
Management of pancreatic cancer: a case report Giovanni Brandi Institute of Hematology end Medical...
49
Management of pancreatic Management of pancreatic cancer: a case report cancer: a case report Giovanni Brandi Giovanni Brandi Institute of Hematology end Medical Oncology “L e A Seràgnoli” Bologna University
-
Upload
silvester-douglas -
Category
Documents
-
view
216 -
download
0
Transcript of Management of pancreatic cancer: a case report Giovanni Brandi Institute of Hematology end Medical...

Management of Management of pancreatic cancer: a case pancreatic cancer: a case
reportreport
Giovanni BrandiGiovanni Brandi
Institute of Hematology end Medical Oncology “L e A Seràgnoli”
Bologna University

The patient
Male, 68 year-old
Presentation with epigastric pain by 2
months
Negative the abdominal and thoraco-
pulmonary objectivity
X-ray of the abdomen: negative
X-ray of the chest: negative

Nonhomogeneus pancreatic nodular Nonhomogeneus pancreatic nodular areaarea
Abdomen computed tomographyAbdomen computed tomography

Serum markers Serum markers levellevel
CEA = 3.4
Ca 19.9 = 0
Within the normal rangeWithin the normal range

Carbohydrate antigen 19.9
Recognized by a monoclonal antibody
targeting a sialylated Lewis A blood
group antigen epitope
5-10 % of people lack
fucosyltransferase and do not
synthesize the antigen
CEACEA
SMALL CANCERSMALL CANCER
VIRAGGIO P. C. IN CA
VIRAGGIO P. C. IN CA
Low SensitivityLow Sensitivity
MASAFUMI IKEDA, AMERICAN CANCER SOCIETY 2001MASAFUMI IKEDA, AMERICAN CANCER SOCIETY 2001
CA 19.9CA 19.9
PANCREATIC CARCINOMAPANCREATIC CARCINOMAPANCREATIC CARCINOMAPANCREATIC CARCINOMA
Negative (4-15 % of population)
Negative (4-15 % of population)
>CA 19.9
CA 19.9
Small Cancer
Only in the 50% of cases
Small Cancer
Only in the 50% of cases
Lewis Blood Group Antigen

CA19-9CA19-9 determined 72/78 (92.3%)
CA19-9 ≤ 37 U/μL 26/72 (36.1%)CA19-9 > 37 U/ μ L 46/72 (63.9%)
In 50 patients with histology/cytology:Sensitivity* 27/47 (57.4%)Specificity 0/3 (0%)VP + 27/30 (90.0%)VP - 0/20 (0%)
* 42 patients with pancreatic cancer and 5 with biliary tract cancer

Carbohydrate antigen Carbohydrate antigen 19.919.9
ASCO Guidelines 2006

Pancreatic Masses
Abscess
Acute autoimmune pancreatitis
Pseudocyst
Cyst
Tumor
…
AdenocarcinomaCystic tumorNeuroendocrine tumorSoft tissue sarcomaMetastases

Select between
Biopsy MRI
FDG-PET CEUS
What is the next step?15 $1 MILLION14 $500.00013 $250.00012 $100.00011 $50.00010 $25.0009 $16.0008 $8.0007 $4.0006 $2.0005 $1.0005 $1.0004 $5003 $3002 $2001 $100

Biopsy of pancreatic noduleBiopsy of pancreatic nodule
Adenocarcinoma
Surgical intervention ?

Vascular involvementVascular involvement
Radiological stagingRadiological stagingRadiological stagingRadiological staging
Portal vein
Superior mesenteric vein
Superior mesenteric artery
Celiac tripode

GRADE O: no vascular involvement
GRADE O: no vascular involvement

GRADE 1: disappear of
adipous resection plane
GRADE 1: disappear of
adipous resection plane

GRADE 2: circumferential infiltration < 2/3 of the vessel
lumen
GRADE 2: circumferential infiltration < 2/3 of the vessel
lumen

GRADE 3:≥ 2/3
circumferential infiltration
GRADE 3:≥ 2/3
circumferential infiltrationDong IL Park, J. Kyun LeeJ CLIN GASTROENT. 2001Dong IL Park, J. Kyun LeeJ CLIN GASTROENT. 2001
T.Hough,V. Raptopoulos AJR 1999
T.Hough,V. Raptopoulos AJR 1999
TEARDROPTEARDROP
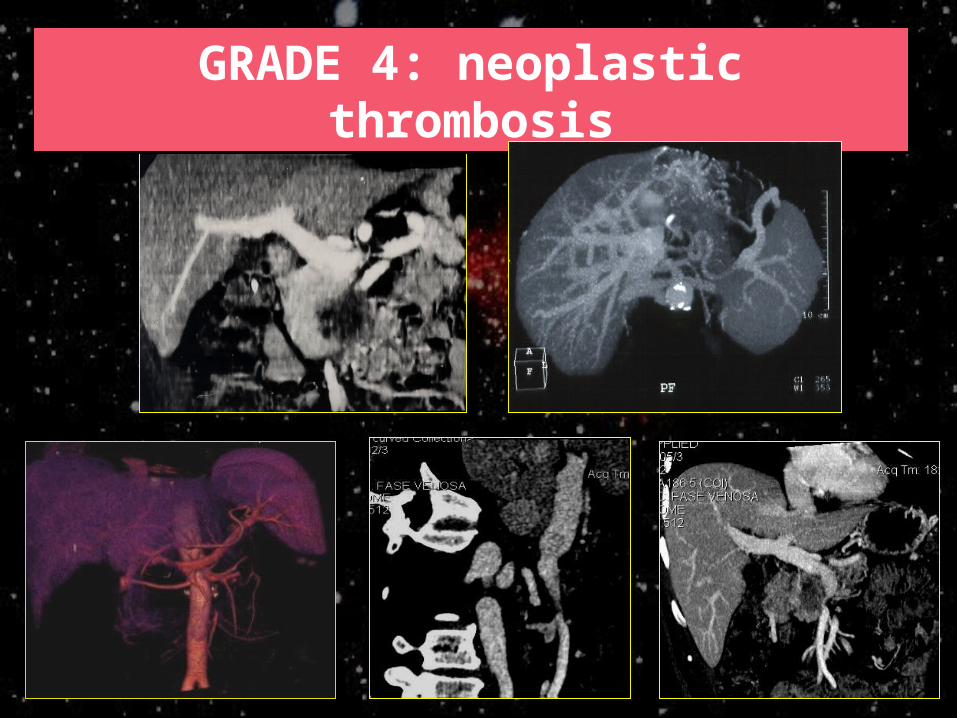
GRADE 4: neoplastic thrombosis
GRADE 4: neoplastic thrombosis

Criterion for surgical
intervention
Criterion for surgical
intervention
Pancreatic cancer

No arterial (hepatic or superior mesenteric)
infiltration
No arterial (hepatic or superior mesenteric)
infiltration

Nodistant metastases

No peritoneal involvementNo peritoneal involvement
Filmsy peri-hepatic ascites: suspicion of peritoneal involvement

Should we perform extended Should we perform extended pancreatic resection ?pancreatic resection ?
Total pancreatectomy

Extended lymph node dissection

Venous resectionVenous resection
No prospective randomized trials comparing pancreatectomy with and without VnR.
Morbidity and mortality with and without VnR are similar. No study dimostrated that Vnr increase R0 resection
rate. Despite great diversity in OS, pooling results of 23
studies showed that addition of VnR did not provide longer 5-years OS, with 3 studies noting shorter survival after VnR.
Rationales for vein resection (VnR)
*tumor invasion of vessels or infiammatory adhesions that preclude adequate separation from tumor to veins
*gain benefits for extended pancreasectomy

Arterial resectionArterial resectionMesenteric, celiac and hepatic arteries
resection are more rarely performed compared with VnR
Long term survival is lower with combined VnR and arterial resection compared with VnR alone (2y OS 0% vs 17%; p<0,02. Nakao WJS 2006)
Long term survival is similar between patients treated with arterial resection and patients completly unresected. (Nakao WJS 2006) SRINEVAS K.
Extended Resection for Pancreatic Adenocarcinoma.Oncologist 2007
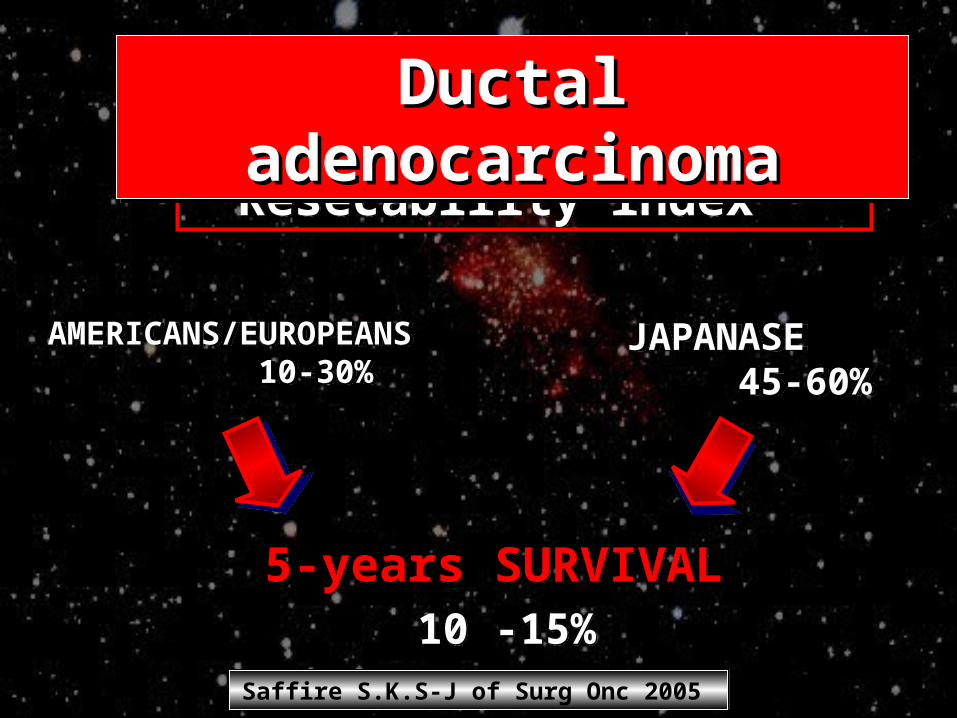
Resecability index Resecability index
AMERICANS/EUROPEANS 10-30% AMERICANS/EUROPEANS 10-30%
JAPANASE 45-60% JAPANASE 45-60%
5-years SURVIVAL 10 -15%
5-years SURVIVAL 10 -15%
Ductal Ductal adenocarcinomaadenocarcinoma
Ductal Ductal adenocarcinomaadenocarcinoma
Saffire S.K.S-J of Surg Onc 2005 Saffire S.K.S-J of Surg Onc 2005

Surgical intervention
Resection of tail and body of pancreas with Resection of tail and body of pancreas with splenectomy and lymphadenectomysplenectomy and lymphadenectomy

Pathologist response
Moderately differentiated
adenocarcinoma associated with a neuroendocrine
neoplastic component
immunoreactive for insuline, glucagon and somatostatin.
Resection border infiltrated by the neoplasm

Post-operative analysis
CEA = 2.9Ca 19.9 = 0
For error we measured the -fetoprotein level
2259 ng/mL (normal value < 10 ng/mL)

-fetoprotein
Glycoprotein of 65 kd molecular
weight
Serum marker of hepatocellular
carcinoma
Serum marker of germ line
tumors
Rarely described in pancreatic
cancer

Pancreatic cancer with high level of
-fetoprotein
Kawamoto ‘92; McIntire ’75; Lokich ’87; Scheithauer ’89; Kubo ’74; Tomada ’74Ikida ’77; Nagamine ’78; Nagata ’80; Katoh ’81; Inui ’83; Ono ’84; Harnazoe ‘87
N of cases
AgeFP
(ng/mL)Range
Liver mets
Histology
29 28-78
42
65000
22 Yes
13 adenocarcinoma
6 insular carcinoma
3 acinar carcinoma
7 No
2 ductal carcinoma
2 undifferentiated
1 unknown

Select between
Occult HCC Hard discount ELISA kit
Common neoplastic precursor with
transdifferentiation ability
Drunk laboratorist
Pancreatic cancer esocrine/endocrine with
hepatoid behaviour?Hypotesis:
15 $1 MILLION14 $500.00013 $250.00012 $100.00012 $100.00011 $50.00010 $25.0009 $16.0008 $8.0007 $4.0006 $2.0005 $1.0004 $5003 $3002 $2001 $100

HypotesisA. HCC escluded by hepatic US and CT
Hepatic nodules was signaled 7 months after surgeryreasonably indicating their secondary nature
The patient did not have any risk factors forhepatocellular carcinoma

Hypotesis
C. Supported by: _Peters J. Ontogeny, differentiation and Growth of the endocrine pancreas. Wirchows
Arch. 2000.
_Yang YH. The relation of pancreatic ducts to the islets of Langerhans; study of three
cases. AMA Arch Pathol. 1959 _Pour PM. What is the origin of pancreatic
adenocarcinoma ? Mol Cancer. 2003

An islet in theAn islet in thevicinity of a well-differentiated vicinity of a well-differentiated
adenocarcinoma containing large atypical adenocarcinoma containing large atypical cells intermingled with intact islet cells.cells intermingled with intact islet cells.
Pour PM.Mol Cancer. 2003

Pathologist analysis
Strong and diffuse
immunoreactivity for
-fetoprotein.

Pathologist response
Focal reactivity for albumin mRNA on
in-situhybridization

Select between
Observation Chemotherapy
Chemoradiation Radiotherapy
Anything else to improve the patient’s
outcome?
15 $1 MILLION14 $500.00013 $250.00013 $250.00012 $100.00011 $50.00010 $25.0009 $16.0008 $8.0007 $4.0006 $2.0005 $1.0004 $5003 $3002 $2001 $100

Adjuvant treatment ?
Wolff et all. JAMA 2008
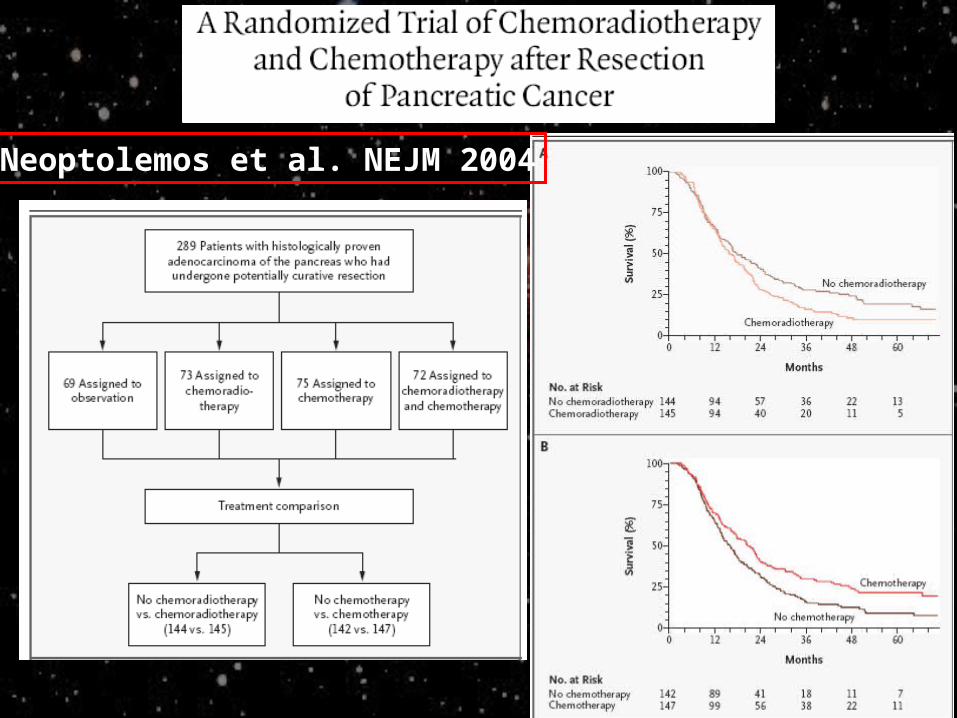
Neoptolemos et al. NEJM 2004

Oettle H. JAMA 2007
Adjuvant treatment: the CONKO-001
DFS OS
Adjuvant treatment
External radiotherapy on pancreatic region
(total dose of 4140 cGy)
Followed by
10 infusion of gemcitabine (1000 mg/m² weekly)
Revaluation 1 lesion of 3 cm of diameter in the
gastric curves 1 lesion of 1 cm of diameter in the
fourth hepatic segment 1 lesion of 1 cm of diameter in the
caudal lobe
Abdomen CTAbdomen CT
PetPet Confirm of the CT’s findings
Markers CEA and Ca 19.9 within the normal rangeFP > 7000 ng/ml
What about the What about the neuroendocrineneuroendocrine component ? component ?

Octreoscan® was performed to evaluate the possibility of treatment with somatostatine’s analogues
No expression of somatostatin’s receptors
Somatostatin’s receptors

10 further infusion of gemcitabine due 10 further infusion of gemcitabine due to a clinical benefitto a clinical benefit
But..But..
3 months after a CT found progression of the disease
Meanwhile, clinical condition gradually worsenedwith signs and symptoms of hepatic failure

Treatment was modified:Gemcitabine 1500 mg/m²
+5-fluorouracil 600mg/m² on day 1, 8
and 15
(repeated every 28 days)

In the end…Chemotherapy was interrupted 6
months later due to a clinical progression of the disease
Support therapy was performed at home because of worsening clinical
conditionThe patient died 1 month later, 1 year after the surgery

Brandi G. Pancreas 2008Exocrine/endocrine pancreatic cancer and -fetoprotein.


















