
Locked plate fixation - olc-cuhk.org · Biologic fixation-- plate bridges the fracture site and...
67
Locked plate fixation Locked plate fixation – – Principle and applications Principle and applications Dr. Edmund Wong Dr. Edmund Wong 16th CUHK 16th CUHK - - AADO AADO Comprehensive Comprehensive Bioskill Bioskill Course on Fracture Fixation Course on Fracture Fixation April 14 April 14 - - 16, 2007 16, 2007
Transcript of Locked plate fixation - olc-cuhk.org · Biologic fixation-- plate bridges the fracture site and...

Locked plate fixation Locked plate fixation ––Principle and applicationsPrinciple and applications
Dr. Edmund WongDr. Edmund Wong16th CUHK16th CUHK--AADOAADO
Comprehensive Comprehensive BioskillBioskill Course on Fracture FixationCourse on Fracture FixationApril 14April 14--16, 200716, 2007

StabilityStabilityStability of fixation is crucial for both Stability of fixation is crucial for both anatomical and biological fixationanatomical and biological fixation
Stability affords early motion to maintain Stability affords early motion to maintain articular surfaces and soft tissuesarticular surfaces and soft tissues

Absolute StabilityAbsolute StabilityStrain at fracture site Strain at fracture site must be less than 2% must be less than 2% for lamellar bone, 10% for lamellar bone, 10% for woven bonefor woven bone
Example compression Example compression platingplating
Lead to primary bone Lead to primary bone healinghealing

Relative StabilityRelative StabilityBased on controlled motionBased on controlled motion
More physiological; leads to More physiological; leads to callus formationcallus formation
Example buttress plating, Example buttress plating, IM nailingIM nailing
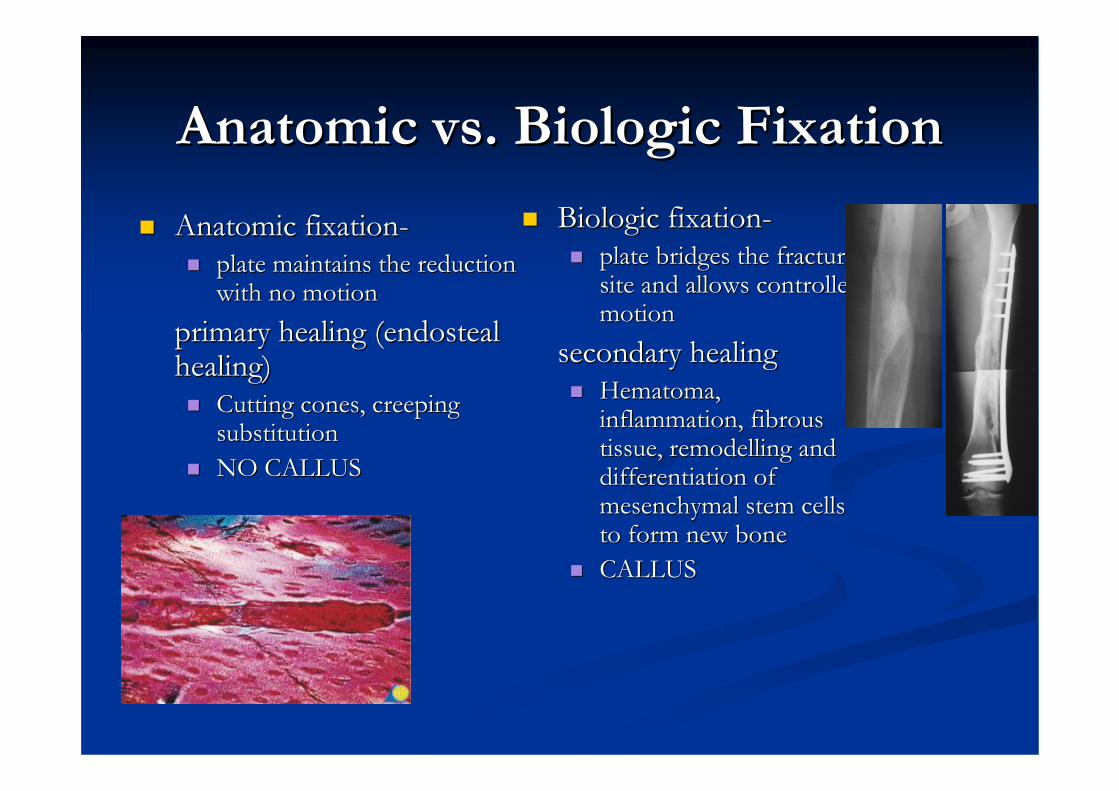
Anatomic vs. Biologic FixationAnatomic vs. Biologic Fixation
Anatomic fixationAnatomic fixation--plate maintains the reduction plate maintains the reduction with no motionwith no motion
primary healing (primary healing (endostealendostealhealing)healing)
Cutting cones, creeping Cutting cones, creeping substitution substitution NO CALLUSNO CALLUS
Biologic fixationBiologic fixation--plate bridges the fracture plate bridges the fracture site and allows controlled site and allows controlled motionmotion
secondary healingsecondary healingHematomaHematoma, , inflammation, fibrous inflammation, fibrous tissue, tissue, remodellingremodelling and and differentiation of differentiation of mesenchymalmesenchymal stem cells stem cells to form new boneto form new boneCALLUSCALLUS

Achieving Stability: Overcoming the Achieving Stability: Overcoming the Forces at the Plate Bone InterfaceForces at the Plate Bone Interface
Axial stress (tension and compression)Axial stress (tension and compression)Shear stress at plate bone interfaceShear stress at plate bone interface
1. Axial Load
2. Bending Load
3. Torsion

Stability by plate bone frictionConventional Plate BiomechanicsConventional Plate Biomechanics

Stability by plate bone friction

Periosteal NecrosisPeriosteal Necrosis
Plate/bone interface Plate/bone interface creates creates ““compartmentcompartment””under the plateunder the platePeriostealPeriosteal necrosisnecrosisLCLC--DCP plates only DCP plates only reduce contact by 50%reduce contact by 50%
Remember that Remember that plate/bone interface plate/bone interface crucial for stabilitycrucial for stability

Conventional PlateConventional Plate
2.Movement of plate during axial loading
4.Causes screw to rotate About axis in distal cortex
3. Leading to high stress and bone resorption
Axial Load
1.Screw bending

Conventional PlateConventional Plate
Bending Load
Force applied: screw orients to force. Asthis occurs strength of fixation equals thread pullout strength of single screw at the distal or proximal end of the plate.
Force Axial
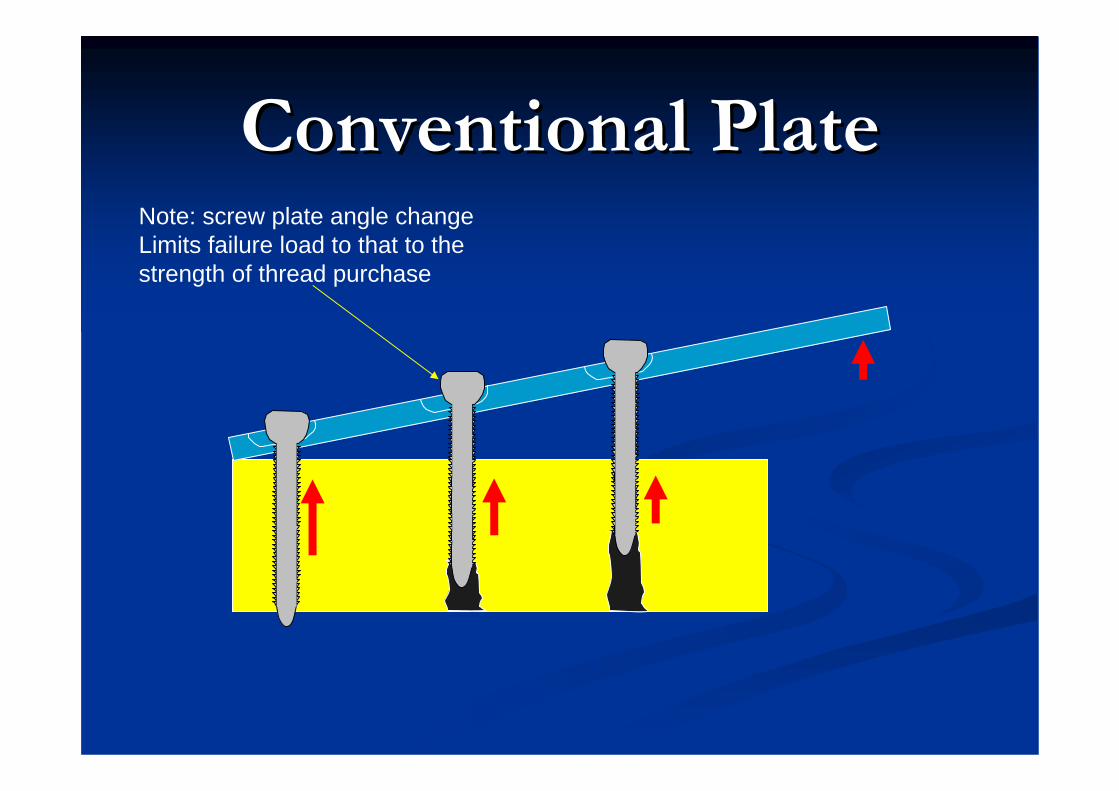
Conventional PlateConventional PlateNote: screw plate angle change Limits failure load to that to the strength of thread purchase


Limitations of Conventional PlatesLimitations of Conventional Plates
Failure in osteopenic boneFailure in osteopenic boneGeriatricsGeriatrics
PeriostealPeriosteal avascularityavascularityTissue necrosis under plateTissue necrosis under plate
Percutaneous platingPercutaneous platingPlate elevated off of the bone. No friction between Plate elevated off of the bone. No friction between plate and boneplate and bone

Locking plate - Internal Fixator
Locking head screw
Threaded plate hole

Internal Fixator

Internal Fixator

Internal Fixator

Internal Fixator
Porotic bone
Theoretical AdvantagesTheoretical AdvantagesNo focal necrosis of bone and soft tissue deep No focal necrosis of bone and soft tissue deep to plateto plate…… improved local resistance to infectionimproved local resistance to infection
Avoids early temporary bone losses under plate Avoids early temporary bone losses under plate induced by vascular damageinduced by vascular damage
Strength of fixation equals the sum of all the Strength of fixation equals the sum of all the bolts (screws) ability to resist shear at the boltbolts (screws) ability to resist shear at the bolt--bone interface. Not that of a single screwbone interface. Not that of a single screw’’s s thread purchasethread purchase
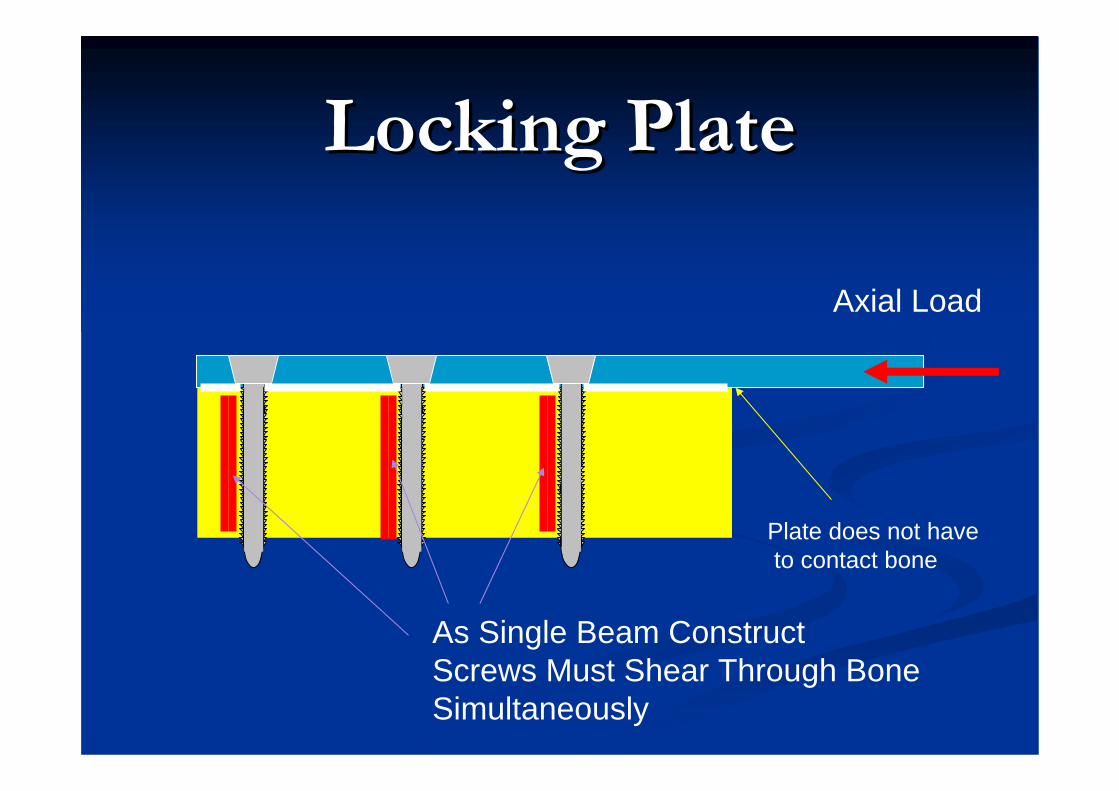
Locking PlateLocking Plate
Plate does not haveto contact bone
Axial Load
As Single Beam ConstructScrews Must Shear Through Bone Simultaneously

Locking PlateLocking Plate

Locking PlateLocking Plate
Fixation fails when bolts overcome bone’s resistanceto shear forces. All bolts must fail as a single construct.
Bolt plate interface allows no motion


Screws with angular stability in different directions


Locking plate = internal, external Fixator
Long
Tub
e
Long
Pla
te
Spac
eSp
ace
Spac
eSp
ace

Biomechanical principlessimilar to those of external fixators
Stress distribution

Biomechanical principlessimilar to those of external fixators
Stress concentration

Advantages of int. Fixators
1. Angular Stability of Screws 2. No accurate Plate Contouring
required3.Less Damage to Periosteum4.Less Screw Loosening

1. Angular Stability of Screws
LIFLC-DCP

2. No accurate Plate Contouring required
LIFLC-DCP

3. Less Damage to Periosteum
LIF
LC-DCP

4. Less Screw Loosening
LIFLC-DCP

ApplicationApplication
LCP LCP Locking Compression PlateLocking Compression Plate

Compression Plate and Compression Plate and FixatorFixator

LCP Locking Compression Plate

= DCP + Limited Contact + Locking Holes + = DCP + Limited Contact + Locking Holes + TitaniumTitanium
Some designed for specific sites.Some designed for specific sites.
LCPLCPLocking Compression PlateLocking Compression Plate

LCPLCPLocking Compression PlateLocking Compression Plate
Both a Both a ““plateplate”” and an and an ““internal internal fixatorfixator””Incorporating features of LCIncorporating features of LC--DCP (Limited DCP (Limited Contact DCP)Contact DCP)Used in MIPO, semiUsed in MIPO, semi--open or open fixationsopen or open fixationsUses nonUses non--locking and/or locking head screws locking and/or locking head screws (LHS)(LHS)No external No external ““targettingtargetting”” devicedevice

Locking Screws
Self Taping & Self Drilling
Self Taping

Metaphysealplate

Pre-op planning
• XR
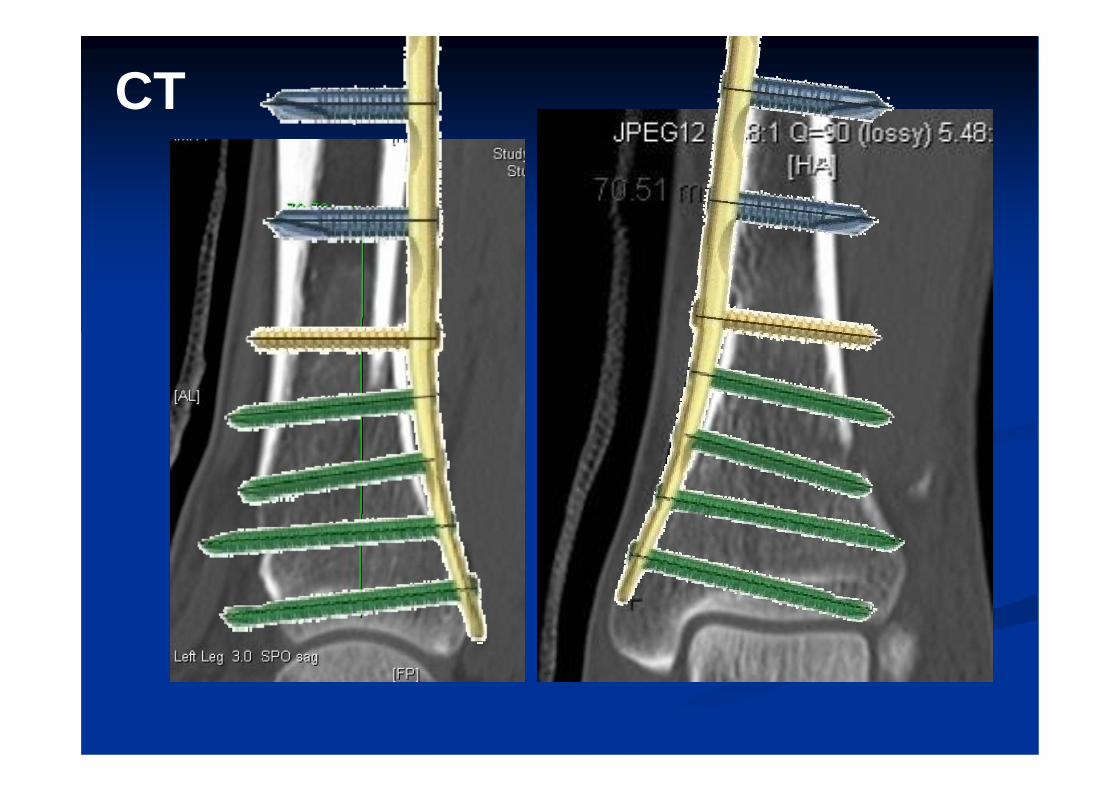
CT

ReductionReduction
TractionTractionExternal fixationExternal fixation

PrePre--contour of platecontour of plate

Insertion of plateInsertion of plate



Place another plate on the surface of skin can guide your percutaneous skin incision for the locking screws.

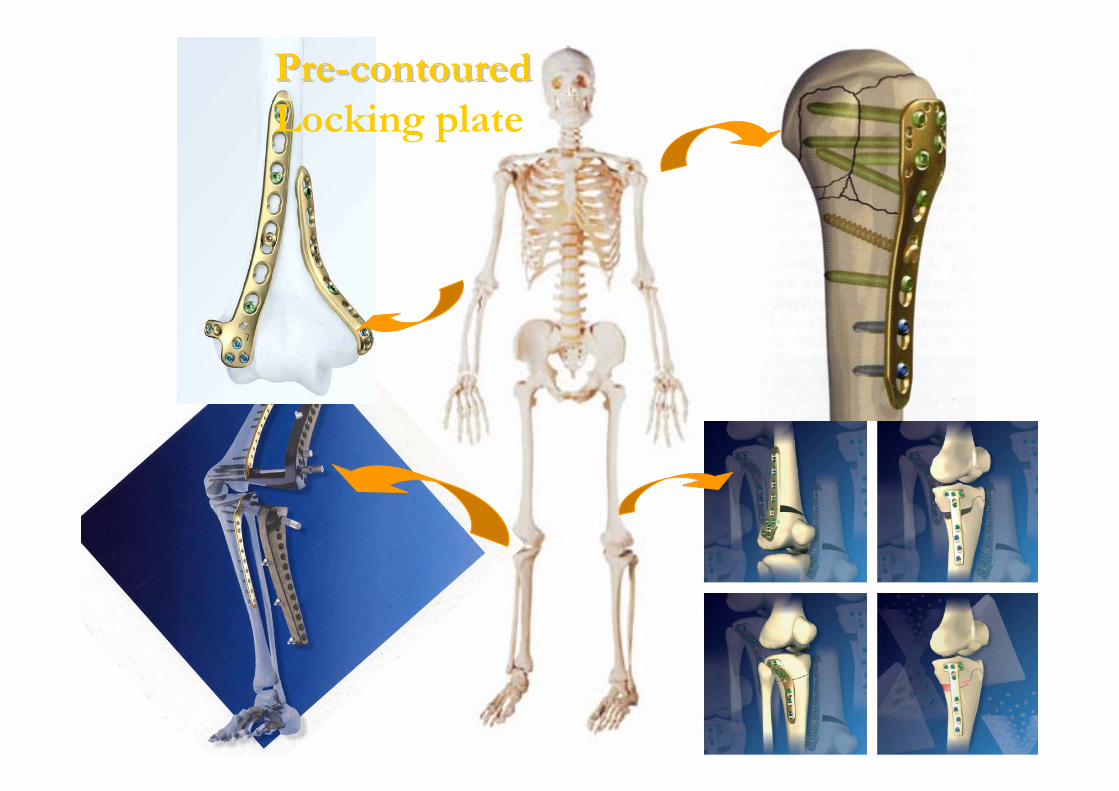
PrePre--contouredcontouredLocking plate

LISSLess Invasive Stabilisation System

LISSLISSLess Invasive Less Invasive StabilisationStabilisation SystemSystem
A special kind of A special kind of LCPLCPOutOut--rigger for rigger for insertion and insertion and targettingtargettingSo far, only distal So far, only distal femur and proximal femur and proximal tibiatibia

LISSLISS


Aiming device with guide sleeve for self-drilling self-tapping screws (only in LISS)Cooling required!

LISS LISS -- Reservations Reservations ““Less InvasiveLess Invasive”” is surgeon / experience is surgeon / experience dependentdependentDifficult to train / superviseDifficult to train / superviseDoubtful anatomical conformity Doubtful anatomical conformity ––
E.g. E.g. ““anteante--curvaturecurvature”” and size of the femoral and size of the femoral condylecondyle
Not forgivingNot forgivingNot adjustable / revisable once implantedNot adjustable / revisable once implanted

Precaution:Precaution:
Important!
If the first screw to be inserted is a Locking Head Screw, it is important to ensure that the plate shows good temporary fixation. Otherwise, the plate rotates simultaneously when locking the screw, and might cause soft-tissue injuries

Locking Head ScrewsLocking Head Screws
Must be placed in exact Must be placed in exact axial alignment with the axial alignment with the hole on the platehole on the plate
Difficult to angle screws in Difficult to angle screws in plate to obtain osseous plate to obtain osseous purchasepurchase
Drill blocks for selfDrill blocks for self--tapping screws (requiring tapping screws (requiring prepre--drill)drill)

Should the plate lie too ventral or too dorsal, the screws will not be centred in the medullary canal. This position may compromise the screw purchase.

••Limited ability to compress fractureLimited ability to compress fracture••Can not use plate as a reduction aidCan not use plate as a reduction aid•Positioning and Compression Device (PCD)

Skin impingement

Removal of locking screw from the Removal of locking screw from the plate sometimes is difficult: plate sometimes is difficult:
need to prepare broken screw need to prepare broken screw removal setremoval set

The End The End
Thank YouThank You







![Meta-analysis of plate fixation versus intramedullary fixation ......intramedullary fixation (IF), the common devices in clinics are Knowles pinning [14,15], elastic stable intramedullary](https://static.fdocuments.net/doc/165x107/60ec8dbb516bc21c1e0f6489/meta-analysis-of-plate-fixation-versus-intramedullary-fixation-intramedullary.jpg)










