
Ludwig_The Limping Child.pptx (2).pdf - s3. · PDF fileTransient synovitis Transient synovitis...
43
The Limping Child Meryl Ludwig, MD Pediatric Orthopaedic Surgeon Pediatric Specialists of Virginia I have nothing to disclose.
Transcript of Ludwig_The Limping Child.pptx (2).pdf - s3. · PDF fileTransient synovitis Transient synovitis...
The Limping Child
Meryl Ludwig, MD
Pediatric Orthopaedic Surgeon
Pediatric Specialists of Virginia
I have nothing to disclose.
Outline
• Normal Gait
• Evaluation
• Causes of Limp
• Treatments

Normal Gait
• Toddlers: wide base
of support, short
asymmetric steps
Normal Gait
• 3-5 year olds:
symmetric strides,
reciprocal arm
motion
Normal Gait
• 7 year olds: coordinated,
longer stride length,
decreased step cadence
Questions to Ask 1. Is there pain?
2. Onset: sudden or gradual?
3. Is the child sick?
4. What type of limp?
5. Can it be localized?
6. Is the limp getting better/worse/same?
LIMP
Trauma Infection Developmental Neurologic Neoplasm
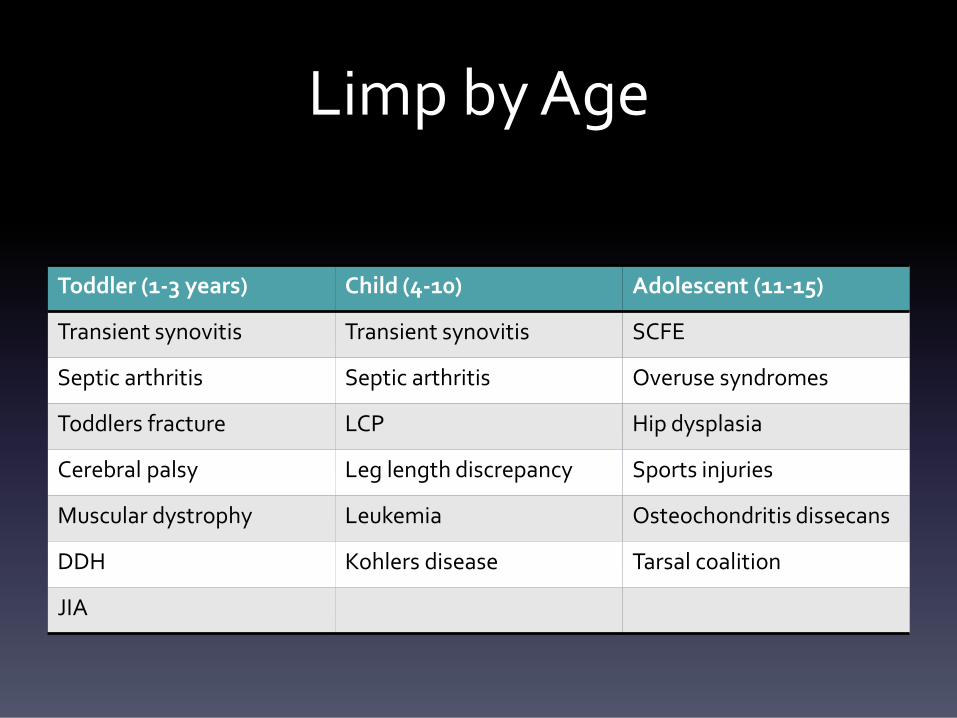
Limp by Age
Toddler (1-3 years) Child (4-10) Adolescent (11-15)
Transient synovitis Transient synovitis SCFE
Septic arthritis Septic arthritis Overuse syndromes
Toddlers fracture LCP Hip dysplasia
Cerebral palsy Leg length discrepancy Sports injuries
Muscular dystrophy Leukemia Osteochondritis dissecans
DDH Kohlers disease Tarsal coalition
JIA
Clinical Evaluation
• History
• Physical exam
• Diagnostic Testing
History
• Bear weight?
• Pain?
• Recent trauma?
• Sports?
• Fever?
• Rashes?
• Travel?

Physical Exam
• Start with nonpainful side
• Observe gait
• Standing
• Supine
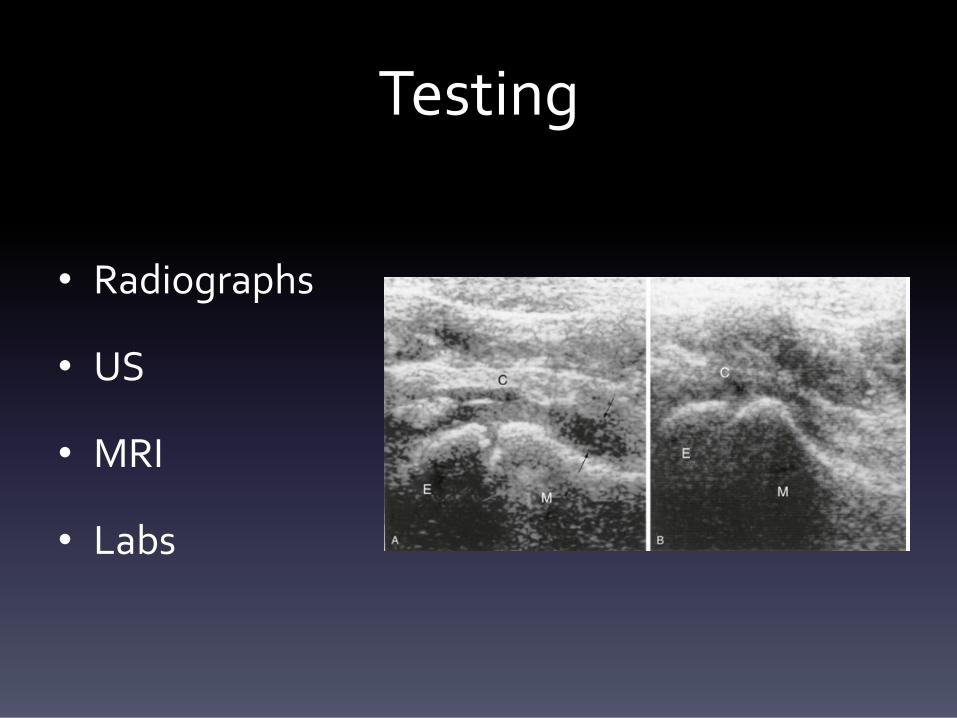
Testing
• Radiographs
• US
• MRI
• Labs
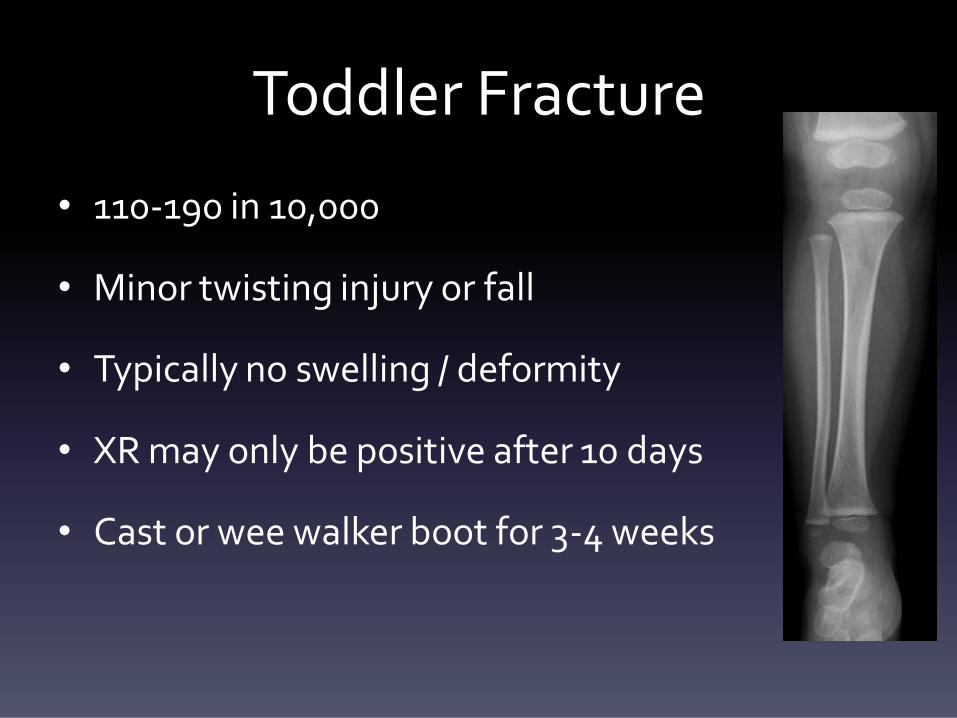
Toddler Fracture
• 110-190 in 10,000
• Minor twisting injury or fall
• Typically no swelling / deformity
• XR may only be positive after 10 days
• Cast or wee walker boot for 3-4 weeks
Evaluating Fracture
• Not all fractures seen on Xray
• Examining young child is hard:
– “One finger at one spot at one time”
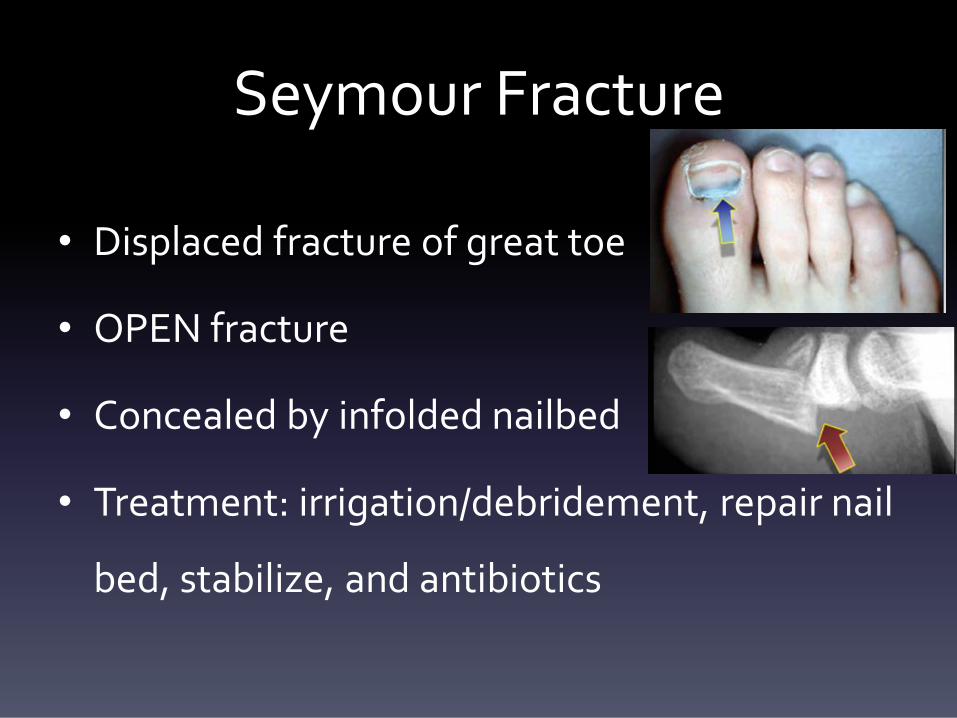
Seymour Fracture
• Displaced fracture of great toe
• OPEN fracture
• Concealed by infolded nailbed
• Treatment: irrigation/debridement, repair nail
bed, stabilize, and antibiotics
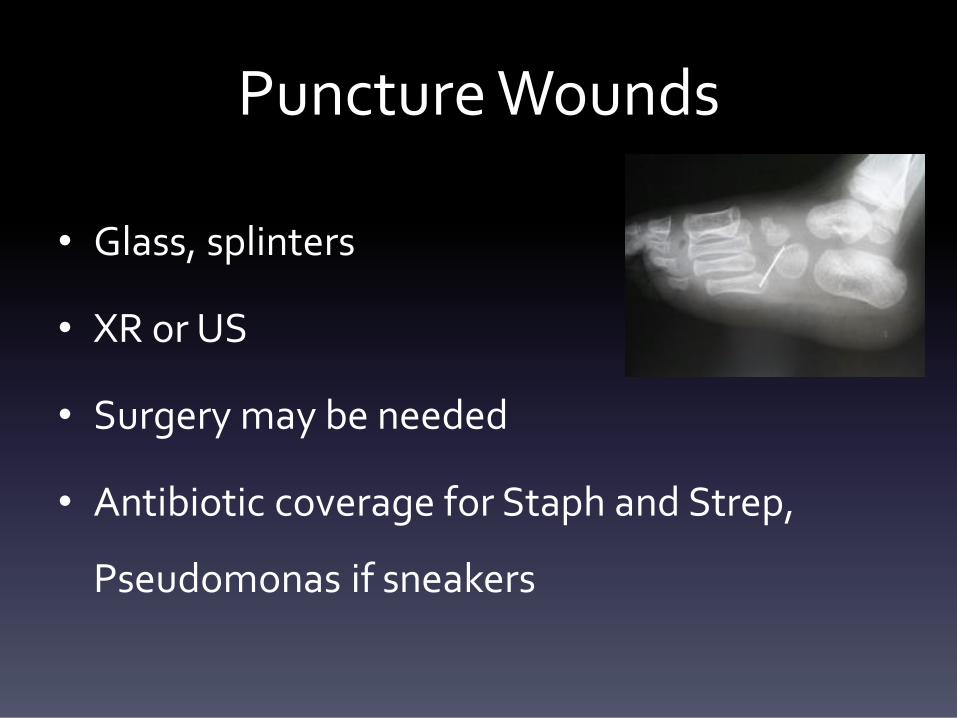
Puncture Wounds
• Glass, splinters
• XR or US
• Surgery may be needed
• Antibiotic coverage for Staph and Strep,
Pseudomonas if sneakers
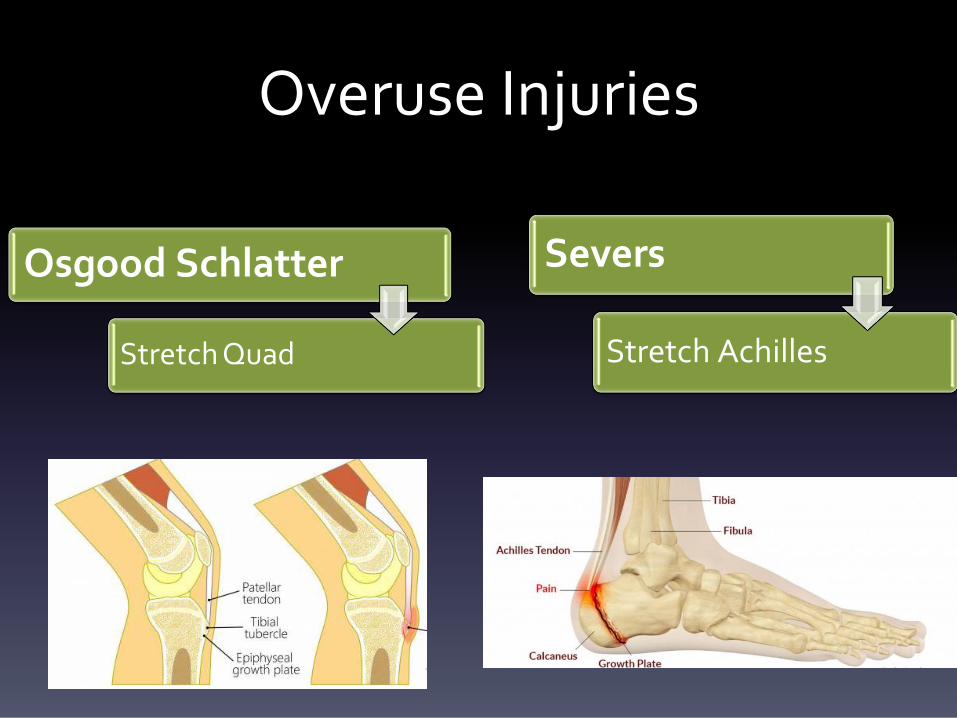
Overuse Injuries
Osgood Schlatter
Stretch Quad
Severs
Stretch Achilles
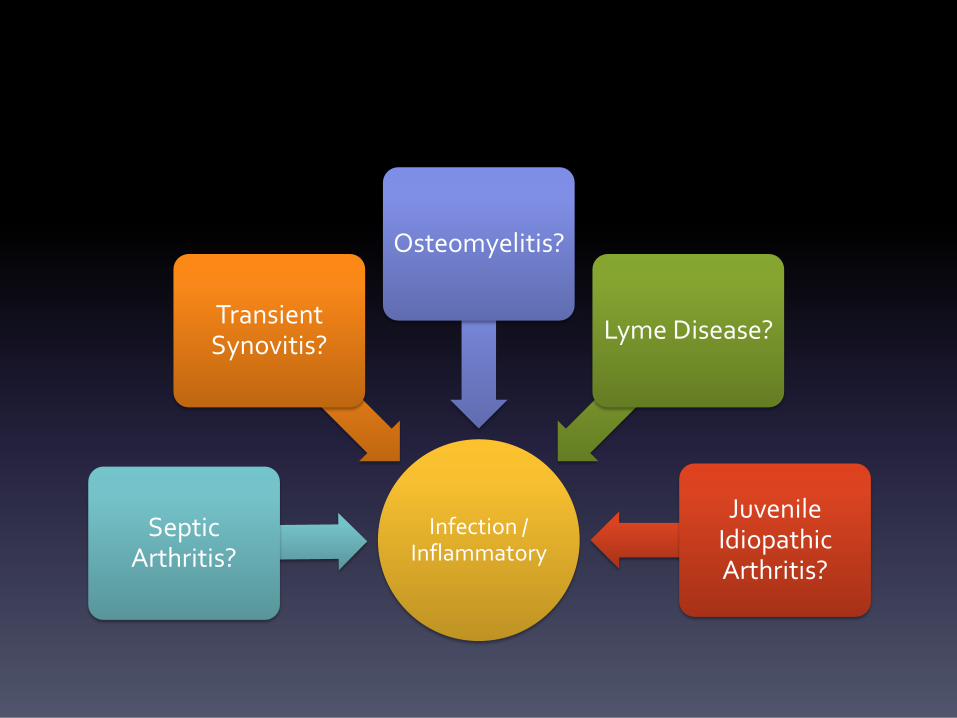
Infection / Inflammatory
Septic Arthritis?
Transient Synovitis?
Osteomyelitis?
Lyme Disease?
Juvenile Idiopathic Arthritis?
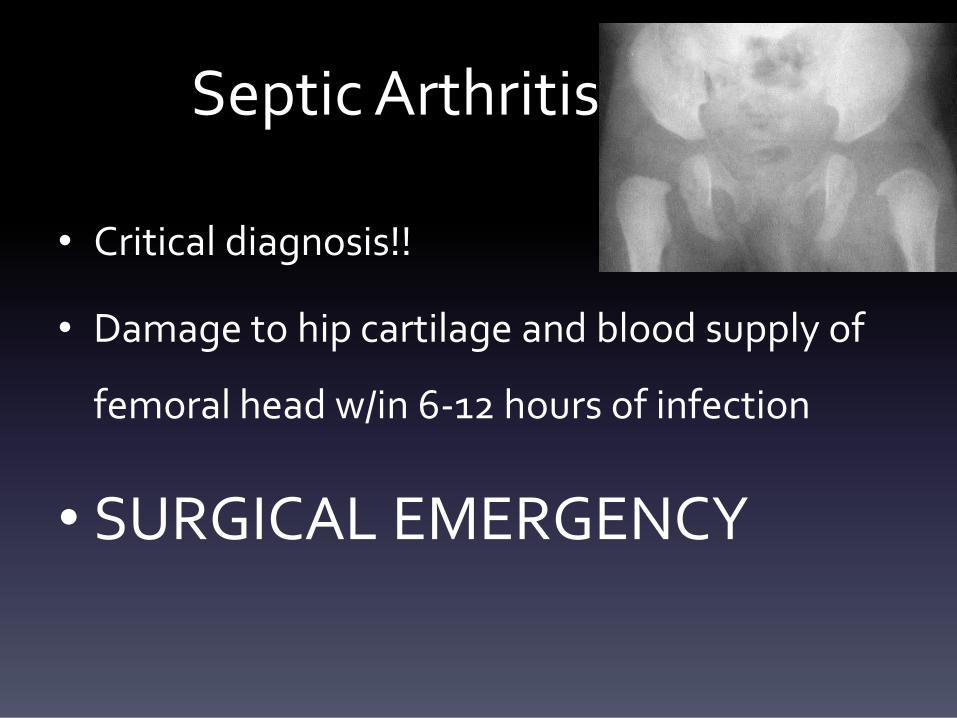
Septic Arthritis
• Critical diagnosis!!
• Damage to hip cartilage and blood supply of
femoral head w/in 6-12 hours of infection
• SURGICAL EMERGENCY
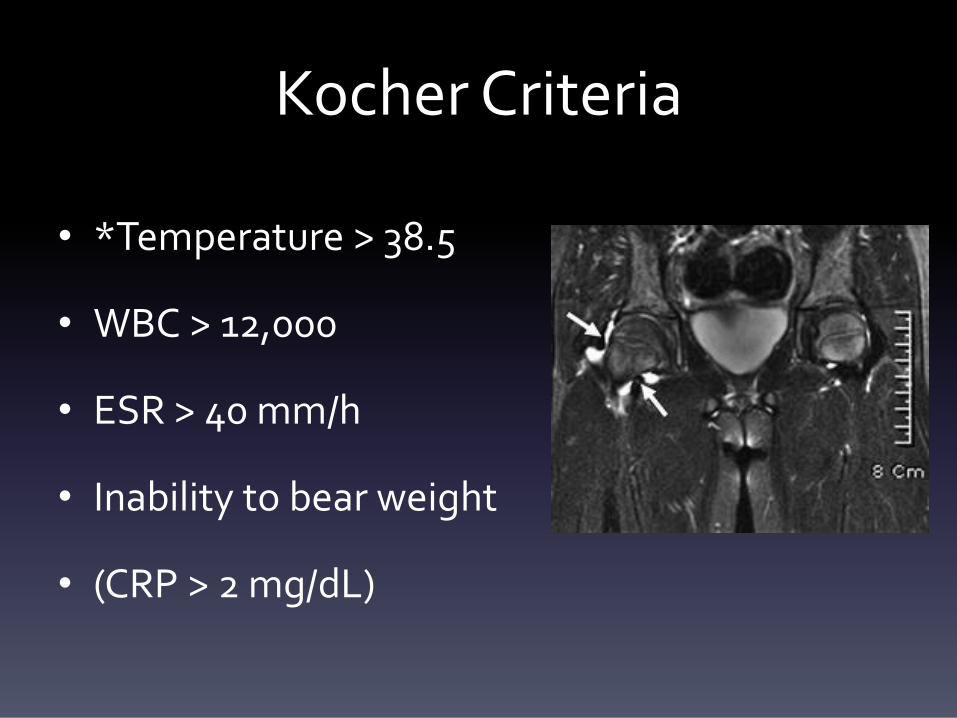
Kocher Criteria
• *Temperature > 38.5
• WBC > 12,000
• ESR > 40 mm/h
• Inability to bear weight
• (CRP > 2 mg/dL)
• Want to see right away!
• Aspiration vs. MRI vs. OR
Transient Synovitis
• 85% of kids with atraumatic hip pain and
limping
• Pain
• Preceding viral infection (URI)
• *Close follow up & anti-inflammatories
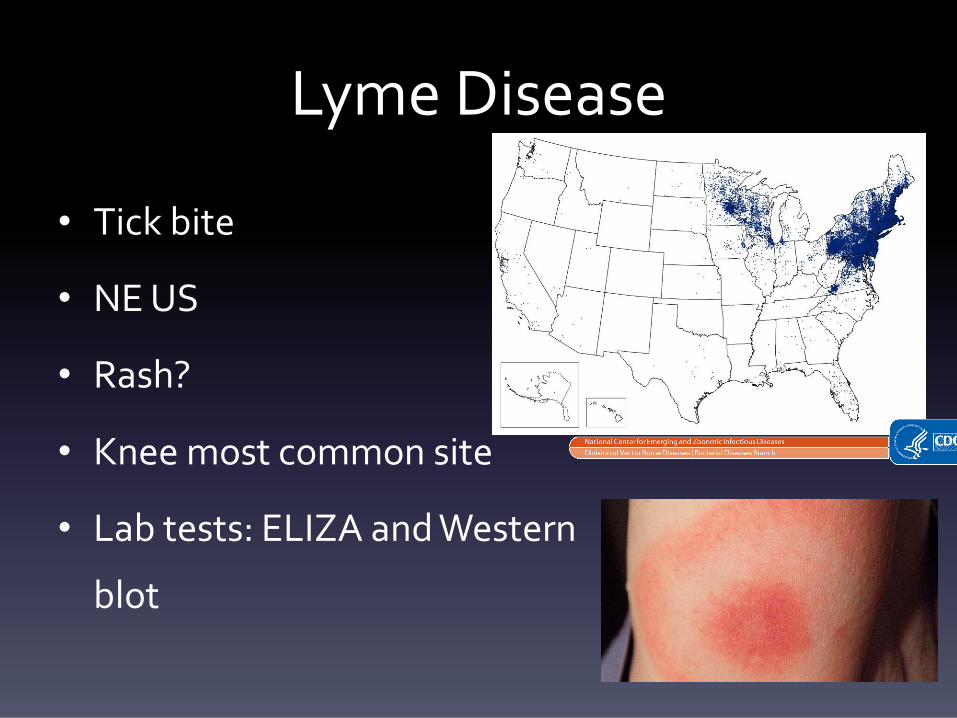
Lyme Disease
• Tick bite
• NE US
• Rash?
• Knee most common site
• Lab tests: ELIZA and Western
blot
Reported Cases of Lyme Disease—United States, 2015 Each dot represents one case of Lyme disease and is placed randomly in the patient’s county of residence. The presence of
a dot in a state does not necessarily mean that Lyme disease was acquired in that state. People travel between states, and
the place of residence is sometimes different from the place where the patient became infected.
• Endemic areas
• Predictive of Septic Arthritis:
– Pain with short arc of motion
– CRP > 4
– History of fever
– Age < 2 years
• Risk increases with # of factors
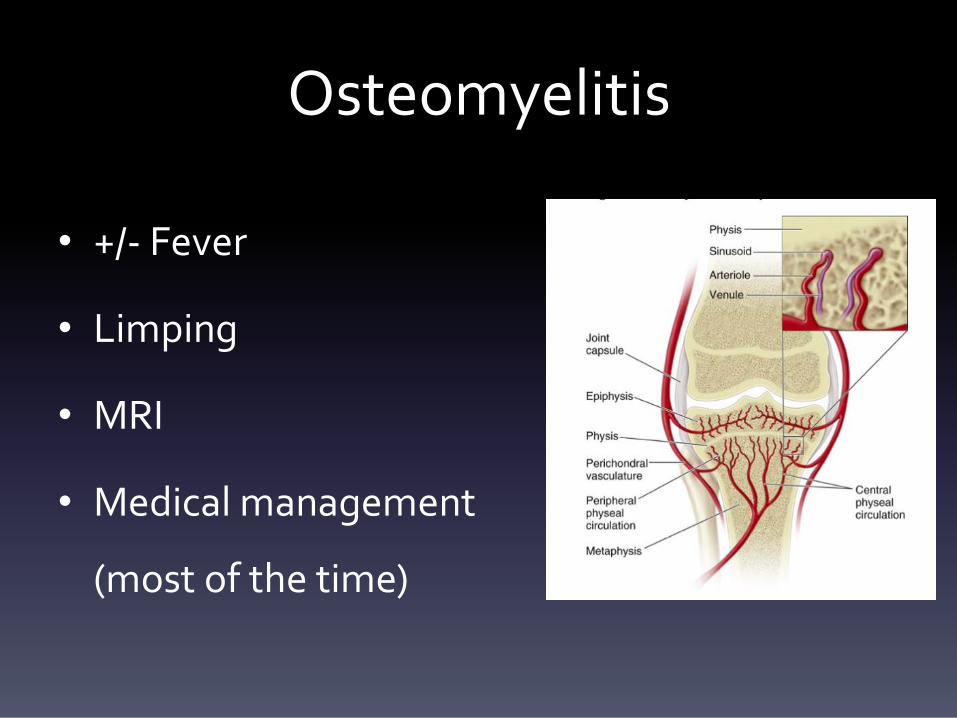
Osteomyelitis
• +/- Fever
• Limping
• MRI
• Medical management
(most of the time)

Juvenile Idiopathic Arthritis
• Autoimmune
• Chronic
• Stiffness in AM
• Labs not dx
• Referral to rheumatology
Dev
elo
pm
enta
l DDH
Perthes
SCFE
DDH
• Check all infants hips!
• Bilateral missed: wide based waddling gait
• Unilateral missed: limb length discrepancy
• Asymmetric abduction
• Late treatment = surgery
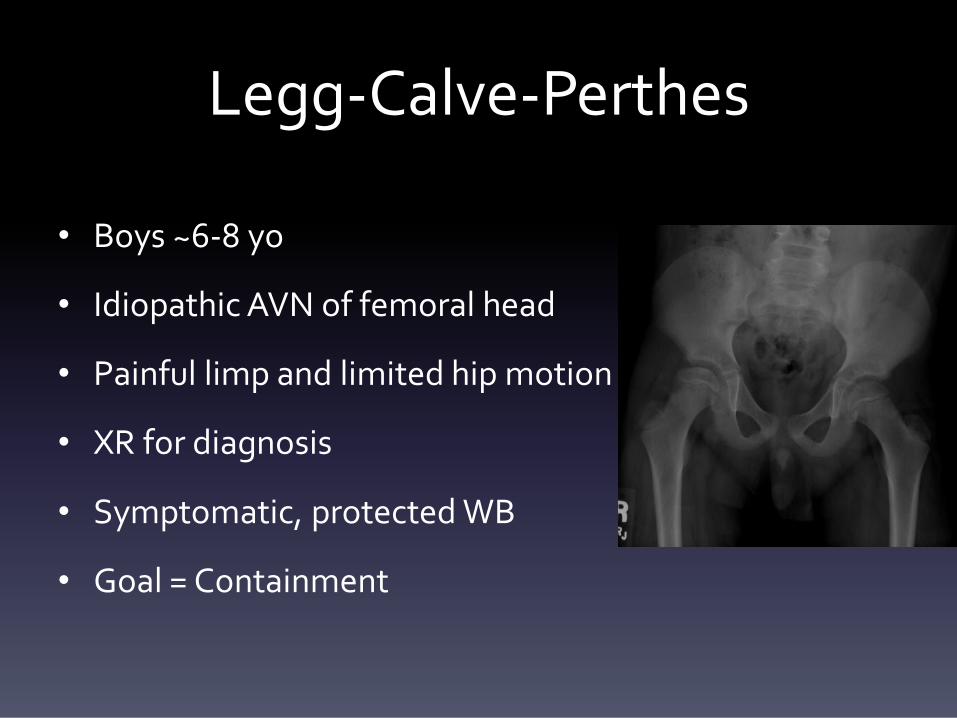
Legg-Calve-Perthes
• Boys ~6-8 yo
• Idiopathic AVN of femoral head
• Painful limp and limited hip motion
• XR for diagnosis
• Symptomatic, protected WB
• Goal = Containment
Slipped Capital Femoral Epiphysis
• Obese, 10-14 years old
• Males, Pacific Islanders
• Complain of knee pain check HIP
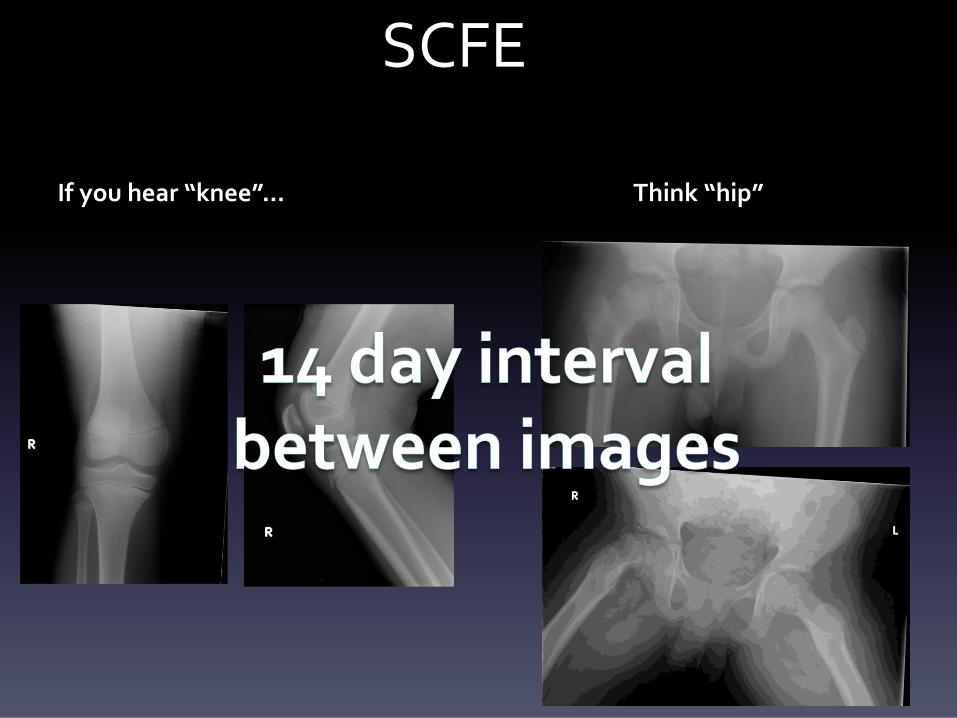
SCFE
If you hear “knee”... Think “hip”
SCFE
• 1st step XR
• 2nd MRI if suspect diagnosis
• Stable SCFE: NWB and send to ER for surgery
• Unstable SCFE: equivalent to hip fracture, ER
surgery ASAP
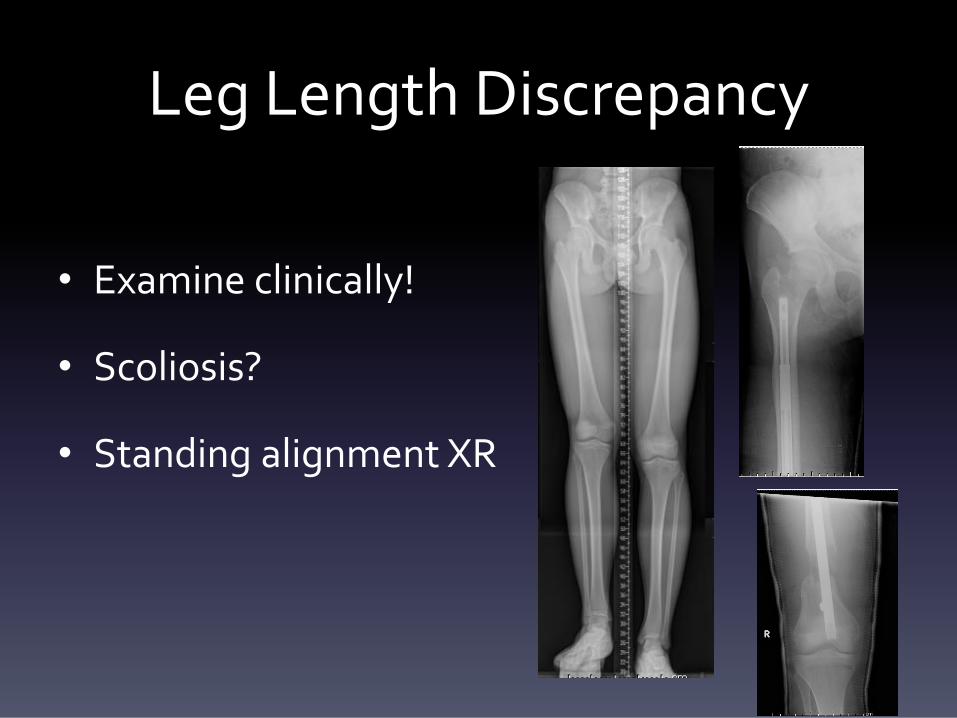
Leg Length Discrepancy
• Examine clinically!
• Scoliosis?
• Standing alignment XR
Neurologic
• Should be considered if child not ambulating
by 18 months
• Prenatal, perinatal, postnatal history
important
Cerebral Palsy
• Static encephalopathy
• History is important!
• Gastrocnemius spasticity
• Hip surveillance
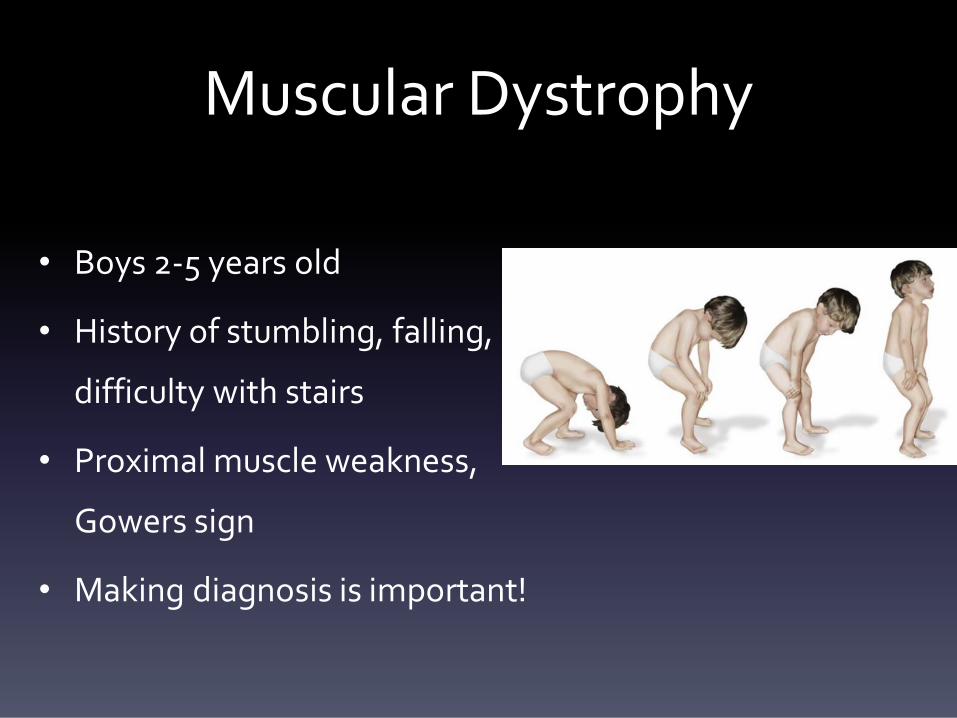
Muscular Dystrophy
• Boys 2-5 years old
• History of stumbling, falling,
difficulty with stairs
• Proximal muscle weakness,
Gowers sign
• Making diagnosis is important!
MSK Tumor Evaluation
• Benign conditions uncommon cause of limp
• PAIN (at night)
• Systemic signs (lethargy, fever, weight loss)
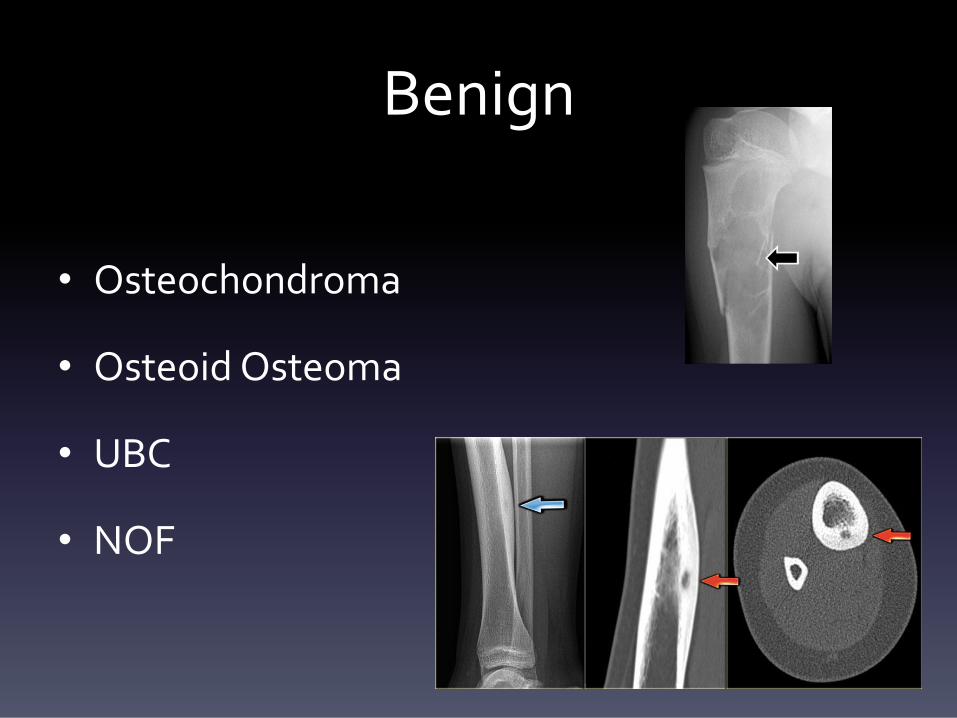
Benign
• Osteochondroma
• Osteoid Osteoma
• UBC
• NOF
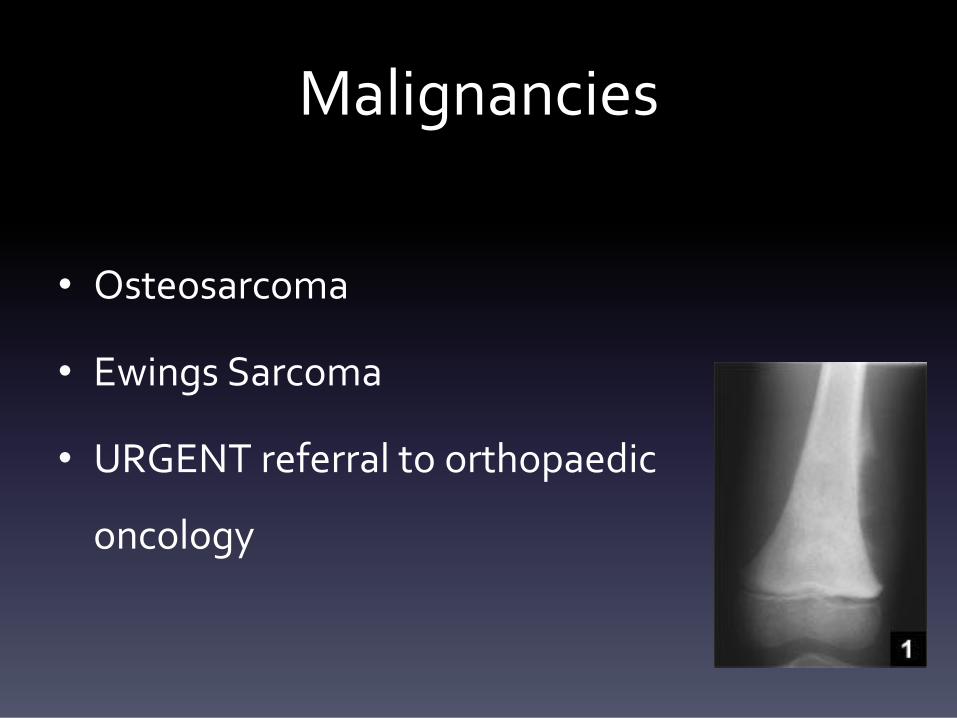
Malignancies
• Osteosarcoma
• Ewings Sarcoma
• URGENT referral to orthopaedic
oncology
Leukemia
• Most common cancer in children < 16
• Normally 2-5 years old
• Lethargy, pallor, bruising, 20% MSK sxs
• *LABS* Anemia, or peripheral leukocyte
count, ESR
• Referral: Ped Heme-Onc!!
Limp Summary
• Adult gait pattern established after age 7
• Wide variety of causes of limp
• 6 questions are helpful
• Orthopaedic evaluation with any concerns!

THANK YOU
Sources
• Baldwin, KD, Brusalis CM, Nduaguba AM, Sankar WN. Predictive Factors for Differentiating Between Septic
Arthritis and Lyme Disease of the Knee in Children. J Bone Joint Surg Am. 2016 May 4;98(9):721-8.
• CDC website. “Lyme Disease Map 2015.” Retrieved from: https://www.cdc.gov/lyme/stats/maps.html
• Flynn JM, Widmann RF. The limping child: evaluation and diagnosis. J Am Acad Orthop Surg. 2001;9(2):89–98.
• Herman, M, Martinek, M. The Limping Child. Pediatr Rev. 2015 May;36(5):184-95.
• Herring, J. “The Limping Child.” Tachdijian’s Pediatric Orthopaedics. 5th edition. Philadelphia: Elsevier Saunders,
2014. 79-89.
• Johnston, James. Tumor Library online. http://www.tumorlibrary.com
• Sawyer JR, Kapoor M. The limping child: a systematic approach to diagnosis. Am Fam Physician. 2009;79(3):215–
224.
• Shah A, Indra S, Kannikeshwaran N, Hartwig E, Kamat D. Diagnostic Approach to Limp in Children. Pediatr
Ann.2015; 44: 548-550, 552-554, 556.
• Special thanks to George Gantsoudes, MD .


















