Magnetic resonance imaging demonstrates long-term changes ... · Cite this article as: Hatfield T,...
8
Magnetic resonance imaging demonstrates long-term changes in brain structure in children born preterm and exposed to chorioamnionitis Tamera Hatfield, MD, PhD; Deborah A. Wing, MD; Claudia Buss, PhD; Kevin Head, BS; L. Tugan Muftuler, PhD; Elysia Poggi Davis, PhD OBJECTIVE: We sought to determine if children born preterm and ex- posed to chorioamnionitis have differences in brain structure measured at 6-10 years of age using magnetic resonance imaging (MRI). STUDY DESIGN: Structural MRI was performed with 11 preterm children (8.5 1.7 years) with chorioamnionitis and 16 preterm children (8.7 1.4 years) without chorioamnionitis. Cortical surface reconstruction and volu- metric segmentation were performed with FreeSurfer image analysis soft- ware. Subcortical structures were analyzed using multivariate analysis. RESULTS: Widespread regional differences in cortical thickness were observed. With chorioamnionitis, the frontal and temporal lobes were primarily affected by decreased cortical thickness, and the limbic, pari- etal, and occipital lobes were primarily affected by increased cortical thickness when compared to the comparison group. Subcortical differ- ences were observed in the hippocampus and lateral ventricle. CONCLUSION: Using MRI, chorioamnionitis is associated with long- term widespread regional effects on brain development in children born prematurely. Our study is limited by its small sample size. Key words: chorioamnionitis, infection, magnetic resonance imaging, neurodevelopment, preterm Cite this article as: Hatfield T, Wing DA, Buss C, et al. Magnetic resonance imaging demonstrates long-term changes in brain structure in children born preterm and exposed to chorioamnionitis. Am J Obstet Gynecol 2011;205:384.e1-8. C horioamnionitis, a common etiol- ogy of preterm birth, has often been cited as a risk factor for the development of cerebral palsy and brain injury. 1-5 Addi- tionally, cystic periventricular leukomala- cia (PVL), damage to deep white matter, is thought to be a precursor to cerebral palsy in that 60-100% of infants with cystic PVL go on to develop cerebral palsy suggesting that white matter injury may be associated with intrauterine infection. 6 A metaanaly- sis documented that chorioamnionitis is a risk factor for cerebral palsy in both term and preterm delivered infants. 7 Although cerebral palsy is a severe manifestation of brain injury, there are likely other subclin- ical effects associated with exposure to chorioamnionitis. Subclinical or less se- vere manifestations of abnormal brain de- velopment (including both gray and white matter damage) may ultimately play a role in cognitive development or other patho- logic processes. The association between intrauterine infection and brain injury is strongly supported in experimental studies utiliz- ing animal models. In addition to white matter damage observed following ex- perimentally induced intrauterine infec- tion, 8 Gavilanes et al 9 demonstrated global and diffuse effects on the central nervous system, including decreased number of neurons in the cortex, hippocampus, and substantia nigra. Together, these findings, as well as others, suggest the potential for global and diffuse neurologic injury as a direct result of intrauterine infection and that this damage extends beyond white matter injury alone. There is a paucity of data describing the consequences of intrauterine infec- tion for brain development in human beings. Preterm birth is associated with compromised brain development. 10-12 Given the evidence from animal models that intrauterine infection leads to wide- spread neurological deficits 9 and the prevalence of infection among women delivering preterm, 13 it is plausible that exposure to chorioamnionitis may con- tribute to additional neurologic impair- ments observed in children born pre- term beyond that of prematurity alone. To date, there are only 2 studies attempt- ing to evaluate the effects of chorioam- nionitis on brain structure and neither used a whole-brain approach; one as- sessed the effectiveness of a specific tech- nique in the evaluation of isolated white matter injury 14 in the neonate and the other performed a randomly chosen re- From the Departments of Obstetrics and Gynecology (Drs Hatfield and Wing) and Pediatrics (Drs Buss and Davis) and the Women and Children’s Health and Well-Being Project, Department of Psychiatry and Human Behavior (Drs Buss and Davis and Mr Head), University of California, Irvine, School of Medicine, Irvine, CA, and the Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, WI (Dr Muftuler). Received March 11, 2011; revised July 6, 2011; accepted July 15, 2011. This report was funded in part by National Institute for Child Health and Human Development R01 HD050662 (E.P.D.). The authors report no conflict of interest. Presented at the 31st annual meeting of the Society for Maternal-Fetal Medicine, San Francisco, CA, Feb. 7-12, 2011. Reprints: Tamera Hatfield, MD, PhD, University of California, Irvine, 101 The City Dr., Bldg. 56, Orange, CA 92868. thatfi[email protected]. 0002-9378/$36.00 • © 2011 Mosby, Inc. All rights reserved. • doi: 10.1016/j.ajog.2011.07.027 SMFM Papers www. AJOG.org 384.e1 American Journal of Obstetrics & Gynecology OCTOBER 2011
Transcript of Magnetic resonance imaging demonstrates long-term changes ... · Cite this article as: Hatfield T,...

(
cc
c
SMFM Papers www.AJOG.org
Magnetic resonance imaging demonstrates long-termchanges in brain structure in children bornpreterm and exposed to chorioamnionitisTamera Hatfield, MD, PhD; Deborah A. Wing, MD; Claudia Buss, PhD;Kevin Head, BS; L. Tugan Muftuler, PhD; Elysia Poggi Davis, PhD
OBJECTIVE: We sought to determine if children born preterm and ex-posed to chorioamnionitis have differences in brain structure measuredat 6-10 years of age using magnetic resonance imaging (MRI).
STUDY DESIGN: Structural MRI was performed with 11 preterm children8.5�1.7 years) with chorioamnionitis and 16 preterm children (8.7�1.4years) without chorioamnionitis. Cortical surface reconstruction and volu-metric segmentation were performed with FreeSurfer image analysis soft-ware. Subcortical structures were analyzed using multivariate analysis.
RESULTS: Widespread regional differences in cortical thickness were
observed. With chorioamnionitis, the frontal and temporal lobes wereand exposed to chorioamnionitis. Am J Obstet Gynecol 2011;205:384.e1-8.
bicvvmil
isimpt
0002-9378/$36.00 • © 2011 Mosby, Inc. All rights reserved. • doi: 10.1016
384.e1 American Journal of Obstetrics & Gynecology OCTOBER 2011
primarily affected by decreased cortical thickness, and the limbic, pari-etal, and occipital lobes were primarily affected by increased corticalthickness when compared to the comparison group. Subcortical differ-ences were observed in the hippocampus and lateral ventricle.
CONCLUSION: Using MRI, chorioamnionitis is associated with long-term widespread regional effects on brain development in children bornprematurely. Our study is limited by its small sample size.
Key words: chorioamnionitis, infection, magnetic resonance imaging,
neurodevelopment, pretermCite this article as: Hatfield T, Wing DA, Buss C, et al. Magnetic resonance imaging demonstrates long-term changes in brain structure in children born preterm
pdetmtTinusnm
Chorioamnionitis, a common etiol-ogy of preterm birth, has often been
ited as a risk factor for the development oferebral palsy and brain injury.1-5 Addi-
tionally, cystic periventricular leukomala-cia (PVL), damage to deep white matter, isthought to be a precursor to cerebral palsyin that 60-100% of infants with cystic PVLgo on to develop cerebral palsy suggestingthat white matter injury may be associatedwith intrauterine infection.6 A metaanaly-sis documented that chorioamnionitis is arisk factor for cerebral palsy in both termand preterm delivered infants.7 Althougherebral palsy is a severe manifestation of
From the Departments of Obstetrics and Gyn(Drs Buss and Davis) and the Women and ChDepartment of Psychiatry and Human BehavUniversity of California, Irvine, School of MeNeurosurgery, Medical College of Wisconsin,
Received March 11, 2011; revised July 6, 2011;
This report was funded in part by National InstituR01 HD050662 (E.P.D.).
The authors report no conflict of interest.
Presented at the 31st annual meeting of the SocCA, Feb. 7-12, 2011.
Reprints: Tamera Hatfield, MD, PhD, UniversityOrange, CA 92868. [email protected].
rain injury, there are likely other subclin-cal effects associated with exposure tohorioamnionitis. Subclinical or less se-ere manifestations of abnormal brain de-elopment (including both gray and whiteatter damage) may ultimately play a role
n cognitive development or other patho-ogic processes.
The association between intrauterinenfection and brain injury is stronglyupported in experimental studies utiliz-ng animal models. In addition to white
atter damage observed following ex-erimentally induced intrauterine infec-
ion,8 Gavilanes et al9 demonstrated global
logy (Drs Hatfield and Wing) and Pediatricsen’s Health and Well-Being Project,
(Drs Buss and Davis and Mr Head),ne, Irvine, CA, and the Department oflwaukee, WI (Dr Muftuler).
epted July 15, 2011.
or Child Health and Human Development
for Maternal-Fetal Medicine, San Francisco,
alifornia, Irvine, 101 The City Dr., Bldg. 56,
/j.ajog.2011.07.027
and diffuse effects on the central nervoussystem, including decreased number ofneurons in the cortex, hippocampus, andsubstantia nigra. Together, these findings,as well as others, suggest the potential forglobal and diffuse neurologic injury as adirect result of intrauterine infection andthat this damage extends beyond whitematter injury alone.
There is a paucity of data describingthe consequences of intrauterine infec-tion for brain development in humanbeings. Preterm birth is associated withcompromised brain development.10-12
Given the evidence from animal modelsthat intrauterine infection leads to wide-spread neurological deficits9 and the
revalence of infection among womenelivering preterm,13 it is plausible thatxposure to chorioamnionitis may con-ribute to additional neurologic impair-
ents observed in children born pre-erm beyond that of prematurity alone.o date, there are only 2 studies attempt-
ng to evaluate the effects of chorioam-ionitis on brain structure and neithersed a whole-brain approach; one as-essed the effectiveness of a specific tech-ique in the evaluation of isolated whiteatter injury14 in the neonate and the
ecoildriordiciMi
acc
te f
iety
of C
other performed a randomly chosen re-

tpinnhpnaapcclau
bmtagtto
www.AJOG.org SMFM Papers
gion-specific analysis at term gestationalage.15 Thus far, there have been no long-ermfollow-upstudiesattemptingtoidentifyersisting differences in brain development
nchildrenexposedtochorioamnionitispre-atally using whole-brain magnetic reso-ance imaging (MRI) techniques. Ourypothesis, largely driven by the ex-erimental literature, is that chorioamnio-itis would lead to widespread and diffuselterations in child brain morphology ands such consider the whole-brain approachreferable. Therefore, the objective of theurrent investigation was to determine ifhorioamnionitis is associated with neuro-ogic differences in children born preterms measured by cortical thickness and vol-me of subcortical structures.
MATERIALS AND METHODSThe institutional review board for pro-tection of human subjects at the Univer-sity of California, Irvine, approved thestudy protocol. Written and informed
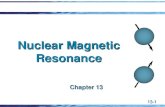
FIGURE 1Flow diagram of subject selection
MRI, magnetic resonance imaging.
Hatfield. Chorioamnionitis exposure and MRI findings. Am
consent was obtained from mothers prior
to study enrollment. Children aged 6-10years were recruited into a study of prena-tal influences on child brain development,and a subset of these were assessed withstructural MRI. Children were born at ei-ther the University of California, Irvine,Medical Center or Long Beach MemorialMedical Center/Miller Children’s Hospi-tal, a community hospital affiliate of theuniversity.
Subject selectionParticipants included 11 children whowere born preterm with documented ex-posure to chorioamnionitis and 16 chil-dren born preterm who were not exposedto chorioamnionitis, but with similar neo-natal characteristics. Subjects participatedin a larger study of prenatal influences onchild development at the University ofCalifornia, Irvine, and were eligible forparticipation in this substudy based on thefollowing criteria: subjects were included ifthey were singletons and �28 and �37
stet Gynecol 2011.
gestational weeks at birth (based on Amer-
OCTOBER 2011 Americ
ican College of Obstetricians and Gynecol-ogists dating criteria).16 Exclusion criteriafor participation included congenital orgenetic anomaly, maternal preeclampsiaor HELLP syndrome, maternal drug use,or postnatal steroid administration (Fig-ure 1). Subjects who met inclusion criteriawere recruited in 2 groups: those with andwithout antenatal exposure to chorioam-nionitis. Exposure to chorioamnionitiswas based on clinical and/or histopatho-logical assessment. Clinical criteria forchorioamnionitis was defined as fever(�100.4°F) in the presence of preterm la-
or (PTL), preterm premature rupture ofembranes (PPROM), maternal or fetal
achycardia, or foul-smelling discharge ormniotic fluid. Subjects in the comparisonroup were born concurrently with thearget group and had placental histopa-hology reports documenting the absencef chorioamnionitis.
Maternal and neonatal characteristicsBackground characteristics including de-mographic variables were determined atthe time of study entry by standardizedmaternal interview. Maternal intellec-tual performance was determined bythe Perceptual Reasoning Scale of theWechsler Adult Intelligence Scale.17
Neonatal and maternal medical charac-teristics including birth outcome datawere determined by chart abstraction.Hypotension was defined by either theuse of pharmacologic pressor support ordocumentation of hypotension in themedical records. The presence of intra-ventricular hemorrhage was evaluatedby cranial ultrasounds that were ob-tained as part of standard convention.Sepsis was defined by positive blood cul-tures and diagnosis documented in themedical record.
MRI protocolT1-weighted scans were acquired in a 3TPhilips Achieva system (Philips Health-care, Andover, MA) using a 3-dimen-sional magnetization prepared rapidgradient echo pulse sequence that cov-ered the whole brain. The images wereacquired in the sagittal orientation withfield of view � 240 � 240 mm2, 1 mm3
isotropic voxel dimensions, 150 slices,
J Ob
time to repetition � 11 milliseconds,
an Journal of Obstetrics & Gynecology 384.e2

gaw
iwswidt
cgps
.
SMFM Papers www.AJOG.org
echo time � 3.3 milliseconds, inversionpulse delay � 1100 milliseconds, flip an-le � 18 degrees. No signal averagingnd no sensitivity encoding accelerationere used.
Image processingCortical surface reconstruction and vol-umetric segmentation was performedwith the FreeSurfer image analysis soft-ware suite, which is available for down-load online (http://surfer.nmr.mgh.harvard.edu/). It should be emphasizedthat the calculations of cortical thicknessare generated directly by the softwareand independent of the operator. Fur-ther, the operator was not aware of thestudy hypothesis. Streamlined imageprocessing procedures are provided inthis software package, which first beginsby applying intensity normalizationprior to segmentation to minimize er-rors in identifying the boundaries.18 Thisis followed by removal of nonbrain tis-sues.19 Then, the images are transformednto the Talairach space and subcorticalhite matter and subcortical gray matter
tructures are segmented.20,21 Pial andhite matter surfaces were located by find-
ng the highest intensity gradient, whichefines the transition from one tissue classo the other.22-24 Once the preprocessing
steps are completed, surface inflation is ap-plied to each individual brain and the in-flated brains are registered to a sphericalatlas.25 This procedure utilizes individualcortical folding patterns to achieve accu-rate registration of cortical geometryacross subjects.26 Cortical thickness is cal-ulated as the closest distance from theray matter/white matter surface to theial surface at each vertex on the tessellatedurface.24 Procedures for the measure-
ment of cortical thickness have beenvalidated against histologic analysis27
and manual measurements.28,29 Thecortical surface images generated bythe FreeSurfer software were visuallyinspected for errors in segmentationand corrections were made as needed.
Analysis of group differencesin cortical thicknessDifferences between groups in corticalthickness were analyzed at each and ev-
ery node on the cortical surface using a384.e3 American Journal of Obstetrics & Gynecolo
standard statistical approach for whole-brain analyses. In this method, the soft-ware represents the brain surface with adense array of vertices. At each vertex,the brain thickness is calculated for eachsubject. Then the software applies a gen-eral linear model to test the significanceof independent variables (ie, chorioam-nionitis) on the variations of corticalthickness across subjects at each and ev-ery vertex location. If an effect has strongcorrelation with the variations in corticalthickness across subjects at that vertex,one gets a strong effect size. This effectsize is tested against the null hypothesisusing a t test and the resultant t scores are
TABLE 1Descriptive data
CharacteristicChori(n �
Subject characteristics...................................................................................................................
Child age at MRI, y 8....................................................................................................................
Total brain volume, cm3 1529...................................................................................................................
Race..........................................................................................................
Hispanic 5..........................................................................................................
White 4..........................................................................................................
African American 0..........................................................................................................
Multiethnic 1..........................................................................................................
Other 1...................................................................................................................
Sex 65
...................................................................................................................
Maternal and householdcharacteristics...................................................................................................................
Household income..........................................................................................................
�$30,000 6..........................................................................................................
$30,001-60,000 2..........................................................................................................
$60,001–100,000 1..........................................................................................................
�$100,000 2...................................................................................................................
Maternal education..........................................................................................................
High school or equivalent 6..........................................................................................................
College graduate 2...................................................................................................................
Maternal WAIS POI score, mean (SD) 92....................................................................................................................
Maternal marital status (percentmarried or cohabitating)
6
...................................................................................................................
Data presented as n (%) or mean � SD. t tests, �2, and FisheMRI, magnetic resonance imaging; POI, Perceptual Organizati
Hatfield. Chorioamnionitis exposure and MRI findings. A
reported. Spatially normalized cortical
gy OCTOBER 2011
thickness maps of each subject were en-tered into an analysis of variance modelusing the false discovery rate (FDR) cor-rection for multiple comparisons (P �05) as recommended by Genovese et al30
and is the standard approach to avoida type 1 error with this whole-brainanalysis.
Analysis of volumetric differencesin subcortical gray matterThe volume of each structure was calcu-lated by the FreeSurfer program. Groupdifferences in volume of subcorticalstructures were analyzed using analysisof covariance with intracranial volume
nionitis Comparison(n � 16)
Significancelevel (P value)
..................................................................................................................
1.7 8.7 �1.4 .61..................................................................................................................
33) 1486 (�212) .56..................................................................................................................
.71..................................................................................................................
%) 10 (62%)..................................................................................................................
%) 4 (25%)..................................................................................................................
2 (13%)..................................................................................................................
) 0..................................................................................................................
) 0..................................................................................................................
le,ale
12 male,4 female
.41
..................................................................................................................
..................................................................................................................
.21..................................................................................................................
%) 4 (25%)..................................................................................................................
%) 4 (25%)..................................................................................................................
) 2 (13%)..................................................................................................................
%) 6 (37%)..................................................................................................................
.11..................................................................................................................
%) 9 (56%)..................................................................................................................
%) 6 (38%)..................................................................................................................
6.8) 92.6 (16.2) .97..................................................................................................................
) 12 (75) .41
..................................................................................................................
ct tests.dex; WAIS, Wechsler Adult Intelligence Scale.
Obstet Gynecol 2011.
oam11)
.........
5 �.........
(�1.........
.........
(46.........
(36.........
.........
(9%.........
(9%.........
mafem.........
.........
.........
(55.........
(18.........
(9%.........
(18.........
.........
(55.........
(18.........
8 (1.........
(55
.........
r exaon In
m J
as a covariate.

csCaglIeo
m J
www.AJOG.org SMFM Papers
RESULTSClinical characteristicsOf the 11 subjects in the chorioamnioni-tis group, 7 were diagnosed by histologic
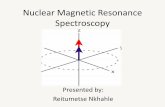
FIGURE 2Inflated brain surfaces of lateral anviews of left and right hemispheres
Blue overlays indicate regions in cortex significancorrection) in chorioamnionitis group. Red overl(P � .05 after FDR correction) in chorioamnionknown anatomical brain regions.Hatfield. Chorioamnionitis exposure and MRI findings. Am
TABLE 2Neonatal outcomes
OutcomeChorioa(n � 11
Gestational age at birth, wk 31.2...................................................................................................................
Birthweight, g 1660 (1...................................................................................................................
1-min Apgar score 8 (6...................................................................................................................
5-min Apgar score 9 (7...................................................................................................................
Mechanical ventilation 3 (2...................................................................................................................
Intraventricular hemorrhage (all) 1 (9...................................................................................................................
Culture-confirmed sepsis 0 (0...................................................................................................................
Antibiotic treatment forpresumed sepsis
9 (8
...................................................................................................................
Hypotension/pressoradministration
1 (9
...................................................................................................................
Mann-Whitney U, Fisher exact, and t tests for all group compa
Hatfield. Chorioamnionitis exposure and MRI findings. A
criteria, 2 by clinical and histologic crite-ria, and 2 by clinical criteria. Indicationsfor delivery in this group includedPPROM (n � 7), PTL (n � 3), and PTL
medial
thinner (P � .05 after false discovery rate [FDR]indicate regions that were significantly thickergroup. Multicolored lines define boundaries of
stet Gynecol 2011.
ionitis Comparison(n � 16) P value
4–35.4) 31.5 (28.4–36.0) .66..................................................................................................................
–2906) 1850 (1042–3179) .35..................................................................................................................
7 (2–9) .09..................................................................................................................
8.5 (8–9) .51..................................................................................................................
6 (37%) .55..................................................................................................................
1 (6%) .66..................................................................................................................
3 (19%) .19..................................................................................................................
13 (81%) .67
..................................................................................................................
2 (12.5%) .78
..................................................................................................................
s. Data presented as n (%) or median (range).
Obstet Gynecol 2011.
a
OCTOBER 2011 Americ
with abruption (n � 1). All 16 subjects inthe comparison group had histopathol-ogy reports available documenting theabsence of chorioamnionitis or funisitis.Indications for delivery in the compari-son group were PPROM (n � 5), PTL(n � 4), nonreassuring fetal status sec-ondary to abruption (n � 2), diabetes(n � 2), and not stated (n � 3).
Background and demographic dataDescriptive data for the study groups canbe found in Table 1. Groups did not signif-icantly differ in child factors (age at MRI,total brain volume, race, or sex), maternalintellectual performance, or sociodemo-graphic characteristics (maternal educa-tion, marital status, or household income).Neonatal health outcomes were not signif-icantly different between groups and areshown in Table 2. Importantly, the 2groups had similar ranges and distribu-tions of gestational age at delivery andbirthweight. A greater percentage of chil-dren in the chorioamnionitis group wereexposed to antenatal steroids compared tothe comparison group (11 chorioamnio-nitis group and 8 comparison group, P �.008). All MRIs were reviewed by a clinicalradiologist and no frank injury was ob-served. A subanalysis of MRIs includingonly those 18 subjects exposed to antenatalsteroids did not significantly change thestudy findings (data not shown). Further, 2subjects in the chorioamnionitis groupwere left handed. Again, a subanalysis ofMRIs including only subjects who wereright handed did not significantly changethe study findings (data not shown).
Analysis of cortical thicknessWidespread and predominantly bilateraldifferences in cortical thickness were ob-served between groups. Regions with as-sociations that achieved statistical signif-icance (P � .05) after standard FDRorrection for multiple comparisons arehown in Figure 2 and Tables 3 and 4.horioamnionitis was primarily associ-ted with a thinner cortex in multiple re-ions within the frontal and temporalobe as shown in Figure 2 (blue overlays).n the frontal lobe, the majority of theffects were bilateral with the exceptionf the pars opercularis in which there was
d
tlyaysitis
J Ob
mn)
(29..........
404.........
–9).........
–9).........
7%).........
%).........
%).........
2%)
.........
%)
.........
rison
unilateral effect in the left hemisphere.
an Journal of Obstetrics & Gynecology 384.e4

loceplcciTonslwofocagccll
crdfpgawn
Hatfield. Chorioamnionitis exposure and MRI findings. Am J Obstet Gynecol 2011.
SMFM Papers www.AJOG.org
The most prominent findings were seenin the precentral (motor cortex), para-central (supplementary motor), parsopercularis (Broca’s area), and lateral or-bital frontal regions. In the temporallobe, the largest group differences wereobserved in the superior temporal (audi-tory cortex) region. Areas of greater cor-tical thickness in the chorioamnionitisgroup were also observed in a few dis-tinct anatomic loci in the frontal andtemporal lobes (Figure 2, red overlays),primarily the caudal middle frontalcortex.
As illustrated in Figure 2 (red over-ays), in areas of the limbic, parietal, andccipital cortex, prenatal exposure tohorioamnionitis was associated with ar-as of higher cortical thickness as com-ared to the comparison group. In the
imbic lobe, there was a predominance ofortical thickening in all regions of theingulate cortex (bilateral anterior, rightsthmus, and left posterior cingulate).he parietal lobe was significant for areasf increased thickness in the right precu-eus and left postcentral gyrus (primaryomatosensory cortex). In the occipitalobe, areas of increased cortical thicknessere observed bilaterally in the lateralccipital (visual association) region. Aew distinct loci within the parietal andccipital lobes demonstrated areas ofortex that were thinner in the chorio-mnionitis group than the comparisonroup (Figure 2, blue overlays). Thinnerortices were observed in the group ofhildren with chorioamnionitis in theeft inferior parietal and right posterioringual regions.
For illustrative purposes, Figure 3 showsortical thickness data with box plots in 4epresentative brain regions where groupifferences were observed. Data are shown
or the pars opercularis and superior tem-oral regions where the chorioamnionitisroup had significantly thinner corticesnd the anterior and isthmus cingulatehere the chorioamnionitis group had sig-ificantly thicker cortices.
Volumetric differences in subcorticalgray matterSubcortical analysis revealed that theright hippocampus was significantly
smaller in children exposed to chorio-384.e5 American Journal of Obstetrics & Gynecolo
TABLE 3Chorioamnionitis thinner than comparison group
Brain regionChorioamnionitiscortical thickness
Comparisoncortical thickness t score
Frontal lobe.....................................................................................................................................................................................................................................
Superior frontal............................................................................................................................................................................................................................
Left hemisphere 2.82 3.06 3.78............................................................................................................................................................................................................................
Right hemisphere 3.12 3.30 2.06.....................................................................................................................................................................................................................................
Precentral............................................................................................................................................................................................................................
Left hemisphere 2.20 2.40 2.56............................................................................................................................................................................................................................
Right hemisphere 2.85 3.09 3.14.....................................................................................................................................................................................................................................
Paracentral............................................................................................................................................................................................................................
Left hemisphere 3.00 3.28 2.28............................................................................................................................................................................................................................
Right hemisphere 2.58 2.86 2.52.....................................................................................................................................................................................................................................
Pars opercularis............................................................................................................................................................................................................................
Left hemisphere 2.77 3.13 3.60.....................................................................................................................................................................................................................................
Lateral orbital-inferior............................................................................................................................................................................................................................
Left hemisphere 3.11 3.48 2.64............................................................................................................................................................................................................................
Right hemisphere 3.30 3.58 3.16.....................................................................................................................................................................................................................................
Paracentral............................................................................................................................................................................................................................
Left hemisphere 2.50 2.82 2.28............................................................................................................................................................................................................................
Right hemisphere 2.58 2.86 2.52.....................................................................................................................................................................................................................................
Rostral middle-inferior............................................................................................................................................................................................................................
Left hemisphere 2.96 3.13 1.91............................................................................................................................................................................................................................
Right hemisphere 2.84 3.08 2.18.....................................................................................................................................................................................................................................
Caudal middle............................................................................................................................................................................................................................
Left hemisphere 2.80 3.01 2.02............................................................................................................................................................................................................................
Right hemisphere 3.49 3.69 2.26..............................................................................................................................................................................................................................................
Temporal lobe.....................................................................................................................................................................................................................................
Superior temporal............................................................................................................................................................................................................................
Left hemisphere 3.00 3.28 2.36............................................................................................................................................................................................................................
Right hemisphere 3.44 3.70 2.16.....................................................................................................................................................................................................................................
Middle temporal............................................................................................................................................................................................................................
Left hemisphere 3.03 3.41 2.71............................................................................................................................................................................................................................
Right hemisphere 2.86 3.09 2.64.....................................................................................................................................................................................................................................
Inferior temporal............................................................................................................................................................................................................................
Left hemisphere 3.23 3.57 2.11.....................................................................................................................................................................................................................................
Superior temporal sulcus............................................................................................................................................................................................................................
Right hemisphere 2.78 3.00 3.16.....................................................................................................................................................................................................................................
Anterior fusiform............................................................................................................................................................................................................................
Left hemisphere 3.12 3.45 3.06..............................................................................................................................................................................................................................................
Parietal lobe.....................................................................................................................................................................................................................................
Inferior parietal............................................................................................................................................................................................................................
Left hemisphere 2.94 3.22 2.14............................................................................................................................................................................................................................
Right hemisphere 2.86 3.05 2.10.....................................................................................................................................................................................................................................
Supramarginal............................................................................................................................................................................................................................
Left hemisphere 3.23 3.60 2.39..............................................................................................................................................................................................................................................
Occipital lobe.....................................................................................................................................................................................................................................
Posterior lingual............................................................................................................................................................................................................................
Right hemisphere 1.88 2.20 2.77..............................................................................................................................................................................................................................................
All data shown (mean cortical thickness in millimeters and t scores) P � .05 after false discovery rate correction.
gy OCTOBER 2011

.vsg
Hatfield. Chorioamnionitis exposure and MRI findings. Am J Obstet Gynecol 2011.
www.AJOG.org SMFM Papers
OCTOBER 2011 Americ
amnionitis as compared to the compari-son group (3957 � 283 vs 4201 � 533cm3; P � .05) and the left lateral ventriclewas significantly larger in the chorioam-nionitis-exposed group (5830 cm3) ascompared to the comparison group(5830 � 2610 vs 4031 � 2150 cm3; P �009) after controlling for intracranialolume. No other subcortical structureshowed significant differences betweenroups.
COMMENTTo our knowledge, this is the first reportdemonstratinglong-termalterationsinbrainmorphology associated with prenatal ex-posure to chorioamnionitis. We foundprofound and persisting differences be-tween groups, which suggests that chorio-amnionitis is associated with global conse-quences for brain development. Althoughthere were diffuse changes in cortical thick-ness in all lobes, the pattern was consis-tent with more areas of thinness in thefrontal and temporal lobes and more ar-eas of thickness in the limbic, parietal,and occipital lobes in children exposedto chorioamnionitis. Although it is notknown why both thinness and thicknessin cortical tissue were observed, we spec-ulate that this observation may representa disorganized pattern of brain develop-ment resulting from disruptions in nor-mal developmental trajectories as thereare clear deviations from expected pat-terns seen in the age-matched compari-son group. Brain development appears to becompromised among children exposed tochorioamnionitis suggesting that these chil-dren may be at risk for neurodevelopmentalimpairments.
The findings from our study suggestthe potential for diverse and widespreadcognitive deficits associated with expo-sure to chorioamnionitis documentingthe need for studies of cognitive func-tioning in children exposed to chorio-amnionitis. Indeed, damage to many ofthe regions altered in the chorioamnio-nitis group is associated with knownfunctional deficits. For example, large ef-fects were found in many regions that areimportant for learning and memory(cingulate and lateral orbital frontal cor-
TABLE 4Chorioamnionitis group thicker than comparison group
Brain regionChorioamnionitiscortical thickness
Comparisoncortical thickness t score
Frontal lobe.....................................................................................................................................................................................................................................
Superior frontal............................................................................................................................................................................................................................
Left hemisphere 4.00 3.78 1.99.....................................................................................................................................................................................................................................
Lateral orbital-superior............................................................................................................................................................................................................................
Right hemisphere 3.35 2.93 2.23.....................................................................................................................................................................................................................................
Rostral middle superior............................................................................................................................................................................................................................
Left hemisphere 2.93 2.68 2.84.....................................................................................................................................................................................................................................
Caudal middle............................................................................................................................................................................................................................
Left hemisphere 3.09 2.77 3.28............................................................................................................................................................................................................................
Right hemisphere 3.00 2.81 2.65..............................................................................................................................................................................................................................................
Temporal lobe.....................................................................................................................................................................................................................................
Insular ridge............................................................................................................................................................................................................................
Left hemisphere 3.55 3.20 3.25............................................................................................................................................................................................................................
Right hemisphere 3.30 3.01 2.80.....................................................................................................................................................................................................................................
Superior sulcus............................................................................................................................................................................................................................
Left hemisphere 2.91 2.46 3.22.....................................................................................................................................................................................................................................
Posterior fusiform............................................................................................................................................................................................................................
Right hemisphere 3.43 3.18 2.5.....................................................................................................................................................................................................................................
Inferior temporal............................................................................................................................................................................................................................
Right hemisphere 3.55 3.26 2.17..............................................................................................................................................................................................................................................
Limbic lobe.....................................................................................................................................................................................................................................
Isthmus cingulate............................................................................................................................................................................................................................
Right hemisphere 3.45 3.08 2.82.....................................................................................................................................................................................................................................
Anterior cingulate............................................................................................................................................................................................................................
Left hemisphere 4.00 3.74 1.87............................................................................................................................................................................................................................
Right hemisphere 3.35 3.06 2.66.....................................................................................................................................................................................................................................
Posterior cingulate............................................................................................................................................................................................................................
Left hemisphere 2.89 2.55 2.12..............................................................................................................................................................................................................................................
Parietal lobe.....................................................................................................................................................................................................................................
Postcentral............................................................................................................................................................................................................................
Left hemisphere 2.25 1.86 2.59.....................................................................................................................................................................................................................................
Precuneus............................................................................................................................................................................................................................
Right hemisphere 3.22 2.95 2.28.....................................................................................................................................................................................................................................
Inferior parietal............................................................................................................................................................................................................................
Left hemisphere3.06 2.77 2.44............................................................................................................................................................................................................................
Right hemisphere.....................................................................................................................................................................................................................................
Superior parietal............................................................................................................................................................................................................................
Left hemisphere 2.78 2.54 1.86............................................................................................................................................................................................................................
Right hemisphere 3.07 2.82 1.91..............................................................................................................................................................................................................................................
Occipital lobe.....................................................................................................................................................................................................................................
Lateral occipital............................................................................................................................................................................................................................
Left hemisphere 2.29 2.03 2.26............................................................................................................................................................................................................................
Right hemisphere 2.74 2.58 1.97.....................................................................................................................................................................................................................................
Anterior lingual............................................................................................................................................................................................................................
Right hemisphere 2.94 2.96 2.18..............................................................................................................................................................................................................................................
All data shown (mean cortical thickness in millimeters) P � .05 after false discovery rate correction.
tex; hippocampus) and executive func-
an Journal of Obstetrics & Gynecology 384.e6

i6
ttiaipcubdrtc
tctipfwactbwta
swsfrtdfijllnt
lssbri
stflaweosfbi
utb
SMFM Papers www.AJOG.org
tions (caudal middle frontal cortex).Broca’s area, which is important in lan-guage processing, was one region withthe most significant reductions in corti-cal thickness in the chorioamnionitisgroup. Additional areas that were foundto have significant differences and are offunctional significance included audi-tory (superior temporal), visual (lateraloccipital), motor (precentral), and so-matosensory (postcentral) processingagain illustrating the range of potentialdysfunction.
Activation of the fetal inflammatory re-sponse to maternal infection is presumedtobethepathogenesisofneurologic injury,and is characterized by systemic activationof the innate fetal immune system. Manymarkers of the fetal inflammatory re-sponse have been linked to adverse neona-tal outcomes including increased risk forPVL and cerebral palsy.31,32 These markersncluding elevated levels of interleukin-,33-35 tumor necrosis factor-�,33 and ma-
trix metalloproteinase-836 and their po-tential role in neurologic injury has beenstudied in both the clinical and experimen-tal literature. Hagberg and Mallard37 ex-ensively reviewed the experimental litera-ure and endorse the role of inflammationn mediating central nervous system dam-ge, which renders it more vulnerable tonsult through the release of cytokines,rostaglandins, trophic factors, and mi-roglial activation. Inflammatory byprod-cts from infection therefore may plausi-ly act in ways to manifest a wide array ofeficits, some may be extreme such as ce-ebral palsy and others more subtle. None-heless, these deficits may have pervasiveonsequences for neurologic development.
A strength of this study is the long-erm follow-up of a well-characterizedohort of children assessed 6-10 years af-er exposure to chorioamnionitis. Strictnclusion and exclusion criteria were ap-lied in an attempt to isolate specific ef-
ects of chorioamnionitis. For example,e excluded all cases with preeclampsia
s the pathophysiology of this diseaseould have confounded the findings ofhis study. Our study, however, is limitedy sample size. Further, our cohorts wereell matched on other variables known
o affect brain structure (ie, gestational
ge, birthweight, and age at MRI). De-384.e7 American Journal of Obstetrics & Gynecolo
pite our small sample size, our resultsere robust and stood up to stringent
tatistical analyses with FDR correctionor multiple comparisons. Further, ouresults cannot be explained by outliers ashe individual cortical thickness plotsemonstrate compelling evidence ofndings affecting the majority of sub-
ects within a group. One report in theiterature evaluated short-term neuro-ogic consequences of antenatal and neo-atal characteristics with MRI in pre-
erm infants at term equivalent age.15
They concluded that abnormal findingson MRI were associated with postnatalhypotension and sepsis but not with cho-rioamnionitis. However, their analysiswas limited to 8 small predefined ran-domly selected brain regions with theopportunity to miss important findingsin regions not represented in the pre-defined areas. Additionally, the data
FIGURE 3Representative brain regions showindividual data for cortical thickne
ox plots showing median cortical thickness and uubject point data for cortical thickness(y-axis iata) demonstrates 2 regions with thicker cortexircles point data) demonstrates 2 regions with t, left hemisphere; R, right hemisphere.
atfield. Chorioamnionitis exposure and MRI findings. Am J
from Chau et al15 do not address the s
gy OCTOBER 2011
ong-term differences evaluated in ourtudy. We believe a major strength of ourtudy is the methodology using a whole-rain approach to observe long-term neu-ologic changes, 6-10 years after exposure,n this carefully selected cohort of children.
Clearly, studies with larger sampleizes are needed to attempt to replicatehese findings as well as to clarify the in-uence of other aspects of clinical man-gement on outcomes. We questionhether or not larger morphologic differ-
nces are observed when there is evidencef activation of the fetal inflammatory re-ponse as demonstrated by the presence ofunisitis. Only with future studies will theree hope of directing care that will lead to
mproved clinical outcomes.The results of our study suggest that in
tero exposure to chorioamnionitis hashe potential to change the trajectory ofrain development with pervasive con-
er and lower quartiles are overlaid with individualillimeters). Upper panel (red-filled circles pointchorioamnionitis group. Lower panel (blue-filleder cortex in chorioamnionitis group.
tet Gynecol 2011.
ingss
B pps n md inc hinnL
H Obs
equences that last at least into child-

www.AJOG.org SMFM Papers
hood. This disruption in neurodevelop-ment may further increase susceptibilityfor impaired cognitive and motor func-tion as well as psychiatric and neurode-velopmental disorders.38,39 f
ACKNOWLEDGMENTSThe assistance of Megan Blair, Natalie Hernan-dez, Kourney Osorio, Angela Pike, and Chris-tine Preslicka is gratefully acknowledged.
REFERENCES1. Alexander JM, Gilstrap LC, Cox SM, McIntireDM, Leveno KJ. Clinical chorioamnionitis andthe prognosis for very low birth weight infants.Obstet Gynecol 1998;91:725-9.2. Bashiri A, Burstein E, Mazor M. Cerebralpalsy and fetal inflammatory response syn-drome: a review. J Perinat Med 2006;34:5-12.3. Dammann O, Leviton A. Maternal intrauterineinfection, cytokines, and brain damage in thepreterm newborn. Pediatr Res 1997;42:1-8.4. Grether JK, Nelson KB. Maternal infectionand cerebral palsy in infants of normal birth-weight. JAMA 1997;278:207-11.5. Thomas W, Speer CP. Chorioamnionitis:important risk factor of innocent bystander forneonatal outcome. Neonatology 2010;99:177-87.6. Leviton A, Paneth N. White matter damage inpreterm newborns–an epidemiologic perspec-tive. Early Hum Dev 1990;24:1-22.7. Wu YW, Colford JM Jr. Chorioamnionitis as arisk factor for cerebral palsy: a meta-analysis.JAMA 2000;284:1417-24.8. Yoon BH, Kim CJ, Romero R, et al. Experi-mentally induced intrauterine infection causesfetal brain white matter lesions in rabbits. Am JObstet Gynecol 1997;177:797-802.9. Gavilanes AW, Strackx E, Kramer BW, et al.Chorioamnionitis induced by intraamniotic lipo-polysaccharide resulted in an interval-depen-dent increase in central nervous system injury inthe fetal sheep. Am J Obstet Gynecol 2009;200:437.10. Inder TE, Warfield SK, Wang H, Hüppi PS,Volpe JJ. Abnormal cerebral structure is pres-ent at term in premature infants. Pediatrics2005;115:286-94.11. Peterson BS, Vohr B, Staib LH, et al. Re-gional brain volume abnormalities and long-term cognitive outcome in preterm infants.
JAMA 2000;284:1973-4.12. Davis EP, Buss C, Muftuler T, et al. Chil-dren’s brain development benefits from longergestation. Front Psychol 2011;2:1-7.13. Romero R, Espinoza J, Goncalves LF, et al.The role of inflammation and infection in pretermbirth. Semin Reprod Med 2007;25:21-39.14. Gaudet LM, Flavin MB, Islam O, et al. Diffu-sion MRI brain findings in neonates exposed tochorioamnionitis: a case series. J ObstetGynaecol Can 2009;31:497-503.15. Chau V, Poskitt KJ, McFadden DE, et al.Effect of chorioamnionitis on brain developmentand injury in premature newborns. Ann Neurol2009;66:155-64.16. American College of Obstetricians and Gy-necologists. ACOG practice bulletin No. 101:ultrasonography in pregnancy. Obstet Gynecol2009;113:451-61.17. Wechsler D. Wechsler adult intelligencescale. 3rd ed. San Antonio: Psychological Corp;1997.18. Sled JG, Zijdenbos AP, Evans AC. A non-parametric method for automatic correction ofintensity nonuniformity in MRI data. IEEE TransMed Imaging 1998;17:87-97.19. Segonne F, Dale AM, Busa E, et al. A hybridapproach to the skull stripping problem in MRI.Neuroimage 2004;22:1060-75.20. Fischl B, Salat DH, Busa E, et al. Wholebrain segmentation: automated labeling of neu-roanatomical structures in the human brain.Neuron 2002;33:341-55.21. Fischl B, Salat DH, van der Kouwe, et al.Sequence-independent segmentation of mag-netic resonance images. Neuroimage 2004a;23:S69-84.22. Dale AM, Fischl B, Sereno MI. Cortical sur-face-based analysis, I: segmentation and sur-face reconstruction. Neuroimage 1999;9:179-94.23. Dale AM, Sereno MI. Improved localizationof cortical activity by combining EEG and MEGwith MRI cortical surface reconstruction: a linearapproach. J Cogn Neurosci 1993;5:162-76.24. Fischl B, Dale AM. Measuring the thicknessof the human cerebral cortex from magneticresonance images. Proc Natl Acad Sci U S A2000;97:11050-5.25. Fischl B, Sereno MI, Dale AM. Cortical sur-face-based analysis, II: inflation, flattening, anda surface-based coordinate system. Neuroim-age 1999a;9:195-207.26. Fischl B, Sereno MI, Tootell RB, Dale AM.High-resolution intersubject averaging and acoordinate system for the cortical surface. Hum
Brain Mapp 1999b;8:272-84.OCTOBER 2011 Americ
27. Rosas HD, Liu AK, Hersch S, et al. Regionaland progressive thinning of the cortical ribbon inHuntington’s disease. Neurology 2002;58:695-701.28. Kuperberg GR, Broome MR, McGuire PK,et al. Regionally localized thinning of the cere-bral cortex in schizophrenia. Arch Gen Psychi-atry 2003;60:878-88.29. Salat DH, Buckner RL, Snyder AZ, et al.Thinning of the cerebral cortex in aging. CerebCortex 2004;14:721-30.30. Genovese CR, Lazar NA, Nichols T. Thresh-olding of statistical maps in functional neuroim-aging use the false discovery rate. Neuroimage2002;15:870-8.31. Gomez R, Romero R, Ghezzi F, Yoon BH,Mazor M, Berry SM. The fetal inflammatory re-sponse syndrome. Am J Obstet Gynecol 1998;179:194-202.32. Gotsch F, Romero R, Kusanovic JP, et al.The fetal inflammatory response syndrome. ClinObstet Gynecol 2007;50:652-83.33. Duggan PJ, Maalouf EF, Watts TL, et al.Intrauterine T-cell activation and increased pro-inflammatory cytokine concentrations in pre-term infants with cerebral lesions. Lancet2001;358:1699-700.34. Viscardi RM, Muhumuza CK, Rodriguez A,et al. Inflammatory markers in intrauterine andfetal blood and cerebrospinal fluid compart-ments are associated with adverse pulmonaryand neurologic outcomes in preterm infants.Pediatr Res 2004;55:1009-17.35. Yoon BH, Romero R, Yang SH, et al. Inter-leukin-6 concentrations in umbilical cordplasma are elevated in neonates with whitematter lesions associated with periventricularleukomalacia. Am J Obstet Gynecol 1996;174:1433-40.36. Moon JB, Kim JC, Yoon BH, et al. Amnioticfluid matrix metalloproteinase-8 and the devel-opment of cerebral palsy. J Perinat Med2002;30:301-6.37. Hagberg H, Mallard C. Effect of inflamma-tion on central nervous system developmentand vulnerability. Curr Opin Neurol 2005;18:117-23.38. Kates WR, Burnett CP, Eliez S, et al. Neu-roanatomic variation in monozygotic twin pairsdiscordant for the narrow phenotype for autism.Am J Psychiatry 2004;161:539-46.39. Koenigs M, Grafman J. The functional neu-roanatomy of depression: distinct roles for ven-tromedial and dorsolateral prefrontal cortex.
Behav Brain Res 2009;201:239-43.an Journal of Obstetrics & Gynecology 384.e8