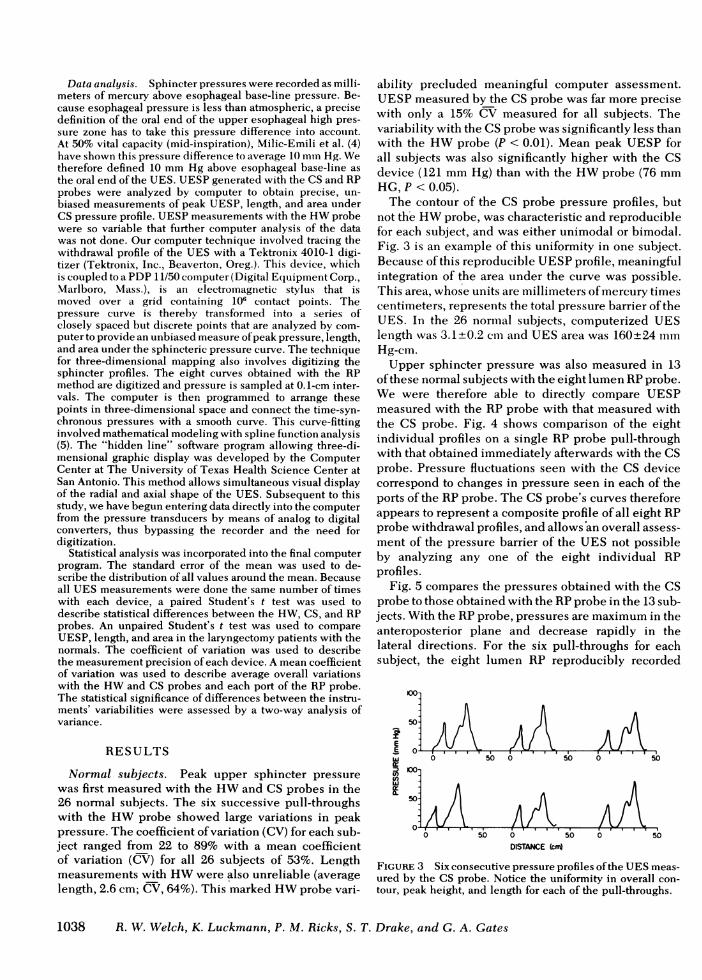
The contour of the CS probe pressure profiles, butnot th'e HWprobe, was characteristic and reproduciblefor each subject, and was either unimodal or bimodal.Fig. 3 is an example of this uniformity in one subject.Because of this reproducible UESPprofile, meaningfulintegration of the area under the curve was possible.This area, whose units are millimeters of mercury timescentimeters, represents the total pressure barrier of theUES. In the 26 normal subjects, computerized UESlength was 3.1+0.2 cm and UESarea was 160+24 mmHg-cm.
Upper sphincter pressure was also measured in 13of these normal subjects with the eight lumen RPprobe.We were therefore able to directly compare UESPmeasured with the RP probe with that measured withthe CS probe. Fig. 4 shows comparison of the eightindividual profiles on a single RP probe pull-throughwith that obtained immediately afterwards with the CSprobe. Pressure fluctuations seen with the CS devicecorrespond to changes in pressure seen in each of theports of the RPprobe. The CS probe's curves thereforeappears to represent a composite profile of all eight RPprobe withdrawal profiles, and allows'an overall assess-ment of the pressure barrier of the UES not possibleby analyzing any one of the eight individual RPprofiles.
Fig. 5 compares the pressures obtained with the CSprobe to those obtained with the RPprobe in the 13 sub-jects. With the RPprobe, pressures are maximum in theanteroposterior plane and decrease rapidly in thelateral directions. For the six pull-throughs for eachsubject, the eight lumen RP reproducibly recorded
50
E
E,w
IF .- Ir r- 1 r Ir0 50 0 5.0 0 5
)0-
<AAt0 1 1 I I~~~~~~~~~
A/
0 5.0 0 .0.O 50DISTANCE (crr
FIGURE 3 Six consecutive pressure profiles of the UESmeas-ured by the CS probe. Notice the uniformity in overall con-tour, peak height, and length for each of the pull-throughs.
1038 R. W. Welch, K. Luckmann, P. M. Ricks, S. T. Drake, and G. A. Gates
6

ANTERIOR-200
LEFT
-' 1f1JJ IJ LEFT POSTERIOR
80
401.LW1McLIj |POSTERIOR
__80 1HHHr 40 jj RIGHT POSTERIORE 111111
40 IL i RIGHT
z 80IILLIJINJJ RIGHT ANTERIOR
801HHH40LLLLWI LJ ANTERIOR
801HHH40j LEFT ANTERIOR
80-HIH400 CIRCUMFERENTIALLYKilSENSITIVE
0- -PROB3E0 25 50DISTANCE(mm)
FIGURE 4 Withdrawal profiles of the eight RPpressures com-pared to pressures measured by the CSprobe. Pressure changesoccurring in one or more RP probe channels are reflected inthe CS probe pressure profile.
peak pressures, with the CV for each port varying from17 to 23%. In Fig. 5, the peak CS probe UESPis repre-sented as a circle and corresponds exactly to the meanpeak RP probe UESPin the anteroposterior plane.
The RP probe data for each subject were then ex-panded into three dimensions with the aid of the com-puter. The eight individual RP profiles were digitizedfor all six pull-throughs in each of the 13 subjects. Eachpull-through produced a three-dimensional pressuremap of both the axial and radial asymmetry. Fig. 6 is athree-dimensional map of eight individual RP probeprofiles obtained in one pull-through and is the samepull-through shown in Fig. 4. To reveal the hidden sideof the sphincter, the graphic representation was rotated1800 on the sphincter's axis as is shown in the lowerpanel of Fig. 6. Notice the marked anteroposterior ac-
/-'/ / -loo
I
LEFT -+I . +200 00 /
// I//\
\fs~~-00
-200POSTERIOR
RIGHT200
SP in mmHg
---RP-CS_- ml: S E M
FIGURE 5 A comparison of RP UESP --- ) to pressuresmeasured with the CS probe ( ).
centuation of pressures in the region of peak pressure.In all subjects studied with the computerized three-dimensional modeling, this prominent pressure bulgewas 1 cm in width and occurred near the upperboundary of the UES. Furthermore, in all 13 subjectsstudied, the anterior peak of this bulge was closer to thepharynx than the posterior peak. Statistical comparisonof the peak posterior pressure vs. the peak anteriorpressure revealed that the anterior peak was located0.8+0.2 cm nearer the pharynx compared to the poste-rior peak, a highly significant difference (P < 0.001).Thus, axial, as well as radial, asymmetry is a consistentfeature of the human UES.
Patients who underwent laryngectomy. Computeranalysis of the CS and RP probe data from the 11 pa-tients who had undergone total laryngectomy was done
S.E
ESOPHAGS
Uso 1ooUESPin mmHg
FiGuRE 6 Three-dimensional pressure profile of the normalUES. Notice the anteroposterior accentuation of pressure andthe axial asymmetry with an orad shift of anterior pressures.In the lower panel, the graphic representation was rotated1800 to reveal the hidden side of the sphincter.
Computer Profiles of Upper Esophageal Sphincter 1039
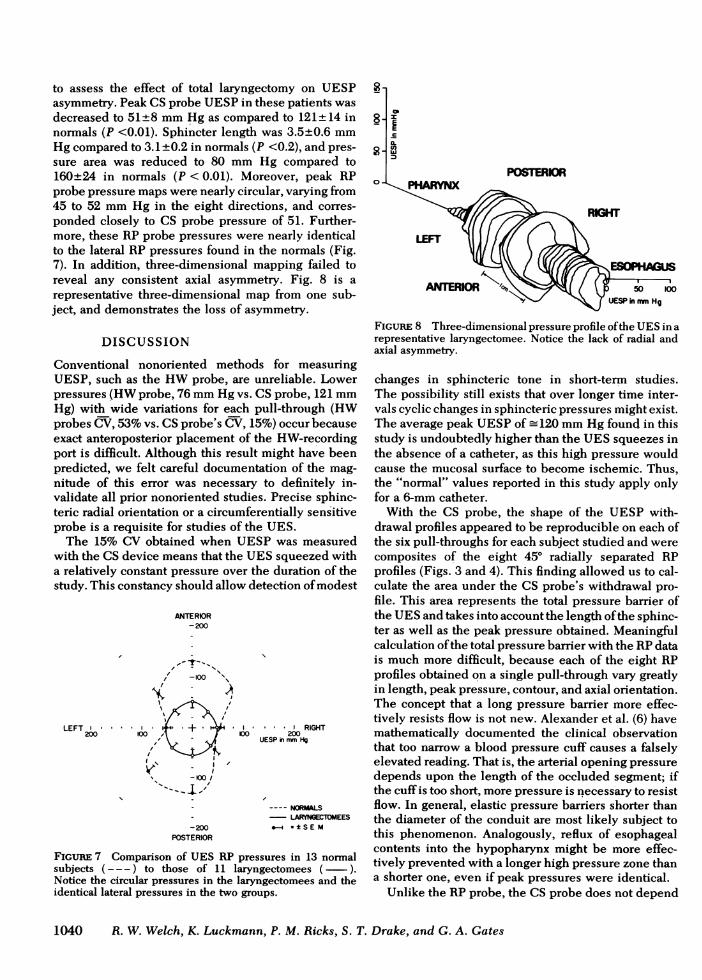
to assess the effect of total laryngectomy on UESPasymmetry. Peak CSprobe UESPin these patients wasdecreased to 51±8 mmHg as compared to 121±14 innormals (P <0.01). Sphincter length was 3.5±0.6 mmHg compared to 3.1±0.2 in normals (P <0.2), and pres-sure area was reduced to 80 mmHg compared to160±24 in normals (P < 0.01). Moreover, peak RPprobe pressure maps were nearly circular, varying from45 to 52 mmHg in the eight directions, and corres-ponded closely to CS probe pressure of 51. Further-more, these RP probe pressures were nearly identicalto the lateral RP pressures found in the normals (Fig.7). In addition, three-dimensional mapping failed toreveal any consistent axial asymmetry. Fig. 8 is arepresentative three-dimensional map from one sub-ject, and demonstrates the loss of asymmetry.
DISCUSSION
Conventional nonoriented methods for measuringUESP, such as the HWprobe, are unreliable. Lowerpressures (HWprobe, 76 mmHg vs. CSprobe, 121 mmHg) with wide variations for each pull-through (HWprobes CV, 53%vs. CSprobe's CV, 15%) occur becauseexact anteroposterior placement of the HW-recordingport is difficult. Although this result might have beenpredicted, we felt careful documentation of the mag-nitude of this error was necessary to definitely in-validate all prior nonoriented studies. Precise sphinc-teric radial orientation or a circumferentially sensitiveprobe is a requisite for studies of the UES.
The 15% CV obtained when UESPwas measuredwith the CS device means that the UESsqueezed witha relatively constant pressure over the duration of thestudy. This constancy should allow detection of modest
ANTERIOR-200
/ -100 "
LEFT ' ' RIGHT200 n0 00 200
UESP in mmtHg
-_I,~~~~n,
- ---- NORMALS- - LARYNGECTOMEES-200 = - ± SEM
POSTERIOR
FIGURE 7 Comparison of UES RP pressures in 13 normalsubjects --- ) to those of 11 laryngectomees (-).Notice the circular pressures in the laryngectomees and theidentical lateral pressures in the two groups.
POSTERIOR
RIGHT
LEFT
ANTERIOR 50 100UESPi nan Hg
FIGuRE 8 Three-dimensional pressure profile of the UESin arepresentative laryngectomee. Notice the lack of radial andaxial asymmetry.
changes in sphincteric tone in short-term studies.The possibility still exists that over longer time inter-vals cyclic changes in sphincteric pressures might exist.The average peak UESPof -120 mmHg found in thisstudy is undoubtedly higher than the UESsqueezes inthe absence of a catheter, as this high pressure wouldcause the mucosal surface to become ischemic. Thus,the "normal" values reported in this study apply onlyfor a 6-mm catheter.
With the CS probe, the shape of the UESP with-drawal profiles appeared to be reproducible on each ofthe six pull-throughs for each subject studied and werecomposites of the eight 450 radially separated RPprofiles (Figs. 3 and 4). This finding allowed us to cal-culate the area under the CS probe's withdrawal pro-file. This area represents the total pressure barrier ofthe UESand takes into account the length of the sphinc-ter as well as the peak pressure obtained. Meaningfulcalculation of the total pressure barrier with the RPdatais much more difficult, because each of the eight RPprofiles obtained on a single pull-through vary greatlyin length, peak pressure, contour, and axial orientation.The concept that a long pressure barrier more effec-tively resists flow is not new. Alexander et al. (6) havemathematically documented the clinical observationthat too narrow a blood pressure cuff causes a falselyelevated reading. That is, the arterial opening pressuredepends upon the length of the occluded segment; ifthe cuff is too short, more pressure is necessary to resistflow. In general, elastic pressure barriers shorter thanthe diameter of the conduit are most likely subject tothis phenomenon. Analogously, reflux of esophagealcontents into the hypopharynx might be more effec-tively prevented with a longer high pressure zone thana shorter one, even if peak pressures were identical.
Unlike the RPprobe, the CS probe does not depend
1040 R. W. Welch, K. Luckmann, P. M. Ricks, S. T. Drake, and G. A. Gates

upon the idiosyncrasies of fluid flow through elastictubes. Perfused manometry measures the opening pres-sure of a catheter orifice occluded by the sphincterand may depend upon the compliance of structuressurrounding the opening. The UES is anatomicallycomplex; its mucosa is backed partially by muscle andpartially by cartilage. It has not been proven that all ofthe perfused opening pressures actually reflect sphinc-teric squeeze. For example, when the catheter orificeis resting against the unyielding cricoid cartilage onemight expect a higher sphincter pressure than whenresting upon muscle. The ability to simultaneouslycompare conventional perfused pressures (RP probe)with an independent measure of sphincter pressure(CS probe) helps evaluate the wide range of pressuresfound in the UES. The CS-RP probe comparison con-firms that maximum recorded perfused pressures doreflect true sphincteric squeeze and are not measure-ment artifacts. The CSprobe appears to be a rapid, con-venient method for recording maximum sphincter pres-sure without the need for radial orientation.
Insight into the cause of the radial pressure asym-metry of the UES can be gained by inspecting the RPand CS probe data in laryngectomees. All of these pa-tients had the usual total laryngectomy with peri-operative irradiation for localized laryngeal carcinoma.This operation results in excision of the laryngeal struc-tures including the cricoid cartilage from the musclelayer in the region of the UESwith a three-layer, mid-line reapproximation of the incised muscle. Surgerymay disrupt some, but not all of the nervous supply tothe UES. When the UES loses the anterior situatedlarynx and cricoid cartilage, the radial asymmetryvanishes, pressure and area decrease, and the pressuremap becomes circular. Sphincter length is not sta-tistically different than the normals. Furthermore, themean lateral RP pressures in normals are very similarto the RPpressures found in the laryngectomy patients.
UESP axial asymmetry also disappears when thecricoid cartilage and other laryngeal structures are re-moved. There are several possible explanations for thedisappearance of UES asymmetry postlaryngectomy,such as radiation injury, surgical denervation, narrow-ing or destruction of the sphincter. Another more rea-sonable hypothesis is that the sphincteric musculature,which attaches anteriorly to the cricoid cartilage, func-tions like the jaws of a vise. The anterior moveable jawwould be the cricoid cartilage and other laryngealstructures and the posterior, fixed jaw would be thesphincteric muscle applied to the cervical spine. TheUES axial asymmetry implies that the "jaws" of theUES do not exactly oppose each other but rather arepartially offset. Asoh and Goyal (7) have recentlydemonstrated UES axial asymmetry in the opossum.Interestingly, in this species the posterior, not theanterior, pressure peak is closer to the pharynx.
Sophisticated computer analysis of RP motility trac-ings has allowed us to topographically map the com-plex asymmetric pressures of the UESin three dimen-sions. The eight simultaneous and seemingly dis-cordant profiles obtained with one pull-through of theRP system have been shown to be part of a series ofharmonious and smooth changes in pressure that arestrikingly demonstrated by the three-dimensional com-puter mapping. This mapping technique graphicallydisplays the radial and axial asymmetry of the humanUES. Webelieve computer processing and displayingof the total family of pressures obtained in physiologichigh pressure zones is an excellent way to study thesphincter's normal and pathological behavior. It ap-pears premature to accept any single value for sphincterpressure, such as the CS probe produces, without ex-tensive comparison with all the sphincteric pressuresgenerated from the three-dimensional technique.
Our computer techniques may have additional ap-plications in the measurement of other biologic systemsunder pressure. Not only can three-dimensional pres-sure profiles be generated, but by using analog todigital convertors direct on line computer processing ofpressure data is possible.
ACKNOWLEDGMENTSThe authors wish to thank Cindy Lozano for her typing of themanuscript and Bernie Schelper, medical technician, for hertechnical assistance.
This investigation was supported in part by research grants7ROlAM25609-01, 5501RR05654-07, subgrant S07RR05654from the National Institutes of Health, and R18CA18629 fromthe National Cancer Institute.
REFERENCES1. Winans, C. S. 1972. The pharyngoesophageal closure
mechanism: a manometric study. Gastroenterology. 63:768-777.
2. Kaye, M. D., J. P. Showalter, K. C. Rock, and E. Johnson.1973. A circumferentially-sensitive miniature transducerfor study of human esophageal motility. Gastroenterol-ogy. 64: 752. (Abstr.)
3. Dodds, W. J., W. J. Hogan, J. J. Stef, W. N. Miller, S. B.Lydon, and R. C. Arndorfer. 1975. A rapid pull-throughtechnique for measuring lower esophageal sphincter pres-sure. Gastroenterology. 68: 437-443.
4. \lilic-Emil, J., J. Mead, J. NI. Turner, and E. M. Glauser.1964. Improved techni(lue for estimating pleural pressurefrom esophageal balloon. J. Appl. Physiol. 19: 207-211.
5. Cline, A. K. 1974. Scalar and planar-valued curve fittingusing splines under tension. In Communications of theAssociation for Computing Machinery. R. Willoughby,editor. 17: 218-221.
6. Alexander, H., M. L. Cohen, and L. Steinfeld. 1977.Criteria in the choice of an occluding cuff for the indirectmeasurement of blood pressure. Med. Biol. Eng. Comput.15: 2-10.
7. Asoh, R., and R. K. Goyal. 1978. Manometry and electro-myography of the upper esophageal sphincter in theopossum. Gastroenterology. 74: 514-520.
Computer Profiles of Upper Esophageal Sphincter 1041