Looking for Patterns in Brain Atrophy Gerard R Ridgway (Supervisors: Prof DLG Hill, Prof NC Fox)...
1
Looking for Patterns in Brain Atrophy Gerard R Ridgway (Supervisors: Prof DLG Hill, Prof NC Fox) Principal Component Analysis of Structural MR Images Ged Ridgway & Derek Hill are at the Centre for Medical Image Computing, Dept of Medical Physics & Bioengineering, University College London, WC1E 6BT. Contact: [email protected] Nick Fox is at the Dementia Research Centre, Institute of Neurology, Queen Square, UCL. The DRC provided the anonymised patient data used for the analysis presented here. References [1] NC Fox, PA Freeborough, and MN Rossor. Visualisation and quantification of rates of atrophy in Alzheimer's disease. Lancet. 1996 Sep 21;348(9030):829-30. [2] RO Duda, PE Hart, and DG Stork. Pattern Classification. 2nd Edition, Wiley 2000. Introduction The brain undergoes structural changes in diseases such as Alzheimer’s, the progression of which can be tracked using serial MR Imaging [1]. Statistical learning theory [2] provides techniques that allow patterns in data to be analysed, enabling for example, the development of automated tools for measuring disease severity. We present here early investigations into the use of Principal Component Analysis for exploring patterns in data, and producing lower-dimensional feature vectors suitable for use in classification algorithms. Future Work Consider different options for input images (segmentations, subtraction images, displacement fields, compression maps) and pre-processing (brain extraction, bias correction, contrast equalisation). Explore use of surfaces, eg from segmentations. Following Principal Component Analysis, develop a classifier using for example, Fisher’s Linear Discriminant, or a Support Vector Machine [2]. (Note that PCA’s goal is representation, not discrimination, so must take care not to lose information that separates classes.) Investigate more advanced non-linear methods, eg Kernel-based PCA and Generalised Discriminant Analysis. Try Support Vector Regression for evaluating disease progress. Analyse greater quantities of data – particularly more time-points. Use techniques such as Incremental PCA if necessary. Method All work has been performed on three- dimensional T1-weighted volumes acquired at 1.5T, which have been affinely registered to the MNI Atlas shown above. For simplicity, results are presented for a single coronal slice (position indicated on other views) which was chosen to exhibit some anatomical areas of interest in Alzheimer’s Disease. Template used for spatial normalisation, with results plane of interest indicated. Longitudinal Fissure Lateral Ventricle Insula Hippocampus Principal Component Analysis The ‘principal components’ or ‘modes’ essentially represent the most pronounced ways in which the data vary. PCA indicates their relative significance, and by removing components with lower variance the data is reconstructed as well as possible (with respect to least squared error) using that number of modes. MRI brain volumes contain millions of voxels; by using PCA we can represent the images by a much smaller numbers of features, which may still characterise important aspects of patient variability and disease progression (or disease characteristics as in [3]). Investigation 1 Natural variability within patient brains is explored for a cohort of 16 individuals with suspected Alzheimer’s Disease. Raw images shown right. The most noticeable feature is the large variability in ventricular size and shape. The fifteen non-zero principal components are shown below: Ventricular modes are prominent, as expected. Variability around the hippocampus can be identified. Scalp is significant in many components. Low-variance modes are still anatomically meaningful; there is no clear cut-off (see graph). The graph to the right shows the proportion of the total variance accounted for (y- axis) by each of the 15 principal components (x). The general decline indicates that the strongest components explain the majority of the variation seen in the data. We now investigate the reconstruction of a randomly chosen image (the 6 th ) using the first five principal components (those left of the red line above). From left to right below: original, reconstruction, residual error. Most major gyral, sulcal, ventricular and hippocampal features are reproduced acceptably with just five modes. Residuals still show anatomical patterns, indicating some loss of information, as would be expected. This project is funded through an EPSRC CASE Studentship with GSK Investigation 2 We consider two time- points, roughly 12 months apart, for 8 individuals with suspected AD, in order to explore longitudinal changes caused by the disease. Images are shown in registered pairs, with time 2 below time 1. The fifteen non-zero principal components are shown below: Ventricula r components important again. Several modes show Hippocampal variability. Distinguishi ng atrophy from natural variability is difficult though. First seven modes clearly dominate in terms of anatomically interesting change (later modes are chiefly scalp, or motion artefact). The graph of relative component variance shows a distinct drop after the 7 th mode, providing mathematical support for the above anatomical conclusion. Each of the 16 images is reconstructed as a linear combination of the 15 Principal Components; below, the 16-by-15 coefficients for this combination are illustrated as an image (red +ve, blue -ve). Image pairs have very similar ‘score profiles’ along rows. Again, importance of first 7 modes clear. Some hints that certain columns might help to distinguish (some?) of the time-points well, eg the 8 th feature. [3] CE Thomaz, JP Boardman, DLG Hill, JV Hajnal, AD MA Rutherford, DF Gillies, and D Rueckert. Using a Maximum Uncertainty LDA-based Approach to Classify and Analyse MR Brain Images. MICCAI 2004, LNCS 3216, pp. 291-300. Investigation 3 Instead of raw images, we now analyse grey matter segmentations (to be precise, Jacobian-modulated spatially-warped images from SPM5). Eighteen AD patients at two time-points were used, only some of which are displayed here. The sharp drop in proportional component variance (after the 16 th PC) indicates that the variability in the data can be characterised with relatively few modes, and perhaps distinguishes between components due to real variation and those due to registration or segmentation errors (?) This hypothesis is not readily apparent from visual inspection of the modes, but might be confirmed with further modelling and analysis. Components 7 to 24 fail to show any clear transition s that correspond to the drop seen in the graph above.
-
Upload
margarita-ware -
Category
Documents
-
view
216 -
download
3
Transcript of Looking for Patterns in Brain Atrophy Gerard R Ridgway (Supervisors: Prof DLG Hill, Prof NC Fox)...

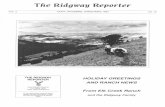
Looking for Patterns in Brain Atrophy
Gerard R Ridgway (Supervisors: Prof DLG Hill, Prof NC Fox)
Principal Component Analysis of Structural MR Images
Ged Ridgway & Derek Hill are at theCentre for Medical Image Computing,Dept of Medical Physics & Bioengineering,University College London, WC1E 6BT.
Contact: [email protected]
Nick Fox is at the Dementia Research Centre,Institute of Neurology, Queen Square, UCL.
The DRC provided the anonymised patient dataused for the analysis presented here.
References [1] NC Fox, PA Freeborough, and MN Rossor.
Visualisation and quantification of rates of atrophy in Alzheimer's disease.Lancet. 1996 Sep 21;348(9030):829-30.
[2] RO Duda, PE Hart, and DG Stork.Pattern Classification. 2nd Edition, Wiley 2000.
IntroductionThe brain undergoes structural changes in diseases such as Alzheimer’s, the progression of which can be tracked using serial MR Imaging [1].
Statistical learning theory [2] provides techniques that allow patterns in data to be analysed, enabling for example, the development of automated tools for measuring disease severity.
We present here early investigations into the use of Principal Component Analysis for exploring patterns in data, and producing lower-dimensional feature vectors suitable for use in classification algorithms.
Future WorkConsider different options for input images (segmentations, subtraction images, displacement fields, compression maps) and pre-processing (brain extraction, bias correction, contrast equalisation). Explore use of surfaces, eg from segmentations.
Following Principal Component Analysis, develop a classifier using for example, Fisher’s Linear Discriminant, or a Support Vector Machine [2]. (Note that PCA’s goal is representation, not discrimination, so must take care not to lose information that separates classes.)
Investigate more advanced non-linear methods, eg Kernel-based PCA and Generalised Discriminant Analysis. Try Support Vector Regression for evaluating disease progress.
Analyse greater quantities of data – particularly more time-points. Use techniques such as Incremental PCA if necessary.
MethodAll work has been performed on three-dimensional T1-weighted volumes acquired at 1.5T, which have been affinely registered to the MNI Atlas shown above.
For simplicity, results are presented for a single coronal slice (position indicated on other views) which was chosen to exhibit some anatomical areas of interest in Alzheimer’s Disease.
Template used for spatial normalisation, with resultsplane of interest indicated.
Longitudinal Fissure
Lateral Ventricle
Insula
Hippocampus
Principal Component AnalysisThe ‘principal components’ or ‘modes’ essentially represent the most pronounced ways in which the data vary. PCA indicates their relative significance, and by removing components with lower variance the data is reconstructed as well as possible (with respect to least squared error) using that number of modes.
MRI brain volumes contain millions of voxels; by using PCA we can represent the images by a much smaller numbers of features, which may still characterise important aspects of patient variability and disease progression (or disease characteristics as in [3]).
Investigation 1Natural variability within patient brains is explored for a cohort of 16 individuals with suspected Alzheimer’s Disease.
Raw images shown right.
The most noticeable feature is the large variability in ventricular size and shape.
The fifteen non-zero principal components are shown below: Ventricular modes
are prominent, as expected.
Variability aroundthe hippocampuscan be identified.
Scalp is significantin many components.
Low-variance modesare still anatomicallymeaningful; there is noclear cut-off (see graph).
The graph to the right shows the proportion of the total variance accounted for (y-axis) by each of the 15 principal components (x).
The general decline indicates that the strongest components explain the majority of the variation seen in the data.
We now investigate the reconstruction of a randomly chosen image (the 6th) using the first five principal components (those left of the red line above).
From left to right below: original, reconstruction, residual error.
Most major gyral, sulcal, ventricular and hippocampal features are reproduced acceptably with just five modes. Residuals still show anatomical patterns, indicating some loss of information, as would be expected.
This project is funded through an EPSRC CASE Studentship with GSK
Investigation 2We consider two time-points, roughly 12 months apart, for 8 individuals with suspected AD, in order to explore longitudinal changes caused by the disease.
Images are shown in registered pairs, with time 2 below time 1.
The fifteen non-zero principal components are shown below:
Ventricular componentsimportant again.
Several modes show Hippocampal variability.
Distinguishing atrophy from natural variability is difficult though.
First seven modes clearly dominate in terms of anatomically interesting change (later modes are chiefly scalp, or motion artefact).
The graph of relative component variance shows a distinct drop after the 7th mode, providing mathematical support for the above anatomical conclusion.Each of the 16 images is reconstructed as a linear
combination of the 15 Principal Components; below, the 16-by-15 coefficients for this combination are illustrated as an image (red +ve, blue -ve).
Image pairs have very similar ‘score profiles’ along rows.
Again, importance of first 7 modes clear.
Some hints that certain columns might help to distinguish (some?) of the time-points well, eg the 8th feature.
[3] CE Thomaz, JP Boardman, DLG Hill, JV Hajnal, AD Edwards,MA Rutherford, DF Gillies, and D Rueckert.Using a Maximum Uncertainty LDA-based Approach toClassify and Analyse MR Brain Images.MICCAI 2004, LNCS 3216, pp. 291-300.
Investigation 3Instead of raw images, we now analyse grey matter segmentations (to be precise, Jacobian-modulated spatially-warped images from SPM5). Eighteen AD patients at two time-points were used, only some of which are displayed here.
The sharp drop in proportional component variance (after the 16th PC) indicates that the variability in the data can be characterised with relatively few modes, and perhaps distinguishes between components due to real variation and those due to registration or segmentation errors (?)
This hypothesis is not readily apparent from visual inspection of the modes, but might be confirmed with further modelling and analysis.
Components7 to 24 fail toshow any cleartransitions that correspond to the drop seen in the graph above.