Lumbar and sacral Biomechanics
43
Spine
-
Upload
sreeraj-s-r -
Category
Education
-
view
4.526 -
download
9
Transcript of Lumbar and sacral Biomechanics

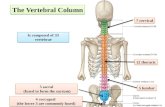
Spine

Sreeraj S R
BIOMECHANICS

Sreeraj S R
Lumbar Anatomy
� 5 vertebrae L1-L5
� 5 intervertebral discs
� 5 pair of exiting nerve roots
� Lumbar lordosis L1-S1 ranges from 30°–80°
� The apex of lumbar lordosis L3-L4
1
2
3
4
5

Sreeraj S R
Lumbar Spine Anatomy
Typical lumbar vertebra (L2)
� Body
� Vertebral foramen/canal
� Intervertebral foramen
� Pedicle
� Transverse process
� Lamina
� Spinous process
� Facet joints
� Pars interarticularis
inferior
Superior
Anterior (oblique)
A Lateral P
Posterior (oblique)
Superior
Inferiorsuperior

Sreeraj S R
Intervertebral Disc
� Soft fibro-cartilaginous cushions
� Between two vertebra
� Allows some motion
� Serve as shock absorbers
� Total – 23 discs
� ¼ th of the spinal column's length
� Avascular
� Nutrients diffuse through end plates
� Collagen

Sreeraj S R
Intervertebral Disc
NUCLEUS PULPOSUS
� Has more water and PGs
� PG are macro-molecules
� Attract and retain water
� Hydrophilic gel–like matter � Resists compression
� Amount of water
� Activity related
� Varies throughout the day

Sreeraj S R
Intervertebral Disc
NUCLEUS PULPOSUS
� Eccentrically positioned posteriorly
� Young & healthy, 90% water, bound to proteoglycans
� Aging> desiccation> increase viscosity> fissuring
� Young nucleus> even distribution of load
� Old nucleus> undue concentration on vertebral body edges
� Small displacement w/ ROM, ball-bearing like
� Compressive stress predominates

Sreeraj S R
Intervertebral Disc
NUCLEUS PULPOSUS� Pascal’s law: Fluid mass within closed
container> local increase in pressure> transmit around entire side wall (annulus)
� Nucleus pulpous imbibes water
� Develops internal pressure
� Pressure exerted in all directions
� Lateral forces against annulus
� Superiorly and inferiorly directed forces against end plates
� Increases stiffness of end plate and annulus fibrosus

Sreeraj S R
Intervertebral Disc
ANNULUS FIBROSUS
� Strong radial tire–like structure
� Series of lamellae
� Concentric sheets of collagen fibers
� Connected to end plates
� Orientated at various angles
� Under compression� Become horizontal
� Encloses nucleus pulposus

Sreeraj S R
Intradiscal Pressure
INTRADISCAL PRESSURE
� Compressive loads in vivo: 500N standing, 700N sitting
� Increased to 3000 to 6000N during lifting of moderate weights, decreases with load closer to body
� Estimate of P = 1.5X compressive load divided by the cross sectional area
� Disk pressure is usually uniform
� Pressure lowest in supine position
� Disk usually does not fail, but end plates fracture

Sreeraj S R
Spinal Ligaments
� Anterior Longitudinal
� Posterior Longitudinal
� Ligamentum Flavum
� Interspinous Ligaments
� Supraspinous Ligaments
� Intertransverse Ligaments

Sreeraj S R
Lumbar Spine

Sreeraj S R
Lumbar Spine
Thoraco lumbar fascia
� Stabilizing corset
� Transmit load longitudinally to the spinous process
Ilio lumbar ligament
� Stabilize 5th lumbar vertebrae from ant. Displacement

Types of motion

Sreeraj S R
Stress-Strain Curve

Sreeraj S R
The Motion Segment
� Functional Spinal Unit
� 2 adjacent vertebrae & intervening soft tissue
� Anterior
� Vertebral body
� Disk
� ALL, PLL
� Support, absorb impact, restrict vertical translation
� Posterior
� Neural arch & its processes
� Facet joint

Sreeraj S R
STABILITY
The vertebral column subject to
� Axial compression
� Bending
� Torsion
� Shear

Sreeraj S R
STABILITY
� Primary load-transmitting element, 80-90%
� Bone Mineral Content, Size
� Osteoporosis> loss of horizontal trabeculae
� Increasing size from C to L spine
� Compressive load> pressure higher in center of end plates than periphery
� In vivo, filled with blood> greater strength, hydraulic shock absorber

Sreeraj S R
STABILITYPOSTERIOR ELEMENTS� pedicles, lamina, facet joints,
spinous & transverse processes� Bony processes> lengthen
moment arms of muscles� Forces on processes>
transmitted to Lamina� Forces on posterior elements>
transmitted to vertebral bodies from Pedicles
� Pars Interarticularis� Large bending forces;
excessive extension� Thicker than rest of lamina� Common site of
stress/fatigue fractures> weakens motion segment> spondylolithesis

Sreeraj S R
STABILITY
� Facet Joints� Major role in controlling motion
� Resist torsion & shear, role in compression
� Lumbar FSU – facets 40% torque resistance, 40% disk, 20% ligaments
� Load sharing varies with flexion & extension� Seated position> decreased lumbar lordosis> increased
intradiscal pressure & decreased load-bearing of the facets
� Orientation of facets� C spine - 45º transverse, parallel frontal
� T spine - 60º transverse, 20º frontal
� L spine - 90º transverse, 45º frontal
� Capsules lax> allow gliding

Sreeraj S R
MOBILITY
� Flexion-Extension
� large, due to sizable disks & lack of facet restraint
� posterior half of disk, moves w/ flex-ext
� Lateral bending
� Axial rotation

Sreeraj S R
MOBILITY
Lumbo pelvic rhythm
� Coordinated simultaneous activity of lumbar flexion and tilting of pelvis
� LPR can increase the range of forward flexion, anterior pelvic tilt and flexion of lumbar spine

Sreeraj S R
Lumbo sacral angle
� Ferguson’s angle
� Is formed by the fifth lumbar vertebra and first sacral segment
� The first sacral segment , which inclined anteriorly and inferiorly forms an angle with the horizontal
� 35-40⁰ considered normal

Sreeraj S R
Sacral Anatomy
� The sacrum is a series of 3, 4, or 5 fused coccygeal vertebrae
� The coccyx articulates with the inferior aspect of the sacrum1
234C

Sreeraj S R
SACROILIAC JOINT
� A joint that connects the spinal column with the pelvis. The V-shaped sacrum near the base of the spine fits like a wedge between the wide wings of the ilium (hipbone).

Sreeraj S R
SACROILIAC JOINT

Sreeraj S R
MOBILITY AND STABILITY
� Poorly understood
� Permits a small amount of motion
� Stiff, coarse interdigitating articular surfaces
� Complete ankylosis in up to 76% over age of 50
� Nutation, as described by Kapandji, is the anterior inferior motion of the sacral base.
� counter- nutation as the movement of the sacral base posteriorly and superiorly.
� This nutation and counter- nutation motion of the sacrum is a pivoting type of motion, so that when the base moves forward, the sacral apex (inferior part of the sacrum) moves posteriorly.

Sreeraj S R
Muscles

Sreeraj S R
Iliocostalis Lumborum
� O� Common tendon origin in
sacrum, iliac crest, lumber vertebrae
� I� Lower borders ribs 6-12
� N� Dorsal rami of spinal nerves
� F� Bilateral
� Spinal extension� Maintenance of erect posture� Stabilization of spine during
flexion
� Unilateral� Lateral flexion� Ipsilateral rotation

Sreeraj S R
Longissimus Thoracis
� O� Common tendon origin
in sacrum, iliac crest, lumber vertebrae
� I� T1-12 transverse
processes
� N� Dorsal rami of spinal
nerves
� F� Same as above

Sreeraj S R
Spinalis Thoracis
� O� Common tendon origin
in sacrum, iliac crest, lumber vertebrae
� I� T3-8 spinous processes
� N� Dorsal rami of spinal
nerves
� F� Same as above

Sreeraj S R
Multifidus� O
� Transverse processes C4-L5
� Sacrum
� PSIS
� I� Spinous process of vert above
origin
� N� Spinal nerve roots
� F� Extend and lateral flexion of
vertebral column

Sreeraj S R
Quadratus Lumborum� O
� Iliolumbar Ligament� Iliac crest
� I� Lower border 12th rib� L1-L4 transverse processes
� N � ventral branches of T12 and L1 to
L4.
� F� Pelvis elevation� Trunk extension� Trunk lateral flexion� Pulls down rib 12 to fix origin of
diaphragm

Sreeraj S R
Rotatores� O
� Transverse processes from axis to sacrum
� I� Laminae of vert above
� N� Direct branches over spinal
nerve roots
� F� Spine extension
� Rotation to opposite side

Sreeraj S R
Disorders Of The Back/Spine
� Back Strain/Sprain
� Ankylosing Spondylitis
� Cauda Equina
� Herniated Nucleus Pulposus (HNP)
� Spinal Stenosis
� Kyphosis/Scoliosis
� Low Back Pain (LBP): Spondylolysis, Spondylolisthesis

Sreeraj S R
Back Strain/Sprain
� LBP is the most frequent cause of lost work time and disability in adults <45 years
� Most symptoms of limited duration
� 85% of patients improve and returning to work within 1 month

Sreeraj S R
Ankylosing Spondylitis
� Progressive spinal flexion deformities (may progress to a chin-on-chest deformity)

Sreeraj S R
Cauda Equina symdrome

Sreeraj S R
Herniated Nucleus Pulposus (HNP) of the
Lumbar Spine
� Displacement of the central area of the disc (nucleus) resulting in impingement on a nerve root

Sreeraj S R
Kyphosis
� Defined: abnormally increased convexity in the curvature of the thoracic spine as viewed from side
� Scheuermann’s Disease
� Hyperkyphosis that does not reverse on attempts at hyperextension

Sreeraj S R
Scoliosis
� Lateral curvature of the spine of greater than 10 degrees, usually thoracic or lumbar, associated with rotation of the vertebrae and sometimes excessive kyphosis or lordosis
� Idiopathic scoliosis
� Lateral deviation and rotation of the spine without an identifiable cause

Sreeraj S R
Low Back Pain
� Spondylolysis
� Unilateral Pars defect is the result of a fatigue fracture from repetitive hyperextension

Sreeraj S R
Low Back Pain
� Spondylolisthesis
� Bilateral Pars Interarticularis defect
� Forward slippage of one vertebra on another
� Usually L5-S1