
Life and death of helicobacter azadi
28
The life and death of Helicobacter pylori in stomach Davoud azadi
-
Upload
dedalosd -
Category
Health & Medicine
-
view
49 -
download
3
Transcript of Life and death of helicobacter azadi
The life and death of Helicobacter pylori
in stomach
Davoud azadi
Introduction
• Colonisation of the normal stomach has been achieved only
by Helicobacter spp., such as H.pylori, H. felis or H.
mustelae
• Gram negative, motile, microaerophilic, spiral shaped
organisms that dwell on the gastric surface and within the
gastric mucus
• They are found more frequently in the antrum than in the
fundus and often within antral glands
• grow between pH 6.0 and 8.5 and survive between pH 4.0
and 8.5 in the absence of urea

The gastric environment
• The pH of the gastric lumen:
median pH is 1.4 .The pH can fall to below 1.0 with acid
secretion at night
The pH at the gastric surface(neutral) is thought to be
significantly higher than in the lumen(pH:2)
The pH of the lumen of the fundic glands, is much lower, The
pH on the antral surface likely to be higher
HCO3 secretion is able to neutralise 10% of maximal acid
secretion.( gastric surface pH:6)
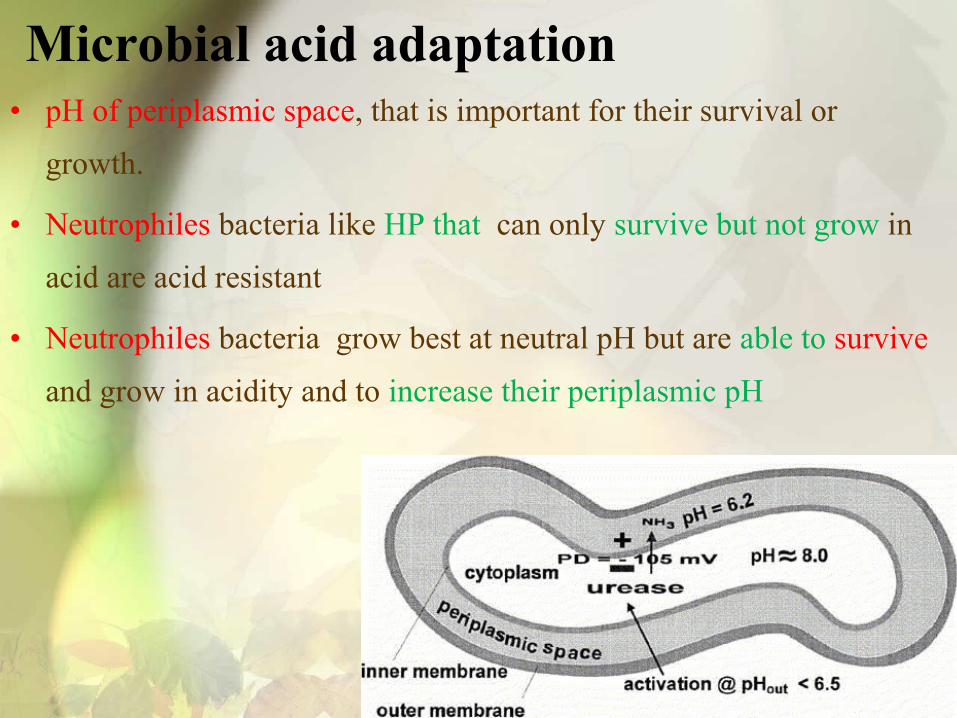
Microbial acid adaptation• pH of periplasmic space, that is important for their survival or
growth.
• Neutrophiles bacteria like HP that can only survive but not grow in
acid are acid resistant
• Neutrophiles bacteria grow best at neutral pH but are able to survive
and grow in acidity and to increase their periplasmic pH

1. All are designed to maintain a tolerable electrochemical
gradient of H+ across the inner membrane of these bacteria.
This can be achieved by alterations in transmembrane potential
lead to reducing the effective gradient
2. Acid tolerance can be achieved by the generation of neutralising
buffers either inside the cell or in the periplasmic space.
3. Many bacteria respond to acidity by changes in gene expression
of specialised proteins.

Molecular mechanisms of acid adaptation of Helicobacteria

STRUCTURAL ASPECTS OF MEMBRANE PROTEINS
• The outer membrane of Gram negative containing a variety of proteins
• some membrane spanning, porins are able to mediate the flux of various small molecules across the outer membrane.
• some associated with only one face(LPS)
STRUCTURAL ASPECTS OF MEMBRANE PROTEINS
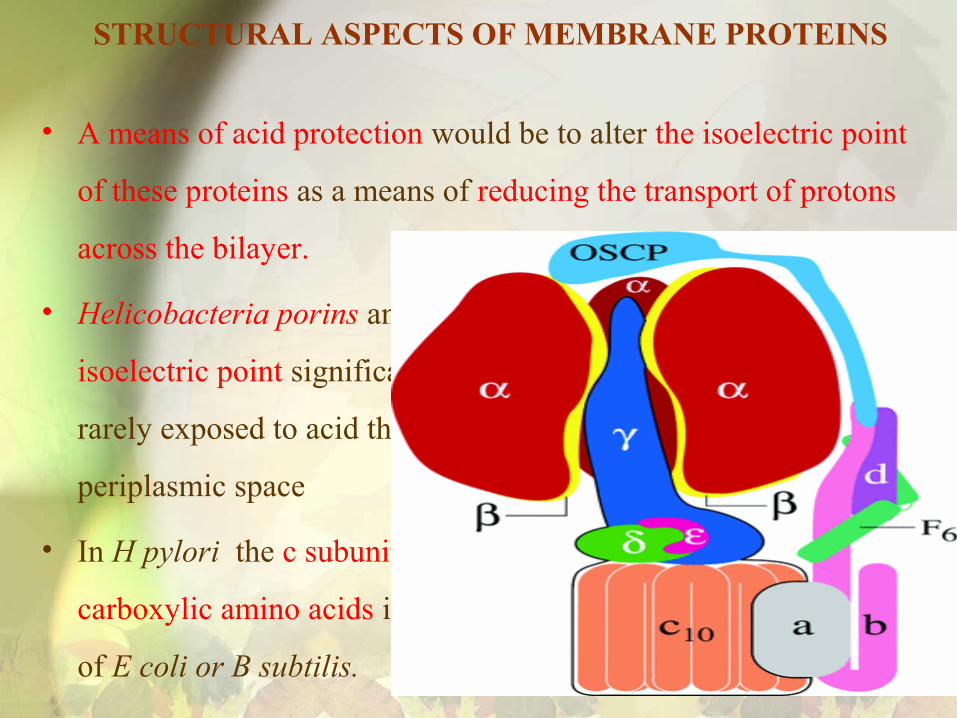
• A means of acid protection would be to alter the isoelectric point
of these proteins as a means of reducing the transport of protons
across the bilayer.
• Helicobacteria porins and some inner membrane proteins have an
isoelectric point significantly more alkaline than that of bacteria
rarely exposed to acid thereby retarding flux of protons into the
periplasmic space
• In H pylori the c subunit of the F1F0ATP synthase. loss of four
carboxylic amino acids in the sequence of the compared with that
of E coli or B subtilis.

• increase in isoelectric point suggests that both the outer and inner
membrane of the organism can be exposed to high acidity
• increase in numbers of positively charged amino acids or
decrease in the number of carboxylic acids in the membrane
proteins
• Helicobacter pylori use of this adaptive mechanism is acid
resistance when is exposed directly to luminal acidity.
• This mechanism provide transient protection. Thus other
mechanisms must be present to allow both long term survival
and growth in the gastric environment.
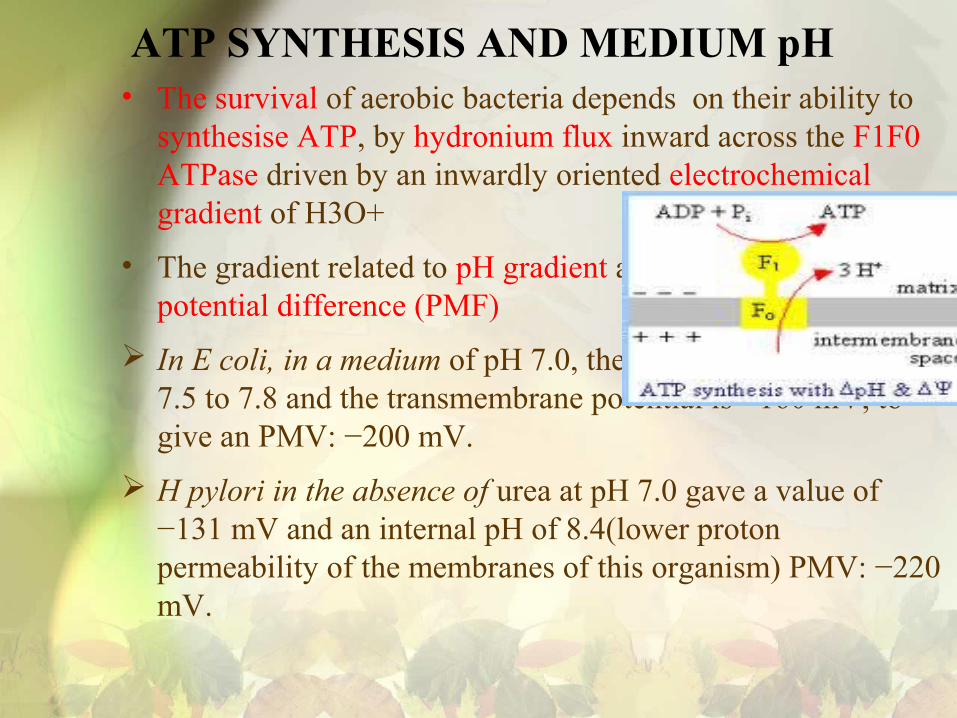
ATP SYNTHESIS AND MEDIUM pH• The survival of aerobic bacteria depends on their ability to
synthesise ATP, by hydronium flux inward across the F1F0 ATPase driven by an inwardly oriented electrochemical gradient of H3O+
• The gradient related to pH gradient and the transmembrane potential difference (PMF)
In E coli, in a medium of pH 7.0, the cytoplasmic pH is about 7.5 to 7.8 and the transmembrane potential is −160 mV, to give an PMV: −200 mV.
H pylori in the absence of urea at pH 7.0 gave a value of −131 mV and an internal pH of 8.4(lower proton permeability of the membranes of this organism) PMV: −220 mV.

• H.pylori is able to maintain a membrane potential between
pH 4.0 and 8.5. If the pH was outside these limits there was
a relatively rapid and irreversible loss of the membrane
potential
• The addition of urea restored the membrane potential
within about pH 3.5.
• Addition of urea at neutral pH in the absence of buffer
resulted in medium alkalinisation to a pH > 8.5
• Urease activity is a two edged sword for H pylori, enabling
survival in acid, preventing survival in the absence of acid

REGULATION OF PERIPLASMIC pH IN ACID
• Above mechanism that used by H pylori would not
ensure its survival in the stomach
• this organism is synthesis of a neutral pH with urease at
high concentrations.
• 15% of the protein synthesis is devoted to the production
of ure A or ure B.and active urease enzyme need Ni2−
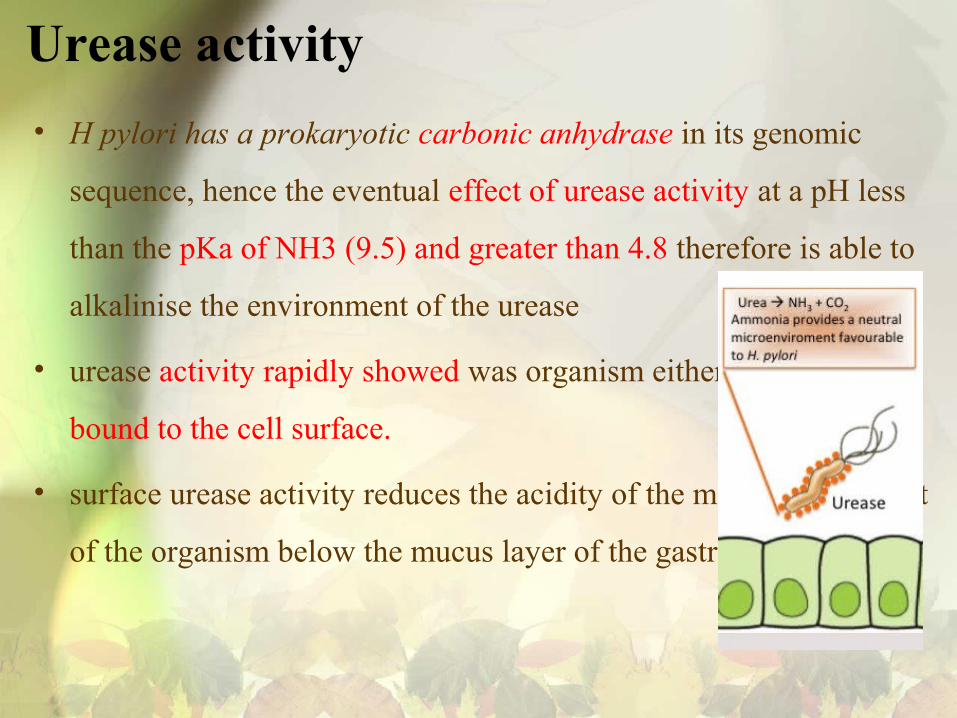
Urease activity
• H pylori has a prokaryotic carbonic anhydrase in its genomic
sequence, hence the eventual effect of urease activity at a pH less
than the pKa of NH3 (9.5) and greater than 4.8 therefore is able to
alkalinise the environment of the urease
• urease activity rapidly showed was organism either in solution or
bound to the cell surface.
• surface urease activity reduces the acidity of the microenvironment
of the organism below the mucus layer of the gastric mucosa

• H. pylori have two urease :internal urease and surface urease
• This microenvironment located external to the organism or in the
periplasmic space
• Internal urease was designated as the responsible urease
compartment, it was neutralisation of the external
microenvironment

Urease activity
• External urease activity low at pH > 6.5 At pH < 6.5, there is a
notable increase in urease activity(about 10-fold) reaching maximum
at pH 5.5 and remaining steady until pH 3.0
• internal urease is activated at a pH < 6.5 and cytoplasmic pH
remains steady
• 95% of the urease is found inside and not on the surface or outside
majority of the protein is found in the cytoplasm thus inaccessible
for immune system elements

• internal urease is responsible for acid protection
• The inner membrane potential of H pylori at fixed medium pH
between 3.0 and 6.0 rose to −105 mV with the addition of 5mM
urea,
• internal urease activity was responsible to periplasmic pH was
elevated to pH 6.2
• Addition of urea also enabled protein synthesis at a fixed medium
pH of 3.0 to 6.0 where normally no protein synthesis is found.

RESPONSE TO ELEVATED pH
• external urease is toxic at neutral pH
• ureas elevates medium pH to 8.5 or greater
resultant irreversible loss of membrane potential
and death
• This latter effect may explain the absence of H
pylori infection in pernicious anaemia
• H.pylori show no Internal urease activity at a pH >
6.5 prevents alkalinisation in the absence of acid.

• In summary, internal urease is active at a gastric
pH of < 6.5 and enables survival and growth at pH
between perhaps 2.0 and 6.0 depending on the
gastric urea concentration
• urea concentrations for effective internal enzyme
activity is about 1 mM
• External urease does not function as a
gastroprotective mechanism but reducing the
immune response in the gut


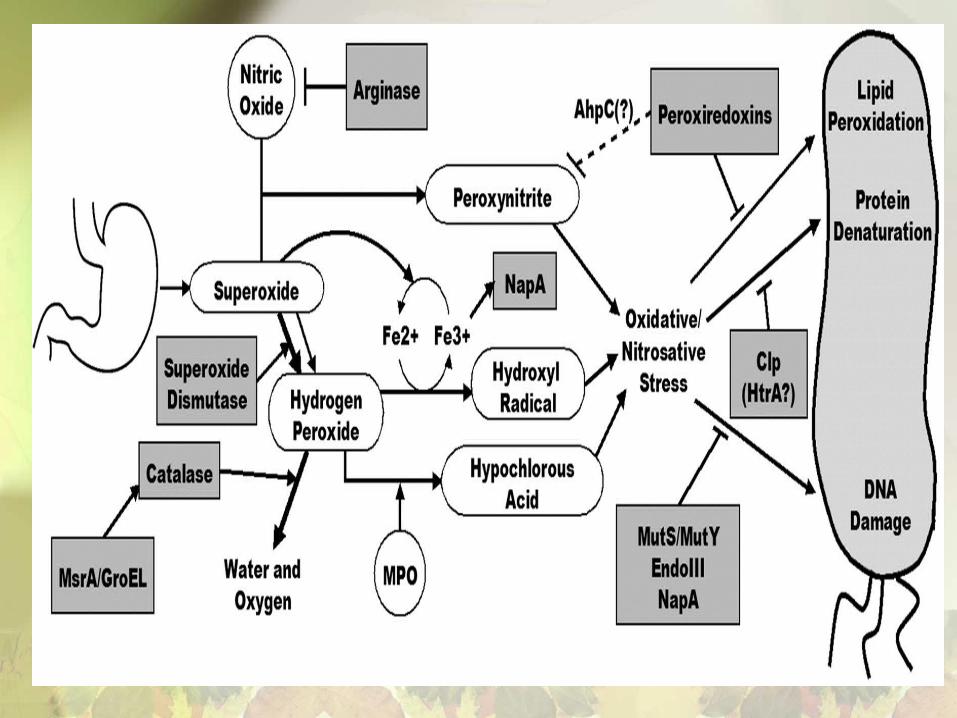
Detoxification
• H. pylori microaerophilic and able to protect themselves from the
toxic products of oxygen metabolism
• H. pylori possess a superoxide dismutase and a catalase
• H. pylori has two genes encoding peroxidases (JHP991/HP0390 and
JHP1471/HP1563) located adjacent to the superoxide dismutase
gene
• Theability to isolate catalase-negative mutants of H. pylori suggests
that at least one of the peroxidases can function as a catalase

The ecological niche of H pylori
• pH 6-8 Optimum for H.pylori growth(growth or
protein synthesis)
• for effective colonisation, the periplasmic pH
must be kept within those pH 6-8
• H pylori would inhabit only those regions of
the gastric mucosal surface that remain largely
within this pH range
• population of Fundus of stomach is sparse but
population of is high Antral(absence of acid
secretion and the presence of HCO3)

• The organism is motile but pH not affect on chemotaxis of
Helicobacteria
• If the gastric pH is changed, intragastric population would tend
to redistribute on the gastric surface
• the ability of the bacteria to colonise the gastric surface where
the pH is between 3.0 and 6.0
• Hence with proton pump inhibition the antrum would tend to
lose organisms but the fundus would tend to acquire organisms
where the surface pH would exceed 3.0
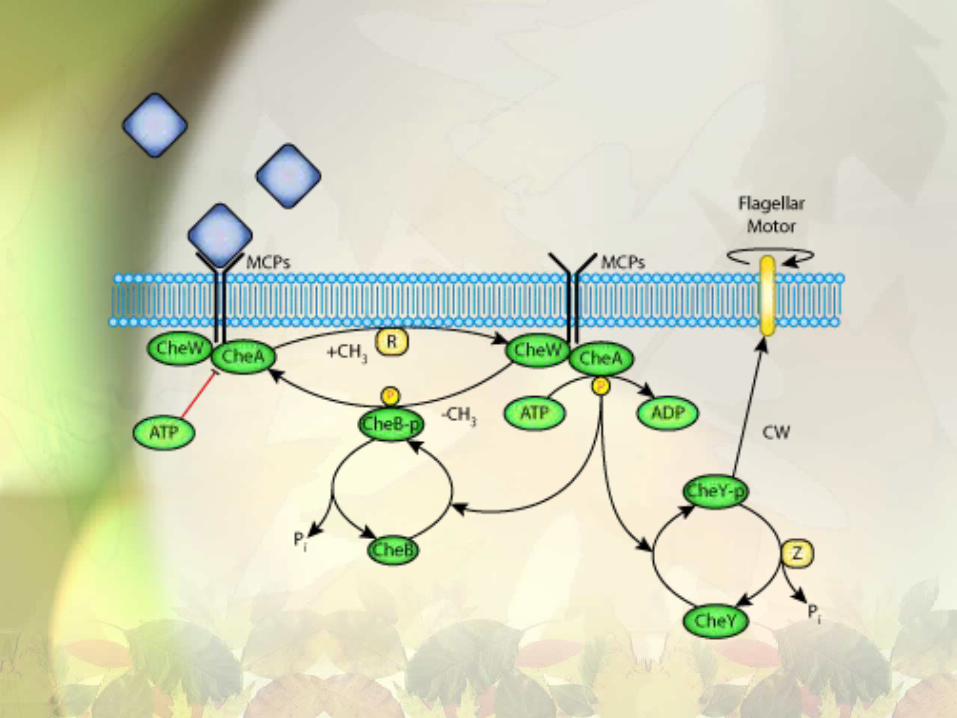
Chemotaxis
• H. pylori motile bacteri and have chemotaxi like
other motile bacteria
• Three homologues of the chemotaxis pathway in
E. coli (CheW, CheA, and CheY)
• four methyl-accepting chemotaxis proteins
(MCPs), which mediate specificity for
ligands,sens environment conditions

Strategies for eradication

2013 regimens • Triple therapy:
• proton pump inhibitor (PPI) (lansoprazole 30 mg twice daily, omeprazole 20 mg twice daily, pantoprazole 40 mg twice daily, rabeprazole 20 mg twice daily, or esomeprazole 40 mg once daily), amoxicillin (1 g twice daily), and clarithromycin (500 mg twice daily) for 7 to 14 days. We suggest treatment for 10 days to two weeks.
• Quadruple therapy
• bismuth (525 mg four times daily) and two antibiotics (eg, metronidazole 250 mg four times daily and tetracycline 500 mg four times daily) given for 10 to 14 days. Quadruple therapy is appropriate as initial therapy in areas in which the prevalence of resistance to clarithromycin or metronidazole is ≥15 percent, or in patients with recent or repeated exposure to clarithromycin or metronidazole [18]. If tetracycline is not available, doxycycline (100 mg twice daily) may be substituted

1. PETER DOIG,1* BOUDEWIJN L. DE JONGE,1 RICHARD A. ALM.et al. Helicobacter pylori Physiology Predicted from Genomic Comparison of Two Strains. MICROBIOLOGY AND MOLECULAR BIOLOGY REVIEWS, Sept. 2006, p. 675–707
2. David j. KellyThe Physiology and Metabolism of the Human Gastric PathogenHelicobacter pylori. Advances in Microbial Physiology. Volume 40 .1998, Pages 137–189
3. D Scott, D Weeks, K Melchers, et al. The life and death of helicobacter pylori . Gut 1998;43(suppl 1):S56–S60
4. Marco Romano, and Antonio Cuomo. Eradication of Helicobacter pylori: A Clinical Update. MedGenMed. 2004; 6(1): 19.
5. Sheila E Crowe. Treatment regimens for Helicobacter pylori. Gut2013 . : 19,


















