Upper Gastrointestinal Overview 2007- 2008: Practical Implications of the Newest Data Esophageal and...
30
Upper Gastrointestinal Overview 2007-2008: Practical Implications of the Newest Data Esophageal and Gastric Cancers Johanna Bendell, MD Sarah Cannon Research Institute
-
Upload
aubrie-rose -
Category
Documents
-
view
220 -
download
5
Transcript of Upper Gastrointestinal Overview 2007- 2008: Practical Implications of the Newest Data Esophageal and...

Upper Gastrointestinal Overview 2007-2008: Practical Implications of the Newest Data
Esophageal and Gastric Cancers
Johanna Bendell, MDSarah Cannon Research Institute

Conflict of Interest Disclosure• Consultant or Advisory Role
– Amgen – Array Pharmaceuticals – Genentech – Roche
• Honoraria– Amgen– Roche– Genentech– Array Pharmaceuticals
• Research Funding– Bristol-Myers Squibb – Genentech – Roche – Sanofi-Aventis– Novartis

Esophageal Cancer• 16,470 new cases estimated for 2008
– 14,280 estimated deaths
• Adenocarcinoma incidence rate increasing by 20% per year in U.S– EtOH, tobacco, obesity, genetics, diet– Barrett’s esophagus– Older trials have more patients with SCC– Adenocarcinomas predominate most trials now– Is there a difference?
• GE junctional cancers– Increase in distal esophageal and proximal gastric
cancers– Is there a difference?

Localized disease
• Controversy– Surgery alone– Preoperative chemotherapy– Preoperative chemoradiation therapy– Chemoradiation therapy alone

Preoperative chemotherapyStudy #
Patients
Pathology Chemotherapy Tumor Location
5-year survival
MRC OEO-2, 2002
Chemo: 400
Surgery: 402
SCC, Adeno
Cisplatin/5-FU Stomach10%Distal eso65%
Chemo: 23% Surgery: 17%P = 0.03
Cunningham et al, 2006
Chemo: 250
Surgery: 253
Adeno ECF Stomach 74%
GE jn12%Distal eso14%
Chemo: 36.3% Surgery:
23.0% P = 0.001
Kelsen et al, 2007
Chemo: 233
Surgery: 234
SCC, Adeno Cisplatin/5-FU Esophagus Chemo: 26% Surgery: 23%3 yearP = 0.53

FP FP (*)(*) x 2/3 every 28 days x 2/3 every 28 days
ResectionResection
Within 4 weeksWithin 4 weeks4 - 6 weeks4 - 6 weeks
ResectionResection
4 – 6 weeks4 – 6 weeks
FP x 3/4 or no treatmentFP x 3/4 or no treatmentFollow-upFollow-up
RandomizatioRandomizationn
CT + CT + SS
SS
ACCORD 07-FFCD 9703
(*) FP = 5FU: 800 mg/m² CI x 5 days - CDDP: 100 mg/m² at d1 or d2, 1-hr infusion Boige, ASCO 2007

CT + SCT + SN = 113N = 113
Preop CT (2-3 Preop CT (2-3 cycles)cycles)
N = 98 N = 98 (89%)(89%)
SurgerySurgeryN = 109 N = 109 (96%)(96%)
Postop CT (1-4 Postop CT (1-4 cycles)cycles)
N = 54 N = 54 (51%)(51%)
SSN = 111N = 111
SurgerySurgeryN = 110 N = 110 (99%)(99%)
Trial profile
Boige, ASCO 2007

Disease-free survival
5-year DFS: 21% (14-30%) vs 34% (26-44%)
Disease-free survivalusing landmark methods
681113141921242829354257111
14161717253134384448536277113
0.00
0.20
0.40
0.60
0.80
1.00
0 12 24 36 48 60 72Months
Surgery
Chemotherapy + Surgery
At risk
logrank : p = 0.0033
0-0.5 1 2 3 4 5 6 7
111 57 35 28 21 14 11 6 113 77 53 44 34 25 17 14
yearsyears
At riskAt risk
___ S___ CT + S
Logrank p value = 0.0033Logrank p value = 0.0033Hazard Ratio = 0.65 Hazard Ratio = 0.65 (95% CI 0.48-0.89)(95% CI 0.48-0.89)
Boige, ASCO 2007

713162738537911114172741536593113
0,00
0,20
0,40
0,60
0,80
1,00
0 1 2 3 4 5 6 7
A risque
logrank : p = 0,021
___ S___ CT + S
yearsyears
Overall survival
At riskAt risk
5-year OS: 24% (16-33%) vs 38% (28-47%)
Logrank p value = 0.021Hazard Ratio = 0.69 (95% CI 0.50-0.95)
Boige, ASCO 2007

ACCORD07-FFCD 9703
• Preoperative chemotherapy• 14% improvement in 5 year OS
– Similar to MAGIC (13%)– MRC Preop ECF vs. CF
• Decrease in systemic recurrence– Local recurrence 26% (S) vs. 24% (CT+S)– Systemic recurrence 56% (S) vs. 42%
(CT+S)

Preoperative ChemoradiationStudy # Patients Patholo
gyChemotherapy Radiatio
n (Gy)3-yearsurvival
Walsh et al, 1996
Trimodality: 58
Surgery: 55
Adeno Cisplatin/5-FU 40 Tri: 32% Surgery: 6%P = 0.01
Bosset et al (EORTC),
1997
Trimodality: 143
Surgery: 139
SCC Cisplatin 37 Tri: 37% Surgery:
35%P = NS
Urba et al, 2001
Trimodality: 50
Surgery: 50
SCC,Adeno
Cisplatin/5-FU/vinblastine
45 Tri: 30% Surgery:
16%P = 0.15
Burmeister et al, 2005
Trimodality: 128
Surgery: 128
SCC, Adeno
Cisplatin/5-FU 35 Tri: 33% Surgery:
30%P = 0.57
Tepper et al (CALGB), 2006
Trimodality: 30
Surgery: 26
SCC,Adeno
Cisplatin/5-FU 50.4 Tri: 39%Surgery:
16%5 yearP < 0.008

POET TrialArm A
Week
Arm B
PLF I PLF III (3 weeks)
15 x 2 Gy in 3 weeks
PE (1 week)
Surgery
Surgery
1 1314 17 20-21
PLF: Cisplatin 50mg/m2, 1h, d 1,15,29. Leucovorin/5-FU 500mg/m2 2h / 2g/m2 24h, d 1,8,15,22,29,36PE: Cisplatin 50 mg/m2, 1h, d 2+8. Etoposide 80 mg/m2, 1h, d 3-5
PLF II
6 7
PLF I PLF II
Stahl, ASCO 2007

Overall Survival
Logrank Logrank p = 0.07p = 0.07HR Arm B vs. AHR Arm B vs. A0.67 (0.41-1.07)0.67 (0.41-1.07)
Arm B
Arm A
Follow-up 45.6 mo
47.4%
27.7%
Stahl, ASCO 2007

Freedom from Local Tumor Progression
Logrank Logrank p = 0.06p = 0.06HR Arm B vs. AHR Arm B vs. A0.45 (0.19 -1.05)0.45 (0.19 -1.05)
76.5%
59.0%
Arm B
Arm A
Stahl, ASCO 2007

Neoadjuvant vs. adjuvant approach• Roth, et al. World GI 2007• Randomized 70 patients with locally
advanced gastric cancer to 4 cycles of preoperative or adjuvant DCF
• Original plan to randomize 252 patients– Closed early due to poor accrual

TCF => STCF => SN = 34N = 34
Preop CT (4 Preop CT (4 cycles)cycles)
Started N=33 Started N=33 (97%)(97%)
Completed N= Completed N= 25 (74%)25 (74%)SurgerySurgery
N = 32 (94%)N = 32 (94%)Postop CT (4 Postop CT (4
cycles)cycles)Started N = 23 Started N = 23
(66%)(66%)Completed N = Completed N =
12 (34%)12 (34%)
S =>TCF S =>TCF N = 35N = 35
SurgerySurgeryN = 35 (100%)N = 35 (100%)
SAKK Neoadjuvant vs. Adjuvant Trial
pCR in 4 patients (12.9%)pCR in 4 patients (12.9%)
Roth, World GI 2007

What do we see in local treatment of esophageal cancer?• Many of these trials are mixed populations
– Adeno, SCC– Esophageal, GE junction, gastric cancers –
accrual issues• Surgery alone is not enough• Preoperative chemotherapy improves survival for
patients (now 3/4 trials, 1 meta-analysis)• Preoperative chemoradiation therapy likely better
than surgery alone, and maybe better than chemotherapy alone– Chemoradiation more toxic– True for squamous and adenos– Subgroup of patients who do not need surgery?

What do we do now?• CRITICS Trial
– Preoperative ECX, rand postop chemoradation or chemo alone
• Korean Trial– Preoperative cisplatin/capecitabine, then randomization to
chemoradiation or chemo alone• CALGB 80101
– Postoperative chemoradiation with 5-FU or ECF• MRC OEO5
– Preoperative ECF vs. CF• MAGIC 2
– Preoperative ECX with or without bevacizumab• RTOG 0436
– Preoperative chemoradiation with or without cetuximab• CALGB 80302
– PET as prognostic indicator

Metastatic Gastric Cancer
• Gastric cancer– 21,500 new cases expected in the U.S. in
2008, 10, 880 deaths
• Unclear as to what is best metastatic regimen– ECF, DCF, IC, EOX?– Role of oral fluoropyrimidines
• Is combination therapy better than sequential?

S-1• Oral fluoropyrimidine consisting of tegafur,
CDHP, and OXO in a 1:0.4:1 molar ratio– tegafur is converted to 5-FU– CDHP (chloro-2.4-dihydroxypyridine) inhibits
DPD, preventing 5-FU degradation– OXO (potassium oxonate) protects against drug
induced diarrhea caused by phosphorylation of 5-FU by inhibiting the responsible enzyme – OPRT (oronate phosphoribosyl transferase)

S-1 40 mg/m2, po, bid, days 1-28q 6 weeks
5-FU CI
CPT-11 + CDDP
S-1
Randomization
800 mg/m2/day, ci, days 1-5q 4 weeks
CPT-11 70 mg/m2, div, days 1&15CDDP 80 mg/m2, div, day 1q 4 weeks
Phase III Study (JCOG9912)Phase III Study (JCOG9912)
Continued until disease progression, unacceptable toxicities, patient’s refusal
BSA < 1.25 80 mg/body/day 1.25 < BSA < 1.5 100
mg/body/day 1.5 < BSA 120
mg/body/day
Boku, ASCO 2007

Progression-free Survival and Response rateProgression-free Survival and Response rate
Response rate
- in pts with target lesion -
5-FU CI
CPT-11
+CDDP S-1
CR+PR 15 68 49
n 175 181 175
RR 9% 38% 28%
CR and PR were confirmedby central review
0.0010.62-0.900.754.2M234
<0.001
-
0.57-0.83
-
95%C.I.
-2.9M234
0.694.8M236
HRMedian n P-value†
12 24 (months)
0
50
(%)100
†: one-sided log-rank test (superiority)
S-1
5-FU CI
CPT-11+CDDP
PFS
Boku, ASCO 2007
12 24 36 (months)0
50
(%)100
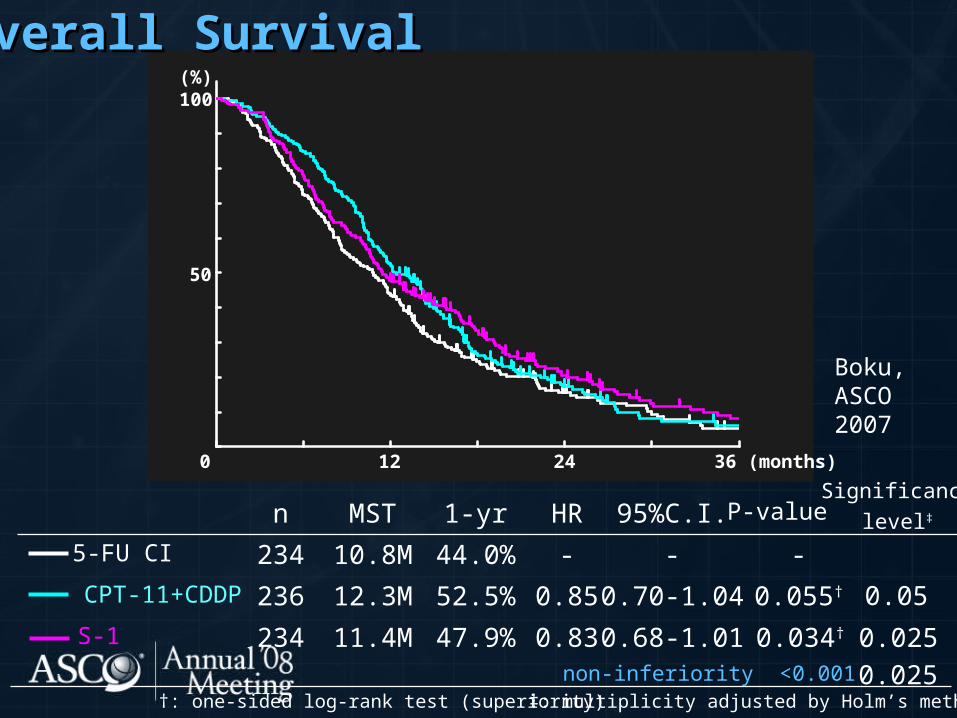
Overall SurvivalOverall Survival
P-value
0.034†
0.055†
-
0.68-1.01
0.70-1.04
-
95%C.I.
-44.0%10.8M2345-FU CI
0.8347.9%11.4M234S-1
0.8552.5%12.3M236CPT-11+CDDP
HR1-yrMSTn
†: one-sided log-rank test (superiority)non-inferiority <0.001
‡: multiplicity adjusted by Holm’s method
Significancelevel‡
0.05
0.0250.025
Boku,ASCO2007

JCOG 9912
• S-1 is non-inferior to CI 5-FU• Cisplatin/irinotecan better than CI 5-
FU• Cisplatin/irinotecan (this regimen)
more toxic• S-1 results approximate combination
therapy

SPIRITS TrialSPIRITS Trial
AGCAGC
No priorNo priorChemo.Chemo.
RR
S-1 aloneS-1 aloneS-1: 40-60 mg BID for 28 days q6wksS-1: 40-60 mg BID for 28 days q6wks
S-1 + CDDPS-1 + CDDPS-1: 40-60 mg BID for 21 days q5wksS-1: 40-60 mg BID for 21 days q5wks
CDDP: 60 mg/mCDDP: 60 mg/m22 iv on day 8 iv on day 8
Central RandomizationCentral Randomization (dynamic balancing)(dynamic balancing)Adjustment Factors:Adjustment Factors: InstituteInstitute PSPS Unresectable vs RecurrentUnresectable vs Recurrent
Narahara, ASCO 2007
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54
MonthsMonths
Esti
mate
d p
rob
ab
ilit
y
Esti
mate
d p
rob
ab
ilit
y
(%)
(%)
11.011.0 13.013.0
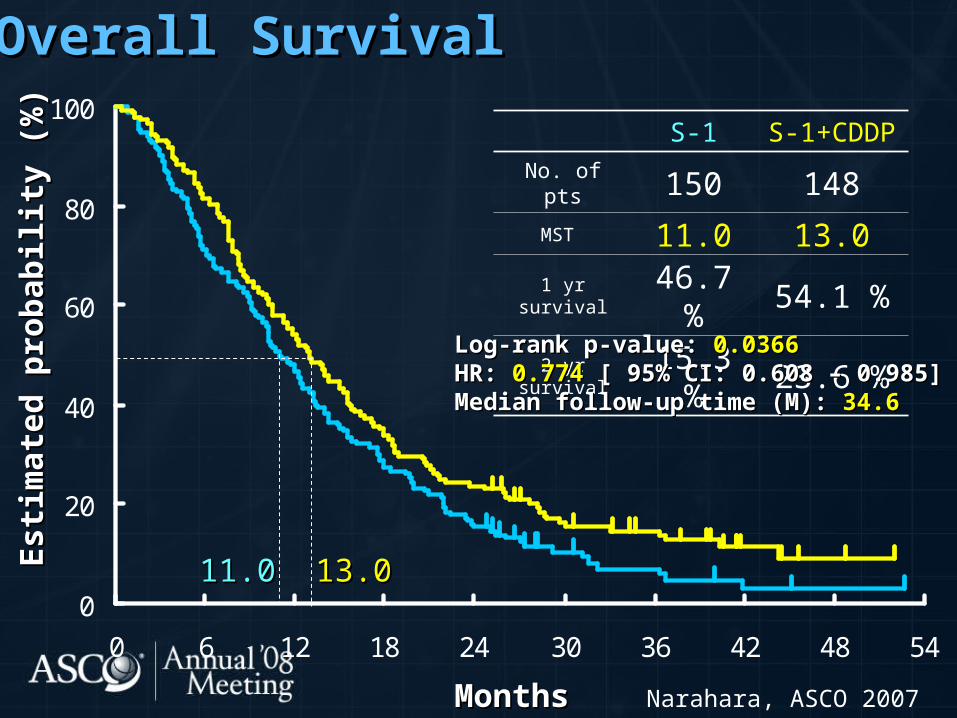
Overall SurvivalOverall Survival
S-1S-
1+CDDP
No. of pts 150 148MST 11.0 13.0
1 yr survival46.7
%54.1 %
2 yr survival15.3
%23.6 %
Log-rank p-value:Log-rank p-value: 0.0366 0.0366HR: HR: 0.774 0.774 [ 95% CI: 0.608 – 0.985][ 95% CI: 0.608 – 0.985]Median follow-up time (M): Median follow-up time (M): 34.634.6
Narahara, ASCO 2007

0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54
Progression-Free SurvivalProgression-Free Survival
Log-rank p-value: Log-rank p-value: <0.0001<0.0001HR:HR: 0.5670.567 [ 95% CI: 0.437 – 0.734] [ 95% CI: 0.437 – 0.734]
Esti
mate
d p
rob
ab
ilit
y
Esti
mate
d p
rob
ab
ilit
y
(%)
(%)
MonthsMonths
6.06.04.04.0
S-1 S-1+CDDP
No. of pts 150 148PFS 4.0 6.0
Narahara, ASCO 2007

Overall ResponseOverall Response
No. Response
Overall RR CR PR SD PD NE
S-1 106 1 32 34 34 5 31 %S-1+CDDP
87 1 46 13 24 3 54 %
Criteria : RECIST (Extramural Review)Criteria : RECIST (Extramural Review)
Fisher’s Exact Test p-value: Fisher’s Exact Test p-value: 0.00180.0018
Narahara, ASCO 2007

IRIS GC0301/TOP-002
• Randomized phase III study• 326 patients randomized• S-1 alone vs. S-1 plus irinotecan• Response rate
– 26.9% vs. 41.5%
• 1-year survival– 44.9% vs. 52.0%, NS
• 22% of patients were censored
Imamura, GI ASCO 2008

Metastatic Gastric Cancer• We still don’t know the optimal regimen for
patients with metastatic disease– Combination vs. sequential therapy– Role of oral fluoropyrimidines, newer platinum agents,
taxanes
• More S-1 studies are forthcoming– FLAGS - 1053 pts, accrual completed 3/07– 5-FU/cis vs. S-1/cis
• Trials of biologics are underway– AVAGAST – capecitabine/cisplatin with or without
bevacizumab– CALGB 80403 – FOLFOX-cetuximab, cisplatin/irinotecan-
cetuximab, ECF-cetuximab– ToGA – capecitabine/cisplatin with or without
trastuzumab