Long-Term Outcomes in Hypertrophic Cardiomyopathy Caused by Mutations in the Cardiac...
31
1 Long-Term Outcomes in Hypertrophic Cardiomyopathy Caused by Mutations in the Cardiac Troponin T Gene Running title: Pasquale et al.; Outcomes in troponin T mutations Ferdinando Pasquale, MD, PhD 1,2 ; Petros Syrris, PhD 3 ; Juan Pablo Kaski, BSc, MBBS, MD 4 ; Jens Mogensen, MD, PhD 5 ; William J. McKenna, MD, DSc, FRCP, FESC 1 ; Perry Elliott MD 1 1 The Heart Hospital, Institute of Cardiovascular Sciences, University College London, London, United Kingdom; 2 Istituto di Cardiologia Ospedale S.Orsola Malpighi, Bologna, Italy; 3 Institute of Cardiovascular Science, University College London; 4 Great Ormond Street Hospital for Children, London, United Kingdom; 5 Skejby University Hospital, Åarhus, Denmark Address for correspondence: Dr Perry Elliott The Heart Hospital 16-18 Westmoreland Street London, W1G 8PH, United Kingdom Tel: +44-207-573-8888 Fax: +44-207-573-8838 E-mail: [email protected] Journal Subject Codes: [109] Clinical genetics; [11] Other heart failure; [193] Clinical studies; [15] Hypertrophy; [16] Myocardial cardiomyopathy disease l L a r e l, In In In In Inst st st s stit it it t tut ut ut ut ute of o o o o Cardiovascul ar S S Sci ci ci ci iences, U U U U Uni n n n ve ve ve ve versity College L s s sti t t t t tu t t t to di Ca C Card d dio io io i lo o o og g gi a Os O O Os Osp p peda d dale e S.Or Or Or Or Orso so so s la a Mal al alpi pi pi i ig g gh g g i, B B B B Bol ol l l log g gn n na r Sci ie i ie ien nc n e, U U U U Uni ni ni ivers s s sit it it it ity Coll l l ll l ege Lo L Lo Lo L nd d d d don on n n n; 4 4 4 4 Gr G G G G eat t t t Or O O O O mond d d S S S St t tree d d don on on, , Un Unit ited d ed K K Kin i ingd d gdom om om; ; ; 5 5 5 5 5 Sk Sk Sk Sk S ej ej j ejb by by by U U Uni ni nive ve vers rs rsi it it ity y y Ho Ho Ho H sp sp spit i it it i al al al, , Åa Åa Åarh rh rhus us s us by guest on May 12, 2018 http://circgenetics.ahajournals.org/ Downloaded from by guest on May 12, 2018 http://circgenetics.ahajournals.org/ Downloaded from by guest on May 12, 2018 http://circgenetics.ahajournals.org/ Downloaded from by guest on May 12, 2018 http://circgenetics.ahajournals.org/ Downloaded from by guest on May 12, 2018 http://circgenetics.ahajournals.org/ Downloaded from
-
Upload
truongquynh -
Category
Documents
-
view
216 -
download
2
Transcript of Long-Term Outcomes in Hypertrophic Cardiomyopathy Caused by Mutations in the Cardiac...

1
Long-Term Outcomes in Hypertrophic Cardiomyopathy Caused by
Mutations in the Cardiac Troponin T Gene
Running title: Pasquale et al.; Outcomes in troponin T mutations
Ferdinando Pasquale, MD, PhD1,2; Petros Syrris, PhD3; Juan Pablo Kaski, BSc, MBBS, MD4;
Jens Mogensen, MD, PhD5; William J. McKenna, MD, DSc, FRCP, FESC1; Perry Elliott MD1
1The Heart Hospital, Institute of Cardiovascular Sciences, University College London, London,
United Kingdom; 2Istituto di Cardiologia Ospedale S.Orsola Malpighi, Bologna, Italy; 3Institute
of Cardiovascular Science, University College London; 4Great Ormond Street Hospital for
Children, London, United Kingdom; 5Skejby University Hospital, Åarhus, Denmark
Address for correspondence:
Dr Perry Elliott
The Heart Hospital
16-18 Westmoreland Street
London, W1G 8PH, United Kingdom
Tel: +44-207-573-8888
Fax: +44-207-573-8838
E-mail: [email protected]
Journal Subject Codes: [109] Clinical genetics; [11] Other heart failure; [193] Clinical studies; [15] Hypertrophy; [16] Myocardial cardiomyopathy disease
l L
a
r e
l, InInInInInstststsstitititttututututute ofoooo Cardiovascular SSSciciciciiences, UUUUUninnn veveveveversity College L
ssstittt ttuttt to di CaCCardddioioioi loooogggig a OsOOOsOspppedaddalee S.OrOrOrOrOrsososos laa Malalalpipipiiiggghgg i, BB BBBolollllogggnnna
r Sciieiieienncn e, U UU UUnininiiversrsrsrsititititity Colllllll ege LoLLoLoL ndddddononnnn; 4444GrGGGG eat t t t OrOOOO monddd SS SStttree
dddononon,, UnUnititedded KKKiniingddgdomomom;;; 55555SkSkSkSkS ejjejjejbbybyby U UUnininiveveversrsrsiititity y y HoHoHoH spspspitiititi alalal,, ÅaÅaÅarhrhrhusussus
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from
by guest on M
ay 12, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from
by guest on M
ay 12, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

2
Abstract:
Background - Hypertrophic cardiomyopathy (HCM) caused by mutations in the cardiac troponin
T gene (TNNT2) has been associated with a high risk of sudden cardiac death (SCD) and mild
left ventricular hypertrophy (LVH). However, previous studies are limited by sample size, cross-
sectional design and few data in relatives.
Methods and Results - 552 unrelated HCM probands were screened for TNNT2 mutations. First-
degree relatives were invited for clinical and genetic evaluation. Ninety two individuals (20
probands and 72 relatives) carried TNNT2 mutations (51 (55%) male; 30±17 years). ECGs and
echo were available in 87 (95%) and 88 (96%) individuals, respectively. ECG was normal in 13
(68%) children (< 16 years) and 13 (19%) adults. Echo was normal in 18 (90%) children and 16
(24%) adults; 7 (10%) adults had a normal ECG and Echo.
Thirteen (65%) of 20 families had a history of SCD. Follow-up was available for 75 patients
(mean 9.9 ± 5.2 years); 2/16 adults and 2/18 children with normal echoes developed left
ventricular hypertrophy (LVH). Twenty three (22%) received an implantable cardioverter
defibrillator (ICD) (20 for primary prophylaxis). One child and three adults died from SCD and 2
adults were resuscitated from ventricular fibrillation. One patient had an appropriate ICD
discharge. The rate of cardiovascular death, transplant and ICD discharge was 1.6% (0.016
person/year; CI 0.83-2.79%) and SCD 0.93% (0.0093 person/year; CI 0.37-1.92%).
Conclusions - LVH is rare in children with TNNT2 mutations. LVH is absent in minority of
adults, but most have an abnormal ECG. In spite of adverse family histories, the rate of
cardiovascular death during follow-up was similar to that reported in large referral populations.
Key words: cardiomyopathy; gene mutation; hypertrophic cardiomyopathy; sudden death; troponin T
was avaavavavavavavavavavavavavavavvavvvvaiaiaiaiiaiaiaiaiaiaaaiaiaiaiaiaiaaia lalalalaalalalaalaalaallalalalaaablblblblblbblblblbblbllbblblbblblble eeeee eeeee eeeee eeee fffffofofffffffffff r
r o
p r
2
a r
rs))))); ; ; ; ; 2/2/2/2/2/1616161616 a a dududududults and 2/18 childrenen with nooooormrrrr alalalalal echoes develo
phhhhhyyy yy (LVH)). Twwwennntytytytyy thrhh eeeeee (22222%)%) recececececeieieeie vevved dd annn iiimpmpmppplantnttntntabble cccarn
20 for primararararary yyyy prpppp opopopopophyhyhyyylaxiis)s)))). Onne chhililillild dddd and thhhrrrrrrr ee adults died
atttteded f frororom m m veveventntntriricucuculalarrr fifibrbrrrilillalatitiononon. OnOnOneee papapatitienenenttt hahadd ananan aa apppppprororoprprrpr
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

3
Introduction
Hypertrophic cardiomyopathy (HCM), defined as left ventricular hypertrophy (LVH) in the
absence of abnormal loading conditions, occurs in approximately 1 in every 500 adults1. The
disease can present with cardiovascular symptoms at any age and is a frequent cause of sudden
cardiac death in young people2-4. In the long-term, many patients develop progressive symptoms
caused by a gradual deterioration in left ventricular function5,6.
HCM is usually inherited as an autosomal dominant trait caused by mutations in genes that
encode proteins of the cardiac sarcomere7-10. Based on the assumption that locus and allelic
heterogeneity have different effects on myocyte structure and function, it has been hypothesized
that individual mutations are associated with specific phenotypes10-15. If this is correct, then
mutation analysis could be used to guide therapy (e.g. prophylactic implantation of implantable
cardioverter defibrillators) and counselling strategies for families. One of the first reported
genotype-phenotype associations in HCM was a high prevalence of sudden cardiac death in
young carriers of mutations in the cardiac troponin T gene (TNNT2)9,16-18, paradoxically in the
presence of only mild left ventricular hypertrophy19,20. While, this finding has been used in
subsequent consensus management guidelines for HCM, studies examining the natural history of
troponin T gene mutations are limited by the small size of patient cohorts (often single families),
cross-sectional study design and a lack of data on disease expression in relatives. The aim of this
study was to examine clinical outcomes in a relatively large cohort of patients and relatives with
mutations in the cardiac troponin T gene.
mption that locusuuuuuuuuuuuuuuuu
nctionoononononononononononononononnnn, , ,, ,, ,,, ,, ,, ,,, ,,,,, itiitiitiiitiiiititititititt hh h hhhh hhhh hhh h h hhasasasasasasasasassaasassasasasasass bb b b b b bb bbb b bbb bb b bb b bbee
t o
u
l s
tiononononons are aaaassssssssssococcocciaiaiaiaiateteteteed d d d d wiwiwiwiwiththththh s ss spepepepeecic fficc phphphphphenenenenenotototototypyypyppeseseseses10-15. IfIfIfIfIf t t hihihihih s s s s s isisisiss c o
ulllldd ddd bebebebebe uuuuuseseed ddd totototoo g gggguiuuu dedededede ttttthehhhh rrrrrapapapapapyyy yy (e(e(e(e(e g.gggg. prprprprpropopopopophyhyhyhyhylalalalalactctctccticiciciic iiiiimpmpmpmpmplalalall ntntntntntatatatatioioioioion nn
latatatororors)s) a a andndnn cococounununsesesellllining g g g stststrararatetetegigiggg eseses f ffororor f famamamilillieiesss. OO Onenene oo off ththeee fifirsrssrs
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

4
Methods
This study was approved by the local ethics committees of St George’s Hospital and University
College Hospitals London, United Kingdom. All study participants gave written informed
consent for venesection and DNA analysis. The study conformed to the principles of the Helsinki
declaration. All authors had full access to the data and take responsibility for its integrity. All
authors have read and agree to the manuscript as written.
Clinical evaluation
The study cohort comprised apparently unrelated HCM probands referred to a dedicated
cardiomyopathy clinic over a 10 year period to St. George’s Hospital and then subsequently
followed (2003 to 2005) at The Heart Hospital, UCLH, London, United Kingdom) that were
tested for mutations in the TNNT2 gene. All relatives of mutation positive individuals were
invited for clinical and genetic evaluation.
Patients and consenting relatives underwent supine 12 lead electrocardiography (ECG), M-mode,
2-D and Doppler echocardiography, symptom limited upright exercise testing with simultaneous
respiratory gas analysis and 24-48 hour ambulatory ECG monitoring in accordance with
previously described methods 21. LVH on the 12 lead ECG was defined using the Romhilt-Estes
score system22; LVH was defined as a score 5. ECGs in infants and children were reviewed by
a pediatric cardiologist (JK) and were coded using standard criteria23.
HCM was diagnosed in probands and relatives when the maximum left ventricular wall thickness
(MLVWT) measured 13 mm in one or more myocardial segments on echocardiography or
s referred to a dedddddddddddddd
pital lll lllllllllll ananananananananananananannananananand d dddddddddddddddd thththththththththhththththththhttheneneneneenenenenenenenenennenennnnneenn s u
0 m
i i
n
00505050505)) at TTTTThehehehee H HH HHeaeaeaeaeartrtrtrtrt H H HHHososososospipipipipitatatatat l, U U UUCLLH,H,H,H,H, L LL LLononononondodododdon,n,n,n,n, UU UU Unininininiteteteteted ddd d KiKiKiKiKingngngngngdodddd m
in thththththe eeee TNTNTNTNTNNTNTNTNTT2 2222 ggegegeg nenenenee. AlAAAA l l rererererelalalalalatititititiveveveveves ss ofofofofof mmmmmutututututatatatatatioioioioionnn nn popoopoosisisisis tititititiveeeee ii iiindndndnddivivivivivi
ndnnd gg geneneneteteticic ee evavavaluluatatatioionnn.
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

5
when left MLVWT exceeded two standard deviations corrected for age, size and gender in the
absence of other diseases that could explain the hypertrophy24. The pattern of hypertrophy was
classified as asymmetrical septal, concentric, or predominantly apical25. In probands with sudden
death as the first clinical manifestation, the diagnosis of HCM was, when possible, confirmed at
post-mortem. Relatives were considered clinically affected when they fulfilled extended familial
criteria for HCM26.
During ambulatory monitoring, supraventricular tachycardia was defined as three or more
consecutive supraventricular premature beats at a rate more than 100 beats/min and non-
sustained ventricular tachycardia (NSVT) as three or more consecutive ventricular ectopics at a
rate more than 120 beats/min. An abnormal blood-pressure response during symptom limited
upright exercise testing was defined as a failure of systolic blood pressure to rise by more than
25 mmHg from baseline values, or a fall of more than 10 mmHg from the maximum blood
pressure during upright exercise27.
Clinical Risk Stratification
Risk stratification was considered complete when patients had at least one echocardiogram,
ambulatory ECG recording and exercise test. Major risk factors for sudden cardiac death were
defined as: a family history of sudden cardiac death at an age 40 years; a syncopal episode
suggestive of arrhythmic origin; NSVT during ambulatory electrocardiography; MLVWT
30mm; and an abnormal exercise blood pressure response28.
Genetic evaluation
100 beats/min nnnnnnnnn nnnn a
cutivevvevevevevevveveveveveveveveeveveveve vv v vv vvvvv vvvvv vv veneneneneneneneneneneneneneenenenenne trtrtrttrtrtrtrtrrtrtrrtrtrtrtrrriccicicicicicicciciciciciciciciciciiicccuuuuuluuuuu
m
i e
m
eaeaeaee ttsttt /minnnnn. AnAnAnAAn a aaaabnbnbnbnbnororororrmamamamamal blbblbb oooooooood-d prpressssssususususurerererere rrrrreseesespopopopoponsnnnn e e e ee dududududurirrr ngngngngng s s s ssymymymymy
inggggg w wwwwasasasasas dddddefefefe inininiineeeeeddd dd as aaaaa fffffaiaaa luuuuurerereee oo ooof ffff sysysysysystststttolololololicicicicic bb bbblololololoododododod prpppp esesesesessususuusureeeee tttto ooo riririrr sssess
lllinineee vavavalululuuueseses, , ororor aa a f falalll ofof momomorerere tt thahannn 101010 mm mmHmHmHg g g g frfromomom tt thehe mm maxaxaximimm
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

6
Genomic DNA was extracted from whole blood and protein encoding exons of TNNT2 were
amplified using standard protocols (primer sequences and conditions for polymerase chain
reaction amplification are available upon request). Mutation analysis of TNNT2 was performed
by fluorescent SSCP (F-SSCP) and direct sequencing of abnormal conformers. As reported
previously, the sensitivity of F-SSCP to identify sequence variations in TNNT2 was 100%29,30.
DNA was screened for mutations in TNNT2 hot spot exons 8, 9 and 16. If these did not show
mutations, exons 10, 11, 13, 14 and 15 were also screened. When no mutation was identified the
TNNT2 gene was completely sequenced. When a disease causing mutation was found in
TNNT2, genetic analysis was interrupted.
A cohort of 200 healthy Caucasian volunteers served as controls for TNNT2 sequence variants
reported in this study. A sequence variant was defined as a pathogenic mutation if it was absent
in a cohort of 400 control chromosomes; it was predicted to result in a premature truncation,
frameshift or abnormal splicing or affected conserved amino acid residues; and cosegregated
with disease in the family (when information was available). Variants previously reported as
mutations were considered disease causing unless we could show otherwise. The likelihood of
pathogenic effect of all TNNT2 sequence variants was determined by in silico prediction
methods: PolyPhen-2 and SIFT for missense mutations and splice site prediction software Neural
Network and Genio/splice.
Statistics
SPSS (v13.0) was used for all statistical analyses. Normally distributed data are expressed as
mean (95% confidence intervals (CI). Differences between means were compared using the
for TTTTTTTTTTTTTTTTTTNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNN T2T2T2T2T2T2T2T2T2TT2T22T2T2T2T2T2T2 s s ss s sss s s ssssssssssseqeeeeeeeeeeee
y
o e
m c
y... . AAA AA sequuuuuenenennencecececee vavavavavarirrrr ananananant ttt t wawawawawas sss deddedd finened asasasasas a aa aa pppppatatata hohohohohogegggg nininininic cccc mumumumumutatatatatatitititit onoooo
ontrtrtrtrrololololol ccccchrhrhrhrhromomommmosososossomomomomesesesess;; ; ititititit wwwwwasasasasas pp ppprrrrredededededicicicicicteteteteted dddd totototoo rrrrresesesesesulululuu ttt tt innnnn aa aaa pppppreeeeemamamamam tututututurerr
mmmmalal ss splplicicccining g g g ororor aa affffececectetetedd ccconononseseservrvrveded a a amimim nonono a a acicidd rereresisidudueseses;;; ananandd cccc
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

7
unpaired two tailed Student t-test. The chi-square test was used for comparison of categorical
data. The Mann-Whitney U test was used to analyze non-normally-distributed continuous data.
The predefined end-points in the survival analysis were: sudden cardiac death (witnessed death
with or without documented ventricular fibrillation, death within one hour of new symptoms, or
nocturnal deaths with no antecedent history of worsening symptoms); first appropriate ICD
shock; heart failure death (death preceded by signs and/or symptoms of heart failure, including
cardiogenic shock); orthotopic heart transplantation; and other cardiovascular death (stroke,
pulmonary or peripheral arterial embolization, procedure related and myocardial infarction).
Deaths of unknown cause were classified as non-cardiovascular deaths.
The cumulative probability for the occurrence of an outcome was estimated using the Kaplan-
Meier method. Survival from cardiovascular death, cardiac transplant and appropriate ICD shock
was modelled for all probands and relatives with an identified mutation in the TNNT2 gene from
their first evaluation at our institution.
To facilitate comparison with previously published data, survival was also modelled from birth
incorporating additional data on relatives (alive and dead) identified from pedigree analysis that
were known to have HCM (in life or at autopsy) or were obligate carriers of a TNNT2 mutation.
Analysis of survival from birth was also performed for individual mutations.
A p value <0.05 was considered significant in all analyses.
deaths.
b n
i p
N
baaaaabibibibibility fffffororororor ttt ttheheeee oo o oocccccccccurururururrererererencncncncnce eee ofoofoo ann outututututcococococomememememe wwwwwasasasasas estststststimimimimimatatataa ededededed uuu u usissss n
ivalalalalal f ffffrororororom mmmm cacacacardrdrdrdrdioioioioiovavvv scscscscscululululular dd dddeaeaeaeaeattttth,hhh cccccarararrrdididididiacacacacac ttttrararararansnsnsnsnsplplplpplannnnnt tttt ananananand dddd apapapaapprprprprpropoooo
ppprororobabandndndddsss ananandd rererelalatitivevevesss wiwiww thth ananan i idedeentntntififieied d mumumutatatatitiononon i innn ththeee TNTNNTN
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

8
Results
Genetic investigations
Five hundred and fifty two probands were screened for TNNT2 mutations. Twenty (3.6%) had
pathogenic mutations. Two hundred and thirty six relatives consented to clinical and genetic
testing; of these, 72 (30.5%) had a mutation. Ethnicity data was confirmed in 18 of the 20
families with TNNT2 mutations: 1 family of Indian ethnicity; 1 Caribbean; 1 Pakistani and the
remaining 15 families White British.
Twelve different mutations in exons 8, 9, 11, 15 and 16 were identified in 20 families:
Arg278Cys in 3 families; Arg92Leu in 2 families; Arg92Trp in 3 families; Glu163del in 3
families; IVS15+1G>A in 2 families; and Ala104Val, Arg278His, Arg92Gln, Arg94Leu,
Glu163Lys, Glu83Lys, Ile79Asn in single families. Of the 12 sequence variants in this study, 11
have already been reported (supplemental table 1) as disease causing in HCM.9,16,18,20,29,31,32
A summary of the bioinformatics analysis of the missense mutations (i.e. 9 known and 1 novel)
is provided as a supplemental data file (supplemental table 2).
Analysis of the IVS15+1G>A mutation by splice site prediction software (Neural Network and
Genio/splice) showed that this sequence change completely abolishes the splice donor site of
exon 15 of TNNT2 and is predicted to result in abnormal splicing of the troponin T protein.
The Arg278His sequence variant has not been reported before and was considered pathogenic on
the basis of definition described in the Methods section.
Clinical investigations
3 families; Gluuuuuuuuuu1611111111111
s, Argrrgrgrgrgrgrgrgrgrgrgrgrgrgrggrgrgrgrgggg92992922929929292992929292929292292929 GlGlGlGlGlGlGlGlGlGlGlGlGlGlGGlGGlG n,n,n,n,nn,n,n,n,nn,n,n,n,nn,n,nn,,nn, AAAAAAAA AAAAAAA A Ar
y
p
w
yyys,s,s,s,s, Ile799999AsAsAsAsAsn nnn innininin s s s ssinininininglglglglgle e ee e fafafafaamimimilililll esee . OfOffff ttt t thehehehehe 111112 2 2 22 seseseseequqqqq enennenencecececece v v v vararararariaiaiaiaiantntntntnts
poooortrtrtrtrtededededed (((((sususuupppppppppleleleleemmemmm ntntntntntaaaal llll tttat blblblblble eeee 1)1)1)1)1) aaaaass sss dididididiseseseseseasasasasasee eee cacacacacausususususininining gggg ininininin HHHHHCMCMCMCMCM.999,1
oooininfoformrmrmatataticicsss anananalalysysysyy isis oo of f f f ththeee mimissssssenenensesese mm mutututatatatioionsnsns ( ((((ii.eee. 99 9 k knononowwww
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

9
ECG and echocardiogram at first evaluation were available for review in 87 (95%) and 88 (96%)
of the 92 mutation carriers. At least one ambulatory ECG recording was available in 68 (74%)
patients.
The ECG characteristics of adult and pediatric mutation carriers are shown in table 1 Thirteen
adults and 13 children had a normal ECG. In the pediatric population, the echo was normal in 18
individuals (90%). Two children aged 14 and 15 years had an abnormal echo with asymmetric
septal hypertrophy (ASH) and concentric hypertrophy, respectively; the ECG was abnormal in
both children. In adults, the echo was normal in 16 individuals (24%). The echo features of the
adult population are shown in Table 2. The relation between echo and ECG findings in adults are
shown in figure 1. The relation between age and echo findings at initial evaluation is shown in
figure 2.
Risk stratification at the initial clinical evaluation was complete for 54 (76%) adults and 10
(47%) children (table 3). A history of sudden cardiac death at any age was present in 13 (65%) of
the 20 families analyzed. Eight of these 20 families (40%) had a family history of multiple
sudden cardiac deaths; in 5 families (25%) there was only one sudden cardiac death.
Pedigree Analysis
In addition to the 92 proven carriers of a TNNT2 mutation, 29 cases of sudden cardiac death
were identified from pedigree analysis. Of these, five (age of death: 17, 21, 26, 22, and 51 yrs)
had a post-mortem report consistent with HCM; five (age of death: 38, 42, 59, 53, 50 yrs) were
obligate carriers of a mutation; and two were known to be affected with HCM before death but
were followed at other centers. A further 17 relatives (mean age 24 years; range: 5 to 59 years)
o and ECG finnnnnnnnnndidddddddddddddd
t initittiitititiitiiittititiialalallalaalalalalalalalalalalalalalal e eee eeeee eeeeee eevvvvvvvvvvvvvvvvvvvvalalaalalaalalalalalalalalalaaa uauauauuauauauauauauauauauauauauauuauuuaatttttitttttt o
utttthehe i ininititiiiiaaall clclininicicalal ee evavavaluluuuatatatioionnn wawawasss cococompmpmpppleletetete f fororor 55 5444 (7(7(( 6%6%6%)) adaddu
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

10
died suddenly in circumstances suggesting a cardiac origin, but as the diagnosis of HCM could
not be confirmed they were excluded from further analysis.
Changes in echocardiographic parameters during follow-up
Follow up echoes were available in 45 adults and 14 children (mean intervals between echoes 9.3
± 5 years and 6.9 ± 2.9 years, respectively). There were no significant changes in mean cardiac
dimensions or systolic function, but 3 patients (MLVWT: 23, 15 and 11 mm) aged 26, 60 and 58
years at first evaluation (follow up 16 ± 2yrs (13 to 17 years)) developed left ventricular
dilatation and impaired systolic function.
Follow-up echoes were available in 11 of 16 adults with a normal echo at presentation (interval
between echoes 8.7 ± 5.2 years (range 1 to 18 years). Two developed hypertrophy: one with a
normal echo at 27 years had concentric hypertrophy with a maximal wall thickness of 17mm
when 42 years old; the second had a normal echo (MLVWT: 9mm) aged 65 and ASH (13 mm)
by the age of 74 years.
Thirteen of the 18 children with normal echoes at first evaluation had follow-up echoes (range 4
to 15 years, mean 6.7 ± 3 years): two developed asymmetric left ventricular hypertrophy at the
age of 19 and 29 years, respectively.
Events during follow-up
Clinical follow-up was available for 75 patients (81%) (mean 9.9 ± 5.2 years). The duration of
follow-up in adults (n=57) was 10.3 ± 5.4 years and in children (n=18) 8.2 ± 3.5 years.
e n
± h
e e
errrrre e eee availalalalal blblblblble eee innininin 1111111111 ooooof f ff f 1616161616 a aa adududududultl s wwiththththth a aa aa nn nnnororororo mamamamamal ll eccccchohohohoho a a aaat t t prprprprpreseseseseseneeee
± 55555 2.222.2 yyyyyeaeaeaeaearsrsrss ( ((((rarararaangngngngge 111 11 tototototo 1888 88 yyyyyeaeaeaeaarsrsrsrss)).) TTTTTwowowowowo dd dddevevevevevelelelelelopopopopopededededed hhhhhypypyyypererererertrtrtrtropopopopoph
earararsss hahad d d d cococoncncncenenentrtrtricic h hypypypppererertttrororophphpp y y y yy wiwiiththtth aa a mm maxaxaximimalal ww waaattttt llll tt thihickckneneene
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

11
Twenty three individuals (22%) received an ICD: 20 for primary prophylaxis; 2 for secondary
prophylaxis; and one biventricular device for congestive cardiac failure. Three persons received
a dual chamber pacemaker for AV nodal disease and one for left ventricular outflow tract
obstruction. One individual underwent radiofrequency ablation for atrial fibrillation and later
required atrio-ventricular node ablation and biventricular pacemaker insertion. One individual
underwent septal myomyectomy for left ventricular outflow tract obstruction.
Three adults died from sudden cardiac death and 2 were resuscitated from ventricular fibrillation
(VF); of these, three (age at death or VF 20, 29, and 63 years) were males of Indian ethnicity
from the same family with the Arg92Gln mutation. The maximal wall thickness in these
individuals was 27mm, 15mm and 20mm, respectively. The third sudden death occurred in a
female carrier of Glu163del, aged 62 years with NSVT, a family history of multiple sudden
deaths and MVLWT 18mm. No post-mortem data were available. One female carrying the
Arg278Cys mutation was resuscitated from VF arrest aged 26. At that time she had a concentric
hypertrophy and the maximal wall thickness was 23 mm. She is still alive 18 years later, but has
left ventricular dilatation and impaired left ventricular systolic function. She has a monozygotic
twin who had an ICD implanted for primary prophylaxis, but during follow up she did not
receive any ICD therapies.
Of the remaining adults, one (MLVWT 23mm) received an appropriate ICD shock for
symptomatic VT (IVS15+1G>A) and four (Glu163del; Arg94Cys; Arg278Cys; IVS15+1G>A)
died from heart failure aged 29, 65, 65 and 68 years. In the pediatric cohort, one patient with the
ated from ventttttttttrirrrrrrrrrrrrrr
ere mmmmmmmmmmmmmmmmmmalalaalalalalalalalalalalalalalalalalesesesesesesesesesesesesesesesseseses oo o oooooo oo oooo ooof f f fff ffff fff f ff f InIInInInInInnInInnInnInInInInInInIInd
y
m o
u i
y wwwwwith thhhhhe e ee ArArArAArg9g9g9g9g92G2G2G2G2Glnlnlnlnln m mm mmututututu atatatatioioiii n. TTheehehee m mm mmaxixixixiximamamamamalllll waaaaallllllll t t tthihhhh ckckckckcknenenenen ssssss
mm, 1515151515mmmmmmmmmm aaandndndndnd 22 2220m0m0m0mmmmmm,m resesessspepepepepectctctctctivivivvveleleele y.yyyy TTTTThehehehehe ttttthihihihihirdrdrdrd ss ssudududududdededededen dededededeatatatatathhh hh o
u1uu1u1636363dedel,l,,, a a agegegeg dd 626262 y y yyyeaeaearsrsrs w w witithh NN NSVSVSVT,T,T, a a a f famamamililii y y y y hihistststororory y y yy ofof mm mulultitti
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

12
Ile79Asn mutation died suddenly aged 16 with no echo features of HCM (maximal wall
thickness was 9 mm); his cousin died from complications during an ICD lead extraction at
another center.
Kaplan-Meier survival curves for the study population are shown in figures 3 A and B. When
modelled from the time of first evaluation at our institution, (including two individuals who
presented with cardiac arrest as a first event), the annual rate of cardiovascular death, transplant
and ICD discharge in probands and relatives with a TNNT2 mutation was 1.6% (0.016
person/year; CI 0.83-2.79%) and the rate of sudden cardiac death 0.93% (0.0093 person/year; CI
0.37-1.92%).
When survival was modelled from birth for definite TNNT2 carriers and additional relatives
identified from pedigree analysis that were known to have HCM or were obligate gene carriers
the annual rate of cardiovascular death, transplant and ICD discharge was 0.64% (0.0064
person/year; CI 0.41-0.96%) and the rate of sudden cardiac death 0.51% (0.0051 person/year; CI
0.31-0.79%).
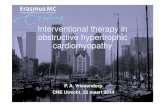
Figure 4 shows survival from birth for individual mutations. Two mutations (Ile79Asn and
Arg92Gln on exon 8 and 9, respectively) appeared to be associated with a higher rate of sudden
death at a juvenile age, at least in comparison with IVS15+1 G>A and Glu163del mutations. The
small number of SCDs (n=7) means that it is very difficult to perform sub-group analyses
(supplemental table 3). However, comparing probands with relatives there was no difference in
cardiac mortality (Kaplan Meier log rank test p=0.62). Similarly, there was no difference in
h 0.93% (0.009399393939999999999
mo r n
g
modededededellllllllllededededed f fffrorororoom mmmm bibibibib rtttthhh hh fofofofofor dededededefififififinininininitetetetee T TTTTNNNNNNNNNNT2T2T2T2T2 cccccararaararriririrriereeee s ssss ananananand dddd adadadadaddidididiititititiionoo
grggrgreeeeee aa anananalylylylyysisisss ththatatat ww wererereee knknknknowowownnn tototo h hhavavaveee HCHCHCM M M ororor ww wererereee obobliligagagatttt
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

13
cardiac mortality in patients with echocardiographic expression of disease versus carriers without
LVH (Kaplan Meier log rank test: p=0.21).
Discussion
This is the largest study of patients with mutations in the TNNT2 gene since the first clinical
report suggesting that this form of hypertrophic cardiomyopathy is characterized by a high
incidence of sudden cardiac death16. The findings confirm that a history of young sudden cardiac
death is common in many families and that mild or absent hypertrophy is present in a minority of
adult mutation carriers.
Disease penetrance
In common with most other reports, this study shows that disease penetrance (defined by
echocardiographic evidence for HCM) is low in children. A substantial minority of adults with
TNNT2 mutations also have normal echoes, although most of these had an abnormal ECG,
emphasizing the role of both tests in clinical screening. In those adults with an abnormal echo,
the distribution and severity of myocardial hypertrophy was very similar to that reported in other
sarcomere protein mutations33. The one major difference with larger studies was a lower
prevalence of LVOTO, which was present in less than 10% of patients. The reasons for this are
not clear from this study, but we cannot exclude the possibility that some individuals had
provocable obstruction.
Survival analyses
A recent meta-analysis of large cohort studies indicates that the rate of sudden death in patients
s e
v
st otototototheheheheher rrrr rererrrepopopopoortrtrttrtss,s ttthihihihihisss ss stststststudududududyyy yy shshshshshowowowowowss sss thththththatatatatat dd dddississseaeaeaeaeasesesesse pepeeepenenenenen trtrtrtrtrananannncecececce ((((dddedd
vvvvididenenencecece f fororor HH HCMCMCM) ) )) isis l lowowow i innn chchilildrdrenenen. AAA sususubsbstatatantntntiaiall miminononorrritity yyy
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

14
fulfilling diagnostic criteria for HCM is less than 1% per annum34. However, prospective data on
outcomes in genotyped patients are scarce and studies rarely consider both probands and
relatives that carry the same mutation.
In the case of TNNT2, we identified five studies that have reported on survival16;18;32;35;36.
Overall, 166 carriers of TNNT2 mutations identified by genetic and pedigree analysis are
reported. Of these, 61 died from an apparent cardiac cause, the majority (n=50) of whom died
suddenly. In two studies, however, the number of sudden deaths was low, in accord with the
prospective data in this report (Table 4).
In this study, while we adopted a conservative approach to the coding of deaths in relatives,
pedigree analysis still demonstrated a high prevalence of sudden cardiac death in affected
families. However, when we examined survival in the prospectively followed cohort, the annual
rate of sudden death was less than 1% and in line with the average seen in large follow-up
studies34. One possible explanation for this apparent paradox is the use of prophylactic ICDs in
patients and relatives deemed to be at high risk, but this seems unlikely given that only a single
patient (out of 23 with a device) had an appropriate ICD therapy for sustained ventricular
arrhythmia during follow-up. Another possibility is the inclusion of relatives with a mild or
absent clinical phenotype, which could have resulted in better outcomes. This study was too
small to conduct adequately powered sub-group analyses, but the annual rate of sudden death
was similar in probands and relatives suggesting that other mechanisms Including genetic,
epigenetic and environmental factors were at least partially responsible for the better outcomes in
individuals with a phenotype.
w i
l n
w o
wwwwweee ee adoptetetteted d d dd a aa cococococonsnsnsnsnsererererervavavavavatitititt vevevevev apapapaa prrooachchchchh t t t tto oooo thththththe e e e cococococodingngngngng o o oooffff dddddeaeaeaeaeaththththths if
ll dededededemomomomomonsnnnn trtrtrtrtratatataatedededede aaaa hhhhhigigigigigh hhhh prrrrrevevevevevalalalalalenenenenencececcec ooooof ffff sususususuddddddddddenenenenen cc cccararararrdididididiacacacacac dd dddeaeaeaeaththththh ii in
wwwwhehennn wewewe ee exaxaxamiminenenedd sususurvrvrvivivivivalal i innn ththeee prprprp ososospepepepp ctctctivivelely y y yy fofollllowowoweded cc cooo
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

15
A number of studies have reported sudden deaths in TNNT2 mutation carriers with little or no
hypertrophy. The same phenomenon was seen in a few patients in this study, but the relative
paucity of events in the prospectively followed cohort means that we can not determine the
relative risk of sudden death in mutation carriers with normal echoes. Similarly, although most
deaths occurred in families with mutations in exons 8 and 9 this study was not powered to detect
differences in outcome between specific mutations.
Comparison with other sarcomere protein gene mutations
A lack of prospective survival data in patients with other sarcomere protein gene mutations
makes direct comparison with this study challenging. A recent study37 evaluating not only
probands, but also asymptomatic relatives carrying MyBPC3 mutations (a total of 235 mutations
carriers) reported an annual rate of sudden cardiac death of only 0.1%. However, approximately
two thirds of the population carried a well recognized Dutch founder mutation, limiting
comparison with our own population in which there was a greater spectrum of genetic
abnormalities including single base substitutions, deletions and splice-donor site mutations.
Disease progression
Progressive myocardial thinning and contractile impairment is a well recognized phenomenon in
HCM5-6. In this study, the rate of disease progression appeared slow in that only three patients
developed ventricular dilatation after more than a decade of follow-up. However, five patients
already had ventricular dilatation at presentation (age 48 to 64 yrs) and four patients died from
ere ppppppppppppppppppppprorooororrororororororororoorororororrootetetettettetetetetteteteteteeteteininininininininininininininininininin g g g g g g g g gg g gg gg g ggg gggggeneneeneneneeeneneneneneenenenee e
r g
s o
risososososon withthththt t t t tthihhhh sssss sss sstututututudydydydydy ccc cchahahahahallllllenenennngig ngng. A A A A A rerererereceeeeentntntn s ss sstututututudyyyyy37 e e eeevavavavaalululululuatatatatatiniiii g
sympmpmpmpmptototototomamammam tititit ccc cc rerererr lalalalal tiiiiivevevvvessss s caaaaarrrrrrrr yiyiyiyiyingngngngng MMMMMyByByByByBPCPCPCPCPC3 3333 mumumumumutatatattatitititiiononononons ssss (a(a(a(a(a tttttotototottalalalalal o
ananannununualal r r ratatateee ofof ss sududdedennn cacacardrdiaiaccc dedeatatath h hh ofof oo onlnlnlly y y yy 000.1%1%1%. HoHoHoweweweveveverrrr
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

16
heart failure during follow-up, suggesting that progression to heart failure may be relatively
common in patients with TNNT2 mutations.
Limitations
The population in this study is inevitably subject to referral and ascertainment bias. The selection
of the population is also different from some previous reports in that we included only patients
with genetic, clinical or pathologic confirmation of the disease, whereas in previous outcome
studies all relatives who died suddenly were presumed affected with disease. This means that the
burden of sudden death caused by TNNT2 mutations may have been underestimated in some
families.
The extreme phenotypic variability observed in this study shows that outcomes in individuals
carrying mutations in TNNT2 is influenced by many factors other than the position and nature of
the mutation itself. Due to financial and other inevitable constraints in a study performed over
two decades, we were unable to exclude the possibility that some patients harbored additional
sarcomere protein gene mutations. However, contemporary genetic studies indicate that this
occurs in only 5% of patients38. While double mutations could account for a high mortality in
individual families, it is unlikely that the presence of additional mutations explains for the
relatively low annual incidence of sudden death observed in the prospective cohort.
Conclusion
Investigation of genotype-phenotype relations in a diverse and complex disorder such as HCM is
challenging. While this study shares many of the limitations of previous studies, it is reasonable
been underestiimmmmmmmmmmmmmmmmm
y i
n i
ypicicicicic v vvvvararararariaiiaiaiabibibib lililillitytytytyty o oooobsssssererererervvevvv d dddd ininininin thththththisisisiss s sssstututuuudydydydydy ss ssshohohohohowswswswsws tt ttthahahahaattt tt ouououououtctccccomomomomomeseseseses i
n nn n TNTNTNNTNTNT222 isis i infnfluluenenencececedd bybybybyy mm mananany y y y fafaaaactctctorororsss otototheherrr ththananan tt thehe popoposisititii
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

17
to conclude the following about TNNT2 mutations: ventricular hypertrophy is uncommon in
children and adolescents; ventricular hypertrophy on echo is absent in an important minority of
adult patients; irrespective of echocardiographic findings, most adult carriers have an abnormal
ECG; sudden cardiac death is an important complication, but at least in this prospectively
managed cohort, its incidence is no greater than in most contemporary cohort studies; and
finally, although rare, sudden cardiac death can occur in individuals with little or no hypertrophy.
Acknowledgements: We are grateful to Dr. Letizia Bacchi Reggiani (biostatistician at
Cardiology Department, S.Orsola-Malpighi Hospital, Bologna) for the assistance with the
statistical analysis. Professor McKenna, Dr Elliott and Dr Syrris acknowledge support from the
UCLH/UCL NIHR Comprehensive Biomedical Research Centre.
Conflict of Interest Disclosures: None
References:
1. Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults: echocardiographic analysis of 4,111 subjects in the CARDIA study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995;92:785–789. 2. Maron BJ, Bonow RO, Cannon RO 3rd, Leon MB, Epstein SE.Hypertrophic cardiomyopathy: interrelations of clinical manifestations, pathophysiology, and therapy. N Engl J Med. 1987;316:780–789. 3. Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO. Sudden death in young competitive athletes: clinical, demographic, and pathological profiles. JAMA. 1996;276:199–204. 4. Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA. 2006;296:1593-1601.
aaaaaaaaaaaaaaaaaackkckckckckckckckckckckckckckckckckcckkkkkknononononononononononononoonoonononononnoowlwlwlwlwllwlwlwlwlwwlwlwlwlwlwlwlwllwlededededededededededededededededededededddedgegegeggegegeggegggeggeggegggg suuuuuuuuuuuuuuuuu
pp
DDDDDisisisisisclossssururuuu esees: NNNonenenenene
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

18
5. Spirito P, Maron BJ, Bonow RO, Epstein SE. Occurrence and significance of progressive left ventricular wall thinning and relative cavity dilatation in hypertrophic cardiomyopathy. Am J Cardiol. 1987;60:123-129.
6. Biagini E, Coccolo F, Ferlito M, Perugini E, Rocchi G, Bacchi-Reggiani L, et al. Dilated-hypokinetic evolution of hypertrophic cardiomyopathy: prevalence, incidence, risk factors, and prognostic implications in pediatric and adult patients. J Am Coll Cardiol. 2005;46:1543-1550. 7. Maron BJ, Moller JH, Seidman CE, Vincent GM, Dietz HC, Moss AJ, et al. Impact of laboratory molecular diagnosis on contemporary diagnostic criteria for genetically transmitted cardiovascular diseases: hypertrophic cardiomyopathy, long-QT syndrome, and Marfan syndrome. [A statement for healthcare professionals from the Councils on Clinical Cardiology, Cardiovascular Disease in the Young, and Basic Science, American Heart Association]. Circulation. 1998;98:1460–1471. 8. Geisterfer-Lowrance AA, Kass S, Tanigawa G, Vosberg HP, McKenna W, Seidman CE, et al. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999–1006. 9. Thierfelder L, Watkins H, MacRae C, Lamas R, McKenna W, Vosberg HP, et al. Alpha-tropomyosin and cardiac troponin T mutations cause familial hypertrophic cardiomyopathy: a disease of the sarcomere. Cell. 1994; 77:701–712. 10. Niimura H, Patton KK, McKenna WJ, Soults J, Maron BJ, Seidman JG, et al. Sarcomere protein gene mutations in hypertrophic cardiomyopathy of the elderly. Circulation. 2002;105:446–451 11. Seidman JG, Seidman CE. The genetic basis for cardiomyopathy: from mutation identification to mechanistic paradigms. Cell. 2001;104:557–567. 12. Watkins H, Rosenzweig A, Hwang DS, Levi T, McKenna W, Seidman CE, et al. Characteristics and prognostic implications of ß-myosin missense mutations in familial hypertrophic cardiomyopathy. N Engl J Med. 1992;326:1108–1114. 13. Charron P, Dubourg O, Desnos M, Bennaceur M, Carrier L, Camproux AC, et al. Clinical features and prognostic implications of familial hypertrophic cardiomyopathy related to the cardiac myosin-binding protein C gene. Circulation. 1998;97:2230–2236. 14. Van Driest SL, Ackerman MJ, Ommen SR, Shakur R, Will ML, Nishimura RA, et al. Prevalence and severity of “benign” mutations in the beta-myosin heavy chain, cardiac troponin T, and alpha-tropomyosin genes in hypertrophic cardiomyopathy. Circulation. 2002;106:3085–3090. 15. Sorajja P, Elliott PM, McKenna WJ. The molecular genetics of hypertrophic cardiomyopathy: prognostic implications. Europace. 2000;2:4-14.
eta cardiac myyyyyyyyyyyyyyyyyoooooooooooo
tkins H MacRae C, Lamas R McKenna W Vosberg HP, etd o
m
o lo
tkinninnns s s ss H,H,H,HH, M MM M Macaaaa Rae C, Lamas R, , , McMMMM Kenna W,W,W,W,W, V osberg HP, etddddiaiaiaiaiac troppppponononnoninininn T TT TT m m m mmutututututatatatatatioioioioionsnnnn cccccauaa sese famamamamamilililililiaaaaall lll hyhyhyhyypepppp rtttttrororororophphphphphicciccic ccc ccararararardidddd o
meeeeerrrer . Cell. 1994944; 77777777:7010 –––712112.
on KK, McKeKeKeKeKennnnnnnnnna a a a a WJWJWJWJWJ,, , , SoSoSoSoSoululululultststststs J,J,JJ MMMMMaraaaa ononononon BB BB BJ,J,JJ,J SSSSSeieieiidmdmdmdmdmaaanaa JG, et alnsnsns i innn hyhyyyypepepepp rtrtrtrororophphpp icic cc cararardidiiiomomomyoyoyoyy papapapp ththhy y y y ofof tt theheee e e eldlderererlylyyyy. CiCiCircrcrcululatatatioiooio
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

19
16. Watkins H, McKenna WJ, Thierfelder L, Suk HJ, Anan R, O’Donoghue A, et al. Mutations in the genes for cardiac troponin T and -tropomyosin in hypertrophic cardiomyopathy. N Engl JMed. 1995;332:1058–1064. 17. Ackerman MJ, Van Driest SL, Ommen SR, Will ML, Nishimura A, Tajik J, et al. Prevalence and age-dependence of malignant mutations in the betamyosin heavy chain and troponin T genes in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;39:2042–2048.
18. Moolman JC, Corfield VA, Posen B, Ngumbela K, Seidman C, Brink PA, et al. Sudden death due to troponin T mutations. J Am Coll Cardiol. 1997;29:549–555. 19. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778–1785 20. Varnava A, Baboonian C, Davison F, de Cruz L, Elliott PM, Davies MJ, et al. A new mutation of thecardiac troponin T gene causing familial hypertrophic cardiomyopathy without left ventricular hypertrophy. Heart. 1999;82:621–624. 21: Monserrat L, Elliott PM, Gimeno JR, Sharma S, Penas-Lado M, McKenna WJ. Non-sustained ventricular tachycardia in hypertrophic cardiomyopathy: an independent marker of sudden death risk in young patients. J Am Coll Cardiol. 2003;42:873-879. 22. Romhilt DW, Estes Jr EH. A point-score system for the ECG diagnosis of left ventricular hypertrophy. Am Heart J. 1968;75:752-758. 23. Rijnbeek PR, Witsenburg M, Schrama E, Hess J, Kors JA. New normal limits for the paediatric electrocardiogram. Eur Heart J. 2001;22:702-711. 24. Maron BJ, Spirito P, Wesley YE, Arce J. Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med. 1986;315:610–614. 25. Shapiro LM, McKenna WJ. Distribution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a two-dimensional echocardiographic study. J Am Coll Cardiol. 1983;2:437–444. 26. McKenna WJ, Spirito P, Desnos M, Dubourg O, Komajda M. Experience from clinical genetics in hypertrophic cardiomyopathy: proposal for new diagnostic criteria in adult members of affected families. Heart. 1997;77:130–132. 27. Sadoul N, Prasad K, Elliott PM, Bannerjee S, Frenneaux MP, McKenna WJ. Prospective prognostic assessment of blood pressure response during exercise in patients with hypertrophic cardiomyopathy. Circulation. 1997;96:2987–2991. 28. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, et al. Task Force on Clinical Expert Consensus Documents. American College of Cardiology;
phic cardiomyoyoyoyoyoyooyyoyoyyyoyyyyy
iott PM Gimeno JR, Sharma S, Penas-Lado M, McKenna Wr
t fa
iotttttt P P P PPM,M,M,MM, G G GGimimimimimeno JR, Sharma SSSSS, Penas-Ladooooo MM MM M, McKenna Wr tatatatataccchcc ycarararara dididididia aaa innininin hh h h hypypypypypererererertrtrtrtrtropopopopo hihihiiic c c c caarrdioioooomymymymymyopopopopopatattathyhyhyhyhy: aaaaan n n nn ininininindeedededepepepepependndndndndeyyyyyouououo ng patieiientts. J AmAAAA CCColololl CaCCarddiolllll. . . 20202022 033;4222:8787877333-33 877777999.99
tes Jr EH. AAAAA ppp ppoioioioiointntntntnt-ss-s-sscococococorerererere s s sssysysysysystetetetemmmmm f ff ffororororo ttttthehehehehe EEEE ECGCGCGCGCG ddddiaiaiaiaiagngggg osis of lefmmmaaaartrtrt JJ J. 191919686868;7;7;75:5:5:757575222-757575888. JJJJ
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

20
Committee for Practice Guidelines. European Society of Cardiology. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687-1713. 29. Mogensen J, Bahl A, Kubo T, Elanko N, Taylor R, McKenna WJ. Comparison of fluorescent SSCP and denaturing HPLC analysis with direct sequencing for mutation screening in hypertrophic cardiomyopathy. J Med Genet. 2003;40:e59. 30. Mogensen J, Murphy RT, Shaw T, Bahl A, Redwood C, Watkins H, et al. Severe disease expression of cardiac troponin C and T mutations in patients with idiopathic dilated cardiomyopathy. J Am Coll Cardiol. 2004;44:2033-2040. 31. Forissier JF, Carrier L, Farza H, Bonne G, Bercovici J, Richard P, et al. Codon 102 of the cardiac troponin T gene is a putative hot spot for mutations in familial hypertrophic cardiomyopathy. Circulation. 1996;94:3069-3073. 32. Nakajima-Taniguchi C, Matsui H, Fujio Y, Nagata S, Kishimoto T, Yamauchi-Takihara K. Novel missense mutation in cardiac troponin T gene found in Japanese patient with hypertrophic cardiomyopathy. J Mol Cell Cardiol. 1997;29:839-843. 33. Van Driest SL, Ommen SR, Tajik AJ, Gersh BJ, Ackerman MJ. Yield of genetic testing in hypertrophic cardiomyopathy. Mayo Clin Proc. 2005;80:739-744. 34. Elliott PM, Gimeno JR, Thaman R, Shah J, Ward D, Dickie S, et al. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart. 2006;92:785-791. 35. Anan R, Shono H, Kisanuki A, Arima S, Nakao S, Tanaka H. Patients with familial hypertrophic cardiomyopathy caused by a Phe110Ile missense mutation in the cardiac troponin T gene have variable cardiac morphologies and a favorable prognosis. Circulation. 1998;98:391-397. 36. Torricelli F, Girolami F, Olivotto I, Passerini I, Frusconi S, Vargiu D, et al. Prevalence and clinical profile of troponin T mutations among patients with hypertrophic cardiomyopathy in tuscany. Am J Cardiol. 2003;92:1358-1362. 37. Christiaans I, Birnie E, van Langen IM, van Spaendonck-Zwarts KY, van Tintelen JP, van den Berg MP, et al. The yield of risk stratification for sudden cardiac death in hypertrophic cardiomyopathy myosin-binding protein C gene mutation carriers: focus on predictive screening. Eur Heart J. 2010;31:842-848. 38. Richard P, Charron P, Carrier L, Ledeuil C, Cheav T, Pichereau C, et al. EUROGENE Heart Failure Project. Hypertrophic cardiomyopathy: distribution of disease genes, spectrum of mutations, and implications for a molecular diagnosis strategy. Circulation. 2003;107:2227-2232.
moto T,T,T,T,T,T,T,T,T,T,T,T,T,T,,T,T,T,T,T, Y Y YYY Y Y Y YY YY Y Y Y YY Y Yamamamamamamamamammamamammamamamamamamauauauauauauauauauauauauaauaaauauaauauuauchation in cardiac troponin T gene found in Japanese patient w
M
O nm
eno JR Thaman R Shah J Ward D Dickie S et al Historic
atiooooon n n n n inininnn c cc ccarrrrrdidddd ac troponin T genenenenene found in Japapapapapanese patient wMoMoMoMoMol lll l Cell CCCCCararararardididiidiololololol. 1999999797979797;2;2;2;229:99 8388388 9-843.3.3.3.
Ommmmmmmmmmenenenenen SSSSSR,RRR T TTTTajajajaja ikikikiki AAAAAJ,JJJJ GGGGGererererershshshshsh B BBBBJJJJJ, AcAcAcAcAckekekekekermrmrmrmrmananananan MMMMMJ.JJJ Y YYYYieieieieieldldldldld ooooof fff gegegegegenmyopathy. MaMaMaMaMayoyoyoyoyo C C CCClililililin n n nn PrPrPrPrProcococococ. . 202020202 050505055;888880::::73737373739-9-9-9-9-74747474744.4.4.4
eenono JJRR TTTThahhah mamann RRRR SSShahhah hhhh JJJJ WWWWarardddd DDDD DDDDDicicii kikikiiee SSSS eett alall HiHHiH ststororiccic
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

21
Table 1: Baseline clinical characteristics in adults and children with TNNT2 mutations Adults 16 years p value n 71 21 Male 36 (51%) 15 (71%) 0.44 Age (yrs) 37 ± 14 9 ± 5 na NYHA I-II (assessed in 62 adults and 18 children)
59 (95%) 18 (100%) 0.9
Chest Pain 18 (29%) 0 (0%) 0.06 Palpitations 10 (17%) 0 (0%) 0.21 Obstruction 6 (9%) 0 (0%) 0.48 ECG available 68 19 PR msec 157 ± 30 123 ± 15 0.001 QRS msec 95 ± 21 89 ± 11 0.3 QTc msec 427 ± 29 412 ± 23 0.23 QRS axis deviation 10 (15%) 2 (10%) 0.86 LVH 35 (51%) 4 (21%) 0.76 Q wave 25 (37%) 3 (16%) 0.07 Repolarization abnormalities 42 (61%) 4 (21%) 0.91 LBBB 1 (1%) 0 (0%) na RBBB 4 (6%) 0 (0%) na LAH 4 (6%) 0 (0%) na Normal ECG 13 (19%) * 13 (68%) 0.01 Key: LVH: left ventricular hypertrophy; LBBB: Left Bundle Branch Block; RBBB: Right Bundle Branch Block; LAH: Left Anterior Hemiblock; na: not applicable. Yates correction was employed when appropriate. *related to 68 available ECGs
Table 2: Echocardiographic characteristics at baseline in all adult carriers of a TNNT2 mutation compared to those observed in adults with a mutation and an abnormal echocardiogram. All Adults TNNT2+ Adults with abnormal echo N 68 52 Male 35 (51%) 27 (52%) Age yrs 38 ± 15 37 ± 15 LVEDd mm 45 ± 6 45 ± 6 LVESd mm 28 ± 6 28 ± 6 LVMWT mm 17 ± 6 19 ± 5 FS% 38 ± 8 37 ± 8 LA mm 41 ± 10 42 ± 9 ASH 37 (54%) 37 (71%) Concentric Hypertrophy 12 (18%) 12 (23%) Apical Hypertrophy 3 (4%) 3 (6%) Left ventricular dilatation and/or low FS* 5 (7%) 5 (10%) Biventricular Hypertrophy 3 (4%) 3 (6%) Normal Echo 16 (24%) --- Key: Echo+: phenotypic expression of disease on Echocardiography; LVEDd: left ventricular end diastolic diameter; LVESd: left ventricular end systolic diameter; LVMWT: maximal left ventricular wall thickness: FS: fractional shortening; LA: left atrium diameter on M-Mode; ASH: asymmetrical septal hypertrophy *end-diastolic cavity dimension measured by M-mode echocardiography exceeding the reference upper 95% confidence interval (CI) for body surface area or a FS 25%
4444444444444444444 ( ( ((((( ( ( ( ( ( ( ( (((( (((212121212121212122112122121211%)%)%)%)%)%)%)%)%)%%%%%)%)%)%%%%) 0 00000000000000000000 (0(0(0(0(0(0(0(0(0(0(0(0(0(00(0(0(0(0(((00%)%)%)%)%%)%)%)%)%)%)%)%)%)%)%)%%)%)%)%))%%) 000000000000000000000000 (0(0((0(0(0(0(0(0(0(0(0(0(0(0(0(00(0(0((0%)%)%)%)%)%)%)%)%)%%)%)%)%)%)%)%)%)%)%)%%%))%)
u Berior n app ca orre was em oy e
44 44 ((6%) 0 (0%) 1313 (1919191919%)%)%)%)%) ***** 11 113 33 33 (6(6(6(6(68%8%8%%8%)) )))
ulululllararararar h ypererererertropopophyyy;;; LBBBBBBBBBBB : : : :: LeLeLeeL ft BBBBBuundldle BrBBBB anananchhh BBBloloocck; RRRBRR BBBBBBBBB: RRRighghghgg t Berior HHHHHemiblblblococococo k;kkk na:::: n nnn tttott applilillicablblblbb e.e.e Y YYatttttessss c cc correcttioioion nnn was em llploy dedd e ECGs
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

22
Table 3: Prevalence of risk factors for sudden cardiac death in adults and children with TNNT2 mutations. Risk profile Adults 16 years Complete stratification (5 RF) 54 10 Number of risk factors 1.9 ± 0.9 1.6 ± 0.8 Number of patients with 2 RF 35 (65%) 6 (60%) Family History SD age 40yrs 45 (83%) 9 (90%) Multiple SD in the family 35 (65%) 8 (80%) SD in 1st degree relative 27 (50%) 4 (40%) NSVT 13 (24%) 0 - recorded in first ECG Holter 8 (61%) 0 - recorded in subsequent ECG Holter 5 (39%) 0 Maximal wall thickness 30 mm 3 (5%) 0 Syncope 17 (31%) 3 (30%) Abnormal blood pressure response 26 (48%) 4 (40%) Key: SD: sudden cardiac death; RF: risk factors; NSVT: non sustained ventricular tachycardia.
Table 4: Studies reporting on survival of TNNT2 mutations Study No of
Patients No of Cardiac Deaths
No of Sudden Deaths
No of Families
Mutation
Watkins H, et al. 199516 112 50 39 11 Ile79Asn Arg92Gln Phe110Ile �Glu160 Glu163Lys Glu244Asp Intron 15 G�A Arg278Cys
Nakajima-Taniguchi C, et al. 199732
4 2 2 1 Ala104Val
Moolman JC, et al. 199718 22 7 7 2 Arg92Trp Anan R, et al 199835 18 2 2 6 Phe110Ile Torricelli F, et al 200336 10 0 0 5 Phe110Leu
Arg130Cys Glu160del Arg92Gln Arg278Cys
Total 166 61 50 25
Figure Legends:
Figure 1: Relation between ECG and echocardiographic findings in adult patients with TNNT2
mutations. Echo+: phenotypic expression of disease on Echo; ECG+: phenotypic expression of
orti rviv l f TNNT2 t ti
5
NNNNNo o f f ff fPaaattiennttts
NNNNNo oo ooof f f f fCaCardiaiiac DeDeDeDeDeatatatatathshshshshs
NNNNNo ooooof f f fSuSuSuSS dddden DeDeDeDeDeatatattthshshshshs
ortititititingngngngng o o o o on nnnn sususususurvival of TNNT2 m m mmmutations NNNNNo o oof f f ff Faaammimm llies
516 1122222 5 5 5 550 0000 3939393939 1 1 11 11
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

23
disease on ECG; Echo-: no phenotypic expression of disease on Echo; ECG-: no phenotypic
expression of disease on ECG.
Figure 2: Prevalence of normal echocardiogram at different ages.
Figure 3: Kaplan Meier survival curves for survival from birth (A) and from first evaluation (B).
The cohort evaluated from birth includes 12 cases of SD identified from pedigrees (obligate
mutation carriers, post-mortem evidence for HCM and known HCM prior to death).
Figure 4: Kaplan Meier survival curves showing survival from cardiovascular death and sudden
cardiac death from diagnosis and from birth for individual mutations. The cohort evaluated from
birth includes 12 cases of SD identified from pedigrees (obligate mutation carriers, post-mortem
evidence for HCM and known HCM prior to death).
cardioiioioioioiooioooioioioioooovavavvavaavavavavavavavvvavavavavavavav scscscsccssscscsccscscsscscscsccs ulululululuulululluululluuluululullararararararararararararaaraaarararar d
t
e
n
iaaaaagggngg osisss a a aandndnndn fffffrororororom mmmm bibbibib rtrtrtrtrth h h hh fofofor rrr iindn ivviddddduauauauaual lll l mumumumum tatatataatititititionooo s.s.s.s.s. TT TT Theheheheh cocococoohohohohohort
es ofofofofof SSSSSD DDDD idididdenenenenentitititit fifififif eddddd ff fffrororororom mmmm pepepepepedididididigrgrgrgrgreeeeeeee sss ss (o(o(o(o(oblblblblbligigigiggatatatatate eeee mumumumumutatatatatatititititiononnonon cccccararararrririririieee
ndnnd k knononownwnwn HH HCMCMCM p p pppririororor tt to o o dedeatatath)h)))).
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

1,0
0,8
0,6
0,4
0,2
0,0
0 5 10 15 20 25 years
Arg92Gln
Arg92Trp
Glu163del
Ile79Asn
IVS15+1G>A
Other mutationsCu
mul
ativ
e su
rviv
al
Follow up
SD
1,0
0,8
0,6
0,4
0,2
0,0
0 5 10 15 20 25 years
Arg92Gln
Arg92Trp
Glu163del
Ile79Asn
IVS15+1G>A
Other mutations
Cum
ulat
ive
surv
ival
Follow up
CV death
1,0
0,8
0,6
0,4
0,2
0,0
0 10 20 30 40 50 60 70 80 years
Arg92Gln
Arg92Trp
Glu163del
Ile79Asn
IVS15+1G>A
Other mutations
Cum
ulat
ive
surv
ival
Age
SD
1,0
0,8
0,6
0,4
0,2
0,0
0 10 20 30 40 50 60 70 80 years
Arg92Gln
Arg92Trp
Glu163del
Ile79Asn
IVS15+1G>A
Other mutations
Cum
ulat
ive
surv
ival
Age
CV death
10101010101010000011111111 20222222220 10 20ears 0 10 20ears
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

Perry ElliottFerdinando Pasquale, Petros Syrris, Juan Pablo Kaski, Jens Mogensen, William J. McKenna and
Troponin T GeneLong-Term Outcomes in Hypertrophic Cardiomyopathy Caused by Mutations in the Cardiac
Print ISSN: 1942-325X. Online ISSN: 1942-3268 Copyright © 2011 American Heart Association, Inc. All rights reserved.
TX 75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas,Circulation: Cardiovascular Genetics
published online December 5, 2011;Circ Cardiovasc Genet.
http://circgenetics.ahajournals.org/content/early/2011/12/05/CIRCGENETICS.111.959973World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circgenetics.ahajournals.org/content/suppl/2011/12/05/CIRCGENETICS.111.959973.DC1Data Supplement (unedited) at:
http://circgenetics.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Genetics Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information aboutnot the Editorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center,Circulation: Cardiovascular Genetics Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 12, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

SUPPLEMENTALMATERIAL
SupplementalTable1:Numberofcontrolstestedformutationsinpreviousstudies
Mutation Reference Controls
(normalchromosomes)
ThierfelderLetal.Alpha‐tropomyosinandcardiactroponinTmutations
causefamilialhypertrophiccardiomyopathy:adiseaseofthesarcomere.
Cell1994;77(5):701‐12.
200
WatkinsHetal.MutationsinthegenesforcardiactroponinTandalpha‐
tropomyosininhypertrophiccardiomyopathy.NEnglJMed
1995;332(16):1058‐64.
200
Ile79Asn
VarnavaAMetal.Hypertrophiccardiomyopathy:histopathological
featuresofsuddendeathincardiactroponinTdisease.Circulation.
2001;104(12):1380‐4.
180
Glu83Lys MogensenJetal.ComparisonoffluorescentSSCPanddenaturingHPLC
analysiswithdirectsequencingformutationscreeninginhypertrophic
cardiomyopathy.JMedGenet2003;40:e59
na
Varnava AM et al. Hypertrophic cardiomyopathy: histopathological
features of sudden death in cardiac troponin T disease. Circulation.
2001;104(12):1380‐4.(180normalchromosomes)
180Arg92Leu
RichardPetal.Hypertrophiccardiomyopathy:distributionofdisease
genes,spectrumofmutations,andimplicationsforamoleculardiagnosis
strategy.Circulation2003;107(17):2227‐32.
200
Moolman‐SmookJCetal.SuddendeathduetotroponinTmutations.J
AmCollCardiol1997;29(3):549‐55.
200Arg92Trp
VanDriestSLetal.Prevalenceandspectrumofthinfilamentmutationsin
anoutpatientreferralpopulationwithhypertrophiccardiomyopathy.
Circulation2003;108(4):445‐51.
400
ThierfelderLetal.Alpha‐tropomyosinandcardiactroponinTmutations
causefamilialhypertrophiccardiomyopathy:adiseaseofthesarcomere.
Cell1994;77(5):701‐12.
200
WatkinsHetal.MutationsinthegenesforcardiactroponinTandalpha‐
tropomyosininhypertrophiccardiomyopathy.NEnglJMed
1995;332(16):1058‐64.
200
Arg92Gln
VanDriestSLetal.MyosinbindingproteinCmutationsandcompound
heterozygosityinhypertrophiccardiomyopathy.JAmCollCardiol
400

2
2004;44(9):1903‐10.
VarnavaAMetal.AnewmutationofthecardiactroponinTgenecausing
familialhypertrophiccardiomyopathywithoutleftventricular
hypertrophy.Heart1999;82(5):621‐4.
200Arg94Leu
VarnavaAMetal.Hypertrophiccardiomyopathy:histopathological
featuresofsuddendeathincardiactroponinTdisease.Circulation.
2001;104(12):1380‐4.
180
Ala104Val Nakajima‐TaniguchiCetal.Novelmissensemutationincardiactroponin
TgenefoundinJapanesepatientwithhypertrophiccardiomyopathy.J
MolCellCardiol1997;29(2):839‐43.
>50
Glu163Lys WatkinsHetal.MutationsinthegenesforcardiactroponinTandalpha‐
tropomyosininhypertrophiccardiomyopathy.NEnglJMed
1995;332(16):1058‐64.
200
WatkinsHetal.MutationsinthegenesforcardiactroponinTandalpha‐
tropomyosininhypertrophiccardiomyopathy.NEnglJMed
1995;332(16):1058‐64.
200Glu163del
RichardPetal.Hypertrophiccardiomyopathy:distributionofdisease
genes,spectrumofmutations,andimplicationsforamoleculardiagnosis
strategy.Circulation2003;107(17):2227‐32.
200
IVS15+1G>A ThierfelderLetal.Alpha‐tropomyosinandcardiactroponinTmutations
causefamilialhypertrophiccardiomyopathy:adiseaseofthesarcomere.
Cell1994;77(5):701‐12.
200
WatkinsHetal.MutationsinthegenesforcardiactroponinTandalpha‐
tropomyosininhypertrophiccardiomyopathy.NEnglJMed
1995;332(16):1058‐64.
200
VanDriestSLetal.Prevalenceandspectrumofthinfilamentmutationsin
anoutpatientreferralpopulationwithhypertrophiccardiomyopathy.
Circulation2003;108(4):445‐51.
400
Garcia‐CastroMetal.Hypertrophiccardiomyopathy:lowfrequencyof
mutationsinthebeta‐myosinheavychain(MYH7)andcardiactroponinT
(TNNT2)genesamongSpanishpatients.ClinChem2003;49(8):1279‐85.
400
Arg278Cys
InglesJetal.Compoundanddoublemutationsinpatientswith
hypertrophiccardiomyopathy:implicationsforgenetictestingand
counselling.JMedGenet.2005;42(10):e59.
300

3
Supplemental Table 2: The following is a summary of the bioinformatics analysis of themissensemutations(i.e.9knownand1novel).Thisisprovidedasasupplementaldatafile.Sequencevariant PolyPhen‐2prediction SIFTprediction
Ile79Asn Probablydamaging NottoleratedGlu83Lys Probablydamaging NottoleratedArg92Leu Probablydamaging NottoleratedArg92Trp Probablydamaging NottoleratedArg92Gln Probablydamaging NottoleratedArg94Leu Probablydamaging NottoleratedAla104Val Benign NottoleratedGlu163Lys Probablydamaging ToleratedArg278Cys Probablydamaging ToleratedArg278His(novel)
Probablydamaging Tolerated
Supplemental Table3: numberof carriers for eachmutationgroup starting the followupfromdateofbirth.
Mutation Carriers Events FUP yrs Rate SD CI 95% Arg92Gln 6 3 242.9 0.21 0.04-0.06 Ile79Asn 6 1 166.8 0.1 0.00-0.56 Arg92Trp 13 2 361 0.04 0.01-0.15 Glu163del 27 6 1098.5 0.02 0.01-0.04 IVS15+1G->A 20 1 843.2 0.01 0.00-0.03 Other mutations 27 6 1019.4 0.02 0.01-0.05 Commentary: Ever since the first gene for hypertrophic cardiomyopathy was identified in the late 1980s, investigators have sought to link genotypes with clinical phenotypes. One of the best known putative associations is that between mutations in the troponin T gene (TNNT2) and a high risk of sudden cardiac death. In this study we present the first large-scale longitudinal cohort study in patients and genotyped relatives with TNNT2 mutations. Themostimportantfindingisthat,despiteahighprevalenceofhistoricdeathsinfamilies,theincidenceofsuddendeathinthisprospectivelymanagedcohortwassimilartothatobservedinothersarcomereproteingenemutations.Wealsodemonstratethatventricularhypertrophyisuncommoninchildrenandadolescentsandthatventricularhypertrophyisabsentinanimportantminorityofadultpatients.Together,thesefindingshavemajorimplicationsforclinicalandgeneticscreeningoffamilieswithTNNT2mutations.
![GENETIC BASIS OF HYPERTROPHIC CARDIOMYOPATHYThroughout the years, names such as idiopathic hypertrophic subaortic stenosis[5], muscular subaortic stenosis[6] and hypertrophic obstructive](https://static.fdocuments.net/doc/165x107/60571329c95e4748070a14f6/genetic-basis-of-hypertrophic-cardiomyopathy-throughout-the-years-names-such-as.jpg)