Low-Invasive Imaging Guided Treatment of Tubo-Ovarian Abscess Malkhaz Mizandari, MD, PhD Ultrasound...
21
Low-Invasive Imaging Low-Invasive Imaging Guided Treatment of Guided Treatment of Tubo-Ovarian Abscess Tubo-Ovarian Abscess Malkhaz Mizandari, MD, PhD Malkhaz Mizandari, MD, PhD Ultrasound Education Centre “GEOJEFF” Ultrasound Education Centre “GEOJEFF” State Medical University State Medical University Tbilisi, Georgia Tbilisi, Georgia
-
Upload
jemima-price -
Category
Documents
-
view
221 -
download
4
Transcript of Low-Invasive Imaging Guided Treatment of Tubo-Ovarian Abscess Malkhaz Mizandari, MD, PhD Ultrasound...

Low-Invasive Imaging Guided Low-Invasive Imaging Guided Treatment of Tubo-Ovarian Treatment of Tubo-Ovarian
AbscessAbscess
Malkhaz Mizandari, MD, PhDMalkhaz Mizandari, MD, PhDUltrasound Education Centre Ultrasound Education Centre
“GEOJEFF”“GEOJEFF”State Medical UniversityState Medical University
Tbilisi, GeorgiaTbilisi, Georgia
Etiology-PathogenesisEtiology-Pathogenesis
TOA is a complication of PIDTOA is a complication of PID (15.0 to 30.0% of cases)(15.0 to 30.0% of cases)
PathogenesisPathogenesis Ascending lower genital tract infectionAscending lower genital tract infection Tube epithelium inflammation and necrosisTube epithelium inflammation and necrosis a) Aa) Altered pH ltered pH b) Devitalized or necrotic tissue from infectionb) Devitalized or necrotic tissue from infection c) Impaired blood supply from edema c) Impaired blood supply from edema d) Pathogenic organism growth d) Pathogenic organism growth
DiagnosisDiagnosis- - Clinical Findings
Pain in Small PelvisPain in Small Pelvis
High TemperatureHigh Temperature
Vaginal Discharge (Purulent)Vaginal Discharge (Purulent)
Painful Mass in Adnexal RegionPainful Mass in Adnexal Region
Tenderness or Pain of Cervix on Physical Tenderness or Pain of Cervix on Physical ExaminationExamination

Diagnosis - ImagingDiagnosis - Imaging
UltrasoundUltrasound
CT CT
MR imagingMR imaging
Ultrasound DiagnosisUltrasound Diagnosis
Irregularly Shaped Mass in AdnexaIrregularly Shaped Mass in Adnexa
Thick WallsThick Walls
Complex Mass (Predominantly Cystic)Complex Mass (Predominantly Cystic)
Internal Septi Internal Septi
Fluid-Fluid LevelFluid-Fluid Level
Fluid-Debris levelFluid-Debris level
Gas (Gas-Forming Microorganizms)Gas (Gas-Forming Microorganizms)
Often Adnexal Region Occupied BilaterallyOften Adnexal Region Occupied Bilaterally

MicrobiologyMicrobiology
The Most Common Primary Causes:The Most Common Primary Causes: a) a) Chlamydia trachomatisChlamydia trachomatis b) Neisseria gonorrheab) Neisseria gonorrhea
Less CommonLess Common Gardneralla vaginalis, PeptostreptococcusGardneralla vaginalis, Peptostreptococcus sp, sp,
Streptococcus agalectiae, UreaplasmaStreptococcus agalectiae, Ureaplasma sp, sp, Mycobacterium tuberculosisMycobacterium tuberculosis, Haemophilus influenzae,, Haemophilus influenzae, ActinomycesActinomyces
Supplemented InfectionSupplemented Infection Escherichia Coli Escherichia Coli
TreatmentTreatment
Medical (Broad Spectrum Antibiotics for PIDMedical (Broad Spectrum Antibiotics for PID))
TOA - Content Evacuation:TOA - Content Evacuation: SurgerySurgery
Surgical options include laparoscopy or laparotomy with Surgical options include laparoscopy or laparotomy with unilateral adnexectomy or total abdominal hysterectomy unilateral adnexectomy or total abdominal hysterectomy with bilateral oophorectomywith bilateral oophorectomy
Low-Invasive Low-Invasive InterventionIntervention
Imaging guided percutaneal or endocavity Imaging guided percutaneal or endocavity
aspiration/drainage:aspiration/drainage: a) CT b) Ultrasound c)Combined (Ultrasound-a) CT b) Ultrasound c)Combined (Ultrasound-
Fluoroscopy) Fluoroscopy)
Invasive Ultrasound - Invasive Ultrasound - AdvantagesAdvantages
No Ionizing RadiationNo Ionizing Radiation
Real-Time TechniqueReal-Time Technique
Doppler CapabilityDoppler Capability
Puncture Aiming and Needle Puncture Aiming and Needle Movement Guidance CapabilityMovement Guidance Capability
Abdominal and Endocavity Abdominal and Endocavity ApproachApproach
Cost-SavingCost-Saving
Material and MethodsMaterial and Methods
TOA – 28 patientsTOA – 28 patients
Percutaneal approach (Drainage) – 4 patientsPercutaneal approach (Drainage) – 4 patients
Perrectal approach (Aspiration, Rinsing) – 4 Perrectal approach (Aspiration, Rinsing) – 4 patientspatients
Pervaginal approach (Aspiration, Rinsing) – 22 Pervaginal approach (Aspiration, Rinsing) – 22 patient patient
(Note – all patients received antibiotics according (Note – all patients received antibiotics according the findings of bacteriology of aspirated material) the findings of bacteriology of aspirated material)
ProceduresProcedures
Rinsing (Saline and Antiseptics) was performed Rinsing (Saline and Antiseptics) was performed to all patientsto all patientsProteolythic Enzyme Injection was performed to Proteolythic Enzyme Injection was performed to
6 patients because of inadequate rinsing due 6 patients because of inadequate rinsing due to TOA Septi and viscous contentto TOA Septi and viscous contentSingle Procedure - 7 patients total (2 Single Procedure - 7 patients total (2 percutaneal drainages and 5 aspirations)percutaneal drainages and 5 aspirations)2 procedures – 10 patients (among them – 1 2 procedures – 10 patients (among them – 1 after percutaneal drainage)after percutaneal drainage)3 and more procedures – 11 patients (among 3 and more procedures – 11 patients (among them – 1 after percutaneal drainage)them – 1 after percutaneal drainage)

Abdominal vs. endocavity Abdominal vs. endocavity approach - Indicationsapproach - Indications
Abdominal Approach – Relatively Big Abdominal Approach – Relatively Big Mass, Fixed to Anterior Abdominal Wall Mass, Fixed to Anterior Abdominal Wall (advantage – Drainage Easily Performed)(advantage – Drainage Easily Performed)
Rectal Approach – Big Amount of Purulent Rectal Approach – Big Amount of Purulent Vaginal Discharge, Painful Vaginal Vaginal Discharge, Painful Vaginal Examination, Virgo PatientExamination, Virgo Patient
Vaginal Approach – Small Masses Easily Vaginal Approach – Small Masses Easily Achievable for Puncture Achievable for Puncture

Needle Inserted in TOA
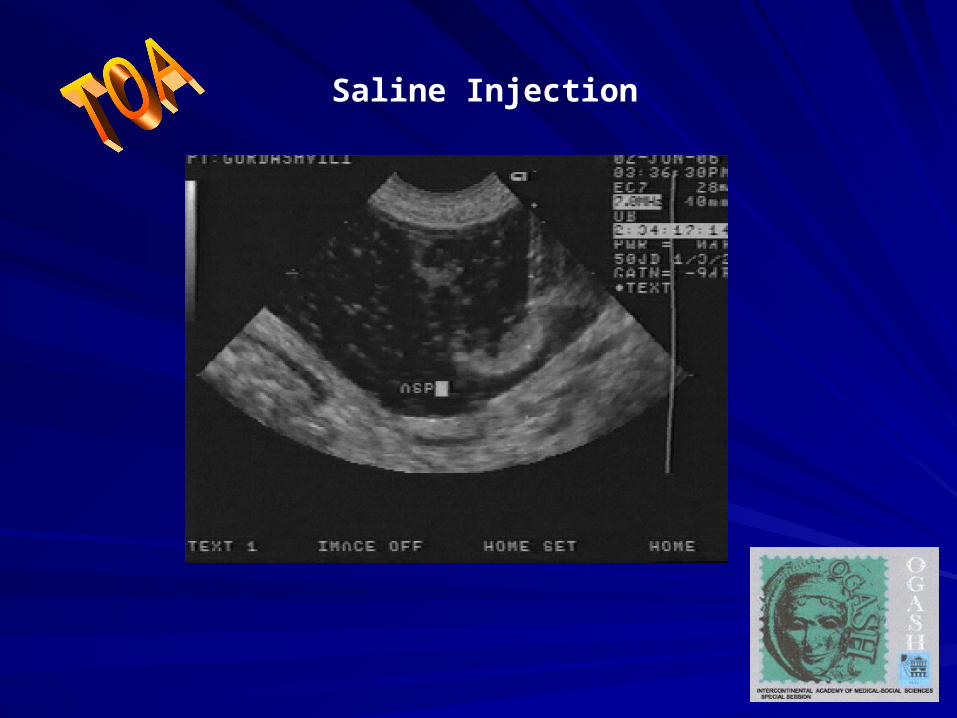
Saline Injection

Rinsing (Bubbles in TOA cavity)

Betadine Injected
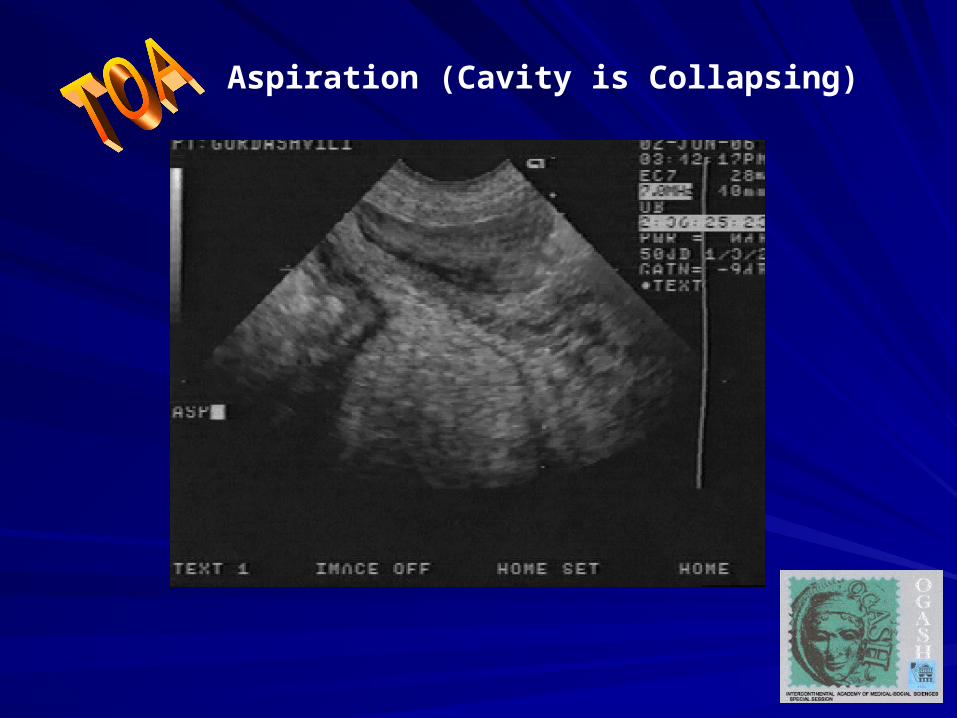
Aspiration (Cavity is Collapsing)
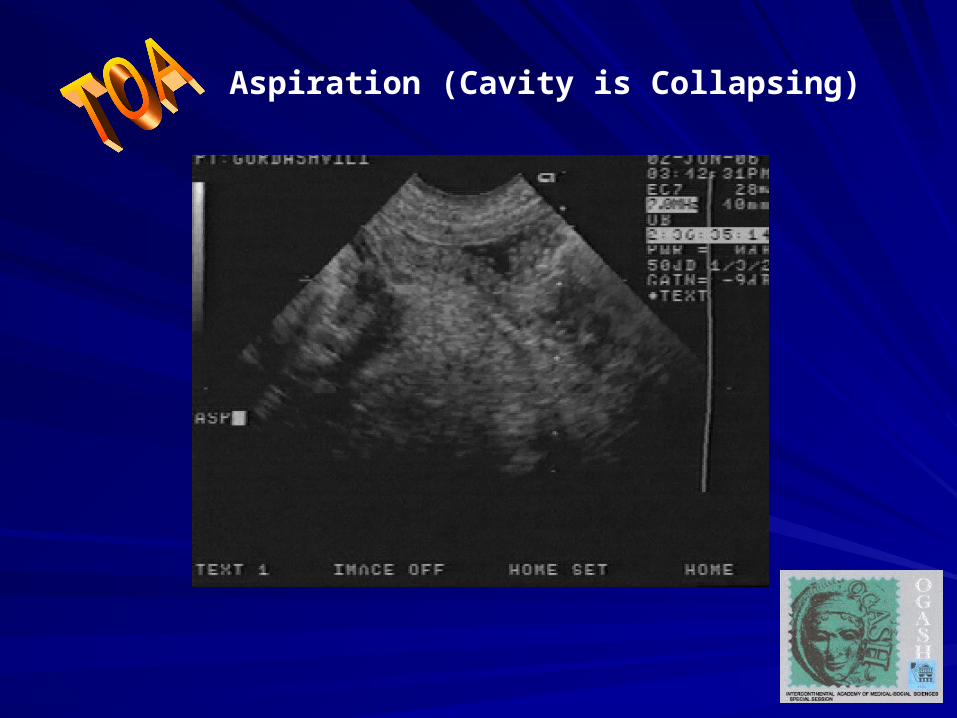
Aspiration (Cavity is Collapsing)
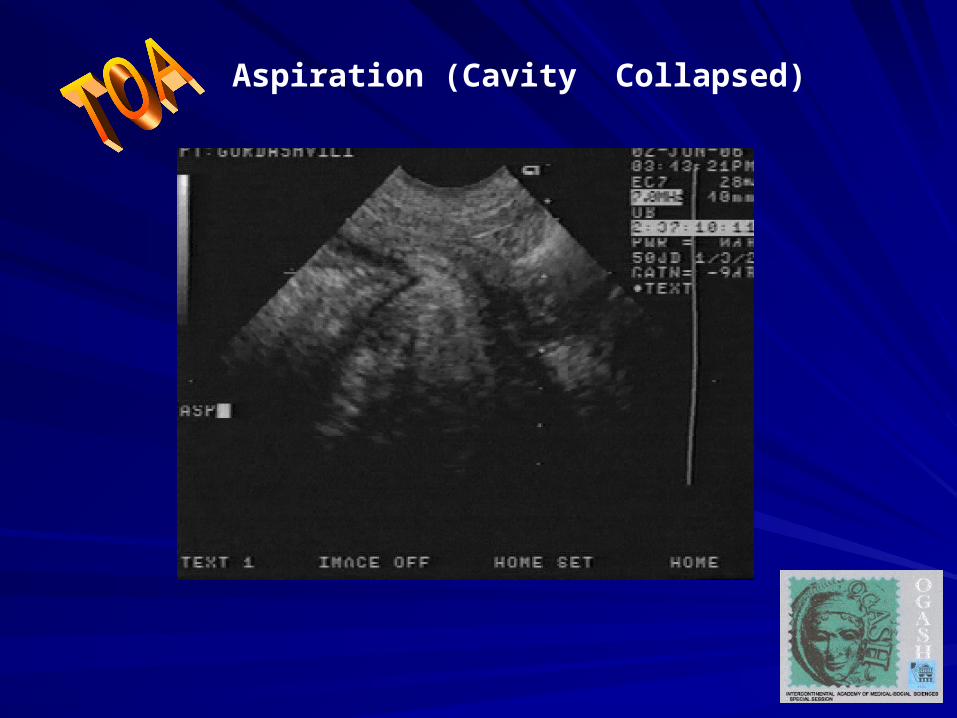
Aspiration (Cavity Collapsed)
ResultsResults
Positive Result was Achieved in 27 Positive Result was Achieved in 27 (96.6%) cases(96.6%) cases
Open Surgery RequiredOpen Surgery Required ( (TTotal otal Abdominal Hysterectomy with Bilateral Abdominal Hysterectomy with Bilateral Oophorectomy) – 1 (3.4Oophorectomy) – 1 (3.4 %) %) casecase
SummarySummary
Low-Invasive Treatment (LIT) under Imaging Low-Invasive Treatment (LIT) under Imaging Guidance Control Is Safe, Effective and Cost-Guidance Control Is Safe, Effective and Cost-Saving TechniqueSaving Technique
LIT is Easily Tolerated by Patients (Multiple LIT is Easily Tolerated by Patients (Multiple Procedures)Procedures)
Combination of Percutaneal Drainage and Combination of Percutaneal Drainage and Endocavity Aspiration Might Be HelpfulEndocavity Aspiration Might Be Helpful
LIT Should Be Used as a First Choice Treatment LIT Should Be Used as a First Choice Treatment Procedure in TOA Patients ManagementProcedure in TOA Patients Management