
Malignant oesophageal strictures: a review of … paper is concerned primarily with the technology...
8
Br. J. Surg. Vol. 69 (1982) 61-68 Printed in Great Britain Proffered review Malignant oesophageal strictures: a review of techniques for palliative intubation RICHARD EARLAM AND J. R.CUNHA-MELO The London Hospital, Whitechapel, London El IBB. A review of the different designs for palliative oesophageal intubation tubes confirms Souttar's original suggestion that they should be flexible, incompressible, non-traumatic, compact, have an adequate lumen and stay in place. The internal diameter should be at least 10mm. The thickness of the wall should be about 1 mm. The length will vary according to the stricture and should be as short as possible, provided that the proximal rim prevents future longitudinal growth occluding the lumen. Various methods of achieving the ability to stay in place are described, which comprise either a large proximal rim or a roughened barrel. No details about results are given because the original patient populations vary so much. Success probably depends more on the technical expertise and experience of the surgeon than specific variations in design. Dysphagia is the leading symptom in oesophageal cancer and its relief must be the main aim of treatment. Approximately 60 per cent of all patients with squamous cell carcinoma of the oesophagus have extensive tumours that cannot be resected (1,2). In one large series, 45 per cent had intubation because they were unsuitable for surgery (3), but even after surgical resection about 20 per cent will have further dysphagia either due to recurrence or a stricture at the site of the anastomosis (4, 5). Similarly, radiotherapy is followed by dysphagia in over 25 per cent, usually caused by a fibrotic cicatricial narrowing rather than local recurrence (6). The treatment of dysphagia by oesophageal dilatation is essentially similar to that for a benign stricture but with additional complications due to the nature of the malignant process. The minimal requirement is for the patient to swallow his own saliva and since this is often thick he will easily swallow clear liquids through such a lumen. Patients can survive on modern clear fluids such as Vivonex, Amicalorin, Aminutrin or Clinifeed for months. Any large lumen will enable more solid food to be taken. There is a mistaken idea that normality is the perfection that should always be achieved. The average length of time with symptoms prior to diagnosis is over 6 months (1,7) and perhaps some patients are not really worried by some trouble swallowing food. Each patient has his threshold for what suits him and many are happy if they can settle down with their spouse to the same food, provided it is minced or mashed and they can eat slowly in their own time. A recent study has confirmed that over 50 per cent of patients with oesophageal cancer die in hospital (8). If treatment cannot achieve a radical cure then surely it should enable the patient to die at home if he and the relatives so wish under the care of his family doctor who can treat all his other difficulties symptomatically but relies on the surgeon to deal with the mechanical problems of stenosis or fistula. In the past 25 years there has been more interest in the subject of palliative intubation. Numerous tubes have been described and their sizes, materials and special properties are listed in Table I. Presently available ones may be suitable or new tubes require invention, but what may be lacking is the experience in using them. This paper is concerned primarily with the technology of intubation. Indications for palliation, which are closely connected with non-resectability, are not discussed; nor are the results included, because they vary so much with the patient population and details are given in the individual papers ciled in Ihe text. Optimal diameter of the oesophageal lumen Every individual has a different optimal diameter for an oesophageal stricture because it depends on the actual nature of the obstruction, its degree of elasticity, length, the power of the muscle pushing the bolus through as well as the patient's threshold for tolerating discomfort on swallowing. It is not possible to be dogmatic, therefore, about the minimal diameter to be achieved by dilatation, but it is the authors' aim with malignant strictures to achieve dilatation to at least 10mm diameter or 30 FG. Using modern techniques, this can almost always be achieved with repeated dilatations so there is no reason to accept a smaller diameter. The internal diameter of most palliative tubes lies between 10 and 12mm, with only a few being 14 or 15mm. Larger tubes are not used because a stricture which can be dilated to more than 15 mm diameter or 45 FG does not need an indwelling tube. The only justification for inserting a tube with a large lumen is to block off a fistula unaccompanied by narrowing of the oesophagus. A tube will maintain a given lumen but there are several methods other than simple dilatation to achieve this. They are all based on the fact that most oesophageal tumours are proliferative and the tumour itself encroaches on the lumen to narrow it, frequently leaving the muscle walls themselves widely separated. Radiotherapy gradually causes necrosis of the tumour and then the act of swallowing removes the dead tissue. Occasionally, radiotherapy gives no relief because patients have had a complete oesophageal block prior to the start of the course. In such a case, dilatation or reaming out the lumen will enable the scouring process to begin. Barlow's borer (9) or reamer (see Fig. 1) is the only instrument specially designed for this. Heat provided by diathermy (10) and extreme cold from cryosurgical probes have also been used (11). None of these particular methods changes the natural history of the disease but does achieve symptomatic relief. Historical aspects The great advances of the past century in palliative intubation were made in the 1880s. There were several case reports of catheters being passed enabling a patient to obtain nutrition and survive for a few months (12-16). Sir Charles Symonds is usually cited as the first to use an indwelling tube rather than a catheter in 1885 (17,18). This relied for its fixation on strings emerging through the nostrils and tied behind the ears but in another method it was attached to the moustache, if available. In 1845 a French surgeon Leroy d'Etoilles had used a short
Transcript of Malignant oesophageal strictures: a review of … paper is concerned primarily with the technology...

Br. J. Surg. Vol. 69 (1982) 61-68 Printed in Great Britain
Proffered review
Malignant oesophageal strictures:a review of techniques forpalliative intubation
RICHARD EARLAM ANDJ. R.CUNHA-MELO
The London Hospital, Whitechapel, LondonEl IBB.
A review of the different designs for palliative oesophageal intubationtubes confirms Souttar's original suggestion that they should beflexible, incompressible, non-traumatic, compact, have an adequatelumen and stay in place. The internal diameter should be at least10mm. The thickness of the wall should be about 1 mm. The lengthwill vary according to the stricture and should be as short as possible,provided that the proximal rim prevents future longitudinal growthoccluding the lumen. Various methods of achieving the ability to stayin place are described, which comprise either a large proximal rim ora roughened barrel. No details about results are given because theoriginal patient populations vary so much. Success probably dependsmore on the technical expertise and experience of the surgeon thanspecific variations in design.
Dysphagia is the leading symptom in oesophageal cancer andits relief must be the main aim of treatment. Approximately 60per cent of all patients with squamous cell carcinoma of theoesophagus have extensive tumours that cannot be resected(1,2). In one large series, 45 per cent had intubation becausethey were unsuitable for surgery (3), but even after surgicalresection about 20 per cent will have further dysphagia eitherdue to recurrence or a stricture at the site of the anastomosis(4, 5). Similarly, radiotherapy is followed by dysphagia in over25 per cent, usually caused by a fibrotic cicatricial narrowingrather than local recurrence (6). The treatment of dysphagia byoesophageal dilatation is essentially similar to that for a benignstricture but with additional complications due to the nature ofthe malignant process. The minimal requirement is for thepatient to swallow his own saliva and since this is often thick hewill easily swallow clear liquids through such a lumen. Patientscan survive on modern clear fluids such as Vivonex,Amicalorin, Aminutrin or Clinifeed for months. Any largelumen will enable more solid food to be taken. There is amistaken idea that normality is the perfection that shouldalways be achieved. The average length of time with symptomsprior to diagnosis is over 6 months (1,7) and perhaps somepatients are not really worried by some trouble swallowingfood. Each patient has his threshold for what suits him andmany are happy if they can settle down with their spouse to thesame food, provided it is minced or mashed and they can eatslowly in their own time.
A recent study has confirmed that over 50 per cent of patientswith oesophageal cancer die in hospital (8). If treatment cannotachieve a radical cure then surely it should enable the patient todie at home if he and the relatives so wish under the care of hisfamily doctor who can treat all his other difficultiessymptomatically but relies on the surgeon to deal with themechanical problems of stenosis or fistula.
In the past 25 years there has been more interest in thesubject of palliative intubation. Numerous tubes have beendescribed and their sizes, materials and special properties arelisted in Table I. Presently available ones may be suitable ornew tubes require invention, but what may be lacking is theexperience in using them. This paper is concerned primarilywith the technology of intubation. Indications for palliation,which are closely connected with non-resectability, are notdiscussed; nor are the results included, because they vary somuch with the patient population and details are given in theindividual papers ciled in Ihe text.
Optimal diameter of the oesophageal lumenEvery individual has a different optimal diameter for anoesophageal stricture because it depends on the actual natureof the obstruction, its degree of elasticity, length, the power ofthe muscle pushing the bolus through as well as the patient'sthreshold for tolerating discomfort on swallowing. It is notpossible to be dogmatic, therefore, about the minimal diameterto be achieved by dilatation, but it is the authors' aim withmalignant strictures to achieve dilatation to at least 10mmdiameter or 30 FG. Using modern techniques, this can almostalways be achieved with repeated dilatations so there is noreason to accept a smaller diameter. The internal diameter ofmost palliative tubes lies between 10 and 12mm, with only afew being 14 or 15mm. Larger tubes are not used because astricture which can be dilated to more than 15 mm diameter or45 FG does not need an indwelling tube. The only justificationfor inserting a tube with a large lumen is to block off a fistulaunaccompanied by narrowing of the oesophagus.
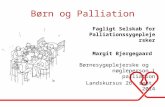
A tube will maintain a given lumen but there are severalmethods other than simple dilatation to achieve this. They areall based on the fact that most oesophageal tumours areproliferative and the tumour itself encroaches on the lumen tonarrow it, frequently leaving the muscle walls themselveswidely separated. Radiotherapy gradually causes necrosis ofthe tumour and then the act of swallowing removes the deadtissue. Occasionally, radiotherapy gives no relief becausepatients have had a complete oesophageal block prior to thestart of the course. In such a case, dilatation or reaming out thelumen will enable the scouring process to begin. Barlow's borer(9) or reamer (see Fig. 1) is the only instrument speciallydesigned for this. Heat provided by diathermy (10) and extremecold from cryosurgical probes have also been used (11). Noneof these particular methods changes the natural history of thedisease but does achieve symptomatic relief.
Historical aspectsThe great advances of the past century in palliative intubationwere made in the 1880s. There were several case reports ofcatheters being passed enabling a patient to obtain nutritionand survive for a few months (12-16). Sir Charles Symonds isusually cited as the first to use an indwelling tube rather than acatheter in 1885 (17,18). This relied for its fixation on stringsemerging through the nostrils and tied behind the ears but inanother method it was attached to the moustache, if available.In 1845 a French surgeon Leroy d'Etoilles had used a short

62 R. Earlam and J. R. Cunha-Melo
ATKINSON Keymed
CELESTIN simple
CELESTIN flange
COLLIS
COYAS
DIDCOTT
HOLINGER
MOUSSEAU-BARBIN
PALMER
PROCTER-LIVINGSTONE
SACHS
SOUTTAR
STIRNEMANN
TYTGAT (a)
MACKLER TYTGAT (b)

Malignant oesophageal strictures 63
BARLOW'S BORER
GOTTSTEIN
Fig. 1. Various designs for palliative oesophageal intubation tubes.
tube of decalcified ivory (19). Symond's tube was made ofboxwood and ivory. Although oesophagoscopy had alreadybeen developed, by Kussmaul (20) and Mikulicz (21), tubeswere placed blindly at this time. In 1901 Gottstein (22)developed a short rubber tube with an inverted funnel top and arim distally which did not require strings for fixation (see Fig.1). This was developed later by Guisez (22,23), who used a tubewith a de Pezzer catheter type of end (see Fig. 1). In his articlethere is an illustration of a small tube of earlier design held inplace by strings. The Mosher plug was another method (24).The honour for developing an indwelling palliative tube withno external fixation must go to Gottstein in 1901; previousattempts had succeeded in isolated cases but his tubes were ofmore practical use.
In 1924 the next progress was made by Sir Henry Souttarwho developed a tube based on the design of a spring and heldin place by the roughness of its exterior and a proximal lip (25).Souttar was an engineering student at Oxford before becominga surgeon at the London Hospital so his knowledge of theaccurate measurement needed helped him in producing thistube. It was originally made of German silver covered with goldplating. The secondary spiral in the spring appeared later(26,27) and, in the Souttar tube modified by Professor LeighCollis, was lost (28). These tubes were all smaller than thelumen of the rigid oesophagascopes available and were insertedunder direct vision through the oesophagoscope and notblindly.
For the next 30 years there was no great interest in palliativeintubation. It was, however, apparent that there was a demandfor a tube that could be pulled downwards through anobstruction in the oesophagus, cardia or upper stomach,whereas the Souttar tube was only suitable for pushing fromabove. The Mousseau-Barbin tube was the first of this type tobe designed in 1956 with a long leading catheter end (29). In1959 this was developed by Celestin and later manufactured inlatex rubber rather than plastic (30-32). In an article dated1974 (33), detailing the methods and attempting to assess thebest tube available, there were only 2459 patients described inthe literature between 1960 and 1971, which is not manyconsidering that the need for palliation is so high. Exceptions tothis were two large series described by O'Connor (34) andMounler-Kuhn (35). Recently, there has been a change ofemphasis and Procter has described his own personalexperience in over 2000 patients (36).
Although most tubes can be divided into either push or pulltypes, there has recently been a solution to the problem of howto 'push a piece of string'. The Celestin tube, which wasoriginally designed for the pull method, was first actuallypushed in 1974 (37) and now a commercially available methodhas been developed by Atkinson (38-40) and called theNottingham introducer (see Fig. 1).
Throughout the years, attempts have been made to excise aportion of the oesophagus and bridge the gap with a prosthesis.Experimentally, this was achieved in dogs (41) and then the
GUISEZ
NOTTINGHAM INTRODUCER
same technique was applied to one patient (42). Replacement ofa segment of the thoracic oesophagus has been attempted but isnot accepted as a practical procedure because of the danger ofmediastinal leaks (43). Replacement of portions of the cervicaloesophagus, after pharyngolaryngectomy, is more successful(44-46).
The majority of indwelling tubes that had an opening to theexterior were brought out through the nostril but attempts havebeen made to ease the patient's discomfort by bringing themout through the cervical oesophagus below the cricopharyngealsphincter (47-51) or above through the pyriform fossa (52).
Technical aspectsMaterial: The different materials and their properties aresummarized in Table II. The majority of the new tubes areplastic. The essential properties of flexibility andincompressibility which can be provided by the old materials ofreinforced rubber or a stainless steel spring have not beenimproved by the modern ones. Even with plastic there is acertain thickness below which the tube is too easily compressed.Internal diameter: The majority of the tubes have an internaldiameter between 10 and 12 mm. Those with the figure 12-5 mmmerely reflect a conversion of the imperial measurement of halfan inch to metric size. American plastic tubing comes in suchmeasurements (53,54). Historically, Chevalier Jacksonconsidered that half an inch (12-5 mm or 39 FG) was sufficientdiameter for dilatation of a stricture to enable swallowing to beimproved.Wall: The thickness depends on the material used. Technically,it is difficult to obtain a thickness ofless than 1 mm. The thickerthe wall, the greater the outside diameter becomes andobviously this should be minimized.Outside diameter: From Table I it will be seen that the majorityhave an external diameter of between 14 and 17 mm. Some havea measurement of 18mm, which is 54 FG. This is probably anunacceptably large size because dilatation to such a diameterrelieves dysphagia in the majority of patients. A size of 15mmor 45 FG seems to be the maximum acceptable. For any givenoutside diameter the largest lumen is provided by those with thethinnest walls such as the Goni, Mousseau-Barbin, Sachs andSouttar tubes.Proximal end: The majority of tubes depend on the size of theproximal end (Fig. 2) to prevent them slipping downwards intothe stomach. Some have a thin collar, 1-2 mm wider indiameter than the barrel, but this is too small a limit for safetybecause it loosens due to movement and pressure necrosis. Aproximal end that is much wider serves the two purposes of (a)preventing distal displacement and (h) directing the bolus into anarrowing. The shapes can be subdivided as follows: collar(Souttar), funnel (Palmer), cup (Mousseau-Barbin and Palmer)and tulip (Celestin).
The tulip shape was developed to prevent the rimintussuscepting if floppy or causing pressure necrosis if it weremore firm. If the soft end, when compressed, is still too rigid,

R. Earlam and J. R. Cunha-Melo
Table I: PALLIATIVE TUBES
Author
Atkinson
Celestin
Collis
Coyas
Didcott
FellGoni
Gourevitch
Haring
Holinger
Mackler
Mousseau-Barbin
Palmer
Procter-Livingstone
Sachs
Souttar
Stirnemann
Tytgat
Weisel
Year
1978
1959
1971
1955
1973
19661964
1959
1964
1955
1954
1956
1970
1968
1959
1924
1965
1976
1959
Reference Method
(38-40) Push
(30-32) LaparotomyPullPush
(28) Push
(61,84) Push
(82-84) Push
(85) Pull(86, 87) Pull
^
(88) Pull
(58, 89) Pull
(59) Push
(90) Thoracotomy
(29,91) Pull
(53,55, Push92-94)
(36,95-98) Push
(66) Push
(7,25-27) Push
(99,100) Pull
(54,65) Push
(101,102) Push
Material
Silastic rubber
Originallypolyethylenethen latexrubber withnylonreinforcedspiral
Stainless steel
Polyvinyl
Stainless steelwire embeddedin rubber
PolyvinylPolyethylene
Armoured latexrubber
Latex rubberreinforcedwith stainlesssteel
Polyvinyl
Polyvinyl
Neoplex
TygonR8420
Latex rubberarmoured withmonofilamentnylon
Nylon
Gold platedGerman silver
Porflex
Tygon R3693Tygon R8420
Polyethylene
ID OD Wall Length(mm) (mm) (mm) (cm)
11 15 2 14
12 15 1-5 34
11 13 1 7
10 14 2 13
1 6 ? ? 9111519
10 14 2 4015 17 1 40
? ? ? 16
13 17 2 9,12,18
7-10 ? ? 7-12
? 9-12 ? ?
10 12 1 30 + 7014 16
12-5 15-7 1-6 Any
12 18 3 10,15,19
8 10 1 ?
A 8 10 1 5-20B I O 12C12 14
11 14 1-5 ?
12-5 15-7 1-6 8-35
10 13 1-5 10-25
Comments
Funnel top (29 mm) withnon-return flange
Proximal end tulip-shaped (28 mm) distalend tapered but canbe cut or trimmed,later distal flange
}
Similar to Souttarbut stainless steeland no spiral in thebody
Proximal collarprojecting 1-5 mmwith metallic ringfor radiology, bodyhas multiple rings
Self expanding, whencompressed itelongates andnarrows for ease ofinsertion
Proximal end 3 mmrim (23mmOD),distal end duck-billed
Proximal end funnel-shaped distal endbevelled
Proximal end soft funnel
Both ends mushroom-shaped de Pezzer cathetershape
Proximal end funnel-shaped, inserted afteropening oesophagusthrough a thoracotomy
Proximal end floppyfunnel (24mm OD),distal end can betrimmed
Heated plasticmoulded to funnelshape
Proximal end fish-mouthed 3-0x2-5 cm,distal end also fish-mouthed
Format of a hollow screwthat is actuallyscrewed into place,proximal end two notches
Held in place byproximal lip, roughexterior and spiralbody
Proximal end funnel-shaped and distal endreversed funnel
Transparent plasticwith two radioopaque rings, can bepushed in place overflexible fibrescopeproximal end diameter25 mm. One type hasa spiral ring barrel.
Flanged proximal endwith bevelled distalend
-

Malignant oesophageal strictures
PROXIMAL ENDS
65
collar funnel cup tulip
Fig. 2. Proximal ends of tubes.
the rim will form angles at both sides which may perforate theoesophageal wall. For this reason Procter (36) developed thefish-mouthed end to avoid this (see Fig. 1). When atube is made of polyethylene or polyvinyl chloride the end. canbe heated and formed as a funnel, or indeed any shape which isthen maintained at body temperature (55,56). A floppyproximal end such as the Celestin tube can be compressed to asmaller size during insertion. The cricopharyngeal sphincterlimits the size of the proximal end. Although it presents as atransverse slit, it can be dilated up to 75 FG, but it will notusually take instruments of one inch diameter (23-9 mmdiameter is equivalent to 75 FG). One inch diameter isequivalent to 24-5 mm or 78 FG, if the conversion uses n as3-142 rather than 3-0. At smaller diameters this difference forthe value of re does not matter for all practical purposes, but itis essential for a surgeon to know whether his tubes and dilatorsare measured accurately and with what conversion factor. Inthe past much trouble occurred because dilatation wasmeasured in inches and their fractions but tubes were insertedin metric sizes or vice versa.
Too large a proximal end is cumbersome during insertionand may cause pressure necrosis in situ. It must be rememberedthat the oesophagus is normally collapsed with a negativeintraluminal pressure. These problems are exacerbated withintubation of the cervical oesophagus. Here, there is very littlespace between vertebrae and the trachea and it is essential alsofor the length of the proximal end to be so short that it does notimpinge on the cricopharyngeal sphincter. Tubes of a smaller
Table II: MATERIALS
Material Author
Boxwood and ivoryGerman silver, an
alloy of brass andnickel
IvoryLatex rubber
NcoplcxNylonPolyethylene PE 410Polyvinyl chloride
(PVC)
Portex
ResinylSilicon rubberSolid silverStainless steel
Tygon R84203693
Symonds (17,18)Souttar (25-27)
Etoilles(19)Celestin (32)Procter-Livingstone
(36,95)Mousseau (29)Sachs (66)Carter (56)Clauss (103)Coyas (81)Dubois(104)Fell (85)Greening (105)Grewe (106)Heimlich (50)Holinger (59)Mackler (90)O'Connor (34)Weisel (101)Zaslavsky (107)Hayes (108)Stirnemann (100)Kropff(109)Atkinson (40)Brown (110)Amman and Collis (28)Farlam (7)Palmer (53)Jager(65)Tytgat (54)
DISTAL ENDS
flush bevel fishmouth
Fig. 3. Distal ends of tubes.
f lapvalve
size with a narrow collar are to be preferred in this anatomicalsituation.Distal end: Most tubes have the distal end cut off at right anglesto the long axis (Fig. 3). Some have suggested an oblique end toenlarge the lumen at the exit. Another advantage proposed forthis is that compression of the end will not occur. The formeridea ignores the fact that the internal diameter of the barrel willlimit the flow and the latter the fact that the barrel should benon-compressible anyway.
Proximal dislodgement is a problem with some tubes. Distalcollars have been provided as with the original Guisez tube (seeFig. 1) (22) and others have an additional flange or end (57)some of which can be screwed on through the laparotomyincision (50, 58). A de Pezzer or mushroom-shaped end has alsobeen used (22, 59,60). Three designs presently available, byCelestin, Atkinson and Procter, have a distal flange or collar toprevent proximal movement.
Reflux back through the tube can be a problem if it traversesthe gastro-oesophageal junction. Flap valves (61), similar tothose provided in the Aldon bag (62), can prevent reflux (Fig. 3).Most surgeons will deal with this particular problem by adviceto go to bed with an empty stomach and to sleep propped up,similar to that given patients after an oesophagogastrectomy.Oesophagitis, due to gastric reflux proximal to the tube, doesoccur, is infrequent and rarely causes complications.Barrel: The majority are smooth. None is made of Teflonwhich has the lowest possible surface tension, but on thecontrary many rely on a rough external surface for fixationsuch as the Souttar tube, which is a spiral screw with 10 turnsper cm, pushed in rather than screwed in. The Souttar tube hasbeen modified by coating it with plastic to prevent tumourinfiltration (63), but this modification eliminates the roughnesswhich prevents the normal Souttar tube moving. The tubedesigned by Coyas (64) has multiple rings to prevent dislodge-ment, as does one described by Tytgat (54, 65). Two designshave a spiral superimposed upon the barrel, which is made ofplastic (65,66). The only tube with a deliberate continuousspiral specifically made for screwing into place is the one Sachsdescribed (see Fig. 1) (66).
Complications (36, 67)Bolus obstructionThis is often cited as the main contraindication to intubationbut it is rare. Some patients can swallow normal food withoutobservers being aware that they have a tube in situ. The patientshould aim to take the same diet as is cooked for othermembers of the household. Specifically, steaks and fresh breadmay cause trouble and should be avoided. Minced meat andtoast are less likely to stick. All patients should have their teethproperly looked after so that they can chew well. Bolusobstruction in the majority of instances will relieve itself byautodigestion and softening but if there is still total blockageafter 12-24 hours the patient should go to hospital. Meattenderizer or fresh pineapple juice have been suggested asmethods for the patient to clear the block himself. All theauthors' patients are given a letter describing the size and site ofthe tube inserted in case they attend a strange hospital or theirnotes cannot be found on admission. The first procedure is topass a large nasogastric tube to try and push the bolus through.If this fails, endoscopy is necessary. It is doubtful whether apreliminary Gastrografin radiological examination is helpful.

66
PerforationThe most dangerous complication is perforation. This maybe caused by making a false passage through the tumour orbelow, early during the process of dilatation, later as thepalliative tube is inserted or delayed due to pressure necrosis.The use of guide wires can help to reduce the incidence ofmaking a hole through the oesophageal wall and carefulattention to- the size of the lumen in relation to the outsidediameter of the tube reduces the risk of splitting the muscle.
Most tubes arc inserted over a guide rod as described withthe original Souttar tube (25). The modern ones can be guidedover a flexible fibrescope. If a Souttar tube is passed blindly it ishelpful to block the open distal end with a soluble device, eithera glycerine suppository acting like an obturator, as firstdescribed by Souttar, or a moulded toffee.
Tumours at the gastro-oesophageal junction are moredifficult to intubate because of the change in axis. Previouslythe pullthrough technique was used exclusively but it is possibleto push either a Celestin (38), a Souttar (68) or a Tytgat tube(65) from above provided that there is a guide wire or a bougiein place. Pulling a tube through a tumour via a gastrostomydoes not completely avoid perforation or a false passage. Itmay help to have a nasogastric tube, guide wire or thread (69)in situ first. Hegar's dilators are usually the most suitable forretrograde dilatation. Another technique of use with agastrostomy is gradual dilatation from above downwards usingthe 'endless-string' technique and passing increasing sizedbougies through the narrowing (70).
The earliest signs of perforation are pain, rising pulse rateand temperature, but exploration is not necessarily essential as'small leaks can be treated conservatively. The procedureshould be covered with preoperative antibiotics. Local pressuremay lead to perforation as a delayed phenomenon (71).Tracheal compression may be caused by a tube with a verylarge lip (72) but perforations caused apparently by pressuremay be part of the natural process of the disease and not due tothe inert material penetrating through local structures. Fistulasdue to necrosis may enter the trachea, bronchi or the lungs (73),aorta, other mediastinal vessels or the pericardium. If fluidenters the lung through a fistula, a palliative tube can beinserted to block off the hole and provide a preferentially largelumen for the bolus passing down the oesophagus. Coughingimmediately after swallowing, worse with liquids than solids,should be interpreted as a tracheo-oesophageal fistula andtreated as an emergency by intubation. If acute haemorrhageoccurs due to erosion of a large vessel it is doubtful whetheranything can or should be done. When air is seen in thepericardium, intubation is not helpful but it can persist forweeks before death.
Proximal displacementProximal displacement can occur with any palliative tube as aresult of too loose a tube being inserted or it not being jammedtightly enough against the upper edge of the tumour. It is asimple matter to re-insert a correct size of tube. Early diagnosisof this complication can be made by a comparison of thepostoperative X-ray with a preoperative film. It is essential tohave films of the tumour in relation to the whole chest or upperabdomen. These are obtained by radiotherapists so that the sizeand position of the growth can be measured for subsequentirradiation. They are also essential before inserting a tube sothat its appropriate length can be assessed, any curves or axisdeviation can be recognized and the correct position be easilyseen on a straight film after insertion. If this latter film is correctand the patient is swallowing normally there would appear tobe no advantage in postoperative barium or Gastrografinswallows.
Different designs have been developed to prevent tubesmoving upwards, which are either in the form of a de Pezzercatheter, a collar or a flange (Fig. 4). The tubes are designed toprevent proximal dislodgement; consequently, if they arepushed too far originally or slip down, it is almost impossible towithdraw them through the mouth and they have to beremoved through a gastrostomy. It is suggested that this is anunnecessary complication which can easily be avoided by notusing this type of design. If a tube dislodges proximally it can
R. Earlam and J. R. Cunha-Melo
PREVENTION OF PROXIMAL DISPLACEMENT
\
collar de Pezzer flangeFig. 4. Prevention of proximal displacement.
easily be pushed back or changed. The complications of thedistal collar or flange far outweigh the risk of either having topush the tube back down again or change it.
Distal displacementDistal displacement with the tube passing into the stomach canoccur with any of the tubes and it is more likely to occur inthose with a relatively small proximal lip. Careful attention tothe accurate measurement of diameters is the most essentialfactor in prevention. The new stainless steel Souttar tubes havea wider rim than the older type and are less likely to pass intothe stomach. Short small tubes have been known to passthroughout the bowel but some may remain for ever in thestomach causing no symptoms. The Souttar, Procter -Livingstone, Celestin and Mousseau-Barbin types have beenknown to pass per rectum. If a tube passes into the stomach atleast adequate dilatation of the stricture has occurred.
RefluxReflux occurs when a tube is inserted in the lower one-third ofthe oesophagus bridging the gastro-oesophageal junction.Macroscopic oesophagitis is usually unaccompanied bysymptoms whether due to reflux or stasis above an obstructionand should not necessarily be treated per se. Heartburn orreflux up through the cricopharyngeal sphincter should betreated symptomatically by antacids, posture and theavoidance of large meals before going to bed.
Wound infectionWound infection occurs in almost half the patients when athoracotomy or a laparotomy is necessary to insert a tubedirectly or to pull one down through a gastrostomy. It isprobably always wise to drain the laparotomy incision. Thereasons lie in the poor general condition of the patient, theabsence of high acidity in the stomach to sterilize its contentsand the unavoidable contamination of pulling the tube throughthe mouth and oesophagus. Wound infection must be acceptedas one of the complications to be assessed when decidingwhether to push or pull a tube through an oesophagealobstruction.
Guide wire complicationsThese can occur during the course of dilatation. A guide wireprovides safety for the inexperienced but there are a few specificcomplications which should be avoided. The wire must becarefully looked after since once it has been kinked it isdamaged for ever and should be replaced. The guide wiresprings are delicate and can break if pushed too hard (73).Loops and knots can also cause obstruction and this can beavoided by not passing too much wire into the stomach.
Complications related to tube materialSpecific complications of the Celestin tube include rubberdestruction or decomposition (74). This can be avoided byreplacement of the tubes at 6-monthly intervals but there is noadvantage in regular endoscopic inspection even if Celestintubes are used for benign strictures (75) because thiscomplication is rare. In the latest tubes the nylon spiral is inshort lengths. Originally the nylon spiral was continuous andwhen the latex decomposed the distal part attached by thenylon passed down the bowel and perforation was caused bythe bowstring sawing effect (76). Any tube with the old-

Malignant oesophageal strictures 67
fashioned design should be discarded because the rubber doesnot have an indefinite shelf life.
The other types of tube have not been in use long enough forspecific complications to be described or were discarded earlybecause too many complications occurred. Polyethylene doesnot have an indefinite life in the body and becomes brittleand fractures with time. Each material has its own specificcomplications but they can be avoided by replacement. If this isdone together with further dilatation, a larger tube can bepushed in. If the tube was originally one of the pullthroughtype, further laparotomy is unjustified. The problems ofmaterial decomposition in the majority of instances are of nopractical importance because the natural history of the diseaseat this stage is so short.
OthersProximal prolapse of the rim has been described (77) but thetulip shape was designed to avoid this. Prolapse of theoesophageal mucosa has been described once, but only with aMousseau-Barbin tube (78).
Assessment of results. Very few papers have been concerned with measurement of thequality of life after intubation, in spite of this being the mainfactor in palliation (79). Apart from the ability to swallow, it isessential to assess such items as sleeping at night withoutcoughing or choking (80). The ability to enjoy leisure and beable to work are rarely measured but are actually extremelyimportant.
The ideal palliative tubeSir Henry Souttar originally proposed that an ideal tube shouldbe (27): flexible, incompressible, non-traumatic and compact,should have an adequate lumen and remain in place. Nothingmore can be said except perhaps to add the questions: what isthe name of this ideal tube and from where can it be obtained?The authors consider that the basic tube types, Celestin (with orwithout flange, Medoc (Glos.) Ltd, Tetbury, Gloucestershire)or Atkinson (with flange, Ke'ymed, Southend-on-Sea) andSouttar (stainless steel, Seward's, Blackfriars, London), are-asnear to ideal as can be obtained. They are available in differentsizes, and can be pushed or pulled according to the particulartumour. The Didcott dilator and the Procter-Livingstone tubescan also be obtained in this country (Staniforth Limited,Penarth, South Glamorgan). It is essential that tubes arestocked in every operating theatre because suitable patients areadmitted frequently as emergencies.
AcknowledgementDr Cunha-Melo would like to thank the Brazilian National Council ofScientific and Technological Development (CNPq) for a grant.
References1. Earlam R. J. and Cunha-Melo J. R.: Oesophageal squamous cell
carcinoma: I. A critical review of surgery. Br. J. Sure. 1980; 67:381-90.
2. Saunders N.- R.: The Celestin tube in the palliation of carcinoma .of the oesophagus and cardia. Br. J. Surg. 1979; 66: 419-21.
3. Angorn I. B. and Hegarty M. M.: Palliative pulsion intubation inoesophageal carcinoma. Ann. R. Coll. Surf. Engl. 1979; 61-212-4.
4. Sanfelippo P. M. and Bernatz P. E.: Celestin-tubc palliation formalignant esophageal obstruction. Surg. Clin. North Am. 1973;53: 921-6.
5. Jackson J. W., Cooper D. K. C., Guvendik L. et al.: The surgicalmanagement of malignant tumours of the oesophagus and cardia;a review of the results in 292 patients treated over a 15-year period(1961-75). Br. J. Surg. 1979; 66: 98-104.
6. Earlam R. J. and Cunha-Melo J. R.: Oesophageal squamous cellcarcinoma; II. A critical review of radiotherapy. Br. J. Surg. 1980-67: 457-61.
7. Earlam R. J.: Souttar tube for oesophageal carcinoma. Chir.Caxlroenterol. 1979; 13: 15-20.
8. Earlam R. J., Cunha-Melo J. R., Donnan S. P. B. et al.: Theepidemiology of oesophageal cancer. 1982. (In the press.)
9. Barlow D.: Alternative methods of oesophageal replacement andreconstruction. In: Rob C. and Smith R. (ed.): Operative Surgery-Service. London: Butterworths. 1965; 5: 23.
10. Schomacher P. H.: Treatment of inoperable oesophageal malig-nancies with a thermal probe. Dtsch. Med. Wochenschr. 1977; 102:647-9.
11. Wittrin G.: Die palliative Behandlung tumorbedingterinoperabler Oesophagusstenosen mil der Thermosonde. Chirurg1973; 44: 285-7.
12. Krishaber A.: De la sonde oesophagienne a demeure. Trans. Int.Med. Congress 1882; 2: 393-6.
13. Durham. A.: Gastrostomy and oesophagostomy in cancer of theoesophagus. Lancet 1881; 2: 872-5.
14. Croft J.: Treatment of cancerous obstruction of the oesophagusby permanent catheterism. St Thomas' Hospital Reports 1882; 12:45-53.
15. Bird G.: Gastrostomy and oesophagostomy in cancer of theoesophagus. Lancet 1881; 2: 872-975.
16. Mackenzie M.: A Manual of Diseases of the Throat and Noseincluding the Pharynx, Larynx, Trachea, Oesophagus, Nose andNaso-pharynx. London: J. A. Churchill, 1884.
17. Symonds C. J.: A case of malignant stricture of the oesophagusillustrating the use of the new form of oesophageal catheter.Trans. Chir. Soc. Land. 1885; 18: 155-8.
18. Symonds C. J.: The treatment of malignant stricture of theoesophagus by tubage or oral catheterism. Br. Med. J. 1887; 1:870-4.
19. d'Etoilles L.: In de Lanacherie de I'Oesophagotomie. Brussels.1845.
20. Kelly H. D. B.: Origins of oesophagology. Proc. R. Soc. Med.1969; 62: 781-6.
21. Mikulicz J.: Ueber Gastroskopie und Oesophagoskopie. Zen-tralbl. Chir. 1881:8: 43.
22. Guisez J.: De 1'intubation caoutchoutee oesophagienne. PresseMed. 1914; 22: 85-7.
23. Guisez J.: Traite des Maladies de I'Oesophage. Paris. Libraire J. B.Bailliere et fils, 1911.
24. Mosher H. P.: Some observations on esophageal cases and thepresentation of two new instruments. Laryngoscope 1909; 19:401-27.
25. Souttar H. S.: Method of intubating the oesophagus for malig-nant stricture. Br. Med. J. 1924; 1: 782-3.
26. Souttar H. S.: Treatment of carcinoma of the oesophagus basedon 100 personal cases and 18 post-mortem reports. Br. J. Surg.1927; 15: 76-94.
27. Souttar H. S.: Cancer of the oesophagus. Br. Med. J. 1934; 2:797-800.
28. Amman J. R. and Collis J. L.: Palliative intubation of theoesophagus. Analysis of 59 cases. /. Thorac. Cardio vase. Surg.1971; 61: 863-9. '
29. Mousseau M., Le Forestier J., Barbin J. et al.: Place de1'intubation a demeure dans le traitement palliative du cancer de1'oesophage. Arch. Mai. Appar. Digest. 1956; 45: 208-16.
30. Celestin L. R.: Permanent intubation in inoperable cancer of theoesophagus and cardia. A new tube. Ann. R. Coll. Surg. Engl.1959; 25: 165-70.
31. Celestin L. R.: Intubation in carcinoma of the esophagus andcardia. Armamentarium 1965; 4: 8.
32. Celestin L. R.: Improvements in the Celestin tube for endo-oesophageal intubation in carcinoma and strictures. Armamen-tarium 1969; 5: 10.
33. Giradet R. E., Ransdell H. T. jun., Wheat M. W. jun. et al.:Palliative intubation in the management of esophageal car-cinoma. Ann. Thorac. Surg. 1974; 18: 417-30.
34. O'Connor T., Watson R., Lepley D. jun. et al.: Esophagealprosthesis for palliative intubation. Further evaluation of 378patients. Arch. Surg. 1963; 87: 275-9.
35. Mounier-Kuhn P., Gaillard J., Haguenauer J. P. et al.: Lesindications de Fintubation par voie haute des cancers de1'oesophage. J. Fr. Olorhinolaryngol. 1968; 17: 491-5.
36. Procter D. S. C.: Esophageal intubation for carcinoma of theesophagus. World J. Surg. 1980; 4: 451-61.
37. Heafitz M., Irarrazvavai M., Huebl H. et al.: A simple techniquefor intubation of the oesophagus for fistulae and obstructions.Chest 1974; 65: 359-60.
38. Atkinson M. and Ferguson R.: Fibreoptic cndoscopic palliativeintubation of inoperable oesophagogastric neoplasms. Br. Med. J.1977; 1: 266-7.
39. Atkinson M., Ferguson R. and Parker G. C.: Tube introducerand modified Celestin tube for use in palliative intubation ofoesophagogastric neoplasms of fibreoptic endoscopy. Gut 1978;19:669-71.
40. Atkinson M., Ferguson R. and Ogilvie A. L.: Management ofmalignant dysphagia by intubation at endoscopy. J. R. Soc. Med.1979; 72: 894-7.
41. Berman E. F.: The experimental replacement of the esophagus bya plastic tube. Ann. Surg. 1951; 135: 337-43.
42. Berman E. F.: A plastic prosthesis for resected esophagus. Arch.Surg. 1952; 65: 916-9.
43. Watanabe K. and Mark J. B. D.: Segmental replacement of thethoracic esophagus with a silastic prosthesis. Am. J. Surg. 1971;121: 238-40.

68 R. Earlam and J. R. Cunha-Melo
44. Chu W., Rics G., Jaurigue V. G. et al.: Restoration of pharyngo-csophaeeal continuity with a replaceable prosthetic conduit: anew method. Am. ./. Surg. 1978: 135: 269-71.
45. Skerik P. and Tichy S.: Neue Indicationen fur Endoprothesen derSpeisewege bei Stenosen im Bereiche des SpeiserohremundesMonatsschr. Ohrenheilkd. Laryngorhinol. 1971; 105: 38-42.
46. Stuart D. W.: Surgery of cancer of the cervical oesophagus withplastic tube replacement. /. Laryngol. 1966: 80: 382-6.
47. Shilling B. B.: Hypopharyngostomy. Laryngoscope 1971: 81:1119-25.
48. Klopp C. T.: Cervical csophagostomy. J. Thorac. Surg. 1951; 21:490-1.
49. Davidson J. S.: Puncture of the cervical esophagus in thepalliative treatment of carcinoma of the esophagus. J. Thorac.Surg. 1955; 30: 348-55.
50. Heimlich H. J.. Greenless T. W. and Winfield J. M.: Carcinoma ofthe esophagus. A palliative procedure with use of a plastic tubeintroduced through a cervical incision. JAMA 1956; 101: 192-5.
51. Heimlich H. J.: Two palliative operations for cancer of theesophagus using plastic prostheses. Am. J. Surg. 1962; 103:376-82.
52. Ritter J. A.: Pyriform sinusostomy. JAMA 1969; 207: 365-8.53. Palmer E. D.: Peroral prosthesis for the management of incurable
esophageal carcinoma. Am. J. Gastroenterol. 1973; 59: 487-98.54. Tytgat G. N., Hartog-Jagcr F. C. A. and Hauerkamp H. J.:
Positioning of a plastic prosthesis under fibre endoscopic controlin the palliative treatment of cardio-esophageal cancer. Endos-copy 1976; 8: 180-5.
55. Boyce H. W. and Palmer E. D.: Techniques of Clinical Gastro-enterology. Springfield, 111., Charles C. Thomas, 1975.
56. Carter M. G.: Endoscopic intubation and dilatation in themanagement of esophageal carcinoma. Am. J. Surg. 1957; 93:266-70.
57. de Souza L. J.: Palliative intra-oesophageal intubation in ad-vanced cancer of the oesophagus. Ind. J. Cancer 1971; 8:116 22.
58. Haring R.: Eine neue Oesophagusendoprothese als Palliativmas-snahme beim inoperablen Oesophagus- und Kardiacarcinom.Chirurg 1964; 35: 549-51.
59. Holinger P. H.: Self retaining esophageal intubation tube. Ann.Owl. Rhinol. Otolaryngol. 1955; 64: 921.
60. Lcvine S.: Palliative treatment of carcinoma of the esophagus.Rocky Mt. Med. J. 1959; 56: 39-41.
61. Davidenko N., Chifflct J., Fossati C. G. et al.: Intubation ofneoplaslic esophageal stenoses. A new prosthesis with an anti-reflux device. Nvuv. Presse Med. 1975; 4: 2396-8.
62. Beaugie J. M. and Earlam R. J.: The Aldon bag flutter valve. Br.J. Urol. 1971; 43: 608-10.
63. Leonard J. R., Rossi N. P. and Blaedel M.: Esophageal car-cinoma. Palliation by indwelling tubes. Ann. Otol. Rhinol.Laryngol 1969; 78: 1169-78.
64. Coyas A. and Triboulet-Piton J.: Resultats obtenus par unnouveau procede d'intubation palliative du cancer inoperable deFoesophage. Ann. Otolarvngol. 1955; 72: 143-7.
65. Jager F. C. A. H., Bartefsman J. F. W. M. and Tytgat G. N. J.:Palliative treatment of obstructing csophagogastric malignancyby endoscopic positioning of a plastic prostheses. Gaslro-enterology 1979; 77: 1008-14.
66. Sachs L.: A plastic prosthesis for palliating carcinoma of theesophagus. Surgery 1959; 45: 377-88.
67. Adams C. L.: The complications of endoesophageal tubes.J. Thorac. Cardiovasc. Surg. 1966; 51: 685-93.
68. Kaloor, G. H. and Collis J. L.: Palliative push-through intubationfor malignant stricture of the esophagus. Lancet 1960; 1: 923.
69. Anscombe A. R., Pearson K. and Taylor T. V.: A simple methodfor the introduction of an oesophageal tube in advanced car-cinoma of the oesophagus. Br. J. Surg. 1976; 63: 944-8.
70. Crossing F. T.: A set of guide and bougies to facilitate insertionof Mousseau-Barbin lubes. Br. Med. J. 1961; 1: 1032.
71. Jamieson R. A., Cameron E. and Clark R. G.: Palliation inmalignant stricture of the esophagus. Lancet 1960; 1: 923.
72. Holden M. P., Wooler G. H. and lonescu M. I.:Mousseau-Barbin tubes for the treatment of carcinoma of thelower two-thirds of the oesophagus. Results and operative tech-niques. Br. J. Surg. 1973; 60: 401-2.
73. Bancewicz J.: A hazard of the Eder-Puestow system for oeso-phageal dilatation. Br. J. Surg. 1979; 66: 66.
74. Ranson M. B. and John H. T.: Complications associated with theuse of the Celestin tube for benign oesophageal obstruction. Br. J.Surg. 1979; 66: 110 2.
75. Wilson M. G., Bristol J. B., Mortcnsen N. J. et al.: The Celestintube in the treatment of benign oesophageal strictures. Br. J.Surg. 1980; 67: 506 8.
76. Shaw J. F. L. and Coombes G. B.: Multiple intestinal perforationdue to Celestin tube. Br. J. Surg. 1979; 66: 807-8.
77. Mackenzie I., Whyte A. S. and Tankel H. I.: Structural deterior-ation in Celestin tubes. Br. J. Surg. 1976; 63: 851-2.
78. Adams C. L. and Emerson D. M.: Obstruction of aMousseau-Barbin tube from prolapsed esophageal mucosa.J. Thorac. Cardiovasc. Surg. 1965; 49: 259-63.
79. Das S. K. and John H. T.: Oesophageal intubation in obstructivelesions of the-oesophagus. Br. J. Surg. 1973; 60: 403-6.
80. Stoller J. L., Toppin D. I. and Flores A. D.: Carcinoma of theesophagus; a new proposal for the evaluation of treatment. Can.J. Surg. 1977; 20: 454-9.
81. Coyas A.: Palliative intubation in carcinoma of the oesophagus.Lancet 1955; 2: 647-9.
82. Didcott C. C.: Oesophageal strictures. Treatment by slow con-tinuous dilatation. Ann. R. Coll. Surg. Engl. 1973; 53: 112-26.
83. Didcott C. C.: Simplified oesophageal intubation for cancerpalliation. 5. Afr. J. Surg. 1974; 12: 173-5.
84. Didcott C. C.: Simplified oesophageal intubation for carcinoma.In: Silber W. (ed.): Carcinoma of the Oesophagus. Rotterdam:Balkema, 1978: 352-7.
85. Fell S. C., Grunwald R. P. and Hurwitt E. S.: Palliation ofesophageal carcinoma by prosthetic intubation. J. Thorac.Cardiovasc. Surg. 1966; 51: 272-8.
86. Goni-Moreno I.: Cirurgia del Esofago y Hernias par el Hiato-esofagico. Buenos Aires: Editorial Universitaria, 1964.
87. Segura J., Martinez A. and Olarter H.: Palliative treatment ofesophageal obstruction with Goni's plastic tube. Surg. Gvnecol.Obstet. 1966; 122: 1021-4.
88. Gourevitch A.: Intubation of the cardia for inoperable car-cinoma. Lancet 1959; 2: 258-60.
89. Fornaro M., Sauerberli H. and Baumgartner D.: The Haringtubes for palliative surgery of inoperable esophageal cancer. Animprovement of the quality of life. Helv. Chir. Acta 1976; 43:533-6.
90. Mackler S. A. and Mayer R. M.: Palliation of esophagealobstruction due to carcinoma with a permanent intraluminaltube. /. Thorac. Surg. 1954; 28: 431-45.
91. Moghissi K.: Palliation in malignant stricture of the oesophagus.Lancet 1960; 1: 679-80.
92. Palmer E. D.: Experiences with management of malignant oeso-phagorespiratory fistula by peroral esophageal prosthesis. Gastro-intest. Endosc. 1970; 17: 12-16.
93. Boyce W. H.: Peroral prosthesis for palliating malignantesophageal and gastric obstruction. Gastroenterology 1979; 77;1141-1153.
94. Boyce H. W. jun.: Non-surgical measures to relieve distresses oflate oesophageal carcinoma. Geriatrics 1973; 28: 97-102.
95. Procter D. S. C.: Carcinoma of the oesophagus. A review of 523cases. S. Afr. J. Surg. 1968; 6: 137-59.
96. Haffejee A. A. and Angorn I. B.: Oral alimentation followingintubation for esophageal carcinoma. Ann. Surg. 1977; 186:759-61.
97. Hegarty M. M., Angorn I. B., Bryer J. V. et al.: Palliation ofmalignant esophago-respiratory fistulae by permanent indwellingprosthetic tube. Ann. Surg. 1977: 185: 88-91.
98. Hegarty M. M., Angorn I. B., Bryer J. V. et al.: Pulsionintubation for palliation of carcinoma of the oesophagus. Br. J.Surg. 1977; 64: 160-5.
99. Stirnemann H. and Kammer B.: Zur palliativen Behandlung desOesophaguscarcinoms: Weitere Erfahrung mit dem Doppcltrich-terschlauch. Chirurg 1971; 42: 130-3.
100. Stirnemann H. and Roth F.: Erfahrungen mit Plastikrorohen beider palliativen Behandlung des Oesophagus Kardiacarcinoms.Helv. Chirurg. Acta 1965; 32: 139-43.
101. Weisel W., Raine F., Watson R. R. et al.: Palliative treatment ofesophageal carcinoma. A method and its evaluation. Am. Surg.1959; 149: 207-16.
102. Weisel W.: Palliation of advanced carcinoma of the esophagus byintubation. In: Ellison E. H. and Freisen S. R. (ed.): CurrentSurgical Management III. Philadelphia: Saunders, 1965; 23-9.
103. Clauss D. and Baudisch J.: Der Wert der Endoprothesen bei derpalliativen, Behandlung inoperable Oesophagus und Kardiacar-cinom. Zentralbl. Chir. 1971; 96: 602-607.
104. Dubois J., Michel A., Naudin E. et al.: Valeur de Fappareillagcplastique dans le traitment palliatif des cancers de Focsophage etdu cardia. Arch. Fr. Mai. App. Dig. 1962; 51: 920-5.
105. Greening W. P. and Ramsay G. S.: Cancer of the oesophaguspalliation by intubation. Lancet 1960: 2: 1122 3.
106. Grewe H. E. and Bircks W.: Palliative Behandlung durch Endo-prosthese beim inoperable Oesophagus; kardia-karcmom. Thor-axchirurgie 1964; 11: 328-38.
107. Zaslavsky U. K.: Rehabilitation of esophageal permeability ininoperable patients. Acta Union Int. Cancer 1963; 19: 1025-6.
108. Hayes A. V.: Observations on a new method of canalizingstrictures of the oesophagus. S. Afr. Med. J. 1959; 33: 1071 -6.
109. Kropff G.: Intubation oesophagienne par tube en matiere plas-tique suivie de radiumtherapie dans le traitmcnt du cancer deFoesophage. Mem. Acad. Chir. (Paris) 1954; 80: 628-34.
110. Brown A. L.: Carcinoma of the esophagus. Use of rigid indwell-ing esophagcal tube. J. Thorac. Surg. 1949; 18: 493-5.
Paper accepted 16 June 1981.














![Endoscopic incisional therapy for benign esophageal ... · caustic strictures and radiation strictures are known to be complex strictures[2]. Dilatation by bougie or balloon dilators](https://static.fdocuments.net/doc/165x107/5f80c75354e157596f1a7ef6/endoscopic-incisional-therapy-for-benign-esophageal-caustic-strictures-and-radiation.jpg)


