
Abscess Formation Complicated in Ovarian Mucinous...
5
416 臨 床 Abscess Formation Complicated in Ovarian Mucinous Cystadenoma: A Case Report Po-Ren HSUEH, Chyng-Chuang HWANG, Kao-Pin YEN* , Mao LIN* and Chenden YOUNG** Department of Medicine and *Department of Obstetrics and Gynecology , Taiwan Provincial Tainan Hospital **Division of Infectious Disease , National Cheng Kung University Medical College (Received: February 18, 1991) (Accepted:October 8, 1991) Key words: ovarian mucinous cystadenoma, abscess Introduction Isolated ovarian abscess is an unusual gynecologic infection which involves the parenchyma of the ovray1). Tuboovarian abscess, by contrast, involves the ovary and fallopian tube which is almost always a sequel of repeated attacks of acute salpingooorhoritis. In 1869, Aitken gave the earliest report of an ovarian abscessl". Case reports were also offered by Coe2), Ohman1,4) and Brindeau1,4) and Brindeau1,5). Black presented the first major series of 42 cases of ovarian abscess in 19363). Thereafter, several serial studies of ovarian abscesses were reported continuously. Here, we present a case of ovarian mucinous cystadenoma complicated with abscess formation. The patient was treated successfully with operative removal and parenteral antibiotics. To our knowledge, the presence of abscess formation in an ovarian mucinous cystadenoma has not been described in the past English literature. Case Report A 75-year-old housewife (G4P3A1) was admitted to Taiwan Provincial Tainan Hospital because of progressive body weight loss and prominent abdominal mass for 6 months. The patient had been well before. Her past medical history was unremarkable except for uterine currettage 30 years ago. Since then, she had experienced body weight gain (15 kilogram) and increasing abdominal girth in these 30 years. Six months before admission, she began to suffer from progressive body weight loss (12 kilogram), a palpable abdominal mass and frequency of micturition. She denied fever, abdominal pain, bowel habit changes, night sweats or dyspnea in the recent 6 months. There was no history of diabetes mellitus, tuberculosis, syphilis, gonorrhea or other venereal diseases. On physical examination, the patient appeared mildly ill and anemic. The body temperature was 36.7•Ž, the pulse was 84/min, regular, and the respiration was 20/min. The blood pressure was 150/70 mmHg without orthostatic change. The head and neck were normal. The lungs were clear. The heart beat was regular and no murmur was audible. The abdomen was soft and globular; the liver and spleen were not felt; the mid- and low-abdomen was occupied with a huge mass (30 X 35 cm in size) which was soft , nontender, slightly movable and no skin change. No tenderness was found in the costovertebral angles or spine. The extremities were normal. No lymphadenopathy was found. Neurologic examination was normal. Examination of the genitalia and rectum was negative. 別 刷 請 求先:(〒414)伊 東 市 桜 木 町1-2-24 佐藤病院内科 楊 振典 感染症学雑誌 第66巻 第3号
Transcript of Abscess Formation Complicated in Ovarian Mucinous...

416
臨 床
Abscess Formation Complicated in Ovarian Mucinous Cystadenoma:
A Case Report
Po-Ren HSUEH, Chyng-Chuang HWANG, Kao-Pin YEN* ,Mao LIN* and Chenden YOUNG**
Department of Medicine and *Department of Obstetrics and Gynecology , Taiwan Provincial Tainan Hospital**Division of Infectious Disease
, National Cheng Kung University Medical College
(Received: February 18, 1991)
(Accepted: October 8, 1991)
Key words: ovarian mucinous cystadenoma, abscess
Introduction
Isolated ovarian abscess is an unusual gynecologic infection which involves the parenchyma of the
ovray1). Tuboovarian abscess, by contrast, involves the ovary and fallopian tube which is almost always a
sequel of repeated attacks of acute salpingooorhoritis.
In 1869, Aitken gave the earliest report of an ovarian abscessl". Case reports were also offered by Coe2),
Ohman1,4) and Brindeau1,4) and Brindeau1,5). Black presented the first major series of 42 cases of ovarian
abscess in 19363). Thereafter, several serial studies of ovarian abscesses were reported continuously.
Here, we present a case of ovarian mucinous cystadenoma complicated with abscess formation. The
patient was treated successfully with operative removal and parenteral antibiotics. To our knowledge, the
presence of abscess formation in an ovarian mucinous cystadenoma has not been described in the past
English literature.
Case Report
A 75-year-old housewife (G4P3A1) was admitted to Taiwan Provincial Tainan Hospital because of
progressive body weight loss and prominent abdominal mass for 6 months.
The patient had been well before. Her past medical history was unremarkable except for uterine
currettage 30 years ago. Since then, she had experienced body weight gain (15 kilogram) and increasing
abdominal girth in these 30 years. Six months before admission, she began to suffer from progressive body
weight loss (12 kilogram), a palpable abdominal mass and frequency of micturition. She denied fever,
abdominal pain, bowel habit changes, night sweats or dyspnea in the recent 6 months. There was no
history of diabetes mellitus, tuberculosis, syphilis, gonorrhea or other venereal diseases.
On physical examination, the patient appeared mildly ill and anemic. The body temperature was
36.7•Ž, the pulse was 84/min, regular, and the respiration was 20/min. The blood pressure was 150/70
mmHg without orthostatic change. The head and neck were normal. The lungs were clear. The heart beat
was regular and no murmur was audible. The abdomen was soft and globular; the liver and spleen were not
felt; the mid- and low-abdomen was occupied with a huge mass (30 X 35 cm in size) which was soft ,
nontender, slightly movable and no skin change. No tenderness was found in the costovertebral angles or
spine. The extremities were normal. No lymphadenopathy was found. Neurologic examination was
normal. Examination of the genitalia and rectum was negative.
別刷請求先:(〒414)伊 東市桜木町1-2-24
佐藤病院内科 楊 振典
感染症学雑誌 第66巻 第3号
Abscess in Ovarian Mucinous Cystadenoma 417
The routine blood tests were: Hemoglobin, 8.4 mg/dl; hematocrit 26%; white blood cell count,
10500/mm3, with 74% neutrophils, 1% band forms and 25% lymphocytes; platelet count, 300,000/mm3;
erythrocyte sedimentation rate, 130 mm/hour. The urine examination gave no abnormal finding. Blood
biochemical studies showed: urea nitrogen, 10 mg/dl; creatinine, 0.9 mg/dl; glucose, 80 mg/dl; albumin, 3.0
mg/dl; globulin, 4.0 mg/dl; glutamate oxaloacetic transaminase, 13 U/l; glutamate pyruvate transaminase,
72 U/l; lactic dehydrogenase, 476 U/l; gammaglutamyl transferase, 25 U/l; alkaline phosphatase, 72 U/l;
cholesterol, 128 mg/dl; triglyceride 124 mg/dl; amylase, 179 SU; sodium, 144 mEq/l; potassium 3.2 mEq/l;
chloride, 110 mEq/l; IgG, 2680 mg/dl; IgA, 682 mg/dl; IgM, 143 mg/dl. The electrocardiogram was normal.
The admission chest roentgenogram revealed no abnormality and plain radiograph of the abdomen
showed a huge mass which almost occupied the whole abdomen with lateral displacement of the bowel.
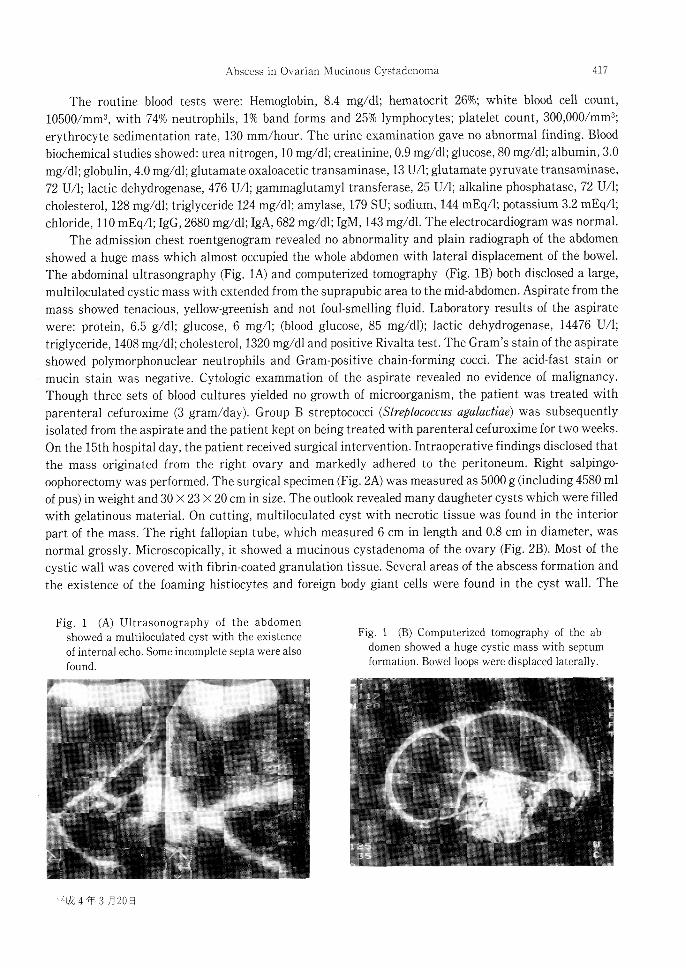
The abdominal ultrasongraphy (Fig. 1A) and computerized tomography (Fig. 1B) both disclosed a large,
multiloculated cystic mass with extended from the suprapubic area to the mid-abdomen. Aspirate from the
mass showed tenacious, yellow-greenish and not foul-smelling fluid. Laboratory results of the aspirate
were: protein, 6.5 g/dl; glucose, 6 mg/l; (blood glucose, 85 mg/dl); lactic dehydrogenase, 14476 U/l;
triglyceride, 1408 mg/dl; cholesterol, 1320 mg/dl and positive Rivalta test. The Gram's stain of the aspirate
showed polymorphonuclear neutrophils and Gram-positive chain-forming cocci. The acid-fast stain or
mucin stain was negative. Cytologic exammation of the aspirate revealed no evidence of malignancy.
Though three sets of blood cultures yielded no growth of microorganism, the patient was treated with
parenteral cefuroxime (3 gram/day). Group B streptococci (Streptococcus agalactiae) was subsequently
isolated from the aspirate and the patient kept on being treated with parenteral cefuroxime for two weeks.
On the 15th hospital day, the patient received surgical intervention. Intraoperative findings disclosed that
the mass originated from the right ovary and markedly adhered to the peritoneum. Right salpingo-
oophorectomy was performed. The surgical specimen (Fig. 2A) was measured as 5000 g (including 4580 ml
of pus) in weight and 30 •~ 23 •~ 20 cm in size. The outlook revealed many daugheter cysts which were filled
with gelatinous material. On cutting, multiloculated cyst with necrotic tissue was found in the interior
part of the mass. The right fallopian tube, which measured 6 cm in length and 0.8 cm in diameter, was
normal grossly. Microscopically, it showed a mucinous cystadenoma of the ovary (Fig. 2B). Most of the
cystic wall was covered with fibrin-coated granulation tissue. Several areas of the abscess formation and
the existence of the foaming histiocytes and foreign body giant cells were found in the cyst wall. The
Fig. 1 (A) Ultrasonography of the abdomenshowed a multiloculated cyst with the existenceof internal echo. Some incomplete septa were alsofound.
Fig. 1 (B) Computerized tomography of the ab-domen showed a huge cystic mass with septumformation. Bowel loops were displaced laterally.
平成4年3月20日

418 Po-Ren HSUEH et al
Fig. 2 (A) Grossly, the removed mass was measured as 5000 g in weight and 30•~23•~20cm
in size. The outlook revealed many daughter cysts which was filled with gelatinous
materials.
Fig. 2 (B) Microscopically, a mucinous cystadenoma of the ovary was revealed from the
intact part of the inner wall. (Haemotoxyline-Eosin stain, 100•~).
A B
mesothial surface showed markedly fibropurulent adhesion. There was no evidence of malignant change.
The fallopian tube was normal microscopically.The patient received another 2 weeks of treatment with parenteral antibiotics after operation. Her
postoperative occurse was smooth and she was discharged uneventfully on the 30th hospital day.Throughout the whole clinical course of this patients, there was no fever (except for one day of
postoperative fever), abdominal pain or any sign of intestinal or ureteral obstruction. The white blood cellcount was elevated on the admission but returned to normal after the 5th hospital day.
Discussion
An ovarian abscess, which develops as an isolated lesion without simultaneous involvement of the
fallopian tube, is an unusual gynecologic infection1}. However, a tuboovarian absces occurs more frequently
than isolated ovarian abscess in clinical aspect1,01. It is difficult to distinguish between them until a
laparotomy is performed. The first case of ovarian abscess was reported by Aitken in 1869'). This patient
died from rupture of an ovarian abscess during pregnancy and was diagnosed postmortemly. Many cases of
ovarian abscesses had been reported since then and more details about this disease were well elucidated11
Three major etiologies have been proposed for ovarian abscesses6). Those include: (1) bacteria have
been already present around the ovary and gain access into the stroma when the ovarian capsule is
damaged. (2) bacteria enter the ovary by hematogenous spreading. (3) bacteria invade the ovary by
lymphatic spreading5,11). Ovaluation may cause a natural break of the ovarian capsule. Furthermore, the
ovarian capsule may be violated with a stitch, a knife blade or by blunt dissection intraoperatively. The
bacteria, which colonize the genitourinary tract or seed the peritoneum in conditions of appenddicitis,
diverticulitis, may subsequently enter the ovary with diseased capsule5.11). An abscess then forms and
slowly expands as the bacteria multiply within the parenchyma of the ovary.
感染症学雑誌 第66巻 第3号

Abscess in Ovarian Mucinous Cystadenoma 419
Wagner stated that an isolated ovarian absces might develop after the manipulations of cervicaldilatation, uterine curretage or salpingographyl). Harrison, Petterson Virata, and Niebyl et al all presentedovarian abscesses in the presence of intrauterine devices5,8,9). The ovarian abscess following streptococcaltonsillitis with hematogenous spreading was reported by Black3). Several systemic diseases (tuberculosis,typhoid fever) and some local disorders (parotitis, cellulitis, pelvic inflammatory diseases, rupture of follicleor corpus luteum) might complicate with ovarian abscesses. However, some cases of ovarian absces withundetermined etiology were described').
Recent studies have shown that ovarian abscess usually contain mixed bacteria, including aerobicGram-negative organisms and anaerobes. E. coli, Bacteroides species, streptococci and Staphylococcusaureus were the most common isolates. Pseudomomas species, mycobacteria and Actinomyces species werealso identified1,4,5,11). Group B streptococci (Streptococcus agalactiae), as we isolated in this case, is one of thecommon bacterial flora in the female genitourinary tract. The exact cause of infection for this patientremained unclear. She had no past ill history of systemic diseases, genitourinary disorders or veneraldiseases except for uterine currettage 30 years ago. Therefore, we postulate that the cause of thestreptococcal ovarian abscess in our case may be an ascending infection via genitourinary tract from the
procedure of uterine curretage 30 years ago.Ovarian abscesses might complicate in the preesisting anatomical abnormalities of the ovaries, such
as dermoid cysts, simple cysts and serous cystadenomaL" . As we known, an abscess formation resultingfrom an ovarian mucinous cystadenoma in this patient is the first case reported.
Usually, the clinical features of ovarian abscesses are abdominal or pelvic pain, fever, bowel habitchange, frequency of micturition, leukocytosis, anemia and elevated erythrocyte sedimentation rate1,5,11).Diffuse peritonitis due to rupture of the abscess or hydroureters with renal dysfunction because of ureteralcompression might be complicatedl1). Our patient had abdominal mass, body weight change, frequency ofmicrurition, leukocytosis and elevation of erythrocyte sedimentation rate on admission. However, theabundant pus accumulated in the huge abdominal mass without systemic toxic signs or any gastrointes-tinal disturbance was rarely seen in the previous reports. Two possibilities of mechanism for lexplainingthis phemomenon were (1) the thick cyst-wall with heavy granulation tissue which prevented the bacterialspreading from the abscess cavity to the peritoneum or systemic circulation (2) the probable inhibition ofexpanded multiplication of bacteria in the abscess by unknown substance in the cystic contents.
In summary, an ovarian mucinous cystadenoma complicated with abscess formation has never beenreported. We experienced such a case with unusual clinical manifestations and successful treatment withsurgical removal and parenteral antibiotics. The exact portal or timing of entry for the causativemicroorganism and the duration of the existence of the abscess were both obscure. The probable inhibitoryeffect of the cystic contents on the isolated streptococci is under investigation.
References
1) Willson, J. R.& Black, J. R.: Ovarian abscess, Am. J. Obstet. Gynecol. 90: 34-43, 1964.2) Coe, H. C.: Acute oophoritis complicating pregnancy. Am. Gynecol. J. 670-672, 1891.3) Black, W. T.: Abscess of the ovary. J. Obstet. Gynecol. 31: 487-489, 1936.4) Friedaman, S.& Bobrow, M. L.: Pelvic inflammatory disease in pregnancy, a review of the literature and report of 5
cases. Obstet. Gynecol. 14: 417-419, 1959.5) Harrison, N. A.: Ovarian abscess, a case report and review of the literature. S. Afr. Med. J. 54: 1147-1148, 1978.6) Ginsberg, D. S., Stenn, J. L., Hamod, K. A. et al: Tuboovarian abscess. A retrospective review. Am. J. Obstet. Gynecol.
138: 57-60, 1980.7) Daniel, V. L.& Richard, L. S.: Current treads in the diagnosis and treatment of tuboovarian abscess. A. J. Obstet.
Gynecol. 151: 1098-1110, 1985.8) Pederson, J.& Virata, R. L.: Ovarian abscess secondary to actinomyces isreali. Wis. Med. J. 75: 547-548, 1976.
平成4年3月20日

420 Po-Ren HSUEH et al
9) Miebyl, J. R., Parmky, T. H., Spence, M. R., et al.: Unilateral ovarian abscess associated with the intrauterine device.Obstet. Gynecol. 52: 165-168, 1978.
10) Sidhammed, H.& Hasson, A.: Salmonella infection of ovarian dermoid cyst. Br. Med. J. 3: 140-142, 1975.11) Stewart, J. W.& Leo, J. D.: Ovarian abscess. Report of a case and a review of the literature. Obstet. Gynecol. Surg. 50:
476-485, 1985.
膿 瘍を伴 った卵 巣粘 液 性 の う腫 の1例
台湾省立台南病院内科,*同 産婦人科**台 湾國立成功大学医学院感染症科
酵 博仁 黄 情川 巌 高彬*
林 茂*楊 振典**
(平成3年2月18日 受付)
(平成3年10月8日 受理)
我 々 は稀 に しか み られ な い膿 瘍 を 伴 った 卵 巣 粘
液 性 の う腫 を 経 験 した の で 報 告 す る.
患 者 は75歳 の 女 性,最 近6ヵ 月 間 下 腹 部 腫 脹 お
よび12kgの 体 重 減 少 を 主 訴 とし て 入 院.入 院 時 患
者 は平 熱,軽 い 貧 血 の 他 に 下 腹 部 に30×35cm大
き さの 無 痛 性腫 瘤 が 触 れ た.検 査 所 見 に て 白血 球
数10,500/mm3,血 色 素8.49/dl,血 沈138mm/h,
コ レ ス テ ロール128mg/dl,ト リグ リセ ラ イ ド124
mg/dl,IgG2,680mg/dlで あ った.腹 部 超 音 波 お
よ び腹 部CTに て恥 骨 上 部 か ら中 腹 部 に か け て多
分 葉 状 の 腫 瘤 が認 め られ た.腫 瘤 の 抽 出 液 は 緑 黄
色 で コ レ ス テ ロー ル値1,320mg/dl,ト リグ リセ ラ
イ ド値1,408mg/dlと 高 値 で あ った.排 出 液 を 培
養 し,Streptococcus agalactiaeを 分 離 した.外 科
手 術 を 行 い,摘 出 し た 腫 瘤 は20×25×30cmの も
の で 病 理 検 査 で は感 染 した 粘 液 性 の う腫 で あ っ
た.
患 者 は 入 院30日 後 軽 快 退 院 とな った.
感染症学雑誌 第66巻 第3号


















