Liver Transplantation for Alcoholic Liver Disease · Alcoholic Liver Disease ABHINANDANA...
13
Liver Transplantation for Alcoholic Liver Disease ABHINANDANA ANANTHARAJU, M.D., AND DAVID H. VAN THIEL, M.D. In many patients, long-term heavy drinking leads to chronic liver disease, liver failure, and even death. Orthotopic liver transplantation (OLT) is the only definitive treatment for end-stage liver disease, including alcoholic liver disease (ALD). Because of a shortage of donor organs, OLT for ALD patients remains controversial out of concerns that patients may resume drinking, therehy harming the transplanted organ. Therefore, transplant centers conduct careful screening proce- dures that assess patients' coexisting medical problems and psychosocial status to identify those patients who are medically most suited for the procedure and who are most likely to remain abstinent after OLT. Studies assessing the outcomes of ALD patients after OLT found that the sur- vival rates of the transplanted organ and the patient were comparable to those of patients with nonalcoholic liver disease and that relapse rates among the ALD patients were low. Similarly, ALD patients and patients with other types of liver disease had comparable rates of compliance with complex medication regimens after OL T. Enhanced efforts to identify risk factors for relapse among OL T candidates with ALD and to target interventions specifically to those patients who are at high risk of relapse may further improve patient outcome and enhance the acceptance of OLT for alco- holic patients in the general population. KEY WORDS: aicohoiic liver disorder; urgjn transplantation; liver; patient assessment; patient compliance; comorbidlty; cardiomyopathy; pancreatitis; malnutri- tion; hepatocellular carcinoma; AODR (alcohol and other dru^ related) structural brain damage; bone mineral density; hepatitis C virus; AOD abstinence; alcohol use test treatment outcome; quality of life; AODD (alcohol and other drug dependence) relapse; predictive factor; patient monitoring; med- ical ethics P optilatlon-based surveys indicate that 68 percent oi aduJr Americans drink at least one alcoholic beverage per month. About 10 percent consume more thati two drinks per day, which is a commonly used definition of "heavy drinking" (Hoofiiagle et aJ. 1997). How- ever, substantial differences exist in the prevalence of heavy drinking among population subgroups. For example, 18 percent of men but only 3 percent of women ate cLissified as heavy drinkers, and heav\' drinking is more common among Whites than among African Americiins or Hispanics. Heavy drinking and its consequences are itnportant public health problems, as illustrated by the following statistics: • Five percent of the deaths occurring annuiilly in the United States (approx- imately 100,000 per year) are either directly or indirectly attributable to alcohol abuse (Hoofriagle et al. 1997). Only about 10 percent of all drinkers account for 30 percent of the total alcohol consumption in the United States per year (Li 1997). About 13.8 million people in the United States meet the diagnostic criteria for alcohol abuse or depen- dence specified in the fourth edition of the American Psychiatric Associations Diagnostic and Statistical Manual of Mental Disorders (Grant et al. 1994). About 13 percent of U.S. alcoholics eventually will develop alcoholic liver disease (ALD), a broad spectrum of liver injuries—ranging trom asymp- tomatic fatty liver (i.e., steatosis) or abnormalities of liver enzymes to end-stage liver disease—that result from alcohol ingestion. Women in general show greater susceptibility to ALD than men, and African Americans show greater susceptibil- ity than Whites. • Among heavy drinkers, liver disease is highly prevalent. Thus, 90 to lOO ABHINANDANA ANANTHARAJU, M.D., is a fellow, and DAVID H. VAN THIEL, M.D., is a professor of medicine and surgery and director oj Liver Transplantation and Hepatology. Both are associated with the Liver TranspLmt Program in the Division ofGiistroenterohgy, Hepatology, and Nutrition, at Loyola University Medical Center, Maywood, Illinois. VOL. 27. No. 3, 2003 257
Transcript of Liver Transplantation for Alcoholic Liver Disease · Alcoholic Liver Disease ABHINANDANA...

Liver Transplantation forAlcoholic Liver Disease
ABHINANDANA ANANTHARAJU, M.D., AND DAVID H . VAN THIEL, M . D .
In many patients, long-term heavy drinking leads to chronic liver disease, liver failure, and evendeath. Orthotopic liver transplantation (OLT) is the only definitive treatment for end-stage liverdisease, including alcoholic liver disease (ALD). Because of a shortage of donor organs, OLT forALD patients remains controversial out of concerns that patients may resume drinking, therehyharming the transplanted organ. Therefore, transplant centers conduct careful screening proce-dures that assess patients' coexisting medical problems and psychosocial status to identify thosepatients who are medically most suited for the procedure and who are most likely to remainabstinent after OLT. Studies assessing the outcomes of ALD patients after OLT found that the sur-vival rates of the transplanted organ and the patient were comparable to those of patients withnonalcoholic liver disease and that relapse rates among the ALD patients were low. Similarly, ALDpatients and patients with other types of liver disease had comparable rates of compliance withcomplex medication regimens after OL T. Enhanced efforts to identify risk factors for relapse amongOL T candidates with ALD and to target interventions specifically to those patients who are at highrisk of relapse may further improve patient outcome and enhance the acceptance of OLT for alco-holic patients in the general population. KEY WORDS: aicohoiic liver disorder; urgjn transplantation;liver; patient assessment; patient compliance; comorbidlty; cardiomyopathy; pancreatitis; malnutri-tion; hepatocellular carcinoma; AODR (alcohol and other dru^ related) structural brain damage; bonemineral density; hepatitis C virus; AOD abstinence; alcohol use test treatment outcome; quality oflife; AODD (alcohol and other drug dependence) relapse; predictive factor; patient monitoring; med-ical ethics
Poptilatlon-based surveys indicatethat 68 percent oi aduJr Americansdrink at least one alcoholic beverage
per month. About 10 percent consumemore thati two drinks per day, which isa commonly used definition of "heavydrinking" (Hoofiiagle et aJ. 1997). How-ever, substantial differences exist in theprevalence of heavy drinking amongpopulation subgroups. For example,18 percent of men but only 3 percentof women ate cLissified as heavy drinkers,and heav\' drinking is more commonamong Whites than among AfricanAmericiins or Hispanics. Heavy drinkingand its consequences are itnportantpublic health problems, as illustratedby the following statistics:
• Five percent of the deaths occurringannuiilly in the United States (approx-
imately 100,000 per year) are eitherdirectly or indirectly attributable toalcohol abuse (Hoofriagle et al. 1997).
Only about 10 percent of alldrinkers account for 30 percent ofthe total alcohol consumption inthe United States per year (Li 1997).
About 13.8 million people in theUnited States meet the diagnosticcriteria for alcohol abuse or depen-dence specified in the fourth editionof the American Psychiatric AssociationsDiagnostic and Statistical Manual ofMental Disorders (Grant et al. 1994).
About 13 percent of U.S. alcoholicseventually will develop alcoholic liverdisease (ALD), a broad spectrum ofliver injuries—ranging trom asymp-
tomatic fatty liver (i.e., steatosis) orabnormalities of liver enzymes toend-stage liver disease—that resultfrom alcohol ingestion. Women ingeneral show greater susceptibilityto ALD than men, and AfricanAmericans show greater susceptibil-ity than Whites.
• Among heavy drinkers, liver diseaseis highly prevalent. Thus, 90 to lOO
ABHINANDANA ANANTHARAJU, M.D., is
a fellow, and DAVID H. VAN THIEL, M.D.,
is a professor of medicine and surgery anddirector oj Liver Transplantation andHepatology. Both are associated with theLiver TranspLmt Program in the DivisionofGiistroenterohgy, Hepatology, andNutrition, at Loyola University MedicalCenter, Maywood, Illinois.
VOL. 27. No. 3, 2003 257
percent of heiivy drinkers have steatosis,10 ro 35 percent have alcohol-induced inflammation of the liver{i.e., alcoholic hepatitis), and 8 to20 percent have alcoholic cirrhosis(McCullough 1999).
• The 5-year and 10-ye;jr sutrival ratesfor patients with alcoholic cirrhosisare 23 percent and 7 percent, respec-tively (McCuliough 1999). The.serates are significantly worse thansurvival rares for patients whose cir-rhosis was nor caused by alcohol.
Alcohol consumption is one of theleading causes of chronic liver diseasein the United States and worldwide.In Western countries, alcohol is themaior causative factor in about SO percentof deaths from end-stage liver disease(McCullough 1999). Ib date, liver trans-plantation {also ktiown as otthotopic'liver transplantation [OUT]) is the onlydefinitive treatment for end-stage liverdisease. However, OLV for patientswith ALD continues to be controversialbecause of the ever-increasing demandfor donor organs and the inadequaterate of organ donation, combined withconcerns that alcoholic patient.s mightrelapse to drinking, thereby damagingthe transplanted liver.
This review discusses the patterns andcontroversies relating to liver transplan-tation in patients with ALD. After pro-viding some historical perspective andsummarizing the current .status of OLTin these patients, the article discusseselements of the pretransplantation eval-uation that can help identify suitablepatients for the procedure. Outcomesfor ALD patietits who have received livertransplants are reviewed, and the ethicalissues surrounding this procedure inalcoholic patients are discussed. Thisarticle concludes by summarizing futureresearch directions that might improvethe outcomes of liver transplants inalcoholics and thereby tesolve some ofthe ethical concerns,
Orthotopic means "in the normal or usual place."
HISTORICAL PERSPECTIVE ANDCURRENT STATUS OF OLT INALCOHOLIC PATIENTS
Historical Perspective
Before the National Institutes of Health(NIH) C!!onsensus Conference on LiverTransplantation in 1983. OLT rarelywas performed in patients with ALD.The Consensus Conference concludedthat ALD is an appropriate indiaitionfor OLT if the patient is judged likelyto abstain from alcohol after transplan-tation (Lucey 2001). This conclusion,which was adopted by many transplantcenters, led to an increase in the num-ber of transplants performed for ALD.A report by Starzl and colleagues {1988)made the most convincing argiitnent forOLT for ALD patients, demonstratingthat 73 percent of ALD patients whohad received a liver transplant still werealive 1 year after the procedure, and thatonly 3 percent of those panents hadrelapsed to alcoholism. Based on thesefindings, in 1991 the Health CareFinancing Administration (HCFA)identified ALD as one of the seven con-ditions for which it approved paymentfor OLF, but the HCFA recommendeda "significant" period of abstinence foralcoholics before undergoing the proce-dtire as well as the availability of a rea-sonable social support system.
To identify alcoholic patients suitablefor OLT, Beresfotd ;ind coOeagues {1990)proposed a selection method that includedmeasures of the likelihood of abstinence,such as the extent to which alcoholdependence was recognized by the patientand his or her family, the patients degreeof social stability, and the nature andextent of lifestyle changes conduciveto long-term abstinence. Using thisselection method, Lucey and colleagues{1992) reported on a multidisciplinarycollaboration of transplant hepatologists,.surgeons, and psychiatrists that identifiedpsychosocial predictors of long-term.sobriety and compliatice afier OLT inalcoholics. {'I'hcse predictors are sum-marized in the University of MichiganAlcoholism Prognosis Scale, which isdiscussed later.) 'ITiese researchers reportedthat ALD patients judged suitable using
these criteria had outcomes after OLTthat were similar to outcomes for trans-plant patients with non-alcohol-relatedliver disease {non-ALD). People whowere judged suitable for OL'F includedpatients with severe end-stage liver diseasewithout an available alternative therapy,who showed a clear understanding ofthe risks and benefits of the procedure,had a favorable psychiatric assessmentincluding acceptance of alcoholism, andhad fiivorable prognostic factors forfuture sobriety.
The minimal listing criteria estab-li.shed by the United Network for OrganSharing (UNOS) in 1996 do not includean absolute requirement for a 6-monthperl(xl of abstinence before ALD patientsare listed as candidates for OLT {UNOS1996). Furthermore, a 1996 NIHworkshop on OLT for patients with AI.Dconcluded that liver transplantationprovides a good outcome in alcoholicpatients and that relapse rates after OLTwere lower if the patients had success-fiilly completed conventional alcoholrehabilitation programs prior to OLT{Hoofnagleetal. 1997).
ALD now is widely accepted bymany transplant centers as a valid indi-cation for OLT, provided the transplantteam caring for the patient can reason-ably expect him or her to remain absti-nent after the transplant.
Current Status
According to the UNOS database,41,734 liver transplants using organsfrom dead donors (i.e., cadaveric trans-plants) were performed in the UnitedStates between 1992 and 2001 {UNOS2002). Of those, 12,5 percent were per-formed in patients with ALD, and 5-8percent were performed in patientswith ALD and a concurrent infectionwith the hepatitis C virus (HCV).' Thismakes ALD the second most frequentindication (afi:cr HCV infection alone)for which OLl' was performed duringthis period. As of November 2002,17,646 patients in the United States
Infection with HCV (as well as with other related virus-es, such as the hepatitis B virus) can lead to chronicintianimation ol the iiver (i.e., hepatitis), which eventuallycan cause complete liver failure and death.
258 ALCOHOL RESEARCH & HEALTH

LIVER TRANSPLANTATION FOR A L C O H O L I C LIVER DISEASE
were on the waiting list for a cadavericliver transplant; ot these, about 14.1percent had ALD, and 6.2 percent hadcombined ALD and HCV infection.
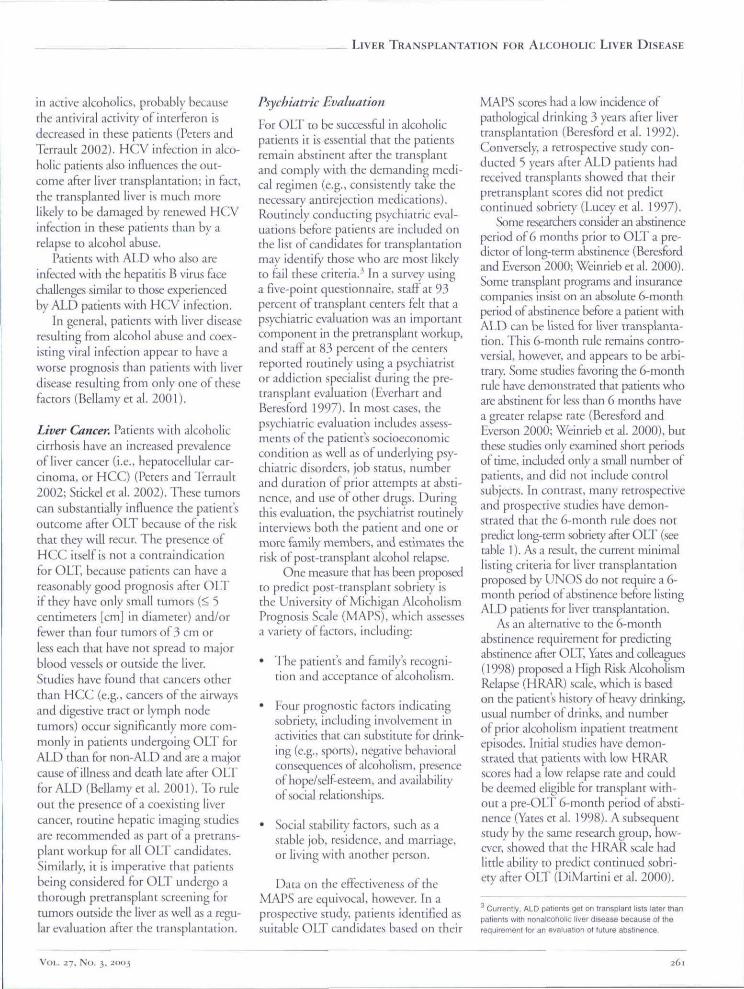
Overall, the number of Hver trans-plants performed annually tor ALD hasbeen relatively constant for many years(see the accompanying figure), but thenumber performed because of chronicHCV infection has increased annually,as has the number of liver transplantsfor combined ALD and HCV infection.
PRETRANSPLANT EVALUATIONOF PATIENTS WITH ALD
To ensure the success of liver transplanta-tion, ALD patients are requited to iindei^a thorough evaluation to determinewhethet they are suitable candidates.This evaluation addresses any coexistingmedical problems that might influencethe outcome of the transplant andincludes a psychological evaluation toidentify those patients who are most likelyto remain abstinent and comply with themedical regimen after the procedure.
Coexisting Medical Problems
Alcohol affects many organ systems inaddition to the liver. For example, asdescribed by Keeffe (1997) and Neubergerand coUeagties (2002), alcohol abusecan lead to:
• Damage of the heart muscles {i.e.,cardiomyopathy) and skeletal mus-cles (i.e., skeletal myopathy).
• Inflammation of the pancreas (i.e.,pancreatitis).
• Mahiutrition.
• Central and peripheral nervous systemdysftjnaion.
• "SoH:" bones that lack minerals forstability (i.e., osteopenia/osteoporosis).
• Cancers of the airways and diges-tive tract.
These conditions, particularly if theyare severe, can complicate the manage-ment of patients with ALD both before
and after OLT, and some may even becontraindiaitions for OLT (KeefFe 1997).However, some of these alcohol-inducedconditions (e.g., cardiomyopathy andacute pancreatitis) can be reversed byabstinence, and when such a reversaloccurs, these conditions do not affectthe decision on a patients suitabilityl"or a transplant.
The clinical approach to evaluat-ing a patient for OLT also may bemarkedly alrered by other disorders thatcan coexist with ALD, such as infec-tion with hepatitis viruses, particularlyHCV, and the presence of liver cancer.The impact of all these coexisting condi-tiotis is discussed in the sections to follow.
Cardiomyopathy. The exact preva-lence of heart disease in patients withend-stage ALD is unknown (Keeffe1997). Overall, catdiomyopathy is formore common in actively drinkingalcoholics than in abstinent alcoholics(Campbell and Lucey 1996). In general,alcohol-related cardiomyopathy rarelyis a reason for refusing liver transplan-tation (Lucey 2001). Anecdotal evidence
6000
5000Cfl
na 4000(0cn• - 3000
HCV ALD ALD + HCV Total
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Year
Liver transplantation for alcoholic liver disease (ALD) and hepatitis C (HCV), 1992-2001.
SOURCE: United Network tor Organ Sharing (UNOS) registry, 1988-2001. Public data tfom UNOS/OPTN scientific registry (http;//www,unos.org|. Accessed December 2002.
VOL. 27, No. 3, 259

suggests that coronary artery disease(CAD) may be more ptevalent thancardiomyopathy in patients with ALD(Keeffe 1997). To identify either condi-tion in liver tnmsplatit candidates,many transplant centers routinely assesscardiac function through noninvasivetests (e.g., eiectrocardiography, echocar-diography, and stress tests) ;is part ottheir pretransplant evaluations (Neu-berger et al. 2002). A more invasivetechnique, coronary angiography, usesX rays to visualize the structure oFtheheart and blood vessels following theinjection of a contrast medium, andcan identify more patients with CADthan the various noninvasive cardiactests used (Keefife 1997). AlthoughCAD is not a reason to refuse a patienta transplant because it usually can bereversed by abstinence, the conditioncan create problems if it has not beenidentified prior to the OLT.
Skeletal Myopathy. Muscle damageoccurs in up to 42 percent of alcoholicpatients with ALD; A6 percent of activelyalcoholic men show changes in musclecell strucmre indicative of skeletal myo-pathy (Keeffe 1997). This condition ismanifested as muscle weakness, musclepain, and abnormal tests for muscleenzymes; the disorder results from acombination of alcohol's direct effects onthe muscles, malnutrition, and alcohol-related inflammation or degenerationof nerves (i.e., neuropathy) (Keeffe 1997).The presence of skeletal myopathyappears to depend on how much alco-hol the person has consumed over hisor her lifetime (Keeffe 1997; Campbelland Lucey 1996). In general, skelet;ilmyopathy is not a contraindication forOLT, and severe myopathy is unusualin potential alcoholic OLT candidates.
Pancreatitis. Chronic inflammation ofthe pancreas is five times less commonin people with ALD than in alcoholicswithout liver disease; the reasons forthis difference are not known (Keeffe1997). In general, pancreatitis is notconsidered a contraindication for livertranspliin ration; however, severe chronicpancreatitis can adversely affect theabsorption of medications that preventthe immune system from rejecting the
transplanted liver. Therefore, patientswith pancreatitis may require closermonitoring for rejection of the trans-planted organ as well as administrationof higher doses of antirejection medica-tions to achieve effective concentrations.
Malnutrition. Malnutrition occurs inmany, if not all, patients with ALD.Causes of malnutrition include apoor diet; increased breakdown (i.e.,oitabolism) of carbohydrates, proteins,and lipids in the Uxfy; as well as impairedabsorption of nutrients, interruption ofthe bile flow (i.e., cholestasis), reducedpancreatic function, bacterial over-growth, and/or alcohol-induced injuryto the intestin;il mucosa (Matos et al.2002). In particular, alcoholics com-monly show deficiencies in variousvitamins, including thiamine, which isessential for normal brain functioning.Therefore, alcoholics with ALD rou-tinely should be prescribed thiamineand multivitamins. Severe malnutritionis associated with a poorer prognosisafter OLT and may require postpone-ment of the procedure until the patienthas achieved a better state of nutrition(Matos et al. 2002). The nutritional sta-tus of OLI" candidates can be improvedby providing additional nutrition directlyinto the gastrointestinal tract (i.e., byenteral feeding). Moreover, nutritionalsupport before and after the transplantcan improve the clinical outcome afi:erOLT (Matos et al. 2002).
Neiirolo^al Deficits. Chronic alco-holism may lead to netirologicil deficitsthrough alcohol's direct actions on thebrain and nerve fibers, which can resultin structural damage (Luccy 2001;KeefFe 1997). In patients with ALD,however, neurological deficits also canresult from a condition called hepaticencephalopathy, which is caused by thedamaged liver's inability to remove sub-stances from the blood that can inter-rupt brain function. In these patients,it is difficult to distinguish deficitsrestating from alcohol's direct effects onthe brain from those resttlting from hep-atic encephiilopathy. Severe neurologicaldeficits may contraindicate liver trans-plantation because the patient may notbe able to comply with post-transplant
medication regimens and because OLTmay not improve the patient's qualit)'of life significantly. Therefore, most trans-plant centers routinely perform brain-imaging analysis of OLT candidates toidentify any structural damage thatmay exist before the transplant andwhich could affect the patient's out-come aft:er the transplant (Lucey 2001).
Abnormal Bone StructuTv. Patientswith ALD are prone to bone lossbecause of impaired activity of thebone-producing cells; reduced activityof the ovaries or testes, which producehormones regulating bone formation;reduced body mass index; and limitedphysical activity (Keeffe 1997).Between 10 and 42 percent of patientswith ALD have a reduced bone density,which can lead to a condition calledosteopenia (or, in severe cases, osteo-porosis), which is characterized bybone softening, accompanied by weak-ness and susceptibility to fractures.Therefore, routine bone mineral den-sity measurements and, in appropriatecases, blood tests assessing calciummetabolism and ovarian or testicularflinction are recommended in patientswith ALD. Treatment with calciumand vitamin D (which regulates cal-cium metabolism) can improve bonemineral densit)' in patients with ALD(Rouillard and Lane 200!). Otherapproaches used to improve bone min-eral density in patients with non-ALDinclude administration of hormones tocompensate for reduced ovarian or tes-ticular activity as well as treatment withother compounds that influence cal-cium metabolism (i.e., calcitonin andbiphosphonates) (Rouillard and Lane2001). The effectiveness of theseapproaches in alcoholics, however, hasnot been stitdied specifically.
HCVInfection. About 20 to 30 per-cent of patients with ALD are infectedwith HCV (Keeffe 1997), and the rateof progression of liver disease and thelong-term outcome are worse for thesepatients than for alcoholics not infectedwith HCV (Peters and Ibrrault 2002).In addition, the most commonly usedtreatment for HCV infection—anagent called intcrferon—is less effective
260 ALCOHOL RESEARCH & HEALTH
LIVER TRANSPLANTATION FOR A L C O H O L I C LIVER DISEASE
in active alcoholics, probably becausethe antiviral activity of interteron isdecreased in these patients {Peters andTerrauir 2002). HCV infection in alco-holic patients also influences the out-come after liver transplantation; in fact,the transplanred liver is much morelikely to be damaged by renewed HCVinfection in these patients than by arelapse to iilcohol abuse.
Patients with ALD who also areinfected with the hepatitis B viras facechallenges similar to those experiencedby ALD patients with HCV infection.
In general, patients with liver diseaseresulting from alcohol abuse and coex-isting viral infection appear to have aworse prognosis than patients with liverdisease resulting from only one of thesefactors (Bellamy et al. 2001).
Liver Cancer. Patients with alcoholiccirrhosis have an increased prevalenceof liver cancer (i.e., hepatocellular car-cinoma, ot HCC) (Peters and Terrault2002; Stickel et al. 2002). These tumorscan substantially influence rhe patient'soutcome after OLT because of the riskthat they will recur. The presence ofHCC itself is not a contraindicationfor OLT, because patients can have areasonably good prognosis after OLT\k they have only small tumors {< 5centimeters [cm] in diameter) and/orfewer than four tumors of 3 cm orless each that have not spread to majorblood vessels or outside the liver.Studies have found that cancers otherthan H C C (e.g., cancers of the airwaysand digestive tract or lymph nodetumors) occur significantly more com-monly in patients undergoing OLT forALD than for non-ALD and are a majorcaase ot illness and death late after OLTfor ALD (Bellamy et al. 2001). To ruleout the presence of a coexisting livercancer, routine hepatic imaging studiesare recommended as part of a pretrans-plant workup for ail OLT candidates.Similarly, it is imperative that patientsbeing considered for OLT undergo athorough pretranspiant screening fortumors outside the liver as well as a regu-lar evaluation after the transplantation.
Psychiatric Evaluation
For OLT to be successful in alcoholicpatients it is essential that the patientsremain abstinent after the transplantand comply with the demanding medi-cal regimen (e.g., consistently take thenecessary antirejection medications).Routinely conducting psychiatric eval-uations before patients are included onthe list of candidates for transplantationmay identify those who are most likelyto foil these criteria.' In a survey usinga five-point questionnaire, staff at 93percent of transplant centers felt that apsychiatric evaluation was an importantcomponent in the pretransplant workup,and staff at 83 percent of the centersreported routinely using a psychiatristor addiction specialist during the pre-transpiant evaluation (Everhart andBeresford 1997). In most cases, thepsychiatric evaluation includes assess-ments of the patients socioeconomiccondition as well as of underlying psy-chiatric disorders, job status, numberand duration of prior attempts at absti-nence, and use Q\ other drugs. Duringthis evaluation, the psychiatrist routinelyinterviews both the patient and one ormore family members, and estimates therisk of post-transplant alcohol relapse.
One measure that h;is been profKJsedto predict post-transplant sobriety isthe Univetsity of Michigan AlcoholismPrognosis Scale (MAPS), which assessesa variety of factors, including:
• The patient's and family's recogni-tion and acceptance of alcoholism.
• Four prognostic factors indicatingsobriety, including involvement inactivities that oin substitute tor drink-ing (e.g., sports), negative behavioralconsequences of alcoholism, presenceof hope/self-esteem, and availabilit)'of social relationships.
• Social stability factors, such as astable job, residence, and marriage,or living v '̂ith another person.
Data on the effectiveness of theMAPS are equivocal, however. In aprospective study, patients identified assuitable OLT candidates based on their
MAPS scores had a low incidence ofpathological drinking 3 years after livertransplantation (Beresford et al. 1992).Conversely, a retrospective study con-ducted S years after ALD patients hadreceived transplants showed that theirpretransplant scores did not predictcontinued sobriet)' (Lucey et al. 1997).
Some researchers consider an abstinenceperiod of 6 months prior to OLT a pre-dicror of long-term abstinence (Beresfordand Everson 2000; Weinrieb et al. 2000).Some tnmsplant programs and insurancecompanies insist on an absolute 6-monthperiod of abstinence before a patient withALD can be listed for liver transplanta-tion. This 6-month rule remains contro-versial, however, and appears to be arbi-trary. Some studies favoring the 6-monthrule have demonstrated that patients whoare abstinent for less than 6 months havea greater relapse rate (Beresford andEverson 2000; Weinrieb et al. 2000), butthese studies only examined short periodsof time, included only a small number ofpatients, and did not include controlsubjects. In contrast, many retrospectiveand prospective studies have demon-strated that the 6-month rule does notpredia long-term sobriety after OLT (seetable 1). As a result, the current minimallisting criteria for liver transplantationproposed by UNOS do not require a 6-month period ot abstinence before listingALD patients for liver transplantation.
As an alternative to the 6-monthabstinence requirement for predictingabstinence after OLT, Yates ;md colleagues(1998) proposed a High Risk AlcoholismRelapse (HRAR) scale, which is basedon the patient's history' of heav)' drinking,usual number of drinks, and numberof prior alcoholism inpatient treatmentepisodes. Initial studies have demon-strated that patients with low HRARscores had a low relapse rate and couldbe deemed eligible for transplant with-out a pre-OlT 6-month period of absti-nence (Yates et al. 1998). A subsequentstudy by the same research group, how-ever, showed that the HRAR scale hadlitde ability to predict continued sobri-ety after OLT (DiMartini et al. 2000).
•̂ Currently, ALD patients gel on transplant lists later thanpatients with nonalcoholic \wsr disease because of therequifement tor an evaluation ot future abstinence.
Vol.. 27, No. 3, 2003 2 6 1

OUTCOMES EOR ALD PATIENTSAFTER OLT
When assessing the long-rerm ourcomefor patients receiving OLT or any otherkind of transplant, researchers and clin-icians evaluate numerous factors inaddition to the surviviil of: the patient,including how long rhe transplantedorgan continues to function (i.e., graftsurvival) and the patient's quality oflife. Out of concerns that ALD patientsmay resume drinking after OLT andthereby damage the transplanted liver,investigators frequently assess graft sur-vival in these patients. These assessmentshave found that the graft-survival ratein patients with ALD is comparable tothat of patients with non-ALD (seetable 2) (UNOS 2002). This findingsu^ests that the ALD patients are notmore likely to relapse (or that their
alcohol consumption may not be likelyto damage the transplanted liver). Infact, the 1 - and 3-year graft-survivalrates in patients with ALD are abovethe average graft-survival rates for alldiagnoses fot which OLTs are per-formed (see table 2). Moreover, the pres-ence oi" a concurrent HCV infectiondoes not appear to alter the I-, 3-, and5-year graft-survival rates in patientswith ALD. However, a study by Neu-berger and colleagues (2002) demon-strated that patients undergoing OLTfor combined ALD and HCV infectionwere more likely to develop hepatic fibro-sis than were patients with either ALD orHC^ infection alone. Additional survivalrates reported by various grotips ofinvestigators are summarized in table 1.
A few retrospective studies have beenperformed in abstinent patients whounderwent OLT for ALD. These
patients' livers subsequently weteremoved and examined for the presenceof hepatitis caused by alcohol. Again,the presence of hepatitis appeared tohave no impact on outcome, with thesurvival and relapse rates of thesepatients comparable to those of patientswith alcoholic cirrhosis alone (Lucey2002). No specific studies have assessedOLT survival rates and sobriety inpatients with actite alcoholic hepatitis.
Quality of Life
The term "quality of life" encompassesvarioits faaors that influence a patientssubjective well-being, such as medicalstatus, social status, employment status,or relationships, (derail, the physical ;mdpsychological outaimes for AI ,D patientsaftet OLT appear similar to those ofnon-ALD patients (Pereira et al. 2000).
Table 1 Studies Reporting Outcomes of Orthotopic
Study*
Starzi et al.
Kumar et al.Bird et al.Stevens et al.Knechtle et al.Goldstein et al.Gish et al.Osorio et al.Berlakovich et al. (1994)
Howard et al.Raakow et al.Gerhardt et al.
Tringali et al.Zibari et al.
Lucey etal, (1997)Foster et al.
Anand et al.Everson et al.Stefanini et al.
Fabrega et al.Tang et al.Pageaux et al.
Period
1980-871982-881980-891985-901984-901985-911988-911988-911982-931987-921988-941985-911988-901986-921987-911986-941987-941988-961986-96
N/A1987-961989-94
'For full citations of these studies, see References,
No.
Liver Transplantation (OLT) in Patients
No. ofPatients
of Lost toPatients Followup
41
7324
10414129435820
7867
10342598439
68184471
53
11
21
6-
30400
1420
02645
09
210670
150
With Alcof̂ olic Liver Disease
Patients EmployedMonths of (Part-Time/Full-Time) {%)FollowupAfter OLT
12-3625
4-841-24N/A
6-6612-417-38
3312-72
0.5-6436-9618-46
N/A6-89
28-707-63<90
< 11820-59
NA42
BeforeOLT
N/A
0N/AN/A63
N/AN/A6248
N/AN/AN/A330
N/AN/AN/AN/A
0N/A
8N/A
Used6-Month
After AbstinenceOLT
N/A5494
N/A33
N/A805989
N/A99
N/A4076
N/AN/AN/AN/A73
N/A5230
Criteria?
NoNoNoNoNo
YesNo
YesNo
N/ANoNoNoNoNoNoNo
N/AYes
YesNoNo
262 ALCOHOL RESEARCH & HEALTH
LIVER TkANSPLANTATiON FOR ALCOHOLIC LIVER DISEASE
However, patients who relapse to alco-hol use after receiving rninsplants havepoorer post-transplant scores onquality-of-life measures than patients whodo not relapse (Coffman et al. 1997).
ALD patients in general have prob-lems keeping a job and fulfilling theirjob requirements (i.e., they have lowlevels of occupational functioning).OLT can ameliorate these problems toa certiiin extent. Nevertheless, an analysiscombining the findings oi several stud-ies (i.e., a meta-analysis) demonstratedthat the employment status of ALDpatients both before and after trans-plantation is dismal (Bravata et al.2001). Before transplantation, 29 per-cent of ALD patients and 59 percent ofnon-ALD patients were employed. At3 years after the OLT, employmentrates for non-ALD patients had increasedsubstantially (i.e,, to 80 percent), whereas
employment rates for ALD patients hadincreased only marginally (i.e., to 33percent). Furthermore, no associationswere found between alcohol use andetnployment status after OLl ' orbetween pre- and post-tnmsplant employ-ment and sobriety. With all these findingsit is important to note, however, that theemployment status reported in manystudies is based on self-reports, which havesubstantiiil limitations (i.e., respondentsmay not always answer truthfiiUy or maynot acctirately recall the information).
Relapse to Alcohol Use
As mentioned previously, an importantconcern in selecting alcoholic cindidatesfor OIH" and evaluating the outcomeof the procedure is the likelihood of 3relapse to alcohol use after the trans-plant. The definition of an alcohol
relapse is controversial, varying fromany use of alcohol after OLT to alcoholabuse resulting in physical and socialconsequences or rehospitalization foralcoholism (Fuller 1997). Althotighany alcohol use after OLT should beviewed as serious because it is the earliestindicator of high risk for the long-termviability of the graft (Beresford 1994),not all relapses may be harmful to thetransplanted liver and the patient. Theoccasional use of small amounts ofalcohol (i.e., a "slip") is not consideredharmftil and should not be treated puni-tively (Fuller 1997). These slips maynot progress to an overt relapse that ispotentially harmftil to the new liver.
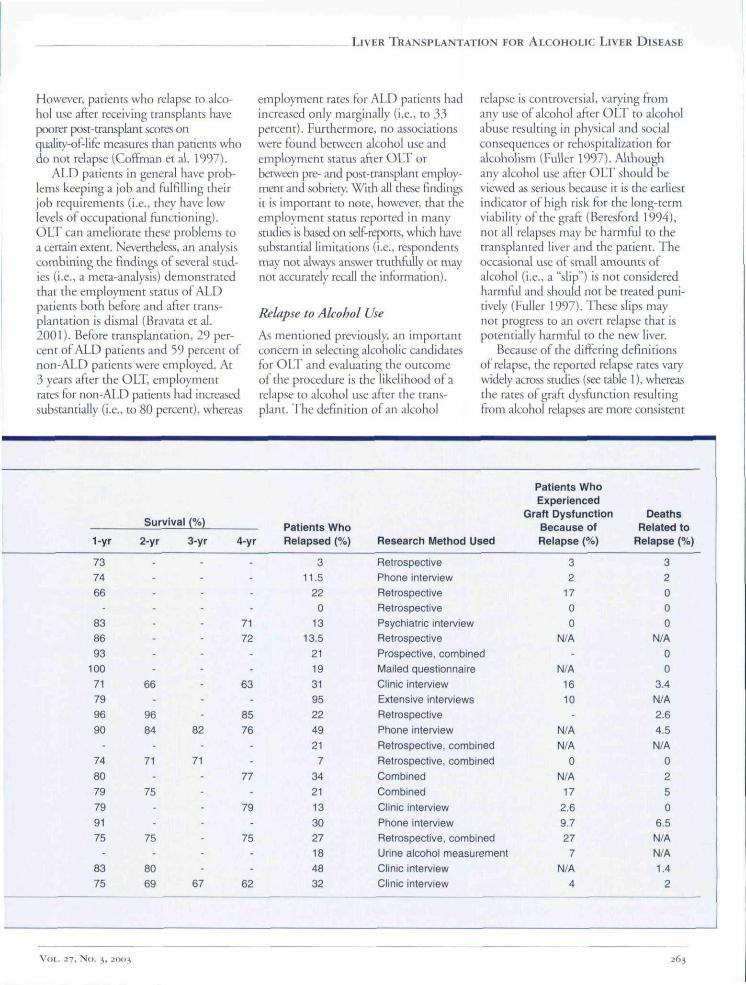
Because of the differing definitionsof relapse, the reported relapse rates var\'widely across snidies (see table I), whereasthe rates of graft dysfunction resultingfrom alcohol relapses ate more consistent
1-yr
73
74
66
-
8386
93
10071
79
98
90-
74
80
79
79
9175
-
8375
Survival (%)
2-yr 3-yr
--
-
-
-
-
-
66-
96
84 82-
71 71-
75-
-
75-
80
89 67
4-yr
--
-
-71
72-
-
63-
85
76-
-
11-
79-
75--
62
Patients Whn
Relapsed (%)
3
11.522
013
13.5
21
19
31
9522
49
21
7
34
21
13
3027
18
4832
Research Method Used
Retrospective
Phone interview
Retrospective
Retrospective
Psychiatric interview
Retrospective
Prospective, combined
Mailed questionnaire
Clinic interview
Extensive interviews
Retrospective
Phone interview
Retrospective, combined
Retrospective, combined
Combined
Combined
Clinic interview
Phone interview
Retrospective, combined
Urine alcohol measurement
Clinic interview
Clinic interview
Patients WhoExperienced
Graft Dysfunction
Relapse (%)
32
17
00
N/A-
N/A
16
10
N/A
N/A
0
N/A
17
2.69.7
27
7N/A
4
DeathsRelated to
Relapse (%}
3
Z0
0
0N/A
00
3.4
^4/A
2.6
4.5
N/A
0
2
5
0
6.5
N/AN/A
1.4
2
VOL. 27, No. 3. 2003 263

regardless of the definition of relapse ased.Furthermore, the transplanted liver isrejected at a similar rate in both abstinentand nonabstinent alcoholic patients{Campbell and Liicey 1996). This rejec-tion reaction can occur if the patientdoes not consistently take necessaryantirejection tnedications. Studies havefound that among patients receivingOLT for ALD, the overall rate of non-compliance with the antirejection med-ications is as high as 16 percent{Berlakovich et al. 2000). However,alcohol relapses per se do not appearto influence the patients" compliancewith their medication regimen.
Interestingly, a meta-analysis foundthat ALD and non-AlD patients reportedsimilar rates of alcohol use at 6 months{4 percent and 5 percent, respectively)and 12 months (17 percent and 16 per-cent, respectively) after OLT (Bravata etal. 2001), although heavy drinking wasmore common in patients who hadundergone liver transplantation forALD. At 7 years after OLT, 32 percentof ALD patients reported drinkingsome alcohol (Bravata et al. 2001). Aspreviously mentioned, continued alco-hol use after OLT puts the patient atrisk for renewed ALD. Studies havefound, however, that from a purely bio-logical perspective, recurrent ALD isless prevalent and less severe after OLTthan recurrent liver disease from othercauses (e.g,, reinfection with a hepatitisvirus) (Bellamy etal. 2001).
The reported relapse rate is influ-enced not only by the different defini-tions of relapse but also by the methodused to identify a relapse. 1 he mostuseful identification method appearsto be a clinical interview conducted bya transplant psychiatrist or a question-naire interview by an assistant (DiMartiniet al. 2001). Biochemical markers (e.g.,alcohol levels in the blood, urine, orbreath, or tests for the presence of certainenzymes) as well as regular liver biopsiesare less effective at identifying relapses(Neuberger et al. 2002; DiMartini etal. 2001; Campbell and Punch 1997).Relapse rates are highest during the ini-tial 6 months afxer the transplant anddecline after this period (Platz et al. 2000),About 93 percent of all relapses occurin the first 2 years after OLT.
Predictors of Relapse After OLT
Most patients with ALD are less severelydependent on alcohol than patientsattending alcohol clinics (Howard andFahy 1997), possibly because patientswho do not exhibit symptoms of severealcohol dependence are at greater riskof developing ALD because they cansustain continuous alcohol consumptionover many years (Wodak et al. 1983).'I'he patient's premorbid social stabilityand Alcoholics Anonymous attendancerecord before OLT are importantdeterminants of sustained abstinenceafter the procedure (Howard and Fahy1997; Beresford 1997). Such factors cmbe assessed prior to a transplant usingmeasures such as the Strauss-Baconand Skinner indices, but few transplantcenters report using these indices(Beresford 1997).
Another factor influencing relapserisk is the presence of other psychiatricdisorders. The prevalence of preexistingpsychiatric disorders in ALD patients isunknown. The few studies conductedin this patient population appear toshow a higher rate ot major psychiatricdisorders among ALD patients than inthe general poptilatioti (Beresford 1997).However, major depre-ssive disorders orschizophrenic conditions, which would
indicate a greater risk of relapse afterOLT, occur only rarely (Howard andFahy 1997; Beresford 1997). The pres-ence of post-traumatic stress disorderalso increases the risk of alcohol relapse.
Coexisting dependence on drugsother than alcohol also is associated withhigher rates of alcohol relapse. Studieshave found that although 30 to 30percent of patients who are dependentonly on alcohol achieve sustained absti-nence after alcoholism treatment, only10 percent of patients who used morethan one drug achieved abstinence(Beresford 1997).' A prolonged periodof documented abstinence from alldrugs am indicate a low risk of relapse.Conversely, multiple failed attempts atalcohol abstinence before OLT ate con-sidered an indication that the prognosisfor sustained sobrietj' after the trans-plant is poor (Beresford 1997).
Based on long-term studies of alco-holism remissions and relapses, Vaillant(1993) proposed four prognostic fac-tors that indicate a favorable otitcome;the patients involvement in activitiesthat can substitute for alcohol, a caring
The lajlure ol investigators to distjnguisd between alcoholdependence and multiple-drug dependence in patienlswith ALD IS one of the reasons tor the variable relapserates after OLT.
Table 2 Percentage of Liver Transplant Patients in Whom the TransplantedOrgan Was Still Functional at 1. 3, and 5 Years After the Procedure,Listed According tc the Underlying Causes of the Patient's Liver Disease
Underlying Cause ofthe Liver Disease
Hepatitis C virus (HCV) infectionAlcoholic liver disease (ALD)Acute hepatic necrosis*Other postnecrotic' causesPrimary sclerosing cholangitis*Primary biliary cirrhosis*ALD + HCV infectionMetabolic diseaseAutoimmune* liver disease
Number ofPatients
9,5256,5273,5463,5003,4693,3452,4021,9581,381
Liver cancer (hepatocellular carcinoma) 1,187All Causes 46,940
1-Year
77,377.166,972,783,080,379,877,378.868.174.5
Survival (%)3-Year
67,568,959,463,877,875.567.971.671.551,267.4
5-Year
61,060,854,256,674,171,361,767,366,037,562.7
'Necrosis Is tissue death occurring \n groups at cells; cholangltls Is an Inflammation of the bile diicts: biliarycirrhosis is an inflammation of the liver resulting when bile How through small ducts in the liver is obstructed;autoimmune diseases are those conditions in which the body's Immune system erroneously attacks the body'sown ceils,SOURCE; United Network tor Organ Sharing (UNOS) registry. 1988-2001, Public data from UNOS/OPTNscientific registry (http://www.unos,org). Accessed December 2002,
264 ALCOHOL RESEARCH & HEALTH

LIVER TRANSPLANTATION FOR ALCOHOLIC LIVER DISEASE
PREDICTORS OF RELAPSE IN PATIENTS WITH ALCOHOLIC LIVER
DISEASE FOLLOWING LIVER TRANSPLANTATION
Psychiatric comorbiditySocial instabilityPrior rehabilitation attemptsLack of involvement with other activities
Poor self-imageAssociated chronic illnessAbuse of more than one drugLack of coordinated care
relationship with another person, asource of hope or improved self-esteem,and negative behavioral reinforcementfor subsequent drinking (e.g., the devel-opment of acute pancreatitis). Whenat least two of these factors are present,the patient is likely to remain abstinentfor 3 t)r more years. If none of these factorsor only one of them applies, the patientis likely to relapse within 2 years.
Individual transplant centers alsoassess long-term abstinence amongtheir patients. Based on their findings,UNOS developed the following guide-lines for considering individual alcoholicpatients for liver transplantation {UNOS1996; Vaillant 1995):
• A few months of sobriety as a testof short-tetm compliance (UNOSdoes not require a 6-month periodot abstinence).
• Presence of a supportive sociiil net-work at home.
• Absence of comorbid risk factors.
• A clinical impression that the patienthas been compliant in the past.
Some transplant centers have usedcontingency contracting as a method toimprove long-term abstinence (DiMartiniet al. 2002). With this approach, thepatient and the center enter a formalagreement that specifies the consequencesof certain actions of both parties. Nosttidies to date have assessed the efficacyof this strategy, however.
Several investigators have proposedadditional risk factors for an alcoholrelapse (also see the textbox). A studyby Platz and colleagues (2000) suggested
that these risk factors include beingfemale, having a poor social environ-ment, having poor personal stability asassessed by a psychologist, and com-pleting less than 6 months of absti-nence. DiMartini and colleagues(2001) identified a history of otherdrug use, a family history of alcoholism,and previous experience with alco-holism treatment as risk factors associ-ated with a higher incidence of alcoholrelapse. These investigators did notfind any relationship between a priorpsychiatric disorder and abstinence at6 months after the transplant.
Types of Liver Damage During anAlcohol Relapse
Although it is not necessary to take atissue sample (i.e., biopsy} of the liverto make a diagnosis of recurrent AL.Din patients who have relapsed to alcoholuse, researchers have examined changesin liver structure (i,e., histologiail changes)that occur in these patients. Theseanalyses found that the bistological fea-tures of rectirrent ALD that affect thetransplanted liver are similar to thoseof ALD in the native liver (Lee 1997).The major histological changes seenwith recurring ALD in transplantpatients are steatosis, which is foundin 83 percent; steatosis accompaniedby inflammation (i.e., steatohepatitis),found in 10 percent of cases; flbrosis incertain areas of the liver, which occursin 28 percent of patients; and cirrhosis,found in 23 percent of patients. Otherless commonly seen changes includeenlarged mitochondria"' in 14 percentof cases, excess levels of iron (i.e.,siderosis) in the liver cells in 24 percentof cases, and interruption of the bile
flow within the liver. These changes arenot specific for ALD, and the physiciantherefore must exclude the presence ofother diseases (e.g., viral infection).
MANAGEMENT OE ALCOHOLICPATIENTS AFTER AN O L T
With the exception of patients who aredependent on other drugs in additionto alcohol, ALD patients do not have ahigher incidence than non-ALD patientsof pre- or postoperative psychiatricproblems that would necessitate addi-tional treatment (Howard and Fahy1997). However, ALD patients at highrisk for relapse should be followed closely,and regular psychiatric followup shouldbe considered in such cases.
To date, no controlled studies haveevaluated specific treatment methodsfor managing relapse after liver trans-plantation. The alcoholism treatmentapproaches used in the general popula-tion are probably applicable to thesepatients as well, with close monitoringby the tnmsplant psychiatrist/psychologistand physician. Several studies havedemonstrated that the involvement ofa transplant psychiatrist or psychologistboth before and after OLT reduces thealcohol relapse rate after transplantation(Lucey et al. 1992; Berlakovich et al.1994,2000).
Several investigators have attemptedto study the effectiveness of motiva-tion;il enhancement therapy in patientswho relapse after liver transplantation(DjMartini et al. 2002). The resultsof such studies are unclear, however,because few patients enroll in thesestudies and because other problems areassociated with the care of such patients.
Another approach to achievingabstinence in alcoholic patients,administering the medication disulfi-ram, which serves to deter people fromdrinking by causing unpleasant effectswhen combined with alcohol, is notrecommended in patients after OLTbecause distilfiram has toxic effects onthe liver.
The mitochondria are membrane-enclosed componentsof the cell that are responsible tor most ot ihe cell's energyproduction.
VOL. 27, No. 3, 2003 265

ETHICAL ISSUES ASSOCIATEDWITH O L T FOR A L D PATIENTS
Although most people In the popula-tion consume alcohol at least occasion-ally, alcoholism and the diseases causedby it continue to carry a stigma amongthe general public. This is true particu-larly for ALD, and no other alcohol-induced organ damage is viewed sonegatively. Many people have a biasagainst liver transplants in alcoholics,resulting at least in part from the contin-ued organ shortage and ever-increasingdemand for donor organs, which neces-sitates rationing of the donor organs.For example, some people considerALD a self-inflicted disease and there-fore propose that ALD patients havelower priority on transplant waiting lists.This attitude is reflected in an opinionpoll conducted in Great Britain, whichshowed that both the general publicand family physicians believed thatalcoholic patients should have a lowerpriority than others for OLT (Neubergeret al. 1998). Similar results were reportedin Oregon, where the gencnil publicwas asked to allocate priorities for 714disorders or treatments. The respon-dents rated the priority of OLT fornon-ALD patients at a moderate level(364 out of 714), but gave a very lowpriority (695/714) to OLT for ALD(McMaster 2000). Transplant psychia-trists and psychologists, however, havea more favorable opinion on OLT foralcoholics. For example, in a survey ofthese health care professionals from 14academic liver transplant centers in theUnited States, a consensus favored offer-ing further alcoholism treatment topatients who continued to use alcoholrather than refusing OLT outright(Snyderetal. 1996).
Re.searchers and clinicians originallythought that ALD patients would havepoorer graB: and patient survival ratesthan non-ALD patients, but such a dif-ference has never been documented.Neither has the assumption of highrelapse rates in ALD patients been con-firmed. Relapse rates following OLTare lower than in patients undergoingalcoholism treatment, and seriousrelapses that adversely affect the trans-planted liver or the patient are uncom-
mon (see table 1). In contrast, patientswho receive OLT because of an infec-tion with hepatitis B or C virusesalways experience disease recurrenceand have an increased likelihood oflosing the transplanted liver primarilybecause of this recurrence. Anotherconcern, that patients with ALD wouldnot be able to comply with the anti-rejection medication regimen, also hasnot been confirmed. Graft-rejectionrates are similar for patients trans-planted for ALD and those trans-planted for other types of liver disease,which indicates comparable rates ofcompliance with the antirejection med-ications. Finally, it was anticipated thatALD patients would utilize moreresources, thereby incurring highercosts, than non-ALD patients, butagain this assumption never has beencorroborated by research evidence(Campbell and Lucey 1996).
In contrast to these negative assump-tions regarding the outcome of OLTin ALD patients, many clinicians arguethat ALD is an excellent indication forliver transplantation. For example, theoverall improvement in the status ofpatients with ALD after OLT, includ-ing the improvement in productivity,supports considering such patients forliver transplantation. Moreover, thelong-term costs of OLl and the subse-quent management of the alcoholicpatient probably are lower than thecosts of managing alcoholism and ALDwithout transplantation. This assump-tion is based on the observation thatonly 22 percent oi ;ill ;ilcohol-dependentpeople seek help within any 1-yearperiod, and fewer than one drug abuserin eight receives formal treatment foralcohol or other drug dependence(KeefFe 1997).
The suitability of ALD patients forOLT also must be considered in thecontext of the three principles of organand tissue allocation identified by UNOS(Ethics Committee, UNOS 1992). First,the principle of medical utility requireschat organs be allocated to those patientswho arc likely to experience the maximtimmedical benefit. This requirement iswell satisfied by patients with ALD.Second, the principle of justice requiresthat equal respect and concern be given
to all patients in need of an organ ortissue. This principle generates someethical questions regarding the potentialwastage of organs by transplantation inpatients who may "voluntarily" revertto alcoholism. Third, the principle ofautonomy requires that the personalchoices of the patients be respected. Inthis reg;ird, the UNOS Ethics Committeeholds the view that a person's pastbehavior (including alcohol consump-tion) should not be considered as anexclusion criterion for OLT.
There is no one-to-one correlationbetween alcoholism and ALD (Benjamin1997). Only a minority of alcoholicsdevelop ALD and may require OLT;conversely, many patients diagnosedwith ALD do not meet the criteria foralcoholism. However, the indiscriminatealloaition of a donor liver to an alcoholicwho may relapse and thus endanger thefunction of the transplanted organ isnot justifiable to the general public. Itis important to remember that the gen-eral public makes up the donor pooland may be discouraged from organdonation by a policy of equal trans-plantation for alcoholics and nonalco-holics. Thus, clinicians must make aneffort to identify' OLT candidates amongthe ALD patients who are at low riskfbr relapse. Moreover, additional educa-tion of the public is necessary to dis-place the stigma for OLT in alcoholicsand to increase organ donation.
FUTURE DIRECTIONS
Because outcome after liver transplan-tation, particularly the risk of relapse, issuch an important concern in patientswith ALD, identifying the factors thatcould indicate the most suitable candi-dates for OLT is a highly desirable goalof research (Li 1997). The following linesof inquiry show promise in this regard:
• Studies have identified genetic char-acteristics that infiuence alcoholintake. Additional in-depth analysesare needed to determine the specificinfiuences of these genes on thedevelopment of ALD or on the riskof alcohol relapse after OLT.
266 ALCOHOL RESEARCH *i HEALTH

LIVER TltANSPLANTATION FOR ALCOHOLIC LIVER DLSEASE
Genetic factors may determine apersons susceptibility to developingliver damage after alcohol consump-tion or to becoming alcohol depen-dent. Such possible hictors shouldbe investigated fiarthet, becausetransplanting a new liver might alteror negate the genetic influence. Forexample, a patient with a high sus-ceptibility to ALD might not be assusceptible to ALD aftet OLT evenif he or she returned to heavy drink-ing because the new liver would begoverned by its own set of genericfactors. Conversely, if genetic factorsdetermining alcohol metabolism bythe liver play a role in maintainingalcohol dependence, then OLl'might "cure" the addiction.
Researchers musr develop bettermeans of identifying ALD patientswho are at risk ot relapse after OLT.With bener identification methods,transplant centers could focus theirresources on this rather small gtotipof patients before OLT in an effortto prevent subsequent relapses.Furthermore, research assessing vari-ous treatment programs may iden-tify those approaches that bestimprove abstinence rates after OLF.
Currently no definite blood tests(i.e., biochemical markers) can iden-tify relapses after OL'F. Isolated ele-vations in a liver enzyme calledgamma-glutamyl transpeptidasewithout concomitant elevation ofanother enzyme, called alkalinephosphatase, may serve as a surro-gate marker of relapse (Pappo et al.1993). Further research directed atidentifying a marker that can indi-cate abstinence over a period of timewould be valuable for monitoringthe patients' drinking behaviorbefore and after OIT.
Investigators must further evaluatethe outcome of liver transplantationin patients with .severe alcoholichepatitis; currently these patientsrarely are considered for an OLT{because they usually do not haveenough time to prove sobriety).
CONCLUSIONS
OLT currently is the only definitivetreatment for liver failure, includingALD. Because of the shortage ofdonated organs, however, OLT inpatients with ALD remains controver-sial, mainly out of concerns that thetransplanted liver could be "wasted"on a patient who eventually relapses todrinking, thereby damaging the trans-planted liver. To address this concern,transplant centers generally perform amultidisciplinary screening procedurebefore the transplant to identify psy-chosocial predictors of relapse andselect suitable ALD patients for OLT.Fligher survival rates and lower relapserates than expected in ALD patientsafter OLT have encouraged manytran.splant centers to reevaluate theircriteria for these patients. As a result,many transplant centers currently donot require that ALD patients com-plete a 6-month abstinence periodbefore being placed on a transplant list.Nevertheless, future studies shouldfocus on identifying patients at risk forrelapse, so that preventive and thera-peutic interventions can be selectivelytargeted to these patients.
The ethical debate regarding the jus-tification of OLT in patients with ALDcontinues, although this subject is lesscontro\'ersial than in the past. Furthereducation of the public regarding theoutcomes of liver trajisplantation in ALDpatients should help eliminate the stigmaand misapprehensions associated withALD in the context of OLT and couldincrease organ donation rates. I
REFERENCES
ANAND, A . C ; FERRAZ-NETO, B.H.; NlGHTlNGALt,
P.; K r Al, Livcr transplantation for alcoholic liverdisease: Evaliidtioii of a seleccion protocol. Hepa-to%2'>;1478-14S4, 1997.
BH.1.AMV, C O . ; DIMARTINI, A . M . ; Ri.'1'i'l-Rr, K.;v:\ M.. Liver rransplaniation for alcoholic cirrhosis:[.onf;-term follow-up and impact ot disease retiir-renie. inutifhntation 72:619-626, 2001.
BENJAMIN, M . Transplantation for alcoholic liverdisease: The ethical issues. Liver Tramplamatwn.S'M/gfjj 3:337-342, 1997.
eds. Liver Transplantation and the Alcoholic Patient:Medical. Surgical and I'sychosocial hsues. Canibridge.United Kingdom: C]aniL>ridge University Press,l')94. pp. 6-28.
, T.P. Predictive factors for alcoholicrelapse- in the seleciion of alcohol-dependent pet-sons for hepatic transplant. Liner Transplantationand Surgery y2%Q~l'n. 1997.
BERESFORD, T.P., AND EvHRSON, G.T. Liver trans-plantation for alcoholic liver disease: Bias, beliefs,6-month rule, and relapse—hut where ate the data?Liver 'Transptamatwn 6:777-778, 2000.
, T.P.;Ti;Ra">Tn-;,J.G.; MI-RION, R.; I TAL. A rational approach to Ijver transplantation for thealcoholic patient./'.rjf/w^owi/to 31:24I-2M, 1990.
BERRSFORD,T.P.; Wii.soN, D.; Blow. F.C; trF Ai. Thfshort-term psychological health of alcoholic and rion-iiicoholic livet transplant recipients. jAkvholism: Clinicaland ExperimmCiJ R/^earch 16:996-1000, 1992,
BKRIAKOVTCH, GA.; SlElNlNCHR, R.; HtRBSr, F.;FT Al. Efficacy of liver transplantation for alcoholiccirrhosis with respect to recidivism and compliance.Transplancaiion'}S:'>(tO-'i(>5. 1994.
BERLAKOVICH, GA.; IJNCIRR, F.; FRF.UN'nORFF,R,
F..; F I AL. General compliance afcet liver transplan-tation for alcoholic cirrhosis. Transplantationhiternatwiuil 13:129-135, 2000.
BiRii, G.L.: O'GiiAFJY, J.G.: HARVI.Y F.A.; i:r AI..Liver transplantation in patients with alcoholic cir-rhosis: Selection criteria and rates of survival andrelapse, British Jounial of Medicine iQ\:\^-\7, 1990.
BRAVATA, D . M , ; OLKIN, I.; BAIINAIO, A.E.; fi' AL.
Lmplojtnent and alcohol use after liver transplantationfor alcoholic and nonalcoholic liver disease: A system-atic review. Liver Transplantation 7:1^^^-20^, 2001.
CA.MI'BF.I.I., n.A., JR., AND LUCEY, M . R . Liver
transplantation for alcoholic cirrhosis. In: Bmuuil.R.W., and Klintmalm, G.B,, eds. Transplantationof the Liver. Ist cd. Philadelphia: W.B. Satindets,1996, pp. \45-\'>(.l
GAMI'IIH.1., D A , JR., AMI PUNCH, J . D , Monitoring
for alcohol use relapse after livet transplantation foralcoholic liver disease. Liver Transplantation and.Surgeiy 3:300-303, 1997.
COFFMAN, K.L.; HllFFMAN, A.; SiHER, L.; ETAL.IVeacment of the postoperative alcoholic liver
transplant recipient with other addictions. LiverTransplantation and Surgejy 3:,^22-327. i 997.
DIMARTINI, A.: MA(;II.L. J.; FFi/ciERAin. M.G.; ET
AL. Use ot a high-risk alcohol relapse scale in evalu-ating livcr transplant candidates. Alcoholism: ClinicalandKxpenmernalResearch24:1198-120]. 2Q0U.
DIMARFINI, A.; DAY, N . ; DEW, M.A.; F:I AL.
Alcohol use following liver transplantation. A com-parison of follow-up methods. Psychosomatics42:55-62,2001-
). T.P. Overt and covert alcoholism. In:l.iicev, M.R.; Merion, R.M.; and Beresfotii, T.P.;
I, A ; WLINRILIi, R.; AND FiRFMAN, M.Liver transplantation in patients with alcohol andother stihstance use disorders. Psychiatric Clinics ofNorth America 25:195-209, 2002.
Vol.. 27, No. 3, 2003

Rchics Commirtt'L', United Network fot OrganSharing. General principles tor allocating humanorgans anii tissues. Tramplamatioii Proceedings24:2227-2235,1992.
EVKRHART, J.H,. AN[> Bl̂ RKSRlRI), T.P. Liver trans-plantation tor alcoholic liver disease: A survey oftransplantation programs in the United States. LiverTransplantation and Surgery 3:220-226, 1997.
Ll->:. R.G. Recurrence of alcoholic liver disease afterliver transplantation. Liver Transplantation and
3:292-295, 1997.
. C ; BiiAKAiWAi, C ; HOUSE. R.; h r . u .Long-term follow-up of patients with alcoholic liverdiiease who underwent hepatic transplantation.Liver TrampLintaiion and Surgery y.lGh—27A, 1997.
FABREGA, E,; CREiK"), J,; CASAKINT, F.: E-T AI..
Alcoholic recidivism after liver transplantation foralcoholic cirrhosis.ywcTM/o/Ci'M/ra/
olog^ 26:204-206, 1998.
FO.STI:R, P.F.; FABR!:C]A, F.; KAR.Ant;MiR, S,; K r AI ,
Prediction of abstinence from ethanol in alcoholicrecipients following liver transplantation. Hepatnlijg^25:1469-1477. 1997.
FULLER, R.IC Definition and diagnosis ol relapse todrinking. Liver Transplantation and Surgery 3:258-262, 1997.
GERHARDT, T.G.; GoLDiirLiN, R.M.; UILSCHLL,
H.G.; E'l'AL. Alcohol use following liver transplan-tation for alcoholic cirrhosis. Transplantation62:1060-1063, 1996.
GLSH. R.G.: LEE, A.H.; KEFJFE, E.B.; KT AI . Liver
transplantation for patients with alcoholism andend-stage liver disease. American Journal ofGastroenterolog)> SS:\5i7-] 542. 1993.
, R.; TRIPP, L ; GLEM.VION.S, J.; tJ AL.
Liver transplantation for alcoholic cirrhosis: Do theymix? Transplant Proceeding 2'^:\\3\-ll52, 1993,
GRAN I , B.F., AND THOMAS, C. Prevalence of
L^SM-IV alcohol abuse and dependence. UnitedStates, 1992. Alcohol Health & Research World18:243-248, 1994.
HOOFNAGLH, J,H,; KRESINA. T . ; Fui.l.tR. R.K.; ETAL. Liver transplantation for alcoholic liver disease:Executive statement and recommendations. LiverTransplantation and Surgery 3:347-350. 1997.
HoWARn, L., AND FAHY, T . Liver transplantationfor alcoholic liver disease. British Journal ofPsychiatry 171:497-500, 1997.
HOWARD. L.; FAHV, T . : W O N G , I',; FT AL. Psychiatric
outcome in alcoholic liver transplant patients.Quarterly Journal of Medicine 87:731 -773. 1994.
KEEFFE, E.B, Oamorbidities of alcoholic liver dis-ease that affect outcome of orthotopic liver trans-plantation. Liver Transplantation and Surgery.3:251-257. 1997.
KNECHTLE. S J . ; FLEMING. M.F.: BARRV, K,L, : LT
AL. Liver transplantation for alcoholic liver disease,Surgeiy 112:694-703. 1992.
KUMAR. ,S,; STAUBKR. R.E.; GAVALLR. J.S.; ET AL.
Orthotopic liver transplantation for alcoholic liverdisease. Hepatology 11:159-164. 1990.
L[, T. Research direction. Liver Transplantation
afidSurgery i:296-29% 1997.
LUGtY, M,R. Liver transplantation in the aJcoholicpatient. In: Maddrey. W,C.; SchifF, E.R.; and Sorrell.M,F,: eds. Transplantation of the Liver, 3d ed. Phila-delphia: l.ippincott Williams & Wilkins. 2001. pp.319-326.
I,u<:i Y. M,R, Is liver transplantation an appropriatetreatment for acute alcoholic hspmna? Journal ofHepa!ologyi6:829-S5l. 2002.
LL:I::EY, M , R , ; MtmoN, R,M,; HENLEY, K,S,; EV M..
Selection for and outcome ofliver transplantationin alcoholic liver disease. Gastroenterology 102:1736-1741. 1992,
LUCI£V, M.R.; C-UIR, K.; BLREiiURL), T.P.; tT At.,Alcohol use after liver transplantation in alcoholics—Clinical-cohort tollow-up study, LLepatolog^ 25:1223-1227,1997.
MATOS, C ; PORAVKU. M.K.; FRANt:i.SCX)-ZiLI.ER.
N,; AND DlCECCO. S, Nutrition and chronic liverdisease. Journal of Clinical Ciostroenterolagy 35:.39I-.397, 2002."
Mc:Cutl.C)yGH, A.J. Alcoholic liver disease. In:Schiff. E,R.; Sorrell M.F.; and Maddre)' W.C; eds.Schiff's Diseases of the Liver, 8th ed. Philadelphia:l.ippincott Williams & Wilkins, 1999. pp. 941-971.
MCMASIER, P. Transplantation for alcoholic liverdisease in an era of organ shortage. Lancet 355:424-425, 2000,
NFL'BERGER, J.; ADAMS, D . : MCMASTER, P.; ET AL.
Assessing priorities for allocation ot donor livergrafts: Stirvcy of public and clinicians. BritishMedical Journal 3\7:\72-\75. 1998.
NF.UHERCER, J, : SCHUIJ'., K.H,; DAY, C ; ET AL.
Transplantation for alcoholic liver disease. Journallo^My.\30-\37, 2002.
OSORIO, R,W.; ASCHFR. N.L; AVKRY. M,: FT AL.Predicting recidivism after orthotopic liver trans-plantation for alcoholic liver disease. Hepatology20:105-110. 1994.
PAGFAUX, G , P , ; MICHEL..].; Gosr t . V.; EI.AL.
Alcoholic cirrhosis is a good indication for livertransplantation, even for cases of recidivism. Gut45:421^26. 1999.
, O . ; RAMOS, H . ; STAR7.L, T.E.; ET AL.
Structural integrity and identification of causes ofliver allograft dysfunction occurring more than 5years after transplantation. American Journal ofSurgical Patholo^ 19:192-206, 1995.
PtRF.iRA. S.P.; HOWARD. L.M.; MUIESAN. P.; E['AI,.
Quality of life after liver transplantation for alco-holic liver disease, LJver Transplantation 6:762-768, 2000.
Pi.iLRS, M.G., AND TERRAULT, N . A , Alcohol useand hepatitis C. Hepatology 36:S220-S225, 2002.
PlATZ, K.; MURLL.FR, A.R.; Sl'REE, E.: ET AL. Livertransplantation for alcoholic cirrhosis. TransplantationInternational 13:S 127-S130, 2000,
RAAKOW, R.; LANGRL'HR, | . M . : ROHMANN, R.; L-T
AL. Is orthotopic liver transplantation for end-stagealcoholic cirrhosis justified? Transplant L'roceedings27:1241-1242,1995,
RouiLLARD, S., AND L\NE, N.E. Hepatic osteo-dystrophy. //f;wroi:;gy 33:301-307, 2001.
SNYDER, S.L.; DROOKER. M . ; AND STRAIN. J.J, A
survey estimate of academic liver transplant teams'selection practices for alcohol-de pen dent applicants.Psychosommcs 37:432^37. 1996.
STAR/X. T.E.; VAN THIEL. D. ; TZ.-VKIS. A.G.; ET AL.
Orthotopic liver transplantation for alcoholic QVT-T\\OSIS. JAMA: Journal of the American MedicalAssociation 260:2542-2544, 1988.
S1T.FAN1N1, G,F.; BlSF.LL,l. M.; GRAZI, G ,L , ; ETTAL.Orthotopic liver transplantation for alcoholic liverdisease: Rates of sur\'ival. complications and relapse.Hepatogastroenterology 44:1356-1360, 1997,
Sn-.VF,NS, L: PIPER, J.; EMOND, J.: ET At., Livertransplantation for ciiniroversial indications: Alco-holic liver disease, hepatic cancers and viral hepati-tis. Transplant Proceeding 23:1915-1916,1991.
STICKF.L,. F,: SCHLTPAN, D. ; HAHN. E.G.; ANL^
SFITZ. H , K , Gocarcinogenic effects of alcohol inhepatocarcinogencsis. G'at51:132-139, 2002.
TANC;, H . ; BOLTTON, R.; GUNSON, B.; ET AL.
Patterns of alcohol consumption after liver trans-plantation. G«i 43:140-145, 1998.
TRINGAIJ, R.A.; TRZF.PACZ, P , T , : DIMARTINI. A.;
AND DFW, M . A . Assessment and follow-up ofalcohol-dependent liver transplantation patients.A ciimcal cohort. General Hospital PsychiatryI8:7OS-77S, 1996.
United Network for Organ Sharing (UNOS). Policyand hy-iaw proposals. Richmond, VA: UNOS, 1996.
United Network for Organ Sharing (UNOS). Publicdata ftom UNOS/OPTN scientific registty. AccessedDecember 2002. Available at http://www, unos.org.
, G . E . The Natural History of AlcoholismRemsited Cambridge, MA: Harvard Utiiversiry. 1995,
WF.TNRIEB. R.M.; VAN HORN, D.H.A.; MCILELLAN.
A.T.: AND LUCEY, M . R . Interpreting the signifi-cance of drinking by alcohol-dependent liver trans-plant patients: Fostering candor is the key to recov-ery. Liver Transplantation 6:769-776. 2000.
WODAK, A.D.; SALINDERS, J.B.; EWL'SI-MENSAH, I.;
ET AI. Severity of alcohol dependence in patients withalcoholic liver disease. British Medical Journal (ClinicalResearch Edition) 287(6403):1420-1422. 1983.
YATF.,S, W , R , ; MARTIN, M. ; L.ABRECQUF. D. ; FT AI.,
A model to examine the validit)' ot the 6-monthabstinence criterion for liver transplantation.Alcoholism: Clinical and Experimental Research22:513-517, 1998,
ZiRARi. G.B.; EDWIN, D . : WALI , L.: Er AL. Livertransplantation for alcoholic liver disease. ClinicalTransplant 10:76-79. 1996.
ALCOHOL RESEARCH & HEALTH