Non alcoholic fatty liver disease(NAFLD)
52
NON ALCOHOLIC FATTY LIVER DISEASSE DR BHAVIN MANDOWARA
-
Upload
bhavin-mandowara -
Category
Health & Medicine
-
view
84 -
download
1
Transcript of Non alcoholic fatty liver disease(NAFLD)
NON ALCOHOLIC FATTY LIVER DISEASSEDR BHAVIN MANDOWARA
OUTLINE OF PRESENTATION
INTRODUCTION AND DEFINITIONS PATHOGENESIS AND RISK FACTORS DIAGNOSIS PROGNOSIS AND COMPLICATIONS MANAGEMENT SUMMARY
INTRODUCTION Most common among all Liver disorders & the cause of CLD Commonest cause of asymptomatic abnormal LFTs Most common cause of End stage liver disease requiring liver
transplantation Present in 75% of the individuals with Obesity and Type 2DM NAFLD exists as a spectrum from simple steatosis to cirrhosis Hepatic steatosis describes accumulation of fat >5% of liver
weight Commonest cause of death in patients with NAFLD, NAFL and NASH
is cardiovascular disease.
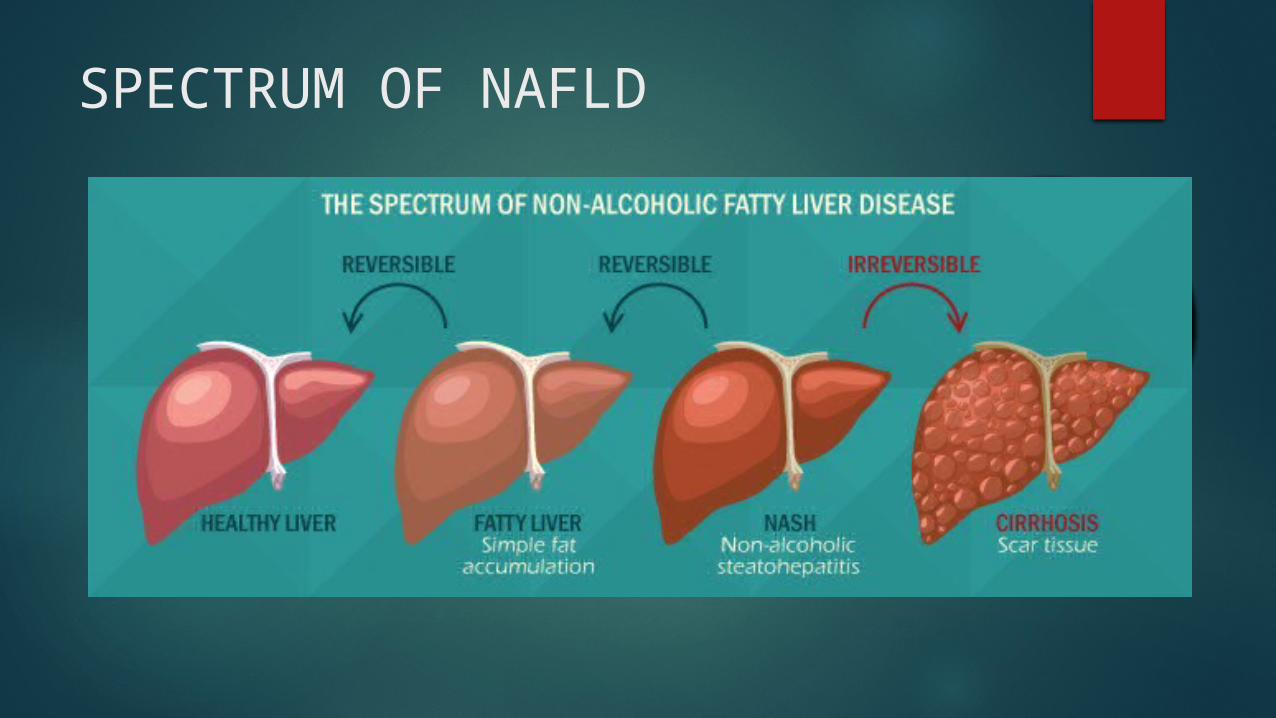
SPECTRUM OF NAFLD
AM
ERIC
AN
ASSO
CA
ITION
OF G
ASTR
OEN
TER
OLO
GY
, 2012 JUN
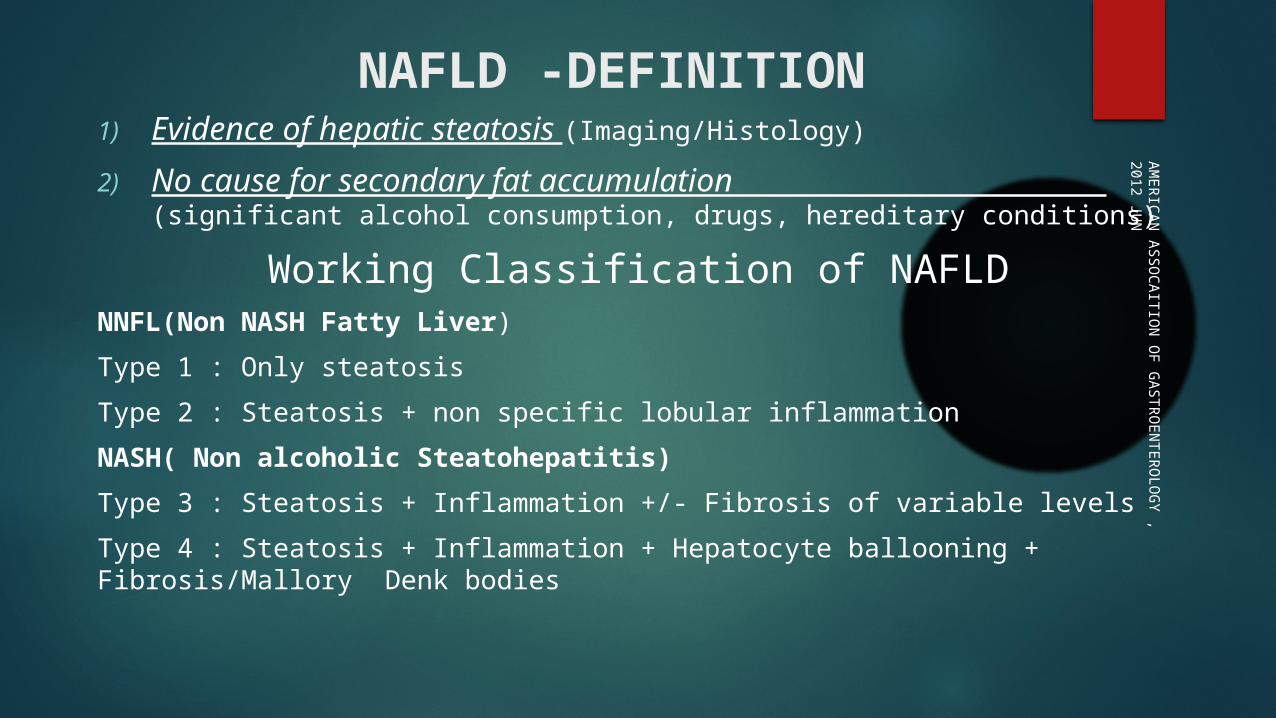
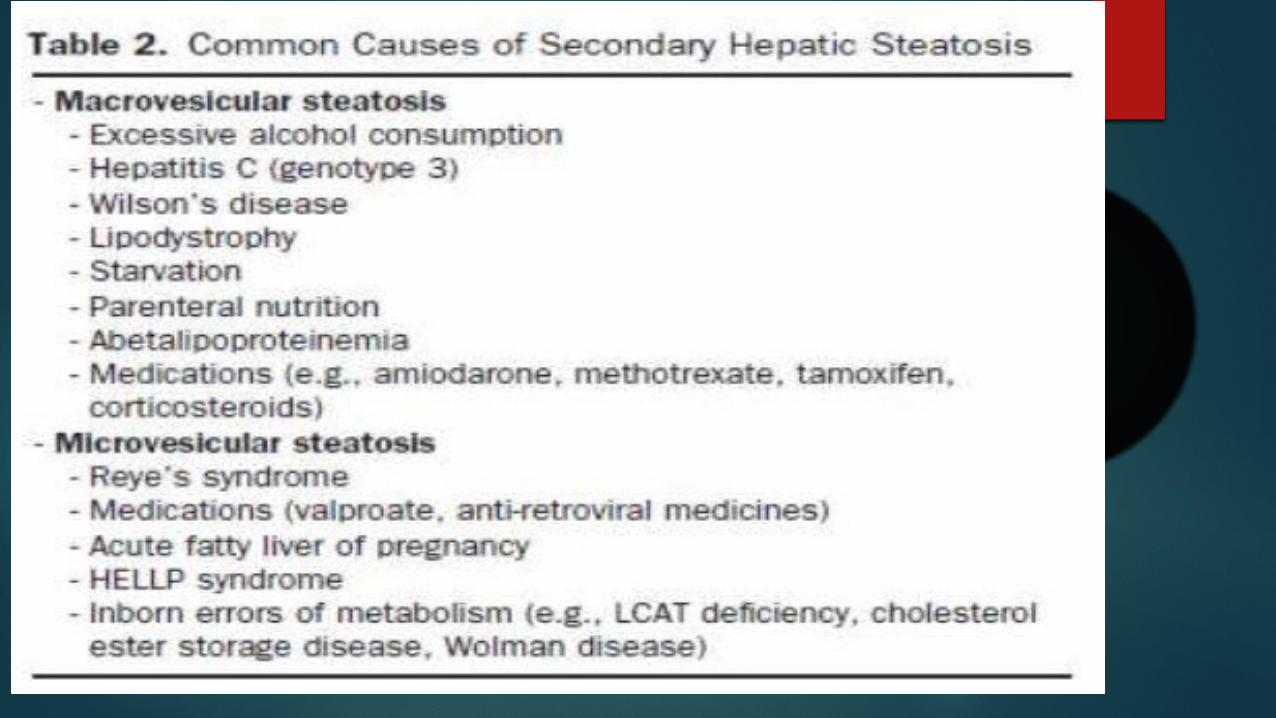
NAFLD -DEFINITION1) Evidence of hepatic steatosis (Imaging/Histology)2) No cause for secondary fat accumulation
(significant alcohol consumption, drugs, hereditary conditions)
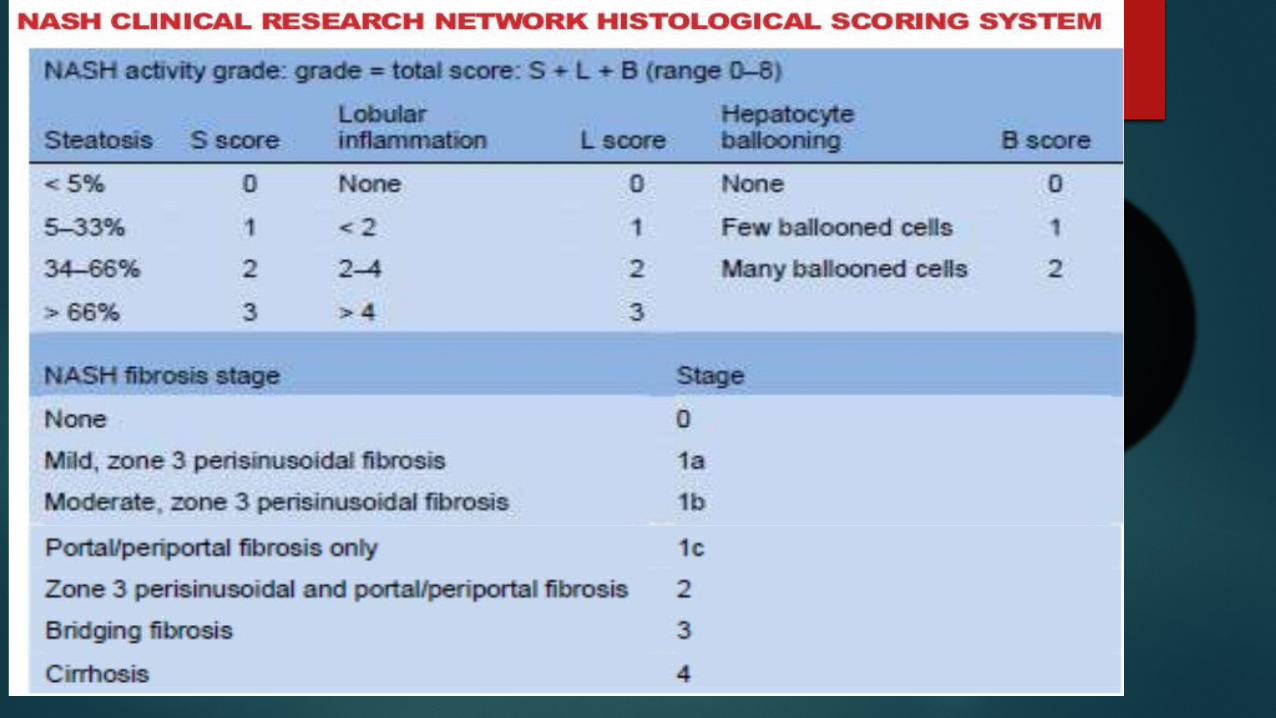
Working Classification of NAFLDNNFL(Non NASH Fatty Liver) Type 1 : Only steatosisType 2 : Steatosis + non specific lobular inflammationNASH( Non alcoholic Steatohepatitis)Type 3 : Steatosis + Inflammation +/- Fibrosis of variable levelsType 4 : Steatosis + Inflammation + Hepatocyte ballooning + Fibrosis/Mallory Denk bodies
Nonalcoholic Fatty Liver Disease and related definitionsNonalcoholic Fatty Liver Disease (NAFLD) Encompasses the entire spectrum of fatty liver disease in individuals without significant alcohol consumption, ranging from fatty liver to steatohepatitis and cirrhosis.
Nonalcoholic Fatty Liver (NAFL) Presence of hepatic steatosis with no evidence of hepatocellular injury in the form of ballooning of the hepatocytes or no evidence of fibrosis. The risk of progression to cirrhosis and liver failure is minimal.
Nonalcoholic steatohepatitis (NASH) Presence of hepatic steatosis and inflammation with hepatocyte injury (ballooning) with or without fibrosis. This can progress to cirrhosis, liver failure and rarely liver cancer.
NASH Cirrhosis Presence of cirrhosis with current or previous histological evidence of steatosis or steatohepatitis
Cryptogenic Cirrhosis Presence of cirrhosis with no obvious etiology. Patients with cryptogenic cirrhosis are heavily enriched with metabolic risk factors such as obesity and metabolic syndrome.
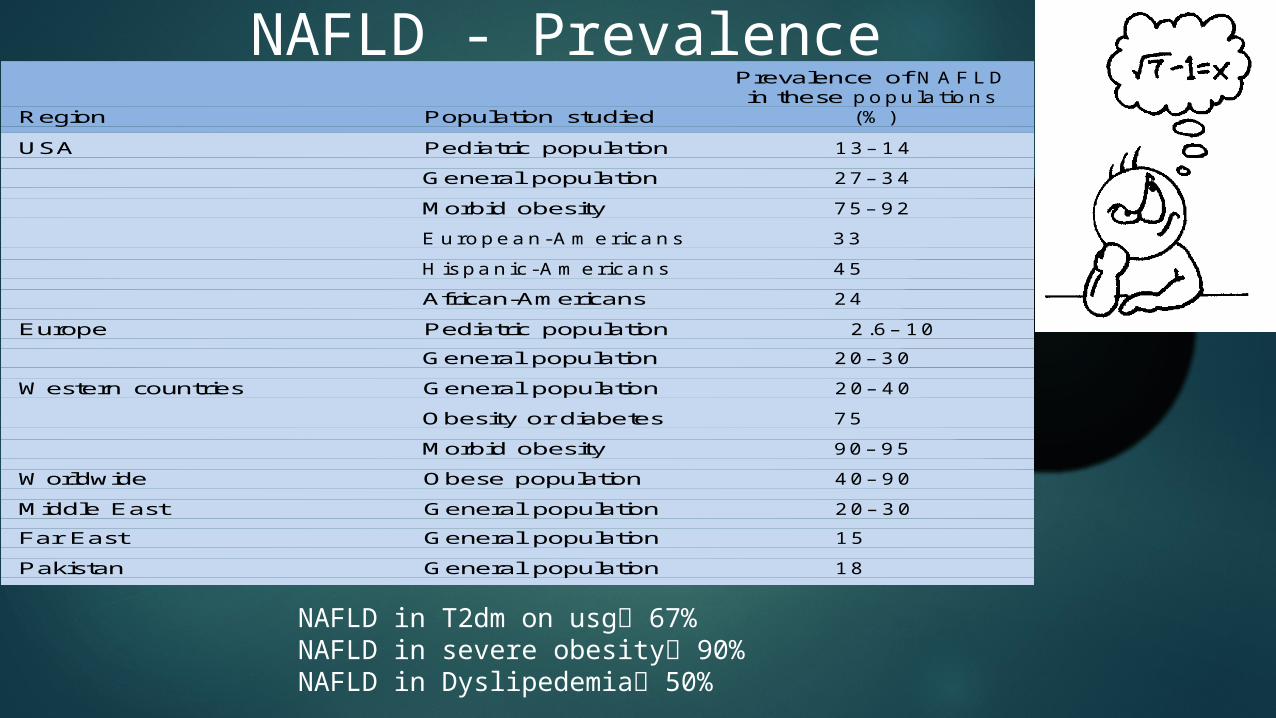
NAFLD - PrevalencePrevalence of N A FL D in these po pu la tio n s
Region Population studied (% )
USA Pediatric population 13–1 4
General population 27–3 4
Morbid obesity 75–92
E u ro p e a n -A m e rica n s 33
H is pa n ic -A m eric an s 4 5
African-Americans 24
Europe Pediatric population 2 .6– 10
General population 20–3 0
Western countries General population 20–4 0
Obesity or diabetes 75
Morbid obesity 90–95
Worldwide Obese population 40–9 0
Middle East General population 20–3 0
Far East General population 15
Pakistan General population 18
NAFLD in T2dm on usg 67%NAFLD in severe obesity 90%NAFLD in Dyslipedemia 50%
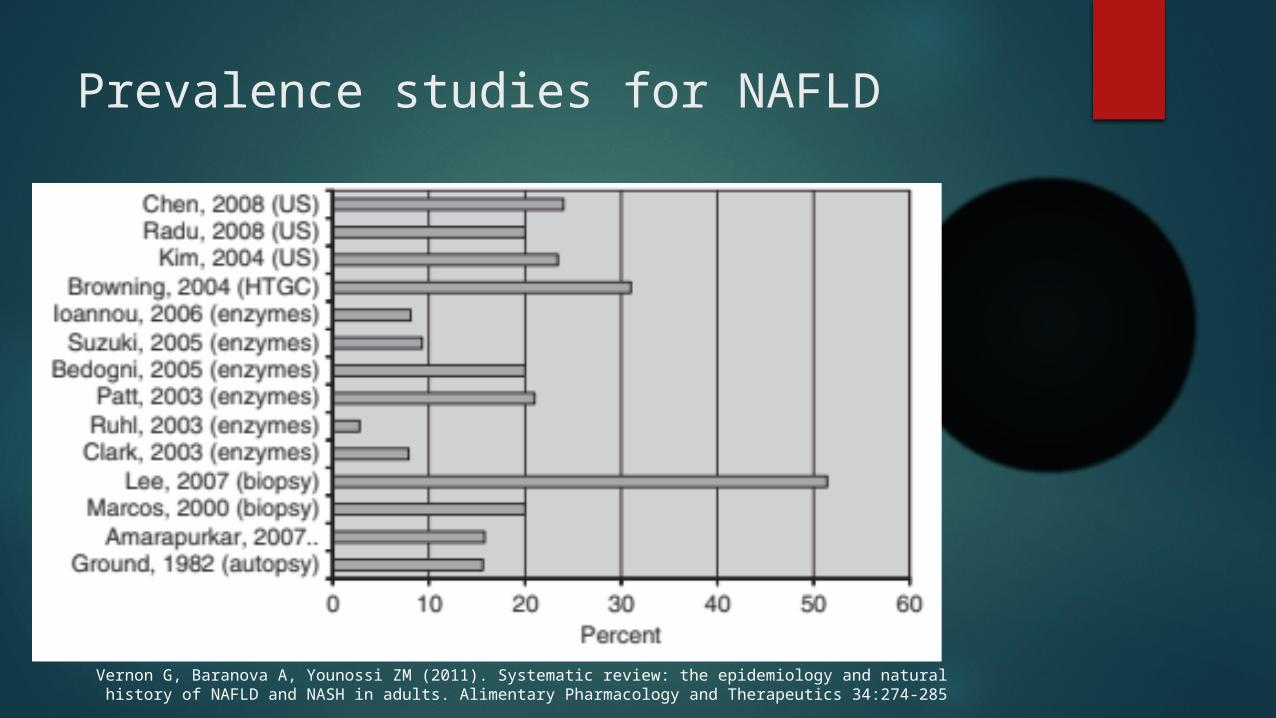
Vernon G, Baranova A, Younossi ZM (2011). Systematic review: the epidemiology and natural history of NAFLD and NASH in adults. Alimentary Pharmacology and Therapeutics 34:274-285
Prevalence studies for NAFLD
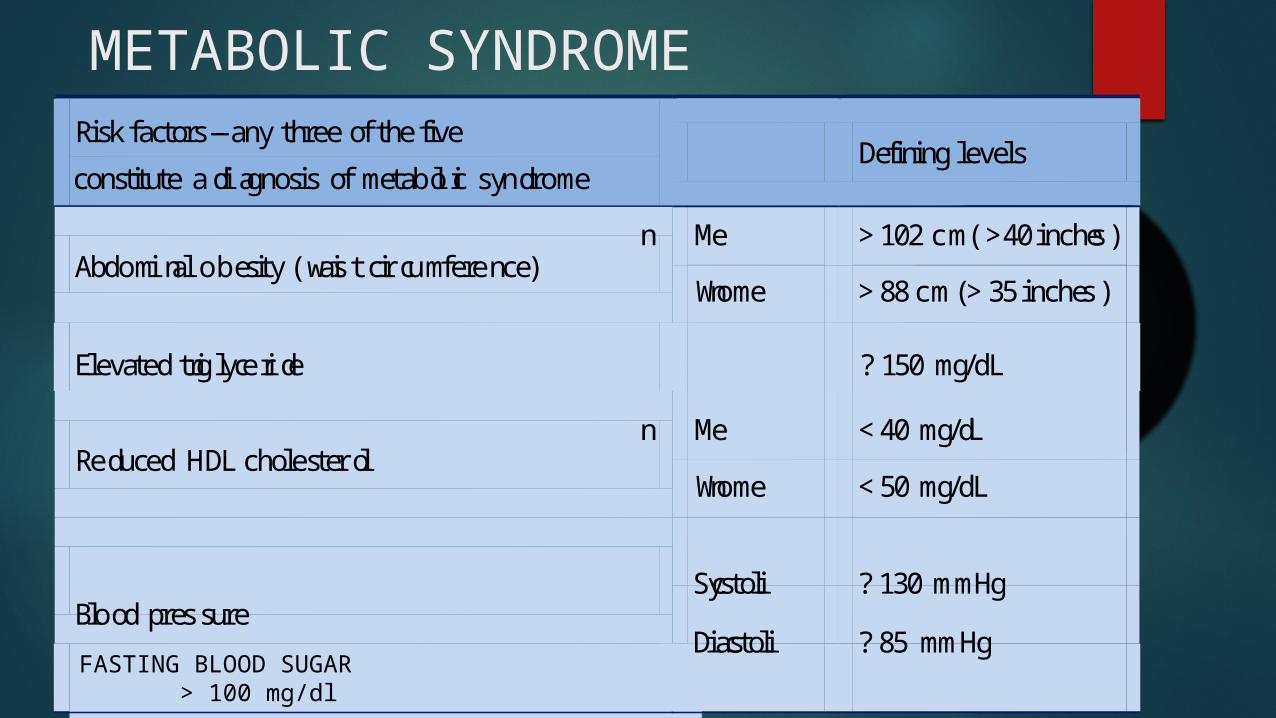
METABOLIC SYNDROME
FASTING BLOOD SUGAR > 100 mg/dl
Risk factors—any three of the five
constitute a diagnosis of metabolic syndrome
Abdominal obesity (waist circumference)
Defining levels
Men > 102 cm (> 40 inches)
Women > 88 cm (> 35 inches)
Elevated triglycerides ? 150 mg/dL
Reduced HDL cholesterol Men < 40 mg/dL
Women < 50 mg/dL
Blood pressure
Systolic ? 130 mmHg
Diastolic ? 85 mmHg
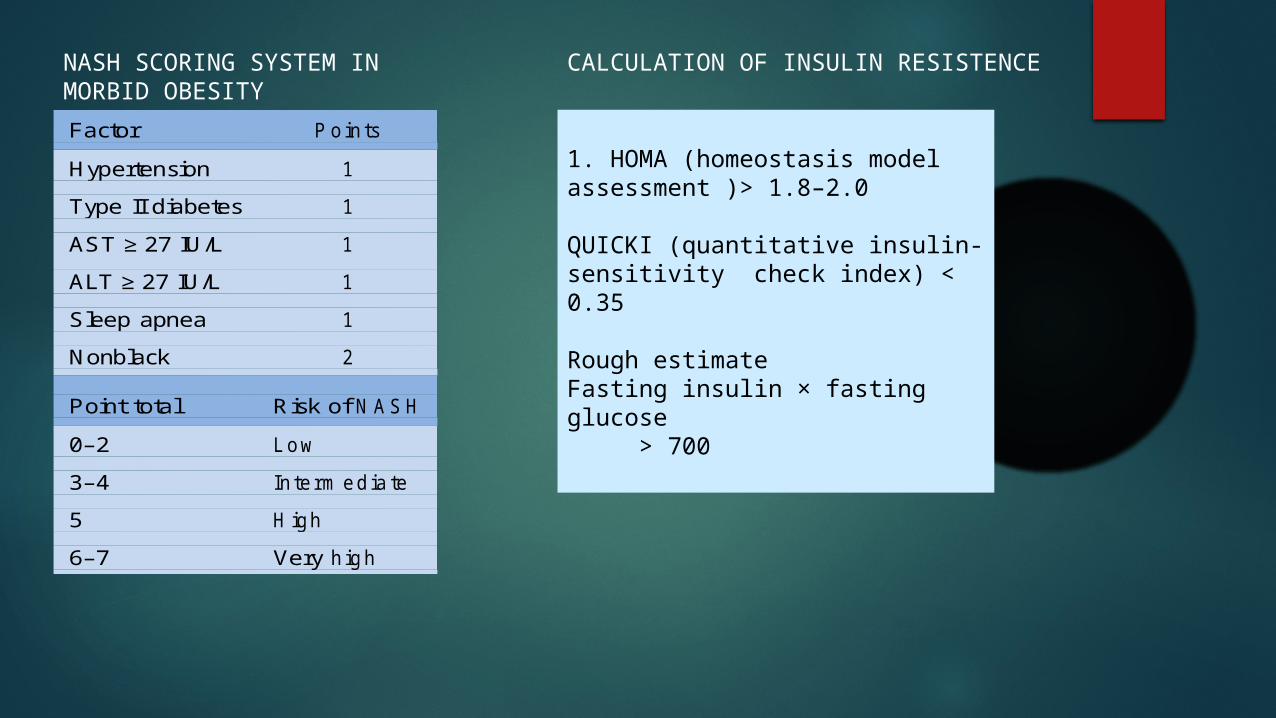
Factor P o in ts
Hypertension 1
Type II diabetes 1
AST ≥ 27 IU/L 1
ALT ≥ 27 IU/L 1
Sleep apnea 1
Nonblack 2
Point total Risk of N ASH
0–2 L ow
3–4 In te rm ed ia te
5 H igh
6–7 Very h ig h
1. HOMA (homeostasis model assessment )> 1.8–2.0
QUICKI (quantitative insulin-sensitivity check index) < 0.35
Rough estimateFasting insulin × fasting glucose > 700
NASH SCORING SYSTEM IN MORBID OBESITY
CALCULATION OF INSULIN RESISTENCE
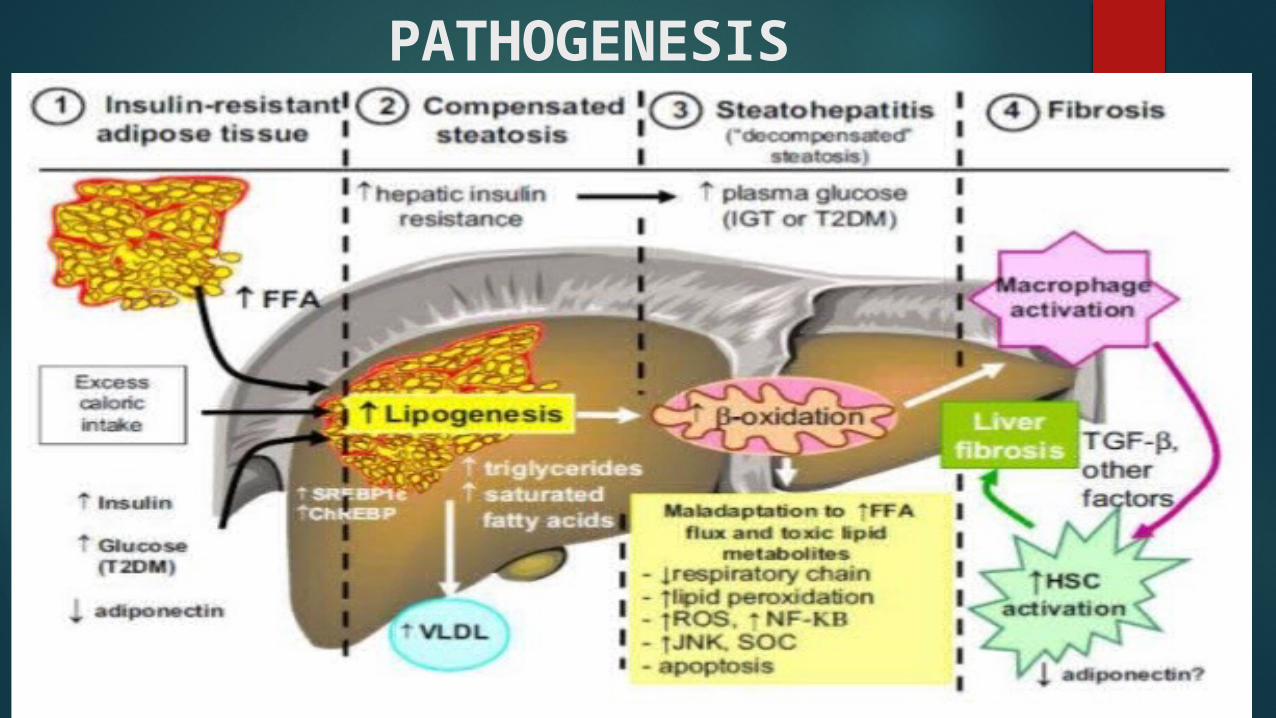
PATHOGENESIS
DIAGNOSISNAFLD/NASH is a diagnosis of exclusion, and liver biopsy will often be required to confirm the diagnosis, stage the disease, rule out other liver diseases, and determine the need for and urgency of aggressive therapy
DIAGNOSISWHEN TO SUSPECT NAFLD???
History : no symptoms ,fatigue, malaise and abdominal discomfort. The presence of any of the following, especially with a history
of abnormal AST/ALT, should lead to a work-up for NAFLD/NASH:1. Presence of obesity, especially morbid obesity (BMI > 35)2. Diagnosis of type 2 diabetes mellitus3. Diagnosis of metabolic syndrome4. History of obstructive sleep apnea5. Presence of insulin resistance 6. Chronic elevation of AST/ALT, otherwise unexplained
DIAGNOSIS Detailed patient history of alcohol consumption—
threshold < 20 g/day in women, < 30 g/day in men. Physical examination :1. Central obesity correlates with severity of inflammation
on biopsy2. dorsocervical lipohypertrophy (buffalo hump) correlates
with hepatocyte injury. 3. advanced liver disease: spider angiomas, ascites,
hepatomegaly, splenomegaly, palmar erythema, jaundice, hepatic encephalopathy.
DIAGNOSISLaboratory Tests Elevated ALT and AST: In 10% of NASH patients, ALT and AST may be normal, especially
with simple steatosis. An abnormal ferritin level in the presence of normal transferrin
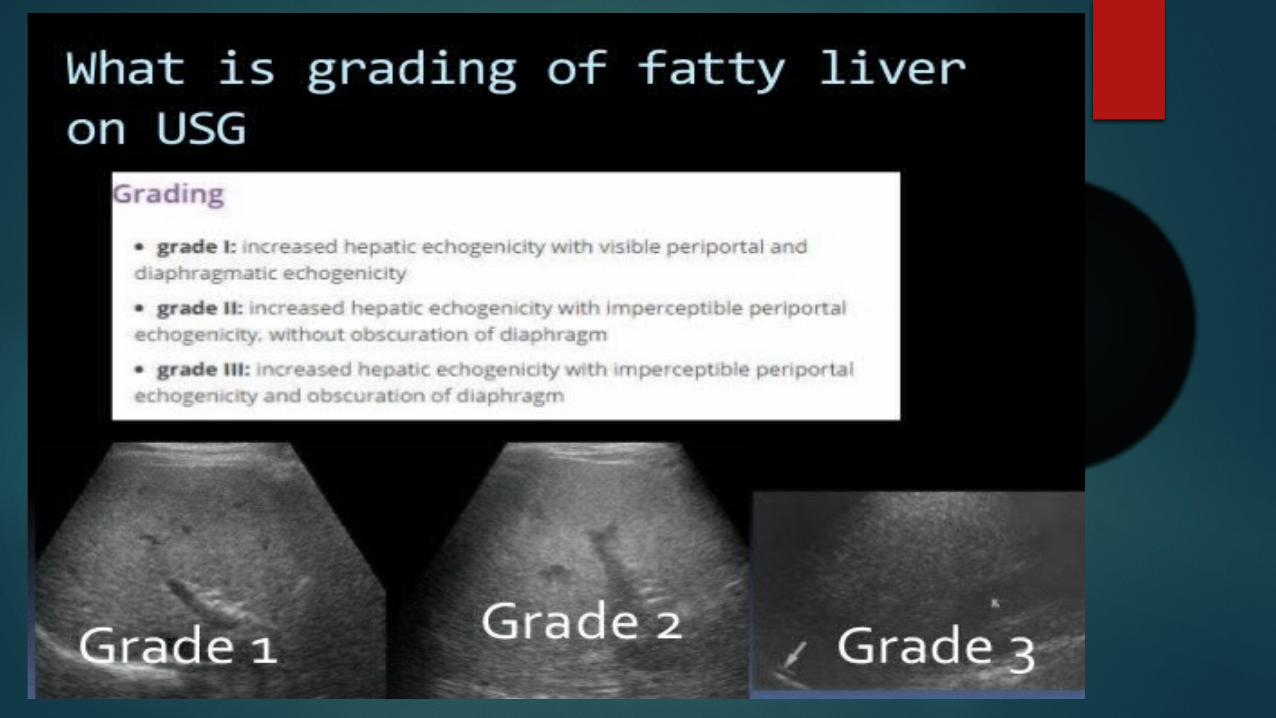
saturation should always suggest a need to rule out NASH. AST/ALT ratio < 1—this ratio is usually > 2 in alcoholic hepatitis.Imaging Tests Ultrasound is the usual screening test for fatty liver. The magnetic resonance imaging (MRI) test has a quantitative
value, but cannot distinguish between NASH and ASH. No imaging study can identify fat accurately if it is < 33% or
distinguish NASH from ASH.
Tests to exclude for diagnosis of NAFLD
Viral hepatitis—hepatitis B surface antigen, hepatitis C virus antibody or HCV- RNA, hepatitis A antibody IgM, hepatitis E antibody (in an appropriate geographical setting); it should be noted that the patient may have coexisting viral hepatitis as well as NAFLD/NASH.
Alcohol-related liver disease including alcoholic steatohepatitis. Autoimmune liver disease. Congenital causes of chronic liver disease: hereditary
hemochromatosis, Wilson’s disease, alpha-1-antitrypsin deficiency, polycystic ovary syndrome.
Drug-induced liver disease.
AASLD RECOMMENDATIONS When patients with unsuspected hepatic steatosis detected
on imaging have symptoms or signs attributable to liver disease or have abnormal liver biochemistries, they should be evaluated as though they have suspected NAFLD and worked-up accordingly. (1A)
In patients with unsuspected hepatic steatosis detected on imaging who lack any liver-related symptoms or signs and have normal liver biochemistries, it is reasonable to assess for metabolic risk factors (e.g., obesity, glucose intolerance, dyslipidemia) and alternate causes for hepatic steatosis such as significant alcohol consumption or medications. (1A)
In patients with unsuspected hepatic steatosis detected on imaging who are asymptomatic and have normal liver biochemistries, a liver biopsy cannot be recommended.(1B)
WHEN TO OBTAIN A LIVER BIOPSY?Liver Biopsy: “Gold standard” To grade and stage the disease, and to rule out other diagnoses in the presence of one or more of the following findings1. Abnormal serum ferritin in the absence of an elevated
transferrin saturation2. Cytopenia3. Splenomegaly4. Clinical signs of chronic liver disease5. Diabetes and abnormal persistently elevated AST/ALT
Obesity and age > 45 or abnormal AST/ALT 6. Unexplained hepatomegaly
WHEN TO OBTAIN A LIVER BIOPSY? AASLD RECCOMENDATIONS
Liver biopsy should be considered in patients with NAFLD who are at increased risk to have steatohepatitis and advanced fibrosis. (Strength – 1, Evidence - B)
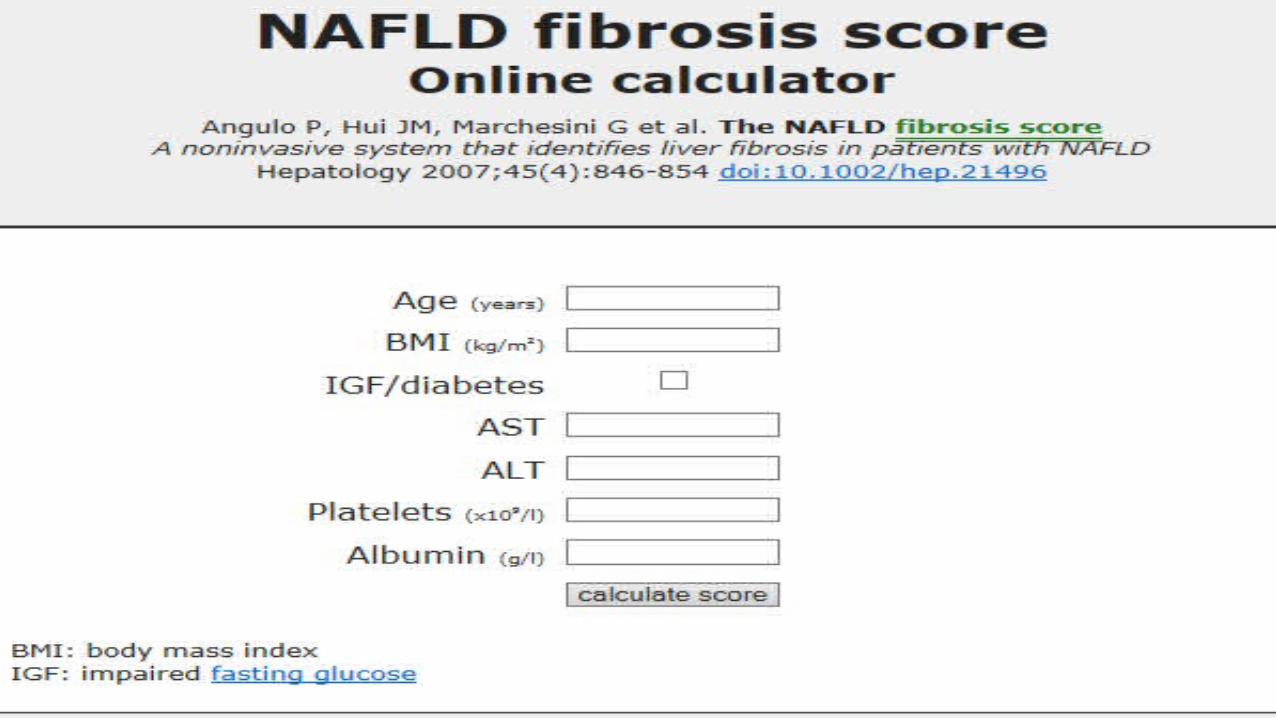
The presence of metabolic syndrome and the NAFLD Fibrosis Score may be used for identifying patients who are at risk for steatohepatitis and advanced fibrosis. (Strength – 1, Evidence - B)
Liver biopsy should be considered in patients with suspected NAFLD in whom competing etiologies for hepatic steatosis and co-existing chronic liver diseases cannot be excluded without a liver biopsy. (Strength – 1, Evidence - B)
NON-INVASIVE ASSESSMENT OF STEATOHEPATITIS AND ADVANCED FIBROSIS IN NAFLD
The NAFLD Fibrosis Score Enhanced Liver Fibrosis (ELF) panel Transient Elastography Circulating levels of cytokeratin-18 (CK18)
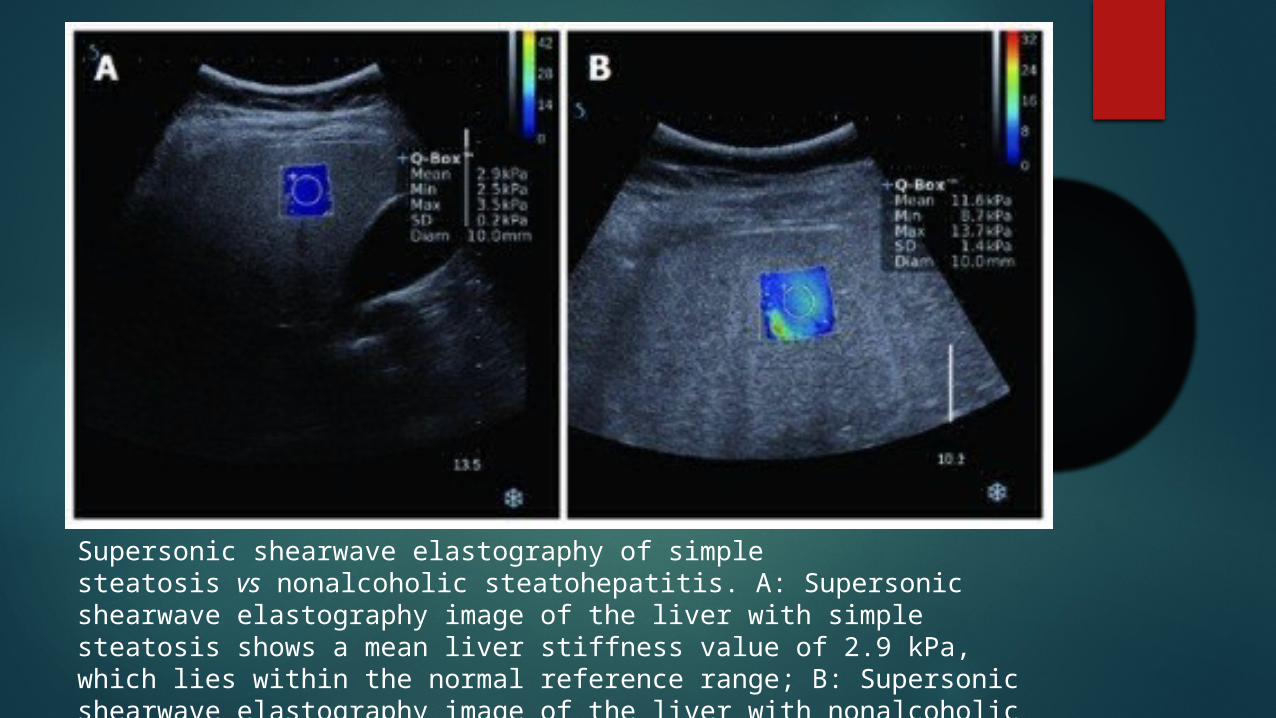
Supersonic shearwave elastography of simple steatosis vs nonalcoholic steatohepatitis. A: Supersonic shearwave elastography image of the liver with simple steatosis shows a mean liver stiffness value of 2.9 kPa, which lies within the normal reference range; B: Supersonic shearwave elastography image of the liver with nonalcoholic steatohepatitis shows an elevated mean liver stiffness value of 11.6 kPa.
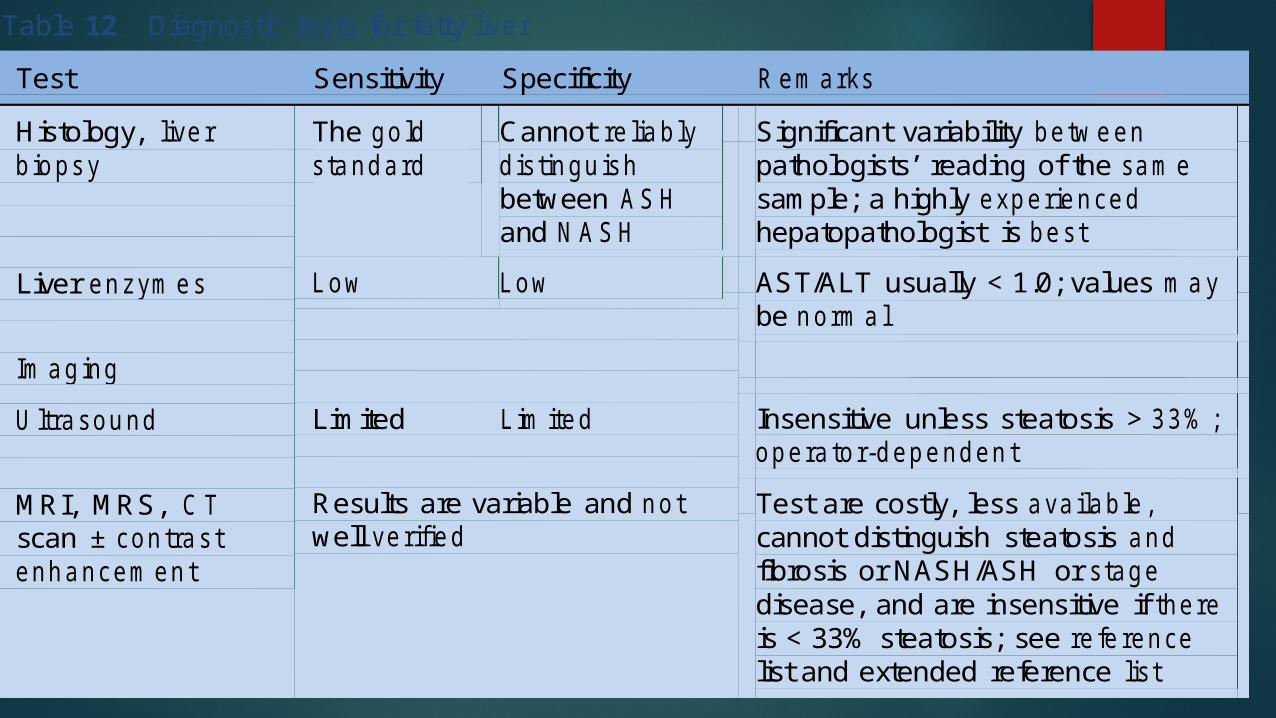
Table 12 Diagnostic tests for fatty live r
Test Sensitivity Specificity R em arks
Histology, live r b io ps y
Liver enzym es
Im ag ing
U ltrasou nd
MRI, MRS, C T scan ± con tra s t enha ncem en t
The go ld s ta nd ard
Cannot re lia b ly d is tin gu is h between A S H and N A S H
Significant variability be tw e en pathologists’ reading of the sam e sample; a highly exp erien ced hepatopathologist is be s t
L ow Low AST/ALT usually < 1.0; values m a y be n orm a l
Limited L im ited
Results are variable and no t well ve rifie d
Insensitive unless steatosis > 33% ; opera to r-d epe nden t
Test are costly, less a va ila b le , cannot distinguish steatosis a nd fibrosis or NASH/ASH or stage disease, and are insensitive if the re is < 33% steatosis; see re fe rence list and extended reference lis t
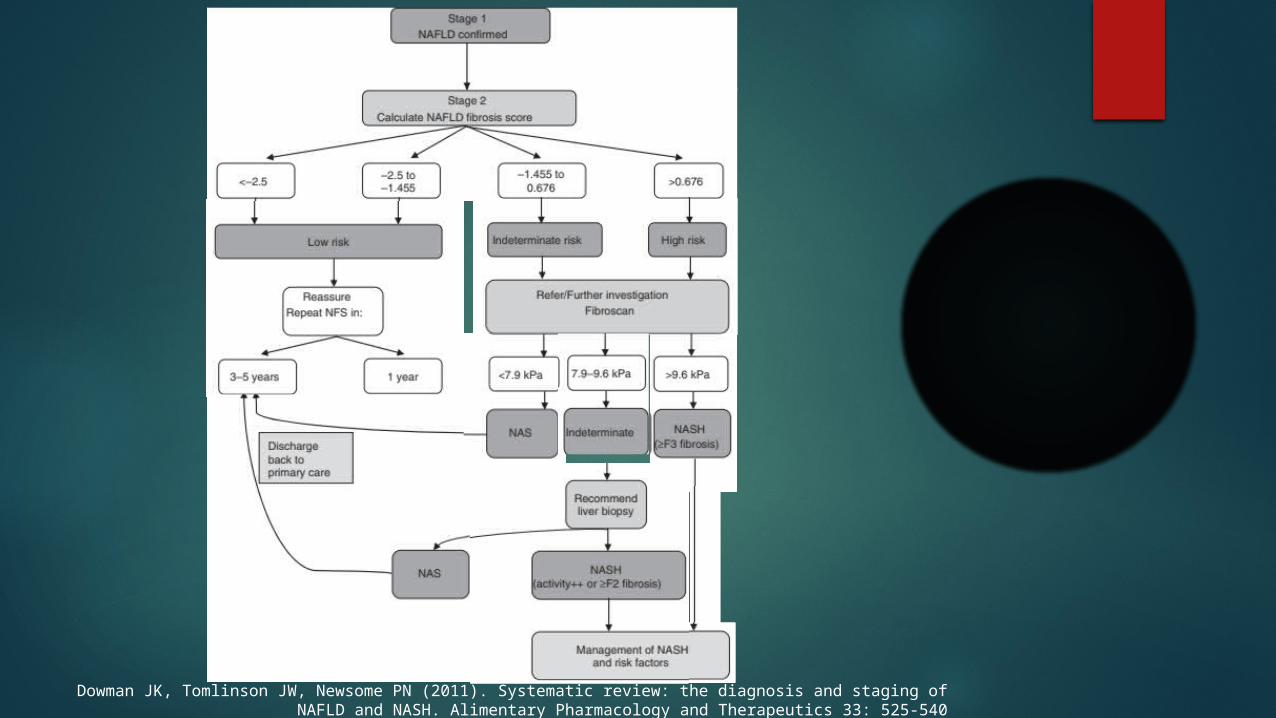
Dowman JK, Tomlinson JW, Newsome PN (2011). Systematic review: the diagnosis and staging of NAFLD and NASH. Alimentary Pharmacology and Therapeutics 33: 525-540
WH
O G
uidelines
WH
O guidelnies and U
ptodate
MANAGEMENT
Targets for therapy : insulin resistance and oxidative stress Goals of treatment: reduce the histologic features and improve
insulin resistance and liver enzyme levels. General Approach to the patient:1. Weight loss2. Vaccinations3. Treatment of risk factors for Cardiovascular diseases4. Avoid alcohol consumptions
AA
SLD guidelines and A
GA
1597
Lifestyle intervention
Weight loss generally reduces hepatic steatosis, achieved either by hypocaloric diet alone or in conjunction with increased physical activity. (Strength – 1, Evidence - A)
Loss of at least 3-5% of body weight appears necessary to improve steatosis, but a greater weight loss (up to 10%) may be needed to improve necroinflammation. (Strength – 1, Evidence - B)
Exercise alone in adults with NAFLD may reduce hepatic steatosis but its ability to improve other aspects of liver histology remains unknown. (Strength – 1, Evidence - B)
Avoid Fructose(Soda, canned products) its associated with liver fibrosis in NASH patients
Explain diagnosis and set realistic target weight Nutritional counselling – refer to dietician Exercise – 3-4 times per week, expend 400 kcal per session
AA
SLD 2012
Pharmacotherapy Metformin has no significant effect on liver histology and is not
recommended as a specific treatment for liver disease in adults with NASH. (Strength – 1, Evidence - A)
A recent meta analysis concluded that 6–12 months of metformin plus lifestyle intervention did not improve aminotransferases or liver histology, compared with lifestyle intervention alone, independently of metformin dose or the presence of diabetes. June 2012 AGA 1597
Uygun, et al A
liment Pharm
Ther 2004 *Nair, et al
Alim
ent Pharm Ther 2004 **R
atziu, et al Gastroent
erology 2008 ***Sanyal, et al NE J M
ed 2010
Pharmacotherapy Pioglitazone can be used to treat steatohepatitis in patients with
biopsy-proven NASH. However, it should be noted that majority of the patients who participated in clinical trials that investigated pioglitazone for NASH were non-diabetic and that long term safety and efficacy of pioglitazone in patients with NASH is not established. (Strength– 1, Evidence-B)
A recent meta-analysis that included 5 RCTs showed that pioglitazone significantly improved steatosis and inflammation but not fibrosis
Pioglitazone: weight gain, but significantly improved aminotransferases, steatosis, ballooning, and inflammation
Rosiglitazone: improved enzymes and steatosis, but not inflammation
Pharmacotherapy
PIVENS STUDY : Pioglitazone , Vitamin E, placebo 96 weeks Adults with NASH without DM, cirrhosis, Hep C, heart failure PIVEN CONCLUSIONS Vitamin E was superior to placebo in adults
with NASH and without DM Pioglitazone may have a role in treating patients with biopsy- proven NASH, however long term safety and efficacy has not been established
PHARMACOTHERAPY Oxidative stress is considered to be a key mechanism of
hepatocellular injury and disease progression in subjects with NASH
Vitamin E is an anti-oxidant and has been investigated to treat NASH the use of vitamin E is associated with a decrease in aminotransferases in subjects with NASH,
It causes improvement in steatosis, inflammation, and ballooning and resolution of steatohepatitis in adults with NASH
vitamin E has no effect on hepatic fibrosis.
AA
SLD 2012
PHARMACOTHERPAY(AASLD Recommendations) Vitamin E (a-tocopherol) administered at daily dose of
800 IU/day improves liver histology in non-diabetic adults with biopsy-proven NASH and therefore it should be considered as a first-line pharmacotherapy for this patient population. (Strength - 1, Quality - B)
Until further data supporting its effectiveness become available, vitamin E is not recommended to treat NASH in diabetic patients, NAFLD without liver biopsy, NASH cirrhosis, or cryptogenic cirrhosis (Strength - 1, Quality - C)
VITAMIN E
OTHER CONCERNS Meta-analysis* including 136,000 participants found
taking Vitamin E supplements > 400 IU/day had a higher risk of all cause mortality Vitamin E** > 400 IU/day increases risk of prostate cancer in relatively healthy men
*Miller et al Annals of Internal M
edicine 2005 ** Klein, et al, JAM
A 2011
AA
SLD 2012
PHARMACOTHERPAY (AASLD Recommendations)
It is premature to recommend omega-3 fatty acids for the specific treatment of NAFLD or NASH but they may be considered as the first line agents to treat hypertriglyceridemia in patients with NAFLD. (1B)
Foregut bariatric surgery is not contraindicated in otherwise eligible obese individuals with NAFLD or NASH (but without established cirrhosis). (1A)
The type, safety and efficacy of foregut bariatric surgery in otherwise eligible obese individuals with established cirrhosis due to NAFLD are not established. (1B)
It is premature to consider foregut bariatric surgery as an established option to specifically treat NASH (1B)
AA
SLD 2012
PHARMACOTHERPAY Given the lack of evidence to show that
patients with NAFLD and NASH are at increased risk for serious drug-induced liver injury from statins, statins can be used to treat dyslipidemia in patients with NAFLD and NASH. (Strength – 1, Quality – B) Why Statins? commonest cause of death is cardiovascular. Reduced rate of HCC and improvement in LFTs Statins are safe in liver disease(NAFLD)
AA
SLD 2012
NAFLD in patients with other chronic liver diseases
When steatosis and steatohepatitis are evident in patients with other types of chronic liver disease, it is important to assess for metabolic risk factors and alternate etiologies for hepatic steatosis. (Strength – 1, Quality – B)
In patients with other types of chronic liver diseases who have co-existing NAFLD and NASH, there are no data to support the use of vitamin E or pioglitazone to improve the liver disease. (Strength – 1, Quality – B)
AA
SLD 2012
Miscellaneous Recommendations Pertinent to Clinical Practice
Patients with NASH cirrhosis should be screened for gastro esophageal varices (1B)
Patients with NASH cirrhosis should be considered for HCC screening.(1B)
Current evidence does not support routinely repeating a liver biopsy in patients with NAFL or NASH. (2C)
NAFLD - Prognosis• Increased overall mortality
compared to matched control populations.
• Commonest cause of death in patients with NAFLD, NAFL and NASH is cardiovascular disease.
• Increased liver-related mortality rate – increasingly common indication for liver transplantation (15-20%).
Kawamura Y et al (2011). Large scale long term follow up study of Japanese patients with NAFLD for the onset of HCC. American Journal of Gastroenterology
World gastroenterology association
PROGNOSIS AND COMPLICATIONS NAFLD does not exacerbate hepatotoxicity, and side effects of
pharmacologic agents, including HMG-CoA reductase inhibitors, are not more likely to occur, NAFLD and coexistent obesity and related metabolic factors may exacerbate other liver diseases—e.g., alcoholic liver disease.
Concurrence of NAFLD with hepatitis C or human immunodeficiency virus.
(HIV) worsens their prognoses and decreases their responses to therapy. Hepatitis C, genotype 3, is commonly associated with hepatic steatosis,
which may confuse a diagnosis of hepatitis C vs. NASH vs. both together. Liver biopsy may indicate the severity of disease, but only fibrosis,
and not inflammation or necrosis, has been confirmed to predict the disease prognosis. Histologic progression to end-stage liver disease may occur: NASH + bridging fibrosis or cirrhosis.
World gastroenterology assocaition
PROGNOSIS AND COMPLICATIONS End-stage NASH is an often under-recognized cause of cryptogenic
cirrhosis; progressive fibrosis may be obscured by stable or improving steatosis and serologic features, especially in older NASH patients.
NASH-related (cryptogenic) cirrhosis increases the risk of hepatocellular carcinoma (HCC).
Causes of mortality in cirrhotic NASH patients:— Liver failure— Sepsis— Variceal hemorrhage— HCC— Cardiovascular disease
PROGNOSIS AND COMPLICATIONS Independent predictors for progression of fibrosis:— Age > 45–50— BMI > 28–30 kg/m2— Degree of insulin resistance— Diabetes— Hypertension Negative impact on NASH survival:— Diabetes and elevated serum alanine (ALT) and aspartate aminotransferase(AST)— Older age and presence of necrotic inflammation on initial liver biopsy
WO
RLD
GA
STRO
ENTER
OLO
GY
ASSO
CIATIO
N
SUMMARY NAFLD and NASH represent a major global public health
problem, which is pandemic and affects rich and poor countries alike.
There is insufficient evidence to justify screening for NASH/advanced liver disease in the general population.
The diagnosis should be sought in all patients who present with risk factors for NASH. Not all patients with risk factors will have NAFLD or NASH, and not all patients with NASH will have standard risk factors.
Not every person with fatty liver needs aggressive therapy. Diet and exercise should be instituted for all patients.
WO
RLD
GA
STRO
ENTER
OLO
GY
ASSO
CIATIO
N
SUMMARY Liver biopsy should be reserved for those patients who have
risk factors for NASH and/or other liver diseases. Patients with NASH or risk factors for NASH should first be treated
with diet and exercise. Vitamin E or pentoxifylline may be added in these patients. Experimental therapy should be considered only in appropriate hands and only in patients who fail to achieve a 5–10% weight reduction over 6 months–1 year of successful lifestyle changes.
Bariatric surgery should be considered in patients in whom the above approaches fail, and it should be performed before the patient becomes cirrhotic.
WO
RLD
GA
STRO
ENTER
OLO
GY
ASSO
CIATIO
N
SUMMARY Liver transplantation is successful in patients who meet
the criteria for liver failure, but NASH may recur after transplantation and is likely to be denied to patients with morbid obesity.
Ultimately, NAFLD and NASH are diagnoses of exclusion and require careful consideration of other diagnoses. Just as the clinician cannot diagnose NASH on the basis of clinical data alone, the pathologist can document the histological lesions of steatohepatitis, but cannot reliably distinguish those of nonalcoholic origin from those of alcoholic origin.
REFERENCES World Gastroenterology Organization Global Guidelines
Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis June 2012
The Diagnosis and Management of Non-alcoholic Fatty Liver Disease: Practice Guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology June 2012
AASLD PRACTICE GUIDELINE The Diagnosis and Management of Non-Alcoholic Fatty Liver Disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association 2012
UPTODATE , SHERLOCK’S

THANK YOU