
Mad as a Hatter Deepti Deshpande, MBBS, MPH, FAAP Assistant Professor, Pediatrics and Public Health...
28
Mad as a Hatter Deepti Deshpande, MBBS, MPH, FAAP Assistant Professor, Pediatrics and Public Health University of Arizona June 2013
-
Upload
jasmine-jenkins -
Category
Documents
-
view
220 -
download
1
Transcript of Mad as a Hatter Deepti Deshpande, MBBS, MPH, FAAP Assistant Professor, Pediatrics and Public Health...
Mad as a Hatter
Deepti Deshpande, MBBS, MPH, FAAPAssistant Professor, Pediatrics and Public Health
University of ArizonaJune 2013
Initial Presentation
20 month old girl admitted with: • Intermittent abdominal pain for 7 weeks. • Diarrhea off and on for 4 weeks.• Increased fussiness and fatigue.• Tactile low grade fevers off and on for 7
weeks. Night sweats. • 5 lbs weight loss. • Brought to the ER because her hands/ toes
were turning cold and purple over past day.
Initial Presentation
• Several PCP, Urgent care and ER visits during this time.
• Diagnosed with a viral illness, constipation, ear infection. Received 1 course of antibiotics. Entire family treated for parasites in Mexico a few weeks prior.
• No sick contacts, No animal exposure.• Travels to Mexico frequently but no other travel.
Initial Thoughts: Differential Diagnoses
• Infectious: infectious gastroenteritis, parasitic illness, pyelonephritis, intra-abdominal abscess, coccidiodomycosis, tuberculosis.
• Non-infectious: nutritional deprivation and deficiencies, inflammatory bowel disease, thyroid disorder, malignancy, other systemic illness.
Additional HistoryOn further directed questioning/ ROS:
• Regression of motor milestones: Over past 7 weeks, stopped running, started walking very slowly and over time stopped walking. Poor balance and falls. Lack of interest in play.
• No suggestion of pain.
• Scalp hair loss and hair pulling for ~ 2 weeks
Physical Exam• Temp 36.8, HR 162, RR 30, BP 122/74, Sats 100% on RA.
– Weight= 9.6 kg (10th percentile), height and head circumference 10-25th percentiles.
• Irritable. Consolable for brief periods. Pulling her hair.
• Cool hands and feet with a dusky bluish-purple color. Centrally well perfused and warm. Distal pulses 2+.
• Abnormal neurological exam: Walks few steps very slowly with some gait instability. Loses balance easily when tries to squat to pick up a toy. Moves all extremities well but unable to stoop and recover. Patellar deep tendon reflexes 2+ but unable to elicit ankle reflexes. Normal tone and strength in the upper body. Fine motor exam appears normal. Tone decreased in the lower extremities. Follows some commands inconsistently. Says a few words.
• Remaining exam within normal limits.
Clinical Presentation in a Nutshell• Neurological: B/L lower extremity weakness and
hypotonia and regression of motor milestones. Gait instability. Inability to elicit ankle reflexes.
• Cardiovascular: Hypertension and Tachycardia.
• Gastrointestinal: Intermittent abdominal pain and diarrhea for several weeks.
• Constitutional: Irritability, weight loss, sweating and dusky hands/ feet. Low grade fever.
Differential Diagnoses
• Guillian Barre syndrome, ADEM, transverse myelitis, encephalitis, intracranial process.
• Endocrine disorders.• Neuroendocrine disorders.• Neuro-degenerative or muscle disorders. • Toxic ingestions.• Genetic disorders.• Metabolic disorders.
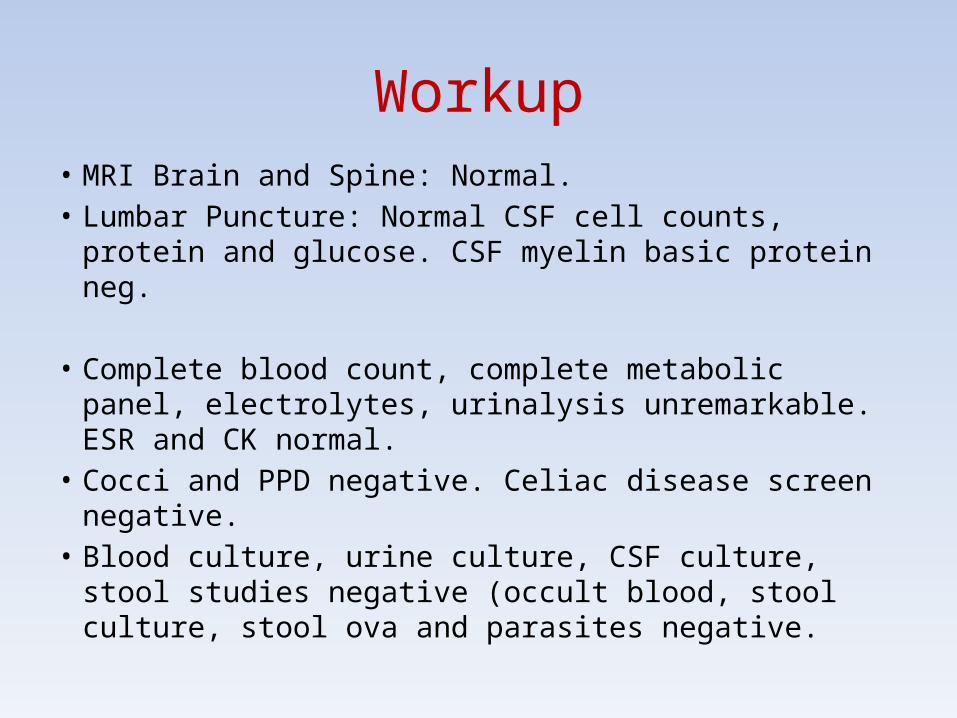
Workup• MRI Brain and Spine: Normal.• Lumbar Puncture: Normal CSF cell counts, protein and
glucose. CSF myelin basic protein neg.
• Complete blood count, complete metabolic panel, electrolytes, urinalysis unremarkable. ESR and CK normal.
• Cocci and PPD negative. Celiac disease screen negative. • Blood culture, urine culture, CSF culture, stool studies
negative (occult blood, stool culture, stool ova and parasites negative.
Workup
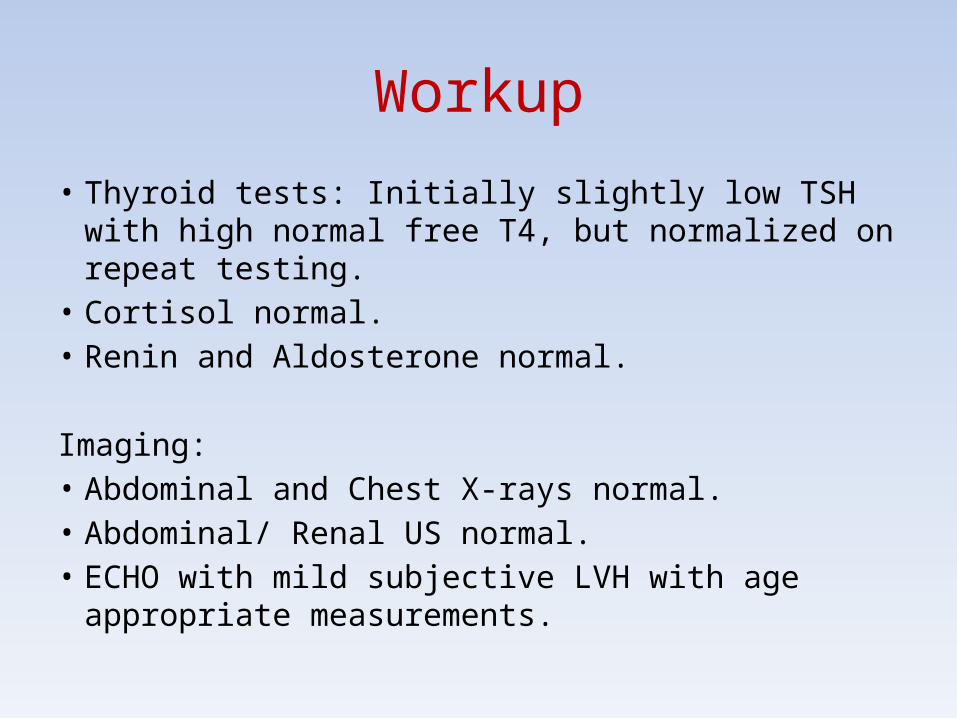
• Thyroid tests: Initially slightly low TSH with high normal free T4, but normalized on repeat testing.
• Cortisol normal.• Renin and Aldosterone normal.
Imaging:• Abdominal and Chest X-rays normal.• Abdominal/ Renal US normal.• ECHO with mild subjective LVH with age appropriate
measurements.
Workup
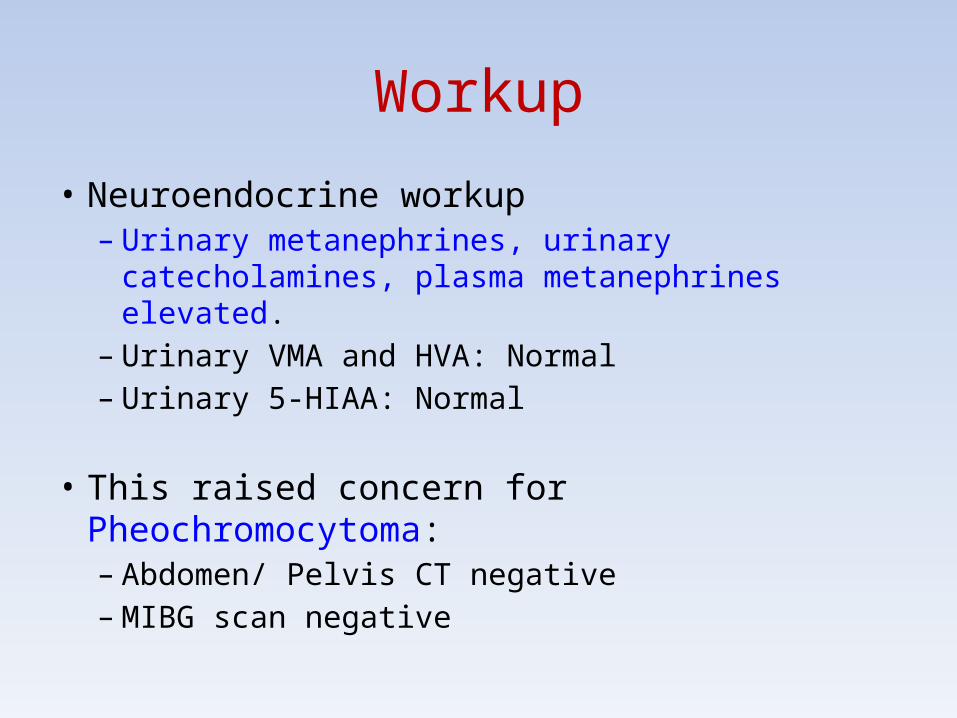
• Neuroendocrine workup– Urinary metanephrines, urinary catecholamines,
plasma metanephrines elevated.– Urinary VMA and HVA: Normal– Urinary 5-HIAA: Normal
• This raised concern for Pheochromocytoma:– Abdomen/ Pelvis CT negative– MIBG scan negative
What have we ruled out? Now what?
• GBS, ADEM, intracranial or spine abnormality• Infectious etiologies• Thyroid disorders• Hyperaldosteronism states• Pheochromocytoma, carcinoid tumor,
neuroblastoma
Further Testing revealed…
ELEVATED MERCURY LEVELS
Day5 Day13 Day17 6 months
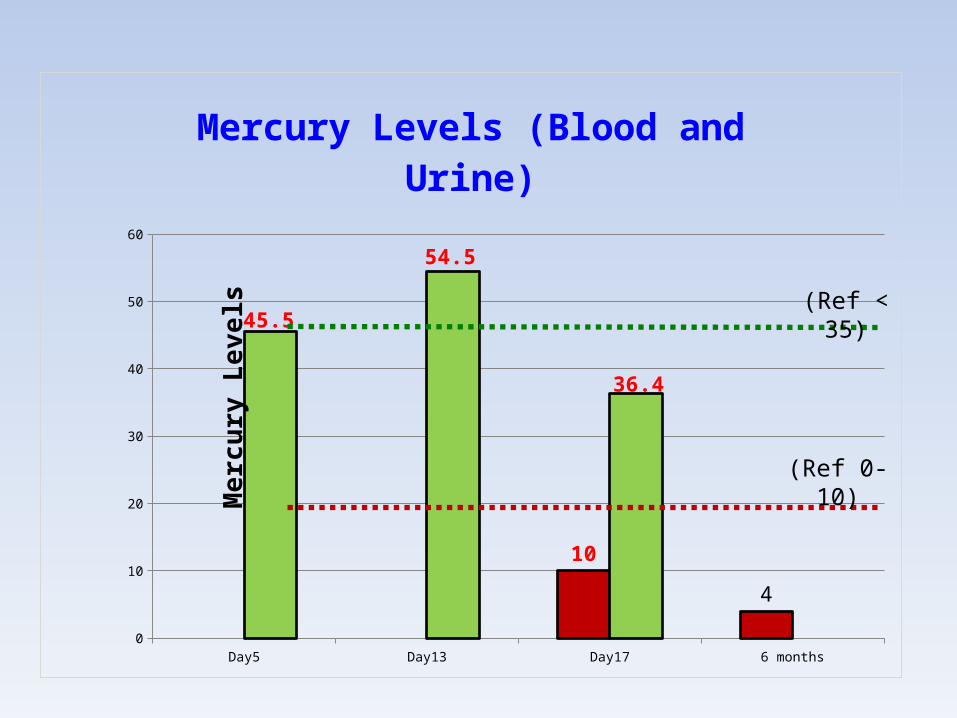
Blood Mercury ug/L NaN NaN 10 4
Urine Mercury ug/gCR 45.5 54.5 36.4 NaN
5
15
25
35
45
55
45.5
54.5
36.4
10
4
Mercury Levels (Blood and Urine)
Mer
cury
Lev
els (Ref < 35)
(Ref 0-10)
Diagnosis: Mercury Toxicity• Mercury toxicity
– Clinical syndrome suggestive of mercury toxicity. – Elevated urinary and blood mercury levels.– Elevated urinary beta2 microglobulin levels indicate possible
early kidney injury.
• No chelation therapy recommended.– Mercury levels not too high and clinical symptoms not severe
with spontaneous improvement.
• Etiology unclear but suspected due to excessive seafood intake.– Child ate 2-3 servings of shrimp/ tuna almost daily. – No other exposure sources identified on detailed questioning.
Hospital Course
• Admitted to the Pediatric Floor for 23 days.
• Hypertension and Tachycardia: Hypertension controlled using PRN Hydralazine and subsequently started on Propranolol.
• Followed by Nephrology, Endocrinology, Neurology,
Toxicology, Ophthalmology, Cardiology, PT/ OT.
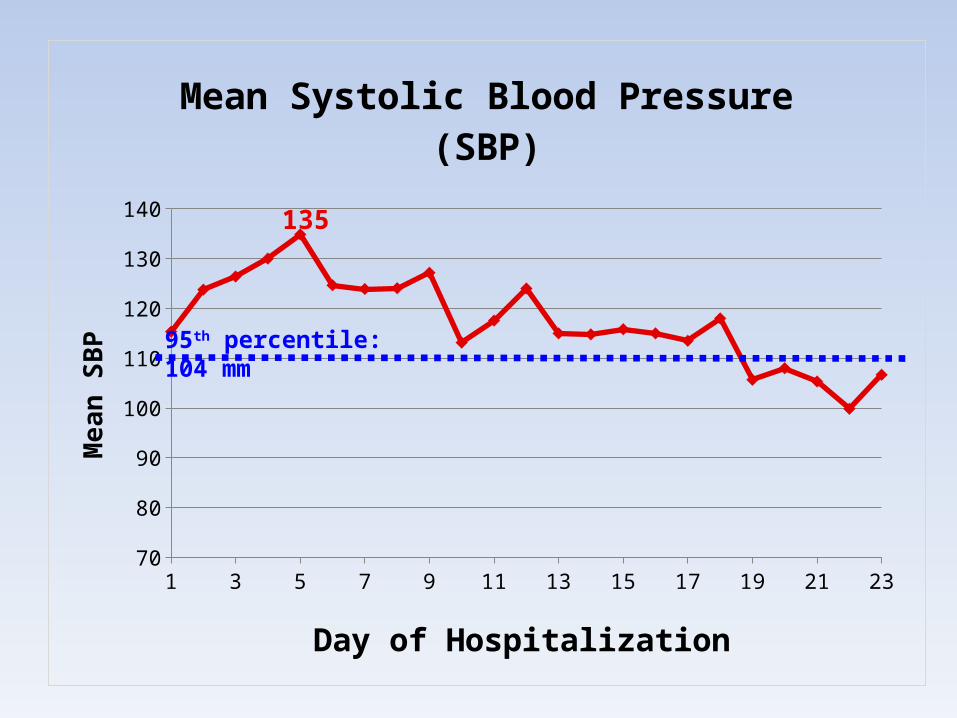
1 3 5 7 9 11 13 15 17 19 21 2370
80
90
100
110
120
130
140135
Mean Systolic Blood Pressure (SBP)
Day of Hospitalization
Mea
n SB
P
95th percentile: 104 mm
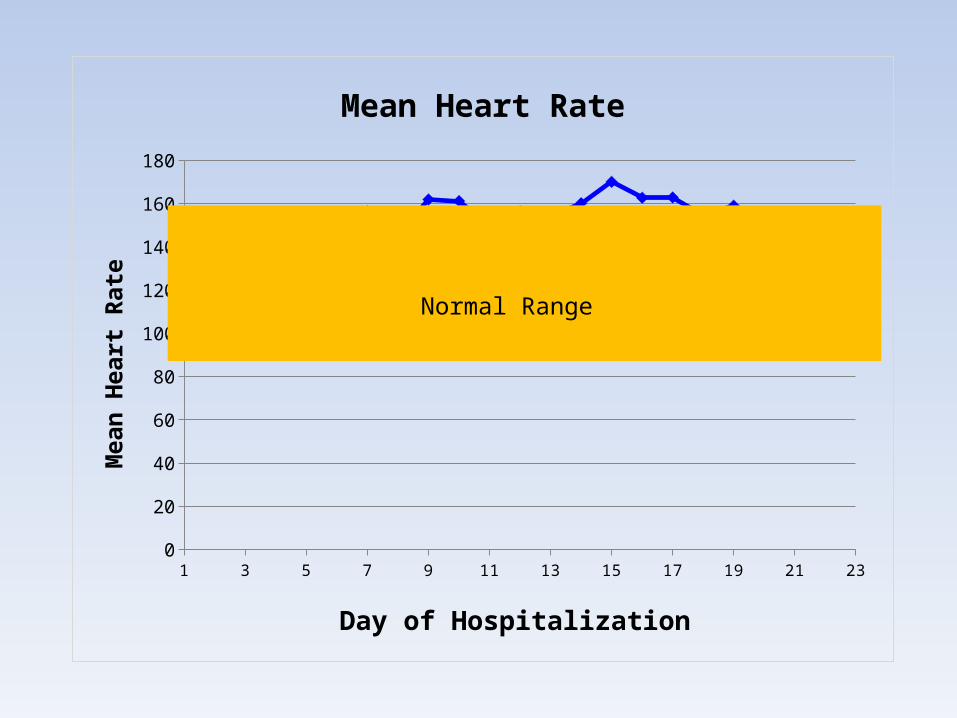
1 3 5 7 9 11 13 15 17 19 21 230
20
40
60
80
100
120
140
160
180
Mean Heart Rate
Day of Hospitalization
Mea
n H
eart
Rat
e
Normal Range
Hospital Course
• Lower extremity weakness improved. Walking well prior to discharge. PT ongoing.
• Dusky hands and feet resolved.
• Abdominal pain, diarrhea, sweating resolved. Afebrile during stay.
• Irritability resolved and child more playful and interactive.
Discharge Plan• Recommended avoiding all seafood.
• Propranolol for hypertension.
• Outpatient management– PCP follow up– Nephrology follow up– Toxicology follow up – Repeat mercury levels in 6 months.
Long Term Outcome
• Mercury levels decreased spontaneously without any further seafood exposure.
• Hypertension and tachycardia resolved over the next 2 months. Propranolol stopped. Repeat ECHO normal.
• All systemic, gastrointestinal, cardiovascular and neurological symptoms resolved and back to baseline within about 2-3 months post discharge.
• Meeting age appropriate developmental milestones.
MERCURY POISONING
Forms of Mercury• Elemental or metallic mercury
– Highly volatile- vapors inhaled.– Pulmonary manifestations most severe.– Sources: Thermometers, sphygmomanometers, metallurgy.
• Inorganic salts: Mercurous/ Mercuric salts– Well absorbed through skin, some via GI tract.– Gastrointestinal and Renal manifestations.– Sources: Paints, topical antiseptics, bleaching creams etc.
• Organic: methyl/ ethyl/ phenyl mercury– Almost 100% absorbed via GI tract.– Primarily neurological manifestations.– Sources: Seafood, vaccinations etc.
Mercury Toxicity: Clinical Features
Clinical presentation depends on the type of mercury, route, dose and duration of exposure.
• Acrodynia: Rare idiosyncratic reaction in children. • Neurological: CNS/ Peripheral nerves• Gastrointestinal• Pulmonary• Renal• Skin/ Gingiva/ Eyes
Acrodynia
• Rare idiosyncratic syndrome of mercury toxicity in young children.
• Symptoms may include irritability, erythema of hands and feet, photophobia, hypotonia, painful extremities, hypertension and tachycardia etc.
Mercury Toxicity• Laboratory Diagnosis– Urinary lead levels– Blood lead levels
• Pheochromocytoma like syndrome– Elevated plasma and urine catecholamines and
metanephrines– Inactivates COMT
• Treatment: Chelation used in severe symptomatic children. – DMSA commonly used.
Consider Mercury Toxicity in your differential
Unexplained hypertension with a pheochromocytoma like
presentation, neurological symptoms, developmental
regression, renal, gastrointestinal or skin symptoms.

Mad as a Hatter!
Questions?


















