Management of tuberculosis(TB, purpose only
24
Management of tuberculosis(TB,結核 ) KY Yuen 2011 Burden (負擔)of the problem of TB • Global population: 1/3 infected • New cases: >8 million/yr • Location: 95% in developing countries • Mortality: 2 million/yr • China: 1.35 billion/6.97 billion: 19.3%/yr (>1.6 million new case, 0.4 million deaths) • Hong Kong: 90 per 100,000 population, about 6000 new cases/yr, 200 deaths/yr Restricted for teaching purpose only 1 Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
Transcript of Management of tuberculosis(TB, purpose only
11/25/2011
1
Management of
tuberculosis(TB,結核 )
KY Yuen 2011
Burden (負擔)of the problem of TB
• Global population: 1/3 infected
• New cases: >8 million/yr
• Location: 95% in developing countries
• Mortality: 2 million/yr
• China: 1.35 billion/6.97 billion: 19.3%/yr
(>1.6 million new case, 0.4 million deaths)
• Hong Kong: 90 per 100,000 population,
about 6000 new cases/yr, 200 deaths/yr
Restric
ted fo
r teac
hing purpose only
1
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
2
J Hosp Infect. 2006 Oct;64(2):100-14.
Sneezing/coughing: Produce as many as 40 000 droplets of 0.5 -12
µm expelled at a velocity of 100 m/s
N Engl J Med. 2004 Apr 22;350(17):1710-2.
Emerg Infect Dis. 2006 Nov;12(11):1657-62.
20 µm
6 µm
≤ 5 µm
Arbitrary cut-off for
the size of the
droplet
Restric
ted fo
r teac
hing purpose only
2
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
3
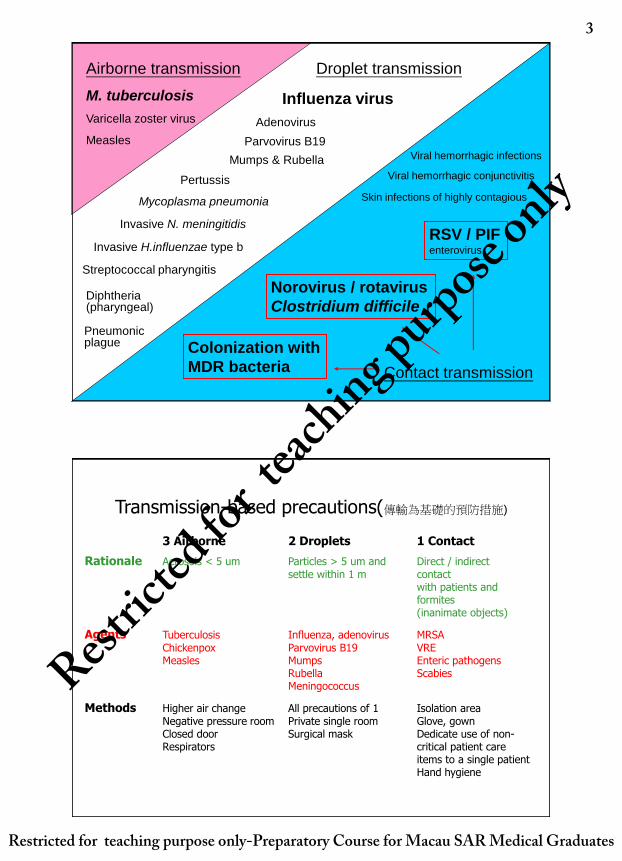
Airborne transmission
M. tuberculosis
Varicella zoster virus
Measles
Droplet transmission
Invasive H.influenzae type b
Invasive N. meningitidis
Diphtheria (pharyngeal)
Adenovirus
Influenza virus
Parvovirus B19
Mumps & Rubella
Mycoplasma pneumonia
Streptococcal pharyngitis
Pertussis
Pneumonic plague
Contact transmission
Colonization with
MDR bacteria
Norovirus / rotavirus
Clostridium difficile
RSV / PIF enterovirus
Skin infections of highly contagious
Viral hemorrhagic conjunctivitis
Viral hemorrhagic infections
Transmission-based precautions(傳輸為基礎的預防措施)
3 Airborne 2 Droplets 1 Contact
Rationale Aerosols < 5 um Particles > 5 um and Direct / indirect settle within 1 m contact with patients and formites (inanimate objects)
Agents Tuberculosis Influenza, adenovirus MRSA Chickenpox Parvovirus B19 VRE Measles Mumps Enteric pathogens Rubella Scabies Meningococcus
Methods Higher air change All precautions of 1 Isolation area Negative pressure room Private single room Glove, gown Closed door Surgical mask Dedicate use of non- Respirators critical patient care items to a single patient Hand hygiene
Restric
ted fo
r teac
hing purpose only
3
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
4
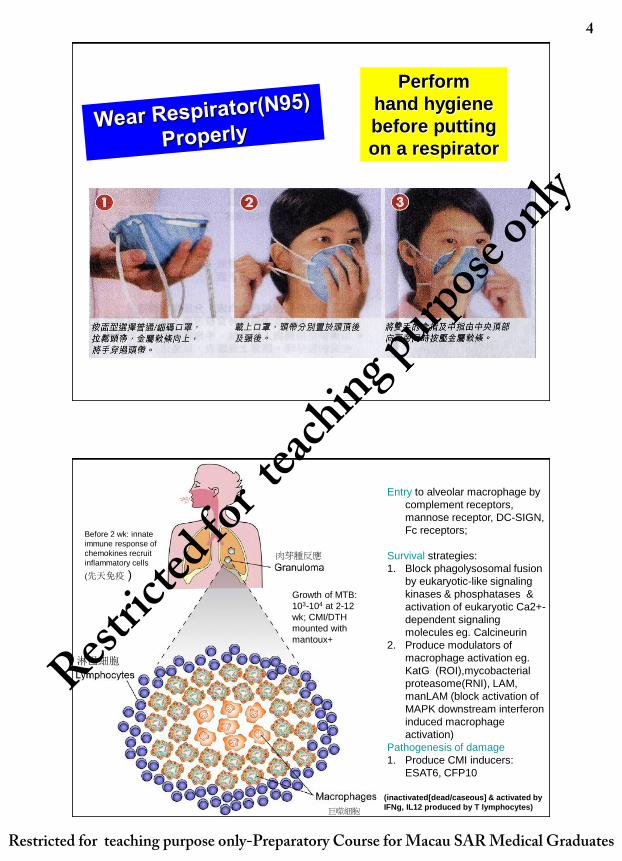
Perform
hand hygiene
before putting
on a respirator
Entry to alveolar macrophage by
complement receptors,
mannose receptor, DC-SIGN,
Fc receptors;
Survival strategies:
1. Block phagolysosomal fusion
by eukaryotic-like signaling
kinases & phosphatases &
activation of eukaryotic Ca2+-
dependent signaling
molecules eg. Calcineurin
2. Produce modulators of
macrophage activation eg.
KatG (ROI),mycobacterial
proteasome(RNI), LAM,
manLAM (block activation of
MAPK downstream interferon
induced macrophage
activation)
Pathogenesis of damage
1. Produce CMI inducers:
ESAT6, CFP10
(inactivated[dead/caseous] & activated by
IFNg, IL12 produced by T lymphocytes)
Growth of MTB:
103-104 at 2-12
wk; CMI/DTH
mounted with
mantoux+
Before 2 wk: innate
immune response of
chemokines recruit
inflammatory cells
(先天免疫 )
巨噬細胞
肉芽腫反應
淋巴細胞 Restric
ted fo
r teac
hing purpose only
4
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
5
停止吞噬體與溶酶體融合融合
Airborne transmission of MTB &
progression to active TB
• Droplet nuclei (飛沫核<0.5 um) suspended in air for long time: sneezing, singing, talking, aerosol generating medical procedure
• Risk of infection: concentration of MTB in the air, length of exposure, & immune status of exposed person
• Risk: amount of contaminated air breathed, not direct contact with index case
• Mantoux(TST) conversion: 50% if 8 hours per day for 6 months with index patient
• Lifetime risk of progression to active TB:10% (5% within first 2 yrs after infection)
• Risk of progression to active TB in HIV cases: 5% to 10% per year
Restric
ted fo
r teac
hing purpose only
5
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
6
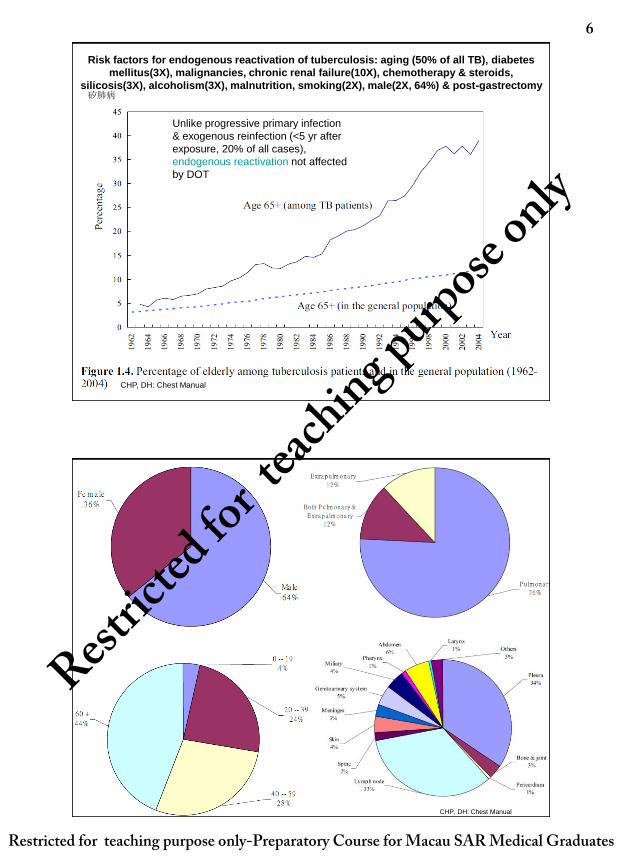
Risk factors for endogenous reactivation of tuberculosis: aging (50% of all TB), diabetes
mellitus(3X), malignancies, chronic renal failure(10X), chemotherapy & steroids,
silicosis(3X), alcoholism(3X), malnutrition, smoking(2X), male(2X, 64%) & post-gastrectomy
Unlike progressive primary infection
& exogenous reinfection (<5 yr after
exposure, 20% of all cases),
endogenous reactivation not affected
by DOT
CHP, DH: Chest Manual
矽肺病
CHP, DH: Chest Manual
Restric
ted fo
r teac
hing purpose only
6
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
7
Ways of making a Diagnosis of
tuberculosis
• Clinical: symptoms & signs; urinalysis
• Radiological: CXR-PA, lateral, CT scan (sensitive but not specific)
• Microbiolgical (Gold standard): early morning sputum, gastric
aspirate, BAL, early morning urine, stool,
pleural/pericardial/peritoneal/joint fluid, CSF, tissue biopsy (pleura,
lymph node, marrow, liver) taken for Microscopy: AFB smear (Ziehl-
Neelsen/Auromine O fluorescent stain) & Mycobacterial Culture with
drug sensitivity testing (Lowentein Jensen/Middlebrook culture
medium for mycobacteria; 藥敏試驗)
• PCR: rapid, specific but have false negative in smear negative
specimens
• Histology of tissue biopsy (needle biopsy or open biopsy)
• Host enzymes (Adenosine deaminase[ADA] in CSF/pleural fluid)
• Tuberculin skin test (結核菌素皮膚試驗)
• Gamma interferon release assay (γ干擾素釋放試驗) from Ex vivo
peripheral blood mononuclear cells
Clinical symptoms & signs
• Primary TB(原發性肺結核): TST/GIRA-, subpleural lesion mid/lower lobe & regional lymph node: ILI, pneumonitis, lobar collapse, bronchiectasis, pleural effusion in 10% who progress; hypersensitivity phenomenon: erythema nodosum/induratum(結節性紅斑), phlyctenular conjunctivitis & dactylitis;
• Serious progression to Miliary (粟粒性肺結核): hematogenous spread to lungs, kidneys, bone marrow, CNS & anywhere; CXR: diffuse micronodular shadows; fever, prostration, dry cough, dyspnea, choroidal tubercles.
• Postprimary pulmonary TB(90%): MT/GIRA+, Apical lesions, chronic cough/hemoptysis, evening fever, night sweating, weight loss;
• Postprimary extrapulmonary(肺外)TB(10%): pleuritis(effusion, man); lymphadenitis(women); urinary(sterile pyuria/haematuria), genito-: epididymo-orchitis, infertility, pelvic pain, dysmenorrhea; arthritis & skeletal deformity; pericarditis(effusion); meningitis/myelitis; intestinal(diarrhea) peritonitis(ascites), abdominal mass; granulomatous hepatitis; adrenalitis;
• Cryptic TB: hematogenous, eldelry; fever, weight loss, dissemination in RES: bone marrow, hepatosplenomegaly, CNS
Restric
ted fo
r teac
hing purpose only
7
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
8
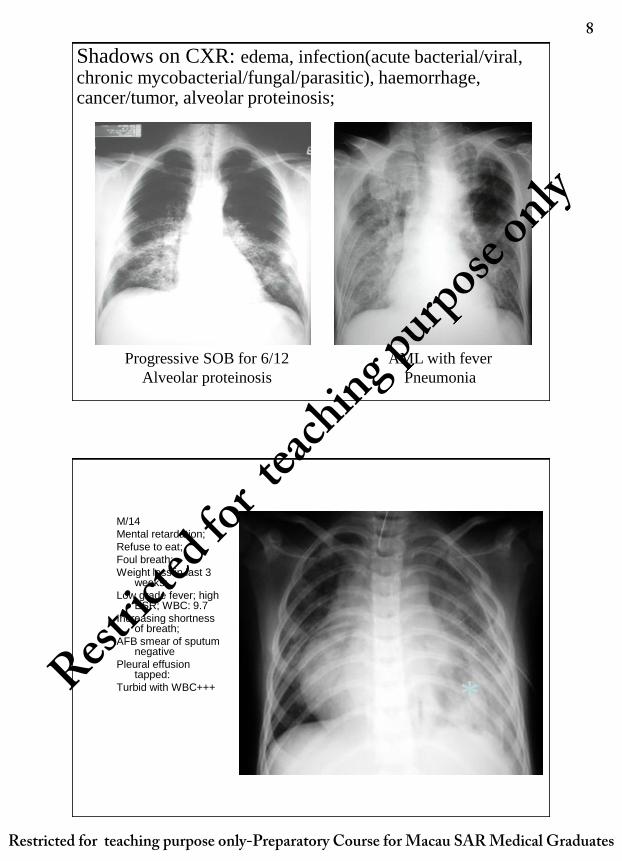
Shadows on CXR: edema, infection(acute bacterial/viral, chronic mycobacterial/fungal/parasitic), haemorrhage, cancer/tumor, alveolar proteinosis;
Progressive SOB for 6/12
Alveolar proteinosis
AML with fever
Pneumonia
M/14
Mental retardation;
Refuse to eat;
Foul breath;
Weight loss in last 3 weeks;
Low grade fever; high ESR; WBC: 9.7
Increasing shortness of breath;
AFB smear of sputum negative
Pleural effusion tapped:
Turbid with WBC+++ * Restric
ted fo
r teac
hing purpose only
8
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
9
*
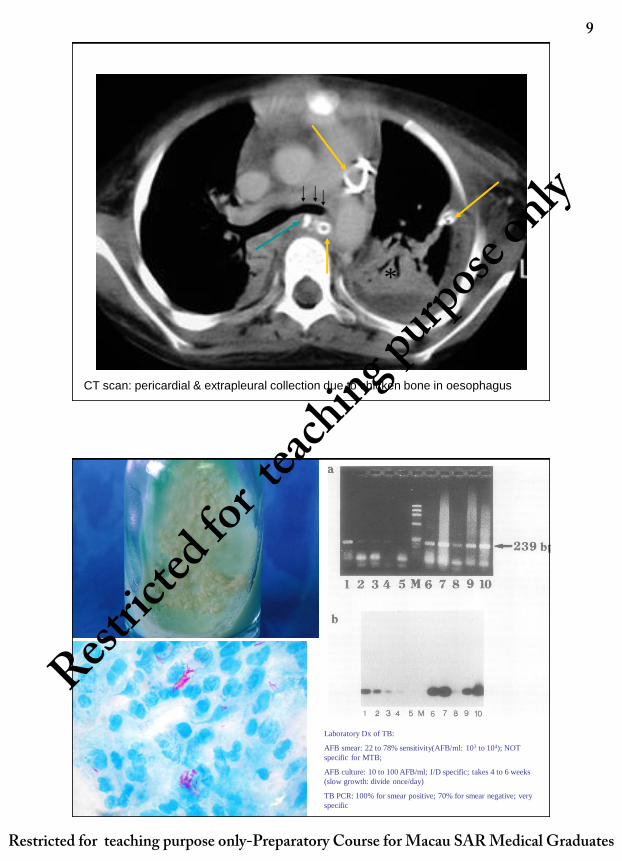
CT scan: pericardial & extrapleural collection due to chicken bone in oesophagus
Laboratory Dx of TB:
AFB smear: 22 to 78% sensitivity(AFB/ml: 103 to 104); NOT
specific for MTB;
AFB culture: 10 to 100 AFB/ml; I/D specific; takes 4 to 6 weeks
(slow growth: divide once/day)
TB PCR: 100% for smear positive; 70% for smear negative; very
specific
Restric
ted fo
r teac
hing purpose only
9
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
10
Nucleic acid amplification(PCR, RT-
PCR): slow/difficult to grow microbes
In vitro reproduction of
one TB bacterium (not
visible on microscopy)
1010-11 organisms
One visible colony on
solid culture medium
In vitro reproduction of
one short segment of
specific DNA/RNA
1012 copies
Readily visible band of
defined size on gel
electrophoresis
One cycle 18–24 h
Time taken 4–6 weeks
One cycle 2 min
Time taken 2 h
Cheng VC, et al, Yuen KY. Clinical evaluation of the polymerase chain reaction for the rapid diagnosis of tuberculosis. J Clin Pathol 2004;57:281–285.
Restric
ted fo
r teac
hing purpose only
10
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
11
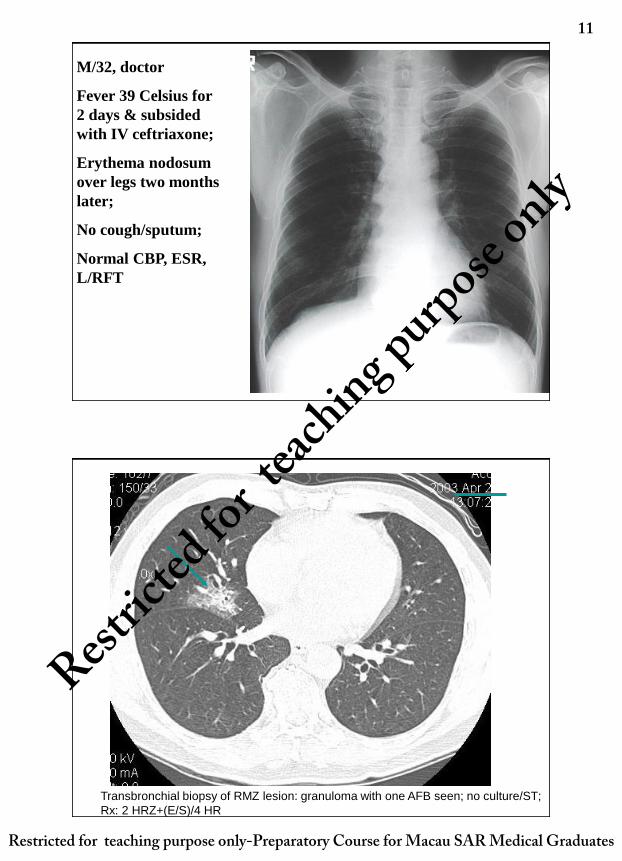
M/32, doctor
Fever 39 Celsius for
2 days & subsided
with IV ceftriaxone;
Erythema nodosum
over legs two months
later;
No cough/sputum;
Normal CBP, ESR,
L/RFT
Transbronchial biopsy of RMZ lesion: granuloma with one AFB seen; no culture/ST;
Rx: 2 HRZ+(E/S)/4 HR
Restric
ted fo
r teac
hing purpose only
11
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
12
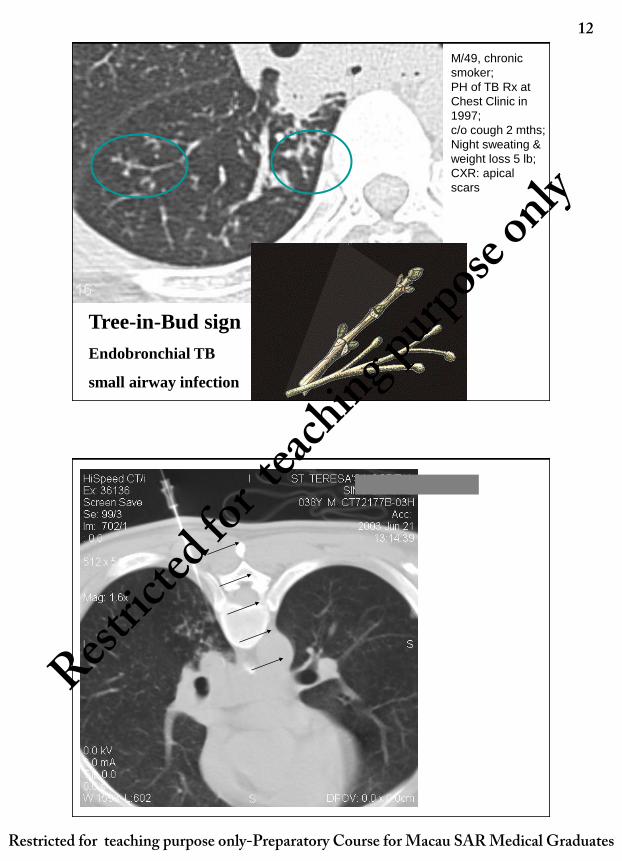
Tree-in-Bud sign
Endobronchial TB
small airway infection
M/49, chronic
smoker;
PH of TB Rx at
Chest Clinic in
1997;
c/o cough 2 mths;
Night sweating &
weight loss 5 lb;
CXR: apical
scars
Restric
ted fo
r teac
hing purpose only
12
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
13
Sputum & BAL smear and
culture negative but TB PCR
positive on BAL;
Only the needle biopsy is
histologically positive for AFB
Retreatment: 3HRZES/6HRE
Postprimary active tuberculosis in a patient with a chronic cough Tree-in-bud appearance
The tree-in-bud pattern on CT scan correlates well with histopathological changes of :
1. bronchiolar luminal impaction with mucus, pus, or fluid,
2. Dilated & thickened walls of the peripheral airways and peribronchiolar inflammation and
therefore visible bronchioles which are affected
Restric
ted fo
r teac
hing purpose only
13
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
14
Principles of anti-TB Rx
• Directly Observed Therapy short-course (DOTS直接觀察短期治療) • Modification according to drug sensitivity test results, disease severity,
underlying illness, organ dysfunction, drug side effects, response to Rx
• Notification for contact tracing & health education;
• Baseline CBP, LFT, RFT, HBsAg; educate on warning signs of hepatoxicity, allergic reaction, visual & hearing impairment
• Usual duration of Rx: 6 months; extension to 9 to 12 or more mths for relapse, cavitation, persistent culture positivity at 2 mths, drug resistance,
• 4 drugs (HRZ+E/S) for initial phase of 2 months to reduce the microbial load & prevent emergence of resistant mutants; 2 drugs (HR) for continuation phase of 4 months for the slow grower; daily or thrice weekly DOTS
• The initial phase can be extended to 3 to 4 months if suboptimal clinical, radiological or microbiological response
• Monitor symptoms, side effects, AFB smear & culture blood tests & imaging;
• H: isoniazid; R: rifampicin; Z: pyrazinamide; E: ethambutol; S: streptomycin; O: levofloxacin/ofloxacin
.
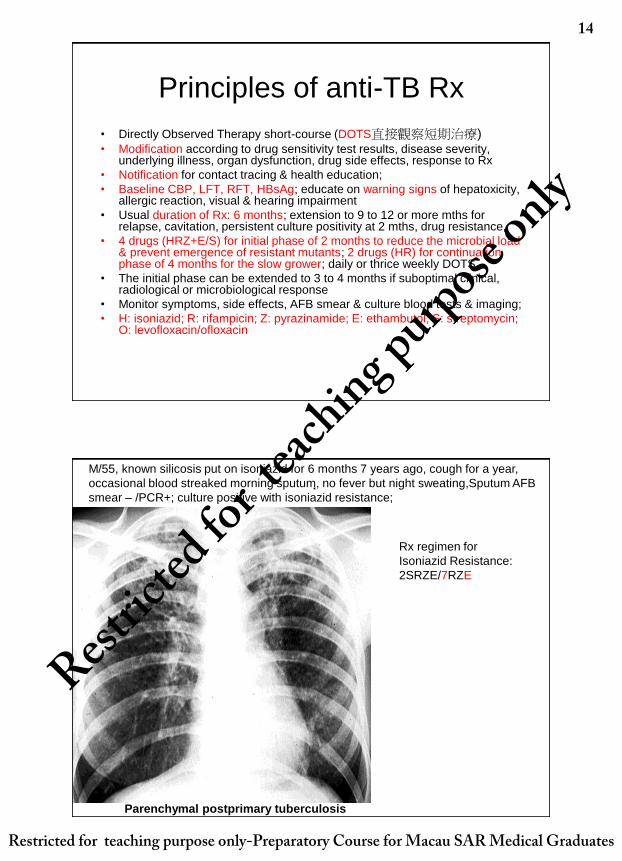
Parenchymal postprimary tuberculosis
M/55, known silicosis put on isoniazid for 6 months 7 years ago, cough for a year,
occasional blood streaked morning sputum, no fever but night sweating,Sputum AFB
smear – /PCR+; culture positive with isoniazid resistance;
Rx regimen for
Isoniazid Resistance:
2SRZE/7RZE
Restric
ted fo
r teac
hing purpose only
14
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
15
Bilateral upper lobes disease, RUL infiltrates, LUL cavities
M/17, recent immigrant from Mainland, occasional blood streak sputum; evening fever & night
sweating; poor performance at school, poor appetite, weight loss; sputum AFB smear+++;
4 HRZE/5 HR
Extension of both initial &
continuation phase
because of
1. Cavitory disease,
systemic upsets
2. Persistent culture
positive at 2 months
M/44, computer engineer, routine check up for a new job; no symptoms; Radiologist report: RUL cavity, posterior segment; early morning sputum AFB smear: occasional+; HBsAg positive, ALT146; HBV viral load: >105
Put on SMO & entecavir
When LFT normalize,
reintroduce H & R; off S;
Total duration of Rx: 9 with 6
months of HR
Restric
ted fo
r teac
hing purpose only
15
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
16
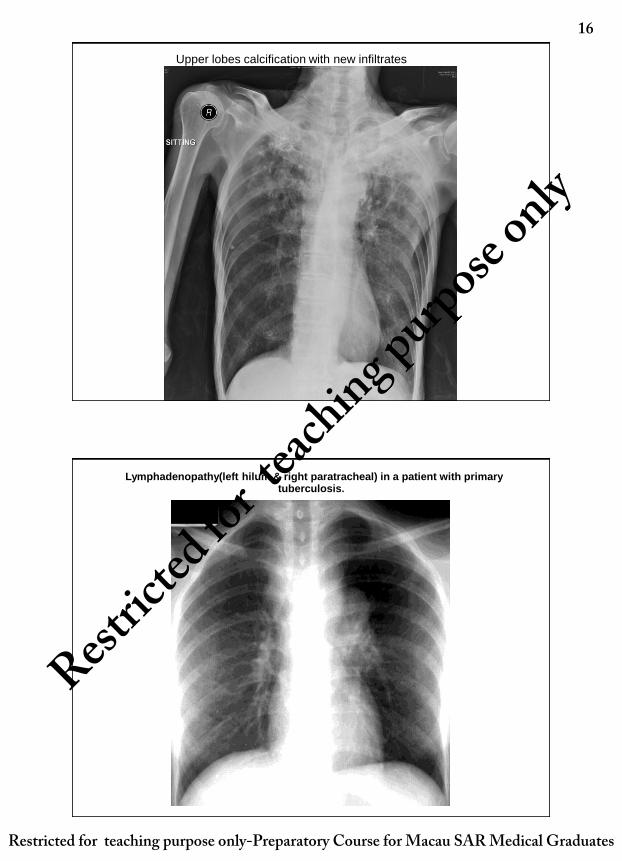
Upper lobes calcification with new infiltrates
Lymphadenopathy(left hilum & right paratracheal) in a patient with primary tuberculosis.
Restric
ted fo
r teac
hing purpose only
16
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
17
Right pleural effusion
Raised right diaphragm - subpulmonary effusion for lateral decubitus & USG aspiration/pleural biopsy
Restric
ted fo
r teac
hing purpose only
17
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
18
F/62, systemic lupus erythematosis on maintenance prednisolone 15mg/D & mycophenolate; recent fatigue and weight loss; sputum AFB smear –; Miliary shadows on CXR; BAL PCR and AFB culture positive;
Miliary TB:
3HRZ+(E/S)
/9HRE
Restric
ted fo
r teac
hing purpose only
18
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
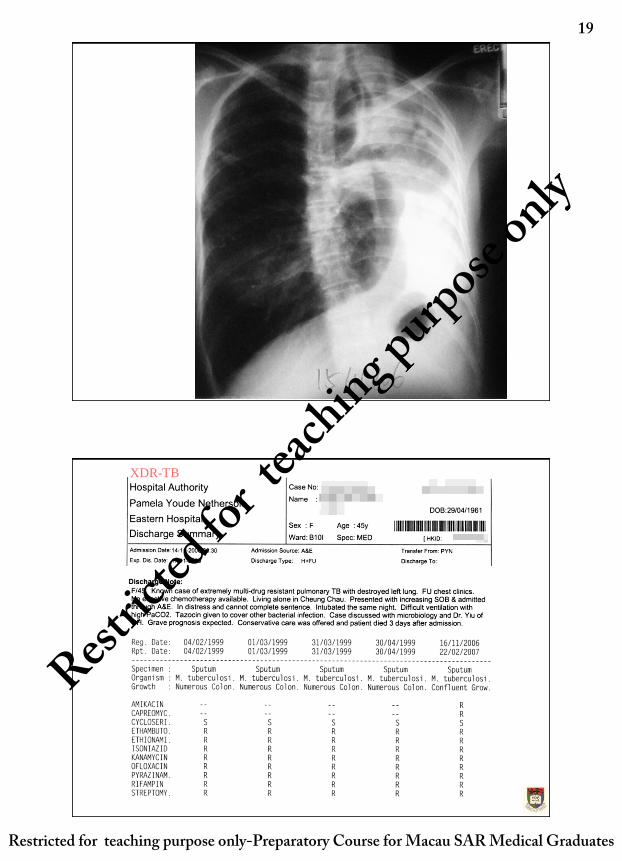
19
CXR at last
admission of a
45 yr old nurse
with XDR-TB
XDR-TB
Restric
ted fo
r teac
hing purpose only
19
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
20
Modification of basic DOTS anti-TB regimen
• New case: 2 HRZ+(E/S)/4 HR
• Retreatment: 3HRZES/6HRE
• Isoniazid R: 2SRZE/7RZE
• TB meningitis: 3HRZES/9HRE
• Miliary TB: 3HRZ+(E/S) /9HRE
• TB bone & joint: 2 HRZ+(E/S) /10 HR
• Diabetes/Immunosuppressed hosts: 2 HRZ+(E/S)/9 HR
• Pregnancy/poor hearing: No S
• Children/poor vision: No E
• Silicosis & TB: 2HRZ+(E/S)/7HR
• Elderly >65 for dose reduction: H(200mg); pyrazinamide(1gm) to decrease hepatotoxicity; add pyridoxine;
• Poor liver function & shown not tolerating HRZ: 12 SMO
• Poor renal function: H(200mg), add pyridoxine; adjust E according to creatinine clearance
Rx of LTBI(latent 潛伏 TB infection)
Initial clinical evaluation and Dx of LTBI (usually household contacts)
Use of TST and definition of positivity (cut-off value depends on risk level and purpose)
• In Hong Kong: 2TU of PPD-RT23
• • 15 mm in general population or conversion
• • 10 mm in silicotic patients/ patients receiving anti-TNF
• • 5 mm in HIV+ve patients/ infants aged below 1
Before Rx of LTBI
• Clients who have past Rx for TB or LTBI are generally not candidates for further Rx of LTBI
• Rule out active TB by CXR,
• Discuss with client the pros & cons
• Choose regimen: drug tolerance, index case INH-resistance, duration
During Rx
• monitor for side effects of drugs, adherence, and possible development of active TB
Restric
ted fo
r teac
hing purpose only
20
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
21
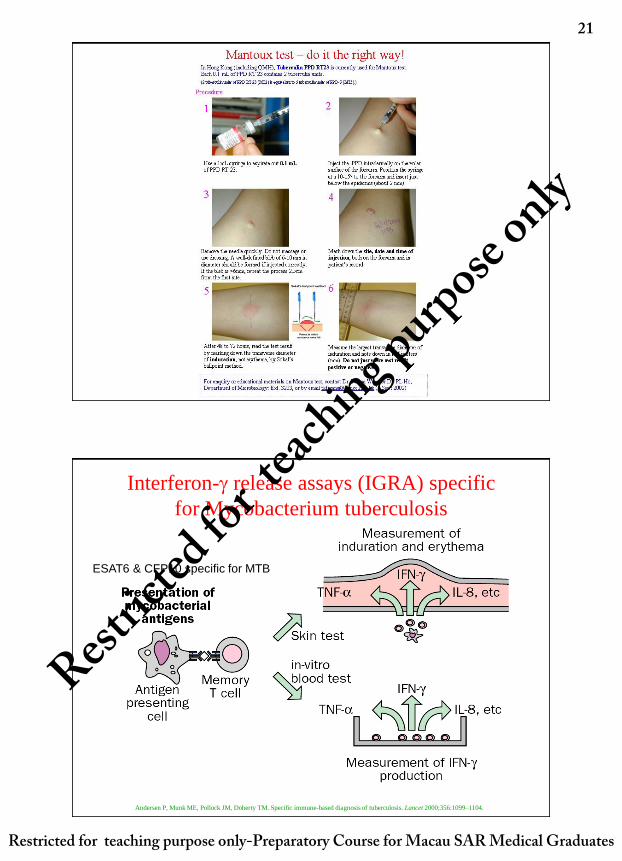
Andersen P, Munk ME, Pollock JM, Doherty TM. Specific immune-based diagnosis of tuberculosis. Lancet 2000;356:1099–1104.
Interferon- release assays (IGRA) specific
for Mycobacterium tuberculosis
ESAT6 & CFP10 specific for MTB
Restric
ted fo
r teac
hing purpose only
21
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
22
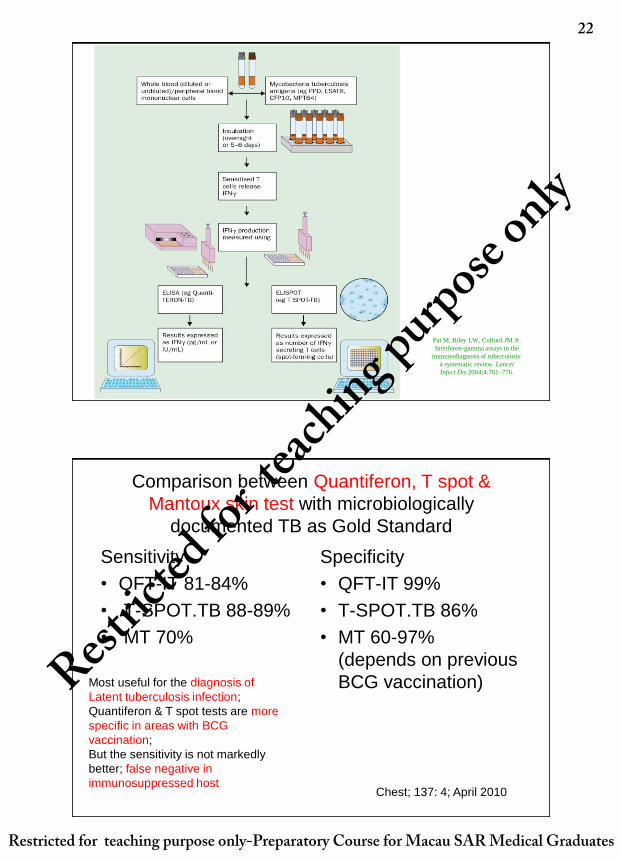
Pai M, Riley LW, Colford JM Jr.
Interferon-gamma assays in the
immunodiagnosis of tuberculosis:
a systematic review. Lancet
Infect Dis 2004;4:761–776.
Sensitivity
• QFT-IT 81-84%
• T-SPOT.TB 88-89%
• MT 70%
Specificity
• QFT-IT 99%
• T-SPOT.TB 86%
• MT 60-97%
(depends on previous
BCG vaccination)
Chest; 137: 4; April 2010
Most useful for the diagnosis of
Latent tuberculosis infection;
Quantiferon & T spot tests are more
specific in areas with BCG
vaccination;
But the sensitivity is not markedly
better; false negative in
immunosuppressed host
Comparison between Quantiferon, T spot &
Mantoux skin test with microbiologically
documented TB as Gold Standard
Restric
ted fo
r teac
hing purpose only
22
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates

11/25/2011
23
Thank you
Current evidence: ELISPOT vs
TST • Diagnosis of active TB More sensitive
(healthy and HIV+,
children and adult)
• Diagnosis of LTBI More sensitive and specific
• Contact tracing Stronger correlation with
exposure
• Prior BCG vaccination Minimal effect
Restric
ted fo
r teac
hing purpose only
23
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates
11/25/2011
24
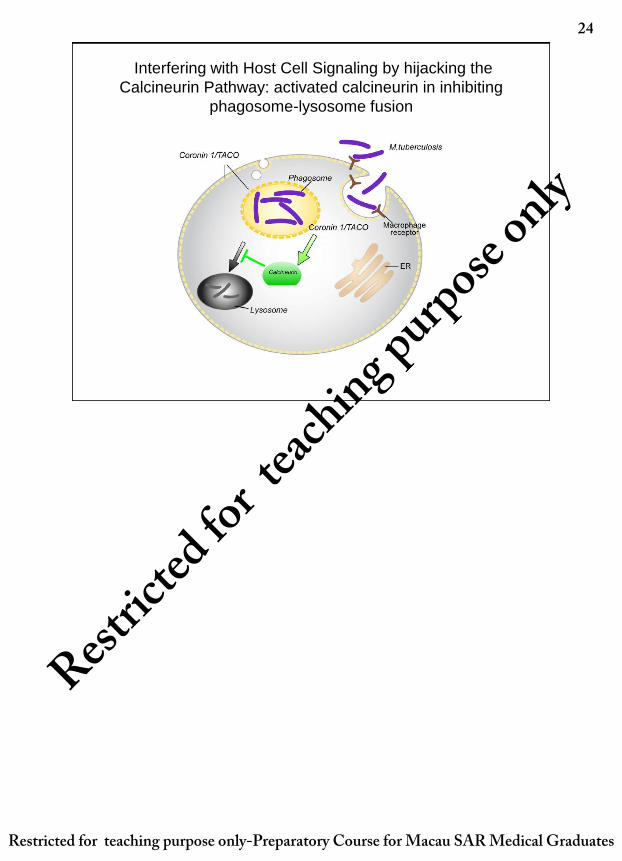
Interfering with Host Cell Signaling by hijacking the
Calcineurin Pathway: activated calcineurin in inhibiting
phagosome-lysosome fusion
Restric
ted fo
r teac
hing purpose only
24
Restricted for teaching purpose only-Preparatory Course for Macau SAR Medical Graduates